Back to Journals » Infection and Drug Resistance » Volume 19
Phenotypic Detection of Extended-Spectrum β-Lactamase and Antimicrobial Resistance Patterns in Multidrug-Resistant Uropathogenic Enterobacterales at a Tertiary-Care Hospital in Bangladesh
Authors Biswas P ![]() , Setu SK
, Setu SK ![]() , Sattar ANI
, Sattar ANI ![]() , Avi AD
, Avi AD ![]()
Received 9 April 2026
Accepted for publication 22 June 2026
Published 30 June 2026 Volume 2026:19 615697
DOI https://doi.org/10.2147/IDR.S615697
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hazrat Bilal
Pratik Biswas, Sanjida Khondakar Setu, Abu Naser Ibne Sattar, Avik Dey Avi
Department of Microbiology and Immunology, Bangladesh Medical University, Dhaka, Bangladesh
Correspondence: Pratik Biswas, Email [email protected]
Background: Urinary tract infections (UTIs) are common bacterial infections worldwide, and increasing multidrug resistance (MDR) and extended-spectrum β-lactamase (ESBL) production among uropathogenic Enterobacterales have increasingly limited empirical and targeted treatment options, particularly in low- and middle-income countries.
Methods: This laboratory-based cross-sectional study was conducted at Bangladesh Medical University, Dhaka, Bangladesh. Eligible MDR uropathogenic Enterobacterales isolates from routine diagnostic urine specimens were collected and tested after Institutional Review Board approval on 13 July 2025. Urine specimens were obtained as part of standard hospital diagnostic procedures from patients with suspected UTI. A total of 122 MDR isolates were included. Bacterial identification was performed using conventional biochemical methods. Antimicrobial susceptibility testing was performed by Kirby–Bauer disk diffusion following CLSI 2024 guidelines, and phenotypic ESBL production was detected by the double-disc synergy test. MDR classification was based on the complete routine antimicrobial susceptibility testing record, including amikacin and gentamicin. Descriptive statistics and exact binomial 95% confidence intervals (CIs) were calculated.
Results: Among these 122 MDR isolates, Escherichia coli was predominant (81/122, 66.4%), followed by Klebsiella spp. (38/122, 31.1%) and Proteus spp. (3/122, 2.5%). Resistance was highest to nalidixic acid (122/122, 100.0%), ceftazidime (117/122, 95.9%), ceftriaxone (116/122, 95.1%), cefepime (113/122, 92.6%), ciprofloxacin (106/122, 86.9%), and meropenem (27/122, 22.1%). Phenotypic ESBL production was identified in 59/122 isolates (48.4%; 95% CI: 39.2– 57.6%). DDST-positive isolates showed descriptively higher cephalosporin resistance than DDST-negative isolates, while ciprofloxacin resistance was similarly high in both groups. In this dataset, meropenem resistance was observed only among DDST-negative isolates.
Conclusion: Among MDR uropathogenic Enterobacterales from a single tertiary-care hospital in Bangladesh, ciprofloxacin and cephalosporin resistance and phenotypic ESBL production were high. Findings support routine ESBL screening, local susceptibility surveillance, and antimicrobial stewardship, but should be interpreted within the study’s MDR-only, single-center scope.
Keywords: urinary tract infection, antimicrobial resistance, ESBL, multidrug-resistant Enterobacterales, double-disc synergy test, Bangladesh
Introduction
Urinary tract infections (UTIs) are among the most common bacterial infections worldwide and are a major cause of morbidity in both community and hospital settings. Uropathogenic Enterobacterales, particularly Escherichia coli and Klebsiella spp., are the predominant etiological agents of these infections.1 In Bangladesh, previous studies have similarly shown E. coli as the leading uropathogen, accounting for 51.6% of community-acquired UTI isolates in Dhaka and 45.24% of urinary isolates in southeastern Bangladesh, while Klebsiella spp. accounted for 12.1% and 20.95% of isolates, respectively.2,3
In recent decades, antimicrobial resistance among uropathogens has increased substantially, posing a significant global public health challenge. The emergence of multidrug-resistant (MDR) strains has complicated empirical treatment and is associated with increased morbidity, healthcare costs, and treatment failure.4 MDR is commonly defined as non-susceptibility to at least one agent in three or more antimicrobial categories.5 In low- and middle-income countries such as Bangladesh, resistance to commonly prescribed antibiotics, including ciprofloxacin and third-generation cephalosporins, has risen markedly.2 A recent tertiary-care hospital study from Dhaka reported that 71.19% of bacterial uropathogens were MDR and 84.27% were resistant to at least one antibiotic, with MDR detected in 73.90% of E. coli and 48.95% of Klebsiella spp. isolates.6 Another study among complicated UTI patients in Dhaka reported E. coli and K. pneumoniae as major pathogens, accounting for 49% and 25% of isolates, respectively.7 Although oral agents such as nitrofurantoin and fosfomycin remain important options for uncomplicated UTIs, antimicrobial selection should be guided by local susceptibility data and clinical context.
One of the key mechanisms of β-lactam resistance in Enterobacterales is the production of extended-spectrum β-lactamases (ESBLs), which hydrolyze a wide range of β-lactam antibiotics, including third-generation cephalosporins and aztreonam. Phenotypic detection of ESBL-producing organisms remains important in routine clinical microbiology laboratories because it helps guide antimicrobial therapy and infection control strategies. The double-disc synergy test (DDST) is a practical phenotypic method for ESBL detection, particularly in resource-limited settings, because it demonstrates enhancement of cephalosporin inhibition zones in the presence of clavulanate.8,9
Despite increasing reports of antimicrobial resistance among uropathogens in Bangladesh, focused data on phenotypic ESBL production and antimicrobial resistance patterns among MDR uropathogenic Enterobacterales remain limited. Therefore, this study aimed to determine antimicrobial resistance patterns and phenotypic ESBL production among MDR uropathogenic Enterobacterales isolated from urine specimens at a tertiary-care hospital in Bangladesh.
Materials and Methods
Study Design and Setting
This laboratory-based cross-sectional study was conducted in the Department of Microbiology and Immunology, Bangladesh Medical University (BMU), Dhaka, Bangladesh, after obtaining Institutional Review Board approval. Sample collection and laboratory testing for the present study were performed only after Institutional Review Board approval on 13 July 2025 and continued through September 2025. Data cleaning, analysis, and manuscript preparation were performed after completion of laboratory testing.
Study Isolates
A convenience sample of 122 eligible MDR uropathogenic Enterobacterales isolates recovered from urine specimens of patients with suspected urinary tract infections was included in the study. No random sampling was performed. Patients were considered to have suspected UTI when urine specimens were submitted to the microbiology laboratory for culture based on clinical suspicion of UTI and/or clinician request. Urine specimens were collected as part of routine hospital diagnostic procedures and were not collected specifically for the purpose of this study.
Significant bacteriuria was interpreted according to the routine diagnostic criteria of the microbiology laboratory. For clean-catch midstream urine specimens, significant bacteriuria was considered as bacterial growth of ≥105 colony-forming units (CFU)/mL. For catheterized or other non-midstream urine specimens, lower colony counts were interpreted according to the specimen type, clinical context, and routine laboratory protocol.
The study focused on Escherichia coli, Klebsiella spp., and Proteus spp. isolated from urine samples and identified as MDR Enterobacterales. Only one isolate per patient was included in the analysis to avoid duplication. When more than one eligible isolate was recovered from the same patient, the first eligible MDR Enterobacterales isolate was included.
Detailed patient-level demographic and clinical data, including age, sex, inpatient or outpatient status, originating department, complicated versus uncomplicated UTI, cystitis versus pyelonephritis, community-acquired versus hospital-associated infection, and polymicrobial infection details, were not available in the anonymized laboratory dataset.
Bacterial Identification
Urine specimens were cultured on MacConkey agar and blood agar and incubated at 37°C for 24 hours. Bacterial isolates were identified using standard microbiological procedures based on colony morphology and conventional biochemical tests, including indole production, citrate utilization, urease production, motility testing, and Kligler iron agar reactions. These conventional microbiological methods were used in the routine laboratory workflow to identify Enterobacterales and differentiate them from non-Enterobacterales organisms.
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing was performed by the Kirby–Bauer disk diffusion method on Mueller–Hinton agar. The antibiotic disks used for the final comparative resistance analysis included ciprofloxacin (5 µg), nalidixic acid (30 µg), ceftriaxone (30 µg), ceftazidime (30 µg), cefepime (30 µg), and meropenem (10 µg). Amikacin and gentamicin were also tested as part of the routine laboratory antimicrobial susceptibility testing panel and were used for MDR classification, but they were not included in the final comparative resistance tables. The six antibiotics summarized in the results were selected because they were consistently available as complete reportable data for all included isolates and represented quinolone, cephalosporin, and carbapenem agents of clinical relevance in the local setting. Zone diameters were interpreted according to CLSI 2024 criteria. Escherichia coli ATCC 25922 was used as the quality-control strain.10
Multidrug resistance was defined as non-susceptibility to at least one agent in three or more antimicrobial categories.5 MDR classification was assigned using the complete routine laboratory antimicrobial susceptibility record for each isolate, rather than the six antibiotics summarized in the main resistance tables alone. The routine panel included quinolone, cephalosporin, carbapenem, and aminoglycoside agents, including amikacin and gentamicin. The final comparative resistance analysis focused on ciprofloxacin, nalidixic acid, ceftriaxone, ceftazidime, cefepime, meropenem, and phenotypic ESBL production because these were the core variables selected for the present study; the absence of detailed aminoglycoside results is acknowledged as a limitation.
Phenotypic Detection of ESBL Production
Phenotypic ESBL production was assessed using the double-disc synergy test (DDST). An amoxicillin-clavulanic acid disk was placed centrally on a Mueller–Hinton agar plate, and disks containing ceftazidime and ceftriaxone were placed 20 mm away from the central disk, as previously described. Enhancement of the inhibition zone of either cephalosporin disk toward the clavulanate-containing disk was interpreted as ESBL production.9
Data Analysis
Data were entered and analyzed using statistical software (SPSS version 27). Frequencies and percentages of bacterial isolates, antimicrobial resistance patterns, and ESBL positivity were calculated using descriptive statistics. Exact binomial 95% confidence intervals were calculated for the main proportions, including organism distribution, antimicrobial resistance rates, and ESBL positivity. No inferential statistical analysis was performed because the study was descriptive in design.
Results
Distribution of Isolates
Among the 122 MDR uropathogenic Enterobacterales isolates included in the study, Escherichia coli was the predominant organism, accounting for 81/122 isolates (66.4%; 95% CI: 57.3–74.7%), followed by Klebsiella spp. with 38/122 isolates (31.1%; 95% CI: 23.1–40.2%) and Proteus spp. with 3/122 isolates (2.5%; 95% CI: 0.5–7.0%) (Table 1).
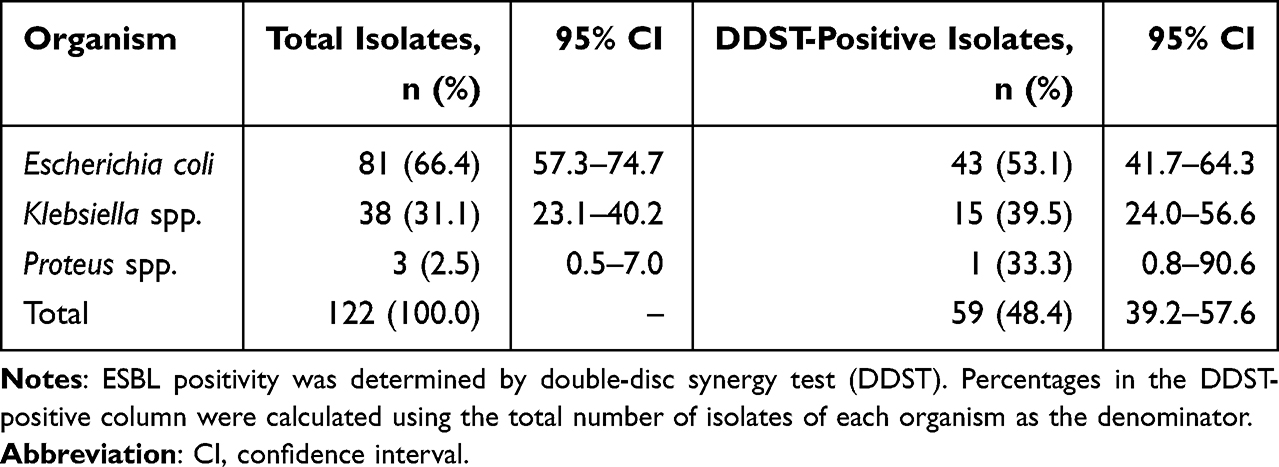 |
Table 1 Distribution of Multidrug-Resistant Uropathogenic Enterobacterales Isolates and Phenotypic ESBL Positivity (n = 122) |
Antimicrobial Resistance Pattern
The highest antimicrobial resistance rate among these MDR isolates was observed for nalidixic acid, with all isolates being resistant (122/122, 100.0%; 95% CI: 97.0–100.0%). High resistance rates were also observed for ceftazidime (117/122, 95.9%; 95% CI: 90.7–98.7%), ceftriaxone (116/122, 95.1%; 95% CI: 89.6–98.2%), cefepime (113/122, 92.6%; 95% CI: 86.5–96.6%), and ciprofloxacin (106/122, 86.9%; 95% CI: 79.6–92.3%). Meropenem resistance was detected in 27/122 isolates (22.1%; 95% CI: 15.1–30.5%) (Table 2).
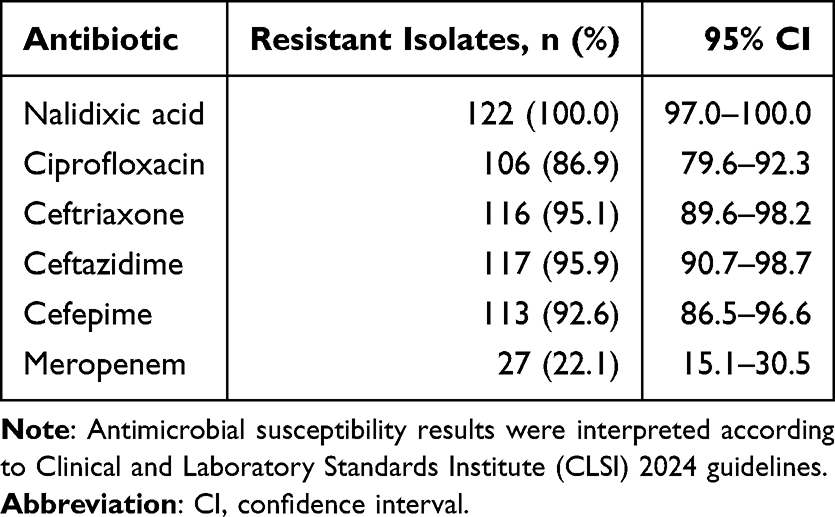 |
Table 2 Overall Antimicrobial Resistance Profile of Multidrug-Resistant Uropathogenic Enterobacterales (n = 122) |
Species-wise analysis showed that ciprofloxacin resistance was observed in 70/81 Escherichia coli MDR isolates (86.4%), 34/38 Klebsiella spp. isolates (89.5%), and 2/3 Proteus spp. isolates (66.7%). Resistance to nalidixic acid was universal in all three species. Resistance to ceftriaxone and ceftazidime was particularly high among Escherichia coli and Klebsiella spp. isolates. Meropenem resistance was more frequent among Klebsiella spp. isolates (14/38, 36.8%) than Escherichia coli isolates (13/81, 16.0%), while no meropenem resistance was observed among Proteus spp. isolates (0/3) (Table 3).
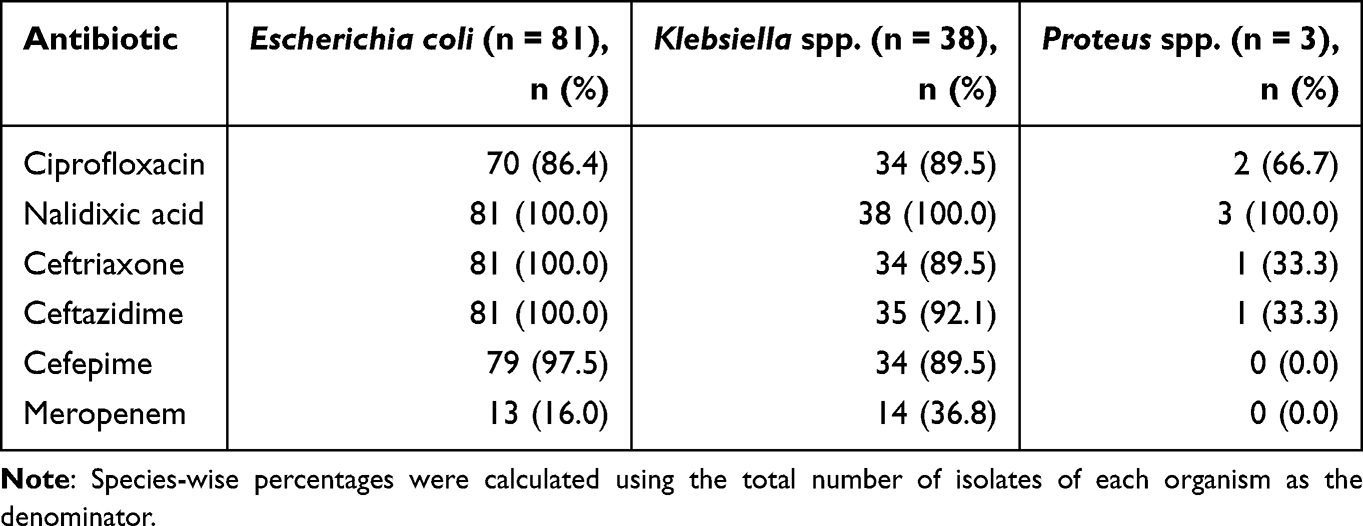 |
Table 3 Species-Wise Antimicrobial Resistance Profile of Multidrug-Resistant Uropathogenic Enterobacterales |
Phenotypic Detection of ESBL Production
Phenotypic ESBL production was detected in 59/122 MDR isolates (48.4%; 95% CI: 39.2–57.6%) by the double-disc synergy test. Species-wise, ESBL production was observed in 43/81 Escherichia coli isolates (53.1%; 95% CI: 41.7–64.3%), 15/38 Klebsiella spp. isolates (39.5%; 95% CI: 24.0–56.6%), and 1/3 Proteus spp. isolates (33.3%; 95% CI: 0.8–90.6%) (Table 1).
When antimicrobial resistance was stratified by phenotypic ESBL status, resistance to ceftriaxone, ceftazidime, and cefepime was descriptively higher among DDST-positive isolates than DDST-negative isolates. All DDST-positive isolates were resistant to ceftriaxone and ceftazidime, and 58/59 (98.3%) were resistant to cefepime. Ciprofloxacin resistance was similarly high in DDST-positive and DDST-negative isolates. Meropenem resistance was observed only among DDST-negative isolates in this dataset (27/63, 42.9%) and was not detected among DDST-positive isolates (0/59, 0.0%) (Table 4).
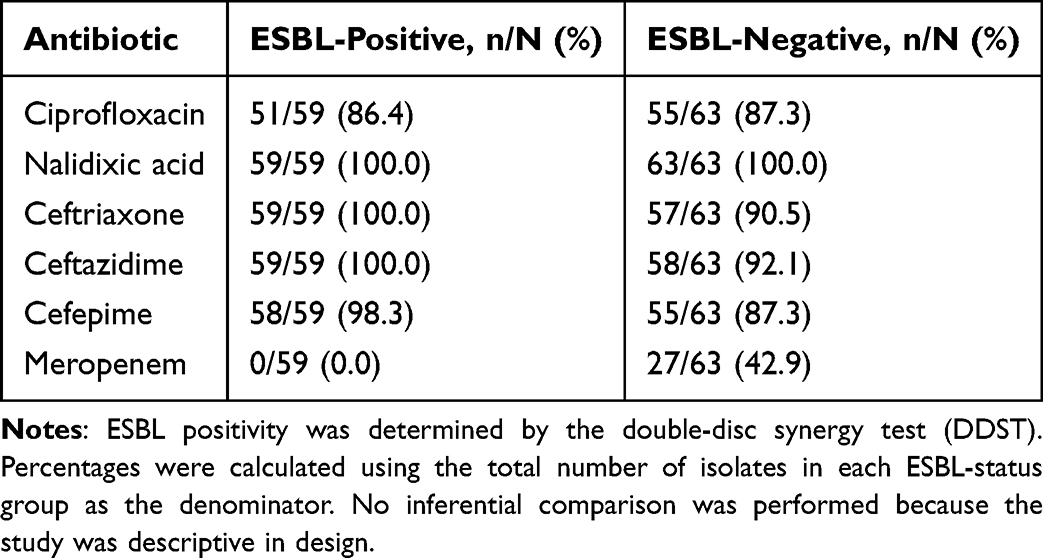 |
Table 4 Antimicrobial Resistance According to Phenotypic ESBL Status Among MDR Uropathogenic Enterobacterales |
Discussion
The present study demonstrated a substantial burden of antimicrobial resistance among MDR uropathogenic Enterobacterales in a tertiary-care hospital in Bangladesh. Escherichia coli was the predominant isolate, followed by Klebsiella spp. and Proteus spp., consistent with the established epidemiology of urinary tract infections and previous reports from Bangladesh.1,2,6,7
This organism distribution is comparable with previous Bangladeshi studies, although the proportions differ according to study population, clinical setting, and inclusion criteria. A community-acquired UTI study from Dhaka reported E. coli as the predominant causative pathogen of community-acquired UTI in Dhaka, accounting for 51.6% of isolates, followed by Klebsiella spp. at 12.1%.2 A tertiary-care hospital study of complicated UTI patients in Dhaka reported 170 culture-positive complicated UTI samples from a tertiary-care hospital in Dhaka, where E. coli accounted for 49% of isolates, followed by K. pneumoniae at 25% and P. aeruginosa at 10%.7 Similarly, a study from southeastern Bangladesh reported E. coli as the leading uropathogen, accounting for 45.24% of isolates, followed by Enterobacter spp. at 24.76% and Klebsiella spp. at 20.95%.3 In the present study, E. coli accounted for a higher proportion of isolates (66.4%), which may reflect the MDR-only Enterobacterales-focused inclusion criteria and the exclusion of non-Enterobacterales uropathogens.
The antimicrobial resistance patterns observed among these MDR isolates were particularly concerning. In the present MDR-only cohort, resistance was universal to nalidixic acid and was also very high to ceftazidime, ceftriaxone, cefepime, and ciprofloxacin, while meropenem resistance was detected in approximately one-fifth of isolates. These findings indicate that ciprofloxacin and extended-spectrum cephalosporins may have limited empirical value in MDR-enriched UTI settings. Similar concerns regarding resistance to quinolones, cephalosporins, and carbapenems have been reported in previous Bangladeshi studies and in regional data from North-East India, although direct comparison should consider differences in study population, isolate selection, and antimicrobial panels.2,3,6,7,11
Compared with previous Bangladeshi studies that included broader urinary isolate populations, the resistance rates in the present MDR-only cohort were higher, particularly for cephalosporins and ciprofloxacin. A community-acquired UTI study from Dhaka reported that E. coli and Klebsiella spp. from community-acquired UTI were resistant to third-generation cephalosporins at 69% and 58%, respectively, fluoroquinolones at 69% and 53%, respectively, and carbapenems at 5% and 9%, respectively.2 In contrast, the present MDR-only cohort showed resistance rates of 95.1% to ceftriaxone, 95.9% to ceftazidime, 92.6% to cefepime, 86.9% to ciprofloxacin, and 22.1% to meropenem. A tertiary-care hospital study from Dhaka also reported a high antimicrobial resistance burden in a tertiary-care hospital in Dhaka, with 71.19% of bacterial uropathogens classified as MDR and 84.27% resistant to at least one antibiotic; MDR was reported in 73.90% of E. coli and 48.95% of Klebsiella spp. isolates.6 These comparisons support the interpretation that the very high resistance rates in the present study reflect the MDR-only inclusion criterion rather than the overall resistance burden among all UTI isolates.
Comparable resistance concerns have also been reported regionally. In North-East India, a regional study reported resistance of more than 80% to third-generation cephalosporins and more than 45% to fluoroquinolones among clinical isolates; among third-generation cephalosporin-resistant isolates, 38% were ESBL producers only, 24% were MBL producers only, and 11% carried both ESBL and MBL genes.11 Therefore, the high cephalosporin and ciprofloxacin resistance observed in the present MDR-enriched cohort is consistent with broader South Asian resistance trends, while still requiring cautious interpretation because of differences in study design, antimicrobial panels, and isolate selection. Because the present study was restricted to MDR isolates, the resistance rates reported here should not be interpreted as representative of all uropathogens or all UTI patients.
Phenotypic ESBL production was identified in 48.4% of MDR isolates using the double-disc synergy test. This indicates that nearly half of the MDR uropathogenic Enterobacterales in this study showed phenotypic evidence of ESBL production. This finding is clinically significant and supports the role of ESBL production as a major contributor to cephalosporin resistance among urinary isolates. However, cephalosporin resistance may also be influenced by additional mechanisms that were not investigated in this study.
Stratification by phenotypic ESBL status showed that DDST-positive isolates had descriptively higher resistance to third- and fourth-generation cephalosporins than DDST-negative isolates. Resistance to ceftriaxone was observed in 100.0% of DDST-positive isolates compared with 90.5% of DDST-negative isolates, while resistance to ceftazidime was observed in 100.0% and 92.1% of isolates, respectively. Cefepime resistance was also higher among DDST-positive isolates than DDST-negative isolates (98.3% vs 87.3%). These findings support the role of ESBL production as an important contributor to cephalosporin resistance in this MDR cohort. However, ciprofloxacin resistance was similarly high in DDST-positive and DDST-negative isolates (86.4% vs 87.3%), indicating that ciprofloxacin resistance was not limited to ESBL-producing isolates. Nalidixic acid resistance was universal in both groups (100.0% each). Notably, meropenem resistance was observed only among DDST-negative isolates (42.9%) and was not detected among DDST-positive isolates (0.0%), suggesting that meropenem resistance was unlikely to be explained by DDST-detected ESBL production alone and may involve other mechanisms requiring phenotypic or molecular carbapenemase confirmation.
The ESBL frequency observed in the present MDR-only cohort is comparable to some regional reports but lower than rates reported in highly resistance-enriched MDR populations. A UTI-based study reported phenotypic ESBL production in 34.2% of Enterobacteriaceae isolated from UTIs, with high resistance among ESBL-producing isolates to several fluoroquinolones, including nalidixic acid and ciprofloxacin.12 A tertiary-care hospital study from central India reported that E. coli was the most frequently isolated uropathogen (55.3%), followed by K. pneumoniae (23.0%); E. coli showed the highest ESBL production (41.6%), followed by P. aeruginosa (36.1%).13 In contrast, a resistance-enriched study from Egypt reported a markedly higher ESBL burden among MDR E. coli isolates from different clinical specimens in Egypt, with 89.4% ESBL production; the same study also reported MBL production among 64.8% of carbapenemase-producing isolates.14 These differences emphasize that ESBL prevalence is strongly influenced by study population, isolate selection, antimicrobial exposure, and whether the study includes all urinary isolates or only MDR or otherwise resistance-enriched subsets. Therefore, the 48.4% ESBL rate observed in the present study should not be compared directly with studies including all urinary isolates, but it supports the role of ESBL production as an important resistance mechanism among MDR Enterobacterales.
In this study, ESBL-positive isolates were most frequently E. coli in absolute numbers, followed by Klebsiella spp., reflecting the overall distribution of isolates. Species-wise, phenotypic ESBL production was observed in 53.1% of E. coli, 39.5% of Klebsiella spp., and 33.3% of Proteus spp. isolates. Although E. coli accounted for most ESBL-positive isolates in absolute numbers, Klebsiella spp. remain clinically important because of their association with multidrug resistance and persistence in hospital environments under sustained antibiotic pressure. However, the very small number of Proteus spp. isolates in the present study limits meaningful interpretation of ESBL frequency in that organism group.
Meropenem resistance was observed in 22.1% of MDR isolates, with a higher rate among Klebsiella spp. than E. coli. This proportion was higher than the carbapenem resistance reported in a Dhaka community-acquired UTI study among broader community-acquired UTI isolates in Dhaka, where carbapenem resistance was 5% in E. coli and 9% in Klebsiella spp., again suggesting that the MDR-only inclusion criterion enriched the present cohort for resistant isolates.2 This finding is concerning because carbapenems are often regarded as last-resort agents for severe infections caused by resistant Gram-negative bacteria. However, meropenem resistance alone does not confirm carbapenemase production. Carbapenem resistance in Enterobacterales may result from carbapenemase production, porin loss combined with ESBL or AmpC β-lactamase activity, altered permeability, efflux mechanisms, or other resistance mechanisms. Because phenotypic carbapenemase confirmation, such as the modified carbapenem inactivation method (mCIM) or EDTA synergy testing, and molecular detection of carbapenemase genes, such as blaNDM, blaOXA-48-like, or blaKPC, were not performed, the mechanism of meropenem resistance could not be determined.10,15
These findings have important clinical and public health implications within the restricted scope of MDR uropathogenic Enterobacterales. The high ciprofloxacin and cephalosporin resistance observed in these MDR isolates suggests that empirical treatment of UTIs in comparable tertiary-care settings should be guided by updated local susceptibility data rather than by conventional prescribing habits alone. In resource-limited settings, routine phenotypic ESBL screening by DDST remains valuable because it provides clinically actionable information and can support antibiotic stewardship and infection prevention programs.8,9 However, because oral agents such as nitrofurantoin and fosfomycin were not included in the final comparative resistance analysis, the present study cannot provide direct guidance regarding these important options for uncomplicated UTI treatment.
This study has several limitations. First, it was conducted at a single tertiary-care hospital and included only available eligible MDR Enterobacterales isolates from the post-approval study period; therefore, the findings should not be generalized to all urinary isolates, uropathogens, or UTI patients. Second, the anonymized laboratory dataset lacked detailed demographic and clinical data, including age, sex, inpatient or outpatient status, UTI classification, acquisition setting, and polymicrobial infection details. The total number of urine cultures, non-Enterobacterales isolates, and the proportion of Enterobacterales among all uropathogens were also unavailable. Third, although resistance patterns were stratified by phenotypic ESBL status, species-specific ESBL-stratified comparisons were limited by small subgroup sizes, particularly for Proteus spp., and no inferential analysis was performed. Fourth, the final comparative resistance analysis was limited to six consistently reportable agents and did not include nitrofurantoin, fosfomycin, folate-pathway inhibitors, or detailed aminoglycoside resistance results, although amikacin and gentamicin contributed to MDR classification. Fifth, carbapenemase production was not confirmed phenotypically or molecularly; therefore, the mechanisms underlying meropenem resistance could not be determined. Finally, no formal sample size calculation was performed because of the descriptive design. Nonetheless, these findings provide useful local evidence on antimicrobial resistance and phenotypic ESBL production among MDR uropathogenic Enterobacterales in a tertiary-care setting in Bangladesh.
Conclusions
The present study demonstrated high ciprofloxacin and cephalosporin resistance, along with a considerable prevalence of phenotypic ESBL production, among MDR uropathogenic Enterobacterales isolated from urine specimens at a single tertiary-care hospital in Bangladesh. Meropenem resistance was also observed, particularly among Klebsiella spp.; however, carbapenemase production was not confirmed phenotypically or molecularly. These findings underscore the importance of routine phenotypic ESBL detection, updated local susceptibility surveillance, and strengthened antimicrobial stewardship to improve empirical treatment decisions and reduce the spread of resistant uropathogens. Because the study was restricted to MDR isolates from a single center, the findings should be interpreted cautiously and should not be generalized to all urinary isolates, all uropathogens, or all UTI patients.
Abbreviations
AST, antimicrobial susceptibility testing; CFU, colony-forming unit; CLSI, Clinical and Laboratory Standards Institute; DDST, double-disc synergy test; ESBL, extended-spectrum β-lactamase; MDR, multidrug-resistant; SPSS, Statistical Package for the Social Sciences; UTI, urinary tract infection.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Ethical approval for this study was obtained from the Institutional Review Board of Bangladesh Medical University (Reference: BMU/2025/10269; Registration number: 5670; Date: 13-07-2025). The study was conducted in accordance with the principles of the Declaration of Helsinki. Sample collection was performed after obtaining ethical approval. Urine specimens were collected from patients with suspected urinary tract infection as part of standard hospital diagnostic procedures and were not collected solely for research purposes. The study was conducted using bacterial isolates and anonymized laboratory records, and no patient-identifying information was included in the analysis. Therefore, the requirement for individual informed consent was waived by the Institutional Review Board.
Acknowledgments
The authors acknowledge the Department of Microbiology and Immunology, Bangladesh Medical University, for providing laboratory facilities for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Bangladesh Medical Research Council (BMRC), Dhaka, Bangladesh. Additional financial support was provided by Bangladesh Medical University (BMU), Dhaka, Bangladesh. The funding bodies had no role in study design, data collection, analysis, interpretation of data, manuscript preparation, or the decision to submit the article for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015;13(5):269–9. doi:10.1038/nrmicro3432
2. Islam MA, Islam MR, Khan R, et al. Prevalence, etiology and antibiotic resistance patterns of community-acquired urinary tract infections in Dhaka, Bangladesh. PLoS One. 2022;17(9):e0274423. doi:10.1371/journal.pone.0274423
3. Sultana KF, Akter A, Saha SR, et al. Bacterial profile, antimicrobial resistance, and molecular detection of ESBL and quinolone resistance gene of uropathogens causing urinary tract infection in the southeastern part of Bangladesh. Braz J Microbiol. 2023;54(2):803–815. doi:10.1007/s42770-023-00942-2
4. Salam MA, Al-Amin MY, Salam MT, et al. Antimicrobial resistance: a growing serious threat for global public health. Healthcare. 2023;11(13):1946. doi:10.3390/healthcare11131946
5. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
6. Chowdhury SS, Tahsin P, Xu Y, Mosaddek ASM, Muhamadali H, Goodacre R. Trends in antimicrobial resistance of uropathogens isolated from urinary tract infections in a tertiary care hospital in Dhaka, Bangladesh. Antibiotics. 2024;13(10):925. doi:10.3390/antibiotics13100925
7. Mahjabin S, Rahman R, Munni UR, Mobin ME, Pyash AS, Shoshi HR. Bacterial profile and antibiotic resistance pattern of uropathogens isolated from patients with complicated urinary tract infections in a tertiary care hospital in Dhaka, Bangladesh. BMC Infect Dis. 2025;25(1):1538. doi:10.1186/s12879-025-11941-z
8. Drieux L, Brossier F, Sougakoff W, Jarlier V. Phenotypic detection of extended-spectrum β-lactamase production in Enterobacteriaceae: review and bench guide. Clin Microbiol Infect. 2008;14(Suppl 1):90–103. doi:10.1111/j.1469-0691.2007.01846.x
9. Biswas SM, Mia MRA, Ara N, Ibrahim M, Nasir TA, Yunus S. Comparison of three dimensional test and double disc synergy test for detection of extended-spectrum β-lactamase-producing gram-negative bacteria. Pulse. 2014;6(1–2):12–19. doi:10.3329/pulse.v6i1-2.20328
10. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing. In: CLSI Supplement M100.
11. Kar B, Sharma M, Peter A, et al. Prevalence and molecular characterization of β-lactamase producers and fluoroquinolone-resistant clinical isolates from North East India. J Infect Public Health. 2021;14(5):628–637. doi:10.1016/j.jiph.2021.02.007
12. Azargun R, Sadeghi MR, Soroush Barhaghi MH, et al. The prevalence of plasmid-mediated quinolone resistance and ESBL-production in Enterobacteriaceae isolated from urinary tract infections. Infect Drug Resist. 2018;11:1007–1014. doi:10.2147/IDR.S160720
13. Bajpai T, Pandey M, Varma M, Bhatambare GS. Prevalence of extended spectrum beta-lactamase producing uropathogens and their antibiotic resistance profile in patients visiting a tertiary care hospital in central India: implications on empiric therapy. Indian J Pathol Microbiol. 2014;57(3):407–412. doi:10.4103/0377-4929.138733
14. Masoud SM, Abd El-Baky RM, Aly SA, Ibrahem RA. Co-existence of certain ESBLs, MBLs and plasmid-mediated quinolone resistance genes among MDR E. coli isolated from different clinical specimens in Egypt. Antibiotics. 2021;10(7):835. doi:10.3390/antibiotics10070835
15. Codjoe FS, Donkor ES. Carbapenem resistance: a review. Med Sci. 2017;6(1):1. doi:10.3390/medsci6010001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Drug Resistance Patterns and Pathogen Distribution in Patients with Urinary Tract Infection in Suzhou, China: A Five-Year Retrospective Study (2020–2024)
Gao J, Wu F, Zhang Y, Wu J, Li W, Su N, Wang Y
Infection and Drug Resistance 2026, 19:554982
Published Date: 29 January 2026
Bacteriological Profile and Antibiotic Resistance Patterns of Uropathogenic Bacteria at HPGRB
Cito B, Corneille KA, Gates IM, Bruno KK, Ruhimbasa KC, Gloire MH, Bahaya J, Kawala ZL, Makeshe OM, Lupande Mwenebitu D
Infection and Drug Resistance 2026, 19:603097
Published Date: 20 April 2026