Back to Journals » International Journal of General Medicine » Volume 19
Downregulated LINC02381 Predicts Tumor Progression and Correlates with Poor Survival in Gastric Cancer
Authors Wang D, Zhou J, Ding T, Yu J ![]()
Received 28 April 2026
Accepted for publication 25 June 2026
Published 9 July 2026 Volume 2026:19 620746
DOI https://doi.org/10.2147/IJGM.S620746
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Dana Kristjansson
Dong Wang,1,* Jiahui Zhou,1,* Tangdan Ding,1 Jingcui Yu1,2
1Scientific Research Centre, The Second Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang, People’s Republic of China; 2Key Laboratory of Preservation of Human Genetic Resources and Disease Control in China (Harbin Medical University), Ministry of Education, Harbin, Heilongjiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingcui Yu, Scientific Research Centre, The Second Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang, People’s Republic of China, Tel +86 451 86605908, Email [email protected]
Purpose: The elevated incidence and mortality rates of gastric cancer (GC) highlight the urgent need to identify novel prognostic biomarkers. In this study, we aimed to evaluate the expression of LINC02381 in GC tissues and its correlation with clinicopathological features, and to assess its prognostic significance.
Methods: The expression of LINC02381 was assessed in 49 cases of GC tissues and noncancerous gastric tissues using real-time PCR. The correlation between the expression of LINC02381 and the clinicopathological parameters of GC patients was analyzed by in situ hybridization histochemistry (ISHH) in 78 GC tissues. Subsequently, univariate and multivariable Cox regression analysis, and Kaplan-Meier survival analysis were performed to correlate with clinicopathological variables.
Results: We found the expression of LINC02381 was decreased in GC tissues (P< 0.05) and was correlated with poorly differentiated GC (Grade III/IV) (P< 0.05). Kaplan-Meier survival analysis showed that the low expression of LINC02381 was significantly correlated with the overall survival rate of patients for GC, GC patients with low expression of LINC02381 had a poor prognosis (P< 0.05). Univariate Cox regression analysis showed the expression of LINC02381, tumor size, grade, T stage, and N stage were associated with the prognosis of GC. Multivariate Cox regression analysis revealed that N stage remained an independent prognostic factor.
Conclusion: LINC02381 is downregulated in GC tissues, and its low expression is associated with malignant progression and shorter survival. Although not an independent prognostic factor, it may serve as a potential adjunct prognostic indicator for GC.
Keywords: gastric cancer, LINC02381, prognosis, ISHH
Introduction
Globally, gastric cancer (GC) ranks as the fifth most prevalent malignant tumor and stands as the fourth leading cause of cancer-related deaths.1 Unfortunately, despite its prevalent occurrence, most patients of GC are diagnosed at advanced stages with poor prognosis, primarily due to the absence of discernible clinical indications.2 Even after receiving radical resection and adjuvant therapy, postoperative recurrence and mortality rates remain persistently high, with the 5-year overall survival rate for patients with stage IV GC being merely 29.0% (± 3.9%).3 This underscores the major challenges in achieving long-term survival for GC patients. Therefore, there is an urgent need to identify novel molecular prognostic markers for GC and explore more effective therapeutic strategies.
Genomics studies have revealed that less than 2% of mammalian genomes are transcribed into proteins, while over 98% are transcribed into non-coding RNAs (ncRNAs).4 Based on their length, ncRNAs are classified into small non-coding RNAs (sncRNAs) and long non-coding RNAs (lncRNAs), with lncRNAs playing a crucial role as potential regulators in physiological processes, particularly at the levels of gene expression and protein synthesis.5,6 Importantly, functional lncRNAs have been shown to regulate the progression of many types of tumors, acting as either oncogenes or tumor suppressors, this indicates that lncRNAs possess significant potential as novel biomarkers and therapeutic targets for cancer.7,8 LncRNA LINC02381 (aliases: LOC400043, RP11-834C11.4) is a well-characterized competing endogenous RNA (ceRNA) that exhibits context-dependent dual roles in tumorigenesis. It exerts tumor-suppressive effects in colorectal cancer, where it partially regulates the PI3K/Akt pathway by upregulating PTEN and downregulating phosphorylated Akt,9 and in breast cancer, where its downregulation correlates with aggressive features including lymph node metastasis and estrogen receptor positivity.10 Conversely, LINC02381 acts as an oncogene in cervical cancer by sponging miR-133b to promote cell proliferation, migration, and invasion;11 in osteosarcoma, its overexpression is associated with advanced disease and poor prognosis via the LINC02381/miR-503-5p/CDCA4 axis,12 and in glioma, it interacts with transcription factor CEBPβ to synergistically activate CBX5 transcription.13 In 2021, Pan et al constructed a prognostic model for GC patients using GEO datasets, in which LINC02381 was included as one of six risk genes involved in predicting clinical features and survival outcomes in GC patients.14 This study provides important preliminary evidence for the prognostic potential of LINC02381 in GC. However, no independent clinical validation of this potential has been reported in the literature to date, which limits its clinical application as a prognostic biomarker for GC.
In this study, we first profiled LINC02381 expression in GC tissues and found it to be significantly downregulated. Subsequently, we further investigated the association of LINC02381 expression with clinicopathological parameters and the prognosis of GC patients, to assess its potential prognostic value in GC.
Materials and Methods
Tissues and Tissue Microarray
A total of 49 cases of GC and their paired corresponding noncancerous gastric (NG) tissues were collected from patients who underwent surgical resection between 2018 and 2019. The inclusion criteria were as follows: (1) patients had not received any preoperative radiotherapy, chemotherapy, or other anticancer treatments; (2) no history of concurrent or previous malignant tumors. This study was approved by the Ethics Committee of the Second Affiliated Hospital of Harbin Medical University (Ethics Number: KY2018-369).
The tissue microarray containing 90 cases of primary GC tissues (Serial number: HStmA180Su11) with corresponding clinicopathological information was purchased from Shanghai Outdo Biotech Co., Ltd. After excluding 3 cases of tissue detachment (C07, D07, G17), 1 case of nonspecific stromal staining (I03), and 8 cases without GC epithelium (A15, B01, B03, F03, F11, F13, H13, I15), the actual remaining valid information encompassed 78 cases of GC, with 1 case missing tumor size information. The follow-up period for all cases commenced in July 2015 and lasted for 7 to 7.4 years, during which 58 GC patients were confirmed deceased. Prior to the experiment, the tissue microarray was approved by the Ethics Committee of Shanghai Outdo Biotech Co. Ltd. (YB M-05-02).
Real-Time PCR
For each case, approximately 0.1g of tissue was taken and ground with liquid nitrogen, followed by transfer into a 1.5mL microcentrifuge tube. The total RNA from these tissues was extracted using TRIzol reagent (Invitrogen, 66003, USA) and subsequently reverse transcribed into cDNA using the All-in-one First Strand cDNA Synthesis Kit (SEVEN, SM131, China). All PCR reactions were carried out using the 2 × SYBR Green qPCR Master Mix (SEVEN, SM133, China). The expression differences of LINC02381 between different tissue samples were normalized against β-actin and presented as fold differences (2−ΔΔ CT). The sequences of the PCR primers are provided as follows:
LINC02381-forward, 5′-GTGGAGGAACAGAAGTGAAATGA-3′
LINC02381-reverse, 5′-CAATGCTTGGCACAGAATAGGTA-3′
β-actin-forward, 5′-ACCGCGAGAAGATGACCCAG-3′
β-actin-reverse, 5′-TTAATGTCACGCACGATTTCCC-3′
Data Collection and Analysis
The RNA level of LINC02381 in 408 GC tissues and 211 normal gastric tissues (comprising 36 normal tissues and 175 stomach tissues) were performed via the Gene Expression Profiling Interactive Analysis (GEPIA) databases, available at https://gepia2.cancer-pku.cn.
In situ Hybridization Histochemistry (ISHH)
The tissue microarray was baked at 63°C, followed by dewaxing with xylene and alcohol. After digestion with proteinase K (SIGMA, 39450–01-6, Germany) and washing with PBS, dehydration was performed. Subsequently, 20μL of hybridization solution (Exiqon, America) was added to the tissue microarray, which was then sealed and hybridized at 50°C. After hybridization, gradient washing was conducted using the Roche DIG Wash and Block Buffer set (Roche, 11585762001, Switzerland), followed by blocking with Block Buffer. After blocking, the tissue microarray was incubated with a 1:800 dilution of anti-DIG-AP Fab fragments (Roche, 11093274910, Switzerland) at 4°C overnight. Then, following the instructions of the BCIP/NBT Substrate kit (VECTOR Laboratories, SK-5400, United States), the color development process was carried out under light-blocking conditions. After that, the tissue microarray was counterstained using Nuclear Fast Red Staining Solution (Beyotime, C0151, China). Subsequently, the tissue microarray was mounted with neutral resin and observed and photographed under a microscope (NIKON, YS100, Japan).
The results of ISHH were evaluated using the immunoreactivity score (IRS) system and were evaluated in a blinded manner by two independent, board-certified pathologists who were unaware of the patients’ clinical and survival data. Inter-observer discrepancies in scoring were resolved via consensus discussion. If no consensus was reached, a third senior pathologist was consulted to render the final decision. Specifically, Staining intensity: 0 points for negative, 1 point for 1+, 2 points for 2+, and 3 points for 3+. Ratio of positive cells: 0 points for negative, 1 point for 1%~25%, 2 points for 26%~50%, 3 points for 51%~75%, and 4 points for 76%~100%. The IRS score was calculated by multiplying the staining intensity and the ratio of positive cells. The cutoff value for defining high versus low LINC02381 expression was set at the median IRS score of all samples (0.1). An IRS score of less than 0.1 is considered negative (low expression), while a score of 0.1 or above is considered positive (high expression).
Statistical Analysis
Statistical analysis and graphing were performed using GraphPad Prism 10.0 software or R software. Experimental data were expressed as mean ± SD. Normality of data distribution was assessed using the Shapiro–Wilk test. For normally distributed data, paired-sample t-tests were used for statistical analysis, while Wilcoxon rank-sum tests were employed for non-normally distributed data. Chi-square tests were applied to analyze the correlation between the LINC02381 expression in GC tissues and the clinicopathological parameters of GC patients. Kaplan-Meier method was used to evaluate the survival prognosis of GC patients, and Log rank tests were performed for statistical analysis. The risk factors affecting the survival of GC patients were assessed using univariate and multivariate Cox proportional hazards regression models. Variables with P<0.05 in univariate analysis were included in the multivariate Cox regression model. P<0.05 was considered statistically significant.
Results
The Expression of LINC02381 was Decreased in Gastric Cancers
To elucidate the expression pattern of LINC02381 in gastric cancer (GC), we conducted an analysis of RNA-sequencing data from the GEPIA database, encompassing 408 GC tissues and 211 gastric tissues and revealed a distinct downregulation of LINC02381 RNA levels in GC tissues compared to those observed in gastric tissues (Figure 1A, P<0.05). Subsequently, real-time PCR analysis was conducted to determine the expression levels of LINC02381 in a cohort of 49 patients, specifically comparing collected GC tissues with non-cancerous gastric (NG) tissues. The findings, presented in Figure 1B, showed a statistically significant decrease in LINC02381 expression in GC tissues compared to NG tissues (P<0.05). Furthermore, we performed an individualized, paired comparative analysis among the 49 patients, assessing the expression levels of LINC02381 specifically in their matched GC and NG tissue samples. As depicted in Figure 1C, an majority of patients (87.76%, 43 out of 49) exhibited a notable downregulation of LINC02381 expression in GC tissues compared to their corresponding NG tissues. These findings consistently demonstrate significant downregulation of LINC02381 in GC.
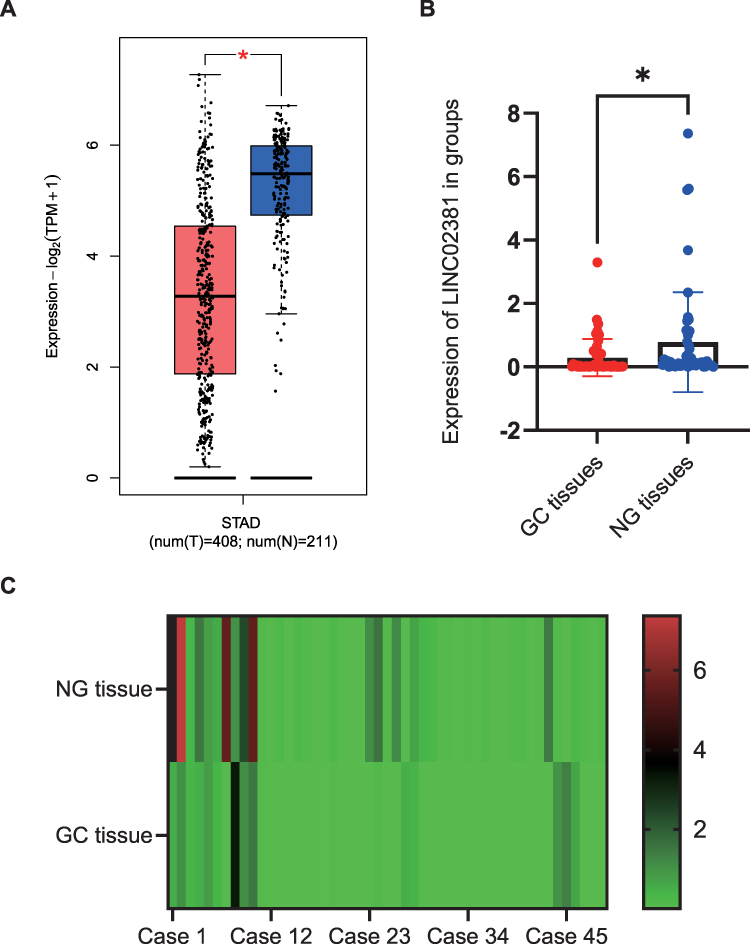 |
Figure 1 The expression analysis of LINC02381 in gastric cancer. (A) The RNA level of LINC02381 (ENSG00000250742) in 408 GC tissues and 211 gastric tissues using GEPIA database. (B) The expression of LINC02381 in 49 GC tissues and 49 NG tissues. (C) Heat maps showing the personalized comparative analysis of LINC02381 expression in GC patients. (*P< 0.05). |
Decreased Expression of LINC02381 is Involved in the Process of Gastric Cancers
Further to evaluate the clinical significance of LINC02381 in GC, we utilized in situ hybridization histochemical (ISHH) to detect the expression of LINC02381 in 78 cases of GC tissues containing valid pathological information (Figure 2A). Based on the IRS score, LINC02381 was categorized into the groups for low expression (<0.1) and high expression (>0.1) (Figure 2B). Chi-square tests were then employed to analyze the correlation between the expression of LINC02381 in GC tissues and clinicopathological parameters of GC patients. The results, as shown in Table 1, indicate that a higher proportion (76.7%, 46/60) of poorly differentiated GCs (Grade III/IV) were observed in GC patients with low LINC02381 expression, whereas in patients with high LINC02381 expression, the proportion of well-to-moderately differentiated GCs (Grade I/II) (50%, 9/18) was significantly higher than the proportion of poorly differentiated cancers (23.3%, 14/60). The low expression of LINC02381 in GC tissues was significantly associated with poorly differentiated GC (Figure 2C, P<0.05). These results suggest the decreased expression of LINC02381 in GC tissues may be involved in the differentiation process of GC.
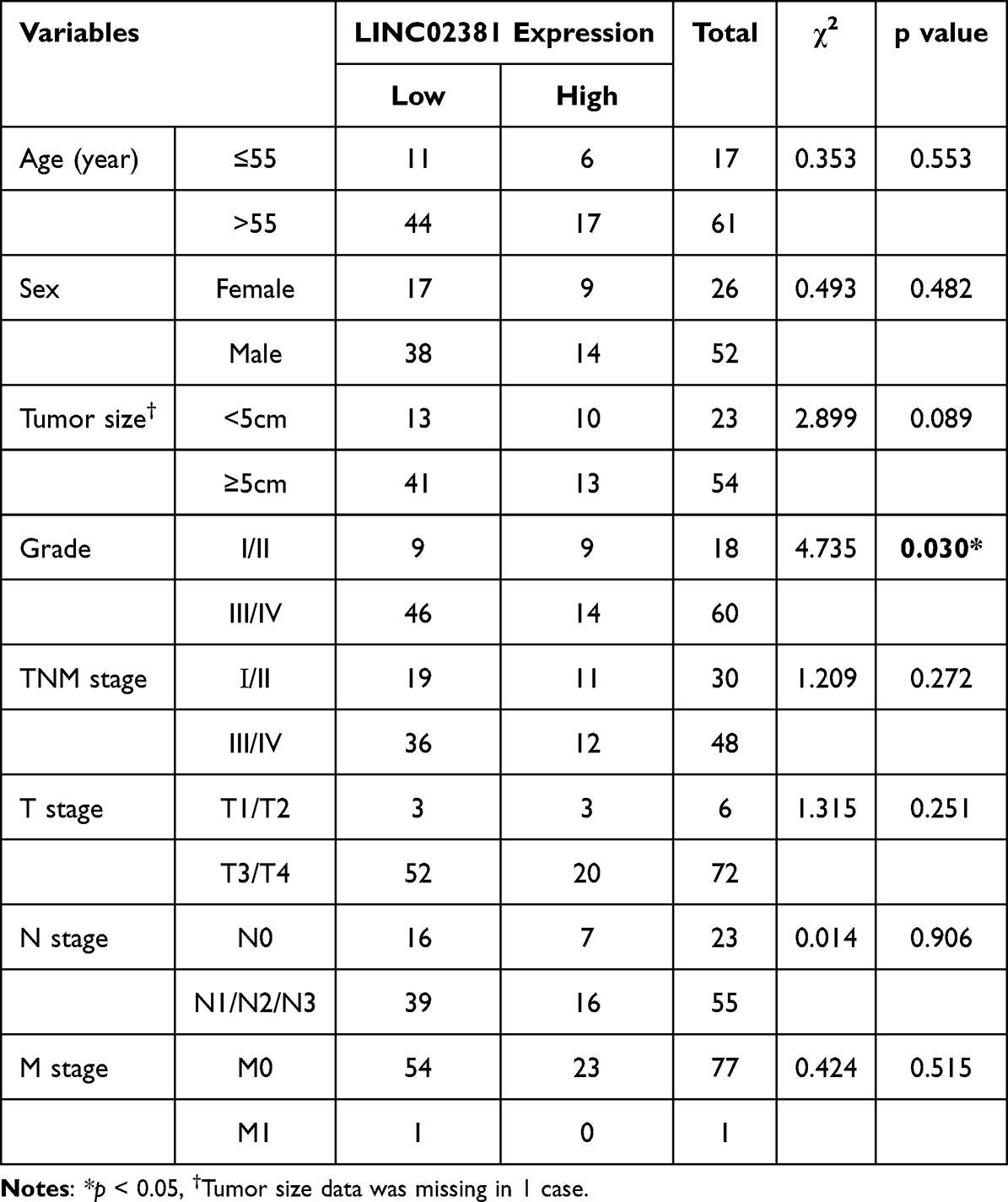 |
Table 1 Correlation Between LINC02381 Expression and Clinicopathological Characteristics in GC Tissues |
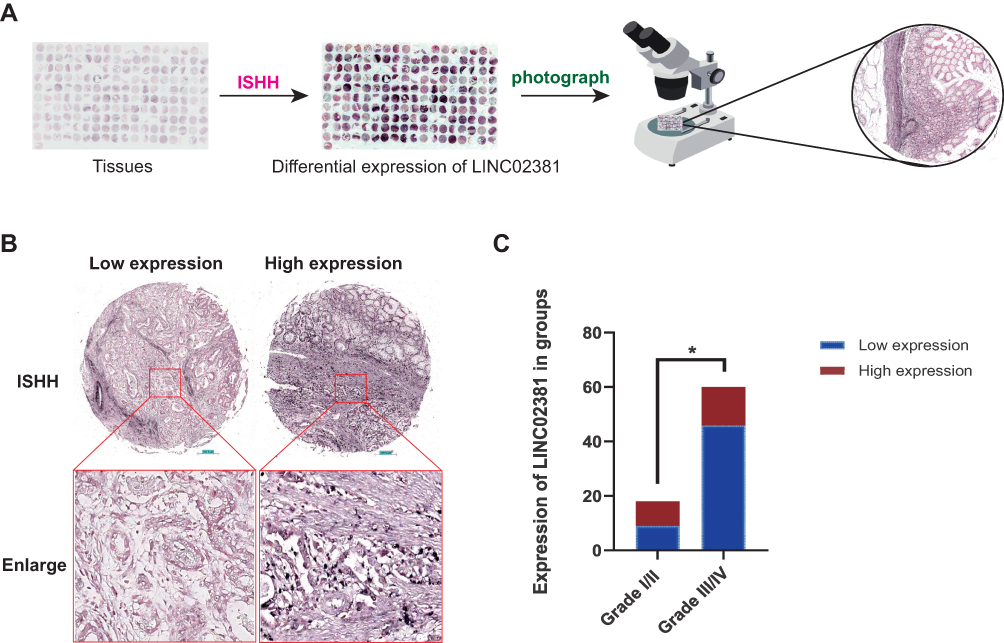 |
Figure 2 ISHH analysis of LINC02381 was performed in gastric cancers. (A) Detection and analysis flow chart of LINC02381 expression in GC tissue microarray. (B) Representative cases showing low and high expression of LINC02381 in GC tissues. (C) The relationship between the expression of LINC02381 in GC tissues and the grade stage of GC. (*p<0.05). |
Decreased Expression of LINC02381 is Association with Poor Prognosis of Gastric Cancer Patients
In order to assess the relationship between LINC02381 expression in GC tissues and the prognosis of 78 GC patients, Kaplan-Meier survival curves were employed, followed by Log-rank statistical analysis. Of these, 55 patients exhibited low LINC02381 expression, while 23 displayed high expression. As shown in Figure 3, a statistically significant correlation (P=0.026) was observed between LINC02381 expression in GC tissues and the patients’ overall survival rate. Notably, patients with low LINC02381 expression demonstrated a poorer prognosis.
 |
Figure 3 Relationship between LINC02381 expression in gastric cancer tissues and overall survival rate of gastric cancer patients. |
To further clarify the independent prognostic variables for predicting the prognosis of GC patients, we performed both univariate Cox regression (UCR) and multivariate Cox regression (MCR) analyses (Table 2). The results of the UCR analysis indicated that LINC02381 expression (P=0.048), tumor size (P=0.026), grade (P=0.045), T stage (P=0.037), and N stage (P< 0.001) could be considered as risk factors for mortality in GC patients. However, after adjusting for confounding factors in the MCR analysis, only N stage (HR=6.704, 95% CI=1.861–24.153, P=0.004) remained a statistically significant independent prognostic factor.
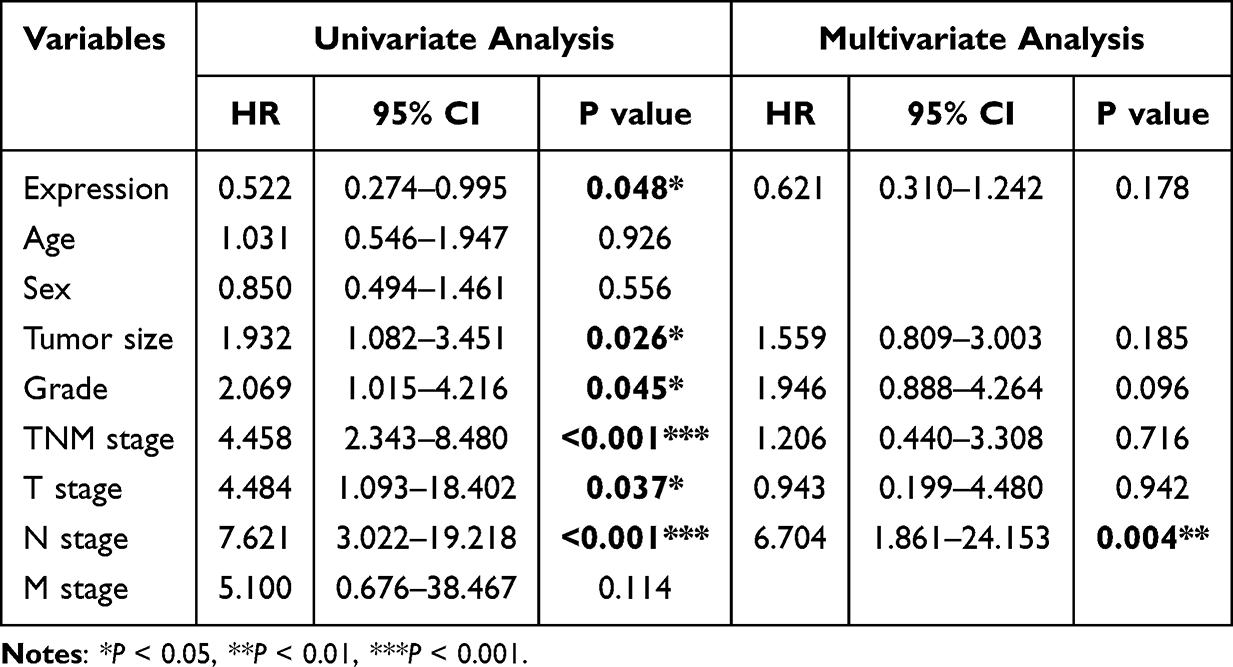 |
Table 2 Univariate and Multivariate Analysis of Factors Associated with Overall Survival in Patients with Gastric Cancer |
Discussion
The high incidence and mortality of GC underscore the urgent need to identify novel prognostic biomarkers. Recent bioinformatics study have predicted that LINC02381 may be a key component of prognostic gene signatures for GC.14 Therefore, clarifying the expression difference of LINC02381 in GC tissues and its association with the clinical prognosis of GC patients may provide additional evidence supporting its potential prognostic value in GC.
To characterize LINC02381 expression in GC, we first analyzed RNA sequencing data from 408 GC and 211 normal gastric tissues via the GEPIA database, which revealed reduced LINC02381 expression in GC. We further validated this finding using real-time PCR in 49 paired GC and NG tissues, with consistent results. The differential expression of LINC02381 in GC may indicates its potential prognostic value and suggests an association with tumor heterogeneity. In colon adenocarcinoma, the expression of LINC02381 was found to be up-regulated in tissues, and it’s up-regulation suppressed the malignant phenotype of tumor cells.9 Notably, a 2022 study identified LINC02381 as a pyroptosis-related lncRNA that is overexpressed in colon adenocarcinoma and associated with poor patient prognosis.15 Similarly, LINC02381 is overexpressed in breast cancer tissues and plays a carcinogenic role.16 Recent studies have shown that LINC02381 is significantly downregulated in breast cancer tissues and is associated with poor survival of patients.17 Therefore, we performed paired analysis of LINC02381 expression in 49 pairs of GC and NG tissues. The results indicated that the expression of LINC02381 was decreased in 87.76% (43/49) of GC tissues, accounting for the majority of cases. This further clarified the decreased expression status of LINC02381 in GC patients.
Bioinformatic analysis revealed that LINC02381 RNA expression was positively correlated with patient age and negatively correlated with T stage in colon adenocarcinoma.18 Furthermore, LINC02381 has been identified as a prognostic lncRNA associated with autophagy,19 ferroptosis,20 glycosyltransferase,21 and pyroptosis,15 and has emerged as an independent prognostic factor for colon adenocarcinoma patients.22 To clarify the clinicopathological characterization of LINC02381 in GC, we analyzed the expression of LINC02381 in 78 GC tissues containing valid case information using ISHH, and further analyzed the correlation between the expression of LINC02381 and pathological parameters as well as the survival of GC patients. Our results showed that low LINC02381 expression was significantly associated with poor histological differentiation in GC, and patients with low LINC02381 expression had shorter overall survival. However, multivariate Cox regression analysis did not confirm LINC02381 as an independent prognostic factor in our cohort, which may be due to the relatively small sample size and retrospective study design.
While our study provides robust clinical evidence, several inherent limitations should be acknowledged. As an initial clinical investigation, we employed a single-center retrospective design with a moderate sample size, which may have reduced the statistical power of multivariate analysis and explains why LINC02381 exhibited a prognostic trend but failed to achieve independent statistical significance. Additionally, our findings were derived from a single Chinese cohort and lack validation in external independent populations. Furthermore, the present study focused exclusively on clinical correlation analysis, and functional experiments were not conducted to elucidate the precise molecular mechanisms by which LINC02381 regulates GC progression. Nonetheless, these limitations do not diminish the clinical relevance of our findings, and future validation and mechanistic studies will help to confirm and extend our conclusions.
Conclusion
In conclusion, the present study provides consistent evidence that suggests LINC02381 is significantly downregulated in GC tissues, and its low expression correlates with poor histological differentiation and reduced overall survival. Although LINC02381 was not identified as an independent prognostic factor in this single-center cohort, it may have potential as an adjunct to conventional prognostic indicators for GC. Further large-scale multicenter prospective studies, functional mechanistic investigations, and exploration of integrating LINC02381 expression with existing clinical prognostic models are warranted to confirm these preliminary findings and improve survival stratification accuracy for GC patients.
Abbreviations
GC, Gastric cancer; ISHH, In situ hybridization histochemistry; ncRNAs, Non-coding RNAs; sncRNAs, Small non-coding RNAs; lncRNAs, Long non-coding RNAs; NG, Noncancerous gastric; GEPIA, Gene Expression Profiling Interactive Analysis; IRS, Immunoreactive score.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author upon request.
Ethics Approval Statement
The study was approved by the Ethics Committee of the Second Affiliated Hospital of Harbin Medical University (Ethics Number: KY2018-369), and was conducted in accordance with the World Medical Association Declaration of Helsinki. All the study participants provided informed consent.
Funding
This work was supported by the Open Project Program of Key Laboratory of Preservation of Human Genetic Resources and Disease Control in China (Harbin Medical University), Ministry of Education (No. LPHGRD2022-007), and the Innovative Scientific Research Fund of Harbin Medical University (No. 31041210020).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–9. doi:10.3322/caac.21660
2. Qiu H, Cao S, Xu R. Cancer incidence, mortality, and burden in China: a time-trend analysis and comparison with the United States and United Kingdom based on the global epidemiological data released in 2020. Cancer Commun. 2021;41(10):1037–1048. doi:10.1002/cac2.12197
3. Batra S, Bhandare MS, Chaudhari V, et al. 1657 resected gastric adenocarcinomas at a single institution: outcomes and trends over 17 years. Ann Surg Oncol. 2024;31(10):7142–7156. doi:10.1245/s10434-024-15842-4
4. Mattick JS, Rinn JL. Discovery and annotation of long noncoding RNAs. Nat Struct Mol Biol. 2015;22(1):5–7. doi:10.1038/nsmb.2942
5. Kornienko AE, Guenzl PM, Barlow DP, et al. Gene regulation by the act of long non-coding RNA transcription. BMC Biol. 2013;11:59. doi:10.1186/1741-7007-11-59
6. Peng W-X, Koirala P, Mo -Y-Y. LncRNA-mediated regulation of cell signaling in cancer. Oncogene. 2017;36(41):5661–5667. doi:10.1038/onc.2017.184
7. Beermann J, Piccoli M-T, Viereck J, et al. Non-coding RNAs in development and disease: background, mechanisms, and therapeutic approaches. Physiol Rev. 2016;96(4):1297–1325. doi:10.1152/physrev.00041.2015
8. Bhan A, Soleimani M, Mandal SS. Long noncoding RNA and cancer: a new paradigm. Cancer Res. 2017;77(15):3965–3981. doi:10.1158/0008-5472.CAN-16-2634
9. Jafarzadeh M, Soltani BM, Soleimani M, et al. Epigenetically silenced LINC02381 functions as a tumor suppressor by regulating PI3K-Akt signaling pathway. Biochimie. 2020;171–172:63–71. doi:10.1016/j.biochi.2020.02.009
10. Ghafouri-Fard S, Asadi M, Sohrabi B, et al. Down-regulation of a panel of immune-related lncRNAs in breast cancer. Pathol Res Pract. 2021;224:153534. doi:10.1016/j.prp.2021.153534
11. Chen X, Zhang Z, Ma Y, et al. LINC02381 promoted cell viability and migration via targeting miR-133b in cervical cancer cells. Cancer Manag Res. 2020;12:3971–3979. doi:10.2147/CMAR.S237285
12. Bian X, Sun Y-M, Wang L-M, et al. ELK1-induced upregulation lncRNA LINC02381 accelerates the osteosarcoma tumorigenesis through targeting CDCA4 via sponging miR-503-5p. Biochem Biophys Res Commun. 2021;548:112–119. doi:10.1016/j.bbrc.2021.02.072
13. Sun Y, Wang X, Bu X. LINC02381 contributes to cell proliferation and hinders cell apoptosis in glioma by transcriptionally enhancing CBX5. Brain Res Bull. 2021;176:121–129. doi:10.1016/j.brainresbull.2021.07.009
14. Pan S, Gao Q, Chen Q, et al. Integrative analysis-based identification and validation of a prognostic immune cell infiltration-based model for patients with advanced gastric cancer. Int Immunopharmacol. 2021;101(Pt B):108258. doi:10.1016/j.intimp.2021.108258
15. Cai X, Liang X, Wang K, et al. Pyroptosis-related lncRNAs: a novel prognosis signature of colorectal cancer. Front Oncol. 2022;12:983895. doi:10.3389/fonc.2022.983895
16. Huang S, Huang P, Wu H, et al. LINC02381 aggravates breast cancer through the miR-1271-5p/FN1 axis to activate PI3K/AKT pathway. Mol Carcinog. 2022;61(3):346–358. doi:10.1002/mc.23375
17. Golestan S, Soltani BM, Jafarzadeh M, et al. LINC02381 suppresses cell proliferation and promotes apoptosis via attenuating IGF1R/PI3K/AKT signaling pathway in breast cancer. Funct Integr Genomics. 2023;23(1):40. doi:10.1007/s10142-023-00965-w
18. Li Z, Wang D, Yin H. A seven immune-related lncRNA signature predicts the survival of patients with colon adenocarcinoma. Am J Transl Res. 2020;12(11):7060–7078.
19. Duan L, Xia Y, Li C, et al. Identification of autophagy-related LncRNA to predict the prognosis of colorectal cancer. Front Genet. 2022;13:906900. doi:10.3389/fgene.2022.906900
20. Chen W, Chen Y, Liu L, et al. Comprehensive analysis of immune infiltrates of ferroptosis-related long noncoding RNA and prediction of colon cancer patient prognoses. J Immunol Res. 2022;2022:9480628. doi:10.1155/2022/9480628
21. Zhang J, Wu Y, Mu J, et al. Glycosyltransferase-related long non-coding RNA signature predicts the prognosis of colon adenocarcinoma. Front Oncol. 2022;12:954226. doi:10.3389/fonc.2022.954226
22. Zhou W, Zhang S, Li H-B, et al. Development of prognostic indicator based on autophagy-related lncRNA analysis in colon adenocarcinoma. Biomed Res Int. 2020;2020:9807918. doi:10.1155/2020/9807918
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of an Age-Related Gastric Cancer-Specific Immune Index
Wang H, Yin X, Fang T, Lou S, Han B, Gao J, Wang Y, Zhang D, Wang X, Lu Z, Wu J, Zhang J, Wang Y, Zhang Y, Xue Y
Journal of Inflammation Research 2022, 15:6393-6407
Published Date: 23 November 2022
A Novel Neutrophil Extracellular Traps Signature for Overall Survival Prediction and Tumor Microenvironment Identification in Gastric Cancer
Qu Z, Han Y, Zhu Q, Ding W, Wang Y, Zhang Y, Wei W, Lei Y, Li M, Jiao Y, Gu K, Zhang Y
Journal of Inflammation Research 2023, 16:3419-3436
Published Date: 14 August 2023
Identification of Hub Genes Associated with Gastric Cancer via Bioinformatics Analysis and Validation Studies
Zhao T, Chen Z, Liu W, Ju H, Li F
International Journal of General Medicine 2023, 16:4835-4848
Published Date: 26 October 2023
TCHH as a Novel Prognostic Biomarker for Patients with Gastric Cancer by Bioinformatics Analysis
Yu F, Zhao LX, Chu S
Clinical and Experimental Gastroenterology 2024, 17:61-74
Published Date: 26 February 2024
High Expression of CLDN 18.2 is Associated with Poor Disease-Free Survival of HER-2 Positive Gastric Cancer
Zhang T, He Z, Liu Y, Jin L, Wang T
International Journal of General Medicine 2024, 17:1695-1705
Published Date: 29 April 2024