Back to Journals » Advances in Medical Education and Practice » Volume 16
Does Curriculum Reform Improve Clinical Practice? Comparing the Quality of Labor and Delivery Care Provided by Midwives in Ethiopia
Authors Wondie AG, Siebeck M ![]() , Sendekie TY, Fischer MR, Berndt M
, Sendekie TY, Fischer MR, Berndt M ![]()
Received 30 June 2025
Accepted for publication 11 October 2025
Published 3 December 2025 Volume 2025:16 Pages 2259—2270
DOI https://doi.org/10.2147/AMEP.S550456
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Awoke Giletew Wondie,1,2 Matthias Siebeck,3 Tegbar Y Sendekie,4 Martin R Fischer,3 Markus Berndt3
1CIH LMU, Center for International Health, LMU University Hospital, LMU, Munich, Germany; 2Department of Reproductive and Child Health, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 3Institute of Medical Education, LMU University Hospital, LMU, Munich, Germany; 4Jhpiego (An Affiliate of John Hopkins University), Addis Abeba, Ethiopia
Correspondence: Awoke Giletew Wondie, Department of Reproductive and Child Health, College of Health Sciences, Debre Tabor University, P. O. Box 272, Debre Tabor, Ethiopia, Tel +251581410495 ; +251 918727586, Fax +251581412260, Email [email protected]
Purpose: Maternal and neonatal health remains a major challenge in Ethiopia. Despite midwives’ potential to prevent over 80% of related deaths, shortages and competence gaps persist due to theory-focused preservice curricula. In 2013, Debre Tabor University introduced a competency-based midwifery curriculum. This study evaluated whether this curriculum reform improved the quality of labor and delivery care provided by midwives.
Methods: A comparative cross-sectional study was conducted among 68 BSc midwifery graduates from ten third-generation Ethiopian universities (32 trained under a competency-based curriculum; thirty-six under a conventional curriculum). Labor and delivery care quality was assessed through direct observation using a validated checklist. Additional data on birth outcomes were collected through record reviews, and facility inventories were used to evaluate the availability of essential supplies. Mean percentage scores were compared using independent t-tests and effect sizes (Cohen’s d) were visualized with Gardner–Altman plots.
Results: On average, midwives performed 75.3% of the tasks required for quality labor and delivery care, with competency-based curriculum graduates (CBCGs) scoring higher (83.3%) than conventional curriculum graduates (CCGs) (68.2%), which was consistent across all components of labor and delivery care. This difference was statistically significant (t (61.77) = 5.29, p < .001), with a large effect size (Cohen’s d = 1.26; Δ = 15%). During the initial client assessment, CBCGs more frequently inquired about vaginal bleeding and practiced hand hygiene. CBCGs also demonstrated higher performance in delivery preparation, neonatal resuscitation readiness, administering uterotonics, early breastfeeding support, and skin-to-skin contact.
Conclusion: Midwives trained under a competency-based curriculum provided higher quality labor and delivery care than the conventionally trained control group, with a large effect size, suggesting clinical relevance. However, the overall performance revealed persistent gaps, highlighting the need for further research to examine long-term outcomes to inform curriculum development and policy.
Keywords: education, competency, quality, labor and delivery, Ethiopia
Introduction
Maternal and neonatal health remain critical public health challenges in low-resource settings such as Ethiopia. Despite some progress, Ethiopia continues to experience high mortality rates, with 195 maternal deaths per 100,000 live births in 2023 and 28 neonatal deaths per 1,000 live births reported in 2022.1 Midwives are pivotal in addressing this issue, as they can provide 87% of essential maternal and neonatal care, with the potential of preventing over 80% of related deaths.2
However, the shortage of healthcare workers, coupled with low skill levels, contributes to poor-quality reproductive, maternal, newborn, and child health (RMNCH) services in Ethiopia.3 The Ethiopian government has significantly expanded midwifery training, increasing the number of practicing midwives from 12,000 in 2020 to approximately 25,285 by 2024.4,5 Yet, the country still faces a shortage of midwives to meet the recommended standards of the World Health Organization (WHO).6
Equally important, evidence from Ethiopia indicates that midwives and other healthcare providers demonstrate inadequate competence in essential obstetric and newborn care, particularly in managing postpartum hemorrhage and performing neonatal resuscitation.7 Although the average competence scores of graduating midwifery students in the core competencies outlined by the International Confederation of Midwives improved from 51.8% in 2013 to 56.6% in 2016, these levels remained suboptimal, reflecting limited proficiency.8,9 Similarly, a nationwide hospital survey identified inadequate practitioner competence as a major barrier to delivering quality emergency obstetric and neonatal care.7,10 In the Ethiopian health professional national licensing examination (which assesses the competence of graduates), the pass rate of midwifery professionals was approximately 41% in 2025.11 These shortcomings are largely attributed to weaknesses in preservice education (PSE).10,12
Effective PSE contributes significantly to the health and well-being of individuals, families, and communities by fostering high-quality services and improved health outcomes.13,14 However, PSE curricula are increasingly misaligned with evolving healthcare needs and local contexts in various countries, including Ethiopia.15 Conventional PSE curricula focus on theoretical instruction with less emphasis on practical, hands-on experience and integration between theoretical knowledge and clinical application. These models also focus on curative care and hospital-based training, neglecting primary care and community health priorities.16,17 In contrast, the competency-based curriculum is student-centered, integrates theory with practice through early and continuous clinical exposure and simulation-based learning, and facilitates the development of core competencies through continuous assessments.16–18
Historically, university midwifery education in Ethiopia was largely content-driven, with a focus on didactic lectures, limited structured clinical practice, and predominantly written summative assessments.19 Consequently, graduates of conventional programs frequently enter clinical practice with insufficient hands-on experience and inadequate preparedness to meet the demands of real-world service delivery. In contrast, the competency-based curriculum emphasizes student-centered and problem-based learning, extensive supervised clinical practice, and performance-based assessments designed to ensure graduates can demonstrate essential competencies.16,18
To address these limitations in Ethiopia, a competency-based curriculum was introduced in 2013 at Debre Tabor University (DTU) with the support of the Jhpiego-led Human Resources for Health (HRH) project, but its adoption has not been uniform across midwifery schools. Some institutions continue to implement the conventional curriculum, while DTU and subsequently other institutions have transitioned to the competency-based approach. The curriculum incorporated transformative educational strategies guided by the SPICES model (student-centered, problem-based, integrated, community-based, elective, and systematic approaches).20,21 It emphasizes early clinical immersion, integrated teaching, and alignment with instructional design principles to improve educational effectiveness and better prepare graduates for clinical practice. Unlike the conventional model, it fosters professional identity formation, improves patient communication and empathy, and strengthens diagnostic and preventive care skills.19,22,23
This reform aligns with Ethiopia’s national health workforce strategy, which prioritizes competency-based education to improve maternal and newborn outcomes. Initially piloted in selected universities, the approach has since been adopted more widely and is central to ongoing national education reforms.
While early evaluations of the competency-based curriculum have shown promise, and this reform aligns with Ethiopia’s national health workforce strategy, which prioritizes competency-based education to improve maternal and newborn outcomes, the nationwide adoption of this model has not been accompanied by a rigorous evaluation of its impact on population health outcomes.19–21 The evidence suggests that integrated teaching and early clinical exposure improve learning retention and clinical performance.24 However, there is a lack of research linking the quality of PSE with subsequent clinical practice and health outcomes (See Supplementary Figure 1).14
Therefore, this study is part of a broader study assessing the effectiveness of a competency-based curriculum on the intermediate health outcomes of the population (lifesaving practices implemented and professional behaviors) in the Ethiopian context. This paper focuses on lifesaving practices, particularly the quality of labor and delivery care, and compares the performance of recently employed midwifery graduates from competency-based and conventional curricula in their workplace.
Skilled care during childbirth is essential for reducing maternal and child mortality, making it crucial to assess how curriculum reforms influence midwifery performance. This study highlights whether curricular reform in midwifery education enhances the quality of clinical practice in labor and delivery care. The findings will inform training institutions and stakeholders in improving PSE quality and strategies for strengthening the health workforce.
Materials and Methods
Study Design
We conducted a comparative cross-sectional study to assess the labor and delivery care performance of midwives trained under a competency-based curriculum against their controls who went through a conventional curriculum.
Population
The study population consisted of recently deployed Bachelor of Sciences (BSc) midwifery graduates from DTU and nine other third-generation universities in Ethiopia. The inclusion criteria were employed midwifery professionals who successfully passed the national health professionals licensure examination, who were employed within one year after graduation, who had served for not more than one year, and who were assigned on the primary focus of study.
Midwifery professionals who failed the national licensure exam, employed after one-year post-graduation, worked for more than one year, took labor and delivery related training or assigned outside their area of training were excluded to prevent the loss of competencies acquired from preservice education and to exclude potential competency development through in-service training and experiences.
To minimize contextual differences, the comparison group was selected from third-generation universities like DTU, which are similar in terms of establishment year, staffing, educational facilities and resources, clinical practice sites, budgets, and student support services.
This study focuses on BSc midwifery providers meeting the eligibility criteria, not the women observed during labor and delivery. Cases that required the involvement of other healthcare providers or procedures beyond a midwife’s scope (like cesarean sections) were excluded from the analysis.
Sample Size and Selection of Study Participants
The sample size was determined via a formula to compare the mean performance of two independent groups. Owing to the absence of a previous similar study, we aimed to detect a relative effect size of d = 0.5, assuming equal variance with 0.8 (80%) power at a significance level of α=.05, which led to a sample of 32 for each group.
We identified thirty-seven recent midwifery graduates from DTU, thirty-two of whom met the inclusion criteria. Five were excluded due to unemployment (1), working outside the study focus (1), career change (1), or employment abroad (2). Of Ethiopia’s nine third-generation universities (excluding Debre Tabor University), three were excluded from the control group: two had implemented similar curricula, and one lacked complete data. Accordingly, the control group consisted of graduates from the remaining five universities that continued using the conventional curriculum. To account for anticipated non-response rates, 10% was added to the comparison group, resulting in a final group size of thirty-six. These participants were randomly selected from graduate lists provided by the registrars of the selected universities.
Data Collection Procedures and Instruments
Data were collected from August 26 to October 12, 2024, through direct observation of labor and deliveries, review of medical records and inventory of the maternal and child health (MCH) unit and pharmacies of the health facilities.
Data Collection Tools
The labor and delivery observations utilized the Labor and Delivery Quality of Care Short Observational Index, a validated clinical tool developed with sub-Saharan African data under the MCHIP (Maternal and Child Health Integrated Program implemented by Jhpiego).25,26 The tool assesses the quality of care provided to mothers and newborns during labor, delivery, and the immediate postpartum period. It covered twenty tasks (yes/no), including initial assessments, first-stage labor monitoring, continuous second- and third-stage observation, and immediate postpartum and newborn care, which were completed one hour postpartum. The tool also included a screening form to record eligibility criteria and sociodemographic information.
Record Review
Observers reviewed charts to uncover details regarding outcomes of labor and delivery.
Facility Inventory
Facility inventory was conducted once at each facility to verify the availability of medications, supplies, and equipment required for normal labor and delivery.
Recruitment and Training of Data Collectors
Clinical midwives with a master’s degree, over one year of maternal and newborn care experience, and no affiliation with study facilities were recruited based on criteria in the validated tool’s user guide.26
A five-day training (August 19–23, 2024) was conducted using the MCHIP Clinical Observer Learning Resource Package.26 The training covered the study protocol, tools, smartphone-based data collection, and ethics, using interactive methods to enhance interrater reliability.
Data Collection Procedure
Supplementary Figure 2 outlines the labor and delivery observation process. At each facility, data collectors screened providers and obtained permission to observe. Women in established labor, as confirmed by clinicians, were invited to participate. Consenting women attended by selected midwives were enrolled. Observations began during the initial assessment before active labor and continued through delivery and one hour postpartum to capture all outcome variables.
Two trained observers independently and simultaneously recorded care, remaining unobtrusive unless intervention was necessary. The average of their scores was used for analysis. Only cases fully managed by the selected midwife were included to ensure all actions recorded reflected the participant’s performance (for example a midwife administering a uterotonic also completed follow-up tasks). Data were collected using the Kobo Collect-based labor and delivery observation tool, deployed via the Kobo mobile app.
Interrater Reliability and Internal Consistency
Although previously validated in a similar setting,25 the tool’s internal consistency was re-evaluated using data from this study. Interrater reliability of the total performance scores (20 items) was assessed using a two-way mixed effects intraclass correlation coefficient (ICC) with a consistency definition. The ICC for average measures was .87 (95% CI:.79 −.92, p < .001), suggesting excellent agreement between the two raters. Additionally, Cronbach’s alpha for the 20-item tool was .66, suggesting acceptable internal consistency for the purpose of this study.
Analysis
Data were analyzed using SPSS Version 27. Descriptive statistics (frequency, percentage, mean, and standard deviation) summarized the data. Performance was calculated as the percentage mean score of completed tasks per domain, with an overall mean score for the outcome variable.
An independent sample t test compared performance between competency-based and conventional curriculum graduates. Effect size was estimated using Cohen’s d and visualized with a Gardner–Altman plot.
This outcome was one of four primary outcomes assessed in a broader study. To account for multiple comparisons, we applied Bonferroni, Holm–Bonferroni, and false discovery rate (FDR) corrections. This outcome remained statistically significant under all methods.
Results
Characteristics of the Participants and Facilities
Service Providers and Clients
The study observed sixty-eight midwives and an equal number of laboring women across 29 public health facilities in Ethiopia. Regarding characteristics of participating midwives, their mean age was 24.6 years, most were males (54.4%), unmarried (77.9%), and had 6–12 months of experience (97.1%). Slightly more than half worked in health centers (54.4%), with comparable representation from both groups (Table 1). Most clients were aged 25–34 years (86.7%), were married (91.2%), and resided in urban areas (64.7%) (Supplementary Table 1).
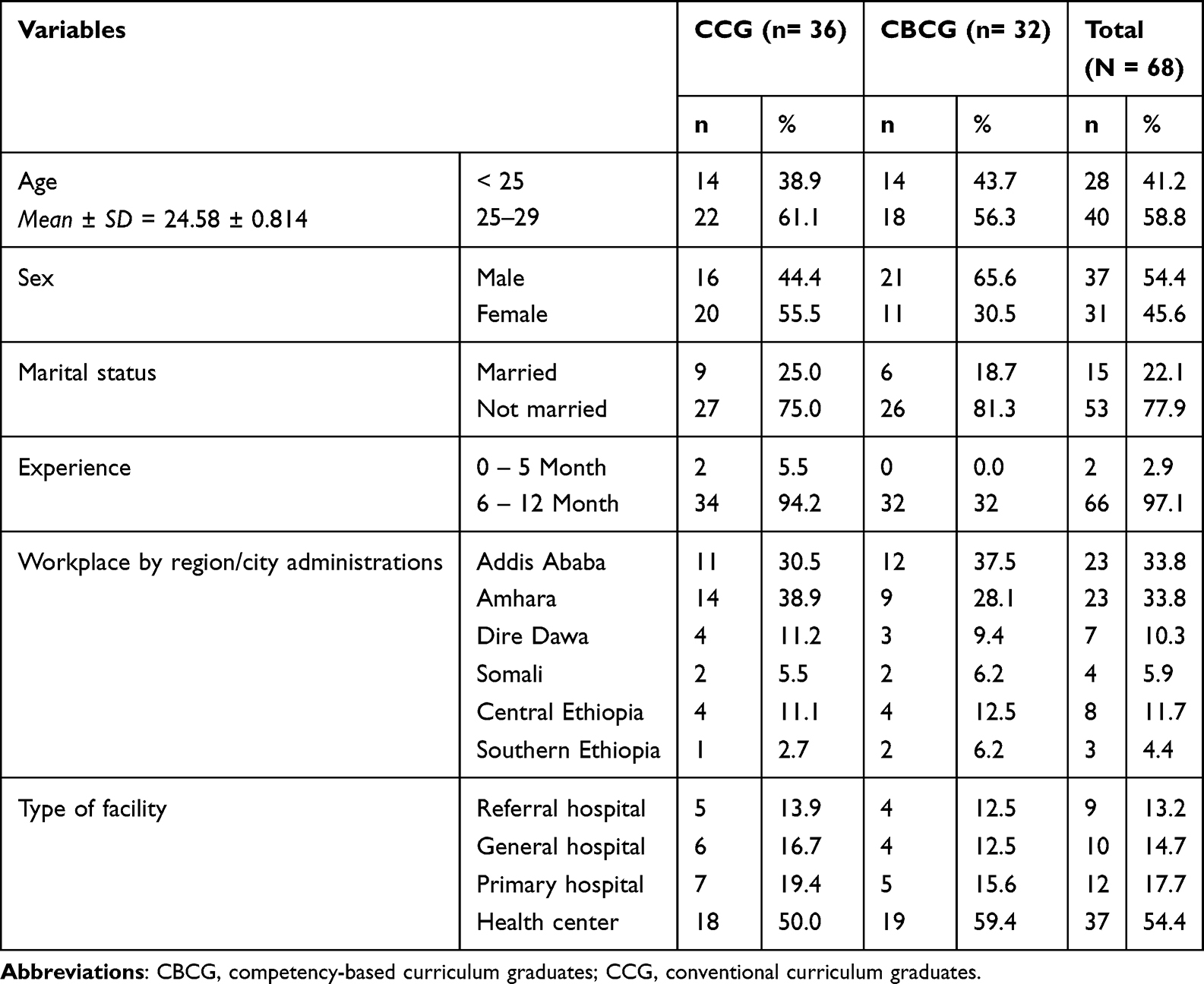 |
Table 1 Characteristics of Midwives Observed by Type of Curriculum in Preservice Education (N = 68) |
Facility Characteristics and Resources
Many facilities (65.6%) were health centers and reported conducting fewer than five deliveries per day, which was evenly distributed between facilities staffed by competency-based and conventional curriculum graduates (Supplementary Table 1). Among the twenty-nine facilities, 83% had essential delivery equipment and 80% had neonatal resuscitation supplies, which were evenly distributed between facilities staffed by competency-based and conventional curriculum graduates (Supplementary Table 2).
Labor and Delivery Care Performance
Initial Client Assessment and Examination
The overall mean performance score for initial client assessment and examination was 73.1%, with competency-based curriculum graduates scoring higher than those from the conventional curriculum (82.6% vs 64.7%).
Notable performance gaps were observed between groups. Hand hygiene was practiced by 48.5% of midwives, with better adherence among competency-based graduates. Most midwives (73.5%) inquired about vaginal bleeding, with higher rates among competency-based graduates. Similarly, 80.9% assessed HIV status, again with better performance from competency-based graduates (Table 2).
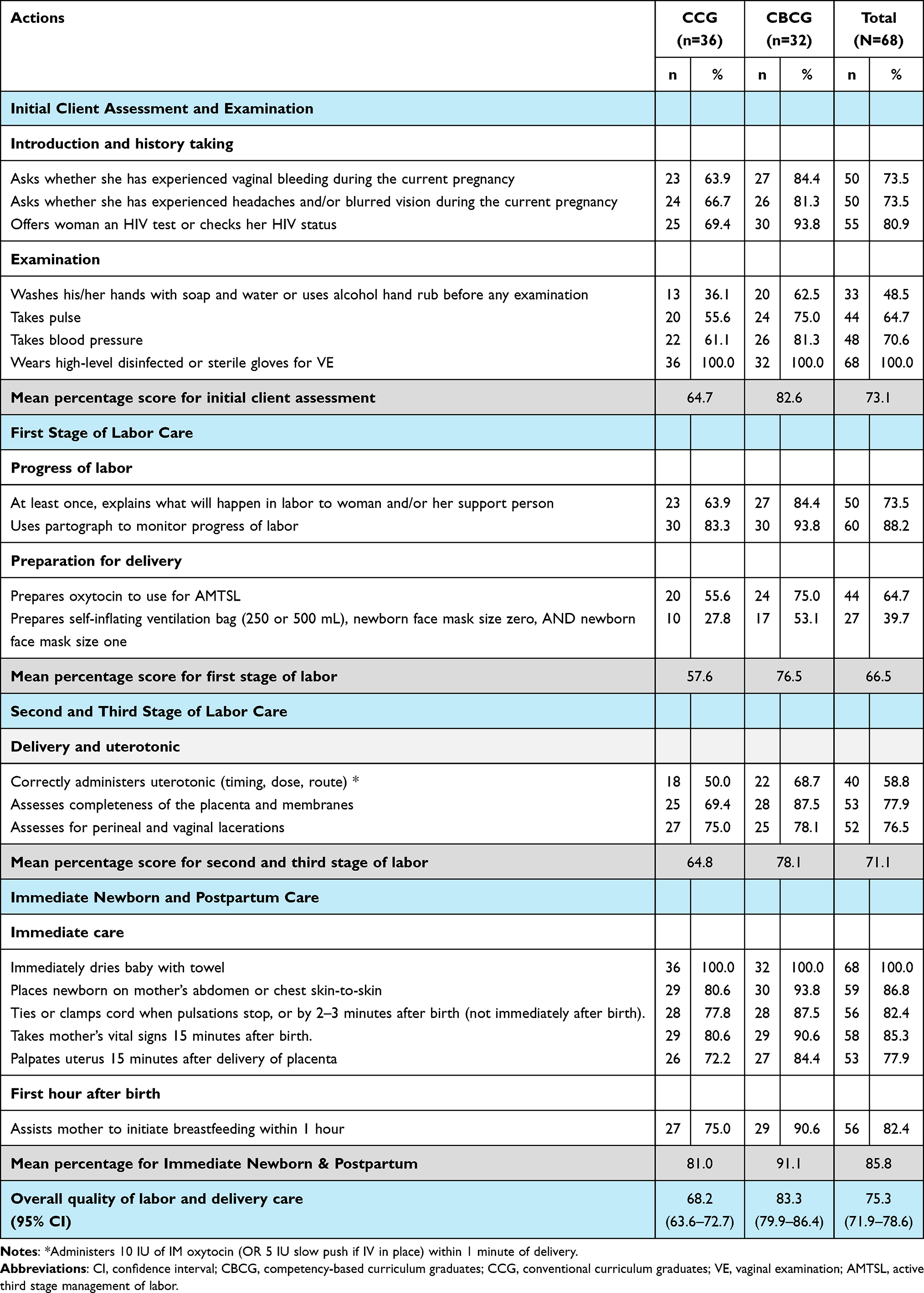 |
Table 2 Observed Quality of Labor and Delivery Care by Curriculum Type, Ethiopia (N=68) |
First Stage of Labor Care
The overall mean score for tasks performed during the first stage of labor was 66.5%. Graduates from the competency-based curriculum scored twenty percentage points higher than conventional curriculum graduates, particularly in tasks related to labor monitoring and preparation for delivery.
Despite midwives of both groups performed better in monitoring labor progress. However, their preparation for delivery was inadequate. About 39.7% of midwifes prepared newborn resuscitation equipment before delivery, such as self-inflating ventilation bags and masks. Compared with conventional curriculum graduates, competency-based curriculum graduates had better preparation rates (53.1% vs 27.8%) (Table 2).
Second and Third Stages of Labor Care
The mean performance during the second and third stages of labor was 71.1%, with graduates from the competency-based curriculum performing better (78.1%) than those from the conventional curriculum (64.8%). During the Active Management of Third Stage of Labor (AMTSL), the midwives correctly administered a uterotonic (timing, dose, route) to 58.8% of the birthing mothers, with competency-based curriculum graduates performed better than conventional controls (68.7% vs 50.0%) (Table 2).
Immediate Newborn and Postpartum Care
Overall performance in immediate newborn and postpartum care was high, with a mean score of 85.8%. Competency-based curriculum graduates performed better than conventional curriculum graduates (91.1% vs 81.0%).
Most midwives supported early breastfeeding (82.4%) and practiced skin-to-skin contact (86.8%). CBCGs demonstrated higher adherence to both newborn care practices, early breastfeeding, and skin-to-skin contact (Table 2).
Overall Quality of Labor and Delivery Care
The mean percentage score for the overall quality of labor and delivery care provided by midwives was 75.3% (95% CI: 71.9–78.6), representing that, on average, midwives performed three-fourths of the quality tasks. Competency-based curriculum graduates had a mean score of 83.3% (95% CI: 79.9–86.4), whereas conventional curriculum graduates had a mean score of 68.2% (95% CI: 63.6–72.7) (Table 2).
For AMTSL, competency-based curriculum graduates performed better than conventional curriculum graduates in preparing oxytocin (75% vs 55.6%) and administering it correctly (68.7% vs 50%) (Table 2).
Comparing Labor and Delivery Care Performance
An independent samples t test was conducted to compare the mean performance scores for quality labor and delivery care provided by competency-based and conventional curriculum midwifery graduates. The results revealed a significant difference (t (61.77) = 5.29, p < .001), with the mean score for CBCGs (M = 0.832, SD = 0.093) being significantly higher than CCGs (M = 0.682, SD = 0.139) (Table 3).
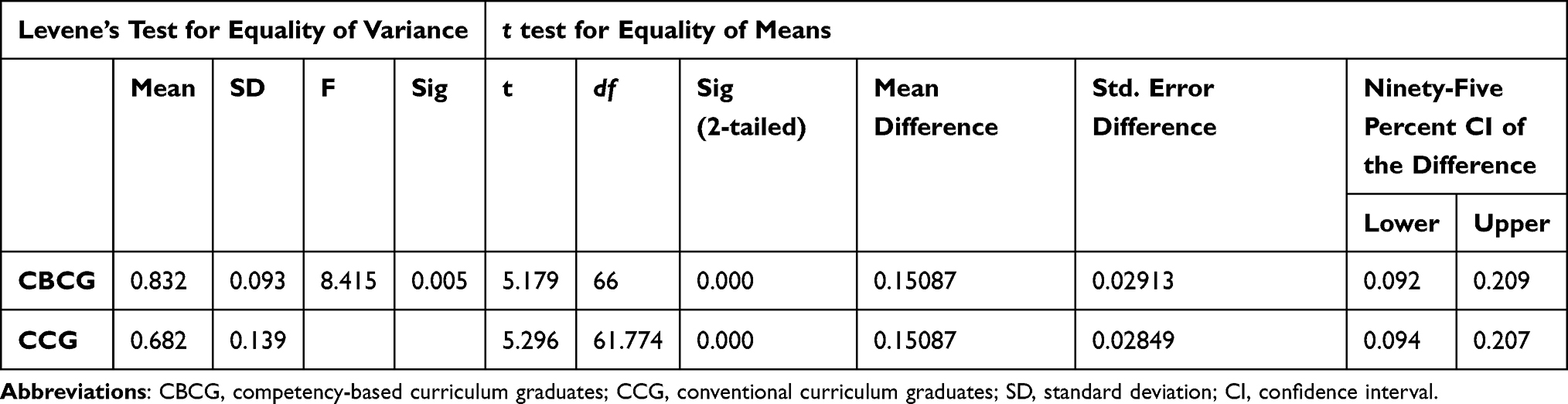 |
Table 3 Comparing the Quality of Labor and Delivery Care Performance Between Competency-Based and Conventional Curriculum Midwife Graduates in Ethiopia |
Effect Size Estimation
The difference in quality of labor and delivery care between the two groups was estimated using a Gardner–Altman plot generated via the DABEST package.27 The analysis revealed a mean difference (∆) of 0.15 [95% CI: 0.09 to 0.21] on a standard 0–1 scale of quality, preferring graduates of the competency-based curriculum (M = 0.832, SD = 0.093, n = 32) than the conventional curriculum graduates (M = 0.682, SD = 0.139, n = 36) (Figure 1)
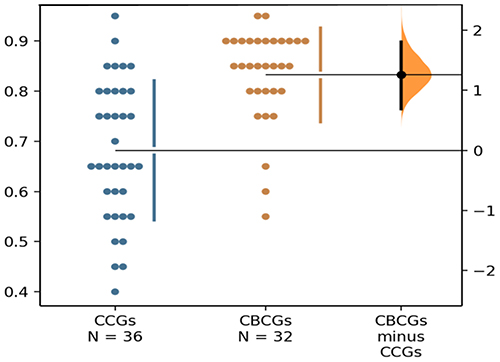 |
Figure 1 A Gardner-Altman plot for quality of labor and delivery care provided by conventional curriculum graduates (CCGs) and competency-based curriculum graduates (CBCGs). |
For comparison, a standardized effect size was also computed, yielding Cohen’s d = 1.26 [95% CI: 0.69, 1.80]. While this indicates a large effect by conventional thresholds, its interpretation should be made with caution due to its dimensionless nature and dependence on distributional assumptions.
Discussion
Skilled care during childbirth is crucial to enhance maternal and neonatal outcomes.28 This study compared the quality of labor and delivery care provided by midwives who graduated from competency-based and conventional curricula deployed in 29 public health facilities across Ethiopia.
Our findings indicate that midwives trained under competency-based curricula (CBCGs) delivered higher quality labor and delivery care than those trained under conventional curricula (CCGs), with a notable effect size (Δ = 15%, Cohen’s d = 1.26). Rather than merely reflecting differences in task completion, this performance gap highlights the successful translation of theoretical knowledge into practical skills, aligning with Miller’s Pyramid framework, where competency progresses from “knows” to “does.” This suggests that competency-based curricula enhance the ability of graduates to perform essential clinical tasks in real-world settings.
The most pronounced differences were observed during initial client assessment and examination. CBCGs outperformed CCGs in key areas such as inquiry about vaginal bleeding, HIV status assessment, and adherence to hand hygiene. Their superior performance in screening for complications, conducting appropriate tests, and following infection prevention protocols reflects stronger preparedness for clinical demands, consistent with Kolb’s experiential learning theory, which emphasizes repeated practice and reflection.
During the first stage of labor, CBCGs scored nearly 20 percentage points higher, particularly in labor monitoring and delivery preparation. They were more effective in anticipating potential complications, including readiness for neonatal resuscitation, highlighting the importance of hands-on, practice-focused training in building clinical confidence and competence. CBCGs also performed better in preparing and correctly administering uterotonics as part of active management of the third stage of labor (AMTSL), demonstrating the curriculum’s impact on life-saving interventions critical for preventing postpartum hemorrhage. Immediate newborn and postpartum care performance was high in both groups, but CBCGs showed greater adherence to thermal care, breastfeeding support, and maternal monitoring, reflecting the broader emphasis on postnatal care in Ethiopia’s maternal health programs.
These findings are consistent with global and regional evidence showing that competency-based education improves clinical performance. Studies across Africa have reported that midwives trained under competency-based curricula exhibit superior labor monitoring and neonatal resuscitation skills compared with conventional program graduates.29–32 In Rwanda, updates to the midwifery curriculum similarly resulted in improved maternal and newborn care outcomes, attributed to stronger clinical mentoring and hands-on training components.33 These findings suggest that graduates from competency-based curricula benefit from more practical and skill-focused training, which enhances their performance in key areas of maternal and newborn care. Midwifery education programs that integrate simulation and competency-based assessments have been shown to lead to better adherence to critical maternal and newborn care practices, including the AMTSL and neonatal resuscitation.34
The higher performance of CBCGs in AMTSL and the first stage of labor aligns with quasi-experimental evaluations in Tanzania and Egypt, where exposure to revised curricula increased adherence to evidence-based intrapartum care practices.35,36 By directly observing real-world performance, our study quantifies the practical impact of competency-based curricula, providing strong evidence for their effectiveness in enhancing essential clinical competencies.
Despite these improvements, certain challenges persist. Inadequate hand hygiene, incomplete labor monitoring, insufficient preparation for neonatal resuscitation, and inconsistent administration of uterotonics remain concerns, consistent with findings from Uganda, Nigeria, and Eastern Ethiopia.37,38 These gaps suggest that curriculum reform alone is insufficient and must be complemented by workplace-based assessments, supportive supervision, and quality improvement initiatives to ensure sustained competence.
Contribution to the Literature
While many studies have evaluated the effectiveness of preservice midwifery education using knowledge tests, self-reported competencies, interviews, simulated assessments (OSCEs), or in-service training evaluations, very few have directly observed real-time clinical practices and linked them explicitly to curriculum type. This study adds a unique contribution by using structured clinical observations by trained observers in actual delivery room settings to compare the performance of graduates from competency-based versus conventional midwifery curricula. By directly capturing provider behaviors during labor and delivery, our study provides robust evidence on how curriculum reform translates into practical clinical competency.
Implications for Policy and Practice
This study provides actionable insights for policymakers and educators to enhance midwifery training and improve clinical practices. Our study emphasizes the importance of competency-based preservice education curricula in improving the quality of labor and delivery care provided by midwives. By integrating active learning, simulation-based training, and evidence-based practices, such curricula can produce highly skilled graduates. Scaling up these approaches is crucial for enhancing maternal and neonatal health outcomes, particularly in low-resource settings where maternal and neonatal mortality rates remain high.
Strengths
The use of direct observation of performance in the actual workplace with multiple expert raters and validated measurement tools ensured the validity and reliability of the scores.
Limitations
Selection bias was minimized by including BSc midwifery graduates from third-generation Ethiopian universities with similar establishment years, resources, and support. All participants had under one year of service, no in-service training, and had passed the national licensure exam, reducing variability from experience or post-graduation learning.
Measurement bias was reduced by using a validated multicounty observation tool and employing two trained, independent observers whose average scores were used. Observer bias was limited by blinding data collectors to participants’ group assignments.
The Hawthorne effect was addressed by ensuring confidentiality, omitting provider and facility identifiers, and presenting the study as process-focused rather than evaluative. Some residual performance changes may remain but likely affected both groups equally.
Conclusion
This study demonstrated that midwives trained under a competency-based curriculum provided higher quality labor and delivery care across all components compared to their conventionally trained counterparts, with a large effect size indicating strong clinical relevance. The most notable improvements were seen in initial client assessment, including complication screening, appropriate testing, and infection prevention, along with delivery preparation, particularly readiness for critical interventions such as neonatal resuscitation and AMTSL. CBCGs also showed greater adherence to essential newborn and postpartum care practices, including thermal care, early breastfeeding, and maternal monitoring.
These findings underscore the value of adopting competency-based curricula while emphasizing the importance of addressing persistent deficiencies to improve quality of care during childbirth.
Abbreviations
AMTSL, active management of third stage of labor; BSc, Bachelor of Sciences; CBCGs, competency-based curriculum graduates; CCGs, conventional curriculum graduates; DTU, Debre Tabor University; ICC, intraclass correlation coefficient; MCH, maternal and child health; MCHIP, maternal and child health integrated program; PSE, preservice education; RMNCH, reproductive, maternal, newborn, and child health; WHO, World Health Organization.
Data Sharing Statement
The dataset that supports the analysis and interpretation of findings from the current study is available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study protocol was approved by the Ethical Review Committee of Debre Tabor University, Ethiopia (Date: 13.07.2023 / No: RP/251/23), and the Ethics Commission of the Medical Faculty of Ludwig-Maximilians-Universität, Munich, Germany (Date: 18.10.2023 / Project Nr.: 23-0757). At each health facility, the supervisor presented an official letter from DTU to the facility director requesting cooperation. Written consent was obtained from facility directors, while oral consent was obtained from midwives and laboring women. Written consent was not collected from midwives due to their engagement in clinical care, although the potential benefits and burdens had been discussed beforehand. For laboring women, written consent was waived owing to literacy challenges and to minimize the burden during labor.
Data collectors were trained to approach participants respectfully, explain the study purpose, and obtain informed consent, including discussion of potential risks and benefits. Providers were assured that participation or refusal would not affect their employment, and women were assured that nonparticipation would not influence the care they received. Participant and facility confidentiality was strictly maintained: no names of facilities, service providers, or clients were recorded, and results were reported anonymously to prevent identification.
All informed consent procedures were reviewed and approved by the respective ethics committees. The study was conducted in accordance with the principles of the Declaration of Helsinki, ensuring ethical recruitment, participant protection, and respect for autonomy throughout the research.
Acknowledgments
We thank our participants, both service providers and observed women in labor, delivery and health facilities, for their generous involvement.
Funding
This study was supported by Jhpiego through the Health Workforce Improvement Program (HWIP), which provided financial assistance for data collection. The sponsor had no role in the study design, data analysis, interpretation of results, or the writing of the manuscript.
Disclosure
The authors declare the following potential conflict of interest: Awoke Giletew Wondie and Tegbar Y Sendekie engaged in the design and implementation of the competency-based curriculum at Debre Tabor University. However, they had no role in data collection or scoring. The assessment was conducted by trained, independent midwife observers who were blinded to the curriculum background of the graduates being evaluated. The authors report no financial or commercial conflicts of interest.
References
1. WHO. World Health Organization Data. Ethiopia HEALTH data overview for the Federal Democratic Republic of Ethiopia Available from: https://data.who.int/countries/231.
2. Fund UNP. The State of the World’s Midwifery 2021. United Nations; 2021.
3. Fattahi H, Abolghasem Gorji H, Bayat M. Core competencies for health headquarters: a systematic review and meta-synthesis. BMC Public Health. 2020;20(1):891. doi:10.1186/s12889-020-08884-2
4. Central Statistical Agency (CSA) [Ethiopia], ICF. Ethiopia demographic and health survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2017 [cited June 19, 2025]. Available from: https://dhsprogram.com/pubs/pdf/FR328/FR328.pdf.
5. Ministry of Health [Ethiopia]. Annual performance report of 2016 EFY: the 26th annual review meeting of the health sector – Ethiopia. Addis Ababa: Ministry of Health; 2024 [cited June 19, 2025]. Available from: https://www.scribd.com/document/801791284/Annual-Performance-Report-2024-Oct20-2024.
6. ICF. Ethiopia mini demographic and health survey 2019: final report. Rockville, Maryland, USA: EPHI and ICF.; 2021.
7. Goshu M, Godefay H, Bihonegn F, et al. Assessing the competence of midwives to provide care during labor, childbirth and the immediate postpartum period – a cross sectional study in Tigray region, Ethiopia. PLoS One. 2018;13(10):e0206414. doi:10.1371/journal.pone.0206414
8. Yigzaw T, Ayalew F, Kim Y-M, et al. How well does pre-service education prepare midwives for practice: competence assessment of midwifery students at the point of graduation in Ethiopia. BMC Med Educ. 2015;15(1):130. doi:10.1186/s12909-015-0410-6
9. Temam G, Ayalew F, Molla Y, et al. Evaluation of the effectiveness of interventions to improve quality of midwifery and anesthesia education: technical report on a pre-post quasi-experimental study. Baltimore (MD): Jhpiego Corporation; 2018.
10. Kibwana S, Haws R, Kols A, et al. Trainers’ perception of the learning environment and student competency: a qualitative investigation of midwifery and anesthesia training programs in Ethiopia. Nurse Education Today. 2017;55:5–10. doi:10.1016/j.nedt.2017.04.021
11. Speedraftaar. HPLE MOH GOV ET exam result 2015–2023: https://www.moh.gov.et login. Speedraftaar. [cited June 19, 2025]. Available from: https://speedraftaar.com/hple-moh-gov-et-exam-result-2015-2023-www-moh-gov-et-login.
12. Kibwana S, Woldemariam D, Misganaw A, et al. Preparing the health workforce in Ethiopia: a Cross-sectional study of competence of anesthesia graduating students. Educ Health. 2016;29(1):3–9. doi:10.4103/1357-6283.178931
13. Gavine A, MacGillivray S, McConville F, Gandhi M, Renfrew MJ. Pre-service and in-service education and training for maternal and newborn care providers in low- and middle-income countries: an evidence review and gap analysis. Midwifery. 2019;78:104–113. doi:10.1016/j.midw.2019.08.007
14. Carr C, Johnson P. Eyes on the prize: linking pre-service education to outcomes. Int J Gynecol Obstet. 2015;130(S2):S74–S76. doi:10.1016/j.ijgo.2015.03.003
15. Majumder MAA, Haque M, Razzaque MS. Editorial: trends and challenges of medical education in the changing academic and public health environment of the 21st century. Front Commun. 2023;8:1153764. doi:10.3389/fcomm.2023.1153764
16. Jhpiego. Ethiopia task analysis study report. for medical doctors, health officers, nurses, medical laboratory professionals, and pharmacy professionals. 2015.
17. Karthikeyan K, Kumar A, B A, R D. Integrated modular teaching in undergraduate medicine. Natl Med J India. 2014;27(2):90–94.
18. Quintero GA, Vergel J, Laverde Á, Ortíz LC. Educational strategies to develop and implement a comprehensive health care model focused on primary care in Colombia. J Med Educ Curric Dev. 2020;7:2382120520930260. doi:10.1177/2382120520930260
19. Gebremickael A, Mulu A. Implementation status of the nationally harmonized competency-based, integrated, modular medical curriculum in Ethiopia: opportunities and challenges. BMC Med Educ. 2024;24(1):799. doi:10.1186/s12909-024-05796-2
20. Misganaw E, Yigzaw T, Tezera R, Gelitew A, Gedamu S. The promise of the new educational strategy for curriculum development (SPICES) model on the development of students’ clinical reasoning ability. a comparative cross-sectional study. Adv Med Educ Pract. 2022;13:71–79. doi:10.2147/amep.S344933
21. Wondie A, Yigzaw T, Worku S. Effectiveness and key success factors for implementation of problem-based learning in Debre Tabor University: a mixed methods study. Ethiop J Health Sci. 2020;30(5):803–816. doi:10.4314/ejhs.v30i5.21
22. Sekkizhar U, Ramanathan R, Sakthivel P, Shanmugam J. Effectiveness of early clinical exposure in competency-based curriculum – a step forward. Nat J Physiol Pharm Pharmacol. 2023;1. doi:10.5455/njppp.2023.13.05280202331052023
23. Krishnasamy N, Hasamnis AA, Patil SS. Developing professional identity among undergraduate medical students in a competency-based curriculum: educators’ perspective. J Educ Health Promotion. 2022;11(1):361. doi:10.4103/jehp.jehp_329_22
24. Savitha D, Iyengar A, Devarbhavi H, et al. Early clinical exposure through a vertical integration programme in physiology. Natl Med J India. 2018;31(5):296–300. doi:10.4103/0970-258x.261191
25. Tripathi V, Stanton C, Strobino D, Bartlett L. Development and validation of an index to measure the quality of facility-based labor and delivery care processes in Sub-Saharan Africa. PLoS One. 2015;10(6):e0129491. doi:10.1371/journal.pone.0129491
26. Tripathi V. The labor and delivery quality of care short observational index: a user guide. Washington (DC): Maternal and Child Survival Program (MCSP); 2016 [cited June 23, 2025]. Available from: https://mcsprogram.org/resource/labor-delivery-quality-care-short-observational-index-user-guide/.
27. Ho J, Tumkaya T, Aryal S, Choi H, Claridge-Chang A. Moving beyond P values: data analysis with estimation graphics. Nature Methods. 2019;16(7):565–566. doi:10.1038/s41592-019-0470-3
28. World Health Organization (WHO). United Nations Children’s Fund (UNICEF), United Nations Population Fund (UNFPA), International Confederation of Midwives (ICM). strengthening quality midwifery education for universal health coverage 2030: framework for action. Geneva: World Health Organization; 2019 [cited June 23, 2025]. Available from: https://www.who.int/publications/i/item/9789241515849.
29. Ige WB, Ngcobo WB, Afolabi O. Implementation of competency-based education for quality midwifery programmes in Africa: a scoping review. BMC Nursing. 2024;23(1):685. doi:10.1186/s12912-024-02333-w
30. Kusrini P, Susanti A. Competency-based education in midwifery: a comprehensive review of implementation strategies and outcomes in developing regions. Inovasi Kurikulum. 2025;22(2):1155–1170. doi:10.17509/jik.v22i2.83661
31. Imanipour M, Ebadi A, Monadi Ziarat H, Mohammadi MM. The effect of competency-based education on clinical performance of health care providers: a systematic review and meta-analysis. Int J Nurs Pract. 2021;28(1):e13003. doi:10.1111/ijn.13003
32. Benewaa D, Agyei RB, Aboagye S, Danso KO, Owusu-Agyeman AK. Bridging theory and practice. Ghana J Nurs Midwifery. 2024;1(3):156–174. doi:10.69600/gjnmid.2024.v01.i03.156-174
33. Bogren M, Nkeshimana M, Nzabahimana I, et al. Rwanda’s success in advancing midwifery education: a blueprint of a sustainable, nationally driven curriculum standardization. Global Health Action. 2024;17.
34. Birhane BM, Assefa Y, Belay DM, et al. Interventions to improve the quality of maternal care in Ethiopia: a scoping review. Front Glob Womens Health. 2024;5:1289835. doi:10.3389/fgwh.2024.1289835
35. Bishanga DR, Charles J, Tibaijuka G, et al. Improvement in the active management of the third stage of labor for the prevention of postpartum hemorrhage in Tanzania: a cross-sectional study. BMC Pregnancy Childbirth. 2018;18(1):223. doi:10.1186/s12884-018-1873-3
36. Kamal Ali F, Abdel-Wahab Afifi Araby Ali O, Mansour Abdel Azeem Barakat F. Effect of competency-based education on maternity nurses’ performance and quality of care regarding management of first stage of labor. Egyptian J Health Care. 2024;15(2):149–170. doi:10.21608/ejhc.2024.350819
37. Yang F, Bohren MA, Kyaddondo D, et al. Healthcare providers’ perspectives on labor monitoring in Nigeria and Uganda: a qualitative study on challenges and opportunities. Int J Gynaecol Obstet. 2017;139 Suppl 1(S1):17–26. doi:10.1002/ijgo.12379
38. Sintayehu Y, Desalew A, Geda B, et al. Basic neonatal resuscitation skills of midwives and nurses in Eastern Ethiopia are not well retained: an observational study. PLoS One. 2020;15(7):e0236194. doi:10.1371/journal.pone.0236194
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Determinants of Knowledge of Musculoskeletal Disorders Among Healthcare Providers and Students in Saudi Arabia: A Cross-Sectional Study
Alrwaily M, Alanazi F
Journal of Multidisciplinary Healthcare 2022, 15:1789-1797
Published Date: 25 August 2022