Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Do Primary Care Providers in Saudi Arabia Have Sufficient Knowledge to Support COPD Management and Patient Education? A National Cross-Sectional Survey
Authors Siraj RA ![]() , Al Rajeh AM
, Al Rajeh AM ![]() , Almulhem MM, Alahmari MA
, Almulhem MM, Alahmari MA ![]() , Aldhahir AM
, Aldhahir AM ![]() , Alqarni AA
, Alqarni AA ![]() , Alqahtani JS
, Alqahtani JS ![]() , Alghamdi SM
, Alghamdi SM ![]() , Alobaidi NY, Alruwaili A
, Alobaidi NY, Alruwaili A ![]() , Algarni SS, Alghamdi AS
, Algarni SS, Alghamdi AS ![]() , Alyami MM
, Alyami MM ![]() , Alrhaili MR, Alsolami NA
, Alrhaili MR, Alsolami NA
Received 14 August 2025
Accepted for publication 24 December 2025
Published 7 January 2026 Volume 2026:19 560589
DOI https://doi.org/10.2147/JMDH.S560589
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Brian Nyatanga
Rayan A Siraj,1 Ahmed M Al Rajeh,1 Maryam M Almulhem,1 Mushabbab A Alahmari,2,3 Abdulelah M Aldhahir,4 Abdullah A Alqarni,5,6 Jaber S Alqahtani,7 Saeed M Alghamdi,8 Nowaf Y Alobaidi,9,10 Abdullah Alruwaili,10,11 Saleh S Algarni,12,13 Abdulrhman S Alghamdi,14 Mohammed M Alyami,15 Majed Rzaiq Alrhaili,16 Nawaf A Alsolami17
1Department of Respiratory Therapy, College of Applied Medical Sciences, King Faisal University, Al Ahasa, Saudi Arabia; 2Department of Respiratory Therapy, Faculty of Applied Medical Sciences, University of Bisha, Bisha, Saudi Arabia; 3Health and Humanities Research Center, University of Bisha, Bisha, Saudi Arabia; 4Respiratory Therapy Program, Department of Nursing, College of Nursing and Health Sciences, Jazan University, Jazan, Saudi Arabia; 5Department of Respiratory Therapy, Faculty of Medical Rehabilitation Sciences, King Abdulaziz University, Jeddah, Saudi Arabia; 6Respiratory Therapy Unit, King Abdulaziz University Hospital, Jeddah, Saudi Arabia; 7Department of Respiratory Care, Prince Sultan Military College of Health Sciences, Dammam, Saudi Arabia; 8Clinical Technology Department, Respiratory Care Program, Faculty of Applied Medical Sciences, Umm Al-Qura University, Makkah, 21961, Saudi Arabia; 9Department of Respiratory Therapy, College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences, Alahsa, 31982, Saudi Arabia; 10King Abdullah International Medical Research Center, Al Ahsa, 31982, Saudi Arabia; 11Emergency Medical Services program, College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences, Al Ahsa, Saudi Arabia; 12Department of Respiratory Therapy, College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 13King Abdullah International Medical Research Center, Riyadh, 12271, Saudi Arabia; 14Department of Rehabilitation Health Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia; 15Respiratory Therapy Department, Batterjee Medical College, Khamis Mushait, Saudi Arabia; 16Department of Respiratory Care, Dawadmi General Hospital, Riyadh Third Health Cluster, Riyadh, Saudi Arabia; 17Department of Respiratory Care, King Abdullah Medical Complex, Jeddah, Saudi Arabia
Correspondence: Rayan A Siraj, Department of Respiratory Therapy, College of Applied Medical Sciences, King Faisal University, Al Ahsa, 31982, Saudi Arabia, Email [email protected]
Background: Chronic Obstructive Pulmonary Disease (COPD) is a leading cause of morbidity and mortality worldwide. Evidence-based education is critical for improving healthcare professionals’ knowledge and promoting optimal clinical practice. However, no study has evaluated COPD-related knowledge among primary healthcare professionals in Saudi Arabia. Thus, this study aimed to assess the level of COPD knowledge in this group and to identify factors associated with higher scores.
Methods: An online cross-sectional survey was conducted from October 2024 to May 2025 among licensed primary healthcare providers in Saudi Arabia, using the Bristol COPD Knowledge Questionnaire (BCKQ). One-way ANOVA was used to compare mean scores across demographic and professional groups, followed by multivariable linear regression to identify independent factors of knowledge.
Results: A total of 1686 responses were received, of which 92 incomplete submissions were excluded, leaving 1594 fully completed questionnaires for analysis. Nurses accounted for 40.4%, general practitioners for 35.8%, and family medicine physicians for 24.0%. The mean (SD) total BCKQ score was 28.2 ± 8.15 out of 65 (43.4%), indicating moderate knowledge overall. The highest-scoring domain was Phlegm (2.96 ± 1.39), while the lowest was Inhaled Steroids (1.26 ± 0.86). Significant differences in knowledge were observed by profession (p = 0.004), region (p = 0.001), workplace (p < 0.001), clinic type (p < 0.001), prior COPD training (p = 0.010), and self-reported knowledge (p < 0.001). In multivariable linear regression, self-reported adequate knowledge (β = 3.99; p < 0.001), prior COPD training (β = 1.89; p = 0.011), and being a family medicine physician versus a general practitioner (β = 1.99; p = 0.027) were independently associated with higher knowledge.
Conclusion: Primary healthcare professionals in Saudi Arabia showed moderate COPD knowledge, with gaps in prevention and pharmacological management. Higher scores were linked to prior COPD training, self-reported adequate knowledge, and being a family medicine physician. Expanding structured, evidence-based training could address these gaps and enhance COPD care nationwide.
Keywords: COPD, primary care, knowledge questionnaire, education
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a progressive respiratory condition associated with significant morbidity, comorbidities, and psychological consequences that collectively impair patients’ health-related quality of life.1 It is, moreover, a serious cause of mortality and is expected to be ranked the third leading cause of death in 2030,2 with a continuing rise in its global burden. This upward trend is also evident in Saudi Arabia, as the prevalence increased steadily between 1990 and 2019.3 As a result, international guidelines emphasise disease-specific education as a central component of COPD management, particularly within self-management and rehabilitation programs. Such education not only enhances disease understanding but, more importantly, equips healthcare professionals with the necessary tools to promote better evidence-based practice.
Educational interventions for both patients and primary care providers have proven to be effective in enhancing COPD management. There is indeed evidence to show that structured educational programs can significantly improve patients’ knowledge, self-management skills, and adherence to treatment plans. For instance, a 1-year academic program for COPD patients led to notable improvements in health-related quality of life, treatment adherence, and inhaler technique, while also reducing unscheduled physician visits.4 Similarly, a 1-month educational program for primary care physicians and patients resulted in significant improvements in disease knowledge and inhaler use.5 A previous study on patients’ experience identified education as a key unmet need and an essential coping strategy for people living with COPD.6 As the role of patient self-management becomes a cornerstone for COPD management, healthcare providers - especially those in primary care - are increasingly responsible for delivering accurate and comprehensive education to patients and their families.
However, despite the fact that growing evidence supports the importance of education, multiple studies have highlighted the limited knowledge of COPD among primary care providers globally. A large international survey involving 600 general practitioners (GPs) across twelve countries found that a large proportion of primary care physicians demonstrated very limited knowledge of COPD, including its definition, risk factors, guideline-based diagnostic methods, and management recommendations.7 Similarly, a study in China found that 67.6% of primary care providers were unaware of COPD-related guidelines and new developments.8 This highlights a critical gap in practice, where insufficient knowledge and poor adherence to COPD guidelines may hinder COPD diagnosis and effective management.
In addition to the global knowledge gaps, there is evidence to suggest that the level of COPD knowledge among primary care providers is significantly influenced by their educational background and professional titles, with higher education correlating with better knowledge.9 Despite recognising the importance of COPD management, many primary care providers continue to demonstrate inadequate knowledge in key guideline domains such as inhaler education, spirometry interpretation, pulmonary rehabilitation referrals, and disease-specific patient education.10 These persistent gaps in essential knowledge among primary care providers indeed underscore the need for targeted educational interventions to ensure effective, guideline-based COPD care in primary care settings, which may impact the quality of care and patient outcomes.
Within the Saudi context, this situation remains poorly understood. While the burden of COPD continues to increase and primary-care providers play a major role in early diagnosis and patient education, there is indeed limited evidence regarding their actual level of COPD-related knowledge. This gap not only limits the ability to assess the educational needs but also reduces the opportunity to design targeted training strategies. To address this, the Bristol COPD Knowledge Questionnaire (BCKQ) was employed in this study, as it is a validated and comprehensive tool for assessing knowledge across key COPD domains. The multidimensional structure and established reliability of the BCKQ make it suitable for evaluating healthcare providers’ preparedness in Saudi primary care settings, in line with GOLD (2025) and Saudi Thoracic Society (2023) recommendations.11,12
To date, there has been no study conducted in Saudi Arabia which assesses the level of COPD-related knowledge among primary care professionals or explores the factors influencing it. Therefore, this study aims to evaluate the level of COPD-related knowledge among primary healthcare professionals in Saudi Arabia and identify associated demographic and professional factors to determine their preparedness in supporting patient education and self-management.
Methods
Study Design
This cross-sectional study was conducted using an online survey distributed via the electronic platform SurveyMonkey. Data collection commenced on October 1, 2024, and concluded on May 31, 2025 and aimed to evaluate the level of COPD-related knowledge among healthcare professionals working in primary care facilities across all regions of Saudi Arabia.
Sampling Strategy
A purposive sampling approach was used to recruit healthcare professionals working in primary care settings who were directly involved in the management of patients with COPD. The target population included general practitioners, family medicine physicians, and primary care nurses practicing in Saudi Arabia. Inclusion criteria required that participants:
- Hold an active license,
- Practice within Saudi Arabia,
- Practice within primary care services, and
- Provide informed consent to participate.
To ensure national representation, authors who contributed to this study from multiple institutions across Saudi Arabia participated in the recruitment process. They were assigned to a specific geographic region, where they coordinated directly with healthcare institutions, hospital officials, and primary care centres to recruit the targeted participants, ensuring coverage of all Saudi regions. In addition to in-person recruitment, the survey was disseminated through social media platforms (X, WhatsApp, and Telegram) to maximise participation. The survey link was shared collaboratively by all co-authors across their institutional networks and professional communication channels to ensure broad national reach.
Questionnaire Tool
The questionnaire consisted of two parts: background information and the Bristol COPD Knowledge Questionnaire (BCKQ).10 Background information section included gender, occupation, region, clinical experience in years, type of clinic (hospital-based or primary care centres), and whether participants had prior training in COPD management. The second part of the questionnaire utilised the original English version of BCKQ10 – since English is the primary language of instruction in the Saudi healthcare system - to assess the level of COPD-related knowledge among primary care healthcare professionals across Saudi Arabia. The BCKQ is a validated multiple-choice tool comprising 13 thematic sections covering key aspects of COPD, including its epidemiology, aetiology, symptoms, and the impact of smoking, exercise, and immunisation. It also evaluates knowledge related to pharmacological management, including bronchodilators, antibiotics, and corticosteroids (both oral and inhaled). Each section contains five items, amounting to 65 questions in total. Correct responses are scored with one point, and incorrect or unanswered items receive zero points, with a maximum score of five per section and 65 overall. (Supplementary File 1).
Validity of the Questionnaire
The BCKQ has demonstrated robust psychometric properties. Its content validity was established through expert input from 60 healthcare professionals, including respiratory consultants, GPs, nurses, and physiotherapists, who were involved in patient education.10 Additionally, face validity was confirmed by a panel of 24 healthcare professionals who evaluated each item for relevance and clarity, with the majority expressing no concerns. The original English version of the BCKQ was used in this study,13 as English is the primary language of healthcare training and documentation in Saudi Arabia. The questionnaire was not piloted locally because it is a publicly available, fully developed instrument, and the complete item set is accessible in the original publication.13 The questionnaire also demonstrated acceptable internal consistency, with a Cronbach’s alpha of 0.73 for the full 65-item scale. Test–retest reliability was strong (r = 0.71), indicating stability over time. Cronbach’s α for the total BCKQ scale was calculated to assess internal consistency within our sample and showed excellent reliability (α = 0.84). This supports that BCKQ is appropriate for both clinical and research settings, including its application among healthcare professionals for assessing knowledge and evaluating the impact of educational interventions.
Sample Size Calculations
The Saudi healthcare system is organised and regulated by the Saudi Health Council, which oversees professional workforce distribution across all healthcare sectors. According to national workforce statistics, there are an estimated 239,208 primary healthcare professionals, including 213,110 nurses, 15,856 general practitioners, and 10,242 family medicine physicians. The sample size for this study was calculated using the single-population proportion formula to estimate the proportion of healthcare professionals with adequate COPD-related knowledge. A conservative expected proportion of 50% was used, together with a 99% confidence level (Z = 2.576) and a 5% margin of error.14,15 The initial calculated sample size was 664; after applying the finite population correction for the total population (N = 239,208), the required sample size remained approximately 662 participants. To account for potential non-response, the minimum target sample size was set at 728 participants. Calculations were performed using OpenEpi (version 3.01).
Ethical Considerations
Ethical approval for this study was obtained from the Independent Research Ethics Committee at King Faisal University (Approval ID: KFU-REC-2023-DEC-ETHICS1720). The study was conducted following the ethical principles outlined in the Declaration of Helsinki.
Before beginning the questionnaire, all participants were provided with detailed information about the study’s objectives, the identity of the principal investigator, and the voluntary nature of participation. An electronic informed consent form was embedded at the start of the online survey. Participants were asked the question: “Do you agree to take part in the study?” and were required to tick “yes” to proceed. A positive response was considered as providing written informed consent.
Participants were assured that their responses would remain confidential and anonymous, with no personal identifiers collected at any stage. The questionnaire was designed to be completed within approximately 10–15 minutes, and only fully completed responses were included in the final analysis. Duplicate entries were avoided by limiting survey access to a single submission per device. (Supplementary File 1).
Statistical Analyses
All data management and statistical analyses were conducted using Stata version 17 (StataCorp LLC, College Station, TX, USA). Before inferential statistical analyses, the distribution of the total COPD knowledge score was evaluated for normality, using the Shapiro–Wilk test, as well as visual inspection of histograms and Q–Q plots.
All statistical procedures focused on the total score of the Bristol COPD Knowledge Questionnaire (BCKQ), which reflects participants’ overall knowledge regarding COPD. Descriptive statistics were used to summarise participant characteristics and knowledge scores. Continuous variables, including total BCKQ scores, were presented as means and standard deviations (SD), while categorical variables were summarised using frequencies and percentages. Categorical predictor variables such as sex, region, institution type, and prior COPD training were coded as binary variables (0 = no, 1 = yes). Professional group and years of experience were entered as categorical variables, with the first category serving as the reference group in regression analyses. Prior COPD training referred to any structured educational session or workshop on COPD management.
To examine differences in knowledge scores across demographic and professional subgroups, one-way analysis of variance (ANOVA) was used. Where statistically significant differences were observed, post hoc comparisons were performed to explore pairwise differences.
To identify factors associated with COPD knowledge, a multivariable linear regression analysis was conducted, with the total BCKQ score as the dependent variable. Regression assumptions, including linearity, residual normality, homoscedasticity, multicollinearity, and influential observations, were performed; no violations were observed. The selection of variables for the multivariable model was determined a priori based on existing literature and conceptual relevance to COPD knowledge (gender, profession, region, workplace, clinic type, years of experience, prior COPD training, and self-reported knowledge). Results were reported as unstandardized and standardised β coefficients with 95% confidence intervals (CIs), p-values, R2, and adjusted R2. A p-value < 0.05 was considered statistically significant. Cases with missing or incomplete data were excluded from the analysis, with no imputation performed.
Although internal consistency was not recalculated in the present study, the BCKQ has previously demonstrated acceptable reliability in the literature. In its original validation, the tool achieved a Cronbach’s alpha of 0.73, indicating satisfactory internal consistency of the 65-item questionnaire. Cases with missing or incomplete data were excluded from the analysis, with no imputation performed.
Results
Out of 1686 responses received, 92 were excluded; thus, 1594 were included in the final analyses (Figure 1). Nearly half of the participants were male (49.7%). Regarding professional background, the sample comprised 40.4% nurses, 35.8% general practitioners, and 24% family medicine physicians. Most participants were practising in the central region (41.4%), followed by the northern (24.1%) and eastern regions (13.2%). A majority were employed in governmental healthcare settings (73.0%) and hospital-based clinics (61.5%).
 |
Figure 1 STROBE Flowchart of Participant Recruitment and Inclusion. |
In terms of clinical experience, 42.0% had less than one year of work experience, while 14.8% had 10 years or more. Notably, 71.1% of participants reported having received prior training in COPD management, and 72.0% self-reported having sufficient knowledge about COPD. Table 1 presents the detailed demographic and professional characteristics of the study participants.
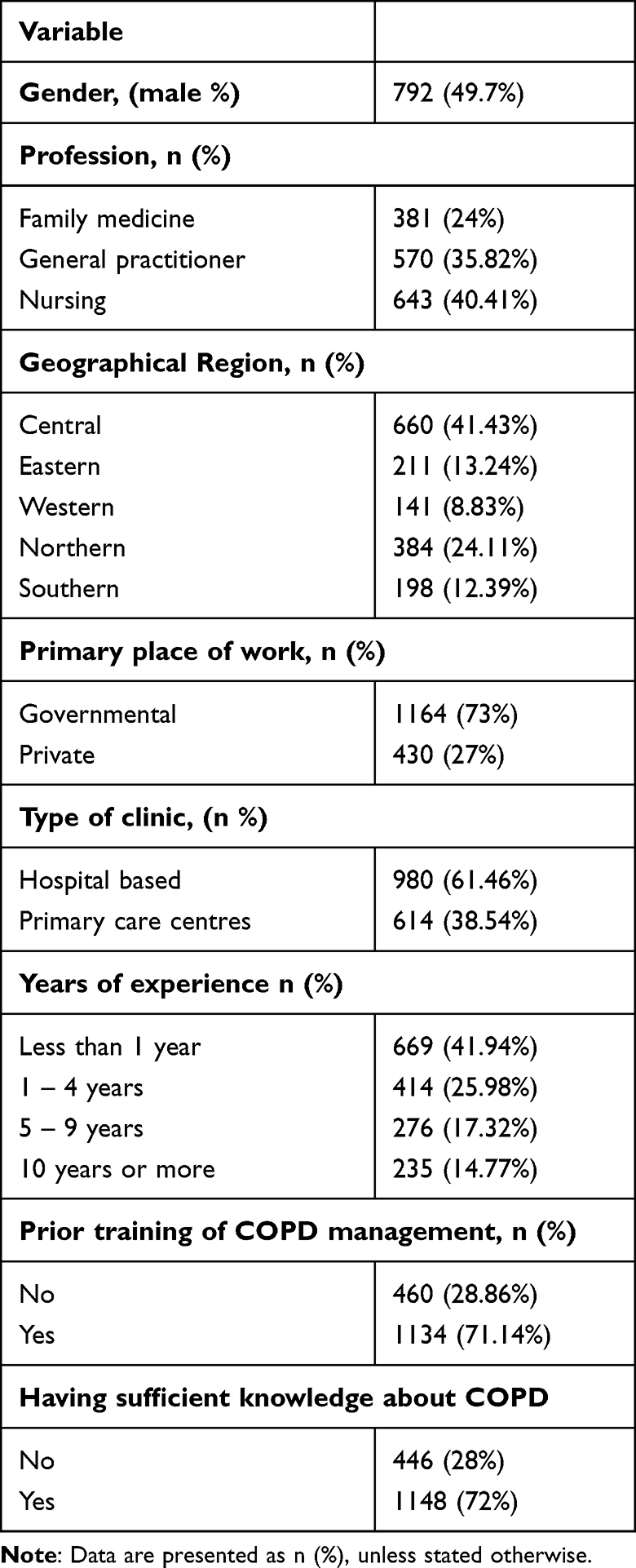 |
Table 1 Demographic Data of Study Participants (n=1594) |
As shown in Table 2, participants scored highest in the Phlegm subscale (mean = 2.96, SD = 1.39), followed by etiology (2.48 ± 1.17), Exercise (2.43 ± 1.06), and Epidemiology (2.43 ± 1.03), suggesting relatively strong knowledge in symptom-related and causal domains. In addition, the percentage of correct answers for all 65 items is reported in Supplementary Table 1.
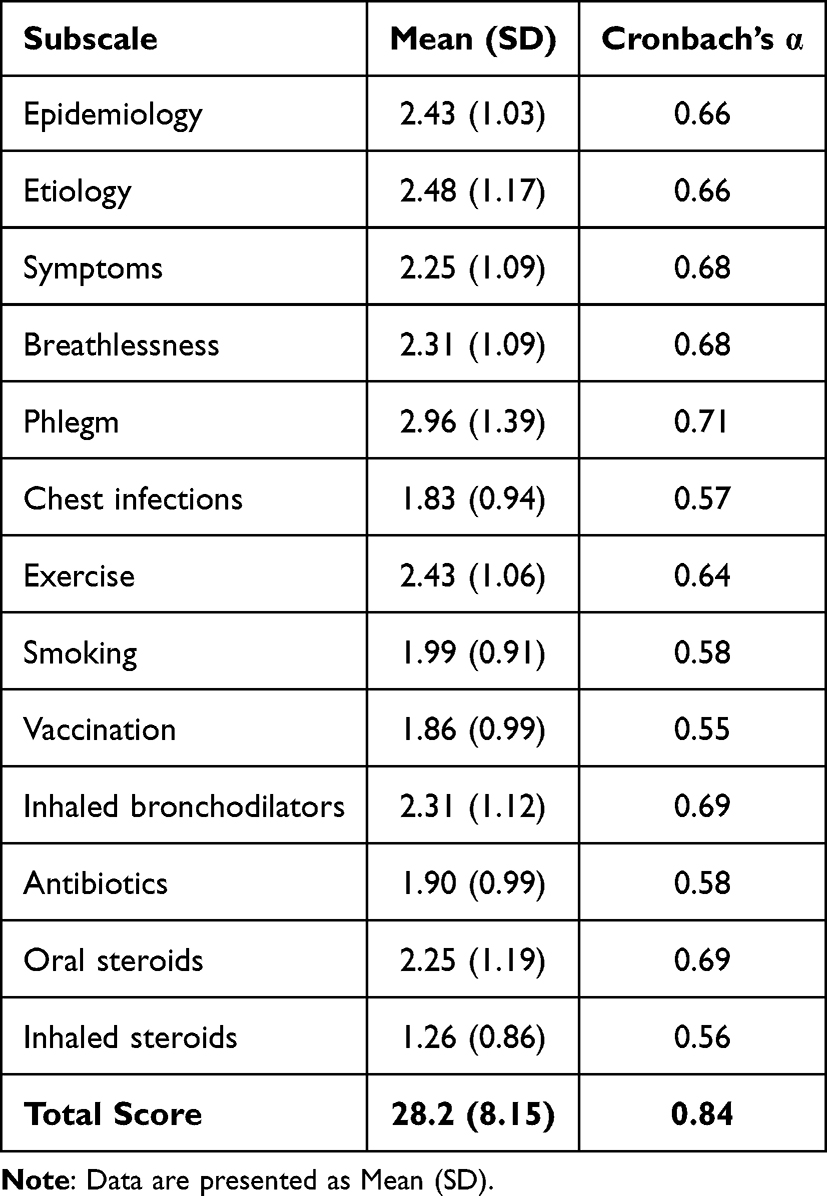 |
Table 2 Results for Each Subscale of the Questionnaire for the Whole Group of Participants |
In contrast, the lowest scores were observed in Inhaled Steroids (1.26 ± 0.86), Chest Infections (1.83 ± 0.94), and Vaccination (1.86 ± 0.99), highlighting notable knowledge gaps in prevention and pharmacological management. The overall total knowledge score across all subscales was 28.2 ± 8.15, indicating a moderate level of COPD knowledge among the participating healthcare professionals.
Total COPD knowledge scores were compared across demographic and participant characteristics (Table 3). There were no significant differences in total scores between males and females (p = 0.54). However, profession was an important factor, with family medicine physicians achieving the highest scores (29.97 ± 7.70), followed by general practitioners and nurses (p = 0.004).
 |
Table 3 Comparison of Total Knowledge Scores Across Demographic and Professional Groups |
Participants from the central and southern regions had significantly higher knowledge scores compared to those from other regions (p = 0.001). Similarly, those working in governmental institutions (29.37 ± 8.04) and hospital-based clinics (29.43 ± 7.54) scored significantly higher than their counterparts in private and primary care settings (p < 0.001 for both).
While years of experience did not significantly impact scores (p = 0.839), participants who had received prior COPD management training demonstrated significantly higher scores than those who had not (28.79 ± 7.64 vs 26.89 ± 9.18; p = 0.010). Additionally, those who self-reported adequate COPD knowledge had markedly higher scores (29.59 ± 7.36) compared to those who did not (24.80 ± 9.05; p < 0.001).
A multivariable linear regression analysis was performed to identify independent variables associated with the total COPD knowledge scores (Table 4). Participants who reported having adequate knowledge scored significantly higher than those who did not (β = 3.99; 95% CI: 2.47 to 5.51; p < 0.001), and those who had received prior COPD management training demonstrated significantly higher scores compared to those without such training (β = 1.89; 95% CI: 0.46 to 3.32; p = 0.011).
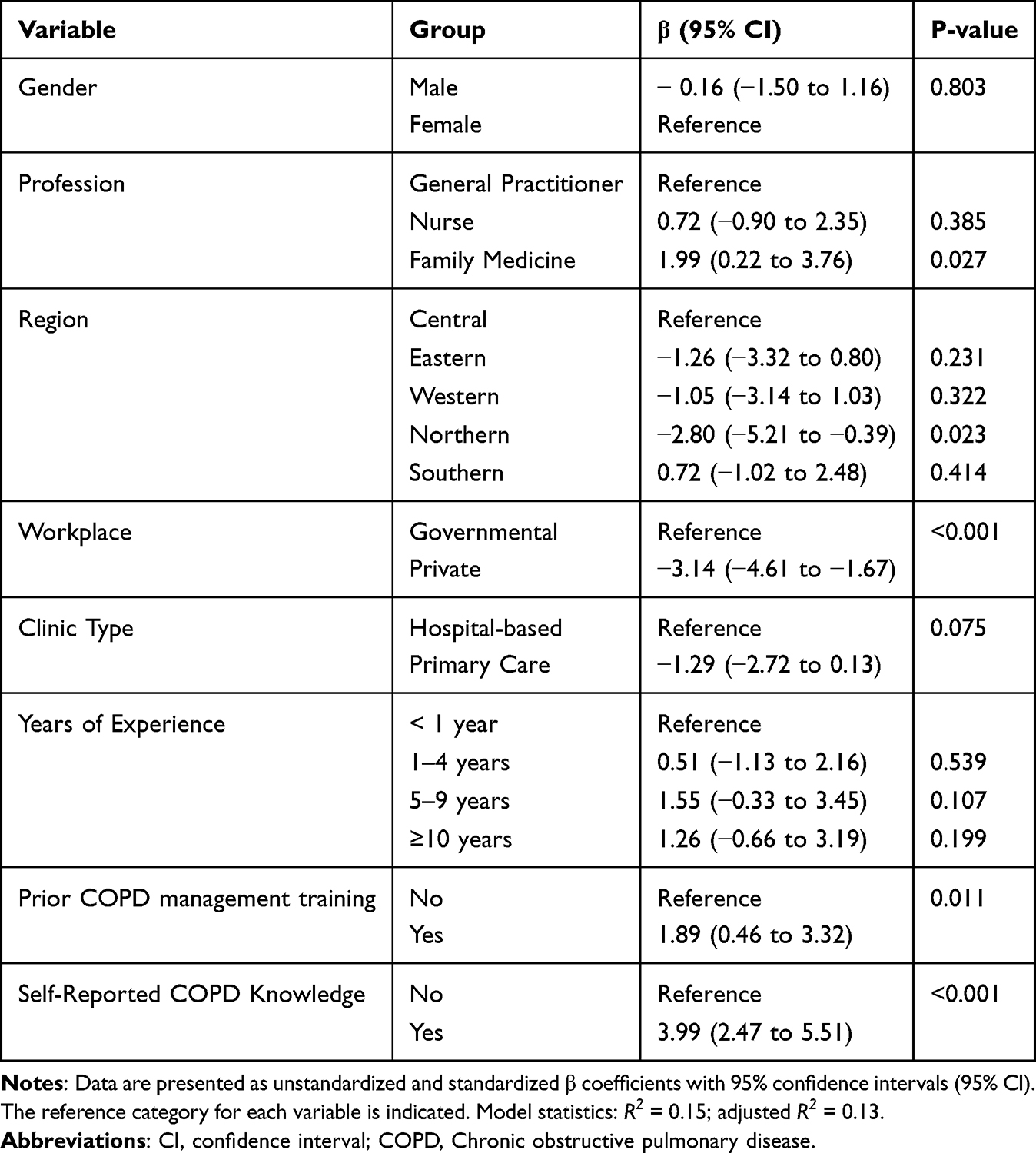 |
Table 4 Multivariable Linear Regression of Factors Associated with Total Knowledge Score |
Profession also showed a significant association, with family medicine physicians scoring higher than GPs (β = 1.99; 95% CI: 0.22 to 3.76; p = 0.027). Regarding geographic region, participants from the northern region had significantly lower scores compared to those from the central region (β = −2.80; 95% CI: −5.21 to −0.39; p = 0.023). Furthermore, working in the private sector was independently associated with lower knowledge scores relative to working in governmental institutions (β = −3.14; 95% CI: −4.61 to −1.67; p < 0.001). After adjustment, no significant associations were observed for gender, clinic type, or years of experience.
Discussion
This study explored the level of knowledge of COPD among healthcare professionals working in primary care settings in Saudi Arabia. The findings revealed a moderate overall knowledge level, with disparities across professional roles, regions, and types of workplaces. Notably, prior training and self-reported knowledge were strong factors contributing to high scores. The findings of this study highlight a significant gap in primary care practice, and suggest the urgent need for targeted educational intervention to enhance COPD-related knowledge.
The findings that healthcare professionals possessed only a moderate level of knowledge about COPD are alarming, given that they are the first point of contact for patients and play an important role in detecting and managing the disease.16 Our finding of moderate overall knowledge of COPD care among primary care providers is consistent with previous studies.7,17,18 International evidence consistently shows that COPD knowledge among primary care providers is moderate rather than optimal. The multinational survey by Aisanov et al9 reported average BCKQ scores of 40–50% across twelve countries, while the Swedish PRIMAIR study demonstrated nearly identical findings, with general practitioners answering 46% of items correctly.16 Likewise, the Turkish study by Göktalay et al15 reported a mean score of 29.8 out of 65 (46%), further underscoring that limited COPD knowledge is a persistent global trend.
Moreover, in China, a large national survey study showed that primary care physicians had poor knowledge of COPD, with a score below 55%. In particular, more than 90% of the respondents lacked knowledge about bronchodilators and managing stable cases, and less than 55% were aware of non-pharmacological treatment options for this disease.19 These results echo ours, especially the low scores in pharmacological and preventive domains, such as inhaled steroids and vaccinations. These low scores reflect a gap in preventive strategies and management in primary care practice. Conversely, our study showed the highest scores in Phlegm, Etiology, Exercise, and Epidemiology, which may be attributed to their familiarity with the symptoms through clinical exposure to symptomatic patients. Nevertheless, these strengths do not offset the need for targeted educational interventions to address the deficits in preventive and therapeutic knowledge. Strengthening COPD knowledge among healthcare professionals is critical for accurate diagnosis and management. It is also playing a pivotal role in supporting self-management in COPD. Evidence suggests that well-informed healthcare providers are more likely to deliver comprehensive, patient-centered education that addresses both medical and lifestyle aspects of COPD management.20 Such education can enhance patients’ understanding of their condition, encourage adherence to treatment plans, and improve their ability to recognise and respond to symptom changes. Ultimately, these improvements in self-management behaviors are associated with better health-related quality of life and reduced healthcare utilisation in COPD.20
Another interesting finding of this study is that the knowledge level differed by profession, with family medicine physicians achieving higher scores than nurses and general practitioners. A possible explanation for this might be that family medicine is exposed to broader training in chronic diseases compared with general practice and nursing. They also have more extensive training during residency, including rotations in pulmonary medicine and preventive medicine, which provides direct exposure to COPD management in both pharmacological and non-pharmacological aspects. In addition, they are more likely to be familiar with international guidelines, such as global initiative for chronic obstructive lung disease (GOLD) and national institute for health and care excellence (NICE), as part of their evidence-based training.21 Moreover, family medicine physicians often collaborate with other specialties, such as pulmonary and internal medicine, which can increase their exposure to a wider range of COPD interventions. Our result is consistent with the findings of Desalu, Onyedum,22 where family physicians had a higher score than general practitioners in COPD knowledge. This variation highlight the need for a tailored role-specific training program, especially for the first line of contact in primary care settings.
Geographic location and workplace sector were additional factors that influenced knowledge. Participants from the central region and those working in governmental and hospital-based clinics showed higher scores on the COPD knowledge scale. Similar location-linked differences have been documented elsewhere, where rural primary care has greater barriers to COPD care compared with urban locations.23,24 However, direct comparisons with other studies should be approached with caution, as the healthcare delivery system in Saudi Arabia differs substantially from those in many other countries. In Saudi Arabia, these variations may be partly explained by better access to continuing professional development, infrastructure, and the number of case mixes. These differences support the need for region-sensitive and sector-tailored implementation strategies to reduce inequities in COPD knowledge in primary care settings.
This study also found that healthcare workers in hospital-based clinics demonstrated higher knowledge scores than those in primary care centers. This difference may be due to the nature of hospital practice, where staff are more frequently exposed to specialised services, complex COPD cases with comorbidities, and a higher volume of patients. This exposure is likely to enhance familiarity with a broader range of diagnostic and management strategies, thereby contributing to higher knowledge levels.
Moreover, our study revealed that participants who had received prior COPD management training demonstrated significantly higher scores, and those who self-reported adequate COPD knowledge had markedly higher scores compared to those who did not. A previous study by Başyiğit, Yildiz,25 assessed the effect of training on knowledge level about COPD and found a significant increase in the rate of correct answers in the COPD survey after training. In addition, our findings align with the evidence from a controlled evaluation of a multicomponent continuous medical education program for primary care clinicians.26 That study reported that training led to significant improvements in both COPD knowledge and clinician confidence. These findings suggest that structured ongoing training and self-awareness are crucial for bridging the gaps and enhancing the skills of primary care healthcare workers to manage effectively.
Although the multivariable regression identified several factors statistically associated with total COPD knowledge scores, it is crucial to understand the practical significance of their real-world implication. Self-reported adequate knowledge was the strongest predictor, accounting for an approximate six percent improvement on the total scale. On the other hand, prior training, profession, and workplace sector contributed only marginally. These differences suggest that although training and professional background are relevant, they have limited practical impact on overall knowledge. Consequently, strategies that improve clinicians’ self-awareness, motivation, and learning context may be as important as formal instruction in improving COPD-related competence in primary care.
Implications for Practice
This study serves as an initial step to assess primary care physicians’ awareness of COPD, which has a steadily rising prevalence and incidence in Saudi Arabia.3 The findings of this study urge the development of a standardised COPD training programme for all healthcare providers, regardless of region or workplace setting. These programs should focus on the weakest areas identified, such as pharmacological and preventive aspects of COPD management, while also including all factors related to COPD knowledge. Although these programs should target all primary care healthcare professionals, particular emphasis should be placed on general practitioners and nurses, as they are the first point of contact for patients. Indeed, strengthening their skills, knowledge, and confidence through structured, role-specific training could facilitate earlier recognition of symptoms, more accurate diagnosis, and timely initiation of treatment. Moreover, better-trained healthcare providers would also be confidently able to educate patients about their disease, empowering them with the knowledge and skills necessary for effective self-management. This would likely contribute to improving patients’ outcomes by reducing exacerbations, fewer hospital admissions, and ultimately, a lower overall burden of COPD. Integrating continuous professional development and self-assessment tools within such training programs could sustain knowledge gains over time and promote a culture of proactive COPD care in primary healthcare settings.
Strengths and Limitations
A major strength of this study is that it is the first to assess the level of COPD-related knowledge among healthcare professionals in primary care settings across Saudi Arabia. The study recruited a relatively large sample from all regions of the country, enhancing its external validity and allowing for broad representation. In addition, the assessment tool used in this study comprehensively examined 13 domains of COPD knowledge, including pharmacological, preventive, and symptomatic aspects, thereby providing a detailed overview of current knowledge levels.
However, this study has several limitations that should be considered when interpreting the findings. First, although national coverage was achieved, participation was uneven across regions and levels of care, which may limit the generalisability of the findings. Second, the cross-sectional design captures knowledge at a single point in time and does not allow assessment of temporal changes or the impact of educational initiatives. Accordingly, the findings should be interpreted as reflecting knowledge patterns among engaged primary care healthcare professionals rather than population-level estimates, while still providing valuable insight into existing knowledge gaps and informing targeted educational strategies within similar primary care contexts.
Conclusion
This nationwide survey provides an updated overview of COPD-related knowledge among primary healthcare professionals in Saudi Arabia. Although overall knowledge levels were moderate, notable deficits were identified in pharmacological management and preventive care. Knowledge scores varied across professions, regions, and workplace sectors, and higher scores were consistently associated with prior COPD training and greater self-reported confidence—highlighting uneven preparedness within the primary care workforce.
These findings underscore the need for structured, role-specific educational programmes that prioritise areas of limited knowledge and support frontline providers in delivering evidence-based COPD care. National training strategies that ensure consistent COPD education across all primary care settings may enhance early recognition, optimise management practices, and strengthen patient education for self-management.
Acknowledgement
The authors acknowledge the Deanship of Scientific Research, Vice Presidency for Graduate Studies and Scientific Research at King Faisal University, Al-Ahsa, for providing financial support under the Ambitious Researcher Track “Grant No. KFU254808”.
Funding
This work was supported by the Deanship of Scientific Research, Vice Presidency for Graduate Studies and Scientific Research, King Faisal University, Saudi Arabia [Grant No. KFU254808].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cavaillès A, Brinchault-Rabin G, Dixmier A, et al. Comorbidities of COPD. Eur Respir Rev. 2013;22(130):454–12. doi:10.1183/09059180.00008612
2. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi:10.1371/journal.pmed.0030442
3. Alqahtani JS. Prevalence, incidence, morbidity and mortality rates of COPD in Saudi Arabia: trends in burden of COPD from 1990 to 2019. PLoS One. 2022;17(5):e0268772. doi:10.1371/journal.pone.0268772
4. Bourbeau J, Farias R, Li PZ, et al. The Quebec respiratory health education network: integrating a model of self-management education in COPD primary care. Chron Respir Dis. 2018;15(2):103–113. doi:10.1177/1479972317723237
5. Lee JY, Yoo KH, Kim DK, et al. Effects of educational interventions for chronic airway disease on primary care. J Korean Med Sci. 2016;31(7):1069–1074. doi:10.3346/jkms.2016.31.7.1069
6. Sigurgeirsdottir J, Halldorsdottir S, Arnardottir RH, Gudmundsson G, Bjornsson EH. COPD patients’ experiences, self-reported needs, and needs-driven strategies to cope with self-management. Int J Chronic Obstr. 2019;14:1033–1043. doi:10.2147/COPD.S201068
7. Aisanov Z, Bai C, Bauerle O, et al. Primary care physician perceptions on the diagnosis and management of chronic obstructive pulmonary disease in diverse regions of the world. Int J Chronic Obstr. 2012;7:271–282. doi:10.2147/COPD.S28059
8. Xingliang H, Juying D, Yingying W, et al. Practice-oriented training improves knowledge levels of chronic obstructive pulmonary disease among primary care physicians. Chin J General Practitioners. 2022;21(5):477–481.
9. Xingyao T, Ke H, Wei L, Cunbo J, Ting Y. Knowledge levels of chronic obstructive pulmonary disease among physicians in primary care and related factors: a survey in Zhumadian City of Henan Province. Chin J General Practitioners. 2022;21(5):422–429.
10. Raghavan D, Drummond KL, Sanders SA, Kirchner J. Use of implementation science to qualitatively identify implementation determinants of COPD practice guidelines in primary care. Chron Respir Dis. 2025;22:14799731251314870. doi:10.1177/14799731251314870
11. (GOLD) GIfCOLD. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2025 report). 2025.
12. Al-Jahdali H, Al-Lehebi R, Lababidi H, et al. The Saudi thoracic society evidence-based guidelines for the diagnosis and management of chronic obstructive pulmonary disease. Ann Thoracic Med. 2025;20(1):1–35. doi:10.4103/atm.atm_155_24
13. White R, Walker P, Roberts S, Kalisky S, White P. Bristol COPD knowledge questionnaire (BCKQ): testing what we teach patients about COPD. Chron Respir Dis. 2006;3(3):123–131. doi:10.1191/1479972306cd117oa
14. Gupta KK, Attri JP, Singh A, Kaur H, Kaur G. Basic concepts for sample size calculation: critical step for any clinical trials! Saudi J Anaesth. 2016;10(3):328–331. doi:10.4103/1658-354X.174918
15. Ministry of Health. Statistical Yearbook - health resources 2023. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/book/Pages/default.aspx.
16. Lin CH, Cheng SL, Chen CZ, Chen CH, Lin SH, Wang HC. Current progress of COPD early detection: key points and novel strategies. Int J Chron Obstruct Pulmon Dis. 2023;18:1511–1524. doi:10.2147/COPD.S413969
17. Göktalay T, Tuncal AN, Sarı S, Köroğlu G, Havlucu Y, Yorgancıoğlu A. Knowledge level of the primary healthcare providers on chronic obstructive pulmonary disease and pulmonary rehabilitation. Pulm Med. 2015;2015:538246. doi:10.1155/2015/538246
18. Sandelowsky H, Natalishvili N, Krakau I, Modin S, Ställberg B, Nager A. COPD management by Swedish general practitioners – baseline results of the PRIMAIR study. Scandinavian J Prim Health Care. 2018;36(1):5–13. doi:10.1080/02813432.2018.1426148
19. Pan Z, Yang T, Chi C, et al. An online survey of primary care physicians’ knowledge of common respiratory diseases in China. Npj Prim Care Respiratory Med. 2022;32(1):28. doi:10.1038/s41533-022-00289-5
20. Cravo A, Attar D, Freeman D, Holmes S, Ip L, Singh SJ. The importance of self-management in the context of personalized care in COPD. Int J Chronic Obstr. 2022;17(null):231–243. doi:10.2147/COPD.S343108
21. Saudi Commission for Health Specialties. Saudi board for family medicine curriculum 3rd ed. 2022.
22. Desalu OO, Onyedum CC, Adeoti AO, et al. Guideline-based COPD management in a resource-limited setting - physicians’ understanding, adherence and barriers: a cross-sectional survey of internal and family medicine hospital-based physicians in Nigeria. Prim Care Respir J. 2013;22(1):79–85. doi:10.4104/pcrj.2013.00014
23. Liu J, Zheng H, Pan H, Ye L, Li C. Chronic disease management professionals’ COPD knowledge: a survey in China’s rural health centres. Chin General Pract J. 2024;1(1):27–34. doi:10.1016/j.cgpj.2024.03.010
24. Robertson NM, Nagourney EM, Pollard SL, et al. Urban-rural disparities in chronic obstructive pulmonary disease management and access in Uganda. Chronic Obstr Pulm Dis. 2019;6(1):17–28. doi:10.15326/jcopdf.6.1.2018.0143
25. Başyiğit I, Yildiz F, Başoğul A, Boyaci H, Ilgazli A. The effect of postgraduate education on COPD knowledge level of primary care physicians. Tuberk Toraks. 2006;54(1):51–55.
26. Adams SG, Pitts J, Wynne J, et al. Effect of a primary care continuing education program on clinical practice of chronic obstructive pulmonary disease: translating theory into practice. Mayo Clin Proc. 2012;87(9):862–870. doi:10.1016/j.mayocp.2012.02.028
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Basic Determinants of Disease Knowledge in COPD Patients: Results from COSYCONET
Fischer C, Jörres RA, Alter P, Trudzinski FC, Yildirim, Bals R, Vogelmeier CF, Kauffmann-Guerrero D, Behr J, Watz H, Holle R, Kahnert K
Patient Preference and Adherence 2022, 16:1759-1770
Published Date: 26 July 2022
GOLD 2023 Update: Implications for Clinical Practice
Tamondong-Lachica DR, Skolnik N, Hurst JR, Marchetti N, Rabe APJ, Montes de Oca M, Celli BR
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:745-754
Published Date: 5 May 2023
A Long-Term Study of Adverse Outcomes Associated With Oral Corticosteroid Use in COPD

Tse G, Emmanuel B, Ariti C, Bafadhel M, Papi A, Carter V, Zhou J, Skinner D, Xu X, Müllerová H, Price D
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2565-2580
Published Date: 15 November 2023
Misdiagnosis of Chronic Heart Failure in Patients with Type 2 Diabetes Mellitus in Primary Care: A Report of Two Cases and Literature Review

Yeshniyazov N, Posokhov IN, Medovchshikov VV, Kurmanalina G, Sartayeva A
Vascular Health and Risk Management 2024, 20:479-485
Published Date: 3 November 2024
Single-Inhaler Triple Therapy in Primary Care Across Europe: Expert Panel Consensus on the Consequences of Payer-Driven Access Rules and Call to Action
Di Marco F, Shahaj O, Valipour A, Legrand B, Jommi C, Micheletto C, Vogelmeier CF, Freeman D, Kocks JWH, Alves L, Rubio MC, Peché R, Palkonen Snr S, Winders T, Roche N
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1595-1612
Published Date: 22 May 2025