Back to Journals » Infection and Drug Resistance » Volume 19
Distribution and Antibiotic Resistance of Pathogens in Bloodstream Infections Among Elderly Patients in Sichuan Province (2020–2024)
Authors You Z ![]() , Huang X, Liu X, Yu H, Long S
, Huang X, Liu X, Yu H, Long S
Received 23 January 2026
Accepted for publication 24 March 2026
Published 31 March 2026 Volume 2026:19 598477
DOI https://doi.org/10.2147/IDR.S598477
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Zhuorui You,1 Xiangning Huang,2 Xin Liu,2 Hua Yu,2 Shanshan Long2
1School of Medicine, University of Electronic Science and Technology of China, Chengdu, 611731, People’s Republic of China; 2Department of Laboratory Medicine, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu, 610072, People’s Republic of China
Correspondence: Shanshan Long, Email [email protected] Hua Yu, Email [email protected]
Objective: To characterize the distribution and antimicrobial resistance patterns of pathogens causing bloodstream infections in elderly patients in Sichuan Province from 2020 to 2024.
Methods: Non-duplicate isolates from blood of patients aged ≥ 65 years in 134 provincial medical institutions (113 tertiary, 21 secondary) were collected and tested per a unified protocol. Species identification and susceptibility were interpreted using CLSI M100 criteria. Data were analyzed with WHONET 5.6. The study period was stratified into pandemic (2020– 2022) and post-pandemic (2023– 2024) phases to assess effects on multidrug-resistant and pandrug-resistant organisms.
Results: 65,603 isolates were obtained from elderly patients’ blood specimens, of which 23,350 (35.6%) were Gram-positive and 42,253 (64.4%) were Gram-negative. The five most frequently detected organisms were Escherichia coli (38.4%), Klebsiella pneumoniae (12.6%), Staphylococcus hominis (6.6%), Staphylococcus epidermidis (6.0%), and Staphylococcus aureus (5.8%). E. coli exhibited low carbapenem resistance (ertapenem 0.8%, imipenem 0.9%, meropenem 0.9%), whereas K. pneumoniae showed carbapenem resistance of 6.7– 8.4%. Methicillin-resistant S. aureus and methicillin-resistant coagulase-negative staphylococci were detected at rates of 29.1% and 70.8%, respectively; no vancomycin-resistant staphylococci were identified. A total of 126 pandrug-resistant Acinetobacter baumannii (PDR-AB) isolates were identified, accounting for 11.2% (126/1124). No pandrug-resistant Enterobacterales or Pseudomonas aeruginosa were detected. In the post-pandemic period, the detection rates of carbapenem-resistant A. baumannii and carbapenem-resistant Klebsiella pneumoniae increased significantly compared with the pandemic period (P < 0.05).
Conclusion: From 2020 to 2024, a diverse spectrum of bacterial species was isolated from bloodstream infections in elderly patients in Sichuan Province. Following the COVID-19 pandemic, the burden of carbapenem-resistant organisms increased. Region-specific antimicrobial resistance surveillance and strengthened in-hospital infection control are essential to guide appropriate antibiotic use and to curb the spread of resistant organisms.
Keywords: elderly patients, bloodstream infections, multidrug-resistant organisms, Sichuan Province, COVID-19 pandemic
Introduction
Bloodstream infection (BSI) is a severe systemic infectious disease characterized by high incidence, high mortality, and rapid progression, and it has become a major global public-health challenge.1 It is estimated that approximately 30 million people worldwide develop BSI each year;2 the risk of death is closely related to pathogen virulence, the host’s immune status, and the timeliness of antimicrobial therapy. Older adults (aged ≥65 years) constitute a high-risk population for BSI because of age-related physiological decline, immunosenescence, and frequent comorbidities such as diabetes mellitus, chronic obstructive pulmonary disease, and cardiovascular disease; they therefore experience more severe illness and poorer outcomes after infection.2 China has entered a moderately aging society, characterized by a large and steadily increasing elderly population. From 2020 to 2024, the number of individuals aged ≥65 years increased from 200.56 million to 220.23 million, with the proportion rising from 14.2% to 15.6%.3 Multiple international studies have documented the heavy burden of BSI in the elderly. Data from the Swiss Antimicrobial Resistance Surveillance System showed a 14% increase in BSI incidence among older patients from 2008 to 2014, substantially higher than in the general population.4 A Canadian population study reported that the incidence of hospital-acquired BSI in older adults (2.7 per 100 admissions) was three times that of younger patients, with 30-day mortality ranging from 17.3% to 26.9%.5 A Brazilian hospital cohort found a mortality rate as high as 31.4% among elderly BSI patients.6 Timely selection of appropriate antimicrobial agents is critical to reducing BSI complications and improving prognosis, and it can also slow the emergence and spread of multidrug-resistant organisms.7 The epidemiology of BSI is influenced by regional environment, health-care resource allocation, and patterns of antimicrobial use; consequently, pathogen distribution and resistance profiles vary significantly across countries and regions. China’s large elderly population creates an urgent need for BSI prevention and control, but large-sample, multicenter systematic studies of pathogen distribution and antimicrobial resistance specifically in elderly patients remain limited, hampering precise, regionally applicable clinical guidance. As a populous province in southwestern China, Sichuan provides representative medical data that reflect regional epidemiological patterns. Leveraging a provincial surveillance network comprising 134 healthcare institutions (113 tertiary and 21 secondary hospitals), this study systematically characterized the distribution of pathogens causing bloodstream infections (BSIs) in elderly patients and the temporal trends in antimicrobial resistance from 2020 to 2024. We further compared resistance patterns between the COVID-19 pandemic and post-pandemic periods and assessed the detection of pandrug-resistant (PDR) organisms. The findings aim to inform evidence-based antimicrobial selection and targeted infection prevention and control strategies, ultimately reducing the incidence and mortality of BSIs in the elderly population.
Materials and Methods
Strain Collection
This study included elderly patients (aged ≥65 years) from 134 medical institutions in Sichuan Province (113 tertiary hospitals and 21 secondary hospitals) between January 2020 and December 2024. Pathogenic isolates recovered from blood specimens of these patients through culture were included in the analysis.
Inclusion criteria: Patients aged ≥65 years with clinically suspected bloodstream infection, manifested by signs of infection such as fever, chills, or hypotension, and with positive blood culture results; Isolates obtained from routine clinical blood culture specimens, with isolation procedures compliant with standard clinical microbiology practices; For each patient, only the first isolate of the same pathogen was retained to ensure non-duplication; Complete isolate identification and antimicrobial susceptibility testing data meeting the requirements of the surveillance protocol.
Exclusion criteria: Patients aged <65 years or those with incomplete clinical information precluding age determination; Blood culture contaminants (eg, single positive cultures yielding skin commensals without clear clinical signs of infection or other supporting evidence); Duplicate isolates of the same pathogen from the same patient; Isolates with insufficient identification reliability (Vitek 2 system confidence <95% or MALDI-TOF mass spectrometry score <2.0) or with key antimicrobial susceptibility data missing; Isolates for which specimen collection, transport, or testing did not conform to standard procedures and could potentially compromise result accuracy.
A total of 65,603 non-duplicate isolates were ultimately included for statistical analysis. The study period was stratified as follows: 2020–2022 as the COVID-19 pandemic period and 2023–2024 as the post-pandemic period, to assess the impact of the pandemic on the epidemiology of multidrug-resistant (MDR) and pandrug-resistant (PDR) organisms. This study was a retrospective surveillance analysis and was approved by the Institutional Review Boards of Sichuan Provincial People’s Hospital and the University of Electronic Science and Technology of China (Approval No. 2025866). All procedures were conducted in strict accordance with relevant medical ethical standards.
Bacterial Identification and Antimicrobial Susceptibility Testing
Bacterial identification was performed using the Vitek 2 automated system (manufacturer: bioMérieux, Inc., Hazelwood, Missouri, USA) or the MALDI-TOF mass spectrometry system (manufacturer: bioMérieux S.A., Marcy-l’Étoile, France). Minimum inhibitory concentrations (MICs) and inhibition zone diameters were interpreted according to the CLSI M100 (34th edition).8 Tigecycline susceptibility was interpreted following FDA-recommended criteria,9 and colistin susceptibility was judged according to the relevant Chinese expert consensus.10
Quality Control
Quality control testing was performed weekly in accordance with CLSI recommendations, using the following ATCC control strains: Escherichia coli ATCC 25922, Klebsiella pneumoniae ATCC 700603, Enterobacter cloacae ATCC 700323, Pseudomonas aeruginosa ATCC 27853, Staphylococcus aureus ATCC 25923, and Enterococcus faecalis ATCC 29212.
Data Analysis
The distribution of pathogens and key antimicrobial susceptibility data, including resistance and susceptibility rates, were analyzed using WHONET 5.6. Differences in pathogen composition across departments and variations in resistant organism detection between the pandemic and post-pandemic periods were evaluated using SPSS 26.0, with a two-sided P < 0.05 considered statistically significant. Multidrug-resistant organisms were defined according to commonly used clinical criteria as isolates resistant to three or more classes of clinically relevant antimicrobial agents, including methicillin-resistant staphylococci (MRSA and MRCNS), carbapenem-resistant Enterobacterales (CRECO and CRKP), and vancomycin-resistant enterococci (VRE). The criterion for pandrug-resistant (PDR) organisms was defined as isolates resistant to all classes of antimicrobial agents tested in this study.
Results
Species Distribution
Between 2020 and 2024, a total of 65,603 non-duplicate pathogenic isolates were recovered from blood specimens of elderly patients. Of these, 23,350 (35.6%) were Gram-positive and 42,253 (64.4%) were Gram-negative. The five most frequently detected organisms were Escherichia coli (25,187; 38.4%), Klebsiella pneumoniae (8252; 12.6%), Staphylococcus hominis (4300; 6.6%), Staphylococcus epidermidis (3919; 6.0%), and Staphylococcus aureus (3827; 5.8%) (Table 1).
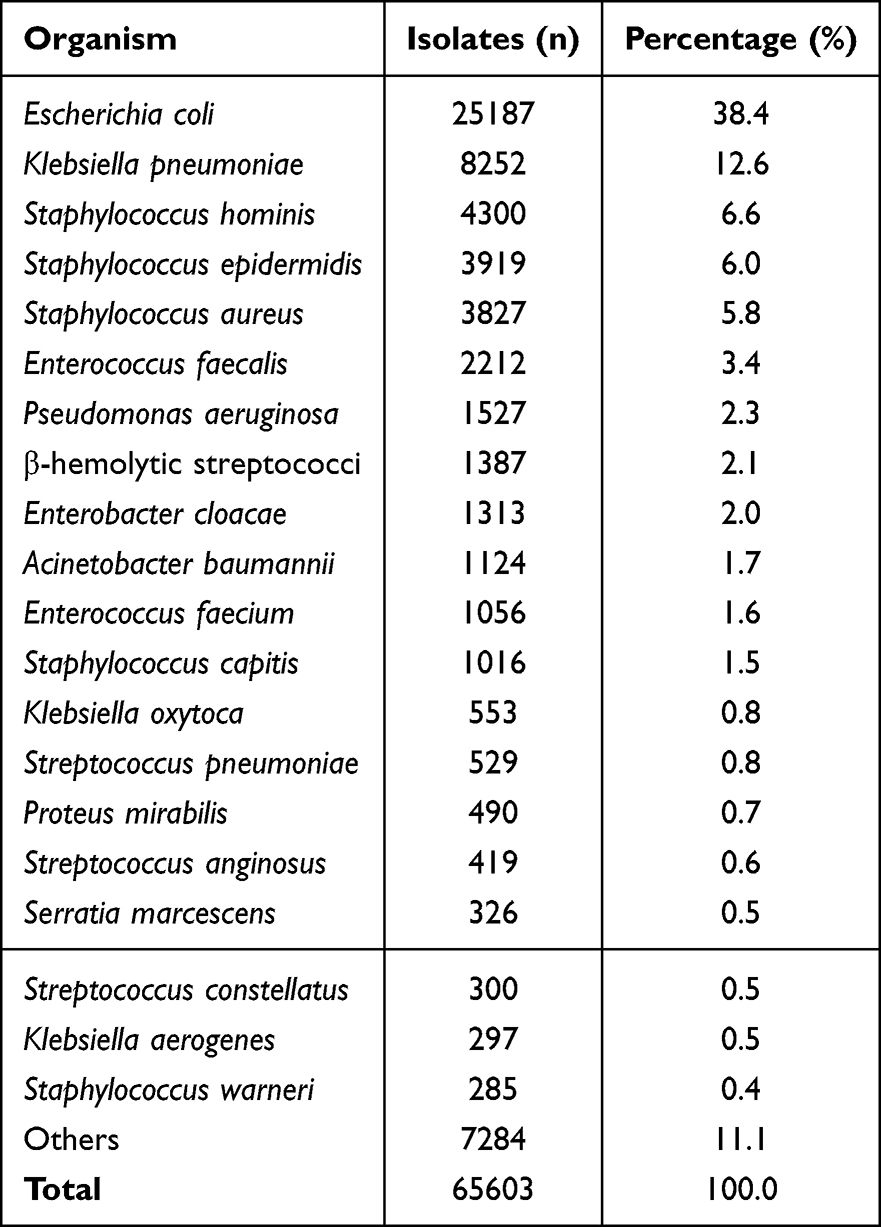 |
Table 1 Bacterial Composition of Blood Samples from Elderly Patients |
Isolates recovered from intensive care units (ICUs) were dominated by coagulase-negative staphylococci (33.6%), whereas non-ICU isolates were dominated by E. coli (42.3%). The proportions of Enterococcus spp. and Acinetobacter baumannii were significantly higher in ICU isolates (10.8% and 4.1%, respectively) than in non-ICU isolates (4.8% and 1.2%, respectively) (Table 2).
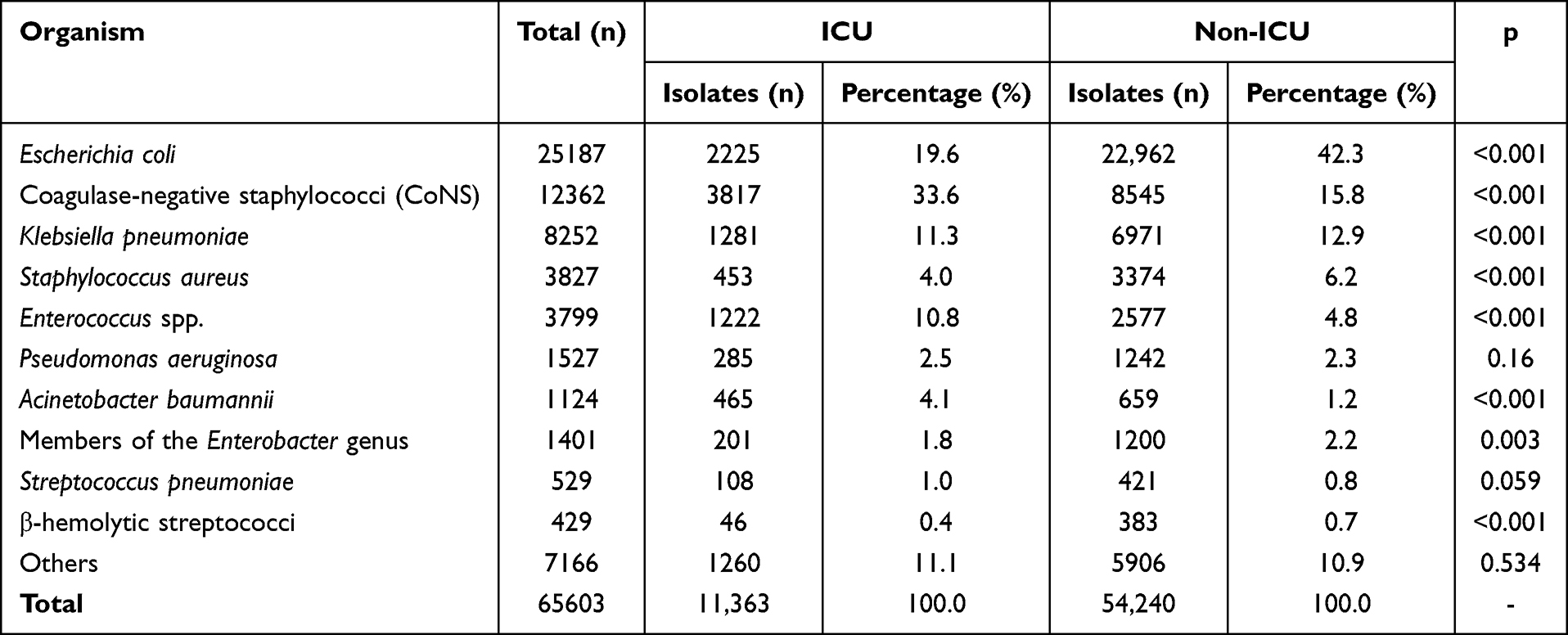 |
Table 2 Bacterial Composition of Blood Samples from ICU and Non-ICU Departments |
Major Gram-Negative Resistance Patterns
Carbapenem resistance rates were below 1.0% for Escherichia coli, and ranged from 3.5% to 8.4% for Klebsiella pneumoniae, Enterobacter cloacae, and Klebsiella aerogenes. Proteus mirabilis exhibited an imipenem resistance rate of 11.7%. Resistance to quinolones exceeded 42.6% in E. coli and P. mirabilis, while the five major Enterobacterales showed ceftriaxone resistance rates above 25.0%. Colistin resistance rates were 0.5% for E. coli, 3.3% for K. pneumoniae, and 1.5% for E. cloacae (Table 3).
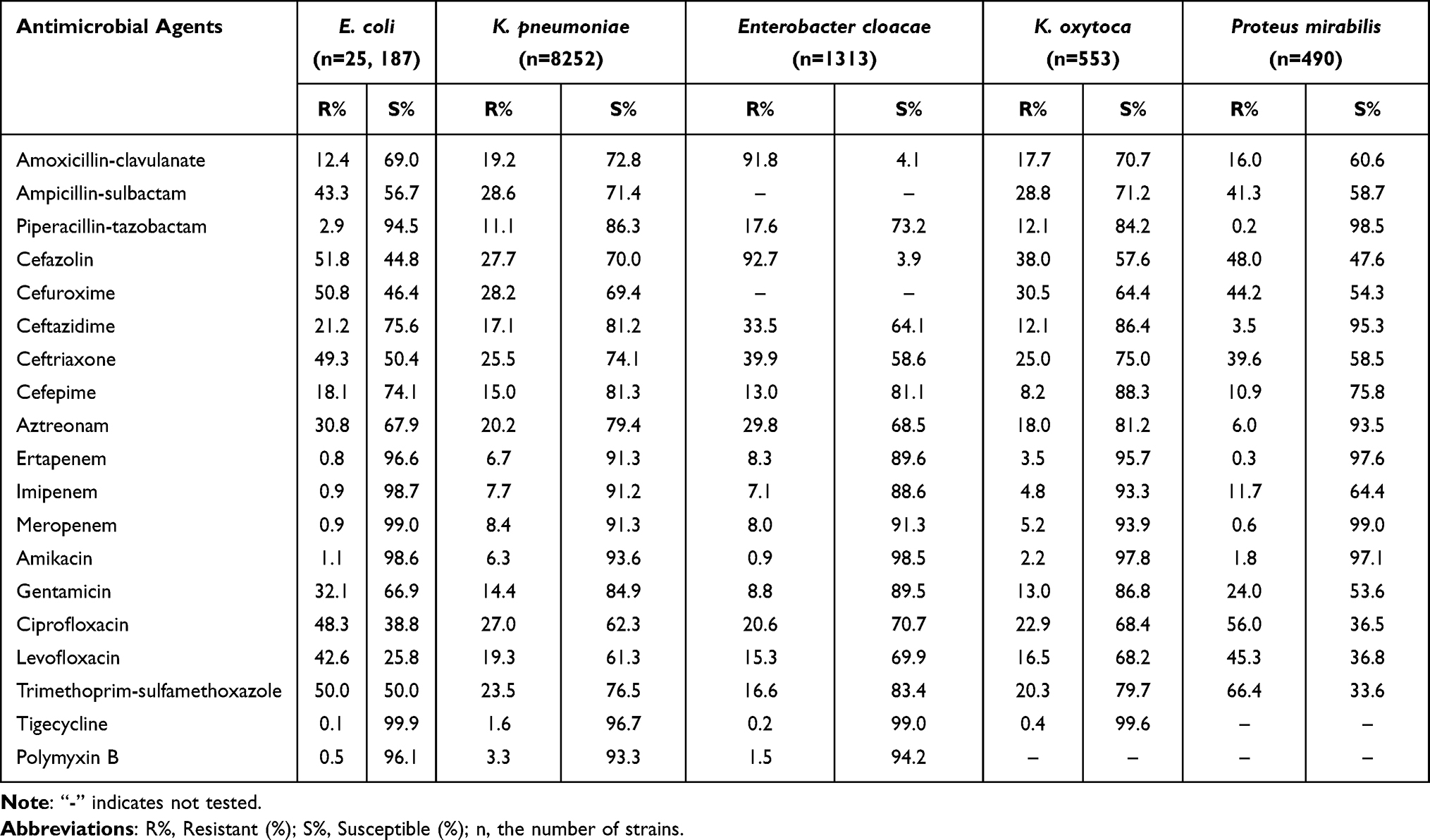 |
Table 3 Antibiotic Resistance and Sensitivity Rates of Enterobacteriaceae in Blood Samples from Elderly Patients |
Among non-fermenting bacteria, Pseudomonas aeruginosa exhibited aminoglycoside resistance below 4.2%, aztreonam resistance of 16.2%, and colistin resistance of 1.0%. Acinetobacter baumannii showed resistance rates of 54.5% to imipenem and 60.2% to meropenem, cephalosporin resistance above 54.9%, and colistin resistance of 0.7% (Table 4).
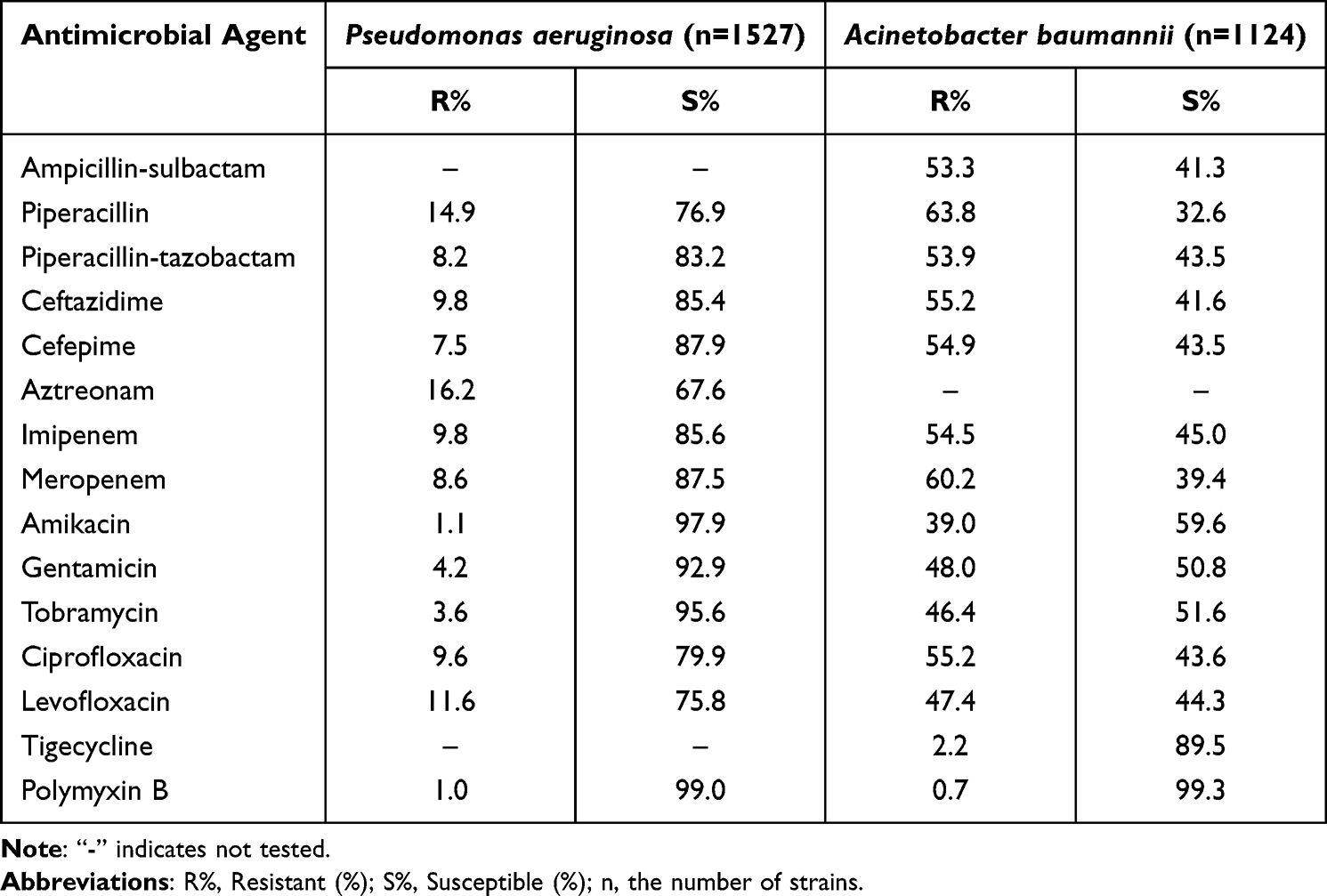 |
Table 4 Resistance and Sensitivity Rates of Major Non-Fermenting Bacteria in Blood Samples from Elderly Patients to Antimicrobial Drugs |
Major Gram-Positive Resistance Patterns
A total of 1113 methicillin-resistant Staphylococcus aureus (MRSA) and 8624 methicillin-resistant coagulase-negative staphylococci (MRCNS) were identified, corresponding to detection rates of 29.1% and 70.8%, respectively. Resistance rates for MRSA and MRCNS were higher than those of their methicillin-susceptible counterparts (MSSA and MSCNS) for most tested agents. No vancomycin-resistant staphylococci were detected (Table 5).
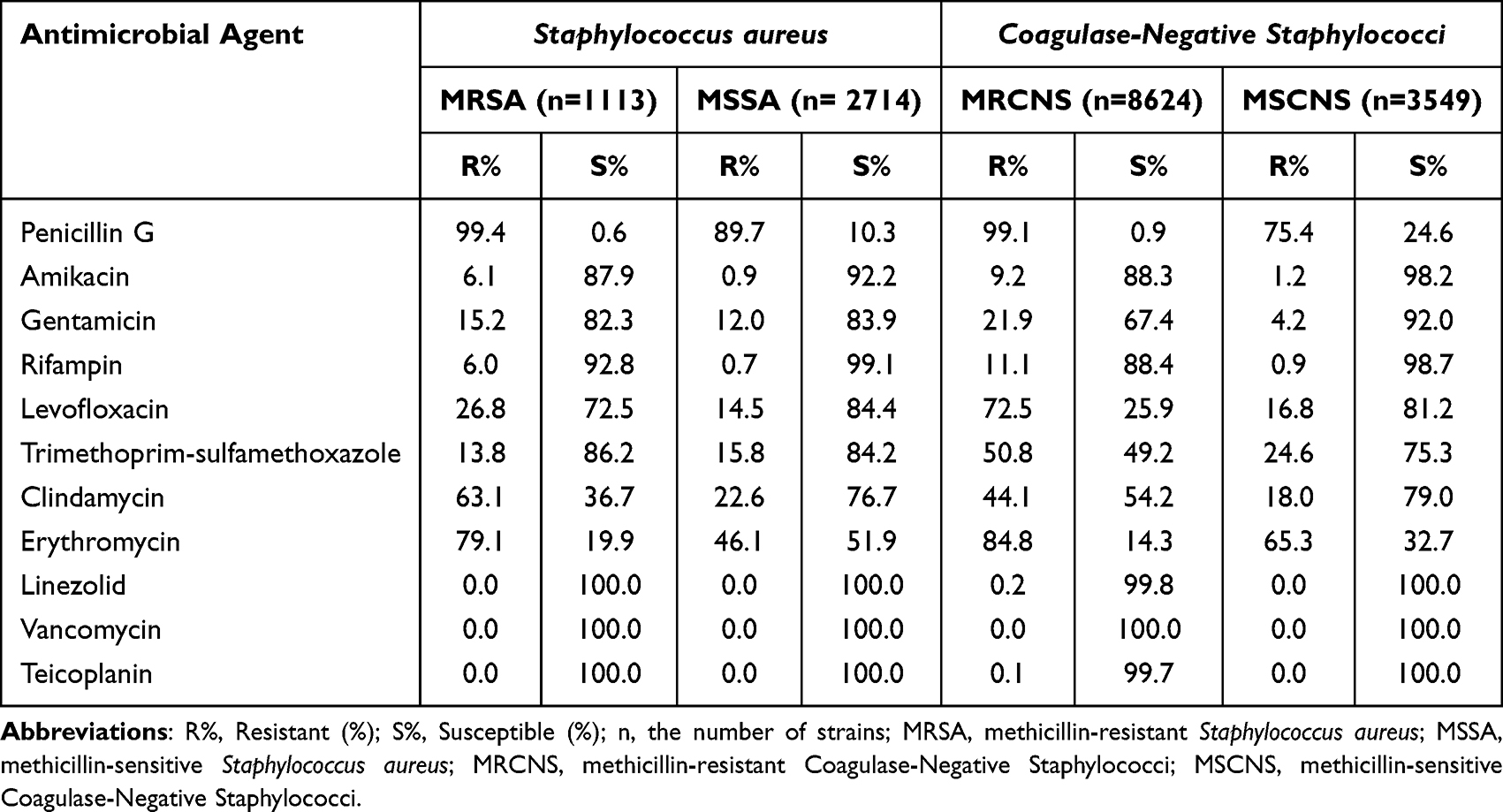 |
Table 5 Antibiotic Resistance and Sensitivity Rates of Staphylococcus Species in Blood Samples from Elderly Patients |
For enterococci, Enterococcus faecalis displayed higher resistance rates to most antimicrobials than Enterococcus faecium. Vancomycin and linezolid resistance rates for E. faecalis and E. faecium were 0.9% and 0.1%, and 0.4% and 2.0%, respectively (Table 6).
 |
Table 6 Antimicrobial Resistance and Susceptibility Rates of Enterococcus Species in Blood Samples from Elderly Patients |
Detection of Pandrug-Resistant Organisms (PDR) and Comparison of Resistant Organism Rates Between Pandemic and Post-Pandemic Periods
During 2020–2024, a total of 126 pandrug-resistant Acinetobacter baumannii (PDR-AB) isolates were identified from bloodstream infection specimens in elderly patients across the province, accounting for 11.2% (126/1124). No pandrug-resistant Enterobacterales or pandrug-resistant Pseudomonas aeruginosa (PDR-PA) were detected.
Comparison between the pandemic period (2020–2022) and the post-pandemic period (2023–2024) revealed a significant increase in the detection rates of carbapenem-resistant A. baumannii (CRAB) and carbapenem-resistant K. pneumoniae (CRKP) (P < 0.05). In contrast, the detection rates of methicillin-resistant Staphylococcus aureus (MRSA), carbapenem-resistant P. aeruginosa (CRPA), and other resistant organisms did not differ significantly (P > 0.05) (Table 7).
 |
Table 7 Changes in the Detection Rate of Drug-Resistant Bacteria in Blood Samples |
Discussion
A total of 65,603 non-duplicate isolates were recovered in this study, of which Gram-negative bacteria accounted for 64.4%—significantly higher than the national average (51.8%)—and Gram-positive bacteria accounted for 35.6%, lower than the national figure (48.2%).11 This regional difference may be closely related to the warm-humid climate of southwest China, which favors bacterial growth, the high regional prevalence of chronic comorbidities in the elderly (eg, diabetes mellitus, chronic obstructive pulmonary disease), and antibiotic prescribing preferences at primary care institutions (eg, frequent use of cephalosporins and fluoroquinolones).
The five most frequently detected pathogens were Escherichia coli (38.4%), Klebsiella pneumoniae (12.6%), Staphylococcus hominis (6.6%), Staphylococcus epidermidis (6.0%), and Staphylococcus aureus (5.8%). These results are consistent with the pathogen distribution reported for elderly BSI in Hebei Province,12 but show slight differences from findings in Jiangxi Province, where the principal isolates were E. coli, K. pneumoniae, S. aureus, Enterococcus faecalis, and S. epidermidis.13 Despite regional heterogeneity in pathogen distribution, E. coli and K. pneumoniae remain the predominant pathogens causing BSI in the elderly nationwide, consistent with national surveillance of blood isolates from 2014−2019,11 indicating that these two species should be the central targets for elderly BSI prevention and control. The high detection rate of E. coli as the primary pathogen may be related to carriage of extended-spectrum β-lactamase (ESBL) genes and transmission of virulence islands;14 given the high ESBL positivity of E. coli reported in national studies,15–17 subsequent molecular epidemiology investigations are warranted to characterize local virulence gene profiles.
Notably, pathogen distribution differed significantly between ICU and non-ICU wards: coagulase-negative staphylococci were most prevalent in the ICU (33.6%), whereas E. coli predominated in non-ICU wards (42.3%); Enterococcus spp. (10.8% vs. 4.8%) and Acinetobacter baumannii (4.1% vs. 1.2%) were detected at significantly higher rates in the ICU than in non-ICU areas, and the differences were statistically significant (P < 0.001). These findings align with a multicenter study from Iran,18 with the primary contributing factor being the higher intensity of invasive procedures in ICU patients—central venous catheterization, duration of mechanical ventilation, and urinary catheterization rates were all significantly higher than in non-ICU settings. Coagulase-negative Staphylococcus, a normal constituent of skin and mucosal flora, can easily cause healthcare-associated infections via these devices. The high prevalence of Acinetobacter baumannii is likely related to the challenges of ICU environmental disinfection, frequent use of immunosuppressive therapies, and severe trauma in patients, all of which result in profound immunosuppression. Additionally, S. aureus was more common in non-ICU wards (6.2% vs. 4.0% in the ICU), which may be related to community-acquired infections and suggests attention to infection risk following community exposure in elderly patients.
ESBL-producing strains, carbapenem-resistant Enterobacterales (CRE), carbapenem-resistant A. baumannii (CRAB), and carbapenem-resistant Pseudomonas aeruginosa (CRPA) were the principal antimicrobial-resistance threats among Gram-negative BSI isolates in elderly patients.
Among Enterobacterales, the resistance rates of Escherichia coli and Klebsiella pneumoniae to carbapenems were <1.0% and 6.7%–8.4%, respectively, both remaining at relatively low levels globally. According to global surveillance data from 2023 to 2024, resistance rates for these two organisms reached 3.2%–10.5% in Southeast Asia, 25.3%–52.0% in India and Brazil, and were also somewhat higher in Europe and North America (1.2%–3.5% and 7.5%–15.3%) than in the present region, with only a few Northern European countries reporting comparable resistance levels.18–22 This favorable situation is largely attributable to the strict implementation of tiered antimicrobial stewardship policies in recent years, with precise regulation of clinical carbapenem use, which has substantially reduced the selective pressure driving the emergence and spread of resistant strains. From 2020 to 2024, the detection rate of carbapenem-resistant E. coli (CRECO) fluctuated between 0.9% and 1.5%, and that of carbapenem-resistant K. pneumoniae (CRKP) ranged from 6.5% to 10.1%. The detection rates of third-generation cephalosporin-resistant E. coli (CTX/CRO-R-ECO) and K. pneumoniae (CTX/CRO-R-KPN) were 46.2%–50.1% and 23.7%–27.0%, respectively—showing a slight upward trend overall but remaining below CHINET national surveillance levels23 and contemporary European data.24 CRKP, as the most prominent carbapenem-resistant Gram-negative pathogen, employs multiple cooperating resistance mechanisms (enzyme production, porin loss, efflux pump activation, plasmid transmission, and biofilm formation),25 and elderly patients infected with CRKP have significantly higher 28-day mortality than those infected with susceptible strains,26 posing major clinical challenges. Of note, Enterobacterales showed low resistance to polymyxin B and tigecycline ((0.5%–3.3% and 0.1%–1.6%, respectively), indicating these agents remain important treatment options for multidrug-resistant Enterobacterales. E. coli resistance to fluoroquinolones exceeded 42.6%; for non-critically ill elderly patients, piperacillin/tazobactam (susceptibility 94.5%) or cefepime (susceptibility 74.1%) may be preferred empiric choices, and empirical fluoroquinolone use should be avoided. K. pneumoniae showed a 25.5% resistance rate to ceftriaxone; in severe infections or when cephalosporin therapy fails, combination therapy with tigecycline and polymyxin B (combined susceptibility 93.3%) may be considered, but renal function must be monitored to mitigate polymyxin B nephrotoxicity. Clinical laboratories should further evaluate combination susceptibility testing of these agents with novel drugs such as ceftazidime-avibactam to expand therapeutic options. In addition, CRKP control measures-targeted rectal screening of high-risk populations, environmental cleaning and disinfection, and regulation of visitors and family contacts-should be reinforced to interrupt transmission of resistance genes.
Among non-fermenters, P. aeruginosa exhibited aminoglycoside resistance below 4.2% (amikacin susceptibility 97.9%) and carbapenem (imipenem, meropenem) resistance rates of 9.8% and 8.6%, respectively, indicating overall low resistance; for mild-to-moderate infections, amikacin combined with ceftazidime (susceptibility 85.4%) can be selected to reduce overuse of carbapenems. In contrast, A. baumannii displayed severe multidrug resistance: imipenem and meropenem resistance rates reached 54.5% and 60.2%, cephalosporin resistance exceeded 54.9%, and high susceptibility was retained only to tigecycline (resistance 2.2%) and polymyxin B (resistance 0.7%). From 2020 to 2024, CRAB detection rates ranged from 50.2% to 64.1%; although lower than the reported national level of 78.0%,23 CRAB prevalence remains high. Prior antimicrobial exposure and ICU admission are independent risk factors for CRAB infection,27 and treatment is particularly challenging in elderly patients once infection occurs. According to expert consensus,28 infections caused by multidrug-resistant or pandrug-resistant strains may be treated with combination regimens including polymyxins or tigecycline. The tigecycline minimum inhibitory concentration (MIC) should be determined before therapy, as treatment success is higher when the MIC is ≤2 mg/L, and dosing should be individualized in elderly patients with hepatic or renal dysfunction.29 In parallel, excessive use of carbapenems should be curtailed, and novel prevention and control strategies, such as decolonization therapy or vaccine-based approaches, should be explored.30
The COVID-19 pandemic has markedly altered the epidemiology of resistant organisms in bloodstream infections among elderly patients. During the pandemic period (2020–2022), increased exposure to invasive procedures and extensive use of broad-spectrum antibiotics intensified the selective pressure for carbapenem-resistant organisms. In the post-pandemic period (2023–2024), the detection rates of CRAB and CRKP rose significantly, indicating a delayed and sustained transmission of resistant bacteria. In this study, pan-drug-resistant strains accounted for 11.2% of Acinetobacter baumannii isolates, with no pan-drug-resistant Enterobacterales or Pseudomonas aeruginosa detected, suggesting that the regional PDR risk remains generally controllable. Pandemic-related changes in clinical practices represent a key driver of increased MDR prevalence, underscoring the need for ongoing antimicrobial stewardship and infection control measures.
Among Gram-positive bacteria, methicillin-resistant S. aureus (MRSA) and methicillin-resistant coagulase-negative staphylococci (MRCNS) detection rates were 29.1% and 70.8%, respectively; the MRSA rate was lower than the CHINET national monitoring result (38.8%).22 Susceptibility testing showed that MRSA and MRCNS had significantly higher resistance to penicillins, aminoglycosides, and fluoroquinolones than methicillin-sensitive strains (MSSA and MSCNS). No isolates resistant to vancomycin, teicoplanin, or linezolid were detected, indicating that glycopeptides and oxazolidinones remain the last line of defense against multidrug-resistant infections. The resistance mechanism of MRSA is primarily mediated by the mecA gene encoding the PBP2a protein,31 and clinical management should therefore be guided by local antimicrobial resistance surveillance data to avoid indiscriminate use of β-lactam agents. In terms of therapy, linezolid may be selected for mild-to-moderate infections, with the oral formulation offering convenience for elderly patients, whereas severe infections may be treated with a combination of vancomycin and rifampin (rifampin susceptibility rate, 92.8%), with therapeutic drug monitoring of vancomycin to ensure safety and efficacy. Concurrently, infection control measures—including strict hand hygiene, environmental disinfection, and sterilization of medical devices—should be reinforced to reduce the risk of nosocomial cross-transmission.
Within Enterococcus spp., Enterococcus faecalis exhibited markedly higher resistance rates to most antibiotics than Enterococcus faecium: resistance of E. faecalis to penicillin G, ampicillin, and ciprofloxacin was 89.7%, 87.9%, and 89.4%, respectively, whereas corresponding rates for E. faecium were only 6.1%, 4.4%, and 23.9%. Vancomycin resistance rates for E. faecalis and E. faecium in this study were 0.9% and 0.1%, and linezolid resistance rates were 0.4% and 2.0%, respectively-both lower than CHINET 2023 reports of 3.2%/0.1% (vancomycin) and 0.4%/3.8% (linezolid).32 Overall, resistance pressure among enterococci was relatively low. Clinically, E. faecalis infections should avoid penicillin/ampicillin and preferentially use linezolid (susceptibility 99.2%) or high-dose daptomycin; for bloodstream infections caused by vancomycin-resistant enterococci (VRE), high-dose daptomycin is recommended, as it is associated with better clinical outcomes than linezolid33 and is more suitable for elderly patients.
This study has several limitations. As a retrospective surveillance analysis, detailed clinical data (for example, comorbidities, prior antibiotic exposure, and outcomes) were not collected, preventing further analysis of risk factors for resistant infections and comparative effectiveness of different treatment regimens. Second, although surveillance data were obtained from 134 medical institutions across Sichuan Province and therefore reflect BSI patterns in southwest China, caution is required when extrapolating these results to other regions of the country. Finally, susceptibility testing for certain antimicrobials was not performed on all isolates, which may affect the completeness of related resistance data. Future prospective cohort studies that integrate clinical information with molecular epidemiology techniques are needed to elucidate transmission mechanisms and clinical determinants of resistant organisms, thereby informing more precise diagnostic, therapeutic, and infection-control strategies.
Conclusion
In southwestern China, bloodstream infections (BSIs) in elderly patients are predominantly caused by Escherichia coli, Klebsiella pneumoniae, and Staphylococcus aureus, with a diverse range of pathogens exhibiting variable antimicrobial resistance profiles. Continuous surveillance of resistance is therefore essential, particularly for CRE, CRAB, and MRSA, as the prevalence of multidrug-resistant organisms differs significantly between the pandemic and post-pandemic periods. As a high-risk population for severe infections, elderly patients should receive antimicrobial therapy guided by local resistance data and susceptibility testing. Healthcare institutions should maintain vigilant post-pandemic resistance monitoring and, whenever possible, isolate patients harboring multidrug-resistant organisms to prevent in-hospital transmission.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu, China (No. 2025866). The ethics committee waived the need for written informed consent provided by participants due to the retrospective nature of this study. Patients’ anonymous information was provided from the microbiology hospital laboratory, which isolated the strains. The study completely followed the principles outlined in the Declaration of Helsinki.
Funding
The authors declare that no financial support was received for the research and/or publication of this article.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Zhang S, Zhang X, Yu W, Lin Z, Chen D. Infection biomarkers in assisting the judgement of blood stream infection and patient prognosis: a retrospective study incorporating principal components analysis. Ann Transl Med. 2020;8(23):1581. doi:10.21037/atm-20-3425
2. Lamy B, Sundqvist M, Idelevich EA. Bloodstream infections – standard and progress in pathogen diagnostics. Clin Microbiol Infect. 2020;26(2):142–11. doi:10.1016/j.cmi.2019.11.017
3. Office of the National Working Commission on Aging, China National Committee on Aging, China Research Center on Aging. China aging development report (2025). Beijing: China Social Publishing House; 2025. in Chinese.
4. Buetti N, Atkinson A, Marschall J, Kronenberg A; the Swiss Centre for Antibiotic Resistance (ANRESIS). Incidence of bloodstream infections: a nationwide surveillance of acute care hospitals in Switzerland 2008–2014. BMJ Open. 2017;7(3):e013665. doi:10.1136/bmjopen-2016-013665
5. Laupland KB, Pasquill K, Steele L, Parfitt EC. Burden of bloodstream infection in older persons: a population-based study. BMC Geriatr. 2021;21(1):31. doi:10.1186/s12877-020-01984-z
6. Da Silva NCZ, Da Rocha JA, Do Valle FM, Silva ASDN, Ehrlich S, Martins IS. The impact of ageing on the incidence and mortality rate of bloodstream infection: a hospital-based case–cohort study in a tertiary public hospital of Brazil. Tropical Med Int Health. 2021;26(10):1276–1284. doi:10.1111/tmi.13650
7. Yadav P, Kumar Yadav S. Progress in diagnosis and treatment of neonatal sepsis: a review article. J Nepal Med Assoc. 2022;60(247):318–324. doi:10.31729/jnma.7324
8. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing. M100-S34. Wayne, PA; 2024.
9. Research C for DE and. Tigecycline – injection products. FDA; 2023. Available from: https://www.fda.gov/drugs/development-resources/tigecycline-injection-products.
10. Yang Q, Xiaoling M, Fupin H. Expert consensus on colistin drug sensitivity testing and clinical interpretation. 2020;(05):559–570.
11. China Antimicrobial Resistance Surveillance System. National antimicrobial resistance surveillance network: evolution of antimicrobial resistance in blood specimen pathogens, 2014–2019. 2021;(02):124–133.
12. Wen H, Sun Q, Xie S. Characteristics of pathogens and antimicrobial resistance in elderly patients with bloodstream infections in Hebei Province, 2016–2019. 2022;(22):4822–4830.
13. Zhou X, Zhou J, Jingwen G, Liu X. Analysis of pathogen distribution and mortality risk factors in elderly patients with bloodstream infections. 2022;(01):48–53.
14. Bharathi SV, Rajamohan G. Biocide-resistant Escherichia coli ST540 co-harboring ESBL, dfrA14 confers QnrS-dependent plasmid-mediated quinolone resistance. Antibiotics. 2022;11(12):1724. doi:10.3390/antibiotics11121724
15. Salman S, Xu H, Chen Y, Ji J, Liu Z, Xiao Y. Characteristics and spatiotemporal changes in phenotypes and genotypes of extended-spectrum β-lactamases in Escherichia coli isolated from bloodstream infections in China from 2014 to 2021. Ann Clin Microbiol Antimicrob. 2025;24(1):7. doi:10.1186/s12941-025-00774-y
16. Wu HN, Yuan EY, Li WB, Peng M, Zhang QY, Liang XK. Microbiological and clinical characteristics of bloodstream infections in general intensive care unit: a retrospective study. Front Med. 2022;9:876207. doi:10.3389/fmed.2022.876207
17. Zhu M, Wang L, Zhuge Z, et al. Risk factors associated with multi-drug resistance in neonatal sepsis caused by Escherichia coli. IDR. 2023;16:2097–2106. doi:10.2147/IDR.S403135
18. Kassaian N, Nematbakhsh S, Yazdani M, Rostami S, Nokhodian Z, Ataei B. Epidemiology of bloodstream infections and antimicrobial susceptibility pattern in ICU and non-ICU wards: a four-year retrospective study in Isfahan, Iran. Adv Biomed Res. 2023;12(1). doi:10.4103/abr.abr_320_22
19. Ajulo S, Awosile B. Global antimicrobial resistance and use surveillance system (GLASS 2022): investigating the relationship between antimicrobial resistance and antimicrobial consumption data across the participating countries. PLoS One. 2024;19(2):e0297921. doi:10.1371/journal.pone.0297921
20. Sader HS, Castanheira M, Huband MD, Shorttidge D, Carvalhaes CG, Mendes RE. Bloodstream infections in the United States and Europe: etiology and antimicrobial susceptibility results from the SENTRY antimicrobial surveillance program (2016–2019). Open Forum Infect Dis. 2020;7(Supplement_1):S20–S20. doi:10.1093/ofid/ofaa417.036
21. World Health Organization. Global antibiotic resistance surveillance report 2025. Available from: https://www.who.int/publications/i/item/9789240116337.
22. One Health Trust. ResistanceMap. Available from: https://resistancemap.onehealthtrust.org/.
23. Zhong M, Huang X, Yu H, et al. Distribution and changes in antibiotic resistance of blood-isolated bacteria in CHINET, 2015–2021. Chin J Infect Chemother. 2024;6:664–677.
24. Pezzani MD, Arieti F, Rajendran NB, et al. Frequency of bloodstream infections caused by six key antibiotic-resistant pathogens for prioritization of research and discovery of new therapies in Europe: a systematic review. Clin Microbiol Infect. 2024;30:S4–13. doi:10.1016/j.cmi.2023.10.019
25. Xie C, Bai Y, Li Y, et al. Revealing sRNA expression profiles of NDM-5-producing CRKP and explore the role of sRNA207 in NDM-5-producing CRKP resistance. Microbiol Spectr. 2024;12(12):e01537–24. doi:10.1128/spectrum.01537-24
26. Chen Y, Chen Y, Liu P, et al. Risk factors and mortality for elderly patients with bloodstream infection of carbapenem resistance Klebsiella pneumoniae: a 10-year longitudinal study. BMC Geriatr. 2022;22(1):573. doi:10.1186/s12877-022-03275-1
27. Xue Y, Zou C, Taijie L. Risk factors and mortality rates in elderly patients with carbapenem-resistant Acinetobacter baumannii bloodstream infections: a ten-year retrospective study. 2024;(02):155–161.
28. Zhou H, Zhou J, Yunsong Y. Interpretation of the Chinese expert consensus on diagnosis, treatment and prevention of Acinetobacter baumannii infections. 2016;(01):26–29.
29. Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, Van Duin D, Clancy CJ. Infectious diseases society of America guidance on the treatment of AmpC β-Lactamase–producing enterobacterales, carbapenem-resistant Acinetobacter baumannii, and Stenotrophomonas maltophilia infections. Clinl Infect Dis. 2022;74(12):2089–2114. doi:10.1093/cid/ciab1013
30. Shi X, Zhang D. Antimicrobial resistance mechanisms associated with Acinetobacter baumannii and novel therapeutic approaches. 2025;(01):97–104.
31. Hou Z, Liu L, Wei J, Xu B. Progress in the prevalence, classification and drug resistance mechanisms of methicillin-resistant staphylococcus aureus. IDR. 2023;16:3271–3292. doi:10.2147/IDR.S412308
32. Guo Y, Fupin H, Zhu D. 2023 CHINET China antimicrobial resistance surveillance. 2024;(06):627–637.
33. White BP, Barber KE, Chastain DB. Treatment decisions in VRE bacteraemia: a survey of infectious diseases pharmacists. JAC-Antimicrob Resist. 2023;5(3):dlad063. doi:10.1093/jacamr/dlad063
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Bacterial Epidemiology and Antimicrobial Resistance Profiles of Respiratory Specimens of Children with Pneumonia in Hainan, China
Mai W, Liu Y, Meng Q, Xu J, Wu J
Infection and Drug Resistance 2023, 16:249-261
Published Date: 12 January 2023
Distribution and Antimicrobial Resistance Analysis of Blood Culture Isolates at a Chinese National Cardiovascular Regional Medical Center: A 7-Year Retrospective Study
Wang Q, Wu F, Li T
Infection and Drug Resistance 2025, 18:4249-4262
Published Date: 22 August 2025
Epidemiology and Antimicrobial Resistance Trends of Bloodstream Infections During and After the Implementation of the National Action Plan on Antimicrobial Resistance in Mwanza, Tanzania: A Comparative Cross-Sectional Study
Silago V, Matthews L, Oravcova K, Mshana SE, Seni J, Claus H
Infection and Drug Resistance 2025, 18:4441-4453
Published Date: 29 August 2025
Retrospective Analysis of Infection Characteristics and Prognostic Factors in ICU Sepsis Patients in Jiaxing Area
Li H, Tan X, Wang S, Shen W, Yuan B
Infection and Drug Resistance 2026, 19:576517
Published Date: 8 April 2026
Antimicrobial Resistance in Intensive Care Units in Somalia: A Commentary on Measurement Gaps and Facility-Level Priorities for Infection Prevention and Stewardship
Hassan AM, Siyad AO, Hussein AM
Infection and Drug Resistance 2026, 19:606434
Published Date: 18 May 2026