Back to Journals » Nursing: Research and Reviews » Volume 15
Discrepancies in Cardiovascular Disease Risk Perception Among African American Emerging Adults
Authors Smith SB ![]() , Magwood GS
, Magwood GS ![]() , Abshire DA, Tavakoli AS, McCutcheon GS
, Abshire DA, Tavakoli AS, McCutcheon GS ![]() , Jenerette C
, Jenerette C
Received 4 November 2024
Accepted for publication 16 April 2025
Published 17 May 2025 Volume 2025:15 Pages 57—77
DOI https://doi.org/10.2147/NRR.S499734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pariya Fazeli
Shannon Bright Smith,1 Gayenell S Magwood,2 Demetrius A Abshire,2 Abbas S Tavakoli,2 Gloria S McCutcheon,3 Coretta Jenerette4
1School of Nursing, Florida Agricultural and Mechanical University, Tallahassee, FL, USA; 2College of Nursing, University of South Carolina, Columbia, SC, USA; 3Biology Department, Claflin University, Orangeburg, SC, USA; 4School of Nursing, University of California, San Francisco, CA, USA
Correspondence: Shannon Bright Smith, Florida Agricultural and Mechanical University, 7620 Joe Allen Drive, Beaufort, SC, 29906, USA, Tel +01-843-437-3790, Email [email protected]
Background: Cardiovascular disease (CVD) disproportionately affects African Americans residing in the southern United States. While often diagnosed later in adulthood, CVD develops over time and risk factors emerge early in life. Perceptions of disease risk significantly influence health behaviors, yet young adults often underestimate their susceptibility.
Objective: This study compares CVD risk perception to actual CVD risk among African American emerging adults (AAEAs).
Methods: Using an explanatory sequential mixed methods approach guided by a situation-specific theory, we assessed CVD risk perception, objective CVD risk based on the American Heart Association’s Life’s Essential 8 metrics, and CVD knowledge in 28 AAEAs enrolled at a southeaster historically Black college/university. Descriptive statistics informed the selection of 16 participants for interviews to explore the reasons behind their perceptions and reactions to their objective risk assessment. These 16 participants were intentionally selected to reflect the distribution of participants across the perceived versus objective CVD risk categories represented in the full sample.
Results: Most participants underestimated their cardiovascular disease (CVD) risk. Specifically, 16 of 28 participants (57.14%) perceived their risk to be low; however, only 4 of these 16 individuals (25%) accurately assessed their risk. Among those with a low perceived risk, 11 (68.8%) were found to have a moderate objective risk, and 1 participant (6.3%) was classified as having a high risk. Upon learning their actual CVD risk, participants’ responses supported three primary themes: emotional awareness, personal analysis, and planned action.
Conclusion: Findings reflect a need to integrate personalized, culturally relevant CVD awareness and prevention strategies for AAEAs. Future research should involve larger cohorts to refine interventions that bridge the gap between perceived and actual CVD risk.
Plain Language Summary: The diagnosis of cardiovascular disease (CVD) in African American adults occurs later than other populations. In addition to late diagnoses, vascular changes and damage occur before clinical manifestations or diagnoses are received. We studied African American emerging adults (AAEAs) because young people form lifelong habits during this 18– 25-year-old period. It is also a time that we may help AAEAs recognize the impact of their behaviors and change negative behaviors to prevent CVD.
We surveyed 28 AAEAs at a southeastern HBCU to determine their perceived heart disease risk and objective heart health status using the American Heart Association’s Life Essential 8 measures. A subset of the group was selected for personal interviews to seek their thoughts after learning their objective CVD risk.
More than half of the participants (57.14%) thought their risk was low, but only 25% of those with low perceived risk were actually right, suggesting that AAEAs may underestimate their CVD risk. We found three primary themes participants expressed: emotional awareness, personal analysis, and planned action. Our small descriptive study is the beginning of how helping participants understand their objective CVD risk may help them understand the need for change and further facilitate behavioral change.
Keywords: cardiovascular disease, African American emerging adults, risk perception, health perception, heart health, CVD prevention, health disparities, Life’s Essential 8, CVD risk, young adult health, behavior change
Background
Cardiovascular or heart diseases include disorders affecting the heart or blood vessels, resulting in diminished oxygen supply to the vital organs.1 While cardiovascular disease (CVD) is predominantly associated with older age groups, its insidious pathogenesis takes root early in life.2 The gradual progression emphasizes the importance of promoting heart health from a young age.3 Emerging adulthood (ages 18–25) is a critical period of self-identity formation, increased autonomy, and adoption of life-long behaviors.4,5 Given that some African American emerging adults (AAEAs) already exhibit some CVD risk factors, addressing Cardiovascular Health (CVH) during this formative stage phase is essential to reduce future disease burden.5,6
Risk Factors for AAEAs
Studies have identified CVD risk factors related to behavioral and biological factors in AAEAs. More specifically, health behaviors include diet,7–11 physical activity (PA),12,13 nicotine exposure,14–23 and sleep health).24–26 Health factor risks refer to body mass index (BMI),27–29 blood lipids,6 blood glucose,30–33 and blood pressure (BP)).34–36 Other biological factors attributed to CVD risk in AAEAs include metabolic syndrome,37–39 biomarkers (eg, triglycerides, large artery stiffness, waist/hip circumference ratios, and neck circumference),40–45 and the physical effects of individual (including both internalized and interpersonal),46 systemic, structural,47 institutional,46 and cultural racism,11,48–56 and stress.57–59
Further, AAEAs encounter a unique combination of financial, academic, and social challenges that increase their stress levels and may increase the incidence of hypertension. Financial or economic stability indicators include income, wealth, employment status, and occupational category, and are determinants of access to care, safe housing, and many other factors that directly or indirectly affect CVD.60 For example, college students from disadvantaged socioeconomic statuses (SES) often use education loans to finance college, and the amount of loans is negatively related to net worth and nonfinancial assets at age 30.61 Lower paying employment opportunities and educational debt contributes to a wider gap in income by race.
African American college students are also more likely to face stress related to their racial and ethnic background than other races, which may prohibit academic success62 and increase CVD risk. Education is the most used indicator of socioeconomic position in the US, provides the most consistent results concerning CVD outcomes,63 and is inversely associated with coronary artery disease risk.64 For instance, people with at least a college degree had 4.12 times the odds of having an ideal CVH score.65 Yet, disparities in educational attainment between White and African American people have widened over time,63 increasing from a 14-point gap in 2016 to 20 points in 2022.66
Like education, health access and quality may contribute to CVH in AAEAs.67 The Affordable Care Act (ACA) decreased the number of African American adults without insurance.67–69 Since the ACA enactment, the percentages have trended downward in all races. However, non-White young adults experienced lower uninsured percentages (12.8% to 6.6%) than non-Hispanic Black (20% to 10%)) and Hispanic (32.6% to 18%) young adults.68 The number of AAEAs without access due to insurance coverage may be even higher, given the transition from parental insurance policies to self-support during emerging adulthood.
Another potential contributor to CVH is the social environment, which includes belonging, life and work stress, marginalization, deprivation, economic status, and community well-being. Racial socialization messages encouraging participants to engage in productive cross-racial interactions with different races positively predict spiritual-centered and collective coping.70 However, individual, interpersonal, institutional, structural, systemic, and cultural level racism are negative predictors of effective communal resilience,46,47,71 and institutional racism, discriminatory policies and practices occurring within social institutions59,62,71 influence health outcomes causing psychosocial stress and physiological dysregulation.
Health perception and culture also contribute to behaviors. Higher risk perception has been associated with greater health responsibility.72 Likewise, lower risk perception was correlated with less health responsibility.73 Culture, or a “set of shared and socially transmitted ideas about the world that are passed down from generation to generation”,74 which influences cultural behaviors. There are varying cultural influences in the African American community. African American emerging adult college students identified culture and race-specific coping styles different from other races,70 such as the benefits of valuing high standards and hard work.75 Benefits may include a sense of family or community that is part of the culture and serves as a source of social support.76 However, cultural influences such as dietary habits or negative racial or healthcare-related experiences may be harmful.77–79 In their compilation, negative health behaviors, abnormal biological factors, and adverse social determinants of health (SDOH)12,61,63,80–84 exacerbate health inequities in AAEAs and the resultant disparities in morbidity and mortality.
The American Heart Association established heart health measures using Life’s Essential 8 (LE8) components grouped into two domains of health behaviors (diet, PA, nicotine exposure, and sleep) and health factors (BMI, blood lipids, blood glucose, and BP) as a broader, more positive construct than disease absence.6 The 2022 update from Life’s Essential 7 (LS7) added sleep as a key measure of CVH.6
The gap in CVH and CVD research for AAEAs using Life’s Simple 7 (LS7) and Life’s Essential 8 (LE8) is significant and warrants attention. While LS7 has been integrated into over 400 studies, there is a notable scarcity of research focusing on AAEAs as the primary population. Four studies examined CVH in AAEAs using Life’s Simple 7 (LS7).35,85–87 Among the few studies using LS7 with AAEAs, Aycock et al86 leveraged LS7 as both a risk assessment tool and an educational framework to promote stroke risk reduction. Prior studies, like the present study, had small sample sizes, limiting generalizability. Acknowledging a small population (n=30), Aycock et al35 repeated the study with a larger sample (n=126), comparing health perception and stroke risk and integrating gender differences comparison. Recommendations included early stroke risk assessment and tailored prevention strategies. Research by Park et al88 used LS7 and Coronary Artery Risk Development in Young Adults (CARDIA) study data to assess CVH from young adulthood to midlife in Black and White men and women 18–30 years, examining how neighborhood environments influenced long-term health outcomes. Findings suggest that proximity to PA resources in early adulthood may play a crucial role in maintaining CVH later in life. Another study87 used LS7 to assess CVH in young adulthood and its long-term impact on CVD events and mortality using CARDIA study data. Findings demonstrate that maintaining high CVH early in life is strongly associated with significantly lower rates of premature CVD and mortality, emphasizing the need for early prevention strategies to promote lifelong heart health. No studies were found in which AHA Life’s Essential 8 (LE8) was used to evaluate CVH primarily in AAEAs. While small, these studies contribute to the growing body of evidence by focusing on a specific understudied population.
Gaps in the Literature
The presence of varied CVD risk factors for AAEAs has been described extensively in the literature.6–23,27–59 However, research to understand the complexity of CVD risk or promote CVH in the population is sparse. Despite these identified risk factors, a critical gap remains in understanding how these risk factors interact to influence overall CVH in AAEAs.
The lack of studies using LE8, a more recent tool from the American Heart Association (AHA), to assess CVH in AAEAs highlights an important research gap. LE8 includes critical factors such as sleep and diet that may offer new insights into addressing CVD risk in this population. Given the higher burden of CVD in AAEAs, understanding how LE8 factors interact within this community could inform tailored interventions and improve CVD outcomes. There is a clear need for research integrating LE8 to develop a comprehensive, culturally relevant framework for CVH promotion and CVD prevention in AAEAs. Addressing this gap could lead to more effective, targeted strategies for improving heart health and reducing disparities in CVD outcomes for this group.
Current Study
The study aimed to provide a descriptive overview of a comparison in the perceived and objective CVD risk among AAEAs, and explore their thoughts when learning their results.89 Ultimately, these findings may help explain the intent to perform health behaviors described in Unlocking Population Specific Treatments to Render Equitable Approaches and Management in Cardiovascular Disease (UPSTREAM CVD).4 This descriptive study utilizes the LE8 metrics and personal interviews in an HBCU setting, addressing a critical research gap. Research questions were 1) Quantitative: What is the relationship between perceived and objective cardiovascular disease (CVD) risk among African American emerging adults? Qualitative: What are African American emerging adults’ responses upon learning their objective risk, and how do they explain their perceived CVD risk?
Methods
This study employed a mixed-methods explanatory sequential design following Creswell and Plano Clark’s90 guidelines to explore underlying reasons for discrepancies between perceived and objective risk. The research was conducted in two phases, beginning with a quantitative assessment, followed by a qualitative exploration to contextualize and deepen the understanding of participants’ experiences. Quantitative data were used to ascertain participants’ perception and objective CVD risk and identify follow-up interview participants based on their perceived and objective CVD risk. Qualitative data were used to explore participants’ thoughts surrounding their results and underlying reasons for discrepancies between perceived and objective CVD risk.91 Figure 1 illustrates the procedure and outcomes for each phase of the mixed methods study, depicting the explanatory sequential design used in the research.
 |
Figure 1 Visual Model of Explanatory Sequential Design. This figure illustrates the procedure and outcomes for each phase of the mixed methods study, depicting the explanatory sequential design used in the research. |
Protection of Human Subjects and Ethical Considerations
Ethical approval for this study was obtained from the Institutional Review Boards (IRBs) of two universities. The first university was the data collection site, and the second was affiliated with the lead author’s Ph.D. program. The study adhered to ethical principles outlined in the Declaration of Helsinki, ensuring respect for participants, beneficence, and justice.
Design, Sample, and Setting
The participants in the convenience sample were selected based on the following inclusion and exclusion criteria: African American adults ages 18–25 enrolled at a southeastern HBCU regardless of housing status (on-campus or off-campus). Exclusion criteria were non-identification as African American and age outside of 18–25 criteria.
Participants were recruited through various channels, including university-wide emails, flyers, distribution of handouts in university 101 classes (required for all first-year students and transfer students), and advertising in prominent student gathering areas, providing access to a diverse group of students. Fifty-six participants entered the study and provided baseline data. However, complete data, including anthropometric and laboratory measurements, were obtained from 28 participants. A subgroup of participants proportionately representing categories of CVD risk perception and objective CVD risk were invited to participate in individual follow-up interviews.
Participants received a $50 gift card for completing the quantitative measures, while those who participated in interviews received a $100 gift card. Quantitative data were collected from August to December 2022, while follow-up interviews were conducted in March 2023.
Quantitative Data Collection and Measurement
A cross-sectional survey was administered to the sample to assess participants’ risk perception and objective CVH score. Data collection was conducted using REDCap (Research Electronic Data Capture), an electronic data capture tool hosted at the University of South Carolina.92,93 REDCap provides a secure platform for data capture, offering features such as audit trails, automated export procedures, and seamless data integration with external sources. Demographic information, CVD risk perception, and self-reported behavior using LE8 metrics6 were collected via an online survey constructed using questions from the PhenX Toolkit.94 Participants provided informed consent, which included the publication of anonymized responses/direct quotes.
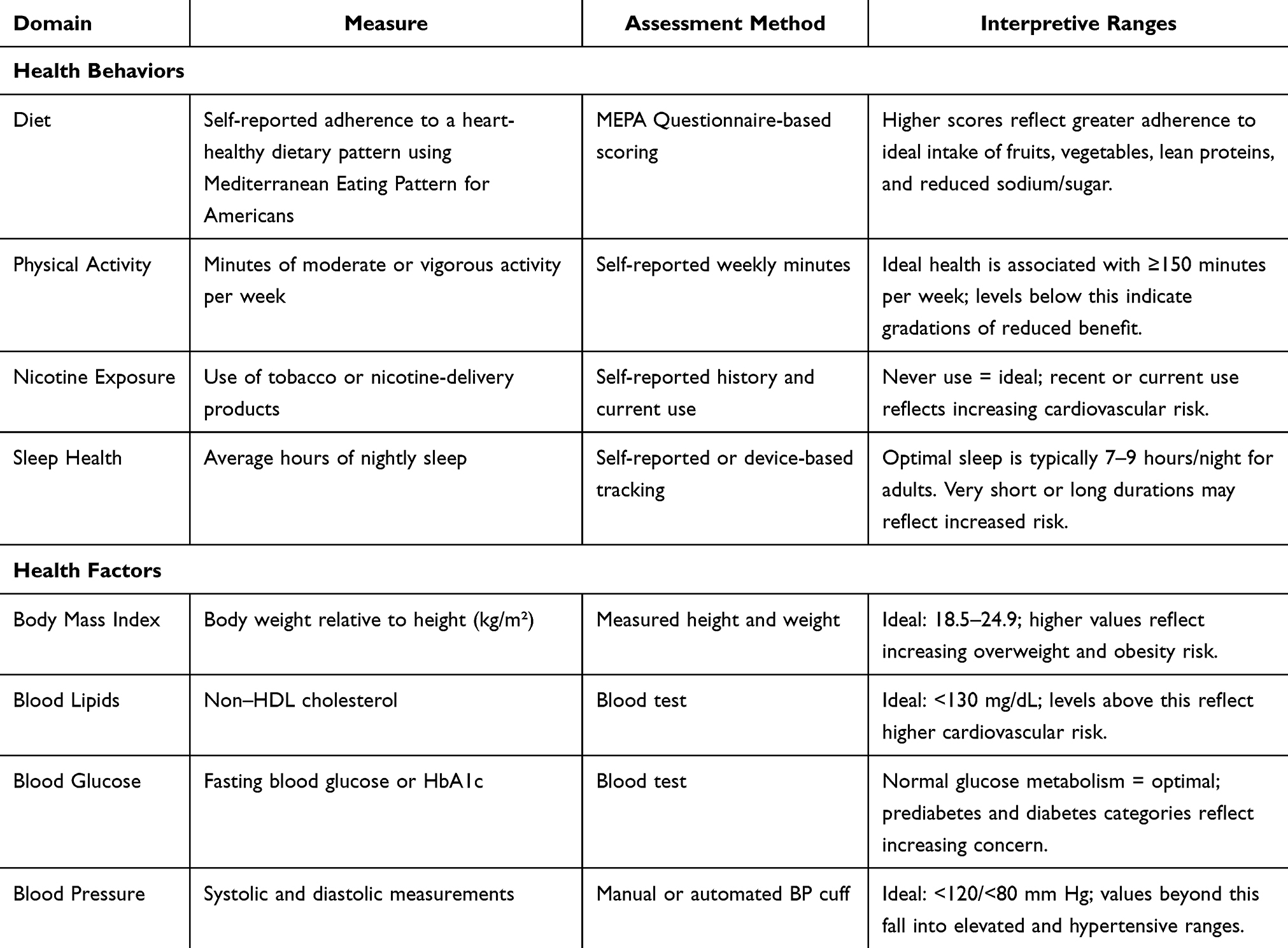 |
Table 1 Cardiovascular Health Metrics |
This study utilized Life’s Essential 8 cardiovascular health measures publicly available at the American Heart Association’s website and detailed in Lloyd-Jones et al.6 Anthropometric measurements and laboratory analyses were conducted to obtain health indicators. The principal investigator (PI) or a trained research assistant obtained blood pressure (BP), and height and weight to calculate BMI. BMI scores were categorized into ideal, overweight, obese, and severely obese categories (see Table 1). A national clinical laboratory service company collected fasting blood lipid and glucose levels. Table 1 displays the domains, CV health metrics, measurement methods, and quantification for the LE8 measures.6
Participants’ CVD risk perception was assessed using the Schwarzer and Renner95 scale (Cronbach’s α =0.78). The scale comprised three questions focusing on participants’ perceptions of the likelihood of experiencing heart disease, high blood pressure, and stroke compared to their peers. Responses were recorded on a Likert scale ranging from −3 (much below average) to +3 (much above average). To determine an overall risk rating, participants’ perceptions of heart disease, hypertension, and stroke were averaged, and participants were categorized into three risk perception groups: high-risk perception (>0 to 3 rating), average risk perception (0 rating), and low-risk perception (<0 to −3).
CVD risk was calculated using the AHA’s robust LE8 CVH scoring system.6 Self-reported data were collected for diet, PA, nicotine exposure, and sleep hours. Dietary intake was assessed using the Mediterranean Eating Pattern for Americans (MEPA),6 which uses 16 questions to evaluate participants’ food consumption by category. Responses were compared to MEPA-recommended servings, with scores assigned based on adherence. The total diet score was calculated by giving one point for each food selection that aligned with the Mediterranean Eating Pattern for Americans (MEPA) guidelines. The final diet score represented the number of healthy choices made, expressed as a percentage of the 16 total points available. Weekly PA was measured through self-reported moderate and vigorous exercise minutes per week, with scores calculated according to AHA’s PA metric. Nicotine exposure from cigarettes or inhaled nicotine delivery systems was also assessed using the LE8 rating, which distributed points based on smoking history and behaviors.
Cardiovascular health scores were calculated using an unweighted average scoring algorithm, resulting in participants categorized as having high CVH (scores of 80–100), moderate CVH (scores of 50–79), or low CVH (scores ≤ 49).6 The accuracy of perceived CVD risk for each participant was assessed by comparing their perceived CVD risk with the actual CVD risk categories. Participants were assigned to one of nine categories based on perception and objective risk: perceived low risk vs low CVD risk, perceived low risk vs moderate CVD risk, perceived low risk vs high CVD risk, perceived average risk vs low CVD risk, perceived average risk vs moderate CVD risk, perceived average risk vs high CVD risk, perceived high risk vs low CVD risk, perceived high risk vs moderate CVD risk, and perceived high risk vs high CVD risk.
Quantitative Data Analysis
Descriptive statistics were computed for all variables using SAS 9.4. For categorical variables, the univariate construction included a frequency distribution. For continuous variables, the statistics included measures of central tendency (mean and median) and measures of dispersion (standard deviation and range). Spearman and Pearson’s correlations were used to examine the relationships among MEPA diet components, between CVD risk perception and CVH, within LE8 components, and CVD risk perception components. The Chi-Square test was used to examine the association between the risk perception categories high, average, and low with CVD risk categories high, moderate, and low.
The primary objective of the quantitative analysis was to identify patterns and explore potential linear relationships between perceived and objective CVH. Given the small sample size, the study was not powered to detect statistical significance, and the findings were not intended to be generalized beyond the sample studied but rather to summarize key characteristics. Rather, the aim was to summarize key characteristics and provide foundational insights for future research with adequate power.
Connecting Quantitative and Qualitative Phases
The final phase involved integrating quantitative and qualitative findings to interpret the data comprehensively. First, the quantitative findings were used to identify participants who would be invited for qualitative interviews based on their CVD risk perception and objective CVD risk category.96 Another crucial connection point was the development of interview questions for the qualitative data collection, guided by the results obtained from the analysis of CVD risk perception accuracy.
Qualitative Data Collection and Measurement
In the qualitative phase, we purposefully selected a subgroup of 16 participants from a total of 28, ensuring that the distribution aligned with representation in the nine perceived CVD risk versus objective CVD risk categories. Additionally, the quantitative results were instrumental in constructing a semi-structured interview guide used during the interviews.
Interviews were conducted over Zoom97 by the first author or a research assistant. While the interviewers were unfamiliar with the participants, the participants may have been familiar with the interviewers from campus. Participants were instructed to keep their cameras off using a study identification number as their name before joining the Zoom session to ensure privacy and minimize the stress associated with one-on-one interviews. Zoom end-to-end encryption provided additional protection for the meetings and required all meeting participants to join from the Zoom desktop app, mobile app, or Zoom Rooms using password protection access. Once the participant joined, they were prompted for their study identification number to confirm identification and match qualitative and quantitative responses. The interview guide was read verbatim to obtain informed consent and participants had to verbally consent to participate. The also used anonymized responses/direct quotes in publications and/or scientific presentations. To assure confidentiality, participants were also apprised that to maintain the privacy of their recorded and transcribed Zoom session, records without identifying information were stored in a secure location and only accessible by the immediate research team. The participants were then informed about their CVD risk perception and actual CVD risk, and their response was solicited. [Appendix 1]. For instance, a participant who perceived their risk as low but had a high CVD risk received the following prompt:
Based on your responses to the survey, the measurements taken by the study nurse, and your lab work results, you perceived your heart disease risk to be low, but you have a low heart health score. This means you thought you had a minimal risk of developing heart disease but have a high or increased risk of developing heart disease.
Participants were then encouraged to share their thoughts about the information provided. Interviews were recorded, and field notes were logged during the interview process. Interviews were transcribed verbatim.
Qualitative Analysis
The first author and research assistant reviewed each transcript to ensure accuracy. Content analysis was performed, and an Excel table was created to document participant risk perception, CVD risk category, responses to the questions, and themes identified. Each transcript was independently coded to recognize these themes, and common responses related to the study’s objectives were recorded. Thematic analysis was completed to interpret participants’ responses. See Table 2, Thematic Analysis. To ensure inter-coder reliability, the coding process was reviewed and refined until a high level of agreement was reached.
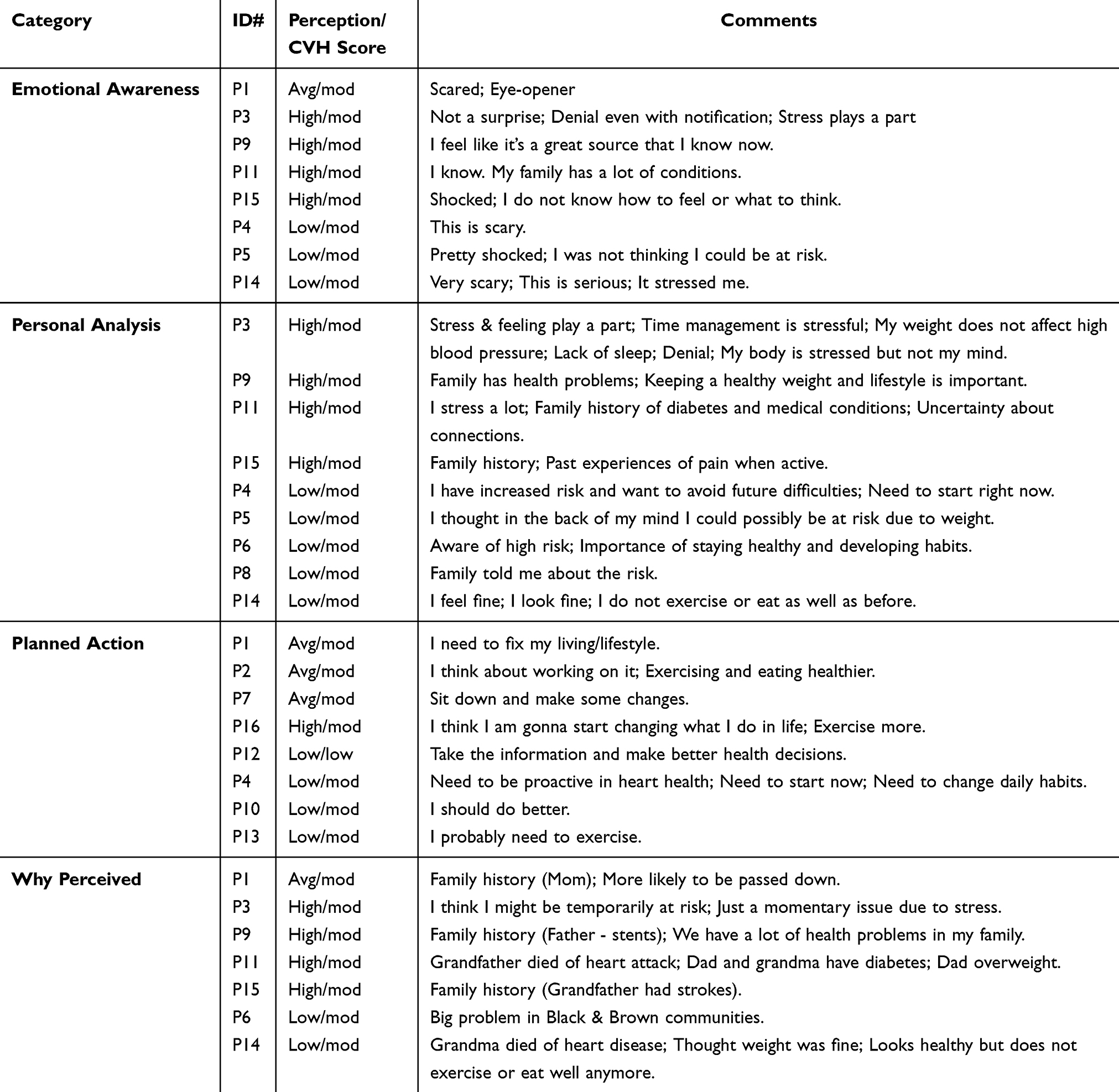 |
Table 2 Thematic Analysis Table |
The research team had extensive experience in qualitative cardiovascular and chronic conditions research. Additionally, two researchers on the team had proven trustworthiness and credibility through long-term faculty and leadership roles at the university. One was a tenured department chair with more than 30 years at the university, and the other a tenured associate professor. Both faculty members had experience collaborating with campus student groups and helping to maintain participant rapport.
Integration and Reporting of Results
The quantitative and qualitative findings were integrated using an explanatory sequential approach.91 A subset of participants that had similar percentages in categories of the perceived/objective CVD risk was selected. For example, if eight of 28 participants perceived their CVD risk as low but had high objective CVD risk, we needed 28.6% of the interviewees to fall into this category. The semi-structured interview guide was developed to reflect perception/risk categories.
Results
Among the 28 participants, 28.6% (8) were first-year college students, 21.4% (6) were sophomores, and juniors and seniors had 25% (7) each. The average age of participants was 20.29 years, with a range from 18.07 to 24.09 years. Twenty-three (82.1%) participants identified as female. Table 3 provides an overview of other demographic characteristics of the group.
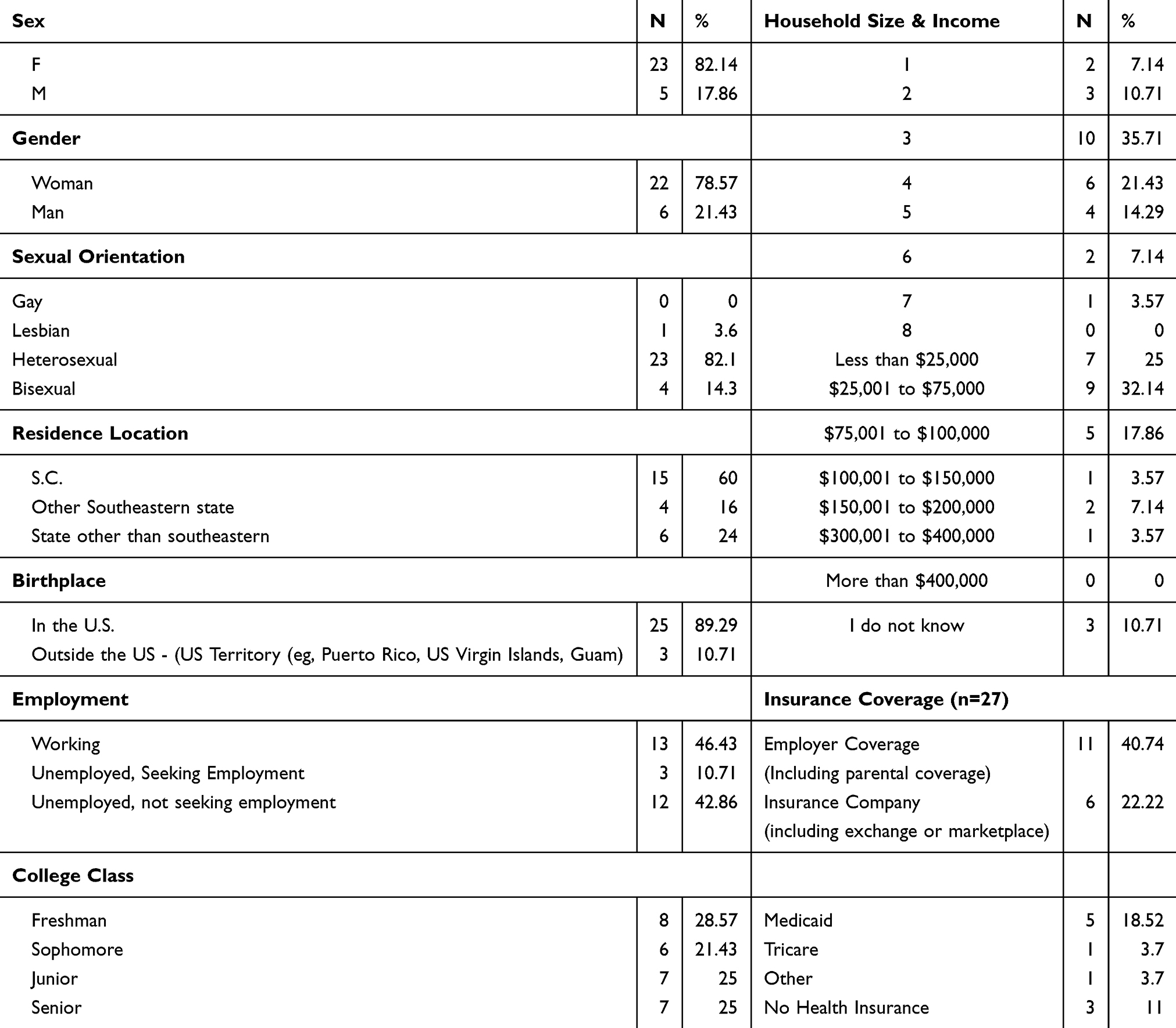 |
Table 3 Summary of Demographic Characteristics |
CVD Risk Perception
Participants had an average overall risk perception score of −0.96, indicating a perception slightly below the average risk. The overall perceived risk categories were distributed as follows: high (21.4%, 6), average (21.4%, 6), and low (57.1%, 16). Participants who rated below average (slightly, moderately, and much) were 57% (16) for heart disease, 46.4% (13) for high blood pressure, and stroke (53.6%, 15). Detailed distribution of participants based on their perceived risk is presented in Figure 2.
 |
Figure 2 CVD Risk Perception portrays a detailed distribution of participants based on their CVD perceived risk. |
CVD Risk
The participants exhibited an average CVH score of 71.96, with scores ranging from 46.88 to 88.13. The distribution of CVD risk was as follows: high (3.57%, 1), moderate (67.9%, 19), and low (28.6%, 8). Table 4 provides mean, standard deviation, and range values for each component of the LE8 Assessment.
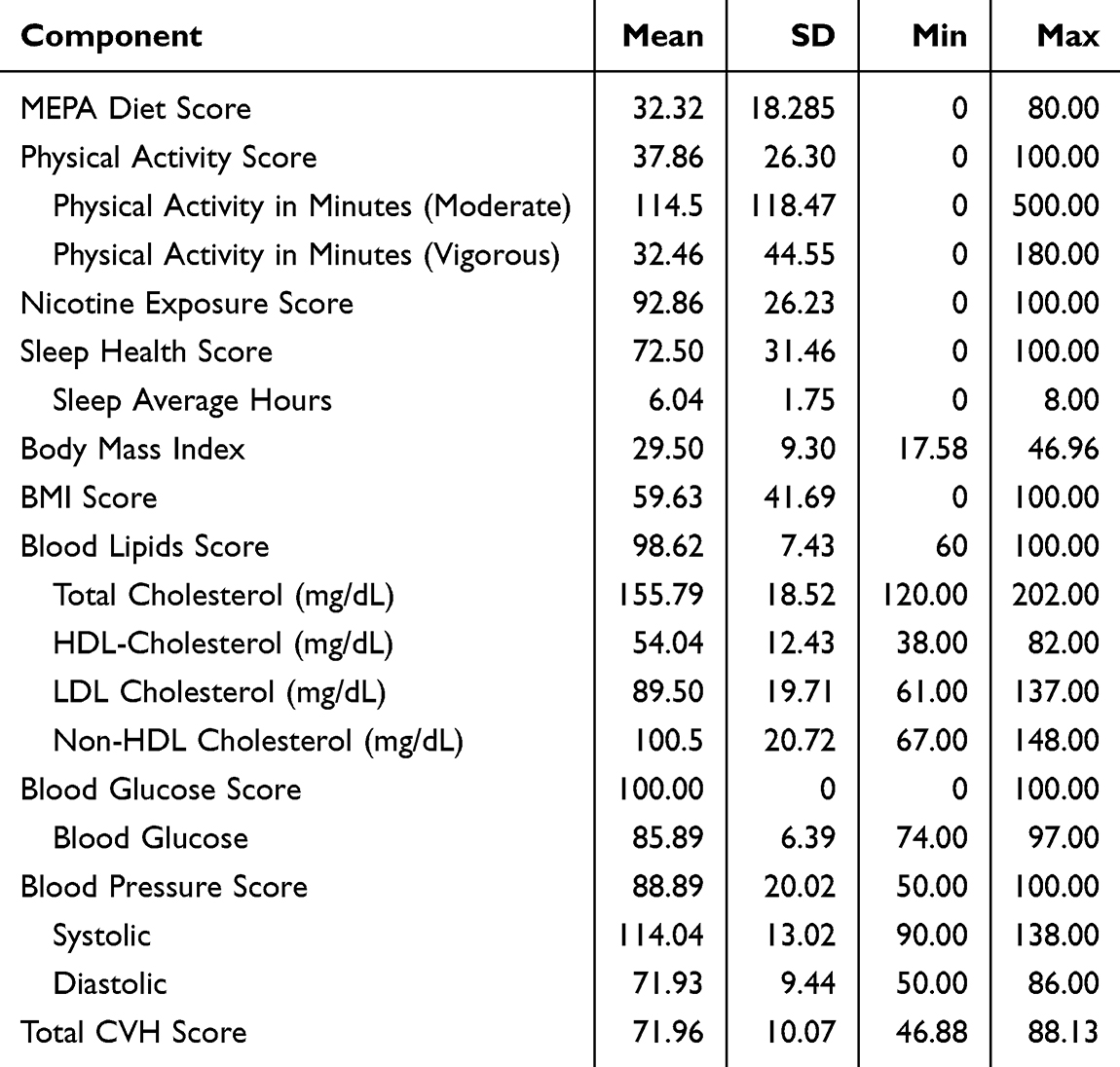 |
Table 4 Life’s Essential 8 Cvh Descriptive Statistics |
Statistical significance was determined using a threshold of 0.05. Pearson’s correlations were employed to investigate the relationships between various variables. Notably, the Pearson Correlation between continuous total scores for CVD risk perception and actual CVD risk was r = −0.09 (p = 0.51) and was not statistically significant. However, significant correlations were observed between CVH and income (0.469, p = 0.012), sleep and diet (0.46, p = −0.0135), and BMI and blood pressure (r = 0.70, p <0.0001). There were also significant correlations noted between age and diet (−0.48, p =0.01), and age and nicotine exposure (−0.62, p <0.001). Although correlations were expected between CVH and its constituent elements, only the following were statistically significant: physical activity (0.49, p = 0.014), sleep (0.529, p = 0.004), BMI (0.678, p <0.001).
Perceived Versus Actual CVD Risk
Participants sorted into seven out of nine perceived CVD risk to objective CVD risk categories: 14.3% perceived low risk vs low CVD risk, 39.3% perceived low risk vs moderate CVD risk, 3.6% perceived low risk vs high CVD risk, 10.7% perceived average risk vs low CVD risk, 10.7% perceived average risk vs moderate CVD risk, 3.6% perceived high risk vs low CVD risk, and 17.9% perceived high risk vs moderate CVD risk.
Overall, participants perceived their CVD risk as slightly below average (−0.96), yet their mean CVH score indicated a moderate risk (71.96). Among those who perceived themselves as having an average or high CVD risk (43%), none had a high CVD risk, while 21.5% had a moderate CVD risk. Among those who perceived their CVD risk as low (57%), 14.3% had a low CVD risk, 39.3% had a moderate risk, and 3.6% had a high risk. The cross-tabulation of perceived risk vs CVD risk categories is detailed in Table 5. No statistically significant correlations were observed between perceived risk, CVH, and LE8 components.
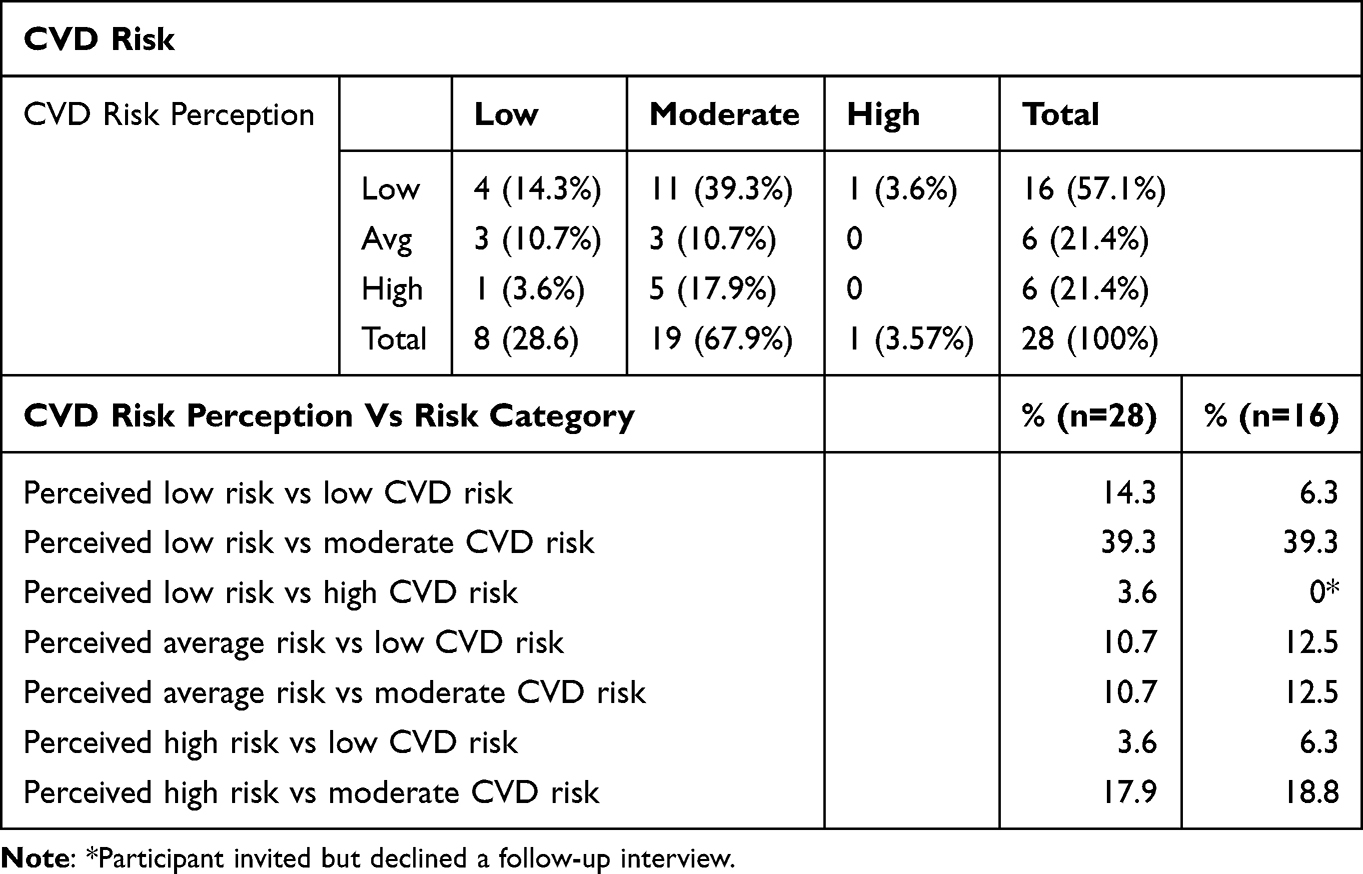 |
Table 5 Cardiovascular Risk Perception / CVD Risk and Participant Selection |
Qualitative Results
Sixteen participants took part in qualitative interviews, representing various perceived risk vs CVD risk categories. These categories included low perceived risk vs low CVD risk (n=1), low perceived risk vs moderate CVD risk (n=6), average perceived risk vs moderate CVD risk (n=2), average perceived risk vs low CVD risk (n=2), high perceived risk vs low CVD risk (n=1), and high perceived risk vs moderate CVD risk (n=3%). There was only one participant in the low perceived risk vs high CVD risk category. The individual declined an invitation to participate in the follow-up interview. To uphold ethical guidelines, all participants were invited to review their results, even if they did not participate in the interviews. Those who came were given a hard copy of their results to avoid potential breaches in electronic communication of results. Table 5 illustrates the purposeful selection of participants, comparing percentages in categories for the entire group and participants in the qualitative phase.
Qualitative analysis revealed three core themes: Emotional Awareness, Personal Analysis, and Planned Actions (See Table 2, Thematic Analysis). Those who did not perceive they were at risk also expressed reasons for their perception. Pseudonyms were used to ensure participants’ privacy.
Emotional Awareness
Emotional awareness was expressed by participants who perceived their CVD risk as low but learned that their CVD risk was high. Expressions included scared, shocked, and “crazy” or “this is an eye-opener.” Ellie expressed multiple emotions when learning she was at risk for CVD, “This is very scary. This is serious. It stressed me.” Likewise, Brenda, a participant who perceived her risk as low but had moderate risk, expressed,
I am pretty shocked because I wasn’t thinking about that I would could be at risk. I feel like, maybe in the back of my head, I thought, you know, I could possibly…possibly be at risk because of, like my weight and whatnot. But I mean, it wasn’t at the forefront.
One participant who had a high perception of CVD risk reflected,
Oh. I remember thinking I had a high risk of, for heart disease again, because there’s issues in my family and quite a bit of heart disease- quite a quite a few bit of history, and also (pause) I don’t know, I don’t know how to feel.
Twelve of the sixteen interviewees reflected an emotional awareness of a need for change. Examples include,
But you know I think it’s still possible for me. So that’s why it’s important to like, you know, stay healthy. You have to develop habits. But so that way I don’t develop heart disease.
I mean, I think it lines up with what I was thinking. I need to be very proactive in my heart health because I do have increased risk & I’m trying to avoid going through difficulties later in life. This is scary. Yes, it is.
andI feel like it’s a great source that I know now that I’m at a great risk of a heart disease. Now I need to know what I need to do to prevent it, stay or try to not towards prevent it.
Emotional awareness was a common theme among participants but appeared across different risk perception categories. All participants but two who expressed emotional awareness had an inaccurate perception of their CVD risk. For example, three participants who believe they were at high risk but had moderate risk expressed shock or surprise. Similarly, two participants who thought their risk was low but had moderate risk also reported shock or surprise. Of the two participants with an accurate perception of their risk one (low perception, low risk) expressed gratitude, while the other (average perception, moderate risk) expressed fear.
Participants in the high perception, moderate score category often expressed shock, stress, or for their results. Comments included,
Not really a surprise, I consider myself healthy., I don’t know how to feel. I hope it doesn’t hinder my goals., or I stress a lot, but I don’t know if that affects heart disease.
Those with low perception and moderate or low scores showed a mixture of relief, mild concern, or acceptance. Their responses were more often neutral, such as “I need to start now. I have increased risk.” Or “I probably need to exercise.”Personal Analysis
The comments of the sixteen participants also reflected a personal analysis of their situation, which was displayed by citing reasons, bargaining, or rationalization. One participant provided a reason for her high CVD risk as, “I probably do have a high risk, especially being an African American woman and my family history” and another stated “my mom has heart disease.” Five of the 16 participants cited “stress” as a risk factor for CVD. Emily stated, “I think it could just tie into the stress or lack of sleep. Like I have assignments from classes, and I also have a day job.” Another participant connected stress to blood pressure:
I stress really, really bad. So I know that, like, cause your like your blood pressure to go up, and all the but not, but well, it comes like a lot of increase in things that create heart disease.
An AAEA male was hopeful that CVD would wait until he was older, appearing to accept vulnerability for CVD in his elder years:
I don’t know how to feel. I don’t know what I think. I don’t. I hope it comes around when I’m older and doesn’t hinder my current goals.
Another participant sought a rationalization for her results while denying the actual risk:
I think that sometimes with high blood pressure, it’s calculating the stress and how you were feeling at that moment. And maybe that can play a part in it. My weight doesn’t have anything to do with high blood pressure. But I do consider myself like healthy.
Participants with high perception and moderate CVH provided rationalization for temporary factors. Reasons included stress, lack of sleep, or assignments, rather than inherent health risk.
Planned Actions
Planned actions expressed by participants included both vague and recognizing the need for change and specific actions. Ten participants recognized the need to change or reported that they would change. For example, Priscilla said,
Um, I’m thinking that if I don’t change what I do, everything my mom told me I should do, I need to start right now, because (pause) I do have people on my side that do have a lot of heart problems, diabetes and stuff like that. So. I really do need to change what I do my everyday life.
Penelope’s reflection demonstrated deep thought but without specific action, “I need a…(pause). I need to fix you know, my living/lifestyle”. One participant who reported a family history of heart disease stated, “I think it’s still possible for me to stay healthy. You have to develop habits. So, I don’t develop heart disease.” Only three participants articulated a plan for specific CVD risk-reduction activities. These specific actions included “eating more healthy”,“exercising more and everything”, and “need to exercise.”
Overall, participants who perceived their risk as average but had a high CVD risk expressed fear and recognized the need for change. Participants who accurately perceived their CVD risk as high acknowledged fear, shock, and the need for change. However, most participants did not express the specific actions they would take to improve their CVD risk. Finally, participants who inaccurately perceived their CVD risk as low varied in their reactions, and their responses ranged from “not a surprise” and “I know. My family has a lot of conditions” to great surprise: “I am a pretty shocked because I wasn’t thinking about that I would could be at risk.” None of the participants with low perception: high CVD risk cited a specific action they would take to improve their CVD risk.
Each of the 25% with high perceived CVD risk had a family history of CVD or CVD risk factors (ie, DM, hypertension, stents, heart attack, or obesity). One perceived high-risk participant described his family history as “grandfather had a fanny pack filled with medications and eventually died of a stroke”. Another participant linked her high-risk perception to, “I have a lot of stress, my whole family has a lot of stress. My mother has depression and things like that”. In the 43.8% who perceived their risk as low but had moderate risk, common themes emerged of “feeling fine”, “I’m young”, and “I feel pretty healthy.” One participant said,
I thought my weight was fine. The only thing I could say was that I don’t exercise as much anymore, and I don’t eat as good anymore. But I look fine. I’ve never had any issues like that.
Some high perception/moderate CVH participants acknowledged the risk but struggled with action. Comments included,
I think I need to change what I do in life., I hope it doesn’t hinder my goals. Or I just try to find a way to get everything done.
Conversely, participants in the low perception and low or moderate CVH category expressed more immediate intention to change. Comments were “I need to start right now.”, “I probably need to exercise.”, or “I should do better.”Perception Rationales
Five of 16 (31.3%) interviewees had a high perception of developing CVD, and all instances were paired with objective moderate CVH. The three interviewees (18.8%) with average risk perception each had moderate CVH. However, of the seven participants who had low risk perception, only one had low CVH (or high CVD risk). Six had moderate CVH, and none had high CVH.
Reasons for their perceptions included family history and genetic predisposition, denial or underestimation of risk, lifestyle and behaviors, awareness of social and cultural influences, and lack of information or knowledge. Five (31.3%) participants mentioned family members who had high blood pressure, strokes, or heart disease and stated that as the reason they felt at risk. Four (25%) participants exhibited a sense of denial or underestimation of their personal risk for heart disease despite acknowledging lifestyle factors. For example, “young and healthy” but downplayed the contribution of personal behaviors (ex. “I mostly eat right”). Four (25%) participants focused on their lifestyle choices and personal behaviors as a reason they perceived themselves as healthy and felt they were protected from heart disease. For example, “I feel pretty healthy, and I try to eat healthy and exercise a few times a week” was cited as a reason by a participant. Awareness of social and cultural influences was used by two (12.5%) participants, indicating a broader awareness of cultural or social factors that contributed to their perception. One participant used the example, “It’s a big problem in Black & Brown communities.” Lastly, a lack of information or knowledge was noted in two (12.5%) participants, citing “I just didn’t know where my body is.”
Discussion
This study aimed to provide a descriptive overview of comparison in the perceived and objective CVD risk among AAEAs and explore their thoughts when learning their results. We sought to understand the relationship between perceived and objective CVD risk among AAEAs, participants’ responses to learning their objective risk, and how they explained the reasons for their perceived CVD risk.
Our participants’ CVH mean score was lower than those of AAEAs in a large-scale retrospective analysis of CVH in 18–30 years olds with premature CVD and mortality.85 The study used LS7 to compute CVH and 71.2% of AAEAs (n=1739) compared to 58.5% for White emerging adults (n=1402). These findings are suggestive that our sample may be at higher risk for CVD than AAEAs in Perak et al,87 who subsequently developed CVD.
Our findings also align with previous research identifying elevated risk for various health behaviors and factors, such as diet,10 PA,13 nicotine exposure,17 and sleep health.23 Health factors were also aligned with previous studies: BMI,28,29 blood lipids,6 blood glucose,32 and BP.35,36 These findings highlight the importance of understanding and addressing racial disparities in cardiovascular health, particularly in the context of heart failure prevention, starting from a young age.
Correlation statistics suggested that individuals with higher incomes may generally have better CVH. The moderate positive correlation suggests that better sleep habits are associated with healthier dietary choices, which could influence heart health. Dietary nutrition is believed to have a significant impact on sleep wellness.98 Several nutritional strategies have been found to enhance sleep, such as consuming high-carbohydrate, high-glycemic index meals in the evening, along with melatonin, tryptophan-rich proteins, tart cherry juice, kiwifruit, and certain micronutrients.99 The moderate negative correlation between age and diet suggests that as people age, their diet may worsen or become less heart-healthy, potentially increasing their risk. Conversely, the strong negative correlation between age and nicotine shows that older individuals tend to have lower exposures, which is a positive indicator for heart health. These changes may be attributed to the transitional phase of emerging adulthood. During this stage, individuals have a broader range of potential activities compared to other age groups, as they are less bound by fixed roles and responsibilities. This flexibility contributes to the unpredictability of their demographic patterns.5 These findings suggest that lifestyle factors like physical activity, sleep, and maintaining a healthy BMI are crucial for heart health, and socioeconomic factors like income and age also play a role in cardiovascular risk.
Our study also identified a discrepancy in CVD risk perception among participants, with most perceiving their risk as lower than actual. Perceived risk plays a pivotal role in motivating behavior change, as demonstrated by previous research indicating associations between risk perception and health responsibility.100,101 Despite a slightly below average mean CVD risk perception, participants exhibited a moderate mean CVH score, emphasizing the importance of objective measures of CVH to complement self-reported perception. Most of our AAEAs overestimated or underestimated CVD risk. Consistent with existing literature, our study suggests that many individuals, including AAEAs, tend to perceive their risk as lower than the objective measures.102 Contrary to other studies, higher risk perception did not equate to higher CVH, as no individuals with high-risk perception had high CVH scores.[72,73] These AAEAs may believe themselves to be at greater CVD risk than they are. Despite the heightened awareness, the CVH scores were all moderate. Conversely, lower risk perception had a slight correlation with lower CVH, but most individuals with low-risk perception still had moderate CVH scores. These participants may have a false sense of security and could suggest a sense of complacency or lack of preventive action for CVD prevention. Identifying these disparities in perceived and objective CVD risks can inform interventions aimed at mitigating potential CVD risks and improving health outcomes. Accurate perception of CVD risk may catalyze the adoption of preventive measures.
When learning their objective CVD risk, some participants showed a willingness to modify their behaviors, aligning with a previous study103 indicating associations between post-intervention risk perception and intentions to exercise in emerging adults. These behavioral intentions highlight the potential of personalized risk feedback as a catalyst for change and set the stage for exploring the emotional and cognitive responses participants shared during follow-up interviews.
Qualitative interviews provided a deeper insight into participants’ emotional responses, personal analyses, and planned actions upon learning their CVD risk, elucidating the complex psychological processes involved. The themes of Emotional Awareness, Personal Analysis, and Planned Actions elucidate the complex psychological processes individuals undergo when confronted with their health status.
These findings offer valuable insights into cognitive and emotional aspects influencing individuals’ readiness to make lifestyle changes. First, participants showed a willingness to modify their behaviors upon becoming aware of their CVD risk, aligning with previous studies103 indicating associations between post-intervention risk perception and intentions to exercise in emerging adults. For some, however, there may be a disconnection between awareness and action, unable to identify actionable change to improve health outcomes. Second, there was a general tendency for participants’ perceptions of risk to reflect their health behaviors (eg, exercise, diet) and family history, but these perceptions are often shaped by personal and cultural factors, such as stress, denial, or a lack of information, as was acknowledged by some participants.
Next, psychological factors and risk perception must be considered. Perception of risk is subjective and influenced by personal experiences, education, and even social media exposure. Such exposure, or lack thereof, can inflate or minimize awareness. The psychological aspect of perception can distort how one evaluates health risks.
Our findings have significant implications for Education, HBCUs, clinical practice, public health, and research related to improving CVD risk awareness and prevention strategies for AAEAs. The emotional responses, personal analyses, and planned actions our participants described revealed key areas that healthcare professionals and educators can integrate to enhance CVH outcomes.
Implications for Education
While emotional response did not always result in concrete action, health messaging can be tailored to provide consistent messages about the significance of CVH. Health messages about CVH are often framed in a one-size-fits-all manner, which may not be relevant to AAEAs’ lived experiences. Effective educational efforts must use relatable examples and storytelling to illustrate risk factors and lifestyle changes. For example, ads discussing a family member’s CVD-influenced dietary or exercise choices may make the information personally relevant.
Nutrition education, as well as other educational strategies, must provide culturally tailored recommendations. For example, education should include ways of making culturally meaningful traditional foods with heart-healthy modifications, such as air-frying instead of pan-frying in oil. Education using the LE8 tool could also be an effective way of integrating the eight metrics into daily living. For example, an eight-week seminar that includes one of the elements each week could be implemented at a community center.
Lastly, given that stress was commonly cited as a perceived risk factor, educators should teach stress management strategies. Simple changes such as lifestyle adjustments (time management, sleep prioritization, etc)., mind-body techniques, or social behaviors (limiting caffeine or engaging in hobbies), with traditional risk reduction approaches (ie, diet and exercise) may improve health outcomes.
Implications for HBCUs
Historically Black colleges and universities have provided culturally enriching environments that many AAEAs seek. As AAEAs transition into emerging adulthood, they represent a key demographic for CVD awareness initiatives. HBCUs are ideally positioned to educate AAEAs about CVD risks and cultivate lifelong habits to prevent CVD. Interventions for AAEAs during this critical life stage can significantly influence future CVD outcomes, potentially reducing health disparities.
HBCUs should also integrate CVH into Greek life events. Fraternities and Sororities frequently host events such as step shows, community service events, and parties. Additionally, student organizations and clubs are key gathering locations. Integrating information on CVH as five-minute snippets can be effective with consistency.
HBCUs should incorporate CVD screening, risk assessments, and educational workshops into campus health services. Student ambassadors could be utilized in campaigns that spread heart healthy messages. Grant funding may even be obtained to provide stipends to student workers to improve engagement. Campuses should implement interventions such as digital health tools, peer-to-peer education and competitions such as healthy weight loss challenges, which can improve student engagement in building positive lifelong habits. Sustained CVD awareness coupled with behavioral changes may contribute to improved cardiovascular health outcomes, with the potential for these changes to extend to families and future generations.
Clinical Nursing Practice Implications
A personalized CVH screening assessment using LE8 will help patients understand their objective risk. Bridging the gap between awareness and action may begin with objective data and assisting patients in building an action plan.
Healthcare providers should improve healthcare communication to build trust in AAEAs. Communications should integrate a non-judgmental, empathetic approach that encourages patient engagement. Explaining CVH scores with real-life examples, visuals, or analogies can also make information more understandable.
Tailoring clinical care plans to address CVD risk factors in AAEAs necessitates individualized assessment. Employing tools like the LE8 assessment and sharing CVH scores with patients can serve as critical initial awareness-building activities. Healthcare practitioners should allocate time for one-on-one counseling sessions, leveraging motivational interviewing techniques to help AAEAs process their emotions and connect them to achievable health goals to facilitate behavioral change. Heightening patient awareness of CVD and its associated risks through personalized risk communication that explains how specific behaviors contribute to risk is an essential starting point for preventive efforts.
Other strategies include providing culturally competent care by leveraging community and faith-based organizations such as churches, sororities, fraternities, and community centers to provide health screenings, fitness programs, peer-led discussions, or workshops may be helpful. Engaging trusted community leaders in these endeavors is critical to success.
Lastly, nurses should recognize how personal beliefs, anxiety, and/or fatalistic attitudes may influence health behaviors. Nurses must help patients identify and eliminate psychological barriers to change and identify strategies or provide referrals to counseling services.
Implications for Public Health
Expanding care to locations other than colleges where AAEAs frequent can expand CVH promotion. Public health initiatives in broader populations are important to reach AAEAs who may be at even greater risk. Culturally trained public health nurses could visit cultural festivals, outdoor music vents, barbershops and beauty salons, local eateries, and even nightclubs or social justice events. Public health nurses can also launch social media campaigns on Instagram, Twitter, and TikTok that feature AAEAs sharing information about CVH and its importance in youth. Ultimately, pairing public health nursing expertise with culturally appropriate marketing can help reach AAEAs in multiple venues.
Research Implications
Our study lays the groundwork to increase CVD awareness research to improve CVH in AAEAs. Expanding the sample size to include a larger, more diverse sample could enhance the generalizability and reliability of findings. Longitudinal studies on risk perception and behavior would provide insight into how CVD risk perception evolves over time and whether behavior change is sustained. Additional studies should examine psychological and social factors that affect risk perception, including the role of social media, personal experiences, and family history. Studies should also be designed to comprehensively explore all aspects of the UPSTREAM CVD theory, including the complex interplay of upstream factors, population factors, healthcare system factors, behavioral intentions, and nursing activities. Further, conducting longitudinal studies would allow for the exploration of changes in CVD risk perception, actual CVD risk, and health behaviors over time.
Limitations
Our study had several limitations. Some participants faced barriers, such as transportation issues, which may have contributed to missing or incomplete data. Additionally, data collection ended due to an early university Thanksgiving holiday break and transition to virtual course completion to prevent COVID-19 spread.
The researchers recognized the potential for biases: social desirability, recall, interviewer, and selection. Participants were told that there were no right or wrong answers, and screens remained off throughout the interview, encouraging honest responses and reducing social desirability bias. Regarding recall bias, we did not implement specific measures to reduce potential inaccuracies of self-reported behaviors but relied on participants’ youthfulness for recollection. Interviewer bias was minimized using a semi-structured structure interview guide, and interviewers read the script verbatim. Although our sample was representative of the target population, we acknowledge the small sample size. The study is not powered for statistical significance, and the findings should not be considered generalizable. However, due to the limited research on this specific group, this study serves as a valuable preliminary exploration. The focus was to identify patterns and explore potential linear relationships between perceived and objective CVH that provide foundational insights to guide future studies with sufficient power. Findings may provide insights to inform future studies with adequate power. Despite these limitations, our study adds to the limited body of research on CVD among AAEAs.
Conclusion
Our study findings demonstrated that the AAEAs in our study are at risk for CVD. The varied range of thoughts experienced by our participants did not directly respond to CVH scores. The mismatch in perception and objective risk reinforces the need for preventative health efforts and public health messages targeting AAEAs to align perceived and objective CVD risk. Strategies to align perception with objective measures could reduce false complacency or overwrought anxiety around CVD and should include clear, personalized risk assessment, actionable messaging, regular screening and education, health communication which integrates psychological factors, and technology and digital tools.
Future research should evaluate long-term trends in risk perception and behavior. Clinical practitioners should bridge the awareness-to-action gap through individualized, culturally sensitive interventions. Educational institutions, particularly HBCUs, have an opportunity to promote lifelong heart-healthy habits through campus-based initiatives.
Protection of Human Subjects and Ethical Considerations
Approval for this study was obtained from the Institutional Review Boards (IRBs) of two universities. The first university was the data collection site (Claflin University on 03/22/2022), and the second was affiliated with the lead author’s Ph.D. program (University of South Carolina Pro00119633) on 04/11/2022.
Funding
The HBCU Title III Seed Grant and the National League for Nursing Educational Research Scholarship funded this study. Demetrius Abshire was supported by the National Institute on Minority Health and Health Disparities of the National Institutes of Health under award number K23MD013899. The content is the sole responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
Dr Gayenell Magwood reports grants from NIH, consulting fee from Lowcountry AHEC, and honorarium from University of Mississippi Medical Center, outside the submitted work. The authors declare that there are no other conflicts of interest regarding the publication of this manuscript.
References
1. “What is Cardiovascular Disease.” American Heart Association. Available from: https://www.heart.org/en/health-topics/consumer-healthcare/what-is-cardiovascular-disease.
2. “Coronary artery risk development in young adults.” National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health (NIH). Available from: https://www.cardia.dopm.uab.edu/.
3. Butler JL, Johnson CM, Hardison-Moody A, Bowen SK. Food insecurity associated with higher stress, depressive symptoms, and lower diet quality among women caregivers in North Carolina. Nutrients. 2024;16(15):2491. doi:10.3390/nu16152491
4. Smith SB, Abshire DA, Magwood GS, Herbert LL, Tavakoli AS, Jenerette C. Unlocking population-specific treatments to render equitable approaches and management in cardiovascular disease: development of a situation-specific theory for African American Emerging Adults. The Journal of Cardiovascular Nursing. 2023. doi:10.1097/jcn.0000000000000986
5. Arnett JJ. Emerging adulthood. A theory of development from the late teens through the twenties. Am Psychol. 2000;55(5):469–480. doi:10.1037/0003-066X.55.5.469
6. Lloyd-Jones DM, Allen NB, Anderson CAM, et al. Life’s essential 8: updating and enhancing the American Heart Association’s Construct of Cardiovascular health: a presidential advisory from the American Heart Association. Circulation. 2022;146(5):e18–e43. doi:10.1161/cir.0000000000001078
7. Koutoubi S, Verbovski MJ, Kestin M, Huffman FG. Essential fatty acid intake and coronary heart disease risk factors among college students of 3 ethnic groups (in eng). J Natl Med Assoc. 2011;103(2):99–108. doi:10.1016/s0027-9684(15)30258-3
8. Savoca MR, Martine TL, Morton TB, et al. Meal patterns and food choices of young African-American men: understanding eating within the context of daily life. J Am Diet Assoc. 2011;111(9):1335–1342. doi:10.1016/j.jada.2011.06.006
9. Brown SR, Hossain MB, Bronner Y. African American Male and Female Student Perceptions of Pulvers Body Images: implications for obesity, health care, and prevention. J Health Care Poor Underserved. 2014;25(3):1328–1340. doi:10.1353/hpu.2014.0140
10. Horton SEB, Timmerman GM, Brown A. Factors influencing dietary fat intake among black emerging adults. J Am College Health. 2018;66(3):155–164. doi:10.1080/07448481.2017.1390669
11. Lee AK, Corneille MA, Hall NM, Yancu CN, Myers M. The stressors of being young and Black: cardiovascular health and Black young adults. Psychol Health. 2016;31(5):578–591. doi:10.1080/08870446.2015.1127373
12. Ajibade PB. Physical activity patterns by campus housing status among African American female college students. J Black Stud. 2011;42(4):548–560. doi:10.1177/0021934710385116
13. Olofintuyi A, Roberson KB, Ilesanmi A, et al. The use of text messaging to promote physical activity in African-American College Students: a Feasibility Study. J Nat Soc Allied Health. 2018;15:30–44. doi:10.1177/0021934710385116
14. Kennedy SM, Sharapova SR, Beasley DD, Hsia J. Cigarette smoking among inmates by race/ethnicity: impact of excluding African American young adult men from national prevalence estimates. Nicotine Tob Res. 2016;18(Suppl 1):S73–8. doi:10.1093/ntr/ntv157
15. Brown Q, Milam AJ, Bowie JV, et al. The moderating role of gender in the relationship between tobacco outlet exposure and tobacco use among African American young adults. Prevent Sci. 2016;17(3):338–346. doi:10.1007/s11121-015-0622-3
16. Carroll WR, R. H, Foushee CMH Jr, Floyd T, Sinclair CF, Scarinci I. Tobacco use among rural African American young adult males. Otolaryngol-Head Neck Surg. 2011;145(2):259–263. doi:10.1177/0194599811404968
17. An RP, Zheng JK, Xiang XL. Projecting the influence of sugar-sweetened beverage warning labels and restaurant menu labeling regulations on energy intake, weight status, and health care expenditures in us adults: a microsimulation. J Acad Nutr Diet. 2022;122(2):334–344. doi:10.1016/j.jand.2021.05.006
18. Kennedy SM, Patel RP, Cheh P, Hsia J, Rolle IV. Tobacco and marijuana initiation among African American and White Young Adults. Nicotine Tobacco Res. 2016;18:S57–S64. doi:10.1093/ntr/ntv194
19. Montgomery L, Ramo D. What did you expect?: the interaction between cigarette and blunt vs. non-blunt marijuana use among African American young adults. J Subst Use. 2017;22(6):612–616. doi:10.1080/14659891.2017.1283452
20. Petrilla C, Cheney MK. The association between chronic disease and smoking beliefs and behaviors in African American young adult smokers. Ethn Dis. 2014;24(4):488–494.
21. Broun A, Phan L, Duarte DA, et al. Physical and sociocultural community-level influences on cigar smoking among black young adults: an in-depth interview investigation. Int J Environ Res Public Health. 2022;19:4430. doi:10.3390/ijerph19084430
22. Kennedy SM, Caraballo RS, Rolle IV, Rock VJ. Not just cigarettes: a more comprehensive look at marijuana and tobacco use Among African American and White Youth and Young Adults. Nicotine Tobacco Res. 2016;18:S65–S72. doi:10.1093/ntr/ntv202
23. Ajith A, Broun A, Duarte D, et al.. “communication on cigar smoking between smokers and healthcare providers: an interview investigation among black young adults,”. Ann Behav Med. 2021;55:S110–S110.
24. Brownlow JA, Brown TS, Mellman TA. Relationships of posttraumatic stress symptoms and sleep measures to cognitive performance in young-adult African Americans. J Trauma Stress. 2014;27(2):217–223. doi:10.1002/jts.21906
25. Huntley ED, Hall Brown TS, Kobayashi I, Mellman TA. Validation of the Fear of Sleep Inventory (FOSI) in an urban young adult African American sample. J Trauma Stress. 2014;27(1):103–107. doi:10.1002/jts.21882
26. McLaurin-Jones TL, Anderson AS, Marshall VJ, Lashley M-B, Carter-Nolan PL. Superwomen and sleep: an Assessment of Black College Women Across the African Diaspora. Int J Behav Med. 2021;28(1):130–139. doi:10.1007/s12529-020-09930-4
27. Price AA, Whitt-Glover MC, Kraus CL, McKenzie MJ. Body composition, fitness status, and health behaviors upon entering college: an examination of female college students from diverse populations. Clin Med Insights Women's Health. 2016;9(Suppl 1):23–29. doi:10.4137/cmwh.S34697
28. Price AA, McCauley G, Duren-Winfield V. Physical activity guideline attainment and gender influence chronic disease risks among African American College Students. Med Sci Sports Exerc. 2018;50(5):70.
29. Galeshi R, Sharman J, Cai JH. Influence of ethnicity, gender, and immigration status on millennials’ behavior related to seeking health information: results from a national survey. Equal Divers Incl. 2018;37(6):621–631. doi:10.1108/edi-05-2017-0102
30. Nguyen QM, Xu J-H, Chen W, et al. Correlates of age onset of type 2 diabetes among relatively young black and white adults in a community: the Bogalusa Heart Study. Diabetes Care. 2012;35(6):1341–1346. doi:10.2337/dc11-1818
31. Bancks MP, Kershaw K, Carson AP, Gordonlarsen P, Schreiner J, Carnethon MR. “factors contributing to disparities in incidence for Diabetes Mellitus (DM) between African Americans (AA) and whites: the Coronary Artery Risk Development in Young Adults (CARDIA) study,”. Diabetes. 2017;66:A415–A416.
32. Bancks MP, Carson AP, Lewis CE, et al. Fasting glucose variability in young adulthood and incident diabetes, cardiovascular disease and all-cause mortality. Diabetologia. 2019;62(8):1366–1374. doi:10.1007/s00125-019-4901-6
33. Bancks MP, Kershaw K, Carson AP, Gordon-Larsen P, Schreiner J, Carnethon MR. Association of modifiable risk factors in young adulthood with racial disparity in incident type 2 diabetes during middle adulthood. JAMA. 2017;318(24):2457–2465. doi:10.1001/jama.2017.19546
34. Montague FE. “Conducting an Assessment for Hypertension in African American College Students,Doctor of Nursing Practice Doctoral Dissertation”. Walden University, Walden University Scholar Works, 2017. Available from: https://login.pallas2.tcl.sc.edu/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=ccm&AN=123313969&site=ehost-live.
35. Aycock DM, Clark PC, Anderson AM, Sharma D. Health perceptions, stroke risk, and readiness for behavior change: gender differences in young adult African Americans. J Racial Ethn Health Disparities. 2019;6(4):821–829. doi:10.1007/s40615-019-00581-0
36. Thomas SJ, Booth JN, Dai C, et al. “cumulative incidence of hypertension by 55 years of age in blacks and whites: the CARDIA study,”. J Am Heart Assoc. 2018;7(14). doi:10.1161/jaha.117.007988
37. Huan Y, DeLoach S, Keith SW, Pequignot EC, Falkner B. High blood pressure and obesity increase the risk of abnormal glucose tolerance in young adult African Americans. J Clin Hypertens. 2011;13(6):397–403. doi:10.1111/j.1751-7176.2010.00421.x
38. Colen CG, Li Q, Reczek C, Williams DR. The intergenerational transmission of discrimination: children’s experiences of unfair treatment and their mothers’ health at midlife. J Health Soc Behav. 2019;60(4):474–492. doi:10.1177/0022146519887347
39. Diggins A, Woods-Giscombe C, Waters S. The association of perceived stress, contextualized stress, and emotional eating with body mass index in college-aged Black women. Eat Behav. 2015;19:188–192. doi:10.1016/j.eatbeh.2015.09.006
40. Arnold TJ, Schweitzer A, Hoffman HJ, et al. Neck and waist circumference biomarkers of cardiovascular risk in a cohort of predominantly African-American college students: a preliminary study,”. J Acad Nutr Diet. 2014;114(1):107–116. doi:10.1016/j.jand.2013.07.005
41. Bauermeister JA, Meanley S, Hickok A, Pingel E, Vanhemert W, Loveluck J. Sexuality-related work discrimination and its association with the health of sexual minority emerging and young adult men in the Detroit Metro Area. Sex Res Soc Policy. 201411(1):1–10. doi:10.1007/s13178-013-0139-0
42. Clark VR, Perkins P, Carson BL, Boyd K, Jefferson TM. Fasting serum glucose and cholesterol as predictors of cardiovascular reactivity to acute stress in a sample of African American college students. Ethn Dis. 2015;25(2):175–179.
43. Breton CV, Wang X, Mack WJ, et al. Carotid artery intima-media thickness in college students: race/ethnicity matters,”. Atherosclerosis. 2011;217(2):441–446. doi:10.1016/j.atherosclerosis.2011.05.022
44. Gafane-Matemane LF, Kruger R, Smith W, et al. Characterization of the renin-angiotensin-aldosterone system in young healthy black adults: the African prospective study on the early detection and identification of hypertension and cardiovascular disease (African-PREDICT study. Hypertension. 2021;78(2):400–410. doi:10.1161/hypertensionaha.120.16879
45. Strauss M, Smith W, Kruger R, van der Westhuizen B, Schutte AE. Large artery stiffness is associated with salt intake in young healthy black but not white adults: the African-PREDICT study. Eur J Nutr. 2018;57(7):2649–2656. doi:10.1007/s00394-018-1791-1
46. “How to explain structural, institutional, and systemic racism.” University of Southern California Suzanne Dworak-Peck School of Social Work. Available from: https://msw.usc.edu/mswusc-blog/how-to-explain-structural-institutional-and-systemic-racism/.
47. Jones CP. Levels of racism: a theoretic framework and a gardener’s tale,”. Am J Public Health. 2000;90(8):1212–1215. doi:10.2105/ajph.90.8.1212
48. Homandberg LK, Fuller-Rowell TE. Experiences of discrimination and urinary catecholamine concentrations: longitudinal associations in a college student sample. Ann Behav Med. 2020;54(11):843–852. doi:10.1093/abm/kaaa033
49. Derricks V, Earl A, Carmichael AG, Jayaratne TE. Psychological pathways through which social norms and social identity influence eating behavior: testing a conceptual model. Int J Behav Med. 2023;30(1):7–18. doi:10.1007/s12529-022-10064-y
50. McClain S, Beasley ST, Jones B, Awosogba O, Jackson S, Cokley K. An examination of the impact of racial and ethnic identity, impostor feelings, and minority status stress on the mental health of black college students. J Multicultural Couns Dev. 2016;44(2):101–117. doi:10.1002/jmcd.12040
51. White-Johnson R. Prosocial involvement among African American young adults: considering racial discrimination and racial identity. J Black Psychol. 2012;38(3):313–341. doi:10.1177/0095798411420429
52. Murray TA. Factors that promote and impede the academic success of African American Students in prelicensure nursing education: an integrative review. J Nurs Educ. 2015;54(9):S74–81. doi:10.3928/01484834-20150814-14
53. Durkee MI, Williams JL. Accusations of acting white: links to black students’ racial identity and mental health. J Black Psychol. 2015;41(1):26–48. doi:10.1177/0095798413505323
54. Szymanski DM, Lewis JA. Gendered racism, coping, identity centrality, and African American College Women’s Psychological Distress. Psychol Women Quart. 2016;40(2):229–243. doi:10.1177/0361684315616113
55. Bell KA, Kobayashi I, Akeeb A, Lavela J, Mellman TA. Emotional response to perceived racism and nocturnal heart rate variability in young adult African Americans. J Psychosom Res. 2019;121:88–92. doi:10.1016/j.jpsychores.2019.03.180
56. Armstead CA, Hebert JR, Griffin EK, Prince GM. A question of color: the influence of skin color and stress on resting blood pressure and body mass among African American Women. J Black Psychol. 2014;40(5):424–450. doi:10.1177/0095798413494404
57. Kosma M, Buchanan DR. Aspects of depression among socioeconomically disadvantaged African American Young Adults. Int Q Community Health Educ. 2019;39(4):199–207. doi:10.1177/0272684X19829612
58. Chae DH, Wang Y, Martz CD, et al. Racial discrimination and telomere shortening among African Americans: the Coronary Artery Risk Development In Young Adults (CARDIA) study. Health Psychol. 2020;39(3):209–219. doi:10.1037/hea0000832
59. Carnevali L, Ottaviani C, Williams DP, Kapuku G, Thayer JF, Hill LK. Hemodynamic profile and compensation deficit in African and European Americans during physical and mental stress. Biol Psychol. 2019;141:17–24. doi:10.1016/j.biopsycho.2018.12.003
60. Javed Z, Haisum Maqsood M, Yahya T, et al. Race, racism, and cardiovascular health: applying a social determinants of health framework to racial/ethnic disparities in cardiovascular disease. Circ Cardiovasc Qual Outcomes. 2022;15(1):e007917. doi:10.1161/circoutcomes.121.007917
61. Zhan M, Xiang X. Education loans and asset building among black and Hispanic young adults. Child Youth Services Rev. 2018;91:121–127. doi:10.1016/j.childyouth.2018.06.006
62. Wright R, Roberson K, Onsomu EO, et al. Examining the relationship between mindfulness, perceived stress, and blood pressure in African-American College Students. J Best Pract Health Prof Divers. 2018;11(1):13–30. doi:10.1177/2055217317726798
63. Havranek EP, Mujahid MS, Barr DA, et al. Social determinants of risk and outcomes for cardiovascular disease: a scientific statement from the American Heart Association,”. Circulation. 2015;132(9):873–898. doi:10.1161/cir.0000000000000228
64. Kelli HM, Mehta A, Tahhan AS, et al. Low educational attainment is a predictor of adverse outcomes in patients with coronary artery disease. J Am Heart Assoc. 2019;8(17):e013165. doi:10.1161/jaha.119.013165
65. Johnson AE, Herbert BM, Stokes N, Brooks MM, Needham BL, Magnani JW. Educational attainment, race, and ethnicity as predictors for ideal cardiovascular health: from the national health and nutrition examination survey. J Am Heart Assoc. 2022;11(2):e023438. doi:10.1161/jaha.121.023438
66. “College enrollment disparities: understanding the role of academic preparation” Center on Children and Families at Brookings, Washington, DC, 2023. Available from: https://www.brookings.edu/articles/college-enrollment-disparities/.
67. Barghi A, Torres H, Kressin NR, McCormick D. Coverage and access for Americans with Cardiovascular Disease or Risk factors after the ACA: a quasi-experimental study. JGIM. 2019;34(9):1797–1805. doi:10.1007/s11606-019-05108-1
68. Hill L, Artiga S, Damico A. “health coverage by race and ethnicity- 2022.”, 2010. Kaiser Family Foundation. Available from: https://www.kff.org/racial-equity-and-health-policy/issue-brief/health-coverage-by-race-and-ethnicity/.
69. (2022). Health Insurance Coverage and Access to Care Among Black Americans: Recent Trends and Key Challenges. Available from: https://aspe.hhs.gov/sites/default/files/documents/08307d793263d5069fdd6504385e22f8/black-americans-coverages-access-ib.pdf.
70. Blackmon SM, Coyle LD, Davenport S, Owens AC, Sparrow C. Linking racial-ethnic socialization to culture and race-specific Coping Among African American College Students. J Black Psychol. 2016;42(6):549–576. doi:10.1177/0095798415617865
71. Churchwell K, Elkind MSV, Benjamin RM, et al. Call to action: structural racism as a fundamental driver of health disparities: a presidential advisory from the American Heart Association,”. Circulation. 2020;142(24):e454–e468. doi:10.1161/cir.0000000000000936
72. Robinson R, Roberson KB, Onsomu EO, et al. Perceived risk of cardiovascular disease and health behaviors in black college students. J Best Pract Health Prof Divers. 2019;12(1):24–45. doi:10.1177/1557988315590836
73. Robinson N, Miller A, Wilbur J, Fogg L. “subjective versus objective estimated cardiovascular disease risk and adherence to physical activity in African American Women.PCNA 21st Annual Symposium Anaheim, California,”. J Cardiovasc Nurs. 2018;32(5):424.
74. Hughes Halbert C, Barg FK, Weathers B, et al. Differences in cultural beliefs and values among African American and European American men with prostate cancer. Cancer Control. 2007;14(3):277–284. doi:10.1177/107327480701400311
75. Elion AA, Wang KT, Slaney RB, French BH. Perfectionism in African American students: relationship to racial identity, GPA, self-esteem, and depression. Cult Divers Ethn Minor Psychol. 2012;18(2):118–127. doi:10.1037/a0026491
76. Kim E, Brown EA, Kwan A, Craig A, Joseph NT, Peterson LM.Sleep, pray, and status: religiosity as A moderator in the association between subjective social status and sleep in African American Young Adults. Psychosom Med. 2021;83(7):A48–A48.
77. Greene M, Holston D, Freightman J, Briley C. African American perceptions of service provided by supplemental nutrition assistance program-education: a qualitative exploration. J Nutr Educ Behav. 2023;55(2):125–134. doi:10.1016/j.jneb.2022.10.004
78. Ardakani A, Monroe-Lord L, Wakefield D, Castor C. Enhancing dietary adherence among African-American adolescents: the role of parenting styles and food-related practices. Front Nutr. 2024;11:1254338. doi:10.3389/fnut.2024.1254338
79. Kannan S, Webster D, Sparks A, et al. Using a cultural framework to assess the nutrition influences in relation to birth outcomes among African American women of childbearing age: application of the PEN-3 theoretical model. Health Promot Pract. 2009;10(3):349–358. doi:10.1177/1524839907301406
80. “Reduce household food insecurity and hunger.” office of disease prevention and health promotion, office of the assistant secretary for health, office of the secretary, U.S. Department of Health and Human Services. Available from: https://health.gov/healthypeople/objectives-and-data/browse-objectives/nutrition-and-healthy-eating/reduce-household-food-insecurity-and-hunger-nws-01.
81. Salami TK, Walker RL. Socioeconomic status and symptoms of depression and anxiety in African American College Students: the mediating role of hopelessness. J Black Psychol. 2014;40(3):275–290. doi:10.1177/0095798413486158
82. Banerjee M, Rowley SJ, Johnson DJ. Community violence and racial socialization: their influence on the psychosocial well-being of African American College Students. J Black Psychol. 2015;41(4):358–383. doi:10.1177/0095798414539174
83. Lee DB, Eisman AB, Stoddard SA, et al. Racial discrimination and cortisol in African American emerging adults: the role of neighborhood racial composition. Cult Divers Ethn Minor Psychol. 2018;24(4):521–529. doi:10.1037/cdp0000217
84. Adams AS, Madden JM, Zhang F, et al. Changes in use of lipid-lowering medications among black and white dual enrollees with diabetes transitioning from Medicaid to Medicare Part D drug coverage. Med Care. 2014;52(8):695–703. doi:10.1097/MLR.0000000000000159
85. Perak AM, Ning H, Khan SS, et al. Associations of late adolescent or young adult cardiovascular health with premature cardiovascular disease and mortality. J Am Coll Cardiol. 2020;76(23):2695–2707. doi:10.1016/j.jacc.2020.10.002
86. Aycock DM, Clark PC, Hayat MJ. Reducing Stroke Risk Among Young Adult African Americans: a Feasibility Study. Res Nurs Health. 2017;40(2):153–164. doi:10.1002/nur.21776
87. Perak AM, Khan SS, Colangelo LA, et al. Age-related development of cardiac remodeling and dysfunction in young black and white adults: the coronary artery risk development in young adults study. J Am Soc Echocardiogr. 2021;34(4):388–400. doi:10.1016/j.echo.2020.11.002
88. Park SW, Wong M, Kiefe CI, Gordon-Larsen P, Kershaw KN. Associations of neighborhood food and physical activity environments in young adulthood with cardiovascular health in midlife: the CARDIA study. J Am Heart Assoc. 2024;13(22):e036035. doi:10.1161/jaha.124.036035
89. Ferrer R, Klein WM. Risk perceptions and health behavior. Curr Opin Psychol. 2015;5:85–89. doi:10.1016/j.copsyc.2015.03.012
90. Creswell JW, Plano Clark VL. Designing and Conducting Mixed Methods Research.
91. Ivankova NV, Creswell JW, Stick SL. Using MIXED-METHODS SEQUENTIAL EXPLANATORY DESIGN: FROM THEORY TO PRACTice. Field Methods. 2006;18(1):3–20. doi:10.1177/1525822x05282260
92. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners,”. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
93. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
94. “The PhenX Toolkit: get the most from your measures.” American Journal of Epidemiology. Available from: https://www.phenxtoolkit.org/about.
95. Schwarzer R, Renner B. Social-cognitive predictors of health behavior: action self-efficacy and coping self-efficacy. Health Psychol. 2000;19(5):487–495. doi:10.1037/0278-6133.19.5.487
96. National Institutes of Health. Best Practices for Mixed Methods Research in the Health Sciences; 2011.
97. Zoom video communications, Inc. (2023). Available from: https://zoom.us/.
98. Zhao M, Tuo H, Wang S, Zhao L. The effects of dietary nutrition on sleep and sleep disorders. Mediators Inflamm. 2020;2020:3142874. doi:10.1155/2020/3142874
99. Doherty R, Madigan S, Warrington G, Ellis J. Sleep and nutrition interactions: implications for athletes,”. Nutrients. 2019;11(4). doi:10.3390/nu11040822
100. Rosenstock IM. Historical origins of the health belief model. Health Educ Monogr. 1974;2(4):328–335. doi:10.1177/109019817400200403
101. Ren H, Guo Y-F, Zhang Z-X, et al. Perception of recurrent risk versus objective measured risk of ischemic stroke in first-ever stroke patients from a rural area in China: a cross-sectional study. Patient Educ Couns. 2023;107:107586. doi:10.1016/j.pec.2022.107586
102. Clawson AH, Robinson LA, Berlin KS. Race, sex, and physician communication about tobacco as predictors of adolescent smoking trajectories in a primarily African American sample. J Ethn Subst Abuse. 2020;19(2):271–288. doi:10.1080/15332640.2018.1520173
103. Imes CC, Dougherty CM, Lewis FM, Austin MA. Outcomes of a pilot intervention study for young adults at risk for cardiovascular disease based on their family history. The Journal of Cardiovascular Nursing. 2016;31(5):433–440. doi:10.1097/JCN.0000000000000261
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cholesterol and Hypertension Treatment Improve Coronary Risk Prediction but Not Time-Dependent Covariates or Competing Risks
Subirana I, Camps-Vilaró A, Elosua R, Marrugat J, Tizón-Marcos H, Palomo I, Dégano IR
Clinical Epidemiology 2022, 14:1145-1154
Published Date: 11 October 2022
Development and Validation of Questionnaires to Assess Workplace Violence Risk Factors (QAWRF): A Tripartite Perspective of Worksite-Specific Determinants in Healthcare Settings
Mohd Hatta FH, Samsudin EZ, Aimran N, Ismail Z
Risk Management and Healthcare Policy 2023, 16:1229-1240
Published Date: 5 July 2023
Study on Risk Factors and Treatment Strategies for Deep Vein Thrombosis in Patients with Multiple Myeloma
Guo Y, Yan L, Yang X, Fan C, Reaila J, Jia Y, Hao X, Ju F, Shi Z
Cancer Management and Research 2025, 17:1667-1677
Published Date: 15 August 2025