Back to Journals » Risk Management and Healthcare Policy » Volume 16
Development and Validation of Questionnaires to Assess Workplace Violence Risk Factors (QAWRF): A Tripartite Perspective of Worksite-Specific Determinants in Healthcare Settings
Authors Mohd Hatta FH ![]() , Samsudin EZ
, Samsudin EZ ![]() , Aimran N, Ismail Z
, Aimran N, Ismail Z
Received 6 March 2023
Accepted for publication 2 June 2023
Published 5 July 2023 Volume 2023:16 Pages 1229—1240
DOI https://doi.org/10.2147/RMHP.S411335
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mecit Can Emre Simsekler
Faizul Haris Mohd Hatta,1 Ely Zarina Samsudin,1 Nazim Aimran,2 Zaliha Ismail1
1Department of Public Health Medicine, Faculty of Medicine, Universiti Teknologi MARA, Selangor, Malaysia; 2College of Computing, Informatics, and Media, Universiti Teknologi MARA, Shah Alam, Selangor, Malaysia
Correspondence: Ely Zarina Samsudin, Email [email protected]
Introduction: Workplace violence (WPV) incidences are prevalent in healthcare, and existing WPV interventions have only moderate evidence for effectiveness. This study aimed to develop and validate an instrument to assess worksite-specific WPV risk factors in healthcare settings based on a tripartite perspective of key stakeholders to facilitate improved interventions.
Methods: Three questionnaires were developed to get the responses from healthcare administrators, workers, and clients, representing the three components of Questionnaires to Assess Workplace Violence Risk Factors (QAWRF). The domains of the questionnaires were developed based on The Chappell and Di Martino’s Interactive Model of Workplace Violence, and the items were generated from 28 studies identified from a systematic review of the literature. Six experts, 36 raters, and 90 respondents were recruited to assess the content validity, face validity, and usability and reliability of the QAWRF respectively. Item and Scale Level Content Validity Index, Item and Scale Level Face Validity Index, and Cronbach’s alpha values were determined for QAWRF-administrator, QAWRF-worker, and QAWRF-client.
Results: The psychometric indices for QAWRF are satisfactory.
Conclusion: QAWRF holds good content validity, face validity, and reliability, and findings from QAWRF can contribute towards worksite-specific interventions that are expected to be resource efficient and more effective than general WPV interventions.
Keywords: workplace violence, healthcare, questionnaire, instrument, tool, risk assessment, risk factors
Introduction
The National Institute for Occupational Safety and Health (NIOSH) defines workplace violence (WPV) as the act or threat of violence, ranging from verbal abuse to physical assaults directed toward persons at work or on duty.1 Among occupations, healthcare workers (HCW) face a significant risk of WPV, having the closest contact with patients and their relatives and being on the healthcare system frontlines.2 Indeed, the rate of WPV among this group of workers is reported to be 20% overall higher than all other workers.3 According to the Injury Prevention Research Center, University of Iowa, there are four types of WPV: 1) Type 1 is WPV with criminal intent; 2) Type 2 is client-to-worker WPV; 3) Type 3 is worker-to-worker WPV; and 4) Type 4 is WPV related to personal relationships.4 Type 2 WPV is the commonest type of WPV experienced by HCW and is perpetrated mainly by patients or their dissatisfied family members.5–7
A meta-analysis of 253 studies published globally revealed that HCW’ reported exposure to any WPV was 61.9%.8 For Type 2 WPV experienced by HCW, a recent meta-analysis found that the pooled one-year prevalence was 19.3%,9 whereas a systematic review reported prevalence ranging from 9.5% to 74.6%.10 Indeed, the International Labour Organisation (ILO) reported that about every second HCW worldwide has been affected by WPV at least once during their work lives,11 whereas the United States Bureau of Labor Statistics indicated that there were 8590 cases of nonfatal intentional injuries by another person among HCW in 2020.12 Despite the above, these figures might be less than actual figures, as multiple studies have shown that WPV is usually underreported.13–15 Among the common reasons given for not reporting WPV were the perceived uselessness of reporting, perceived insignificance of the violence perpetrated, fear of consequences, and the impression that WPV is “part of the job”.15–17 Some HCW also complained that the formal reporting system is problematic due to it being difficult and time-consuming to use.17
The high prevalence of WPV among HCW are concerning as WPV can affect workers’ physical, mental, and social health. In addition, WPV incidences can also affect the quality of care and relationship with patients, work functioning, and financial and social aspects of workers.6,18–22 Among the most commonly reported consequences of HCW exposure to WPV are psychological effects such as anxiety, fear, posttraumatic stress disorder, and depression, as well as effects on work functioning such as prolonged work absences, poor job performances, job dissatisfaction, and burnout.18
Given the significance of WPV among HCW, multiple interventions for WPV have been developed globally. However, there was only moderate evidence of the interventions’ effectiveness.23 This may be because though the risk factors for WPV are well known, they are generalized to all workplace settings. Therefore, a worksite-specific assessment of risk factors needs to be conducted to provide the essential inputs for intervention.23 Moreover, current suggestions to tackle WPV include engaging stakeholders at the regional or local level and considering their collective perspectives to facilitate better policymaking, as the risk factors of WPV can be unique from one setting to another.24 This is even more pertinent given that the prevalence of WPV among HCW varies depending on the level of awareness and cultural norms in particular countries or organisations.25 However, existing survey questionnaires mainly explore workers’ perspectives and rarely consider clients’ or administrators’ perspectives on the WPV incident.
In addition, workplaces currently collect information to identify possible WPV risk factors through records analysis, job hazard analysis, and specified WPV program checklist.3 Although these conventional WPV risk factors identification methods are useful, they require training and may be time-consuming.26 On the other hand, most employee or client survey questionnaires use open-ended questions to explore employees’ or clients’ perspectives or feedback, but this may be limited by inadequate responses due to respondents’ difficulty in articulating the answers, partial responses according to varying dissatisfaction levels, and disinterest in the topic.27 They would also require more time for data collection and subsequent analysis.14 At present, there is no validated questionnaire for policymakers to conveniently collect quantitative data and subsequently determine the level of WPV risk factors existing in their healthcare settings based on the perceptions of all their important stakeholders, to enable them to tailor WPV preventive measures based on the risk factors rated as prevalent at the setting. Due to these reasons, our study aimed to develop, validate, and determine the reliability for a set of structured survey questionnaires to assess WPV risk factors in healthcare settings based on the tripartite perspectives of key stakeholders in healthcare, which are the administrators, workers, and clients.
Materials and Methods
Prior to the conduct of this study, ethical clearance was obtained from the Medical Research & Ethics Committee [NMMR-21-537-58890 (IIR)] and Universiti Teknologi MARA Research Ethics Committee [REC/07/2021 (MR/629)].
Development of the Questionnaires to Assess Workplace Violence Risk Factors (QAWRF)
Three questionnaires were developed for each group of stakeholders, namely the administrators, workers, and clients, in view that each group’s perception of WPV risk factors is different. Administrators are those involved in administrative work at each healthcare department, such as the head of department, the head medical officer, the head of paramedics, and the head nurse. On the other hand, workers are those involved clinically with clients, such as doctors, paramedics, and nurses, whereas clients are patients and those accompanying patient to a healthcare setting.
All questionnaires were developed based on the Chappell and Di Martino’s Interactive Model of Workplace Violence,19 a WPV model accepted by the ILO. In this model, the risk factors for WPV are categorized into the victim’s risk factors, the perpetrator’s risk factors, the workplace risk factors, and the wider contextual and societal risk factors that indirectly affect WPV incidences. These factors were used to form the domains of the questionnaires.
In the Chappell and Di Martino’s WPV model, the risk factors listed under each domain in the model are described in general, and they need to be adjusted according to the setting the users wish to apply the model.28 Therefore, as this study was contextualized to healthcare settings, the risk factors that were used as items in QAWRF were identified by conducting a systematic literature review and the items were placed under the suitable domains according to the description of items in the model. This is appropriate because the risk factors of WPV in healthcare are well known,23 and most literature grouped the risk factors identically to the model used in this study. The criteria for items inclusion were 1) risk factors that are related to WPV in healthcare settings, 2) risk factors that are related to WPV perpetrated by patients or visitors of healthcare settings, the most common type of WPV in healthcare settings, 3) risk factors that are suitable to be assessed using a structured questionnaire, and 4) risk factors that are related to the local setting. Databases such as Web of Science, Scopus, Cochrane, PubMed, and Google Scholar were used for the systematic literature review. The search was conducted using the keywords “workplace violence” or “workplace aggression”, “risk factors” or “predictors”, and “healthcare settings”. Risk factors extracted from primary studies, systematic reviews, and meta-analyses published since 2013 were listed and grouped under the suitable domain as suggested by the Chappell and Di Martino’s WPV model.19
The suitability of domains and items to be included in each questionnaire were then discussed by a three-member committee comprising an investigator studying WPV, an experienced occupational and safety committee member, and an occupational health specialist. The decision to include or remove any domain or item in each questionnaire was based on the committee’s judgement of the perceived ability of each target population to recognize the presence of each WPV risk factor generated. Domains or items judged as impossible for the target population of the questionnaire to detect or recognize were excluded from the respective questionnaire. The committee also assessed the wording used in the questionnaires, as the questionnaires were developed in the Malay language to ensure a better understanding of the questionnaires among the target population. A 5-point Likert scale was used (1 = the level of risk factor existence is very low at the facility, 5 = the level of risk factor existence is very high at the facility) for participants to rate the presence of each risk factor in their respective healthcare settings. Modifications to each questionnaire (elimination of constructs or items, change of wordings or fonts, order of items, and improvement on instructions given to participants) were made iteratively until committee members indicated that they were satisfied with the overall content and appearance of the questionnaires.29
Content Validation of QAWRF
The three component questionnaires, ie QAWRF-administrator, QAWRF-worker, and QAWRF-client were then sent to a panel of experts to empirically determine the content validity of QAWRF.30 The number of raters required for content validation ranged from two to 10 experts.30,31 Therefore, six experts with experience in managing WPV in healthcare settings and handling questionnaires for content validation were recruited for this study. They included 1) a public health specialist, 2) an occupational health specialist, 3) a senior assistant director of the occupational health unit in the Ministry of Health (MOH), 4) an assistant director of the human resource unit in the Department of Safety and Health (DOSH), 5) the head of the Occupational and Safety department in one of Malaysia’s main hospitals, and 6) a questionnaire expert.
The content validation was conducted through email because the national Standard Operation Procedure for Coronavirus Disease 2019 (COVID-19) during the validation process did not allow face-to-face meeting sessions. The experts were asked to rate the relevance of each item and provide further comments or suggest any changes. A 4-point Likert scale was used for scoring, where a score of one indicated that the item was not relevant, whereas a score of four suggested that the item was highly relevant.31 The expert panel was given two weeks to rate the questionnaires, and a reminder email was sent after the first week.
The collected data were compiled in Microsoft Excel, where the relevance rating given by the experts were dichotomized as 1 (agreed) if the experts rated items as 3 or 4 and 0 (disagreed) if the expert rated items as 1 or 2.30,31 Indices used to determine the content validity of each questionnaire included the Item Level Content Validity Index (I-CVI) and Scale Level Content Validity Index (S-CVI), which were calculated independently for each questionnaire. I-CVI for each item was calculated as the number of experts who agreed with the given items divided by the total number of experts [I-CVI = (agreed item) / (number of expert)].30–32 Items with I-CVI of more than 0.790 were considered relevant, items with I-CVI between 0.700 and 0.790 were revised according to the panel’s suggestions, and any item with I-CVI less than 0.700 was eliminated.30,32 Next, S-CVIs were then calculated based on the average method where the sum of I-CVIs for all items was divided by the total number of items on the questionnaire (S-CVI/Ave) [S-CVI/Ave = (sum of I-CVI scores) / (number of item)].30,32 An S-CVI/Ave score of more than 0.900 was considered to indicate excellent content validity.30,33
Face Validation of QAWRF
A quantitative method was used for face validation of the QAWRF, where respondents rated the clarity and comprehension of individual items in the QAWRF using the face validity form.34 Respondents rated each item based on a 4-point Likert scale, with 1 being not clear and understandable and 4 being very clear and understandable. An open-ended commentsection was also provided at the end of the form for raters to write any commentto further improve the QAWRF.
The minimum number of raters for the quantitative method of face validity was 10.34,35 Therefore, 12 raters for each component questionnaire and 36 total raters for QAWRF who fit the inclusion and exclusion criteria of the study (Table 1) were recruited to complete the survey. In a face-to-face session, raters were given the drafted questionnaire, the face validity form, and a pen. They were first instructed to complete the drafted questionnaire and then fill out the face validity form based on their experience when answering the drafted questionnaire.
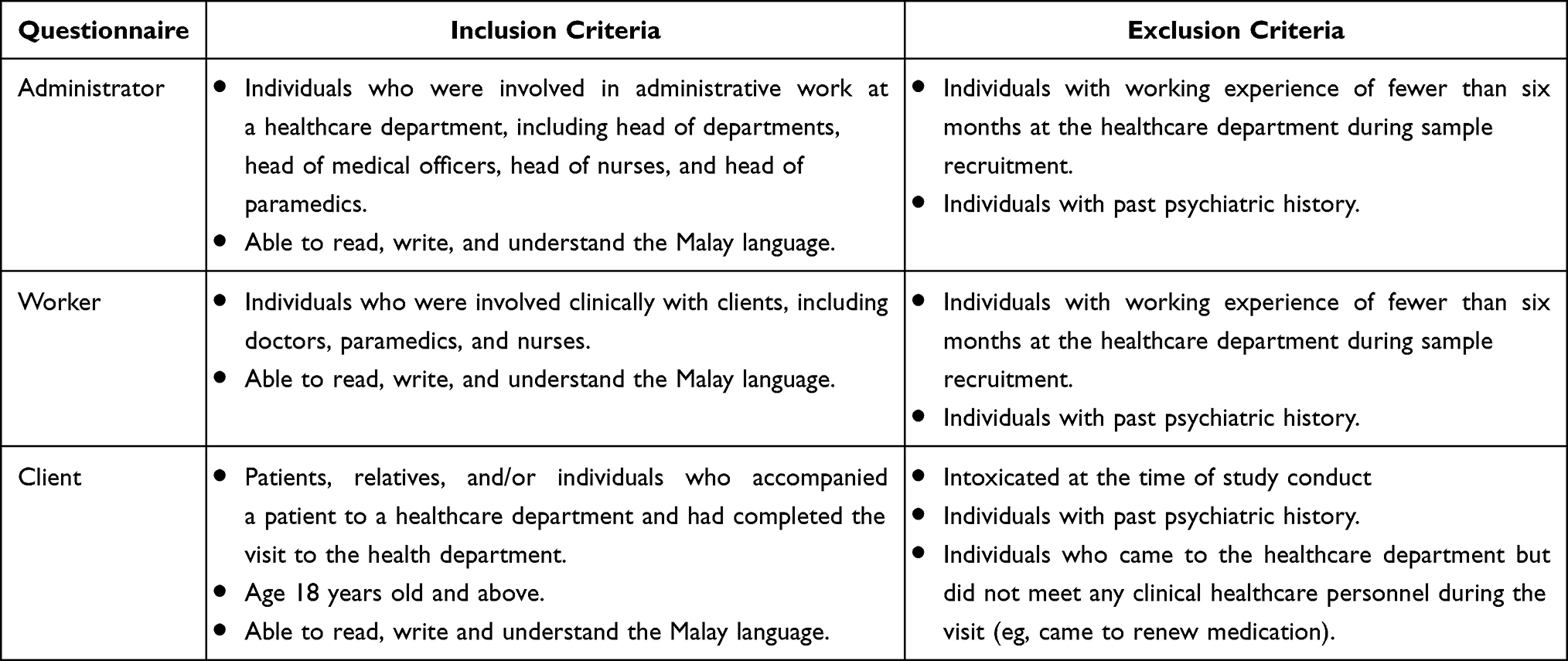 |
Table 1 Inclusion and Exclusion Criteria for the Face Validation and Pilot Survey |
The collected data were entered into Microsoft Excel, where ratings of 3 or 4 were recoded as 1 (clear), and ratings of 1 or 2 were recoded as 0 (not clear).34 The Item Level Face Validity Index (I-FVI), which is the proportion of rater scoring the items as clear was calculated [I-FVI = (agreed item) / (number of rater)].34 Then, the average of the total I-FVIs score on each questionnaire (S-FVI/Ave) [S-FVI/Ave = (sum of I-FVI scores) / (number of item)], and the proportion of items on the questionnaire that reached “Universal Agreement (UA)” where the item achieved 100% experts in agreement (S-FVI/UA) [S-FVI/UA = (sum of UA scores) / (number of item)] were calculated.34 The acceptable value for I-FVI, S-FVI/Ave and S-FVI/UA was 0.83.31,35 Modifications were made to QAWRF based on the scores and comments given by raters.
Pilot Survey and Reliability Testing of QAWRF
After modifications were made to the QAWRF based on the face validation findings, a pilot survey was conducted to ascertain the usability of QAWRF.36–38 In addition, Cronbach’s alpha was calculated to examine the internal consistency reliability of QAWRF questionnaires.39,40 Thirty respondents based on the pre-determined criteria (Table 1) were recruited to answer each questionnaire.39,41 The respondents were recruited from University Teknologi MARA (UiTM) Specialist Private Centre and Hospital Al-Sultan Abdullah, Selangor, Malaysia. Respondents were given a Participant Information Sheet, the self-administered questionnaire, and were asked to complete and return the questionnaire. The investigator recorded the time taken for respondents to answer the QAWRF and identified any logistic needs for a full-scale study. Meanwhile, data obtained from the pilot study were entered into SPSS Version 28 where Cronbach’s alpha was calculated for each questionnaire. A Cronbach’s alpha value of more than 0.7 was considered as acceptable.39,42,43
Results
Four domains were created by adapting Chappell and Di Martino’s Interactive Model of Workplace Violence. The domains include the client’s, worker’s, workplace, and social risk factors; the latter combines both broader contextual and societal risk factors. Twenty-eight studies were used for item generations (Table 2, Supplementary Table 1). A total of 65 items that fulfilled the item’s inclusion criteria were generated.
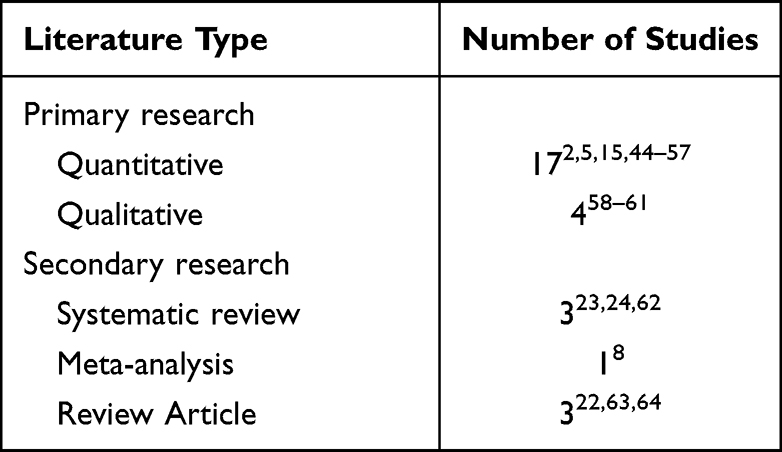 |
Table 2 Summary of Literature Used for Items Generation |
The QAWRF-administrator was developed by including all four domains and a total of 48 items. After content validation, three items with I-CVI score of less than 0.700 were eliminated and nine items were revised based on the comments given by the experts. No item was eliminated or revised during the face validation and pilot survey. The indices for the QAWRF-administrator were 0.920 for S-CVI/Ave (Table 3), 0.983 for S-FVI/Ave, and 0.844 for S-FVI/UA (Table 4). All domains in the QAWRF-administrator had acceptable Cronbach’s alpha values, which ranged from 0.809 to 0.930 (Table 5). The time taken to respond to the QAWRF-administrator ranged from 9 to 16 minutes.
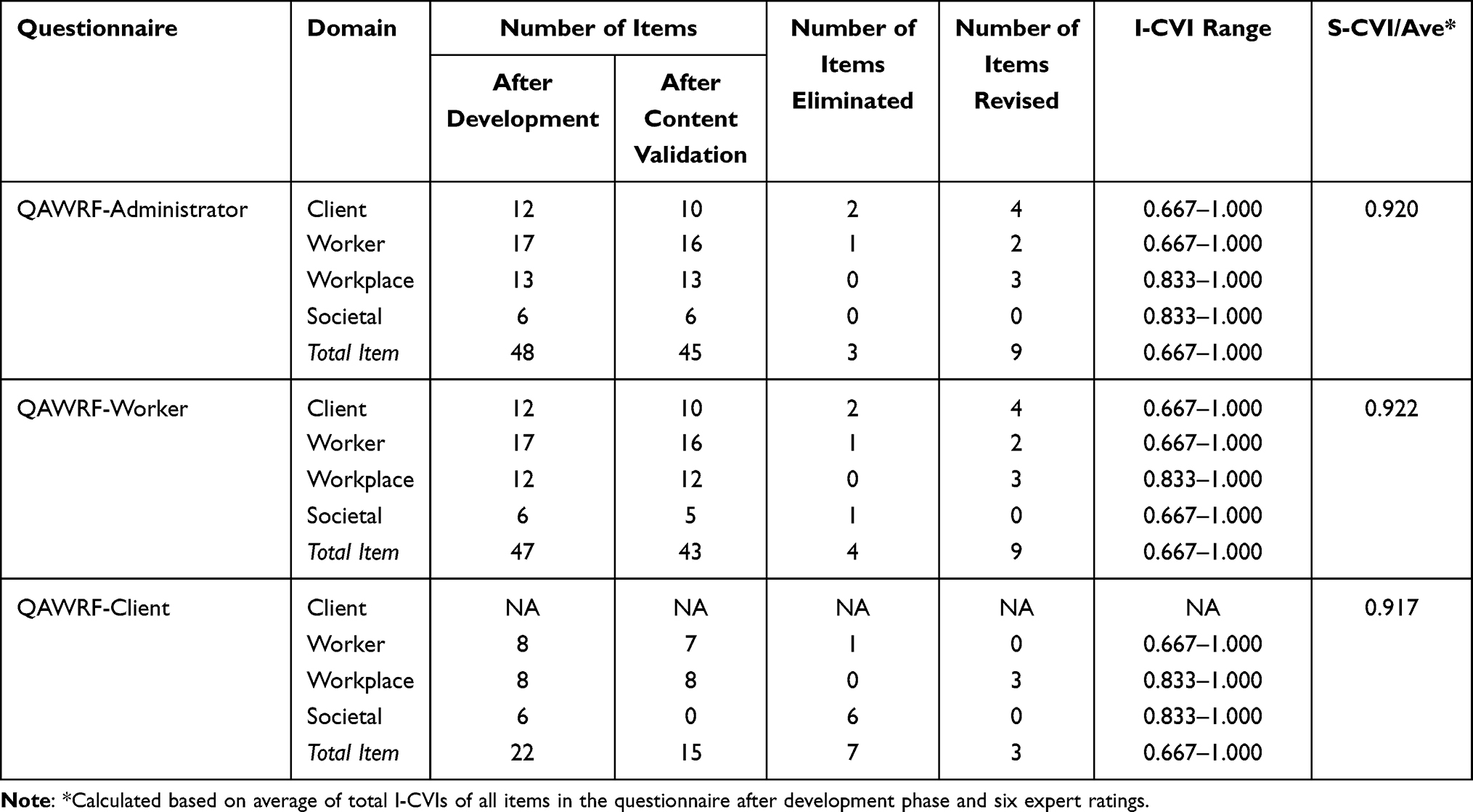 |
Table 3 Content Validity Indices for QAWRF |
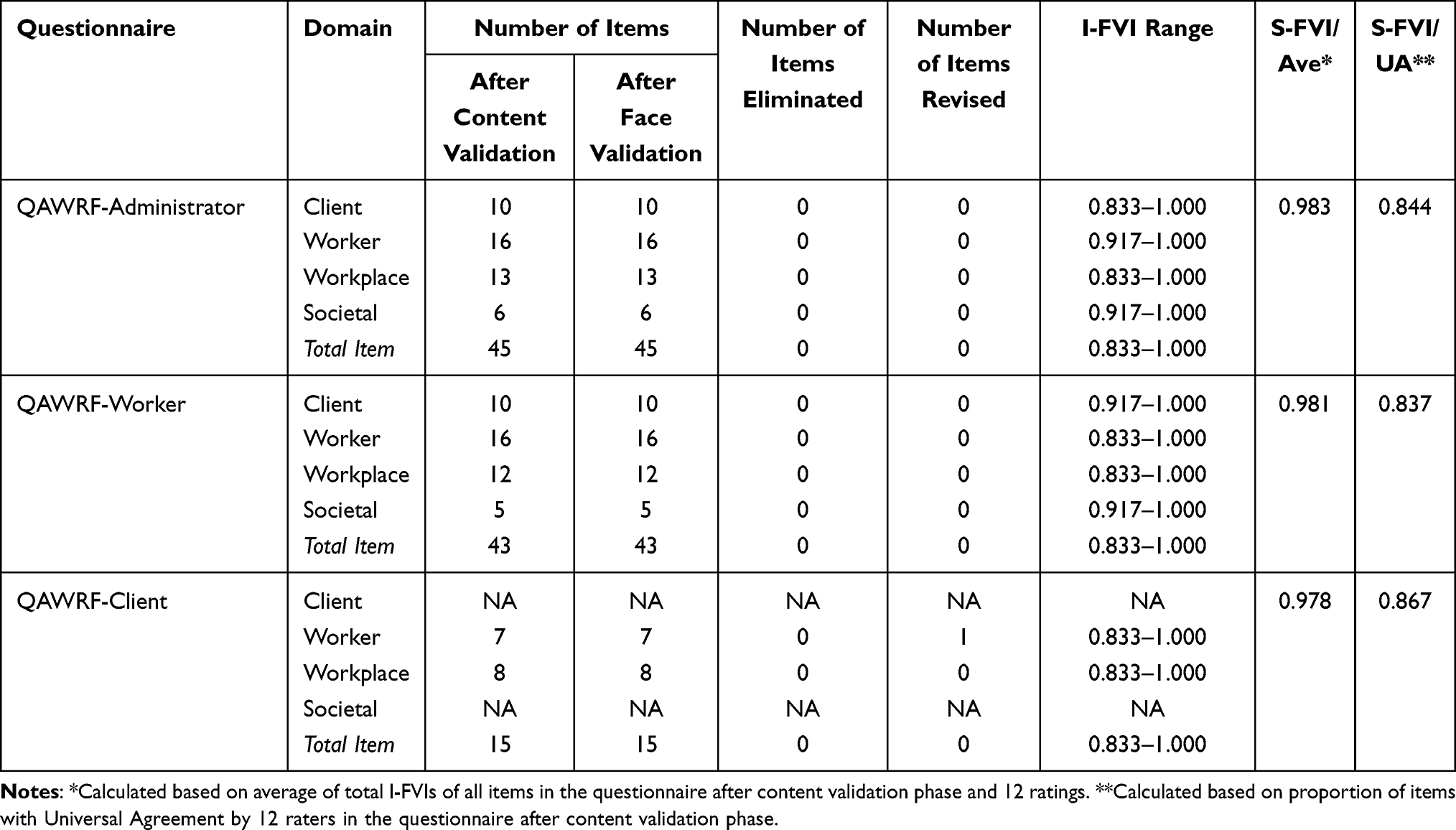 |
Table 4 Face Validity Indices for QAWRF |
 |
Table 5 Internal Consistency Reliability of QAWRF |
The QAWRF-worker started with four domains and a total of 47 items. After content validation, four items with I-CVI score of less than 0.700 were eliminated and nine items were revised based on the comments given by the experts. No item was eliminated or revised during the subsequent face validation and pilot survey. The indices for the QAWRF-worker were 0.922 for S-CVI/Ave (Table 3), 0.981 for S-FVI/Ave, and 0.837 for S-FVI/UA (Table 4). The Cronbach’s alpha values for the QAWRF-worker were acceptable and ranged from 0.892 to 0.949 (Table 5). The time taken to respond to the QAWRF-worker ranged from 8 to 15 minutes.
The QAWRF-client was developed using three domains with 22 items. After content validation, the societal domain, which contained six items, was eliminated following an expert comment. One item with I-CVI score of less than 0.700 from the worker domain was also eliminated. Meanwhile, three items were revised according to the experts’ comments. During the face validation, no item was eliminated, but one item was revised according to raters’ comments. Indices for the QAWRF-client were 0.917 for S-CVI/Ave (Table 3), 0.978 for S-FVI/Ave, and 0.867 for S-FVI/UA (Table 4). During the pilot survey, one item from the worker domain was eliminated because it contributed to low internal consistency (Cronbach’s alpha 0.653). The final Cronbach’s alpha values for the worker domain after the item removal improved to 0.866, whereas Cronbach’s alpha for the workplace domain was 0.770, which were acceptable (Table 5). The time taken to respond to the QAWRF-client ranged from 8 to 15 minutes.
In addition, several face validation raters commented that they had some confusion during the rating of items because of the end descriptors of the Likert scale used in QAWRF. The initial Likert scale end-descriptors used were 1 “the level of risk factor existence is very low at the facility” and 5 “the level of risk factor existence is very high at the facility”. Therefore, the study committee decided to change the scale’s end-descriptors to 1 “highly not apparent at the facility” and 5 “highly apparent at the facility” for users to rate the level of risk factor present at respective healthcare facilities. After the change was made, no further commentwas received for the Likert scale’s end descriptors.
Discussion
This study developed, validated, and determined the reliability of QAWRF, a set of structured survey questionnaires that can be used to assess WPV risk factors in healthcare settings based on a tripartite perspective of key stakeholders. Three different questionnaires were developed separately for each target group, namely administrators, workers, and clients. The separation of questionnaires was deemed essential because the perception of WPV risk factors differs among the three target population. For example, the administrators of departments, who are focused more on the department’s policies, staffing, and environments rather than delivering clinical services,65 might view WPV risk factors differently compared to workers. On the other hand, workers who work directly on the ground are likely more familiar with process activities, facility operations, and potential threats.3 This is supported by previous studies which demonstrate that divergent perceptions often exist between healthcare administrators and workers on different issues.66–68 Moreover, clinical workers were suggested to often report to other clinical workers in their department rather than to the administrators, which can create a gap in the perception of WPV risk factors between workers and administrators.68 Meanwhile, clients who spend the least time at a particular healthcare department compared to the other two target population may only recognize certain risk factors, and their knowledge regarding the presence of risk factors may also be influenced by incidences that might or might not happen during their visit to the healthcare setting. Therefore, three separate questionnaires for each key stakeholders are needed to ensure accuracy in determining WPV risk factors in healthcare settings and avoiding information bias.69,70 The separation also enables QAWRF users to collectively assess the risk factors of WPV at a particular healthcare setting through three different perspectives simultaneously, thus following the suggestion to involve all stakeholders at the local level for better policymaking.24 Ultimately, users can tailor interventions for their WPV prevention programs based on the findings of QAWRF.
The items for each component questionnaire were generated from the same pool of WPV risk factors. However, the instruction wordings, the items, and the number of items included differed. Moreover, since QAWRF is intended to be self-administered, each component questionnaire was designed specifically for each target population to ensure that the respondents can answer the questionnaire without the researcher’s or surveyor’s assistance.71 The component questionnaires were also developed separately to avoid contingency or filter questions, which can be confusing, counterintuitive to respondents, and lead to data error because only a subset of respondents are required to answer specific questions.72,73
A risk assessment approach was used for QAWRF, where respondents are expected to quantitively rate the existence of the risk factors available at a particular health department or facility based on their perception. This approach was selected because WPV incidences are difficult to predict, highlighting the need for WPV risk assessment or predictive tools.74 The quantitative design of QAWRF enable users to independently assess WPV risk factors without the need for interviews or walkthrough surveys. It might also provide better insight into WPV risk factors due to respondents’ anonymity and flexibility in answering the questions.73,75,76
For content validation, the less conservative method, ie, the S-CVI/average method, was chosen.30,32,77 Another method that can be used to calculate S-CVI is by calculating the value based on Universal Agreement among experts (S-CVI/UA). However, S-CVI/UA method will only yield a good score if all experts can 100% agree (Universal Agreement) with most items in a questionnaire.31 A Universal Agreement among experts on an item could not have been achieved during the content validation process which was conducted during the COVID-19 pandemic, because physical meetings were prohibited in Malaysia, and the experts had to rate the component questionnaires independently. Nevertheless, the S-CVI/Ave index indicated excellent content validity for QAWRF, suggesting that it can measure WPV risk factors adequately.
The QAWRF-administrator was developed using 48 items with one extra item related to funding for WPV prevention compared to the QAWRF-worker. After content validation, the items eliminated from the QAWRF-administrator include risk factors like “low educational status of the client”, “client with a history of violence”, and “unprepared worker”. The two items related to the client were eliminated because administrators are unlikely to know about the client’s educational status and violence history. Meanwhile, “unprepared worker” was eliminated because experts believed workers scheduled for work at the healthcare department should be fully prepared physically and mentally and should otherwise be on medical or annual leave.
For the QAWRF-worker, the four items eliminated include “low educational status of the client”, “client with a history of violence”, “worker’s having low self-esteem”, and “high unemployment in nearby communities”. The first two items were eliminated due to the workers being unlikely to know about the client’s educational and violence history as well. “Worker having low self-esteem” item was eliminated because the experts argued that a worker may not be able to evaluate another worker’s self-esteem. “High unemployment in nearby communities” was eliminated because the experts felt that workers might not know about the unemployment rate in the communities where they work.
The QAWRF-client was developed using only three domains where the client’s risk factors domain was excluded. The exclusion was made because clients who attend a healthcare department are only exposed to characteristics of other clients for a minimal time, and thus are not suited to rate the risk factors related to other patients. After content validation, the societal domain was also eliminated from the questionnaire because some clients who visit a particular healthcare department do not live near the facility. In these cases, they might have travelled far to get treatment at a particular healthcare department which may cause them to have poor knowledge regarding the area’s societal risk factors for WPV. In addition, two items were eliminated; one during the content validation whereas another was eliminated during the pilot survey. The item “unprepared worker” was eliminated because experts felt that clients are unlikely to know about a worker’s physical or mental state of preparation at their workplace, whereas “worker probably having high workload” was eliminated because of the initial low Cronbach’s alpha value for the worker domain (Table 5). The low Cronbach’s alpha value might reflect poor inter-relatedness between the eliminated item and other items within the domain,43 which may be due to clients’ difficulties in estimating the workload of HCW, thus causing random responses. Therefore, the committee agreed to eliminate the item from the questionnaire.
The Likert scale’s end descriptors for QAWRF were modified following comments from the face validation, where raters commented that they were confused when using the scale for rating the questionnaire. This supports the suggestion that respondents’ communicative and cognitive processes when answering a questionnaire can be affected by the design of the rating scale.78–80 For QAWRF, the study committee noted that this issue existed because the end descriptors were too wordy. In addition, the QAWRF items were based on risk factors which had to be negatively worded (eg, “workers not knowing workplace violence prevention guidelines at their workplace”), where upon using the initial scale’s end descriptors, some raters reported being confused as to whether the risk factors should be rated as 1 or 5 if the negatively worded items were in a good or desirable condition. Therefore, to improve the understanding of the rating scale among respondents, the scale’s end descriptors were revised to “highly apparent” and “highly not apparent”, which are less wordy and the word “apparent” itself is better understood in Malay compared to the word “existence”.
Some studies recommend avoiding negative statements in a questionnaire as they might affect the construct validity and reliability of a questionnaire.79,81 However, this may not apply to QAWRF as all items included are WPV risk factors despite some being stated in non-negative wording (eg, “overcrowding of patient’s area”). Respondents are required to rate the presence of the WPV risk factors unidirectionally without the need to reverse their cognitive understanding on the rating scale, which might occur if protective factors are also included in QAWRF. This is supported by good internal consistencies of QAWRF as reflected by the Cronbach’s alpha indices.79,81
There are a few limitations to this study. Firstly, QAWRF potentially lacks generalizability because it was developed in Malay, and the risk factors selected were specific to Type 2 WPV in healthcare. Secondly, the administrator and QAWRF-worker were quite lengthy because there were multiple WPV risk factors that had to be included to ensure the robustness of the questionnaire. Nevertheless, efforts were made to use short wording for each item to reduce respondent fatigue.82 Thirdly, as aforementioned, the questionnaires were validated without any physical meeting between expert panels, which may have limited the discussion regarding the inclusion of items in the questionnaires. Nevertheless, the psychometric indices for QAWRF remained adequate. Future studies should include assessment of the construct validity and test–retest reliability of QAWRF, as well as the translation and validation of the English version of QAWRF to strengthen its usability and validity.
Conclusion
This study has developed, validated, and determined the reliability of a set of questionnaires, QAWRF, that can be used to assess risk factors of WPV in healthcare facilities based on the perspectives of three key healthcare stakeholders. In terms of theoretical implications, the QAWRF would be a valid and convenient tool for researchers to collect data on the prevalence of different WPV risk factors in any healthcare setting. In terms of practical implications, the findings from QAWRF will be valuable for policymakers developing WPV prevention policies and programs at a departmental or organizational level. These worksite-specific WPV interventions are expected to be resource efficient and more effective than a general WPV intervention.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to restrictions from data owners.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki. It was approved by the Medical Research & Ethics Committee [NMMR-21-537-58890 (IIR), approval date 18 May 2021] and Universiti Teknologi MARA (UiTM) Research Ethic Committee [REC/07/2021 (MR/629), approval date 2 August 2021].
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgment
We would like to express our special gratitude to the panel of experts for their involvement in validating the questionnaires.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is funded by Universiti Teknologi MARA’s Faculty of Medicine Research Grant [600-TNCPI 5/3/DDF (MEDIC) (010/2021)]. The funding sponsors had no role in the design, execution, interpretation, or writing of the study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. NIOSH. Occupational violence; 2021. Available from: https://www.cdc.gov/niosh/topics/violence/default.html.
2. Tian Y, Yue Y, Wang J, Luo T, Li Y, Zhou J. Workplace violence against hospital healthcare workers in China: a national WeChat-based survey. BMC Public Health. 2020;20(1):582. doi:10.1186/s12889-020-08708-3
3. OSHA. Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers (OSHA, 3148-04R). Washington, DC: OSHA; 2015.
4. University of Iowa Injury Prevention Research Center. Workplace Violence: A Report to the Nation. IA: University of Iowa Iowa City; 2001.
5. Ariffin AA. Workplace violence among healthcare workers in a health district and its predicting factors. Int J Public Health Clin Sci. 2020;7(5):65–80.
6. Mento C, Silvestri MC, Bruno A, et al. Workplace violence against healthcare professionals: a systematic review. Aggress Violent Behav. 2020;51:101381. doi:10.1016/j.avb.2020.101381
7. Saragoza P, White SG. Workplace violence: practical considerations for mental health professionals in consultation, assessment, and management of risk. Psychiatr Clinics. 2016;39(4):599–610. doi:10.1016/j.psc.2016.07.007
8. Liu J, Gan Y, Jiang H, et al. Prevalence of workplace violence against healthcare workers: a systematic review and meta-analysis. Occup Environ Med. 2019;76(12):927. doi:10.1136/oemed-2019-105849
9. Li Y-L, Li R-Q, Qiu D, Xiao S-Y. Prevalence of workplace physical violence against health care professionals by patients and visitors: a systematic review and meta-analysis. Int J Environ Res Public Health. 2020;17(1):299. doi:10.3390/ijerph17010299
10. Pompeii L, Benavides E, Pop O, et al. Workplace violence in outpatient physician clinics: a systematic review. Int J Environ Res Public Health. 2020;17(18):6587. doi:10.3390/ijerph17186587
11. International Labour Organisation (ILO). Joint Programme Launches New Initiative Against Workplace Violence in the Health Sector. Geneva: International Labour Organisation (ILO); 2022.
12. U.S. Bureau of Labor Statistics. Workplace Violence: Homicides and Nonfatal Intentional Injuries by Another Person in 2020. United States of America: U.S. Bureau of Labor Statistics,; 2022.
13. Abdellah RF, Salama KM. Prevalence and risk factors of workplace violence against health care workers in emergency department in Ismailia, Egypt. Pan Afr Med J. 2017;26:21. doi:10.11604/pamj.2017.26.21.10837
14. Copeland D, Henry M. Workplace violence and perceptions of safety among emergency department staff members: experiences, expectations, tolerance, reporting, and recommendations. J Trauma Nurs. 2017;24(2):65–77. doi:10.1097/JTN.0000000000000269
15. Hedayati Emam G, Alimohammadi H, Zolfaghari Sadrabad A, Hatamabadi H. Workplace violence against residents in emergency department and reasons for not reporting them; a cross sectional study. Emerg. 2018;6(1):e7.
16. Hamdan M, Abu Hamra A. Workplace violence towards workers in the emergency departments of Palestinian hospitals: a cross-sectional study. Hum Resour Health. 2015;13:28. doi:10.1186/s12960-015-0018-2
17. Hogarth KM, Beattie J, Morphet J. Nurses attitudes towards the reporting of violence in the emergency department. Australas Emerg Nurs J. 2016;19(2):75–81. doi:10.1016/j.aenj.2015.03.006
18. Lanctôt N, Guay S. The aftermath of workplace violence among healthcare workers: a systematic literature review of the consequences. Aggress Violent Behav. 2014;19(5):492–501. doi:10.1016/j.avb.2014.07.010
19. Chappell D, Di Martino V. Violence at Work. International Labour Organization; 2006.
20. Copeland D, Henry M. The relationship between workplace violence, perceptions of safety, and Professional Quality of Life among emergency department staff members in a Level 1 Trauma Centre. Int Emerg Nurs. 2018;39:26–32. doi:10.1016/j.ienj.2018.01.006
21. Pourshaikhian M, Abolghasem Gorji H, Aryankhesal A, Khorasani-Zavareh D, Barati A. A systematic literature review: workplace violence against emergency medical services personnel. Arch Trauma Res. 2016;5(1):e28734. doi:10.5812/atr.28734
22. Kumari A, Kaur T, Ranjan P, Chopra S, Sarkar S, Baitha U. Workplace violence against doctors: characteristics, risk factors, and mitigation strategies. J Postgrad Med. 2020;66(3):149–154.
23. Raveel A, Schoenmakers B. Interventions to prevent aggression against doctors: a systematic review. BMJ Open. 2019;9(9):e028465. doi:10.1136/bmjopen-2018-028465
24. Hossain MM, Sharma R, Tasnim S, Al Kibria GM, Sultana A, Saxena T. Prevalence, characteristics, and associated factors of workplace violence against healthcare professionals in India: a systematic review and meta-analysis. medRxiv. 2020;2020:1254.
25. Milczarek M. Workplace Violence and Harassment: A European Picture. Publications Office of the European Union; 2010.
26. Albrechtsen E, Solberg I, Svensli E. The application and benefits of job safety analysis. Saf Sci. 2019;113:425–437. doi:10.1016/j.ssci.2018.12.007
27. Geer JG. What do open-ended questions measure? Public Opin Q. 1988;52(3):365–367. doi:10.1086/269113
28. Vidal-Martí C, Testor CP. Is Chappell and Di Martino’s interactive model of workplace violence valid? An article analysing workplace violence towards healthcare professionals in Spain. Aggress Violent Behav. 2017;35:83–90. doi:10.1016/j.avb.2017.05.006
29. Yaddanapudi S, Yaddanapudi LN. How to design a questionnaire. Indian J Anaesth. 2019;63(5):335–337. doi:10.4103/ija.IJA_334_19
30. Rodrigues IB, Adachi JD, Beattie KA, MacDermid JC. Development and validation of a new tool to measure the facilitators, barriers and preferences to exercise in people with osteoporosis. BMC Musculoskelet Disord. 2017;18(1):540. doi:10.1186/s12891-017-1914-5
31. Yusoff MSB. ABC of content validation and content validity index calculation. Educ Med J. 2019;11(2):49–54. doi:10.21315/eimj2019.11.2.6
32. Zamanzadeh V, Ghahramanian A, Rassouli M, Abbaszadeh A, Alavi-Majd H, Nikanfar AR. Design and implementation content validity study: development of an instrument for measuring patient-centered communication. J Caring Sci. 2015;4(2):165–178. doi:10.15171/jcs.2015.017
33. Shi J, Mo X, Sun Z. [Content validity index in scale development]. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2012;37(2):152–155. Chinese. doi:10.3969/j.issn.1672-7347.2012.02.007
34. Yusoff MSB. ABC of response process validation and face validity index calculation. Education in Medicine Journal. 2019;11(3):55–61. doi:10.21315/eimj2019.11.3.6
35. Mohamad Marzuki MF, Yaacob NA, Yaacob NM. Translation, cross-cultural adaptation, and validation of the Malay version of the system usability scale questionnaire for the assessment of mobile apps. JMIR Hum Factors. 2018;5(2):e10308. doi:10.2196/10308
36. In J. Introduction of a pilot study. Korean J Anesthesiol. 2017;70(6):601–605. doi:10.4097/kjae.2017.70.6.601
37. Van Teijlingen E, Hundley V. The importance of pilot studies. Nurs Standard. 2002;16(40):33. doi:10.7748/ns2002.06.16.40.33.c3214
38. Drummond A. Feasibility and Pilot Studies: Why are They Important? London, England: SAGE Publications Sage UK; 2017:335–336.
39. Bujang MA, Omar ED, Baharum NA. A review on sample size determination for cronbach’s alpha test: a simple guide for researchers. Malays J Med Sci. 2018;25(6):85–99. doi:10.21315/mjms2018.25.6.9
40. Bujang MA, Ismail M, Hatta N, Othman SH, Baharum N, Lazim SSM. Validation of the Malay version of Diabetes Quality of Life (DQOL) questionnaire for adult population with type 2 diabetes mellitus. Malays J Med Sci. 2017;24(4):86–96. doi:10.21315/mjms2017.24.4.10
41. Johanson GA, Brooks GP. Initial scale development: sample size for pilot studies. Educ Psychol Meas. 2010;70(3):394–400. doi:10.1177/0013164409355692
42. Cortina JM. What is coefficient alpha? An examination of theory and applications. J Appl Psychol. 1993;78(1):98–104. doi:10.1037/0021-9010.78.1.98
43. Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. 2011;2:53–55. doi:10.5116/ijme.4dfb.8dfd
44. Kaur A, Ahamed F, Sengupta P, Majhi J, Ghosh T. Pattern of workplace violence against doctors practising modern medicine and the subsequent impact on patient care, in India. PLoS One. 2020;15(9):e0239193–e. doi:10.1371/journal.pone.0239193
45. Du Y, Wang W, Washburn DJ, et al. Violence against healthcare workers and other serious responses to medical disputes in China: surveys of patients at 12 public hospitals. BMC Health Serv Res. 2020;20(1):253. doi:10.1186/s12913-020-05104-w
46. Deniz S, Yüksel O. A Study on the Determination of the Reasons for Violence Against Healthcare Workers. Acıbadem Üniversitesi Sağlık Bilimleri Dergisi; 2020.
47. Yenealem DG, Woldegebriel MK, Olana AT, Mekonnen TH. Violence at work: determinants & prevalence among health care workers, northwest Ethiopia: an institutional based cross sectional study. Ann Occup Environ Med. 2019;31:8. doi:10.1186/s40557-019-0288-6
48. Yang SZ, Wu D, Wang N, et al. Workplace violence and its aftermath in China’s health sector: implications from a cross-sectional survey across three tiers of the health system. BMJ Open. 2019;9(9):e031513–e. doi:10.1136/bmjopen-2019-031513
49. Seun-Fadipe CT, Akinsulore AA, Oginni OA. Workplace violence and risk for psychiatric morbidity among health workers in a tertiary health care setting in Nigeria: prevalence and correlates. Psychiatry Res. 2019;272:730–736. doi:10.1016/j.psychres.2018.12.177
50. Sachdeva S, Jamshed N, Aggarwal P, Kashyap SR. Perception of workplace violence in the emergency department. J Emerg Trauma Shock. 2019;12(3):179–184. doi:10.4103/JETS.JETS_81_18
51. Bin Abd Rahman R, Azira Bt Hamis A, Sahiran MNB, Muhamad M. Workplace violence among healthcare workers in health clinics, Melaka Tengah District: a cross sectional study.
52. Olgun S, Adibelli D. The views of patient’s relatives about the violence towards to the health care staff. Int J Caring Sci. 2019;12(3):254.
53. Hanim Abd Aziz K, Pasi H, Nasreen HE, Zubir M, Artika hassan N, Ab Rahman J. Prevalence of workplace violence and its associated factors among healthcare providers at International Islamic University Malaysia Medical Center (IIUMMC).
54. Zainal N, Rasdi I, Saliluddin SM. The risk factors of workplace violence among healthcare workers in public hospital. Malaysian Journal of Medicine and Health Sciences. 2018;14(SP2):120–127.
55. Arnetz J, Hamblin LE, Sudan S, Arnetz B. Organizational determinants of workplace violence against hospital workers. J Occupat Environ Med. 2018;60(8):693–699. doi:10.1097/JOM.0000000000001345
56. Al-Azzam M, Al-Sagarat AY, Tawalbeh L, Poedel RJ. Mental health nurses’ perspective of workplace violence in Jordanian mental health hospitals. Perspect Psychiatr Care. 2018;54(4):477–487. doi:10.1111/ppc.12250
57. AbuAlRub RF, Al Khawaldeh AT. Workplace physical violence among hospital nurses and physicians in underserved areas in Jordan. J Clin Nurs. 2014;23(13–14):1937–1947. doi:10.1111/jocn.12473
58. Spelten E, Thomas B, O’Meara P, van Vuuren J, McGillion A. Violence against Emergency Department nurses; Can we identify the perpetrators? PLoS One. 2020;15(4):e0230793. doi:10.1371/journal.pone.0230793
59. Davey K, Ravishankar V, Mehta N, et al. A qualitative study of workplace violence among healthcare providers in emergency departments in India. Int J Emerg Med. 2020;13(1):33. doi:10.1186/s12245-020-00290-0
60. Beattie J, Griffiths D, Innes K, Morphet J. Workplace violence perpetrated by clients of health care: a need for safety and trauma-informed care. J Clin Nurs. 2019;28(1–2):116–124. doi:10.1111/jocn.14683
61. Ramacciati N, Ceccagnoli A, Addey B, Rasero L. Violence towards emergency nurses. The Italian National Survey 2016: a qualitative study. Int J Nurs Stud. 2018;81:21–29. doi:10.1016/j.ijnurstu.2018.01.017
62. Nowrouzi-Kia B, Chai E, Usuba K, Nowrouzi-Kia B, Casole J. Prevalence of type II and type III workplace violence against physicians: a systematic review and meta-analysis. Int J Occup Environ Med. 2019;10(3):99–110. doi:10.15171/ijoem.2019.1573
63. D’Ettorre G, Pellicani V, Mazzotta M, Vullo A. Preventing and managing workplace violence against healthcare workers in Emergency Departments. Acta Biomed. 2018;89(4–s):28–36. doi:10.23750/abm.v89i4-S.7113
64. Ahmad M, Al-Rimawi R, Masadeh A, Atoum M. Workplace violence by patients and their families against nurses: literature review. International Journal of Nursing and Health Science. 2015;2(4):46–55.
65. Aries NR. Managing diversity: the differing perceptions of managers, line workers, and patients. Health Care Manage Rev. 2004;29(3):172–180. doi:10.1097/00004010-200407000-00002
66. Na E, Jung Y, Kim S. How do care service managers and workers perceive care robot adoption in elderly care facilities? Technol Forecast Soc Change. 2023;187:122250. doi:10.1016/j.techfore.2022.122250
67. Bäckström I. Health-related quality management values – comparing manager and co-worker perceptions. Int J Qual Service Sci. 2019;11(4):588–603. doi:10.1108/IJQSS-08-2018-0071
68. Begun JW, White KR, Mosser G. Interprofessional care teams: the role of the healthcare administrator. J Interprof Care. 2011;25(2):119–123. doi:10.3109/13561820.2010.504135
69. Pearce N, Checkoway H, Kriebel D. Bias in occupational epidemiology studies. Occup Environ Med. 2007;64(8):562–568. doi:10.1136/oem.2006.026690
70. Taherdoost H. How to design and create an effective survey/questionnaire; A step by step guide. Int J Acad Res Manage. 2016;5(4):37–41.
71. Fink A. How to Conduct Self-Administered and Mail Surveys, the Survey Kit.
72. Roszkowski M, Soven M, Glatzer M. The questionnaire looks self explanatory, so to save time i’ll just skip the skip instructions. Survey Pract. 2014;7(5):24.
73. Cohen L, Manion L, Morrison K. Research Methods in Education.
74. Ramacciati N, Ceccagnoli A, Addey B, Lumini E, Rasero L. Violence towards emergency nurses: a narrative review of theories and frameworks. Int Emerg Nurs. 2018;39:2–12. doi:10.1016/j.ienj.2017.08.004
75. Ong AD, Weiss DJ. The impact of anonymity on responses to sensitive questions 1. J Appl Soc Psychol. 2000;30(8):1691–1708. doi:10.1111/j.1559-1816.2000.tb02462.x
76. Krosnick JA. Questionnaire Design. The Palgrave Handbook of Survey Research. Springer; 2018:439–455.
77. Ho JM, Sia JKM. Embracing an uncertain future: COVID-19 and MICE in Malaysia. Local Dev Soci. 2020;1(2):190–204. doi:10.1080/26883597.2020.1818533
78. Höhne JK, Krebs D, Kühnel S-M. Measurement properties of completely and end labeled unipolar and bipolar scales in Likert-type questions on income (in)equality. Soc Sci Res. 2021;97:102544. doi:10.1016/j.ssresearch.2021.102544
79. Chyung SY, Barkin JR, Shamsy JA. Evidence-based survey design: the use of negatively worded items in surveys. Performance Improve. 2018;57(3):16–25. doi:10.1002/pfi.21749
80. Hartley J. Some thoughts on Likert-type scales. Int J Clin Health Psychol. 2014;14(1):83–86. doi:10.1016/S1697-2600(14)70040-7
81. Salazar MS. The dilemma of combining positive and negative items in scales. Psicothema. 2015;27(2):192–199. doi:10.7334/psicothema2014.266
82. Guo Y, Kopec JA, Cibere J, Li LC, Goldsmith CH. Population survey features and response rates: a randomized experiment. Am J Public Health. 2016;106(8):1422–1426. doi:10.2105/AJPH.2016.303198
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cholesterol and Hypertension Treatment Improve Coronary Risk Prediction but Not Time-Dependent Covariates or Competing Risks
Subirana I, Camps-Vilaró A, Elosua R, Marrugat J, Tizón-Marcos H, Palomo I, Dégano IR
Clinical Epidemiology 2022, 14:1145-1154
Published Date: 11 October 2022
Characteristics and Influencing Factors of Post-Traumatic Growth: A Cross-Sectional Study of Psychiatric Nurses Suffering from Workplace Violence in Guangdong China

Wang W, Ye J, Wei Y, Yuan L, Wu J, Xia Z, Huang J, Wang H, Li Z, Guo J, Xiao A
Journal of Multidisciplinary Healthcare 2024, 17:1291-1302
Published Date: 20 March 2024
Willingness to Pay for Telemedicine Services Among Uninsured Individuals in Saudi Arabia: A Cross-Sectional Survey
Almalki ZS, Alrashdi AM, AlHuzaimi DE, Alotaibi JO, Alqahtani MM, Alzahrani RD, Alajmi SA, AlOsaimi RR, Majrashi SM, Alahmari AK, Alshehri AM, Alzarea AI, Imam MT, Alshlowi AA
International Journal of General Medicine 2024, 17:3879-3891
Published Date: 6 September 2024
Discrepancies in Cardiovascular Disease Risk Perception Among African American Emerging Adults
Smith SB, Magwood GS, Abshire DA, Tavakoli AS, McCutcheon GS, Jenerette C
Nursing: Research and Reviews 2025, 15:57-77
Published Date: 17 May 2025
Study on Risk Factors and Treatment Strategies for Deep Vein Thrombosis in Patients with Multiple Myeloma
Guo Y, Yan L, Yang X, Fan C, Reaila J, Jia Y, Hao X, Ju F, Shi Z
Cancer Management and Research 2025, 17:1667-1677
Published Date: 15 August 2025