Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Digital Transformation and Team-Based Care: Pharmacists in Multidisciplinary Models – A Narrative Review
Authors Alshahrani AM, Vasudevan R ![]() , Hmlan A, Mohammed Assiri A, Asiri AM, Asiri OAM, Abduh Mashni A
, Hmlan A, Mohammed Assiri A, Asiri AM, Asiri OAM, Abduh Mashni A
Received 23 October 2025
Accepted for publication 19 January 2026
Published 11 February 2026 Volume 2026:19 576298
DOI https://doi.org/10.2147/JMDH.S576298
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Asma M Alshahrani,1 Rajalakshimi Vasudevan,2 Amjad Hmlan,3 Abdullah Mohammed Assiri,4 Ahmad Mohammed Asiri,5 Omar Ahmed M Asiri,5 Ali Abduh Mashni5
1Department of Clinical Pharmacy, College of Pharmacy, Shaqra University, Dawadimi, Saudi Arabia; 2Department of Pharmacology, College of Pharmacy, King Khalid University, Abha, Saudi Arabia; 3Department of Clinical Pharmacy, College of Pharmacy, King Khalid University, Abha, Saudi Arabia; 4Department of Medical and Dental Supplies, Medical Services, Ministry of Interior, Riyadh, Saudi Arabia; 5Khamis Mushayt General Hospital, Aseer Health Cluster, Ministry of Health, Khamis Mushait, 62433, Saudi Arabia
Correspondence: Rajalakshimi Vasudevan, College of Pharmacy, King Khalid University, Abha, Saudi Arabia, Email [email protected]
Background: Healthcare systems worldwide are increasingly challenged by the rise in chronic diseases, aging populations, and the growing demand for personalized care. Traditional models, where healthcare professionals operate independently with limited interdisciplinary communication are proving insufficient to meet the complex and interconnected needs of modern patients.
Objective: This review explores the growing importance of innovative and multidisciplinary approaches in healthcare, with a specific focus on the expanding role of pharmacists and the integration of digital tools. Unlike reviews that examine either multidisciplinary care or digital health in isolation, this review integrates evidence on how pharmacists function as clinical and digital connectors within multidisciplinary care models across diverse health systems.
Methods: This narrative review synthesized evidence on multidisciplinary care models that integrate pharmacists and digital tools. PubMed, Scopus, and Google Scholar were searched (2015–March 2024) using terms related to multidisciplinary care, pharmacists/clinical pharmacy, and digital health (e.g. EHRs, telehealth, AI, mHealth). English-language peer-reviewed studies describing pharmacist integration in team-based and/or technology-enabled care were included; grey literature and non-peer-reviewed sources were excluded.
Results: Across multiple care models, pharmacist integration in multidisciplinary teams was associated with improved chronic disease indicators (eg, better blood pressure or glycaemic control), fewer medication-related problems, including reports of reduced medication errors (eg, ~45% reduction in rural telepharmacy settings), and reduced avoidable hospitalizations/readmissions in transition-of-care settings. Digital innovations such as clinical decision support and telehealth platforms further enhanced coordination and continuity of care, enabling timely medication optimization and follow-up. Case studies from the UK, Canada, Saudi Arabia, Australia, India and South Africa selected LMICs illustrate context-adapted and scalable approaches.
Conclusion: When supported by enabling policy frameworks and robust digital infrastructure, multidisciplinary healthcare models offer a powerful solution to many of today’s healthcare challenges. Empowering pharmacists, investing in interoperable technologies, and reforming education and reimbursement structures are critical next steps toward resilient, patient-centered healthcare systems.
Plain Language Summary: This review explains how healthcare is changing to meet modern challenges such as chronic diseases and rising patient expectations. It describes how different professionals doctors, pharmacists, nurses, and others—work together as a team to improve care. The paper also shows how digital tools like electronic health records, telemedicine, and artificial intelligence make communication faster and safer between patients and providers. Real examples from countries such as Saudi Arabia, the United Kingdom, Canada, and Australia demonstrate how teamwork and technology help reduce medication errors, improve long-term disease control, and make healthcare more efficient and patient-centred. Overall, the review suggests that supporting pharmacists and using safe, connected digital systems can make care more coordinated and patient-centred across different health systems.
Keywords: multidisciplinary healthcare, clinical pharmacy, digital health, pharmacist integration, telemedicine, artificial intelligence in healthcare, interprofessional collaboration, medication therapy management, pharmacogenomics, health informatics
Introduction
Healthcare systems worldwide are undergoing transformation, driven by demographic shifts, the rising burden of chronic non-communicable diseases (NCDs), increasing demand for personalized care, and rapid technological progress. Traditional siloed approaches, where professionals work independently, are no longer adequate. Patients with multimorbidity, polypharmacy, and psychosocial needs require integrated care delivered by coordinated teams rather than fragmented, profession-specific pathways.
The World Health Organization (WHO) defines multidisciplinary care as coordinated, patient-centered services provided by diverse professionals, each contributing distinct expertise (WHO, 2010).1 Unlike interdisciplinary models, which blur roles, multidisciplinary teams emphasize role distinction while working toward shared goals. Such models improve outcomes in chronic disease management, oncology, geriatrics, and mental health (Reeves et al, 2017).2
Pharmacists exemplify this shift. Once mainly dispensers, they now play clinical roles in pharmacotherapy optimization, safety, and education. Their integration in medication therapy management (MTM), outpatient clinics, and ward rounds reduces errors, improves adherence, and enhances outcomes (Bond & Raehl, 2007).3 In oncology, pharmacogenomic data are used to tailor chemotherapy (Relling & Evans, 2015).4 In community care, pharmacists support adherence, chronic disease management, and patient education. Importantly, these expanded pharmacist roles increasingly rely on digital health infrastructure—such as electronic prescribing, clinical decision support, and data-driven medication management—positioning pharmacists at the intersection of clinical care and digital transformation.
Digital health tools such as electronic health records (EHRs), clinical decision support systems (CDSS), mobile health (mHealth) apps, and telemedicine strengthen collaboration and continuity of care (Bates et al, 2018).5 Pharmacists use AI-driven systems for drug interaction alerts, dosing guidance, and population health monitoring, while telepharmacy extends services to underserved populations. These developments align with global policy directions, including the WHO Global Strategy on Digital Health (2020–2025), which emphasizes interoperable systems and digitally enabled multidisciplinary care.
Non-communicable diseases such as diabetes, hypertension, and cardiovascular disease remain leading contributors to global morbidity and mortality, necessitating long-term, coordinated management. Within multidisciplinary teams, pharmacists are particularly critical for managing polypharmacy, optimizing medication regimens, monitoring adherence, and supporting patient self-management.6
The COVID pandemic highlighted the need for flexible, multidisciplinary systems. Lockdowns drove rapid adoption of telemedicine, digital prescribing, and AI-based triaging. Pharmacists expanded roles in vaccination, counseling, and supply chain management, underscoring their adaptability and importance during crises (Cadogan & Hughes, 2021).7
Despite growing evidence supporting multidisciplinary and digitally enabled care models, significant barriers remain. Barriers include institutional inertia, siloed structures, poor interoperability of digital platforms, inadequate reimbursement models, and professional hierarchies. Many education programs remain discipline-specific, limiting exposure to interprofessional education (IPE) and digital health (IOM, 2015).8
Integration efforts vary worldwide. In the UK and Canada, pharmacists are embedded in primary care networks. In Australia, digital tools such as MedAdvisor support adherence. Saudi Arabia’s Vision 2030 emphasizes pharmacist empowerment and digital health reforms. Interprofessional education, where students from medicine, pharmacy, nursing, and allied health train together, improves teamwork and role clarity (Institute of Medicine, 2015).8 Pharmacists were selected as the central focus of this review because their scope uniquely spans medication optimization, patient education, and digital medication systems across community, primary, and hospital settings.
Despite increasing recognition of multidisciplinary care and rapid digitalization of health services, existing literature often examines professional roles or digital tools in isolation, without a unified framework explaining how pharmacists function within digitally enabled multidisciplinary care models across diverse health systems. This narrative review addresses this gap by synthesizing global evidence on multidisciplinary and innovative approaches, with particular emphasis on pharmacist integration and digital health. It examines conceptual foundations, practical models, global case studies, and implementation challenges, aiming to inform resilient and patient-centered healthcare transformation.
Methodology
Design and Rationale
This work adopts a narrative review framework rather than a systematic meta-analysis, appropriate for synthesising diverse conceptual and policy literature. The approach follows the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) guidelines,9 emphasising breadth and interpretative synthesis over quantitative pooling. A narrative review approach was selected because the literature on multidisciplinary and digitally enabled care models is highly heterogeneous, encompassing policy documents, implementation studies, qualitative evaluations, and diverse health-system contexts. This variability precludes meaningful quantitative synthesis or meta-analysis. A narrative framework was therefore considered most appropriate to integrate conceptual, clinical, and policy-level evidence and to provide an interpretative synthesis of evolving practice models.
Data Sources and Search Strategy
Electronic databases—PubMed, Scopus, and Google Scholar—were searched between January 2015 and March 2024 using Boolean combinations of: “multidisciplinary healthcare” OR “interprofessional collaboration” AND “pharmacist” OR “clinical pharmacy” AND “digital health” OR “telepharmacy” OR “artificial intelligence” OR “health informatics”. Grey literature, conference abstracts, and non-peer-reviewed reports were excluded to maintain evidence quality. Manual reference-tracking from key reviews supplemented the search. Relevance during title and abstract screening was defined as explicit discussion of pharmacist roles within multidisciplinary or digitally enabled care models. Articles focusing solely on drug formulation, laboratory pharmacology, or single-profession practice without team-based integration were excluded. Review articles, implementation studies, and policy-relevant publications were prioritized to capture established models and emerging system-level practices.
Eligibility Criteria
Inclusion criteria:
- Articles in English between 2015–2024;
- Described pharmacist participation in team-based or technology-enabled care;
- Reported outcomes, frameworks, or policy perspectives relevant to integration.
Exclusion criteria: editorials, opinion pieces without data, single-case reports, or studies centred solely on drug formulation or non-clinical pharmacology.
Screening and Selection
Two reviewers independently screened titles and abstracts for relevance. Full texts meeting inclusion criteria were analysed thematically. Discrepancies were resolved by consensus. A total of 96 articles were initially identified; 58 met inclusion after full-text screening and were grouped into four analytic domains. Disagreements between reviewers were resolved through discussion and consensus; formal inter-rater reliability statistics were not calculated due to the narrative and interpretative nature of the review.
Data Extraction and Synthesis
Extracted variables included: country/region, healthcare setting, digital tools employed, pharmacist functions, interprofessional team composition, and reported outcomes. Findings were summarised qualitatively under four domains:
- Foundations of multidisciplinary collaboration;
- Models of pharmacist integration;
- Digital enablers and innovations;
- Global and policy perspectives.
The four analytical domains used in this review were developed inductively through iterative full-text review. Initial coding focused on recurring themes related to team structure, professional roles, digital enablers, and system-level context. These themes were progressively refined through comparison across studies and grouped into four overarching domains by consensus among reviewers. Thematic synthesis followed an inductive approach, allowing concepts to emerge from the literature rather than being imposed a priori.
Quality Considerations
Given the narrative nature, formal bias appraisal tools (eg, ROBIS or CASP) were not applied. However, data credibility was ensured by sourcing from peer-reviewed journals indexed in PubMed or Scopus and by cross-referencing recent systematic reviews. Limitations of this approach are discussed in Discussion. Formal quality appraisal tools (eg, ROBIS or CASP) were not applied because the review aimed to map concepts, models, and policy-relevant practices rather than to estimate effect sizes. To minimize bias, only peer-reviewed articles indexed in major databases were included, and findings were triangulated across multiple study designs and settings.
For the purposes of this review, “global models” refer to multidisciplinary and digitally enabled care approaches implemented across both high-income countries and low- and middle-income countries (LMICs), including examples from Europe, North America, Asia, the Middle East, Africa, and Latin America. A PRISMA-ScR checklist and study selection flow diagram are provided in Supplementary file 1 to enhance transparency of the review process.
The Need for Multidisciplinary Approaches
Healthcare today faces increasing complexity due to the rise of chronic non-communicable diseases (NCDs), fragmented delivery systems, escalating costs, and rising patient expectations for holistic and personalized care. Traditional models where professionals operate independently are insufficient to address these demands. In this context, multidisciplinary approaches have emerged as a cornerstone for improving outcomes, enhancing safety, and delivering cost-effective care.
Definition and Principles
Multidisciplinary healthcare integrates structured collaboration among diverse professionals—including physicians, pharmacists, nurses, dietitians, social workers, psychologists, and digital health specialists—who work together to provide comprehensive patient management. Unlike interdisciplinary care, which often overlaps roles, multidisciplinary models emphasize clear role distinctions coupled with active coordination and shared goals (Reeves et al, 2017).2
The core principles guiding these models include:
- Patient-centeredness: prioritizing patient goals and preferences.
- Collaborative communication: fostering transparent, respectful, and consistent information exchange.
- Mutual respect: recognizing the unique expertise of each professional.
- Evidence-based decision-making: relying on guidelines, digital tools, and clinical evidence.
These principles help create cohesive care plans, ensuring that no dimension of patient care is overlooked.
Chronic Disease Burden and Team-Based Care Outcomes
Chronic non-communicable diseases such as diabetes, hypertension, heart failure, and chronic respiratory conditions require long-term, coordinated management involving pharmacological and lifestyle interventions. Evidence consistently shows that multidisciplinary team-based care improves clinical outcomes in these conditions. Meta-analyses and large cohort studies report that pharmacist integration within care teams is associated with significant reductions in glycated hemoglobin (HbA1c), improved blood pressure control, and enhanced medication adherence, alongside fewer medication-related problems and preventable hospital admissions. In heart failure and diabetes care, pharmacist participation has also been linked to reductions in hospital readmissions, highlighting both clinical and economic benefits of coordinated care models.10–12While chronic disease management illustrates the measurable benefits of multidisciplinary collaboration, similar principles are increasingly recognized as essential in mental health care, where transitions between care settings pose substantial safety risks.
Mental Health and Transitions of Care
Mental health conditions frequently coexist with chronic physical illnesses, increasing treatment complexity and vulnerability during transitions of care, such as hospital discharge or transfer between services. Pharmacists play a critical role in psychiatric multidisciplinary teams by conducting medication reconciliation, identifying high-risk drug interactions, monitoring therapies with narrow therapeutic indices (eg, lithium and clozapine), and supporting adherence to long-term psychotropic regimens. In collaborative care and integrated mental health models, pharmacist involvement during care transitions has been associated with improved medication continuity, reduced adverse drug events, and enhanced coordination between primary care and specialist mental health services. These contributions are particularly important in preventing relapse, rehospitalization, and medication-related harm.13–15
Digital Enablers Beyond Electronic Health Records
Digital technologies substantially enhance multidisciplinary collaboration by enabling real-time communication, shared decision-making, and proactive monitoring. Beyond electronic health records, wearable devices and remote monitoring tools allow continuous tracking of physiological parameters such as blood glucose, blood pressure, and heart rhythm, facilitating early multidisciplinary intervention. Digital therapeutics and mobile health applications support behavior change, medication adherence, and symptom monitoring, while telehealth platforms enable pharmacists and other team members to provide follow-up care to underserved or remote populations. Together, these tools extend multidisciplinary care beyond traditional clinical settings and support timely, coordinated responses to patient needs.16
Patient-Centeredness and Experience-Based Outcomes
Patient-centeredness in multidisciplinary care models is operationalized through structured processes that actively involve patients in decision-making, communication, and care planning. Multidisciplinary teams achieve this by jointly developing individualized care plans that incorporate patient goals, preferences, and social context, rather than relying solely on disease-centered protocols.
Pharmacists contribute to patient-centered care by conducting medication reviews focused on patient understanding, adherence barriers, and treatment burden, particularly in individuals with polypharmacy or chronic conditions. Shared medication decision-making—such as discussing therapeutic alternatives, dosing schedules, and potential adverse effects—enables patients to participate meaningfully in their care.
Practical mechanisms also include coordinated follow-up across care settings, where pharmacists support transitions of care through discharge counseling, medication reconciliation, and follow-up calls or teleconsultations. Digital tools such as patient portals, mobile health applications, and remote monitoring platforms further support patient-centeredness by facilitating bidirectional communication, timely feedback, and access to personalized health information.
Together, these practices move multidisciplinary care beyond parallel professional input toward a coordinated model that prioritizes patient engagement, continuity, and shared responsibility for health outcomes.17,18
Challenges and Economic Implications of Multidisciplinary Care
Despite demonstrated benefits, multidisciplinary care is not without challenges. Coordination across multiple professionals can increase communication complexity, blur accountability, and demand additional time and organizational resources. Without clear role delineation, teams may experience inefficiencies or professional friction. From an economic perspective, poorly coordinated care contributes to avoidable hospital readmissions, duplicated services, and medication-related harm, all of which impose significant costs on health systems. It is therefore important to distinguish multidisciplinary care—where professionals contribute distinct expertise within coordinated structures—from transdisciplinary models, which involve deeper role integration and shared responsibilities. Successful implementation of multidisciplinary care requires explicit governance, effective communication frameworks, and supportive digital infrastructure to balance collaboration with efficiency.
Models of Multidisciplinary Integration
The successful implementation of multidisciplinary healthcare requires structured models that integrate diverse professionals into coordinated workflows. These models vary across health systems but share the goal of improving outcomes, enhancing patient safety, and reducing inefficiencies. Pharmacists are increasingly central to these designs, with digital technologies serving as enablers. Multidisciplinary integration may occur through both formal mechanisms, such as legally defined collaborative practice agreements, and informal team-based arrangements based on shared communication and co-location. Distinguishing between these models is essential for understanding differences in governance, sustainability, and clinical authority.
Collaborative Models for Chronic Disease Management
Chronic conditions such as diabetes, hypertension, asthma, and heart failure require lifelong management. Traditional models often fragment care between specialties, leading to duplication, medication errors, and poor adherence. Collaborative models like the Patient-Centered Medical Home (PCMH) and Chronic Care Model (CCM) embed pharmacists in primary care teams. Pharmacists provide services such as medication therapy management (MTM), adherence counseling, and optimization of regimens.
The Asheville Project in the US demonstrated that pharmacist-led interventions in diabetes resulted in sustained HbA1c reduction, improved lipid profiles, and lower healthcare costs (Cranor et al, 2003).19 Similarly, a meta-analysis confirmed that pharmacist-led multidisciplinary interventions reduced systolic blood pressure significantly compared to usual care (Mekonnen et al, 2020).20 These outcomes highlight the value of embedding pharmacists into chronic disease management structures. Such models are more likely to be sustained in health systems where pharmacists’ clinical services are formally reimbursed or integrated into value-based payment structures, underscoring the importance of aligned funding mechanisms for long-term scalability.
Multidisciplinary Integration in Mental Health Care
Mental health care exemplifies the benefits of multidisciplinary integration. Psychiatric conditions frequently overlap with physical illnesses, requiring holistic management. In the Collaborative Care Model (CoCM), a primary care provider, behavioral health manager, and psychiatric consultant work together, often with pharmacist support. Pharmacists contribute by monitoring therapeutic drug levels, preventing interactions, and ensuring adherence (Unützer et al, 2012).21
The Veterans Affairs system in the US introduced the Pharmacist-Led Mental Health Integration (PLMHI) model, where pharmacists independently manage depression and anxiety under collaborative agreements. This approach improved treatment response and patient satisfaction (Bingham et al, 2019).22 Beyond the United States, pharmacist involvement in mental health teams has been reported in Canada, the United Kingdom, and Australia, particularly in medication reconciliation during psychiatric transitions of care, monitoring of psychotropic therapies, and coordination between primary and specialist services.
Digital Enablers of Multidisciplinary Coordination
Technology strengthens integration by bridging gaps across geography and resources. Telepharmacy enables pharmacists to conduct consultations, verify prescriptions, and provide counseling remotely. In rural Australia, telepharmacy reduced medication errors by 45% in small hospitals (Hale et al, 2018).23
Artificial Intelligence (AI) also enhances multidisciplinary practice. IBM Watson, for example, provides oncologists and pharmacists with treatment recommendations based on genetic data and guidelines. Its integration into tumor boards has improved decision-making efficiency and consistency (Somashekhar et al, 2018).24 These digital systems facilitate multidisciplinary coordination by enabling shared access to clinical information, real-time decision support, and structured communication across professional boundaries, thereby reducing fragmentation and improving continuity of care.
Pharmacist-Led Clinics and Collaborative Practice Agreements
Pharmacist-led clinics are another model of integration, particularly in chronic disease and anticoagulation management. Under Collaborative Practice Agreements (CPAs), pharmacists gain authority to adjust therapy, order labs, and manage patient care within defined boundaries. US Veterans Affairs hospitals and Kaiser Permanente have widely adopted this approach. In anticoagulation clinics, pharmacists using point-of-care INR testing optimize warfarin dosing, reducing adverse events and improving outcomes (Witt et al, 2005).25
Globally, similar initiatives are emerging. In Canada, the MedsCheck program authorizes pharmacists to conduct structured medication reviews for chronic patients, reducing adverse drug events and improving adherence. In the UK, Clinical Pharmacists in General Practice are now integral members of National Health Service (NHS) primary care networks. Despite their benefits, pharmacist-led clinics can be resource-intensive, requiring advanced clinical training, access to diagnostic data, and sustained institutional support. Effective leadership of such clinics typically necessitates postgraduate residency training, credentialing, or formal certification, and their scalability is influenced by regulatory frameworks and reimbursement policies.
Multidisciplinary Rounds, Case Conferences and Global Models
In inpatient and specialized outpatient care, structured multidisciplinary rounds or case conferences bring together physicians, pharmacists, nurses, dietitians, and other professionals. Pharmacists’ participation reduces preventable adverse drug events by 66%, shortens hospital stays, and strengthens antimicrobial stewardship (Leape et al, 1999).26 Digital dashboards and AI-generated summaries now enhance these meetings, making them more efficient and data-driven. Comparable multidisciplinary models have been implemented across Asia, Sub-Saharan Africa, and Latin America, often adapted to local workforce capacity and supported by digital tools such as telepharmacy and protocol-driven care pathways. These examples demonstrate that pharmacist integration is feasible across diverse health-system contexts, including low- and middle-income countries.
Innovations in Multidisciplinary Care
Recent innovations in digital health and clinical practice have accelerated multidisciplinary collaboration, enabling pharmacists and other professionals to contribute more effectively to patient-centered, data-driven care.
Artificial Intelligence and Predictive Analytics
Artificial intelligence (AI) has advanced rapidly in healthcare, offering applications in predictive analytics, decision support, and risk stratification. For multidisciplinary teams, AI acts as a cognitive augmentation tool, providing patient-specific recommendations at the point of care.
Pharmacists use AI-driven systems to detect potential drug-drug interactions, identify patients at risk of adverse drug events (ADEs), and optimize dosing strategies. For instance, machine learning models integrated into hospital EHRs can predict conditions such as sepsis, enabling timely multidisciplinary interventions (Sendak et al, 2020).27 In oncology, IBM Watson for Oncology has been used to suggest chemotherapeutic regimens aligned with guidelines and genomic data, with pharmacists validating and refining recommendations (Somashekhar et al, 2018).24 These tools enhance safety, consistency, and efficiency in care delivery. Artificial intelligence (AI)–enabled tools are increasingly embedded in pharmacy and multidisciplinary practice to support medication optimization, risk stratification, and personalized care. Recent post-2023 applications include AI-driven medication therapy management platforms, predictive analytics for adverse drug events, and machine-learning models integrated into electronic prescribing systems to flag high-risk patients in real time. In multidisciplinary settings, these tools assist pharmacists and physicians by synthesizing large datasets, including laboratory values, comorbidities, and medication histories, to support consistent and timely clinical decisions.
Evidence from implementation studies suggests that AI-supported medication review and monitoring can reduce medication errors and improve process efficiency, with some reports indicating improvements in patient satisfaction and perceived quality of care when digital decision support is used as an adjunct to clinical judgment. However, overreliance on AI poses risks, including algorithmic bias, limited explainability of recommendations, and potential erosion of professional accountability. These concerns underscore the importance of maintaining human oversight and embedding AI within multidisciplinary governance structures. However, overreliance on AI poses risks, including algorithmic bias, limited explainability of recommendations, automation bias, and potential erosion of professional accountability. These concerns underscore the importance of maintaining human oversight, transparent algorithms, and multidisciplinary governance structures to ensure ethical and safe AI deployment.
Pharmacogenomics and Personalized Therapy
The emergence of pharmacogenomics has shifted the paradigm from one-size-fits-all to personalized therapy. Genetic variability significantly influences drug metabolism, efficacy, and risk of adverse effects. Pharmacists play a pivotal role in interpreting pharmacogenomic data, recommending adjustments, and counseling patients.
For example, genetic testing for CYP2C9 and VKORC1 variants informs individualized warfarin dosing, reducing risks of bleeding and thromboembolism (Johnson et al, 2017).28 At institutions like St. Jude Children’s Research Hospital, pharmacist-led pharmacogenomics programs integrate genotyping into EHRs, providing real-time clinical alerts for prescribers. These programs have improved outcomes in oncology, infectious disease, and neurology (Caudle et al, 2014).29 Globally, initiatives such as the UK’s 100,000 Genomes Project and emerging programs in Saudi Arabia and the UAE highlight the growing role of pharmacists in implementing genomic medicine.
Health Informatics and Decision Support
Health informatics platforms underpin effective multidisciplinary care by enabling seamless communication and data sharing. Modern EHRs provide shared medication lists, lab results, immunization histories, and documentation of pharmacist interventions. Embedded CDSS modules generate alerts for duplicate therapy, renal dosing adjustments, or high-risk prescribing, helping pharmacists intervene effectively.
Clinical dashboards further support team-based care by providing real-time visualization of patient progress, risk scores, and adherence data. For example, digital prescribing tools reduce medication errors by validating orders before they are dispensed (Campbell et al, 2006).16 In Saudi Arabia, platforms such as Wasfaty and Nafis integrate prescription data and pharmacist interventions at the national level, creating opportunities for population health monitoring and team collaboration.
Despite these advances, technological barriers remain significant. Many health information systems operate on proprietary architectures with limited application programming interfaces (APIs), restricting interoperability and real-time data exchange across institutions. System fragmentation and poor data portability hinder continuity of care when patients transition between settings, reinforcing digital silos rather than enabling true multidisciplinary integration.
Mobile Health Applications (mHealth)
Mobile health (mHealth) technologies empower patients while strengthening connections with care teams. Apps such as Medisafe, MyTherapy, and Sehhaty provide personalized medication reminders, interaction alerts, and adherence tracking. Pharmacists can monitor patient adherence remotely, provide feedback, and deliver counseling through app-linked portals.
Evidence supports the effectiveness of these interventions. A randomized controlled trial found that a pharmacist-supported mHealth app improved blood pressure control and adherence among hypertensive patients (Santo et al, 2019).30 Importantly, mHealth also facilitates integration of patient-generated data such as glucose levels or ECG recordings into team workflows, allowing coordinated adjustments in therapy by physicians, dietitians, and pharmacists.
However, patient engagement with mHealth platforms is influenced by trust in digital systems. Concerns related to data privacy, cybersecurity breaches, and secondary use of personal health information may reduce uptake, particularly among older adults and individuals managing chronic or mental health conditions. Clear communication, informed consent, and visible data protection measures are therefore essential to sustain patient confidence in digitally enabled multidisciplinary care.
Virtual and Augmented Reality in Training
Innovations also extend to workforce development. Virtual reality (VR) and augmented reality (AR) platforms provide immersive environments for interprofessional education (IPE). These simulations allow pharmacy, medical, and nursing students to train together, practicing collaborative protocols in scenarios such as managing anaphylaxis or cardiac arrest. Research demonstrates that VR-based IPE enhances teamwork skills, protocol adherence, and understanding of professional roles (Gaba et al, 2014).31 By fostering role clarity and communication, VR/AR prepares healthcare graduates for real-world multidisciplinary environments.
Challenges in Implementation
While the benefits of multidisciplinary and innovative healthcare are well established, implementation is often hindered by systemic, professional, technological, and cultural barriers. These challenges must be addressed to realize the full potential of integrated models.
Organizational and Structural Barriers
Fragmentation remains a major obstacle. Many health systems are structured around specialty silos, limiting communication and coordination. For instance, hospital pharmacists may lack access to outpatient records, while community pharmacists may remain unaware of recent inpatient decisions. Incomplete referral pathways and weak administrative support undermine continuity of care (Bates et al, 2014).32 Additionally, institutional policies and evaluation metrics often remain discipline-specific, discouraging collaborative practice.
Professional Resistance and Role Ambiguity
Traditional hierarchies can impede integration. Physician-centered models sometimes restrict pharmacists’ contributions, while unclear scopes of practice may leave pharmacists underutilized. Van Cott et al 2016,33 found that pharmacists in hospitals with poorly defined roles contributed less to therapeutic optimization, even when their expertise was recognized. Building mutual trust and fostering interprofessional education are essential for overcoming this resistance.
Reimbursement and Policy Limitations
Another barrier is the lack of reimbursement for pharmacy-led clinical services. In many countries, pharmacists are compensated for dispensing but not for activities such as medication therapy management, counseling, or chronic disease monitoring. This discourages health systems from adopting pharmacist-integrated models, even when evidence shows cost savings through reduced hospitalizations (Wiedenmayer et al, 2006).34 Policy reforms are required to support payment for clinical contributions and collaborative practice agreements.
Technological Challenges and Digital Inequities
Digital platforms underpin modern multidisciplinary care, but technical limitations persist. EHR systems are often non-interoperable, making it difficult for providers to share data across institutions. Cybersecurity and data privacy concerns add further barriers, particularly in international data exchange. At the provider level, digital literacy gaps remain. A survey in the Gulf region found that 37% of pharmacists felt inadequately trained in digital tools, and 42% found existing systems not user-friendly (Almazrou et al, 2020).35 Without interoperable architectures, standardized data formats, and secure data-sharing governance, digital innovation risks increasing workload and fragmentation rather than supporting integrated multidisciplinary workflows.36
Educational Gaps and Workforce Readiness
Healthcare education continues to lag behind practice needs. Many pharmacy curricula remain focused on pharmacology and dispensing, with limited exposure to interprofessional communication, digital health, or clinical informatics. A 2021 FIP global survey found that only 35% of pharmacy programs offered substantial training in informatics or interprofessional education (FIP, 2021).37 This gap reduces workforce readiness for team-based care and must be addressed through curriculum reform.
Cultural and Patient-Level Barriers
Patient perceptions also influence the success of multidisciplinary models. In many settings, pharmacists are still viewed primarily as dispensers, which can limit engagement in clinical services. Patients may also feel overwhelmed by contact with multiple providers, leading to confusion or reduced adherence. Concerns over data privacy and cultural resistance to digital tools may further reduce uptake. Addressing patient concerns requires transparent communication about digital risks and benefits, reassurance regarding confidentiality, and shared decision-making to ensure that technology enhances—rather than replaces—human care relationships.
Global Perspectives and Case Studies
Multidisciplinary and innovative healthcare approaches are not uniform; they reflect the policy environments, resources, and cultural contexts of different countries. Examining international experiences highlights both the adaptability of these models and the universal role of pharmacists and digital tools in their success. Importantly, meaningful pharmacist integration is observed across both high-income countries (HICs) and low- and middle-income countries (LMICs), albeit through context-specific pathways shaped by regulation, workforce capacity, and available technology.
United Kingdom: Pharmacists in Primary Care
The United Kingdom (UK) has pioneered pharmacist integration within primary care. As part of the NHS Long Term Plan, the Clinical Pharmacists in General Practice program was launched to support general practitioners (GPs), optimize medication use, and manage chronic diseases (NHS England, 2019).38 Pharmacists in primary care networks (PCNs) now conduct structured medication reviews, reconcile medicines post-discharge, and manage long-term conditions.
Evaluations by the King’s Fund found that these pharmacists reduced GP workload, improved patient safety, and increased satisfaction (The King’s Fund, 2020).39 The model’s success has been facilitated by shared EHR systems, allowing pharmacists seamless access to patient data. This demonstrates how structural reforms and digital platforms can normalize multidisciplinary practice. However, implementation has required sustained national funding, standardized training pathways, and integration within centralized NHS governance structures, which may limit direct transferability to more fragmented health systems.
Canada: Pharmacist-Led Chronic Disease Programs
Canada has developed strong pharmacist-led initiatives. Ontario’s MedsCheck Program enables pharmacists to conduct comprehensive reviews for patients on chronic medications. These reviews identify drug-related problems, optimize regimens, and improve adherence (Ontario MOH, 2022).40
Another example is Alberta’s RxOUTMAP program, where pharmacists manage conditions such as diabetes and hypertension under collaborative agreements. A randomized trial by Tsuyuki et al 2015,41 showed that pharmacist-led hypertension management improved blood pressure significantly, with 70% of patients reaching target values versus 30% under standard care. Integration is supported by Alberta Netcare, a province-wide EHR, ensuring coordinated communication across providers. Despite positive outcomes, variation in provincial reimbursement policies and scope-of-practice regulations influences the consistency and scalability of pharmacist-led models across Canada.
Saudi Arabia: Digital Health and Vision 2030
Saudi Arabia’s Vision 2030 reform agenda emphasizes digital transformation and workforce expansion, including pharmacist empowerment. National platforms such as Sehhaty, Mawid, and Wasfaty allow patients to access lab results, book appointments, and manage prescriptions digitally. Pharmacists use Wasfaty to monitor adherence, document interventions, and improve continuity of care.
Clinical pharmacists are increasingly integrated into chronic disease clinics and antimicrobial stewardship programs. Alruthia et al 2020,42 reported that pharmacy graduates in Saudi Arabia anticipate expanded roles in line with Vision 2030 reforms. Telepharmacy is also being implemented in rural areas, ensuring equitable access to pharmaceutical care. Saudi Arabia represents a transitional context, illustrating how middle-income countries can leverage national digital platforms and policy reform to accelerate multidisciplinary integration at scale.
Australia: Community Pharmacy and Technology Integration
Australia’s Community Pharmacy Agreements provide government support for pharmacy-led services such as home medicines reviews (HMRs), smoking cessation, and chronic disease follow-up. The integration of digital platforms such as GuildCare and MedAdvisor enhances collaboration by enabling pharmacists to monitor adherence, send reminders, and share data with prescribers (Australian Government, 2020).43
Taylor et al 2020,44 demonstrated that pharmacist-led models improved chronic disease outcomes in Indigenous populations, particularly through culturally adapted education and follow-up. Telehealth further extends access in rural and underserved areas, highlighting the scalability of multidisciplinary models in diverse contexts. Community engagement, culturally sensitive communication, and trust-building within Indigenous health services have been critical facilitators of pharmacist integration in these settings.
United States: Collaborative Practice Agreements
The US healthcare system, while fragmented, has implemented Collaborative Practice Agreements (CPAs) to expand pharmacists’ roles. Under CPAs, pharmacists can initiate or adjust therapies, order labs, and provide disease management. In Veterans Affairs (VA) hospitals and Kaiser Permanente networks, pharmacists independently manage conditions such as hypertension, anticoagulation, and HIV.
A VA study reported that pharmacist-led anticoagulation clinics achieved therapeutic INR levels in over 70% of patients, reducing stroke and bleeding risks (Carter et al, 2006).45 Integration is supported by advanced informatics platforms such as Epic and Cerner, which enable real-time communication and clinical decision support across teams.
Low- and Middle-Income Countries (LMICs)
In LMICs, resource constraints necessitate creative adaptations. In South Africa, community health workers, nurses, and pharmacists collaborate in antiretroviral therapy (ART) programs. Decentralized pharmacy pick-up points, mobile adherence apps, and community-based counseling have improved retention and viral suppression rates (Fox et al, 2018).46
In India, pilot projects have trained pharmacists in NCD screening and monitoring. Combined with telemedicine and mobile data collection, these programs improved diagnosis and treatment initiation in underserved populations (Mahapatra et al, 2020).47 Similar adaptations have been reported in parts of Latin America, including Brazil and Chile, where pharmacists support chronic disease management and public health initiatives through protocol-driven care and digital reporting systems within resource-constrained environments. While scalability remains a challenge, these cases show that pharmacist-led, digitally supported models are adaptable even in low-resource settings.
Across countries, several common lessons emerge:
- Policy support is crucial: Pharmacist integration thrives when supported by legislation and reimbursement.
- Digital platforms enable continuity: Shared records and mobile tools are essential for communication and monitoring.
- Cultural adaptation enhances success: Tailoring interventions to local contexts, such as Indigenous health in Australia or ART in South Africa, increases effectiveness.
- Scalability depends on resources: While high-income countries can implement advanced informatics, LMICs demonstrate that low-cost, technology-enabled solutions can also be impactful.
Comparative Synthesis and Lessons Learned
Across countries, several common lessons emerge. Policy and regulatory support are critical for legitimizing pharmacists’ clinical roles and enabling reimbursement. Digital platforms—whether advanced national EHRs in HICs or mobile-based tools in LMICs—consistently enhance continuity and coordination of care. Cultural adaptation, community engagement, and trust-building emerge as key facilitators of success, particularly in Indigenous and community-based models. Finally, while HICs benefit from advanced informatics and stable funding, LMICs demonstrate that low-cost, digitally supported pharmacist integration can achieve meaningful impact when aligned with local needs and workforce capacity. Table 1 provides a consolidated summary of the multidisciplinary and digitally enabled care models identified in this review, organized according to the four analytical domains.
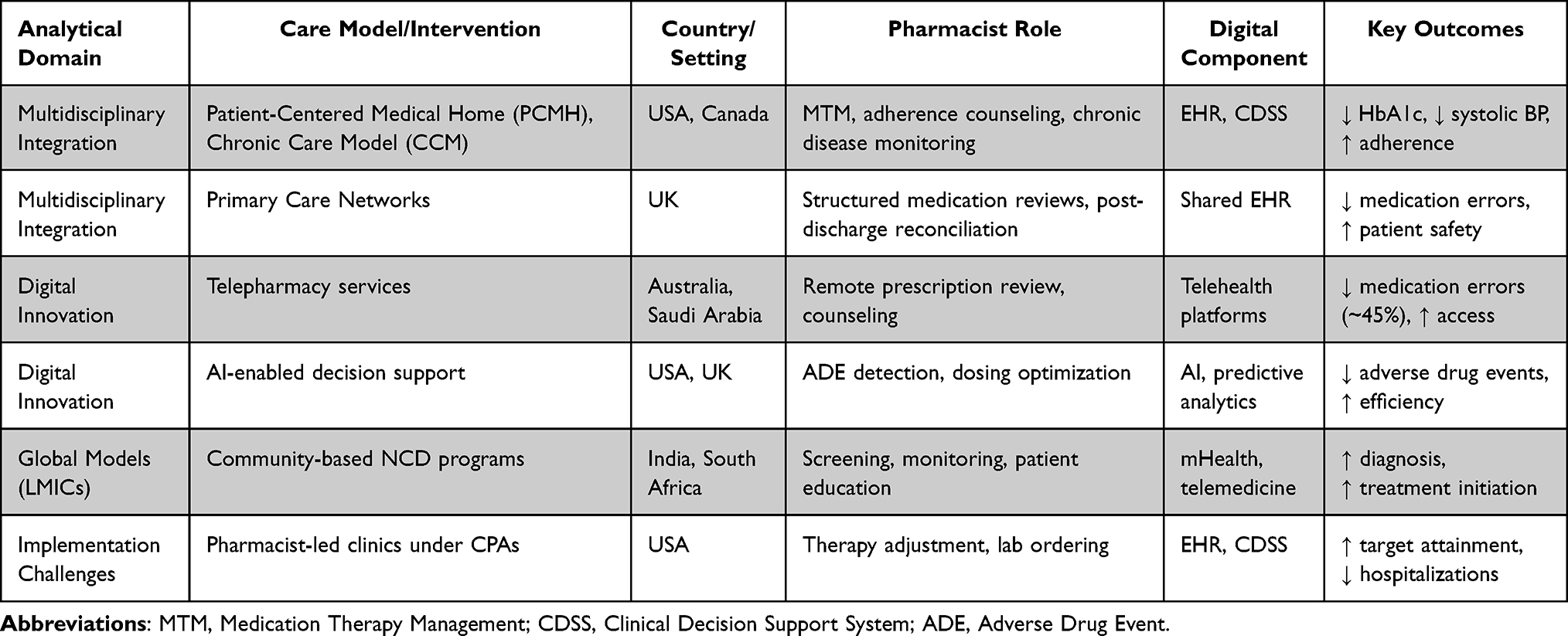 |
Table 1 Summary of Multidisciplinary and Digitally Enabled Care Models Across the Four Analytical Domains |
Discussion
Multidisciplinary Integration and Clinical Impact
This narrative review synthesised recent global evidence underscoring the pharmacist’s expanding role in multidisciplinary, technology-enabled healthcare. Across diverse systems, pharmacist-integrated models consistently improve medication safety, chronic-disease control, and patient satisfaction. Their inclusion translates pharmacological expertise into collaborative decision-making that bridges diagnostic, behavioural, and technological dimensions of care.48 Unlike prior reviews that examined pharmacist services in isolation, this review integrates multidisciplinary structures with digital transformation, offering a more holistic understanding of how pharmacists function within complex care ecosystems. While these benefits are consistently observed across settings, their magnitude and sustainability remain context-specific, influenced by regulatory frameworks, workforce capacity, and digital infrastructure.
Digital Transformation and Emerging Evidence
Compared with earlier literature that focused primarily on clinical outcomes,3 recent studies (2020–2024) reveal how digital infrastructure amplifies pharmacists’ impact. Electronic prescribing, interoperable records, and AI-supported decision systems elevate visibility and efficiency.49 For instance, pharmacists embedded in digitally connected teams intervene earlier on potential drug–drug interactions and ensure continuous adherence monitoring through telehealth platforms.50 These findings align with recent narrative reviews and meta-analyses reporting improved medication safety and workflow efficiency through digital integration, while also highlighting emerging concerns such as technology fatigue, alert overload, and variable system usability. Such limitations underscore that digital tools must augment—rather than burden—multidisciplinary practice.
Global Variation, Policy, and Implementation Gaps
The discussion also exposes variation in implementation. In high-income countries, structural enablers—legislation, reimbursement for cognitive services, and integrated informatics—support pharmacist autonomy.51 Conversely, in low- and middle-income contexts, resource limitations hinder data access and interprofessional coordination.52 Nonetheless, community-based telepharmacy initiatives in India, South Africa, and Saudi Arabia demonstrate that scalable, low-cost digital solutions can compensate for infrastructure gaps.53 Persistent gaps remain regarding optimal scope of pharmacist authority, reimbursement mechanisms, and the extent to which digital tools can substitute for workforce shortages. These findings suggest that policy reforms must be explicitly aligned with practice-level realities, particularly in LMICs, to ensure that multidisciplinary integration translates into equitable and sustainable health gains.
Education, Ethics, and Workforce Readiness
From an educational standpoint, interprofessional education (IPE) remains pivotal. Studies show that students trained through simulation-based multidisciplinary exercises demonstrate improved teamwork scores and clearer role perception.54 Embedding IPE across curricula thus ensures workforce readiness for integrated digital care. Institutions such as St. Jude Children’s Research Hospital, the University of Toronto, and several Australian universities have implemented structured interprofessional and digital health training pathways, illustrating how curricular reform can support future-ready multidisciplinary practice. The increasing reliance on AI in pharmacist-led decision-making also raises ethical considerations, including accountability for automated recommendations, transparency of algorithms, and the risk of bias affecting vulnerable populations. Addressing these concerns requires ethical governance frameworks and continued emphasis on professional judgment within multidisciplinary teams.
Toward a Unifying Framework for Multidisciplinary Digital Care
Collectively, the findings support a theory of change in which pharmacist integration acts as a central mechanism linking multidisciplinary collaboration, digital enablement, and patient-centered outcomes. Policy support and education reform function as enabling inputs, digital tools serve as amplifiers, and coordinated team-based practice produces sustained improvements in safety, efficiency, and care quality.
Overall, pharmacists emerge as both clinical and digital connectors within the evolving care ecosystem. Their success depends on policies recognising their clinical authority, technological literacy, and capacity to interpret complex pharmacogenomic and real-world data.
Limitations
This review employed a narrative rather than systematic methodology. Although guided by PRISMA-ScR principles, the absence of quantitative meta-analysis limits generalisability. A systematic review was not considered feasible due to the conceptual heterogeneity of multidisciplinary care models, wide variation in study designs, outcome measures, and contextual implementation settings, which precluded meaningful quantitative synthesis. Potential publication bias may overrepresent studies reporting positive pharmacist or digital-health outcomes.55 In addition, selection bias may have arisen from preferential inclusion of studies describing successful or well-resourced implementation models. The review was limited to English-language peer-reviewed publications, which may have excluded relevant models reported in other languages or regional sources. Future reviews could address these limitations by incorporating multilingual searches, inclusion of grey literature, standardized outcome frameworks, and mixed-methods synthesis approaches. Finally, heterogeneous outcome measures across studies prevented pooled effect estimation. Despite these limitations, triangulation across multiple data sources supports confidence in the main conclusions.
Future Directions
To institutionalise pharmacist-centred multidisciplinary care, future efforts should prioritise the following:
- Policy and Regulation: Governments must codify pharmacists’ prescribing and monitoring authority through collaborative-practice legislation and reimbursement frameworks.56
- Digital Infrastructure: Investment in interoperable EHRs, AI-driven analytics, and secure telehealth platforms will enable real-time collaboration and equitable access.57,58
- Benchmarking Initatitives: Establishing global benchmarking initiatives to track digital pharmacy transformation would allow comparison of implementation maturity, outcomes, and workforce integration across countries.
- Education and Competency Building: Pharmacy curricula should embed interprofessional and informatics competencies, including data analytics, pharmacogenomics, and virtual-simulation training.8
- Research and Evaluation: Multi-country comparative studies are needed to quantify the economic and clinical return on pharmacist-integrated digital models.59 Future research should adopt standardized outcome metrics—such as medication safety indicators, readmission rates, and patient-reported outcomes—and consider the development of international registries to systematically capture pharmacist-led interventions and their impact.
- Patient Engagement and Equity: Programs must promote patient literacy in digital-health tools and prioritise inclusion of rural, elderly, and socio-economically disadvantaged populations.60
Conclusion
The growing complexity of modern healthcare demands a shift away from siloed practice toward multidisciplinary, digitally enabled models of care. Multidisciplinary approaches, where professionals contribute distinct expertise in coordinated teams offer a pathway to better outcomes, enhanced safety, and more sustainable healthcare systems. At the center of these models is the evolving role of pharmacists. Once limited to dispensing, pharmacists now contribute to chronic disease management, medication safety, pharmacogenomics, and patient education. When integrated into multidisciplinary teams, pharmacists reduce medication errors, improve adherence and chronic-disease control, support safer transitions of care, and enhance patient engagement. Simultaneously, digital health innovations such as EHRs, decision support systems, telemedicine, and mobile health applications have become indispensable enablers of collaboration. These tools foster continuity, reduce duplication, and empower both providers and patients. Emerging technologies, including artificial intelligence and virtual reality, further enhance decision-making and workforce readiness.
Despite the clear benefits, challenges remain. Structural fragmentation, professional hierarchies, insufficient reimbursement, digital inequities, and educational gaps hinder widespread adoption. Addressing these barriers requires systemic reforms in policy, infrastructure, and workforce training.
Global experiences from pharmacist integration in UK primary care to digital platforms in Saudi Arabia and pharmacist-led hypertension programs in Canada—demonstrate that multidisciplinary models can be tailored to diverse settings, including resource-limited environments.
In summary, this review highlights four interconnected domains—multidisciplinary integration, digital innovation, implementation challenges, and global contextual adaptation—that together define the future of pharmacist-led collaborative care. Advancing this agenda will require:
- Institutionalising team-based practice models,
- Expanding pharmacists’ clinical scope through supportive policy,
- Strengthening interoperable digital infrastructure,
- Embedding interprofessional and digital competencies across health professions education.
By aligning policy, practice, technology, and education, healthcare systems can evolve toward more resilient, equitable, and patient-centered care models capable of meeting 21st-century health challenges.
Use of Generative Artificial Intelligence (AI)
The author acknowledges that ChatGPT (OpenAI, GPT-5, 2025 version) was used solely to enhance the clarity and fluency of language during manuscript preparation. The tool was not used to generate scientific content, data interpretation, or references. All intellectual and analytical inputs, interpretations, and conclusions are entirely the author’s own.
Ethics
This study is a narrative review and did not involve human participants, animals, or clinical data; ethical approval and informed consent were not required.
Acknowledgments
The authors thank colleagues at the College of Pharmacy, King Khalid University, for their support during manuscript preparation.
Funding
The authors extend their appreciation to the Deanship of Research and Graduate Studies at King Khalid University for funding this work through Large Research Project under grant number RGP2/443/46.
Disclosure
The authors declare no conflicts of interest related to this work.
References
1. World Health Organization. Framework for Action on Interprofessional Education & Collaborative Practice. Geneva: WHO; 2010.
2. Reeves S, Pelone F, Harrison R, Goldman J, Zwarenstein M. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2017;6. doi:10.1002/14651858.CD000072.pub3
3. Bond CA, Raehl CL. Clinical pharmacy services, pharmacy staffing, and hospital mortality rates. Pharmacotherapy. 2007;27(4):481–16. doi:10.1592/phco.27.4.481
4. Relling MV, Evans WE. Pharmacogenomics in the clinic. Nature. 2015;526(7573):343–350. doi:10.1038/nature15817
5. Bates DW, Bitton A. The future of health information technology in the patient-centered medical home. Health Affairs. 2018;29(4):614–621. doi:10.1377/hlthaff.2010.0007
6. WHO. (2021). Noncommunicable diseases fact sheet. Available from https://www.who.int.
7. Cadogan CA, Hughes CM. On the frontline against COVID-19: community pharmacists’ contribution during a public health crisis. Res Social Administrative Pharm. 2021;17(1):2032–2035. doi:10.1016/j.sapharm.2020.03.015
8. Institute of Medicine. Measuring the Impact of Interprofessional Education on Collaborative Practice and Patient Outcomes. Washington, DC: National Academies Press; 2015.
9. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Internal Med. 2018;169(7):467–473. doi:10.7326/M18-0850
10. American Diabetes Association. Standards of medical care in diabetes—2022. Diabetes Care. 2022;45(Supplement_1):S1–S2. doi:10.2337/dc22-Sint
11. Chisholm-Burns MA, Kim Lee J, Spivey CA, et al. US pharmacists’ effect as team members on patient care: systematic review and meta-analyses. Med Care. 2010;48(10):923–933. doi:10.1097/MLR.0b013e3181e57962
12. Mekonnen AB, McLachlan AJ, Brien JA. Effectiveness of pharmacist-led medication reconciliation programmes on clinical outcomes at hospital transitions: a systematic review and meta-analysis. BMJ Open. 2016;6:e010003. doi:10.1136/bmjopen-2015-010003
13. Finley PR, Crismon ML, Rush AJ. Evaluating the impact of pharmacists in mental health: a systematic review. Pharmacotherapy. 2003;23(12):1634–1644. doi:10.1592/phco.23.15.1634.31952
14. Archer J, Bower P, Gilbody S, et al. Collaborative care for depression and anxiety problems. Cochrane Database Syst Rev. 2012;10. doi:10.1002/14651858.CD006525.pub2
15. Bell JS, Rosen A, Aslani P, Whitehead P, Chen TF. Developing the role of pharmacists as members of community mental health teams: perspectives of pharmacists and mental health professionals. Aust N Z J Psychiatry. 2014;48(8):727–736.
16. Campbell F, Corcoran K, Livinski A. The effectiveness of clinical decision support systems in improving medication safety. Ann Internal Med. 2006;144(7):510–520. doi:10.7326/0003-4819-144-7-200604040-00010
17. Zwarenstein M, Goldman J, Reeves S. Interprofessional collaboration: effects of practice-based interventions on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2009;3.
18. Koshman SL, Charrois TL, Simpson SH, McAlister FA, Tsuyuki RT. Pharmacist care of patients with heart failure. Archiv Inter Med. 2008;168(7):687–694. doi:10.1001/archinte.168.7.687
19. Cranor CW, Bunting BA, Christensen DB. The asheville project: long-term clinical and economic outcomes of a community pharmacy diabetes care program. J Am Pharm Assoc. 2003;43(2):173–184.
20. Mekonnen AB, McLachlan AJ, Brien JA. Effectiveness of pharmacist-led medication reconciliation programs on clinical outcomes at hospital transitions: a systematic review and meta-analysis. BMJ Open. 2020;6(2):e010003.
21. Unützer J, Harbin H, Schoenbaum M, Druss B. The Collaborative Care Model: An Approach for Integrating Physical and Mental Health Care in Medicaid Health Homes. Health Home Information Resource Center; 2013.
22. Bingham JM, Axon DR, Scovis NA, et al. Integrating clinical pharmacists into mental health care teams: a review of models and evidence. Mental Health Clinician. 2019;9(5):255–263.
23. Hale M, Coombes I, Stokes J. The impact of telepharmacy services on medication safety in rural Australian hospitals. Aust Health Rev. 2018;42(4):415–421.
24. Somashekhar SP, Sepúlveda MJ, Puglielli S, Norden AD, Shortliffe EH, Rohit Kumar C. Watson for oncology and breast cancer treatment recommendations: agreement with an expert multidisciplinary tumor board. Ann Oncol. 2018;29(2):418–423. doi:10.1093/annonc/mdx781
25. Witt DM, Sadler MA, Shanahan RL, Mazzoli G, Tillman DJ. Effect of a centralized clinical pharmacy anticoagulation service on the outcomes of anticoagulation therapy. Chest. 2005;127(5):1515–1522. doi:10.1378/chest.127.5.1515
26. Leape LL, Cullen DJ, Clapp MD, et al. Pharmacist participation on physician rounds and adverse drug events in the intensive care unit. JAMA. 1999;282(3):267–270. doi:10.1001/jama.282.3.267
27. Sendak MP, D’Arcy J, Kashyap S, et al. A path for translation of machine learning products into healthcare delivery. EMJ Innovations. 2020;4(1):21–27.
28. Li YC, Kavalali ET. Synaptic vesicle-recycling machinery components as potential therapeutic targets. Pharmacol Rev. 2017;69(2):141–158. doi:10.1124/pr.116.013342
29. Caudle KE, Klein TE, Hoffman JM, et al. Incorporation of pharmacogenomics into routine clinical practice: the Clinical Pharmacogenetics Implementation Consortium (CPIC). Clin Pharmacol Ther. 2014;95(4):394–397. doi:10.1038/clpt.2013.226
30. Santo K, Richtering SS, Chalmers J, et al. Mobile phone apps to improve medication adherence: a systematic review and meta-analysis. J Med Internet Res. 2019;21(1):e13263. doi:10.2196/13263
31. Gaba DM, Howard SK, Fish KJ, Smith BE, Sowb YA. Simulation-based training in anesthesia crisis resource management (ACRM): a decade of experience. Simulation Gaming. 2014;40(3):338–352.
32. Bates DW, Saria S, Ohno-Machado L, et al. Big data in health care: using analytics to identify and manage high-risk and high-cost patients. Health Affairs. 2014;33(7):1123–1131. doi:10.1377/hlthaff.2014.0041
33. Van Cott ME, Dombrowski DA, Stolpe SF. Identifying barriers to clinical pharmacy services: a mixed-methods study. Am J Health-Syst Pharm. 2016;73(20):1624–1631.
34. Wiedenmayer K, Summers RS, Mackie CA, Gous AGS, Everard M, Tromp D. Developing Pharmacy Practice: A Focus on Patient Care. World Health Organization; 2006.
35. Almazrou S, Alfaifi M, Alsubaie N, et al. Exploring the readiness and challenges of digital health implementation in Saudi pharmacy practice: a national survey. Saudi Pharm J. 2020;28(9):1114–1120.
36. Adler-Milstein J, Pfeifer E. Information blocking: is it occurring and what policy strategies can address it? Health Aff. 2017;36(3):438–445.
37. FIP. (2021). Pharmacy education in a digital age: FIP global education report. The Hague: International Pharmaceutical Federation.
38. NHS England. (2019). Clinical pharmacists in general practice. Available from https://www.england.nhs.uk.
39. The King’s Fund. Evaluation of Clinical Pharmacists in Primary Care. London, UK; 2020.
40. Ontario Ministry of Health. MedsCheck Program Guidelines. Government of Ontario; 2022.
41. Tsuyuki RT, Houle SK, Charrois TL, et al. Pharmacist intervention for hypertension control: a randomized controlled trial. Hypertension. 2015;66(5):968–975.
42. Alruthia Y, Alhawassi TM, Almalag HM, et al. Future roles of pharmacists in the Saudi vision 2030: perspectives of pharmacy students and recent graduates. Saudi Pharm J. 2020;28(4):484–490.
43. Australian Government Department of Health. Sixth Community Pharmacy Agreement (6CPA); 2020.
44. Taylor AJ, Thompson SC, Smith JS, et al. Chronic disease management in indigenous Australians: evaluation of a pharmacist-led model. BMC Health Serv Res. 2020;20(1):1–9.
45. Carter BL, Ardery G, Dawson JD, et al. Physician and pharmacist collaboration to improve blood pressure control. Archiv Inter Med. 2006;166(9):967–973.
46. Fox MP, Pascoe SJ, Huber AN, et al. Decentralizing HIV care: lessons from South Africa. Tropical Med Int Health. 2018;23(3):303–310.
47. Mahapatra P, Golechha M, Tripathy JP. Expanding the pharmacist’s role in primary healthcare in India. BMJ Global Health. 2020;5(3):e002188.
48. Pelone F, Harrison R, Goldman J, Zwarenstein M, Zwarenstein M. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2017;6(6).
49. Bates DW, Bitton A. The future of health information technology in the patient-centered medical home. Health Affairs. 2010;29(4):614–621.
50. Al Meslamani AZ. Gaps in digital health policies: an insight into the current landscape. J Med Economic. 2023;26(1):1266–1268. doi:10.1080/13696998.2023.2266955
51. McRae M, Taylor SJ, Swain L, Sheldrake C. Evaluation of a pharmacist-led, medicines education program for aboriginal health workers. Rural Remote Health. 2008;8(4):1–8.
52. Ossomba JP, Ngangue P, Ekani AS, Kamgain ET. De-medicalized and decentralized HIV testing: a strategy to test hard-to-reach men who have sex with men in Cameroon. Front Public Health. 2023;11:1180813. doi:10.3389/fpubh.2023.1180813
53. Choudhary RP, Siddalingegowda SM. Exploring the need and potential of ambulatory pharmacy practice for empowering patient and care delivery in India. Front Health Service. 2024;4:1399621. doi:10.3389/frhs.2024.1399621
54. Lateef F. Simulation-based learning: just like the real thing. J Emerg Trauma Shock. 2010;3(4):348–352. doi:10.4103/0974-2700.70743
55. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between review types. BMC Med Res Method. 2023;23(1):58. doi:10.1186/s12874-023-01873-0
56. FIP. FIP development goals report: the transforming role of pharmacy. International Pharmaceutical Federation. 2021.
57. Goundrey-Smith S. Principles of Health Interoperability. Springer; 2018.
58. Ahmed NJ, Almalki ZS, Alsawadi AH, et al. Knowledge, perceptions, and readiness of telepharmacy among community pharmacists. Saudi Pharm J. 31(9):101713.
59. Alvarez-Rosete A, Baines D, Waring J, Ashcroft DM. Digital transformation in pharmacy practice: a scoping review of economic and clinical outcomes. Res Social Administrative Pharm. 2023;19(8):1234–1246.
60. Koonin LM, Hoots B, Tsang CA, et al. Trends in patient access, digital literacy, and telehealth equity post-COVID-19: global lessons for inclusive digital health. Front Public Health. 2024;12:1365048.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Weight Reduction Interventions Using Digital Health for Employees with Obesity: A Systematic Review
Lee Y, Lee NY, Lim HJ, Sung S
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3121-3131
Published Date: 13 October 2022
Genotyping of Patients with Adverse Drug Reaction or Therapy Failure: Database Analysis of a Pharmacogenetics Case Series Study
Bollinger A, Stäuble CK, Jeiziner C, Wiss FM, Hersberger KE, Lampert ML, Meyer zu Schwabedissen HE, Allemann SS
Pharmacogenomics and Personalized Medicine 2023, 16:693-706
Published Date: 3 July 2023
Economic Evaluation of Remote Monitoring for Implantable Cardiac Devices: Evidence from a Remote-Care Study
Bae H, Hwang Y
ClinicoEconomics and Outcomes Research 2024, 16:697-705
Published Date: 23 September 2024
Identifying Current Practices and Areas for Improvement in Medication Management During Care Transition Through an Interprofessional Collaboration Framework
Solh Dost L, Maillard G, Cardoso E, Schneider MP
Journal of Multidisciplinary Healthcare 2025, 18:4453-4467
Published Date: 30 July 2025