")
Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 16
Genotyping of Patients with Adverse Drug Reaction or Therapy Failure: Database Analysis of a Pharmacogenetics Case Series Study
Authors Bollinger A , Stäuble CK , Jeiziner C , Wiss FM , Hersberger KE , Lampert ML, Meyer zu Schwabedissen HE, Allemann SS
Received 31 March 2023
Accepted for publication 19 June 2023
Published 3 July 2023 Volume 2023:16 Pages 693—706
DOI https://doi.org/10.2147/PGPM.S415259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Anna Bollinger,1 Céline K Stäuble,1,2 Chiara Jeiziner,1 Florine M Wiss,1,2 Kurt E Hersberger,1 Markus L Lampert,1,2 Henriette E Meyer zu Schwabedissen,1 Samuel S Allemann1
1Department of Pharmaceutical Sciences, University of Basel, Basel, Switzerland; 2Institute of Hospital Pharmacy, Solothurner Spitäler AG, Olten, Switzerland
Correspondence: Anna Bollinger, Department of Pharmaceutical Sciences, University of Basel, Klingelbergstrasse 50, Basel, 4056, Switzerland, Tel +41 61 207 66 31, Email [email protected]
Purpose: Pharmacogenetics (PGx) is an emerging aspect of personalized medicine with the potential to increase efficacy and safety of pharmacotherapy. However, PGx testing is still not routinely integrated into clinical practice. We conducted an observational case series study where PGx information from a commercially available panel test covering 30 genes was integrated into medication reviews. The aim of the study was to identify the drugs that are most frequently object of drug-gene-interactions (DGI) in the study population.
Patients and Methods: In out-patient and in-patient settings, we recruited 142 patients experiencing adverse drug reaction (ADR) and/or therapy failure (TF). Collected anonymized data from the individual patient was harmonized and transferred to a structured database.
Results: The majority of the patients had a main diagnosis of a mental or behavioral disorder (ICD-10: F, 61%), of musculoskeletal system and connective tissue diseases (ICD-10: M, 21%), and of the circulatory system (ICD-10: I, 11%). The number of prescribed medicines reached a median of 7 per person, resulting in a majority of patients with polypharmacy (≥ 5 prescribed medicines, 65%). In total, 559 suspected DGI were identified in 142 patients. After genetic testing, an association with at least one genetic variation was confirmed for 324 suspected DGI (58%) caused by 64 different drugs and 21 different genes in 141 patients. After 6 months, PGx-based medication adjustments were recorded for 62% of the study population, whereby differences were identified in subgroups.
Conclusion: The data analysis from this study provides valuable insights for the main focus of further research in the context of PGx. The results indicate that most of the selected patients in our sample represent suitable target groups for PGx panel testing in clinical practice, notably those taking drugs for mental or behavioral disorder, circulatory diseases, immunological diseases, pain-related diseases, and patients experiencing polypharmacy.
Keywords: pharmacogenomics, PGx, personalized medicine, clinical pharmacy, clinical practice, medication review
Introduction
In the era of personalized medicine, the importance of a tailored, individualized pharmacotherapy is constantly increasing and is replacing the approach of “one size fits all”.1
An adequately dosed drug therapy can lead to the desired effect in some patients, while other patients do not respond (therapy failure, TF) or even experience unwanted drug effects (adverse drug reaction, ADR). This interindividual difference in drug response is influenced by several factors.2,3 A distinction can be made between exogenous factors, eg, medication adherence, drug-food-interactions (DFI), drug-drug-interactions (DDI), and endogenous factors, eg, comorbidities, organ functions, or genetics.
Literature and guidelines for medicine optimization and improvement of patient outcomes suggest that these exogenous and endogenous factors need to be comprehensively considered in clinical practice. However, the incorporation of genetic factors is nowhere explicitly mentioned.4–6
The application of individual genetic information in the context of drug therapy is described by the term of pharmacogenetics (PGx).7 PGx can increase efficacy and safety of pharmacotherapy and should therefore be an integral part of clinical pharmacy.2 Increasingly, pharmaceutical companies indicate on drug labels that certain genetic variations affect serum levels and the likelihood of ADRs and/or TF.8,9 Yet, integration of PGx in clinical practice, both in the in- and out-patient setting, is still limited. Potential reasons that PGx has not been fully adopted in practice include the lack of reimbursement for PGx testing, the costs associated with counseling, limited clinical evidence, and a knowledge gap about the appropriate use of PGx information for treatment decisions in specific patient populations.10–13
To achieve a better understanding of the optimal application of PGx information in clinical practice, a PGx case series study (Clinical Trials.gov ID: NCT04154553) was established in 2019 in Swiss primary and secondary care settings.
Hereby, patients experiencing ADR or TF under a certain drug therapy were pharmacogenotyped. The PGx test information was interpreted not only reactively to the patient’s susceptibility to ADR or TF, but also preemptively to provide recommendations for future treatment decisions, which were subsequently included into a medication review report, individualized for each patient. The used PGx panel test covered 100 pharmacologically relevant genetic variants in 30 different genes. Those genes encode enzymes, receptors, and transporters, known to be involved in pharmacokinetics (PK) and pharmacodynamics (PD).7
This study was designed to compile case reports to acquire experience with the application of PGx in Swiss primary and secondary care as a basis for the implementation of a standard of procedure. After three years of collecting those patient cases and publishing selected individual case reports,14–19 we aimed to perform a database analysis of all gathered data of the study population.
The main objective of the database analysis was to identify patient groups which may benefit from a PGx analysis with subsequent optimization of their pharmacotherapy. For this reason, we aimed to identify the drugs and the genes that are most frequently associated with drug-gene-interactions (DGI) in the heterogeneous study population. If possible, we also aimed to assess further factors potentially influencing interindividual drug response (eg, DDI) within the review process of patients’ medication. Next to the analysis of the total study population, we aimed to perform an exploratory subgroup analysis to compare identified differences and similarities within selected patient groups of the study. In addition, we wanted to determine patients’ medication adjustments six months after providing the analysis results, to assess how PGx-based recommendations had been implemented in clinical practice.
Materials and Methods
Study Population and Procedure
The herein analyzed data set was collected between 2019 and 2021 within the case series study “pharmacogenetic testing of patients with unwanted adverse drug reactions or therapy failure” (Clinical Trials.gov ID: NCT04154553). The study population consists of adult patients that experienced ADR or TF under an ongoing or previous pharmacotherapy (reactive test). In addition, patients were included in whom future use of a new drug, known to be affected by genetic variants in drug metabolism (PK) and/or drug target structure (PD) genes, was planned (preemptive test). Also, patients with known family history regarding ADR or TF, probably linked to drugs with potential PGx association, were accepted for study inclusion.
The study procedures are described in detail elsewhere20 and are illustrated in Figure 1.
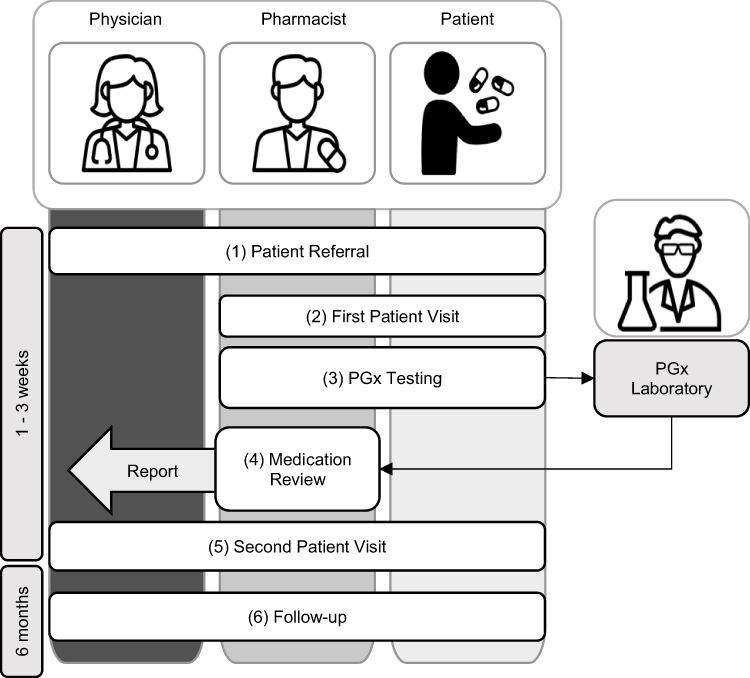 |
Figure 1 Overview about the 6-steps study procedure of the pharmacogenetics (PGx) case series. Adapted from Stäuble CK, Jeiziner C, Bollinger A et al. A Guide to a Pharmacist-Led Pharmacogenetic Testing and Counselling Service in an Interprofessional Healthcare Setting. Pharmacy. 2022;10(4):86. Creative Commons.20 Abbreviations: PGx, pharmacogenetics; DGI, drug-gene-interaction; DDI, drug-drug-interaction. Notes: Step 1 – Patient referral: Patients are selected by physicians (general physician or medical specialist) and referred to the appropriate participating study pharmacy (ambulatory setting or hospital setting). Step 2 – First patient visit: After patients have given their written informed consent, further necessary data is collected (eg, the medication history, self-medication data, family history). A buccal swab as well as blood samples are collected. Step 3 – PGx analysis: The buccal swab sample is shipped to the commercial provider Stratipharm® (humatrix AG, Pfungstadt, Germany), where the PGx panel test is conducted. Additional genetic variants are tested with the blood samples in the Biopharmacy Laboratory of the University of Basel. Step 4 – Medication review: The PGx test results (available after 1–3 weeks) are evaluated, in particular in context of the previously suspected drugs, for potential DGI. A medication review including PGx information is conducted. If available, other factors like DDI, adherence or comorbidities are considered. Step 5 – Second Patient visit: PGx testing results and compiled recommendations for medication optimization are explained to the patient. A written report is forwarded to the treating physicians. Step 6 – Follow-up: After 6 months, a follow-up interview is conducted via telephone to assess the implementation of medication changes based on PGx information. |
Briefly, the study started with the patient referral. Suitable patients were selected by their physicians (general physician or medical specialist) and referred to a study pharmacy. With the referral form, the study pharmacist received the required patient data (eg, gender, age, medication list, medical reports) and the information of the main diagnosis. The term “main diagnosis” is herein defined as principal disease for which the patient was visiting the physician, which referred the patient for study participation (eg, psychiatrist referred a patient with major depressive disorder due to ADR suspicion potentially caused by escitalopram. Although the patient was additionally taking co-medication for treating other diseases, such as arterial hypertension and type-two diabetes mellitus, the main diagnosis for referral was indicated as major depressive disorder). Based on the patient data, the study pharmacist verified the inclusion criteria and contacted the patient for an appointment.
Afterwards, the first patient visit took place in the study pharmacy. After the patient had provided informed consent, the study pharmacists collected further data such as the medication history, the self-medication, the reason for referral (ADR/ TF/family history/preemptive request) and determined the suspected substances for DGI. The term “suspected substance for DGI” is henceforth used when a patient was included in the study based on a specific suspicion, that a substance (current intake or medication history) was causing ADR or TF and therefore was potentially involved in a DGI.
After patient data assessment, a buccal swab sample was taken from the patient for PGx panel test analysis that was conducted with the commercial system Stratipharm® offered by humatrix AG (Pfungstadt, Germany). To determine polymorphisms, they apply real-time PCR using the automated Life Technologies QuantStudio 12k flex (Thermo Fisher, MA, USA) with the respective optimized and commercially available chemistry. The Stratipharm® PGx panel test includes 100 genetic polymorphisms within 30 genes, which are listed in Supplementary Table 1. The buccal swab sample was sent to humatrix AG at the same day of collection. Also, the patient was referred to the nearest participating ambulatory study center (ASC), where two EDTA blood samples were taken. The blood sample analysis was conducted in the Biopharmacy Laboratory of the University of Basel. Here, additional genetic variants reported to influence the PK of respective drugs were tested (Supplementary Table 2).
One to two weeks after the first patient visit, the study pharmacist evaluated the available analysis results and in particular investigated if suspected substances were associated with at least one genetic variation to a potential DGI that could possibly explain the patient’s ADR/TF. If so, the confirmed suspicion was then defined as “confirmed substance for DGI”. If available, also other important factors like DDI, DFI, adherence or comorbidities were considered. Afterwards, individual recommendations were developed in a written medication review report.
Next, the second patient visit took places in the study pharmacy (one to three weeks after the first patient visit). The results and the recommendations were explained to the patient. Beyond that, the written report was handed over to the patient’s physicians.
After six months, there was a follow-up interview via telephone between the study pharmacist and the patient, in which mainly the current status of the medication and potential PGx-based adjustments were assessed.
Database Construction
For the database analysis, all information on each patient from the different stages of the study procedure was archived and transferred to a relationally designed database model. The database was constructed with Microsoft Office Professional Plus, Excel, version 16.0 (2016). It consists of 10 tables with the following content:
- Characteristics: Patient ID, year of birth, age, sex, smoking status, study center affiliation, referring physician, ICD-10 main diagnosis according to physician’s indication on the referral form
- Patient administration: Patient ID, date of signed informed consent, date of first visit, duration of first visit, date of second visit, duration of second visit, time for conducting the written report, date of follow-up, status of EDTA blood sample (received: yes/no/pendent)
- Medication: Patient ID, number of current prescribed drugs, status of self-medication (intake: yes/no)
- Identified DDI (based on the patient’s current medication): Patient ID, medicinal substance name (high-risk potential DDI perpetrator, according to the drug interaction database mediQ (www.mediq.ch, accessed June 05, 2023), medicinal substance code according to ATC classification system
- Pharmacogenotyping panel test results of Stratipharm® (humatrix AG, Pfungstadt, Germany): Patient ID, status of genetic variations (wildtype/heterozygote variant/homozygote variant) of selected polymorphisms (Supplementary Table 1)
- Pharmacogenotyping single test results (Biopharmacy, University of Basel): Patient ID, status of genetic variations (wildtype/heterozygote variant/homozygote variant) of selected polymorphisms (Supplementary Table 2)
- Genotype predicted phenotype: Patient ID, phenotype of selected genes (Supplementary Table 3)
- Suspected substance for DGI: Patient ID, medicinal substance name, medicinal substance code according to ATC classification system, dosage + unit, frequency of intake, reason for suspicion (ADR/TF/family history/preemptive request)
- Confirmed substance for DGI: Patient ID, medicinal substance name, medicinal substance code according to ATC classification system, involved genes of the DGI according to the clinical decision support system of the panel test provider Stratipharm® (humatrix AG, Pfungstadt, Germany) or the pharmGKB database (www.pharmgkb.org, accessed June 05, 2023)
- Medication adjustment: Status of implementing at least one recommendation based on PGx information (yes/no/lost-to-follow-up), medication adjustment type (starting use/discontinuing use/start-stop/dosage increase/dosage decrease/preemptive positive/preemptive negative), medicinal substance name involved in the adjustment, medicinal substance code according to ATC classification system
Data Analysis
Data analyses were performed using Microsoft Office Professional Plus, Excel, version 16.0 (2016) and R, R Studio, version 4.2.2 (2022). Results are presented as absolute number (n), count (%) or as median [interquartile range]. In addition to the analysis of the collected data of the total study population, exploratory subgroup analyses of selected population groups were performed.
It was not aimed to provide any results of statistical significance. The following subgroup analyses were conducted for the purpose of descriptive comparability:
Results
General Results
Characteristics
From 01/2019 to 12/2021, 142 patients were included in the study in two community pharmacy study centers (primary care, 60%) and in one hospital study center (secondary care, 40%). The study population was mainly female (66%) with a median age of 52 [40–63] years (minimum age: 18 years, maximum age: 88 years). Patients were referred to the study by medical specialists (65%) and general physicians (35%). An overview of the patients’ main characteristics is also provided in Supplementary Table 4.
Diagnoses
More than half of the patients had a main diagnosis of the ICD-10 section “F” of a mental or behavioral disorder (61%). Other patients had main diagnoses of musculoskeletal system and connective tissue diseases (ICD-10: M, 21%) or of the circulatory system (ICD-10: I, 11%).
The remaining patients (8%) had main diagnoses in various other ICD-10 group domains (C = neoplasms; E = endocrine, nutritional and metabolic diseases; G = nervous system; U = codes for special purposes; R = symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified; U = codes for special purposes; Z = factors influencing health status and contact with health services).
Medication
The majority of patients had polypharmacy with 5 or more medications prescribed a day (65%). The median prescribed drugs per person was 7 [4–9]. Over half of the patients (55%) reported to take no self-medication drugs.
Suspicion for DGI
A total of 559 suspicions for DGI, potentially caused by 109 different drugs were registered, which represents a median number of 4 [3–5] suspicions for DGI per patient. ADRs were suspected to be associated with a DGI in 225 cases (40%). TFs based on clinically observed ineffectiveness were suspected to be associated with DGI in 222 cases (40%). In 25 cases (4%), there was a suspicion of both ADR and TF in the same patient. A preemptive request regarding a prescription of a new drug was asked for 84 cases (15%). In 3 cases (1%) the PGx test was initiated based on a positive family history (eg, drug intolerance or variable drug response).
In Figure 2, we show the most frequently suspected substance groups (≥5 suspicions) classified according to the 3rd level of therapeutic and pharmacological subgroup of the ATC classification. Illustrated is the number of suspicions per category. Further suspected substance groups (<5 suspicions) are shown in Supplementary Table 5.
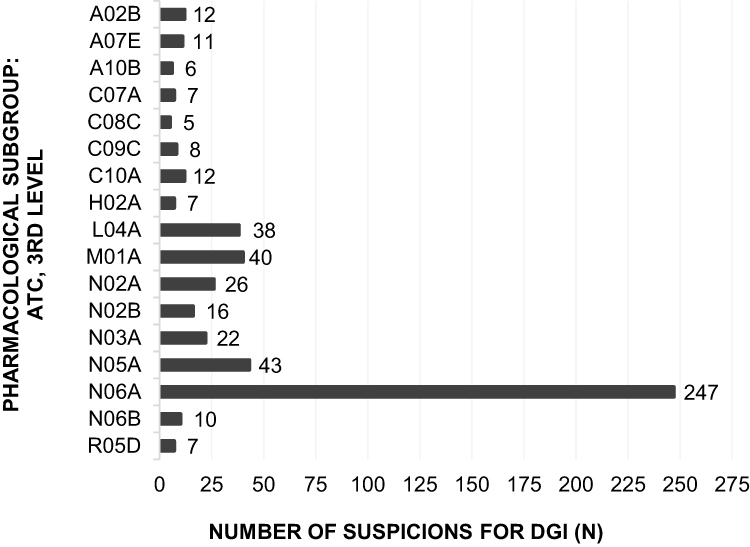 |
Figure 2 Number of DGI suspicions (≥ 5) per substance group, categorized according to the 3rd level of therapeutic and pharmacological subgroup of the ATC classification. Abbreviations: ATC, anatomical therapeutic chemical; DGI, drug-gene-interaction. Notes: A02B: Drugs for peptic ulcer and gastro-oesophageal reflux disease; A07E: Intestinal anti-inflammatory agents; A10B: Blood glucose lowering drugs, excl. insulins; C07A: Beta blocking agents; C08C: selective calcium channel blockers with mainly vascular effects; C09C: Angiotensin-II-Receptor Blockers (ARBs), plain; C10A: Lipid modifying agents, plain; H02A: Corticosteroids for systemic use, plain; L04A: Immunosuppressants; M01A: Anti-inflammatory and antirheumatic products, non-steroids; N02A: Opioids; N02B: Other analgesics and antipyretics; N03A: Antiepileptics; N05A: Antipsychotics; N06A: Antidepressants; N06B: Psychostimulants, agents used for ADHD and nootropics; R05D: Cough suppressants, exclusive combinations with expectorants. |
Confirmation of DGI
After PGx analysis, 324 of the 559 suspicions (58%) in 141 patients (99% of the study population) were confirmed as potential DGI. A median of 2 [3–5] confirmed DGI per patient was identified. The confirmation of a potential DGI is based on an association between the suspected drug and at least one observed genetic variation that could potentially cause the patient’s ADR or TF. Among the 109 suspected drugs, 64 (59%) of them were confirmed to be part of a potential DGI. Out of these 64 drugs, we identified 42 drugs (66%) interacting with at least one gene, for which a PGx-based drug therapy guideline was available according to the Clinical Guideline Annotations of PharmGKB (https://www.pharmgkb.org/guidelineAnnotations, accessed June 05, 2023). The identified drug-gene pairs are summarized in the Supplementary Table 6.
From the 30 genes of the PGx panel test, variations in 21 different genes were detected to be involved in a potential DGI. Genetic variations in CYP2C8, DPYD, HLA-A, HMGCR, IFNL3, IPTA, MTRNR1, NAT-2, and TPMT were detected in the study population, but it was not possible to associate them with any medication. The number of confirmed DGI in comparison to the suspicions for DGI (≥5 suspicions) is shown in Figure 3, again categorized according to the 3rd level of therapeutic and pharmacological subgroup of the ATC classification (cf Figure 2). Individual substances of the ATC-groups (3rd level) and the involved genes of the confirmed DGI are listed in Supplementary Table 7.
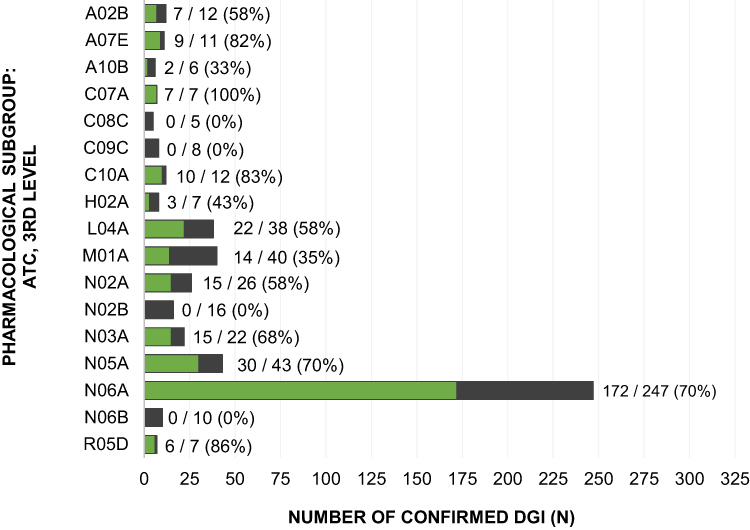 |
Figure 3 Number of confirmed DGI in proportion to number of suspicions for DGI (cf Figure 2), categorized according to the 3rd level of therapeutic and pharmacological subgroup of the ATC classification. Abbreviations: ATC, anatomical therapeutic chemical; DGI, drug-gene-interaction. Notes: A02B: Drugs for peptic ulcer and gastro-oesophageal reflux disease; A07E: Intestinal anti-inflammatory agents; A10B: Blood glucose lowering drugs, excl. insulins; C07A: Beta blocking agents; C08C: selective calcium channel blockers with mainly vascular effects; C09C: Angiotensin-II-Receptor Blockers (ARBs), plain; C10A: Lipid modifying agents, plain; H02A: Corticosteroids for systemic use, plain; L04A: Immunosuppressants; M01A: Anti-inflammatory and antirheumatic products, non-steroids; N02A: Opioids; N02B: Other analgesics and antipyretics; N03A: Antiepileptics; N05A: Antipsychotics; N06A: Antidepressants; N06B: Psychostimulants, agents used for ADHD and nootropics; R05D: Cough suppressants, exclusive combinations with expectorants. |
Identified DDI
In addition to the investigated DGI, potential DDI of the respective current medication of the patients were considered. Drugs with a high interaction risk (relative and absolute contraindications classified by the drug interaction database mediQ21) were identified to cause those DDI and are described in the following as “DDI perpetrator”. Overall, 66 patients (47%) of the study population were affected by potential DDI under their current medication. In total, we detected 148 DDI, which corresponds to a median of 2 [1–3] DDI per affected patient. Those DDI were potentially caused by 73 different DDI perpetrators. DDI, which were caused ≥3 times by a perpetrator out of a substance group, according to the 3rd level of therapeutic and pharmacological subgroup of the ATC classification, are shown in Table 1.
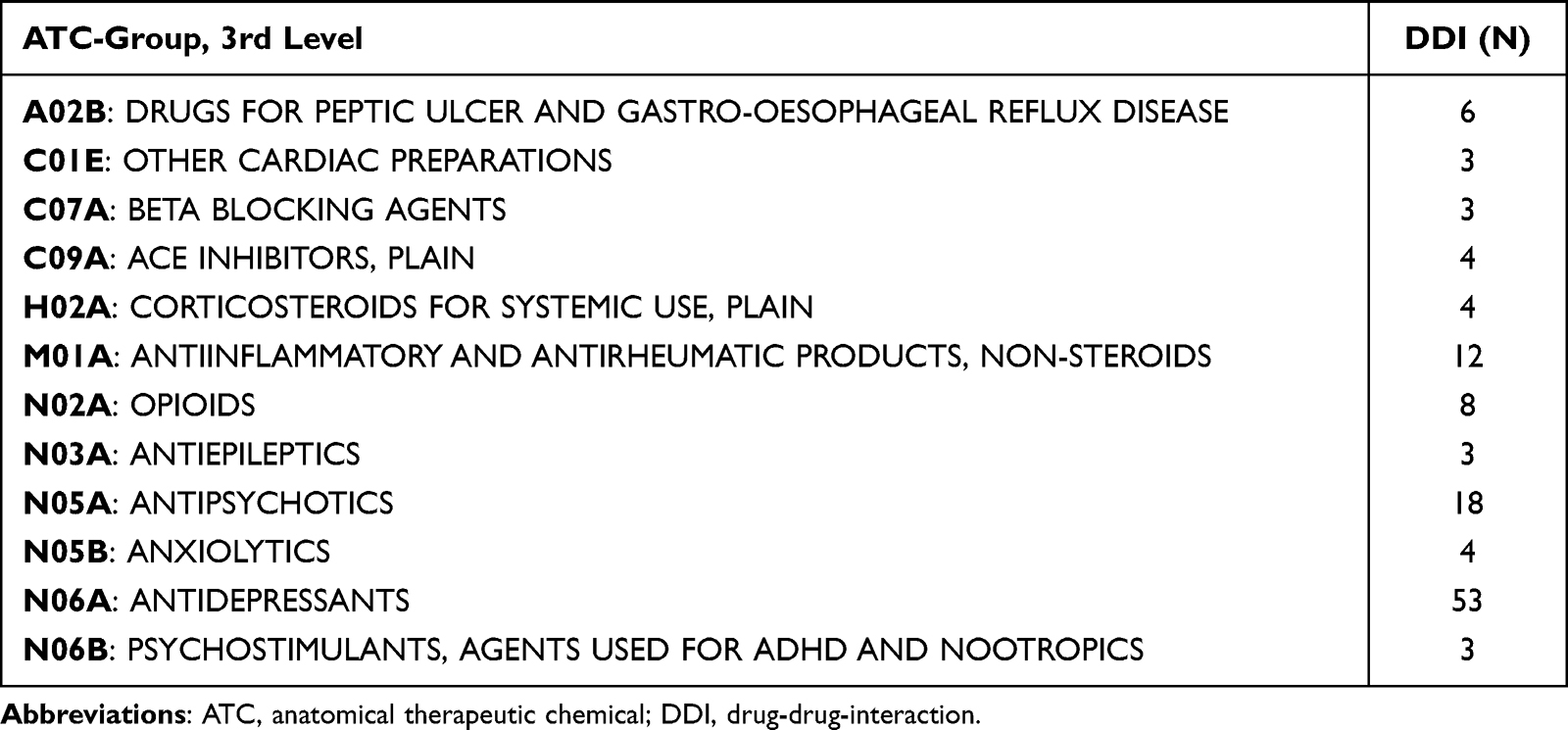 |
Table 1 Number of DDI Caused by Substance Groups, Categorized According to the 3rd Level Therapeutic and Pharmacological Subgroup of the ATC Classification |
Further DDI perpetrators were assigned individually to the following ATC –groups (3rd level): A03F, A06A, A07E, A10A, A10B, A12A, A12B, B01A, C03A, C03C, C03D, C09C, G02C, G04C, H03A, L04A, M03B, N01A, N02B, N05C, R03A, R05D.
Medication Adjustments
Six months after the PGx test and the provided written report to physician and patient, a follow-up interview was conducted with each patient by telephone. In the interview, it was asked whether at least one recommendation (based on the PGx analysis and the written report) was implemented in the patient’s medication by the physician. It was also assessed whether the patient’s PGx information was used in case of any medication adjustments within the six months, as advised.
A total of 173 medication adjustments for 87 patients (62% of the overall study population) were implemented within six months, based on the provided PGx information. Forty-four patients (31% of the overall study population) did not experience any adjustments in their daily medication after the PGx test. Ten patients (7% of the overall study population) were registered as lost-to-follow-up. The 173 PGx-based medication adjustments concerned 74 drugs and are categorized as follows: 73 medication adjustments in regard of the use of a new drug (42% of all medication adjustments); 48 medication adjustments related to the discontinuation of a drug (28% of all medication adjustments); 24 medication adjustments were classified as “start-stop”, which means that the use of a new recommended drug was started, but had to be stopped again within the six months (14% of all medication adjustments); 15 medication adjustments related to the dosage increase of a drug (9% of all medication adjustments); 5 medication adjustments related to the dosage decrease of a drug (3% of all medication adjustments); 5 drugs were tested preemptively and were later on not applied due to relevant genetic variants (= preemptive negative, 3% of all medication adjustments); and 3 drugs were tested preemptively and were afterwards applied, since no relevant genetic variants were detected (= preemptive positive, 1% of all medication adjustments).
Subgroup Results
Comparison SEX: Subgroup “Women” and Subgroup “Men” (Supplementary Table 8)
The study population consisted of 93 women (66%) and 49 men (34%). Polypharmacy was observed in 69% of the women and in 57% of the men. The evaluation of the diagnoses from the ICD-10 section “M” appeared with a 22 higher percentage in women. The number of suspicions for DGI was more than twice as high in women (n = 376) than in men (n = 183). However, the proportion of confirmed DGI was higher in men (67%) compared to women (53%). In addition, women had more medication adjustments after six months (68%) than men (41%).
Comparison AGE: Subgroup “< 65 Years” and Subgroup “≥ 65 Years” (Supplementary Table 9)
The study population consisted of 111 patients “<65 years” (78%) and 31 patients “≥65 years” (22%). 87% of the patients “≥65 years” experienced polypharmacy, which are proportionally distinctly more than patients “<65 years” (58%). The evaluation of the main diagnosis according to ICD-10 showed that the subgroup “<65 years” had more than twice as many diagnoses out of the ICD-10 section “F” (69%) compared to the subgroup “≥65 years” (29%). Whereas patients “≥65 years” had more often main diagnoses of the ICD-10 section “M” (39%). In the evaluation of the confirmed DGI, differences in all sections were detected. In the population “<65 years” almost two times more DGI suspicions were confirmed (69%) compared to the population “≥65 years” (37%). Also, the number of confirmed drugs causing the DGI was higher in the group “<65 years” (68%) than in the group “≥65 years” (42%). In the follow-up after six months, we detected that less patients “≥65 years” (48%) had medication adjustments compared to patients “<65 years” (65%).
Comparison MEDICATION AMOUNT: Subgroup “Polypharmacy” and Subgroup “No Polypharmacy” (Supplementary Table 10)
The study population consisted of 92 patients experiencing polypharmacy with an intake of 5 or more prescribed drugs daily (65%) and 50 patients without polypharmacy with an intake of 4 or less prescribed drugs daily (35%). The subgroup “polypharmacy” was with a median age of 56 years, 12 years older than the subgroup “no polypharmacy”. The population “no polypharmacy” had a median of 4 [3–5] suspicions for DGI per patient, though a median of 1 [1–3] confirmed DGI per patient. The population “polypharmacy” had a median of 3 [2–5] suspicion for DGI and a median of 2 [2–3] confirmed DGI per patient. 52% of the patients with “polypharmacy” were affected by potential DDI under their current medication, compared to 38% of the patients with “no polypharmacy”. Moreover, we identified that more patients of the group “no polypharmacy” (72%) had medication adjustments after six months in contrast to the patients of the group “polypharmacy” (56%).
Comparison MAIN DIAGNOSIS: Subgroup “ICD-10: F”, Subgroup “ICD-10: M” and Subgroup “ICD-10: I” (Supplementary Table 11)
The study population consisted of 86 patients with a main diagnosis of the ICD-10 section “F”, 30 patients with a main diagnosis of the ICD-10 section “M” and 15 patients with a main diagnosis of the ICD-10 section “I”. The median age was the highest for the patients “ICD-10: I” (68 [63–72]) compared to the patients “ICD-10: M” (60 [50–73]) and “ICD-10: F” (46 [34–56]). Moreover, the group “ICD-10: I” had the highest proportion of patients experiencing polypharmacy (87%). In the population “ICD-10: F”, we detected the highest number of confirmed suspicions for DGI (63%) and also of confirmed drugs involved in these DGI (70%). However, the absolute number of drugs causing DGI was lower (n = 40) compared to those drugs that cause DDI (n = 48) in the patients of “ICD-10: F”. Similar observations were made in patients of “ICD-10: M”. Concerning the medication adjustments after six months, we detected that the subgroup “ICD-10: M” had the highest number of patients with medication adjustments in count (74%), followed by the subgroup “ICD-10: F” (65%) and “ICD-10: I” (47%).
Discussion
Identified Interactions
In the overall study population, we confirmed 324 suspicions for DGI (58% of all suspicions) to potentially cause ADR or TF. By design, the included cases represent a convenient sample of patients with suspected DGI. In total, 21 different genes were detected to be involved in the confirmed DGIs. This finding supports the approach to use PGx panel tests instead of PGx single tests. Furthermore, we consider the rate of concordance between DGI suspicions and DGI confirmations with more than half (58%) as high. In literature it was shown that actionable gene variants potentially causing DGI are frequent. Up to 100% of the population may have an atypical response to at least one drug.22 At the same time, exposure to drugs affected by PGx is extremely common, reaching over 95% of the population exposed to at least one relevant drug.23,24
The high concordance rate of suspicions and confirmations in the study can also be considered as a quality control of the study setting and the collaboration with the referring physicians. In other words, the involved physicians and pharmacists seem to be well equipped to identify patients with a potential DGI, which could benefit from PGx testing.
In addition to genetic predisposition, other endogenous as well as exogenous factors are known to affect the patient’s drug response. Based on the results, we want to highlight the importance for awareness to DDI. We identified that 47% of the whole study population were affected by potential DDI. In fact, we found more drugs causing DDI (n = 73) than those causing DGI (n = 64). This result indicates that PGx testing alone is not sufficient for a personalized medication optimization approach. Notably, with a high frequency of DDI and a high frequency of DGI, the probability of drug-drug-gene-interactions (DDGI) increases. DDGI were not specifically aimed to be assessed in our study, but should be addressed in further research, especially for patients experiencing polypharmacy with a high potential for DDI. Also, we want to underline that only the drug causing a potential DDI (= DDI perpetrator) was listed in the database, the second involved drug was not specifically registered. This aspect should be considered for further research to be able to fully evaluate DDI and DDGI.
To summarize, all possible influencing factors should be taken into account for a complete and comprehensive analysis of each individual case. Since this is a descriptive study that was not designed to provide any results of statistical significance, comparisons (ie, DDI and DGI) need to be handled with caution. Nevertheless, the findings are considered as important observations, as the main objective of the study was to gain insight on the application of PGx information. An improvement of the individual patient’s medication can only be achieved with a holistic consideration of all given factors, besides the genetic predispositions.
Medication Adjustments
Six months after PGx testing, 173 medication adjustments were realized for 87 patients. We consider the implementation rate of the provided recommendations in 62% of the overall study population as improvable. Besides, we cannot disclaim a bias. The medication adjustments were assessed within the follow-up interview between study pharmacist and patient. The information about medication adjustments is therefore sensitive for response bias, confounding in both directions. It is possible that certain patients did not exactly know if realized medication adjustments made by their physicians were based on the PGx information. However, it is also possible that further adjustments were realized by other physicians or even during hospitalization without informing the patient, as the patient was instructed to always submit the PGx information in medical institutions. For further research, we propose to also follow-up with the referring physician for selected patients.
The results of the comparisons AGE (subgroup “<65 years” and subgroup “≥65 years”) and MEDICATION AMOUNT (subgroup “polypharmacy” and subgroup “no polypharmacy”) should also be emphasized, especially regarding medication adjustments. The subgroup “≥65 years” and the subgroup “polypharmacy” had comparably low implementation rates of the provided recommendations with 48% and 56%, respectively. Also, the subgroup of the diagnoses “ICD-10: I” had a low implementation rate with 47%. Though, the patients of the subgroup “ICD-10: I” had a median age of 68 [63–72] and a polypharmacy rate of 87% and thus matches the criteria of rising age and high medication amount. We think that the elderly patients experiencing polypharmacy and their associated physicians need different guidance for the application of PGx information. As multimorbidity increases over time, the number of diagnoses and therefore the number of drugs taken increases. It can be assumed that with the increasing complexity of a patient’s medication, changes are less likely to be made, even though the likelihood for DGI increases. Several medical specialists of different disciplines are usually involved in the medication of a multimorbid patient, so that medication adjustments (eg, by the general physician) should not be made without thorough consultation and involvement of all prescribers. This represents a barrier and can result in a possibly decreased compliance of realizing treatment changes in general. We aim to conduct further research and to discuss with involved physicians in a focus group possible reasons for the non-use of PGx information and what they require for a cross-disciplinary application of PGx information, especially in elderly patients experiencing polypharmacy.
In general, the non-use of PGx information in clinical practice could also be addressed to the lack of PGx-based therapy guidelines. As shown in the results, PGx-based therapy guidelines exist for 42 confirmed drugs (66%) interacting with at least one gene. We consider this rate as decent, but improvable. For 15 of those 42 drugs (36%) interacting with a gene, the guideline recommendations indicate to not adapt the dosage or change the therapy, although an interaction with the respective gene is described to influence therapy outcome. From a clinical point of view, we think that the recommendation to not change therapy is not sufficient, when the patient is suffering from ADR or TF and the suspected DGI is even confirmed by a PGx test. Physicians and pharmacists have then no option to justify their therapy decision with a therapy guideline and have to evaluate the need for a therapy change on their own. The lack of PGx-based therapy guidelines could therefore be a barrier for the application of PGx in clinical practice. Further research needs to be conducted to continuously increase the awareness and importance of PGx and the concomitant need for PGx-based therapy guidelines. Although this is a long-term process, it is already processing, considering that the majority of already existing PGx-based therapy guidelines have been developed in the last 10 years (https://www.pharmgkb.org/guidelineAnnotations, accessed June 05, 2023).
Diagnoses’ Distribution
The population of the PGx case series study is heterogeneous in terms of diagnoses, comprising three principal diagnosis groups according to ICD-10. However, the patients’ majority (61%) had a main diagnosis of ICD-10: F (mental or behavioral disorder) and are therefore overrepresented in the study population. A potential reason for the overrepresentation of patients with a mental or behavioral disorder can be referred to the recruitment, which was conducted in primary care (60% of all patients) and secondary care (40% of all patients). The recruitment center of the secondary care setting is associated with a psychiatric hospital department. Thus, all patients recruited in the secondary care were patients with the ICD-10 diagnosis “F”, which represents a selection bias and led to the overrepresentation. However, the recruitment in secondary care was not specifically restricted to this patient group. Therefore, the referral of such a high proportion of patients with a mental or behavioral disorder may also reflect the demand and interest for PGx in this particular patient group and/or of the referring physicians. This aspect is also supported by the comparably high rate (65%) of implemented medication adjustments six months after the PGx test. Consequently, we consider patients with a mental or behavioral disorder to be receptive to PGx testing and to the application of its information, which is described in detail in the discussion section on suitable target groups.
Also, we identified an overrepresentation of women (66%) in the study population. One potential reason can be attributed to the prevalence of the main diagnoses ICD-10 “F” and “M” in the study population.
In general, the prevalence of psychiatric diseases is higher in women than in men.25–27 In Switzerland, 10% of the women have a major depression compared to 8% of the men.28 Beside the ICD-10 “F”, also more diagnoses in the ICD-10 range “M” were found in women compared to men, which was also estimated due to the known epidemiological sex differences in the prevalence of rheumatic diseases.29–31 The second reason for the overrepresentation of women can be related to the fact that women experience in general almost twice as much ADR than men, independently of the diagnosis.32,33 Thus, with the study design searching for patients with ADR or TF, it was not unexpected to include women above average. At this point, the importance of sex differences in medicine and pharmacotherapy should be mentioned and considered for further research.
Suitable Target Groups
The main objective of this analysis was to identify the population that may benefit the most from pharmacogenotyping. As discussed above, we have a heterogeneous study population with a variety of diagnoses, but we also observed a selection bias for patients with a mental or behavioral disorder. Accordingly, our results cannot be inductively extrapolated to the totality of patients with pharmacotherapy. For example, we included only one patient with a main diagnosis of ICD-10: N (neoplasm), but we are aware that a wide range of PGx-actionable drugs are used for oncological patients (www.pharmgkb.org, accessed June 05, 2023), which therefore are a suitable target group. We propose that the identification of the target population benefiting the most from PGx testing should be composed of several aspects.
First, it is important to determine whether the population is prone to be treated with PGx-actionable drugs based on the current treatment guidelines. This is outlined above for oncological patients and was shown in our study results for several patient groups (Figure 3), eg, patients taking antipsychotics or antidepressant for a mental or behavioral disorder, pain patients taking opioids, and patients with circulatory diseases treated with a beta blocking agent or a lipid modifying agent.
Second, the target population and its referring physicians need to be receptive to the use of PGx information and willing to adopt possible medication changes. Here, we especially consider patients with an ICD-10 diagnosis “F” to be receptive, as they appear to be very proactive towards medication changes (Supplementary Table 11).
It remains to be determined, whether their proactiveness is linked to the fact that up to 50% of patients with a depression do not respond to the first-line-treatment, resulting in a longer therapy history of ineffectiveness.34,35 Also, patients from the subgroup “ICD-10: F” had with over 50% the highest rate of DGI suspicions based on reactive therapy failure and also the highest rate of DGI confirmations in general (Supplementary Table 11). To exclude an overrepresentation of specific phenotypes within the study population, which potentially could have influenced the high rate of DGI confirmations, CYP2D6 and CYP2C19 phenotype predicted genotype frequencies were checked. These two enzymes play a significant part in the metabolism of various drugs, particularly for patients with mental or behavioral disorders. The frequencies of CYP2D6 and CYP2C19 phenotype predicted genotypes were comparable to a European reference population,36 so that a bias in terms of genetic predisposition is not assumed.
And third, patient groups for whom medication adjustments may not be easily implemented should be targeted for further research, as explained above in the discussion section of medication adjustments in elderly patients experiencing polypharmacy. These patients and their referring physicians may not be equally receptive to PGx information’s application compared to, eg, patients with mental or behavior disorder; however, there is no indicator to assume that this patient group is not interested in PGx testing. Quite the opposite, as 65% of the patients of the whole study population were experiencing polypharmacy. Therefore, it rather seems that both patients and referring physicians of this population group are interested, perhaps they just do not know how to apply the PGx information and how to proceed with the recommendations for medication adjustments. Since usually different medical specialists are involved in the medication process of an older patient with polypharmacy, the approach of an interdisciplinary collaboration needs to be encouraged even more.
This applies not only to the collaboration of pharmacists and physicians, but also to physicians of different specializations. Here, further research is required to determine what exactly is needed for the application of PGx information for those patients, eg, more detailed explanation of the results, support in the communication process with different physicians, structured involvement of all parties (patient themself, general physician, medical specialist, family members, nursing staff).
After consideration of these aspects, the results of the database analysis, and indications of research,37–44 we consider the following target groups of our patient sample to be suitable for benefiting from pharmacogenotyping: Patients taking drugs for mental or behavioral disorder, circulatory diseases, selected immunological diseases (eg, rheumatic diseases, chronic inflammatory bowel diseases (IBD)), pain patients taking analgesics or opioids on a regular basis and patients experiencing polypharmacy, especially the elderly. However, before genotyping the afore-identified target groups, we suggest to check first if their suspected substances are associated with PGx in literature at all. Our results also revealed that not all drugs taken by a certain population group in our patient sample were confirmed as DGI. For example, patients of the ICD-10 group “I” (circulatory system) showed to have a concordance of 100% between suspected and confirmed DGI for beta blocking agents (ATC, 3rd level: C07A), but also a concordance of 0% for calcium channel blockers (ATC, 3rd level: C08C). Similar applies for psychostimulants (ATC, 3rd level: N06B) in patients of the ICD-10 group “F” (mental or behavioral disorder). Thus, the selection of the target group serves as a broad overview of possible patient populations with certain diagnoses. Still, a differentiation within the target group should be made individually according to the drugs taken.
Conclusion
Overall, we deduce that pharmacogenotyping is an effective method to detect the cause for ADR or TF, considering that 58% of the suspicions were confirmed as potential DGI.
We were also able to confirm suitable target groups with our patient sample that may benefit the most from PGx testing in clinical practice: Patients with mental or behavioral disorder, circulatory diseases, immunological diseases, pain patients taking analgesics or opioids on a regular basis, and in general patients experiencing polypharmacy, particularly the elderly.
Within the target groups, we gained an overview for which drugs a PGx test should be initiated, because they were predominantly confirmed to be part of a DGI.
According to the results, it is also important to emphasize that not only DGI should be considered in a comprehensive medication review, but also DDI and therefore potential DDGI. Indeed, we identify in almost half of the population potential DDI caused by 73 drugs. We therefore want to highlight that every patient case needs to be interpreted individually and that all the given patient information should be considered in addition to the genetic results.
Moreover, we observed an interdisciplinary acceptance in the study setting for the provided PGx information, deducted from the result that in 62% of the cases, medication adjustments based on the provided recommendations were realized by the physicians and patients within six months after the PGx test. Moreover, we were able to get an understanding of which patient groups, and which related physicians potentially require additional support and guidance in the realization of PGx-based medication adjustments. At this point, further research will be needed to determine what the physicians and the patients require (eg, in the case of elderly and/or patients with polypharmacy) to be able to apply PGx information for medication optimization.
To conclude, PGx panel testing can be a useful approach in personalized medicine with optimization of the medication. The implementation of pharmacogenotyping should be further strengthened on a large scale using interprofessional approaches,20 starting with target population groups (ClinicalTrials.gov NCT04507555).45 Since pharmacogenotyping is an intervention that does not harm, it can only be an advantage to know patient’s genetic profile and to be able to have individualized medication recommendations.
Data Sharing Statement
The patient data including genetic data presented in this study are available on request from the corresponding author. The data are not publicly available for ethical and privacy reasons.
Ethics Statement
The observational study “Pharmacogenetic Testing of Patients with unwanted Adverse Drug Reactions or Therapy Failure” was conducted according to the guidelines of the Declaration of Helsinki and was approved by the local ethics committee of “Ethikkommission Nordwest- und Zentralschweiz” (2019-01452, 31.10.2019).
Informed Consent Statement
All study patients provided written informed consent to use the data for research purposes, as well as for publishing.
Acknowledgments
We want to acknowledge all involved parties contributing to the research project: the patients for study participation; the physicians for patient referral, discussions and feedback; the study pharmacists for conducting the study procedure; the research project students for supporting data preparation; the laboratory staff for blood sample preparation; the members of the Biopharmacy Research Laboratory for performing additional genotyping; and humatrix AG for the collaborative effort.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the submitted journal Pharmacogenomics and Personalized Medicine; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Elemento O, Reece R. The future of precision medicine: towards a more predictive personalized medicine. Emerg Top Life Sci. 2020;4(2):175–177. doi:10.1042/ETLS20190197
2. Scott SA, Swen JJ. Pharmacogenomic determinants of interindividual drug response variability: from discovery to implementation. Genes. 2021;12(3):393. doi:10.3390/genes12030393
3. Peck RW. Precision medicine is not just genomics: the right dose for every patient. Annu Rev Pharmacol Toxicol. 2018;58(1):105–122. doi:10.1146/annurev-pharmtox-010617-052446
4. National Institute for Health and Care Excellence (NICE). Nice guideline. medicines optimisation: the safe and effective use of medicines to enable the best possible outcomes; 2015. Available from: https://www.nice.org.uk/guidance/ng5.
5. World Health Organization (WHO). Medication safety in polypharmacy; 2019. Available from: https://www.who.int/publications/i/item/WHO-UHC-SDS-2019.11.
6. U.S. Food and Drug Administration (FDA). Working to reduce medication errors; 2019. Available from: https://www.fda.gov/drugs/information-consumers-and-patients-drugs/working-reduce-medication-errors.
7. Meyer Zu Schwabedissen HE. The Role of Pharmacogenomics in Individualized Medicine. In: Fischer T, Langanke M, Marschall P, Michl S editors. Individualized Medicine: Ethical, Economical and Historical Perspectives. Advances in Predictive, Preventive and Personalised Medicine. Springer International Publishing; 2015:93–112. doi:10.1007/978-3-319-11719-5_7
8. Jeiziner C, Suter K, Wernli U, et al. Pharmacogenetic information in Swiss drug labels – a systematic analysis. Pharmacogenomics J. 2020:1–12. doi:10.1038/s41397-020-00195-4
9. Research C for DE and Table of Pharmacogenomic Biomarkers in Drug Labeling. FDA. Available from: https://www.fda.gov/drugs/science-and-research-drugs/table-pharmacogenomic-biomarkers-drug-labeling.
10. van der Wouden CH, Paasman E, Teichert M, Crone MR, Guchelaar HJ, Swen JJ. Assessing the implementation of pharmacogenomic panel-testing in primary care in the Netherlands utilizing a theoretical framework. J Clin Med. 2020;9(3):814. doi:10.3390/jcm9030814
11. Frigon MP, Blackburn MÈ, Dubois-Bouchard C, Gagnon AL, Tardif S, Tremblay K. Pharmacogenetic testing in primary care practice: opinions of physicians, pharmacists and patients. Pharmacogenomics. 2019;20(8):589–598. doi:10.2217/pgs-2019-0004
12. Haga SB. Challenges of development and implementation of point of care pharmacogenetic testing. Expert Rev Mol Diagn. 2016;16(9):949–960. doi:10.1080/14737159.2016.1211934
13. Abou Diwan E, Zeitoun RI, Abou Haidar L, Cascorbi I, Khoueiry Zgheib N. Implementation and obstacles of pharmacogenetics in clinical practice: an international survey. Br J Clin Pharmacol. 2019;85(9):2076–2088. doi:10.1111/bcp.13999
14. Stäuble CK, Lampert ML, Mikoteit T, Hatzinger M, Hersberger KE, Meyer Zu Schwabedissen HE. Severe Adverse Drug Reactions to Quetiapine in Two Patients Carrying CYP2D6*4 Variants: a Case Report. Int J Mol Sci. 2021;22(12):6480. doi:10.3390/ijms22126480
15. Stäuble CK, Lampert ML, Mikoteit T, Hatzinger M, Hersberger KE, Meyer Zu Schwabedissen HE. Nonresponse to high-dose bupropion for depression in a patient carrying CYP2B6*6 and CYP2C19*17 variants: a case report. Pharmacogenomics. 2020. doi:10.2217/pgs-2020-0087
16. Stäuble CK, Meier R, Lampert ML, et al. Case report: non-response to fluoxetine in a homozygous 5-HTTLPR S-allele carrier of the serotonin transporter gene. Front Psychiatry. 2022:13. doi:10.3389/fpsyt.2022.942268
17. Jeiziner C, Stäuble CK, Lampert ML, Hersberger KE, Meyer Zu Schwabedissen HE. Enriching medication review with a pharmacogenetic profile - a case of tamoxifen adverse drug reactions. Pharmgenomics Pers Med. 2021;14:279–286. doi:10.2147/PGPM.S285807
18. Jeiziner C, Allemann SS, Hersberger KE, Meyer Zu Schwabedissen HE. Is pharmacogenetic panel testing applicable to low-dose methotrexate in rheumatoid arthritis? - A case report. Pharmgenomics Pers Med. 2022;15:465–475. doi:10.2147/PGPM.S354011
19. Stäuble CK, Lampert ML, Mikoteit T, Hatzinger M, Hersberger KE, Meyer Zu Schwabedissen HE. Pharmacogenetic-guided antidepressant selection as an opportunity for interprofessional collaboration: a case report. Life. 2021;11(7):673. doi:10.3390/life11070673
20. Stäuble CK, Jeiziner C, Bollinger A, et al. A guide to a pharmacist-led pharmacogenetic testing and counselling service in an interprofessional healthcare setting. Pharmacy. 2022;10(4):86. doi:10.3390/pharmacy10040086
21. mediQ. Interaktions-Check; 2023. Available from: https://www.mediq.ch/.
22. McInnes G, Lavertu A, Sangkuhl K, Klein TE, Whirl-Carrillo M, Altman RB. Pharmacogenetics at Scale: an Analysis of the UK Biobank. Clin Pharmacol Ther. 2021;109(6):1528–1537. doi:10.1002/cpt.2122
23. Wittwer NL, Meier CR, Huber CA, Meyer Zu Schwabedissen HE, Allemann S, Schneider C. Utilization of drugs with pharmacogenetic dosing recommendations in Switzerland: a descriptive study using the helsana database. Pharmgenomics Pers Med. 2022;15:967–976. doi:10.2147/PGPM.S382214
24. Kimpton JE, Carey IM, Threapleton CJD, et al. Longitudinal exposure of English primary care patients to pharmacogenomic drugs: an analysis to inform design of pre-emptive pharmacogenomic testing. Br J Clin Pharmacol. 2019;85(12):2734–2746. doi:10.1111/bcp.14100
25. Kessler RC, Avenevoli S, Costello EJ, et al. Design and field procedures in the US National Comorbidity Survey Replication Adolescent Supplement (NCS-A). Int J Methods Psychiatr Res. 2009;18(2):69–83. doi:10.1002/mpr.279
26. Boyd A, Van de Velde S, Vilagut G, et al. Gender differences in mental disorders and suicidality in Europe: results from a large cross-sectional population-based study. J Affect Disord. 2015;173:245–254. doi:10.1016/j.jad.2014.11.002
27. Degenhardt L, Bharat C, Glantz MD, et al. The epidemiology of drug use disorders cross-nationally: findings from the WHO’s World Mental Health Surveys. Int J Drug Policy. 2019;71:103–112. doi:10.1016/j.drugpo.2019.03.002
28. Bundesamt für Statistik. Psychische Gesundheit; 2017. Available from: https://www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/gesundheitszustand/psychische.html.
29. Kvien TK, Uhlig T, Ødegård S, Heiberg MS. Epidemiological aspects of rheumatoid arthritis: the sex ratio. Ann N Y Acad Sci. 2006;1069:212–222. doi:10.1196/annals.1351.019
30. Favalli EG, Biggioggero M, Crotti C, Becciolini A, Raimondo MG, Meroni PL. Sex and management of rheumatoid arthritis. Clin Rev Allergy Immunol. 2019;56(3):333–345. doi:10.1007/s12016-018-8672-5
31. Yu C, Liu C, Jiang J, et al. Gender differences in rheumatoid arthritis: interleukin-4 plays an important role. J Immunol Res. 2020;2020:4121524. doi:10.1155/2020/4121524
32. Watson S, Caster O, Rochon PA. Reported adverse drug reactions in women and men: aggregated evidence from globally collected individual case reports during half a century. eClinicalMedicine. 2019;17. doi:10.1016/j.eclinm.2019.10.001
33. Tharpe N. Adverse drug reactions in women’s health care. J Midwifery Women’s Health. 2011;56(3):205–213. doi:10.1111/j.1542-2011.2010.00050.x
34. van Schaik RHN, Müller DJ, Serretti A, Ingelman-Sundberg M. Pharmacogenetics in Psychiatry: an Update on Clinical Usability. Front Pharmacol. 2020;11:575540. doi:10.3389/fphar.2020.575540
35. Keller MB, Lavori PW, Mueller TI, et al. Time to recovery, chronicity, and levels of psychopathology in major depression. A 5-year prospective follow-up of 431 subjects. Arch Gen Psychiatry. 1992;49(10):809–816. doi:10.1001/archpsyc.1992.01820100053010
36. Phan L, Jin Y, Zhang H, et al. National Center for Biotechnology Information, U.S. National Library of Medicine. ALFA: Allele Frequency Aggregator; 2020. Available from: https://www.ncbi.nlm.nih.gov/snp/docs/gsr/alfa/.
37. Elliott LS, Henderson JC, Neradilek MB, Moyer NA, Ashcraft KC, Thirumaran RK. Clinical impact of pharmacogenetic profiling with a clinical decision support tool in polypharmacy home health patients: a prospective pilot randomized controlled trial. PLoS One. 2017;12(2):e0170905. doi:10.1371/journal.pone.0170905
38. Finkelstein J, Friedman C, Hripcsak G, Cabrera M. Pharmacogenetic polymorphism as an independent risk factor for frequent hospitalizations in older adults with polypharmacy: a pilot study. Pharmgenomics Pers Med. 2016;9:107–116. doi:10.2147/PGPM.S117014
39. Pérez V, Salavert A, Espadaler J, et al. Efficacy of prospective pharmacogenetic testing in the treatment of major depressive disorder: results of a randomized, double-blind clinical trial. BMC Psychiatry. 2017;17(1):250. doi:10.1186/s12888-017-1412-1
40. Crews KR, Monte AA, Huddart R, et al. Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6, OPRM1, and COMT Genotypes and Select Opioid Therapy. Clin Pharmacol Ther. 2021;110(4):888–896. doi:10.1002/cpt.2149
41. Abdullah-Koolmees H, van Keulen AM, Nijenhuis M, Deneer VHM. Pharmacogenetics Guidelines: overview and Comparison of the DPWG, CPIC, CPNDS, and RNPGx Guidelines. Front Pharmacol. 2021;11:595219. doi:10.3389/fphar.2020.595219
42. Asiimwe IG, Pirmohamed M. Drug-drug-gene interactions in cardiovascular medicine. Pharmgenomics Pers Med. 2022;15:879–911. doi:10.2147/PGPM.S338601
43. Wiss FM, Stäuble CK, Meyer Zu Schwabedissen HE, Allemann SS, Lampert ML. Pharmacogenetic Analysis Enables Optimization of Pain Therapy: a Case Report of Ineffective Oxycodone Therapy. J Personalized Med. 2023;13(5):829. doi:10.3390/jpm13050829
44. Swen JJ, van der Wouden CH, Manson LE, et al. A 12-gene pharmacogenetic panel to prevent adverse drug reactions: an open-label, multicentre, controlled, cluster-randomised crossover implementation study. Lancet. 2023;401(10374):347–356. doi:10.1016/S0140-6736(22)01841-4
45. Stäuble CK, Lampert ML, Allemann S, et al. Pharmacist-guided pre-emptive pharmacogenetic testing in antidepressant therapy (PrePGx): study protocol for an open-label, randomized controlled trial. Trials. 2021;22(1):919. doi:10.1186/s13063-021-05724-5
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.