Back to Journals » Drug Design, Development and Therapy » Volume 19
Dexmedetomidine’s Effect on Catecholamine and Inflammation in Reducing In-Hospital Adverse Events for Older Patients with STEMI Undergoing Primary PCI
Authors Liu GA, Wu W, Zhou L, Zhang R, Liu F
Received 22 May 2025
Accepted for publication 29 September 2025
Published 2 October 2025 Volume 2025:19 Pages 8935—8947
DOI https://doi.org/10.2147/DDDT.S542160
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Tamer Ibrahim
Guang-An Liu, Wanglong Wu, Linxiao Zhou, Ruoxi Zhang, Feng Liu
Department of Cardiology, Suzhou Kowloon Hospital, Shanghai Jiao Tong University School of Medicine, Suzhou, 215028, People’s Republic of China
Correspondence: Ruoxi Zhang, Department of Cardiology, Suzhou Kowloon Hospital, Shanghai Jiao Tong University School of Medicine, 118 Wansheng Street, Suzhou Industrial Park, Suzhou, 215028, People’s Republic of China, Email [email protected] Feng Liu, Department of Cardiology, Suzhou Kowloon Hospital, Shanghai Jiao Tong University School of Medicine, 118 Wansheng Street, Suzhou Industrial Park, Suzhou, 215028, People’s Republic of China, Email [email protected]
Objective: This study aimed to assess the effects of dexmedetomidine (DEX) on anxiety and inflammation, and its potential in reducing in-hospital adverse events in older patients with ST-elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI).
Methods: We conducted a retrospective, real-world cohort study, enrolling 160 elderly patients with STEMI admitted to the cardiac care unit (CCU) between September 2020 and December 2024. Patients were divided into two groups: DEX and non-DEX. Propensity score matching (PSM, 1:1 ratio) was applied based on demographic and clinical variables, ensuring balanced groups for comparison. We evaluated catecholamine and inflammation levels, anxiety using the Amsterdam Preoperative Anxiety and Information Scale (APAIS), and cognitive function at four time points (T0–T3). The incidence of cumulative MACE (20.00% vs 38.8%, P = 0.015) and VT/VF (1.3% vs 10.0%, P = 0.034) was significantly lower in the DEX group compared to the non-DEX group. Multivariable logistic regression was performed to identify risk factors for in-hospital major adverse cardiac events (MACE).
Results: The DEX group had significantly lower catecholamine (norepinephrine, P < 0.001; epinephrine, P = 0.001; dopamine, P < 0.001) and inflammation levels (hs-CRP, P < 0.001) post-PCI compared to the non-DEX group. Additionally, heart rate (HR) (T1, P < 0.001; T2, P < 0.001; T3, P = 0.007) and respiratory rate (RR) (T1, P < 0.001; T2, P < 0.001) were lower, while blood oxygen saturation (SpO2) (T1, P = 0.045; T2, P < 0.001; T3, P < 0.001; T4, P = 0.016) was higher in the DEX group at various time points. In the DEX group, Ramsay Sedation Scores were higher at T1 (P = 0.007) and T2 (P < 0.001) than at T0, and anxiety scores decreased significantly from T1 (P = 0.021), T1 (P = 0.017) to T3 (P = 0.015) compared with the preceding time point. DEX was identified as an independent predictor of reduced in-hospital MACE [odds ratio (OR) = 0.244, 95% confidence interval (CI) = 0.082– 0.728, P = 0.011].
Conclusion: DEX was associated with lower catecholamine and inflammation levels, provided adequate sedation, and appeared safety, feasibility, and effectiveness for older patients with STEMI undergoing primary PCI.
Keywords: dexmedetomidine, catecholamine, hs-CRP, sedation, STEMI, primary PCI, MACE, ventricular arrhythmia
Graphical Abstract:

Introduction
Convergent experimental and clinical evidence has highlighted the crucial role of pro-inflammatory pathways in the pathophysiology of coronary artery disease (CAD). Specifically, the focus on treating inflammation in patients with acute myocardial infarction (AMI) is shifting from addressing its chronic aspects to targeting the acute phase.1 Myocardial infarction, a life-threatening condition, significant anxiety and psychological distress, which is characterized by symptoms such as dissociation, re-experiencing, avoidance, and hyperarousal.2 Furthermore, anxiety has been identified as a risk factor for subsequent cardiovascular events and interventions.2 Notably, patients with anxiety and stress-related conditions also exhibit elevated circulating levels of pro-inflammatory cytokines, further linking inflammation with adverse cardiovascular outcomes.3
Primary percutaneous coronary intervention (PCI) is considered the preferred reperfusion strategy for patients with ST-elevation myocardial infarction (STEMI). However, the procedure is typically performed under local anesthesia, which may not fully block nerve transmission, leaving patients vulnerable to negative emotions such as fear, pain, and discomfort during the procedure.4 In some patients, both the STEMI and the PCI procedure itself can induce significant psychological stress disorder and possible additional inflammation, leading to a range of preoperative emotional and psychological reactivity, with anxiety being one of the most common.5 Therefore, a key area of interest in the field of anesthesia is the identification of reliable sedative and analgesic agents that can reduce the need for traditional anesthetics, minimize patients’ stress response to pain, and decrease perioperative complications.
AMI is well known to primarily affect the elderly population.6 Notably, cognitive dysfunction, depression, and anxiety have been observed in elderly patients who underwent total intravenous anesthesia (TIVA).7 Therefore, the use of anesthesia and sedative drugs in this group requires careful consideration, with close monitoring to ensure safety and minimize potential complications. Dexmedetomidine is a potent and selective α2 adrenergic receptor agonist that provides dose-dependent sedation, analgesia, anxiolysis, and sympathetic inhibition. It is known for its minimal side effects, making it a valuable and advantageous option in clinical settings.8 Clinical research has demonstrated that dexmedetomidine not only offers neuroprotective and anti-inflammatory benefits but also helps alleviate postoperative cognitive dysfunction in elderly patients.9,10 More recent studies have further highlighted the role of DEX in modulating cardiovascular stress and systemic inflammation, supporting its potential as a protective strategy in acute cardiovascular conditions.11–13
However, a critical knowledge gap remains: while DEX has shown promise in perioperative and critical care contexts, its role in elderly STEMI patients undergoing primary PCI has not been systematically evaluated. Specifically, there is limited evidence regarding its effects on anxiety, inflammatory responses, and in-hospital outcomes in this high-risk population. Therefore, we hypothesized that dexmedetomidine administration in elderly STEMI patients could be associated with attenuation of ASD, lower systemic inflammation, and improve in-hospital outcomes. This study was conducted to evaluate the effect of DEX on ASD and inflammation in reducing in-hospital adverse events for older patients with STEMI undergoing primary PCI.
Methods
Study Population
We retrospectively enrolled 160 patients diagnosed with STEMI who underwent primary PCI and were admitted to the cardiac care unit (CCU) between September 2020 and December 2024. STEMI was diagnosed if a patient exhibited the following: chest pain for >30 min and ST-segment elevation of 2 mm in at least two contiguous precordial electrocardiography (ECG) leads or >1 mm in at least two contiguous limb ECG leads or a newly developed left bundle branch block.14 The exclusion criteria included patients with bradycardia, second-degree or higher atrioventricular (AV) block, a history of coronary artery bypass graft (CABG) surgery, cardiogenic shock, unconsciousness, a life expectancy of less than 2 years, cognitive dysfunction, or mental disorders.
Patients were divided into two groups: the DEX group and the non-DEX group. To account for variations in initial risk factors and baseline characteristics between patients who received DEX or not, we employed propensity score matching, with a 1:1 matching ratio, allowing for replacement. Patients who either received DEX or not, but could not be adequately matched, were excluded from the study population. A systematic comparison of patient information between the two groups was conducted during hospitalization.
The mean arterial pressure (MAP), heart rate (HR), respiratory rate (RR), and blood oxygen saturation (SpO2) were recorded at four time points: before drug infusion (T0), 10 minutes after drug infusion (T1), at the end of the procedure (T2), and 30 minutes after the procedure (T3). Major adverse cardiac events (MACE) included cardiovascular death, reinfarction, repeat target vessel revascularization (TVR), ventricular tachycardia (VT) and ventricular fibrillation (VF), advanced heart failure in hospital. According to the clinical protocol of our medical center, the cardiologist in the CCU is responsible for collecting and evaluating the catecholamine levels, including norepinephrine, epinephrine, and dopamine, in patients both preoperatively and postoperatively.
Covariate Characteristics Included
To ensure data integrity, covariates included in the study were required to have no more than 25% missing values in the original dataset. The study examined a range of patient demographic characteristics, including age, sex, weight, heart beats, respiratory rate, blood pressure, blood oxygen saturation, medical history risk factors, such as alcohol drinking, hypertension, diabetes and smoking, and medications. To compare the characteristics between the DEX and non-DEX groups, absolute standardized differences were calculated.15 This method was chosen given the large sample size, with an absolute standard deviation greater than 10% indicating a meaningful difference between the two groups. The majority of missing data resulted from variability in data recording practices across clinical settings, rather than systematic patient selection.
Match Processing
To account for differences in initial risk factors and baseline characteristics between patients receiving DEX and those not receiving DEX, we employed propensity score matching. The propensity score was derived using a multivariable logistic regression model, which estimated each patient’s likelihood of receiving primary PCI based on selected covariates. Patients who received DEX were then matched 1:1 with non-DEX patients, using a logit-transformed propensity score and a caliper of 0.03, allowing for replacement. Patients who could not be appropriately matched were excluded from the analysis.
DEX Treatment
Patients in the DEX group received a loading dose of 1 μg/kg of DEX (Yangtze River Pharmaceutical (Group) Co., Ltd., Jiangsu, China), followed by a maintenance dose of 0.5 μg/kg administered intravenously over 15 minutes, after which the procedure was performed. The patients in the non-DEX cohort were treated according to the standard primary PCI protocol at our center, without receiving any sedation measures.
Sedation Level Assessment
In our cardiology department, we have dedicated anesthesiologists who routinely evaluate sedation depth and anxiety levels for patients undergoing primary PCI with DEX treatment. The sedation depth was assessed using the Ramsay Sedation Scale,16 a widely accepted tool for measuring sedation levels in clinical settings. Additionally, to quantify preoperative anxiety, we employed the Amsterdam Preoperative Anxiety and Information Scale (APAIS).17 The APAIS is a validated instrument designed to measure patients’ preoperative anxiety and their need for information. It was administered as part of our standard pre-procedural assessment for patients undergoing primary PCI. These assessments were also conducted at four time points: before drug infusion (T0), 10 minutes after drug infusion (T1), at the end of the procedure (T2), and 30 minutes after the procedure (T3). The routine use of these scales allows for a comprehensive evaluation of the patient’s sedation status and anxiety levels throughout the perioperative period, providing valuable data for our retrospective analysis.
Coronary Angiography and Stenting
Primary PCI was typically performed via the percutaneous radial artery approach, although the femoral approach was used if an intra-aortic balloon pump was required. All angiographic data were reviewed using standard techniques from the catheterization laboratory records.18 A target artery was considered clinically significant if the vessel stenosis exceeded 50%. Blood flow in the infarct-related artery (IRA) was assessed using the Thrombolysis in Myocardial Infarction (TIMI) grading system, applicable to cases receiving only primary PCI. Prior to the procedure, all patients were given 300 mg of chewable aspirin (Bayer Healthcare Co., Ltd., Beijing, China) and 180 mg of ticagrelor (AstraZeneca, plc., Shanghai, China). PCI success was defined as achieving a stenosis of less than 20% in the IRA with TIMI III flow post-procedure. Following PCI, all patients were transferred to the cardiac care unit for standardized STEMI treatment.
Blood Sampling
Blood samples were collected from the cubital veins of all patients enrolled in the study. N-terminal pro B-type natriuretic peptide (NT-proBNP), creatine kinase-MB (CK-MB), and troponin I levels were measured daily from admission. Blood samples were taken at the same times for all patients: upon admission, and 24 and 48 hours later. Plasma NT-proBNP levels were assessed using an Elecsys® NT-proBNP analyzer, a commercially available electro chemiluminescent sandwich immunoassay (Roche Diagnostics GmbH, Mannheim, Germany). Fasting serum levels of blood glucose, triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C) were measured after a 12-hour fast using an Olympus AU640 Autoanalyzer (Olympus Corporation, Tokyo, Japan) with an automated spectrophotometric and enzymatic colorimetric method. Other biochemical measurements were performed using the Jaffe kinetic method on a Hitachi 7600 Autoanalyzer (Hitachi, Ltd., Tokyo, Japan). Plasma norepinephrine, epinephrine, and dopamine were measured using a commercial ELISA kit (CatCombi, IBL, Hamburg, Germany), according to the manufacturer’s instructions. This method has been validated in previous studies.19 All assays were performed in duplicate, with intra- and inter-assay coefficients of variation (CVs) <10%. Our hospital’s central laboratory is certified and regularly participates in external quality control programs.
Statistical Analysis
Quantitative variables were expressed as mean ± standard deviation and qualitative variables were expressed as a percentage (%). Independent 2-sample t-test or 1-way analysis of variance with post hoc Student-Newman-Keuls test was used to test differences between ≥ 2 sets of data. Categorical variables were also compared using the χ2 or Fisher’s exact test. For the primary endpoint of in-hospital MACE, logistic regression was used as the main analytical approach, as it is most appropriate for short-term, fixed follow-up periods. Odds ratios (ORs) with 95% confidence intervals were reported. Cox proportional hazards regression was additionally performed to generate hazard ratios (HRs) and to illustrate cumulative incidence using Kaplan–Meier curves. Univariate and multivariate logistic regression analyses were used to identify predictors of in-hospital MACE. A statistically significant difference was indicated when P < 0.05. All data cleaning and preprocessing were conducted using the R software, version 4.3.2. All statistical analyses were performed using the IBM SPSS statistical software, version 26.0 (IBM SPSS Inc., Armonk, NY, USA).
Results
Baseline Characteristics
After propensity score matching, 160 patients were included (80 in the DEX group and 80 in the non-DEX group) (Figure 1). Baseline demographic and clinical characteristics were well balanced between the two groups, with absolute standardized differences <10% for all covariates (Tables 1 and 2).
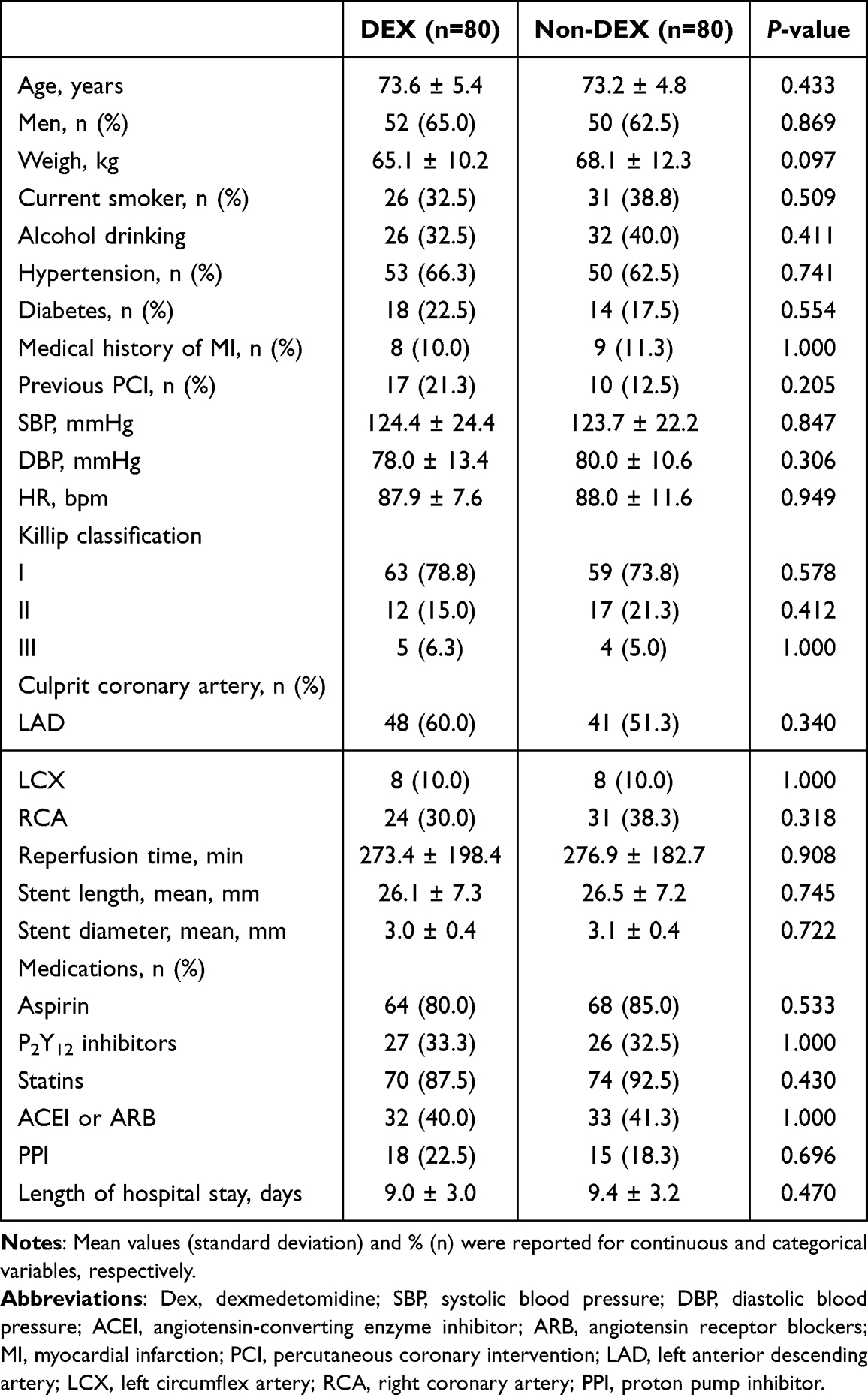 |
Table 1 Baseline Characteristics of Patients Between the Two Groups |
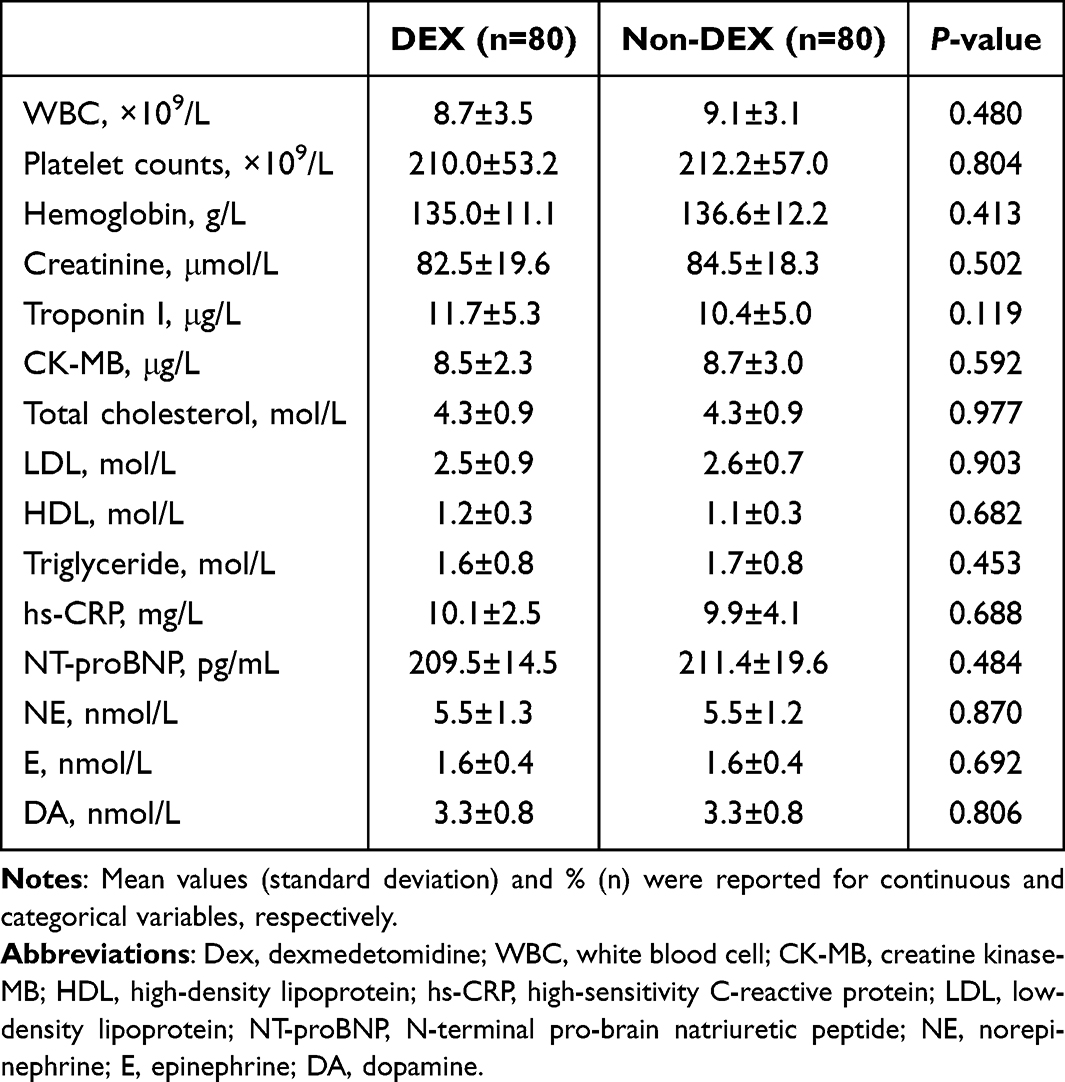 |
Table 2 Baseline Laboratory Characteristics Between the Two Groups |
 |
Figure 1 Study flowchart. |
Catecholamine and Inflammatory Markers
Catecholamine and hs-CRP levels after primary PCI are shown in Figure 2. In the DEX group, the levels of norepinephrine (4.7±2.2 nmol/L vs 7.6±2.5 nmol/L, P < 0.001), epinephrine (1.5±0.5 nmol/L vs 1.9±0.7 nmol/L, P = 0.001), dopamine (2.9±0.7 nmol/L vs 3.9±0.9 nmol/L, P < 0.001), and hs-CRP (mmol/L vs mmol/L, P < 0.001) were significantly lower compared to the non-DEX group. These findings suggest that patients in the DEX group were associated with significantly lower post-PCI catecholamine and hs-CRP levels.
 |
Figure 2 Comparison of catecholamine and inflammation levels after primary PCI. Abbreviations: PCI, percutaneous coronary intervention; hs-CRP, high-sensitivity C-reactive protein. |
Comparison of Vital Signs and Sedation/Anxiety Scores
Compared to the non-DEX group, HR in the DEX group was significantly lower at T1 (71.2±12.5 bpm vs 93.5±11.1 bpm, P < 0.001), T2 (74.1±4.3 bpm vs 97.5±8.5 bpm, P < 0.001), and T3 (76.2±12.0 bpm vs 93.3±7.2 bpm, P = 0.007). Respiratory rate (RR) was significantly lower in the DEX group at T1 (16.3±1.4 bpm vs 17.8±0.9 bpm, P < 0.001) and T2 (16.3±1.0 bpm vs 18.0±1.9 bpm, P < 0.001). Additionally, SpO2 was significantly higher in the DEX group at T1 (96.4±0.9% vs 96.2±0.9%, P = 0.045), T2 (96.3±1.1% vs 95.3±0.9%, P < 0.001), T3 (96.6±0.5% vs 95.6±0.6%, P < 0.001), and T4 (96.4±0.6% vs 96.1±1.0%, P = 0.016) (Table 3). These results indicate that DEX administration was associated with lower HR and RR, and higher SpO2 at multiple time points compared with the non-DEX group.
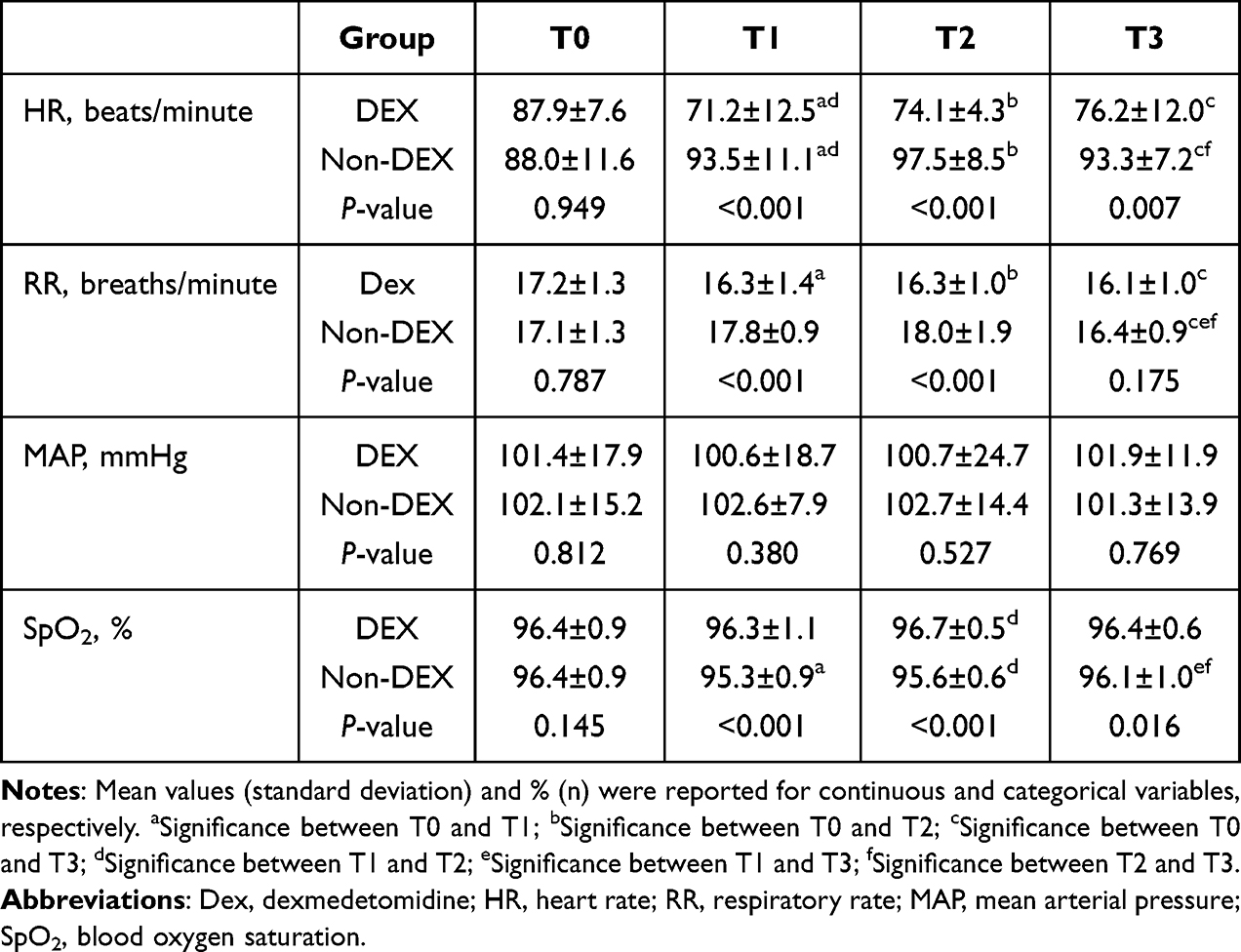 |
Table 3 Comparison of HR, RR, MAP, SpO2 Between the Two Groups |
The trends in the Ramsay and APAIS scores are shown in Figure 3. In the DEX group, Ramsay Sedation Scores were higher at T1 (P = 0.007) and T2 (P < 0.001) than at T0, and anxiety scores decreased significantly from T1 (P = 0.021), T1 (P = 0.017) to T3 (P = 0.015) compared with the preceding time point.
 |
Figure 3 Ramsay and APAIS scores at different time points. Abbreviation: APAIS, Amsterdam Preoperative Anxiety and Information Scale. |
In-Hospital Adverse Cardiovascular Events
For in-hospital adverse cardiovascular events, the incidence of cumulative MACE was significantly lower in the DEX group compared to the non-DEX group (20.0% vs 38.8%, P = 0.015) (Table 4 and Figure 4). When analyzing specific arrhythmic events, we found that the incidence of ventricular arrhythmias was significantly lower in the DEX group compared with the non-DEX group (1.3% vs 10.0%, P = 0.034). In contrast, atrial fibrillation occurred in 1.3% of patients in the DEX group versus 7.5% in the non-DEX group, although this difference did not reach statistical significance (P = 0.117). These findings indicate that the overall reduction in MACE observed in the DEX group was primarily driven by a lower incidence of ventricular arrhythmias. In multivariable logistic regression, DEX treatment remained independently associated with reduced risk of in-hospital MACE (OR = 0.244, 95% CI = 0.082–0.728, P = 0.011;Table 5).
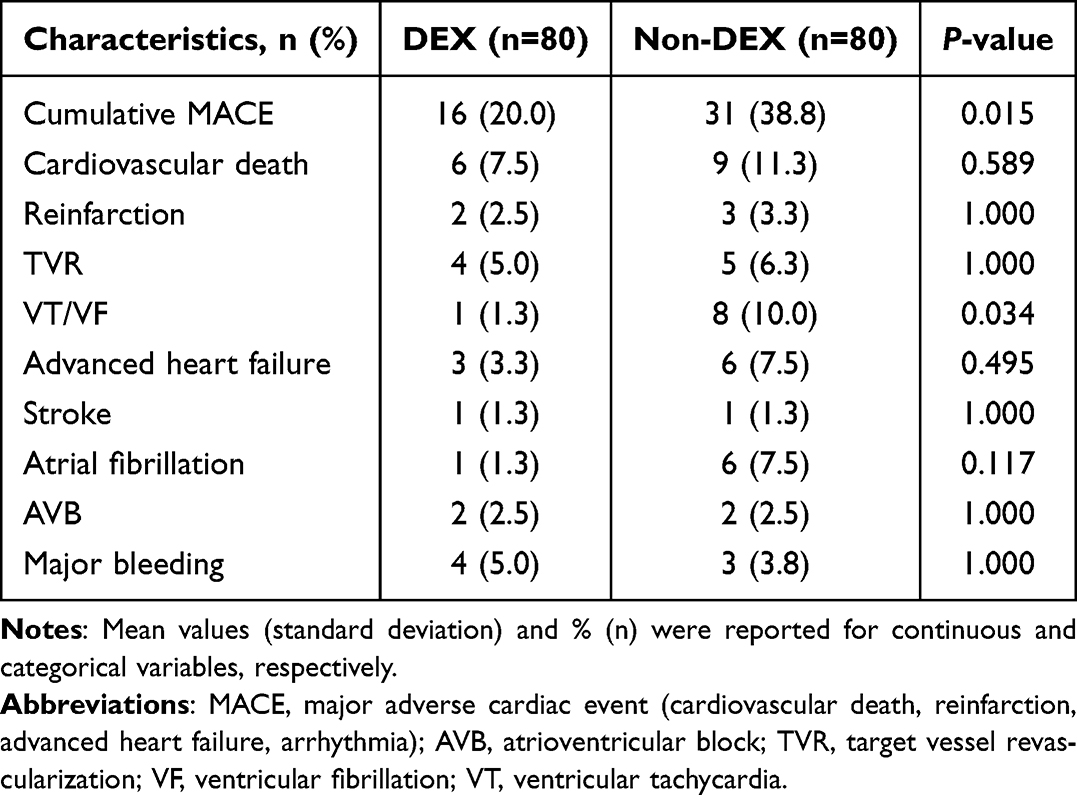 |
Table 4 In-Hospital Adverse Cardiovascular Events |
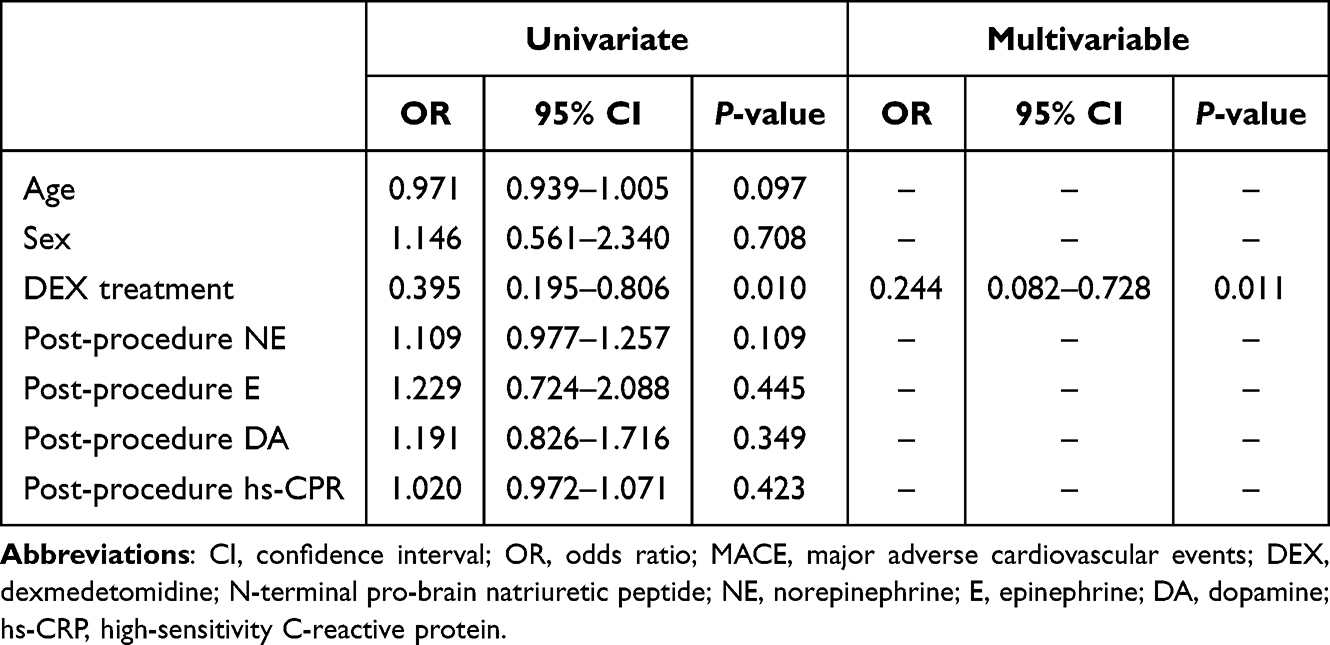 |
Table 5 Univariate and Multivariable Regression Analysis for in-Hospital MACE |
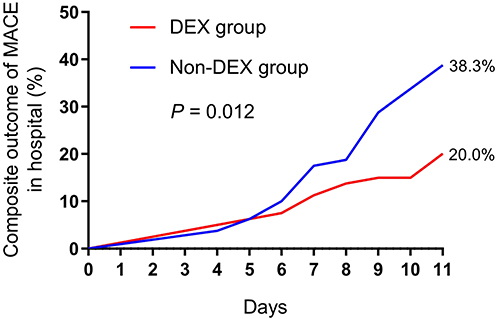 |
Figure 4 Kaplan-Meier curves for cumulative MACE in hospital. Hazard Ratio: 0.472, 95% confidence interval: 0.263 to 0.848, Log-rank (Mantel-Cox) test, P=0.012. Abbreviation: MACE, major adverse cardiovascular events. |
Discussion
Older patients with STEMI and stable hemodynamics typically undergo primary PCI under local anesthesia. However, this approach often leaves patients exposed to significant stress and anxiety, which may adversely affect perioperative stability and outcomes. Anxiety, as a subjective psychological experience, is characterized by fear, tension, and irritability.20 Severe preoperative anxiety can impair cooperation during PCI, increase sedative requirements,21 and elevate the risk of perioperative cardiovascular complications. Thus, it is crucial to promptly identify elderly patients with significant anxiety and provide appropriate management.
In elderly patients undergoing PCI, the administration of sedatives requires comprehensive monitoring due to their limited physiological reserve and heightened sensitivity to medications. DEX, a selective α2-adrenergic agonist, not only provides sedation and anxiolysis but also suppresses sympathetic activation, thereby counteracting the catecholamine surge often triggered during PCI.22–24 By modulating both neuroendocrine and inflammatory pathways, DEX use was associated with lower stress responses, catecholamine release, and systemic inflammation.7 These mechanisms explain why patients in the DEX group exhibited lower catecholamine and hs-CRP levels and fewer in-hospital adverse cardiovascular events.
Our study also demonstrated that patients receiving DEX had lower heart and respiratory rates, and modestly higher oxygen saturation compared with controls. Ramsay sedation scores confirmed adequate but arousable sedation, while APAIS scores showed significantly reduced perioperative anxiety. Importantly, DEX use was associated with fewer malignant arrhythmias and lower incidence of in-hospital MACE. These associations may reflect the sedative and sympatholytic properties of DEX.
Mechanistic and Safety Considerations
Mechanistically, DEX may improve outcomes through its dual action on neuroendocrine and immune pathways: (1) suppression of sympathetic outflow and catecholamine surge, mitigating arrhythmogenic potential and hemodynamic stress; (2) downregulation of pro-inflammatory cytokines such as IL-6 and CRP, reducing systemic inflammatory burden and endothelial dysfunction. Together, these effects likely contributed to the improved hemodynamic stability and lower event rates observed in our study.
Safety also warrants attention. Previous studies reported that high doses of DEX may lead to hypertension and exacerbate ischemic brain injury.25 In addition, DEX can cause dose-dependent reductions in heart rate and blood pressure, and the initial bolus may trigger a biphasic blood pressure response.26 These risks support the use of lower dosing strategies such as those employed in our study. On the other hand, DEX has been shown to provide safe sedation without significant respiratory depression, mimicking natural sleep.27,28 When appropriately dosed and closely monitored, it represents a safe option for sedation during PCI.
Arrhythmias and Adverse Outcomes
Preoperative anxiety and catecholamine surges are well known to increase arrhythmogenic risk.29 Life-threatening ventricular tachyarrhythmias (VTAs), including ventricular tachycardia and ventricular fibrillation, may occur at any stage of MI.30 Paroxysmal atrial fibrillation (PAF) is also frequent in the acute MI setting, occurring in 5–20% of patients,26 and is associated with both heightened vagal tone and sympathetic responses.31 When refractory arrhythmias occur, sedation and mechanical ventilation may be necessary.32
Our results demonstrate that the difference in in-hospital MACE between groups was mainly attributable to a lower incidence of ventricular arrhythmias in patients receiving DEX. This finding is consistent with the known sympatholytic and antiarrhythmic properties of DEX, which may help stabilize electrophysiological activity during acute myocardial infarction.33,34 Although atrial fibrillation was numerically less frequent in the DEX group (1.3% vs 7.5%), the difference was not statistically significant, likely due to the limited sample size and relatively low event rates. Taken together, these findings suggest that the potential protective effect of DEX in this setting is most evident in reducing ventricular arrhythmias, which are clinically important drivers of in-hospital adverse events.
Our findings also align with evidence linking anxiety and inflammation in MI patients. AMI and hospitalization can trigger significant anxiety,35 which has been associated with elevated CRP and worse cardiovascular outcomes.36–40 In our study, the DEX group demonstrated lower hs-CRP levels, supporting the hypothesis that DEX use may be associated with lower anxiety-related stress and inflammation, thereby reducing in-hospital complications.
Strengths and Limitations
A major strength of this study is its real-world, propensity-matched design, which reduces baseline imbalance between groups and enhances clinical relevance. Additionally, by combining biochemical assays, validated anxiety/sedation scales, and clinical outcomes, we provided a multidimensional evaluation of DEX effects. Nevertheless, several limitations should be noted. First, the retrospective and single-center design introduces inherent risk of bias and limits external validity. Second, the relatively small sample size reduces statistical power, particularly for less frequent outcomes. Third, although PSM minimized confounding, unmeasured factors cannot be fully excluded. Fourth, our analysis was limited to in-hospital outcomes; long-term effects of DEX remain unknown. Finally, physiological differences (eg, small SpO2 variations) may not always reflect clinically meaningful changes. These limitations warrant cautious interpretation of the findings.
Another important limitation of our study is the presence of missing data in some propensity score covariates, which led to the exclusion of 54 patients in the DEX group and 232 patients in the non-DEX group prior to matching. The missingness was primarily related to incomplete documentation of laboratory or clinical variables during the acute care setting. However, the higher exclusion rate in the non-DEX group raises concern that the missing mechanism may not be completely random. This differential missingness could potentially affect covariate balance, reduce representativeness of the matched sample, and introduce selection bias. Although propensity score matching improved comparability between groups, residual confounding related to missing data cannot be fully excluded. Therefore, our findings should be interpreted with caution and considered hypothesis-generating rather than definitive.
Generalizability
Our cohort consisted exclusively of elderly Chinese patients with STEMI. As such, the results may not be generalizable to younger patients or to populations with different ethnic, cultural, or healthcare backgrounds. Further studies in broader, more diverse populations are required to confirm external validity.
Future Directions
Future research should focus on large-scale, multicenter randomized controlled trials to validate our findings and clarify causal mechanisms. Longer follow-up is essential to assess whether DEX confers sustained benefits beyond hospitalization. Additionally, trials in younger and ethnically diverse cohorts would be critical to establish generalizability and explore whether the benefits observed extend across different patient subgroups.
Conclusions
DEX use was associated with lower catecholamine and inflammation levels, and appeared to provide adequate sedation with acceptable safety, feasibility, and effectiveness in older patients with STEMI undergoing primary PCI. DEX use was associated with attenuation of sympathetic activity, stress, and inflammation reactivity, while maintaining arousable sedation. These findings support the effectiveness and safety of DEX in older patients with STEMI undergoing primary PCI.
Data Sharing Statement
People can get a copy of study data by emailing the corresponding author, Dr Ruoxi Zhang, upon reasonable request.
Ethics Approval and Consent to Participate
Ethical approval for this study (Ethical Committee HG-2024-010) was provided by the Research Ethics Committee of Suzhou Kowloon Hospital, Shanghai Jiao Tong University School of Medicine, 118 Wansheng Street, Suzhou Industrial Park, Suzhou, China (Chairperson Prof. Zhengguo Huang) on 21 February 2025. In our institution, written informed consent is routinely obtained from all patients at the time of hospital admission, prior to PCI and any potential administration of dexmedetomidine.
Patient Consent for Publication
Informed consent was obtained from each patient.
Acknowledgments
We would like to thank the members of the medical staff of Suzhou Kowloon Hospital, Shanghai Jiao Tong University School of Medicine for their assistance in the preparation of this paper.
Funding
This research was supported by the 2025 Suzhou Science and Technology Program (Project No. SYW2025088) awarded to Prof. Guang-An Liu.
Disclosure
The authors declare no conflicts of interest.
References
1. Matter MA, Paneni F, Libby P, et al. Inflammation in acute myocardial infarction: the good, the bad and the ugly. Eur Heart J. 2024;45(2):89–103. doi:10.1093/eurheartj/ehad486
2. Seferović PM, Ašanin M, Ristić AD. Acute stress disorder and C-reactive protein in patients with acute myocardial infarction. Eur J Prev Cardiol. 2018;25(7):702–705. doi:10.1177/2047487318761091
3. von Känel R, Abbas CC, Schmid JP, et al. Momentary stress moderates procoagulant reactivity to a trauma-specific interview in patients with posttraumatic stress disorder caused by myocardial infarction. J Psychiatr Res. 2010;44(14):956–963. doi:10.1016/j.jpsychires.2010.03.004
4. Wu LP, Kang WQ. Effect of dexmedetomidine for sedation and cognitive function in patients with preoperative anxiety undergoing carotid artery stenting. J Int Med Res. 2020;48(9):300060520938959. doi:10.1177/0300060520938959
5. Lemon J, Edelman S. Psychological adaptation to ICDs and the influence of anxiety sensitivity. Psychol Health Med. 2007;12(2):163–171. doi:10.1080/13548500500448478
6. Feigin VL, Abate MD, Abate YH, et al. Global, regional, and national burden of stroke and its risk factors, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurol. 2024;23(10):973–1003. doi:10.1016/S1474-4422(24)00369-7
7. Fu W, Xu H, Zhao T, Xu J, Wang F. Effects of dexmedetomidine combined with etomidate on postoperative cognitive function in older patients undergoing total intravenous anaesthesia: a randomized, double-blind, controlled trial. BMC Geriatr. 2024;24(1):97. doi:10.1186/s12877-024-04726-7
8. Wang K, Wu M, Xu J, et al. Effects of dexmedetomidine on perioperative stress, inflammation, and immune function: systematic review and meta-analysis. Br J Anaesth. 2019;123(6):777–794. doi:10.1016/j.bja.2019.07.027
9. Lu J, Chen G, Zhou H, Zhou Q, Zhu Z, Wu C. Effect of parecoxib sodium pretreatment combined with dexmedetomidine on early postoperative cognitive dysfunction in elderly patients after shoulder arthroscopy: a randomized double blinded controlled trial. J Clin Anesth. 2017;41:30–34.
10. Goodwin HE, Gill RS, Murakami PN, Thompson CB, Lewin JJ 3rd, Mirski MA. Dexmedetomidine preserves attention/calculation when used for cooperative and short-term intensive care unit sedation. J Crit Care. 2013;28(6):1113.e7–1113.e10. doi:10.1016/j.jcrc.2013.07.062
11. Hou M, Chen F, He Y, et al. Dexmedetomidine against intestinal ischemia/reperfusion injury: a systematic review and meta-analysis of preclinical studies. Eur J Pharmacol. 2023;959:176090. doi:10.1016/j.ejphar.2023.176090
12. Takahashi K, Yoshikawa Y, Kanda M, Hirata N, Yamakage M. Dexmedetomidine as a cardioprotective drug: a narrative review. J Anesth. 2023;37(6):961–970. doi:10.1007/s00540-023-03261-w
13. Yu Y, Li Y, Han D, et al. Effect of dexmedetomidine on posttraumatic stress disorder in patients undergoing emergency trauma surgery: a randomized clinical trial. JAMA Netw Open. 2023;6(6):e2318611. doi:10.1001/jamanetworkopen.2023.18611
14. Tang J, Chu J, Hou H, et al. Clinical implication of QFR in patients with ST-segment elevation myocardial infarction after drug-eluting stent implantation. Int J Cardiovasc Imag. 2021;37(3):755–766. doi:10.1007/s10554-020-02068-0
15. Mamdani M, Sykora K, Li P, et al. Reader’s guide to critical appraisal of cohort studies: 2. Assessing potential for confounding. BMJ. 2005;330(7497):960–962. doi:10.1136/bmj.330.7497.960
16. Rasheed AM, Amirah MF, Abdallah M, P PJ, Issa M, Alharthy A. Ramsay sedation scale and richmond agitation sedation scale: a cross-sectional study. Dimens Crit Care Nurs. 2019;38(2):90–95. doi:10.1097/DCC.0000000000000346
17. Moerman N, van Dam FS, Muller MJ, Oosting H, van Dam FS. The Amsterdam Preoperative Anxiety and Information Scale (APAIS). Anesth Analg. 1996;82(3):445–451. doi:10.1097/00000539-199603000-00002
18. Bradley SM, Spertus JA, Kennedy KF, et al. Patient selection for diagnostic coronary angiography and hospital-level percutaneous coronary intervention appropriateness: insights from the national cardiovascular data registry. JAMA Intern Med. 2014;174(10):1630–1639. doi:10.1001/jamainternmed.2014.3904
19. Westermann J, Hubl W, Kaiser N, Salewski L. Simple, rapid and sensitive determination of epinephrine and norepinephrine in urine and plasma by non-competitive enzyme immunoassay, compared with HPLC method. Clin Lab. 2002;48(1–2):61–71.
20. Nii K, Hanada H, Hiraoka F, Eto A, Mitsutake T, Tsutsumi M. Usefulness of consciousness sedation with dexmedetomidine and pentazocine during endovascular treatment for acute stroke. Neurol Med Chir. 2018;58(2):79–84. doi:10.2176/nmc.oa.2017-0188
21. Mavridou P, Dimitriou V, Manataki A, Arnaoutoglou E, Papadopoulos G. Patient’s anxiety and fear of anesthesia: effect of gender, age, education, and previous experience of anesthesia. A survey of 400 patients. J Anesth. 2013;27(1):104–108. doi:10.1007/s00540-012-1460-0
22. Djaiani G, Silverton N, Fedorko L, et al. Dexmedetomidine versus propofol sedation reduces delirium after cardiac surgery: a randomized controlled trial. Anesthesiology. 2016;124(2):362–368. doi:10.1097/ALN.0000000000000951
23. Pajoumand M, Kufera JA, Bonds BW, et al. Dexmedetomidine as an adjunct for sedation in patients with traumatic brain injury. J Trauma Acute Care Surg. 2016;81(2):345–351. doi:10.1097/TA.0000000000001069
24. Ren C, Xu H, Xu G, et al. Effect of intraoperative infusion of dexmedetomidine on postoperative recovery in patients undergoing endovascular interventional therapies: a prospective, randomized, controlled trial. Brain Behav. 2019;9(7):e01317. doi:10.1002/brb3.1317
25. Nakano T, Okamoto H. Dexmedetomidine-induced cerebral hypoperfusion exacerbates ischemic brain injury in rats. J Anesth. 2009;23(3):378–384. doi:10.1007/s00540-009-0777-9
26. Huncke TK, Adelman M, Jacobowitz G, Maldonado T, Bekker A. A prospective, randomized, placebo-controlled study evaluating the efficacy of dexmedetomidine for sedation during vascular procedures. Vasc Endovasc Surg. 2010;44(4):257–261. doi:10.1177/1538574410363621
27. Hall JE, Uhrich TD, Barney JA, Arain SR, Ebert TJ. Sedative, amnestic, and analgesic properties of small-dose dexmedetomidine infusions. Anesth Analg. 2000;90(3):699–705. doi:10.1097/00000539-200003000-00035
28. Ebert TJ, Hall JE, Barney JA, Uhrich TD, Colinco MD. The effects of increasing plasma concentrations of dexmedetomidine in humans. Anesthesiology. 2000;93(2):382–394. doi:10.1097/00000542-200008000-00016
29. Kowlgi GN, Cha YM. Management of ventricular electrical storm: a contemporary appraisal. Europace. 2020;22(12):1768–1780. doi:10.1093/europace/euaa232
30. Hanada K, Kinjo T, Yokoyama H, et al. Incidence, predictors, and outcome associated with ventricular tachycardia or fibrillation in patients undergoing primary percutaneous coronary intervention for acute myocardial infarction. Circ J. 2024;88(8):1254–1264. doi:10.1253/circj.CJ-23-0023
31. Rathore SS, Berger AK, Weinfurt KP, et al. Acute myocardial infarction complicated by atrial fibrillation in the elderly: prevalence and outcomes. Circulation. 2000;101(9):969–974. doi:10.1161/01.CIR.101.9.969
32. Walkey AJ, Hogarth DK, Lip GYH. Optimizing atrial fibrillation management: from ICU and beyond. Chest. 2015;148(4):859–864. doi:10.1378/chest.15-0358
33. Zhong Q, Kumar A, Deshmukh A, Bennett C, Guasch E. Dexmedetomidine reduces incidences of ventricular arrhythmias in adult patients: a meta-analysis. Cardiol Res Pract. 2022;2022:5158362. doi:10.1155/2022/5158362
34. Chrysostomou C, Sanchez-de-toledo J, Wearden P, et al. Perioperative use of dexmedetomidine is associated with decreased incidence of ventricular and supraventricular tachyarrhythmias after congenital cardiac operations. Ann Thorac Surg. 2011;92(3):964–972. doi:10.1016/j.athoracsur.2011.04.099
35. Meister RE, Weber T, Princip M, et al. Perception of a hectic hospital environment at admission relates to acute stress disorder symptoms in myocardial infarction patients. Gen Hosp Psychiatry. 2016;39:8–14. doi:10.1016/j.genhosppsych.2015.11.004
36. Milwidsky A, Ziv-Baran T, Letourneau-Shesaf S, et al. CRP velocity and short-term mortality in ST segment elevation myocardial infarction. Biomarkers. 2017;22(3–4):383–386. doi:10.1080/1354750X.2017.1279218
37. Helfricht S, Landolt MA, Moergeli H, Hepp U, Wegener D, Schnyder U. Psychometric evaluation and validation of the German version of the acute stress disorder scale across two distinct trauma populations. J Trauma Stress. 2009;22(5):476–480. doi:10.1002/jts.20445
38. Ridker PM, Cook N. Clinical usefulness of very high and very low levels of C-reactive protein across the full range of Framingham risk scores. Circulation. 2004;109(16):1955–1959. doi:10.1161/01.CIR.0000125690.80303.A8
39. Ginzburg K, Kutz I, Koifman B, et al. Acute stress disorder symptoms predict all-cause mortality among myocardial infarction patients: a 15-year Longitudinal Study. Ann Behav Med. 2016;50(2):177–186. doi:10.1007/s12160-015-9744-x
40. Heffner KL, Waring ME, Roberts MB, Eaton CB, Gramling R. Social isolation, C-reactive protein, and coronary heart disease mortality among community-dwelling adults. Soc Sci Med. 2011;72(9):1482–1488. doi:10.1016/j.socscimed.2011.03.016
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Serum IL-38 Level Was Associated with Incidence of MACE in the STEMI Patients

Lu C, Zhou F, Xian H, Sun S, Yue J, Zhang Y, Zhao Q, Luo X, Li Y
International Journal of General Medicine 2023, 16:2987-2997
Published Date: 12 July 2023
Analgesic and Hemodynamic Effects of Dexmedetomidine–Ketamine vs Fentanyl–Ketamine in Healthy Volunteers: A Randomized Trial
Green M, Hayley AC, Downey LA, Keane M, Kenneally ME, Chakravarthy K, Shehabi Y
Journal of Pain Research 2025, 18:2483-2496
Published Date: 16 May 2025
Impact of Dexmedetomidine on Hospital and Intensive Care Unit Stay Duration in Adult Traumatic Brain Injury Patients: A Systematic Review
Alaifan T, Sakhakhni A, Khojah A, Alraddadi EA, Alkhaibary A, Alqahtani AM
Drug, Healthcare and Patient Safety 2025, 17:157-171
Published Date: 11 July 2025
Intranasal Dexmedetomidine with Propofol Provides Superior Sedation for Pediatric Contrast-Enhanced CT: A Randomized Controlled Trial
Zhang SJ, Weng YJ, Lei Q, Lin MY, Chen HL, Fang TF, Lu GL
Drug Design, Development and Therapy 2025, 19:9523-9532
Published Date: 24 October 2025
Dexmedetomidine Dosing Strategies in Sedation and Anesthesia: Pharmacokinetics, Safety, and Clinical Applications — A Narrative Review
Tsai YF, Shih TH, Ho JS, Wu SC
Drug Design, Development and Therapy 2026, 20:606156
Published Date: 28 May 2026