Back to Journals » International Journal of Women's Health » Volume 17
Development of an Interpretable Machine Learning Model to Predict Pregnancy Outcomes Following Cervical Cerclage
Authors Jin J, Zhong W, Sun J, Chen Z
Received 9 August 2025
Accepted for publication 5 November 2025
Published 21 November 2025 Volume 2025:17 Pages 4723—4735
DOI https://doi.org/10.2147/IJWH.S559585
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Jiaxi Jin,* Wan Zhong,* Jingli Sun, Zhenyu Chen
Department of Obstetrics and Gynecology, General Hospital of Northern Theater Command, Shenyang, Liaoning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhenyu Chen, Email [email protected]
Purpose: Cervical insufficiency is a major cause of spontaneous preterm birth. Although McDonald cerclage improves outcomes, adverse events remain frequent. Accurate prediction of post-cerclage outcomes is essential for individualized management. Machine learning (ML) may enhance risk stratification, but clinical evidence remains limited.
Patients and Methods: We retrospectively analyzed 462 pregnant women who underwent McDonald cerclage at the Department of Obstetrics and Gynecology, General Hospital of Northern Theater Command, from June 2021 to June 2024. Clinical, obstetric, and laboratory parameters were incorporated into multiple ML models, including logistic regression, random forest (RF),support vector machines (SVM), decision trees (DT), and extreme gradient boosting (XGBoost). Model performance was evaluated using discrimination, calibration, and clinical utility, with SHAP analysis applied to interpret predictor contributions.
Results: Logistic regression achieved the highest discrimination (AUC = 0.796), while XGBoost provided the best precision–recall balance (F1 = 0.712). RF demonstrated the most balanced performance, combining robust accuracy, interpretability, and reliability. SHAP analysis identified elevated C-reactive protein, increased white blood cell count, and amniotic fluid sludge as the strongest predictors. Conception method, maternal weight, and cerclage subtype also contributed to risk.
Conclusion: The RF model provided a clinically useful and interpretable framework for predicting outcomes after cerclage, emphasizing inflammatory status, maternal characteristics, and cerclage indication as key determinants of preterm birth. An online prediction tool was developed to facilitate individualized risk assessment. Despite the retrospective, single-center design and lack of external validation, these findings support the integration of ML into clinical decision-making, and warrant multicenter prospective validation.
Plain Language Summary: Interpretable machine learning models, particularly the random forest, can accurately predict pregnancy outcomes following McDonald cerclage. An online prediction platform based on the model enables individualized risk assessment and supports personalized clinical management in high-risk pregnancies.
Keywords: machine learning, cervical cerclage, pregnancy outcomes, SHAP, predictive modeling
Introduction
Cervical insufficiency (CIC) is a clinically significant obstetric condition characterized by painless cervical dilatation during the second or early third trimester of pregnancy, which can lead to premature rupture of membranes, pregnancy loss, or spontaneous preterm birth. Epidemiological studies estimate that CIC accounts for approximately 8–15% of all preterm birth etiologies.The pathogenesis of CIC remains multifactorial and incompletely understood, with proposed mechanisms including congenital cervical structural abnormalities, acquired trauma from repeated cervical procedures (e.g.surgical dilatation and curettage, cervical conization), and intrauterine inflammation.1
Cervical cerclage remains the mainstay intervention for preventing preterm birth in women diagnosed with CIC. Among the available techniques,the McDonald cerclage—introduced in 1957—continues to be widely used due to its procedural simplicity, minimal invasiveness, and avoidance of cervical tissue dissection.2 Although cerclage improves perinatal outcomes in selected populations, adverse events such as infection, vaginal bleeding, and recurrent preterm birth still occur despite timely intervention. These challenges underscore the need for improved risk stratification and prognostic tools tailored to individual patient profiles.3
The integration of machine learning (ML) techniques into clinical research presents an opportunity to enhance predictive modeling in obstetrics. Algorithms such as random forests, support vector machines (SVM), and decision trees are capable of managing high-dimensional and non-linear clinical datasets, enabling the detection of complex feature interactions and prioritization of relevant predictors. Previous studies have demonstrated the potential of ML in predicting obstetric complications, including gestational diabetes mellitus,4 preeclampsia,5 and preterm labor risk stratification.6 However, to date, limited research has been conducted on the application of ML approaches to predict pregnancy outcomes following McDonald cerclage in women with CIC.
This study aims to construct a clinically interpretable ML-based model for predicting pregnancy outcomes following cervical cerclage. By incorporating SHAP-based model explanation and visualization tools, we seek to identify and quantify the impact of individual clinical variables on pregnancy outcome. This approach may offer a practical, evidence-based decision support framework to guide personalized clinical management and improve outcomes in this high-risk population.
Materials and Methods
This retrospective cohort study included pregnant women diagnosed with cervical insufficiency (CIC) who underwent McDonald cervical cerclage at the Department of Obstetrics and Gynecology, General Hospital of the Northern Theater Command, between June 2021 and June 2024. Clinical data were obtained from the hospital’s electronic medical record system. A total of 462 patients who met the eligibility criteria were included in the final analysis.
Inclusion criteria were as follows: (1) a diagnosis of CIC based on standard clinical criteria; (2) maternal age between 20 and 42 years; and (3) availability of complete clinical records.
Exclusion criteria included: (1) congenital uterine malformations; (2) severe systemic diseases (eg cardiovascular disease, hepatic or renal insufficiency, malignancy, major trauma); (3) known fetal structural anomalies; (4) contraindications to cervical cerclage; and (5) pregnancy complications such as intra-amniotic infection, placenta previa, or umbilical cord prolapse.
This retrospective study was approved by the Ethics Committee of the General Hospital of the Northern Theater of Operations of the Chinese People’s Liberation Army (Approval No. Y [2024] 299). The requirement for informed consent was waived by the committee due to the retrospective nature of the study, and all procedures were conducted in accordance with the Declaration of Helsinki. Patient data confidentiality was strictly maintained.
Data Collection and Variable Definitions
Demographic, clinical, and obstetric data were collected and structured for analysis. Variables included:
- Maternal baseline characteristics: age, pre-pregnancy body mass index (BMI), prenatal BMI, gestational weight gain, gravidity, parity, history of early miscarriage, mid-trimester induced abortion, preterm delivery, and prior cervical cerclage.
- Conception method: spontaneous conception, ovulation induction, or embryo transfer.
- Pregnancy comorbidities: gestational diabetes mellitus (GDM), hypertensive disorders of pregnancy (HDP), and polycystic ovary syndrome (PCOS).
- Imaging and infection indicators: cervical length, morphology, presence of bulging membranes, amniotic fluid sludge (AFS), abnormal vaginal discharge, and laboratory parameters reflecting infection status.
- Cerclage details: gestational age at cerclage and Timing of cerclage.
- Pregnancy outcomes: cerclage-to-delivery interval (days), gestational age at delivery, delivery mode (vaginal or cesarean), incidence of premature rupture of membranes (PROM), neonatal survival, neonatal intensive care unit (NICU) admission, birth weight, and Apgar scores at 1 and 5 minutes.
Statistical Analysis
All statistical analyses were performed using R version 4.4.1. For continuous variables, normality was assessed using the Shapiro–Wilk test. Normally distributed variables were presented as means ± standard deviation (SD) and compared using the independent-samples t-test. Non-normally distributed data were expressed as medians with interquartile ranges (IQR) and compared using the Wilcoxon rank-sum test. Categorical variables were reported as frequencies and percentages and compared using the Chi-square or Fisher’s exact test, as appropriate. A two-sided p value < 0.05 was considered statistically significant.
Machine Learning Model Development
Five machine learning models—logistic regression (LR), random forest (RF), support vector machines (SVM), decision tree (DT), and extreme gradient boosting (XGBoost)—were developed to predict pregnancy outcomes following cervical cerclage. Participants were classified as preterm (<37 weeks) or term (≥37 weeks), and the dataset was randomly split into training (80%) and validation (20%) sets.
Models were implemented using the caret package with 10-fold cross-validation and SMOTE oversampling to address class imbalance. SVM used a radial basis function kernel, with tuning of C and σ (tuneLength = 3) and probability prediction enabled. RF employed 500 trees, with mtry searched over five values between 2 and √p (p = number of predictors). LR applied α = 0, 0.5, and 1, with λ logarithmically spaced from 10−4 to 10−1; predictors were standardized and outcomes modeled with a binomial distribution. DT tuned cp from 0.001 to 0.05, with maximum depth 30 and minimum split size 20. XGBoost parameters included nrounds = 100, max depth = 3, learning rate = 0.1, γ = 0, min_child_weight = 1, subsample = 0.7, colsample_bytree = 0.7, using a binary logistic objective.
Model performance was assessed using accuracy, precision, recall, F1-score, and area under the receiver operating characteristic curve (AUC), with AUC <0.6, 0.6–0.8, and >0.8 indicating low, moderate, and high predictive value, respectively. Calibration curves were used to evaluate agreement between predicted probabilities and observed outcomes.
Model Interpretability with SHAP Analysis
To address the lack of interpretability inherent to complex ML models, the SHAP framework was employed. SHAP, based on cooperative game theory, calculates the marginal contribution of each feature to the prediction outcome, allowing both global and local interpretability.
SHAP analysis was implemented in R, providing a visual framework for understanding the influence and directionality of each clinical variable. Summary plots, dependence plots, and force plots were used to illustrate the importance of key features and their interactions, thereby enhancing the clinical interpretability and potential applicability of the predictive model in real-world settings.
Results
Baseline Characteristics of Term and Preterm Groups
A total of 462 patients were included in the study, comprising 334 in the term delivery group and 128 in the preterm delivery group. Baseline characteristics of the two groups are summarized in Table 1. Statistically significant differences were observed between the two groups in terms of parity, gestational weight gain, twin pregnancies, and conception method (P < 0.05). No significant differences were found in age, height,pre-pregnancy BMI, BMI at delivery, gravidity, history of early and mid-trimester miscarriage, ≥2 mid-to-late miscarriages or preterm births, History of previouscervical cerclage, gestational diabetes mellitus (GDM), or hypertensive disorders of pregnancy (P > 0.05). (Table 1).
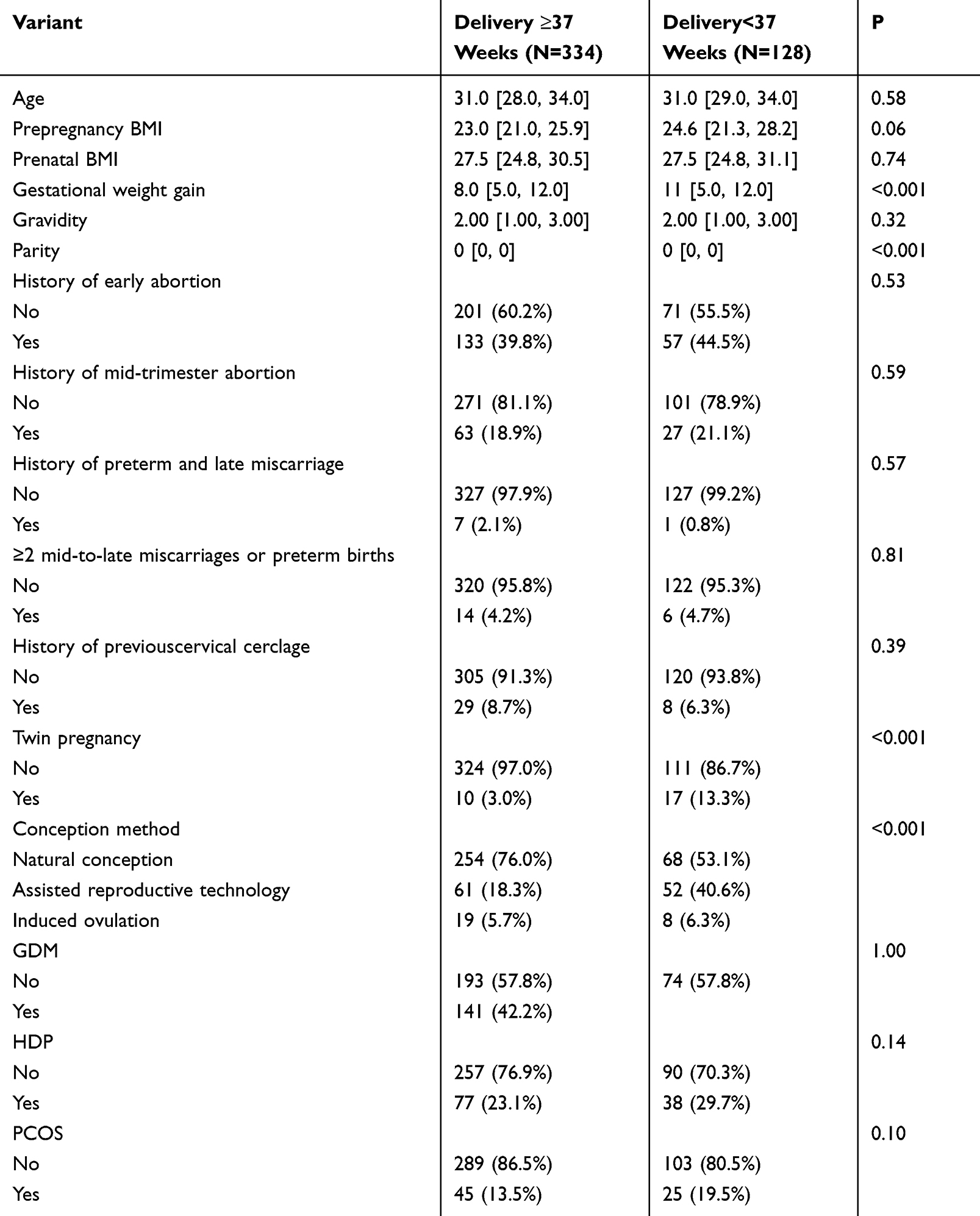 |
Table 1 Comparison of Baseline Characteristics Between Term and Preterm Delivery Groups |
Cervical Ultrasound Findings and Infection Markers
Ultrasound and laboratory parameters are summarized in Table 2. Cervical length, gestational age at cerclage, indication for cerclage, presence of amniotic sac bulging (ASB), cervical funneling, white blood cell count (WBC), and elevated C-reactive protein (CRP > 5 mg/L) differed significantly between groups (P < 0.05). No statistically significant differences were found in the presence of amniotic fluid sludge (AFS) or abnormal vaginal secretions (P > 0.05). (Table 2).
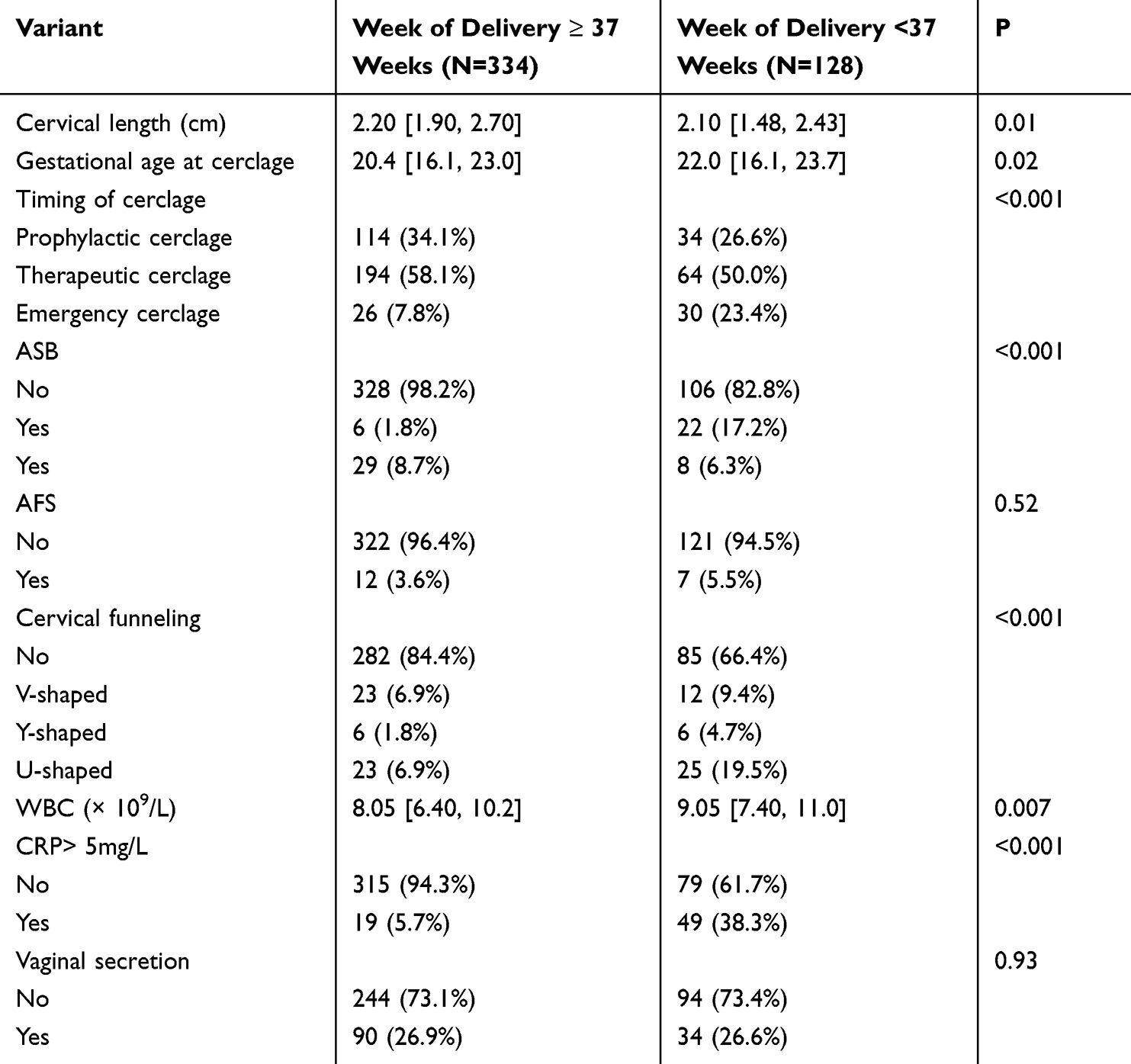 |
Table 2 Comparison of Cervical Ultrasound Findings and Infection-Related Laboratory Markers |
Pregnancy Outcomes
As shown in Table 3, significant differences were observed between groups in the interval between cerclage and delivery, incidence of premature rupture of membranes (PROM), neonatal birth weight, neonatal intensive care unit (NICU) admission rate, and 1- and 5-minute Apgar scores (all P < 0.05). Delivery mode did not differ significantly (P = 0.06). (Table 3).
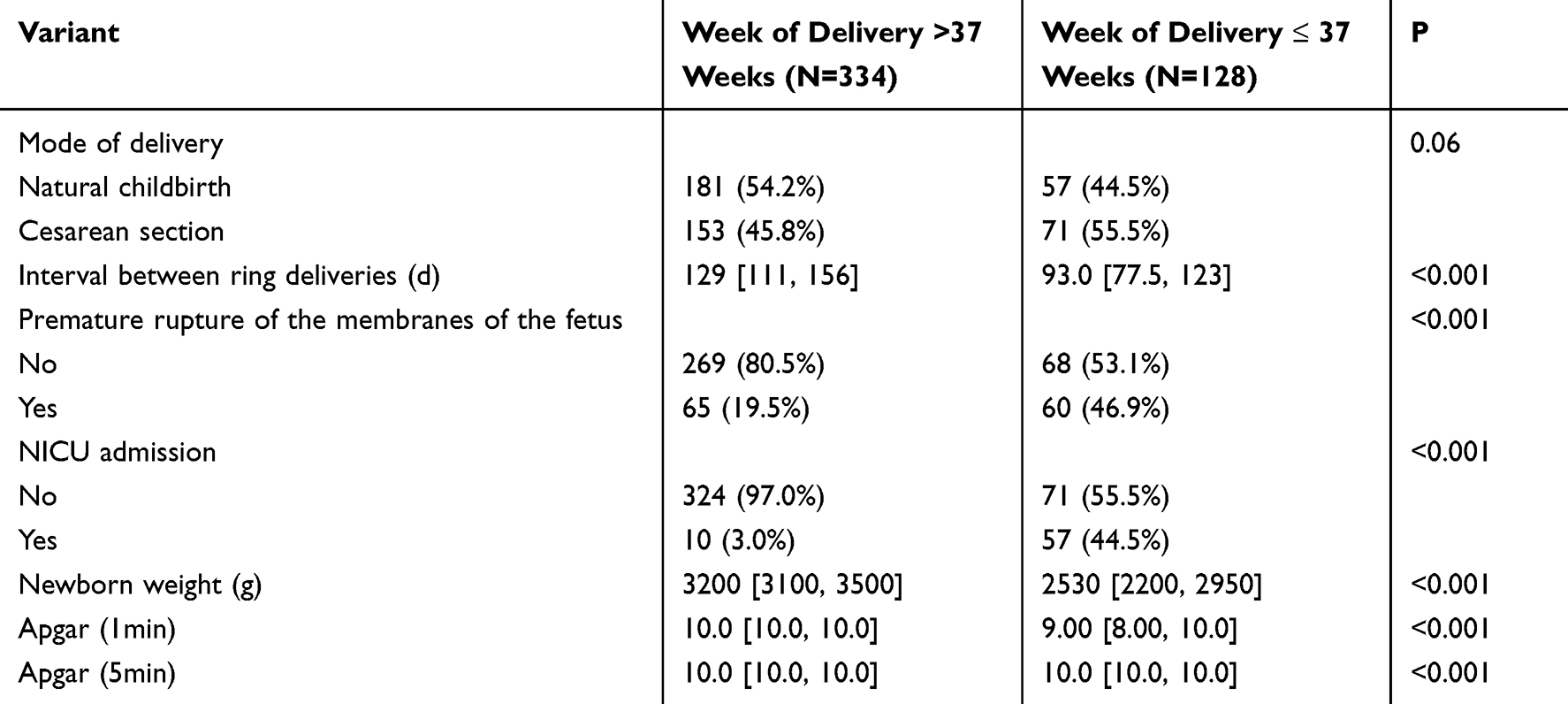 |
Table 3 Comparison of Pregnancy Outcomes Between Term and Preterm Groups |
Machine Learning Model Performance
Using 10-fold cross-validation and LASSO regression for feature selection, 29 optimal variables were retained for model construction. These included pre-pregnancy BMI, mode of delivery, AFS, gravidity, parity, history of early abortion, mid-trimester induction, recurrent miscarriage or preterm birth, cervical length, gestational age at cerclage, interval from cerclage to delivery, ASB, CRP, conception method, GDM, gestational hypertension, PCOS, cervical funneling, cervical laceration, bleeding volume, NICU admission, neonatal weight, Apgar scores, among others.
Five predictive models were evaluated for their performance. Logistic regression achieved the highest AUC (0.796) with high specificity (0.939) and a balanced F1-score (0.679). Decision Tree showed comparable discrimination (AUC 0.769) with slightly higher sensitivity (0.606). Random Forest reached the highest specificity (0.955) but had lower sensitivity (0.485). XGBoost demonstrated a balanced profile with relatively high sensitivity (0.636) and the highest F1-score (0.712). SVM showed moderate performance overall (AUC 0.740, specificity 0.818, F1-score 0.615). (Table 4).
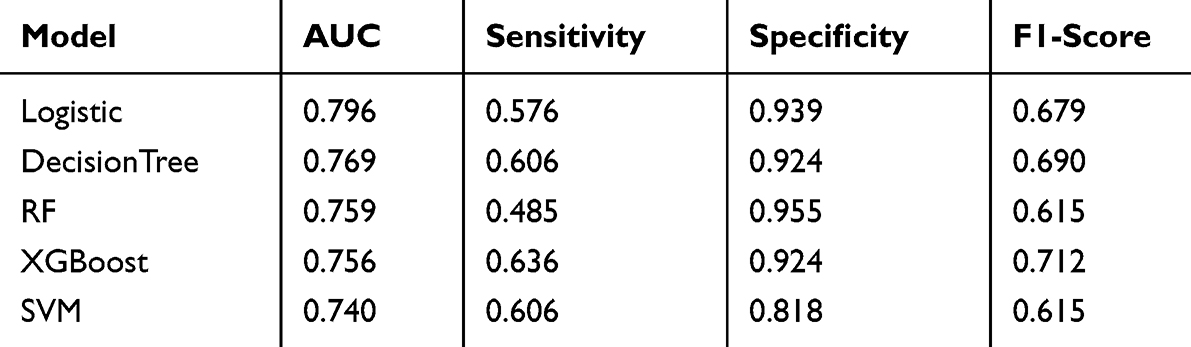 |
Table 4 Performance Metrics of Five Machine Learning Models in Predicting Preterm Birth |
Model Calibration and Clinical Utility
Model performance was evaluated in three aspects. Discriminative ability was assessed using Receiver Operating Characteristic (ROC) analysis, with the area under the curve (AUC) indicating the model’s ability to distinguish between high- and low-risk patients (Figure 1). Calibration was examined using calibration curves to assess the agreement between predicted and observed outcomes (Figure 2). Clinical utility was evaluated via Decision Curve Analysis (DCA), demonstrating the net benefit of the model across different threshold probabilities (Figure 3).
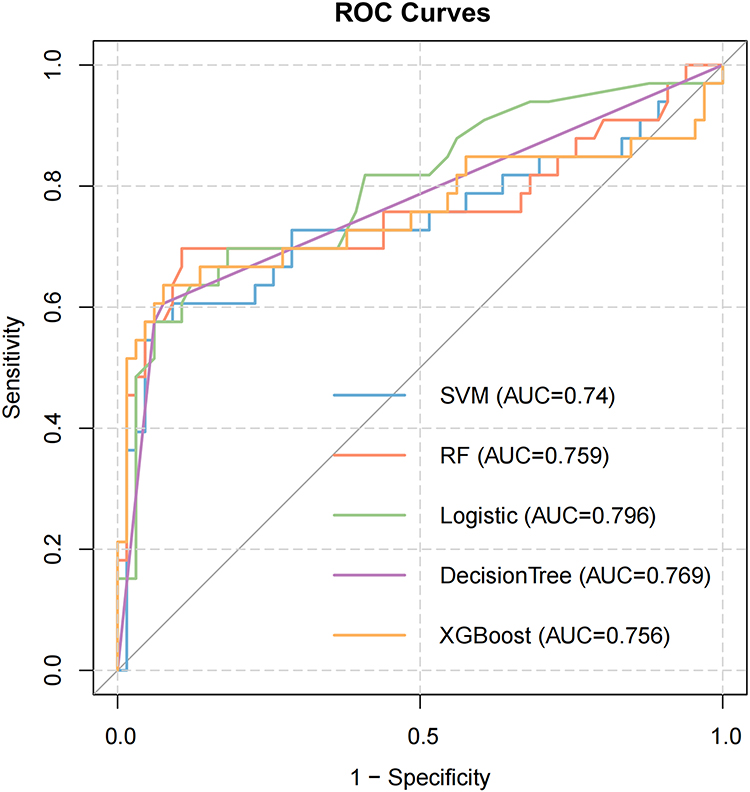 |
Figure 1 ROC curves of the five models. |
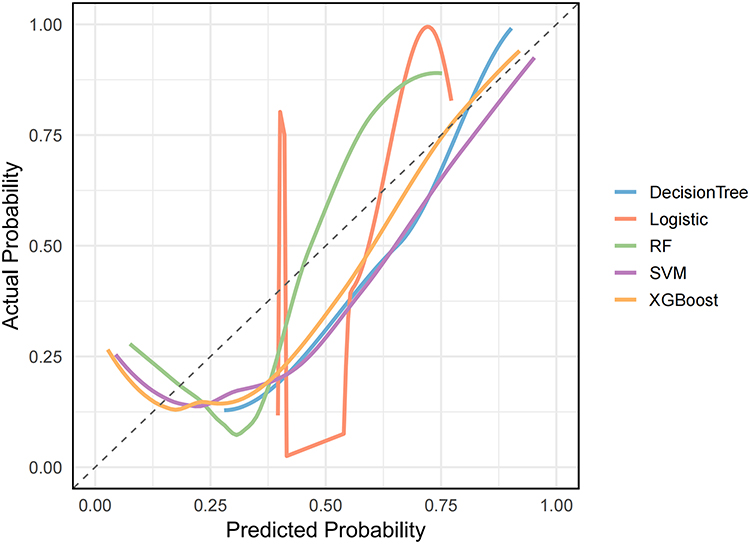 |
Figure 2 Calibration curves of the five machine learning models. |
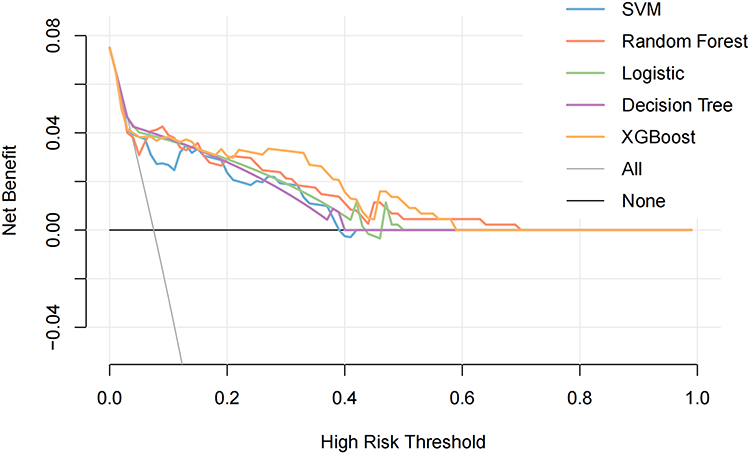 |
Figure 3 Decision curve analysis (DCA) of the five models. |
Model Interpretation
SHAP was used to interpret model outputs and determine feature importance. SHAP summary plots (Figures 4–8) illustrate the impact of each variable on model predictions.
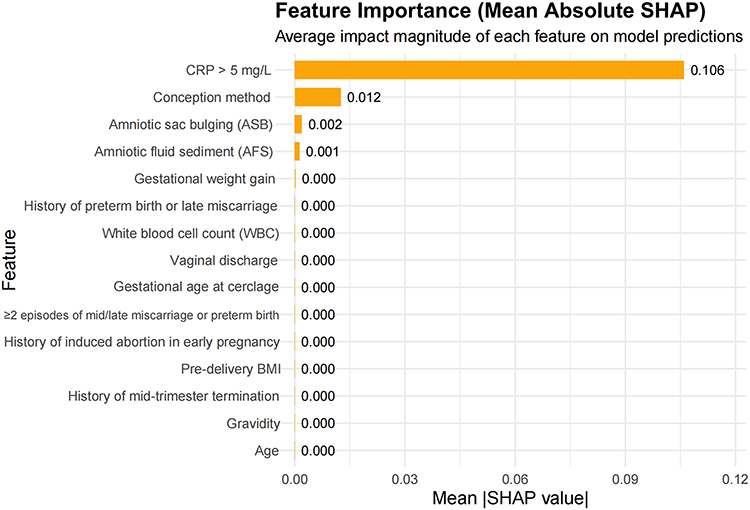 |
Figure 4 SHAP summary plot for the Logistic Regression model. |
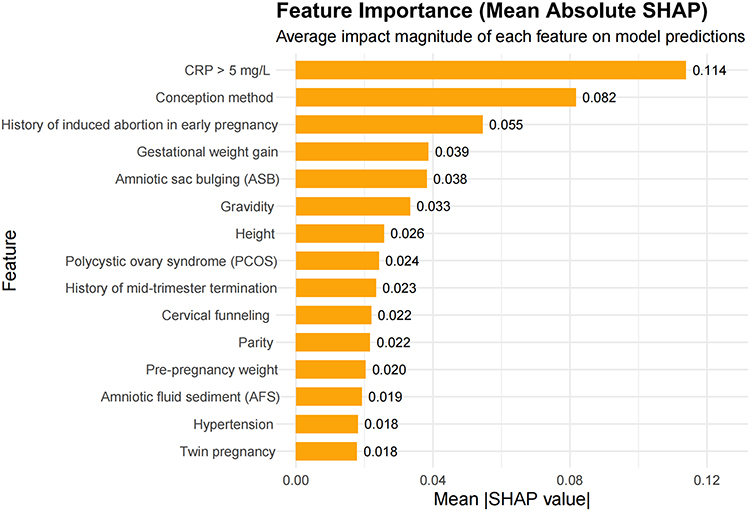 |
Figure 5 SHAP summary plot for the Support Vector Machine (SVM) model. |
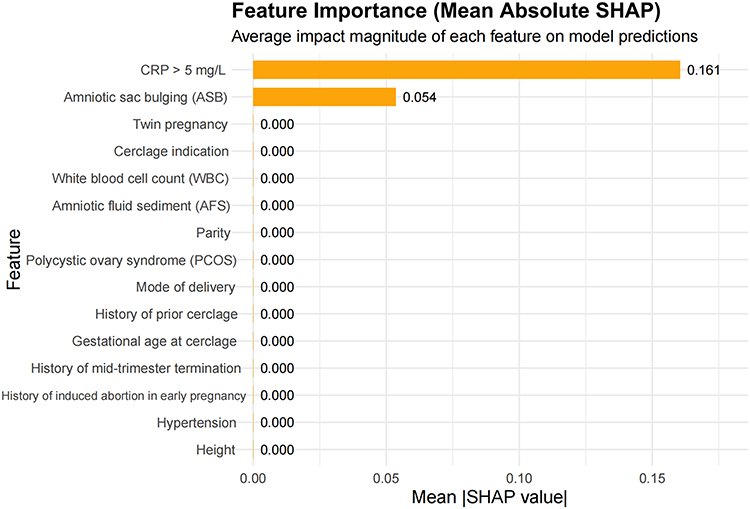 |
Figure 6 SHAP summary plot for the Decision Tree model. |
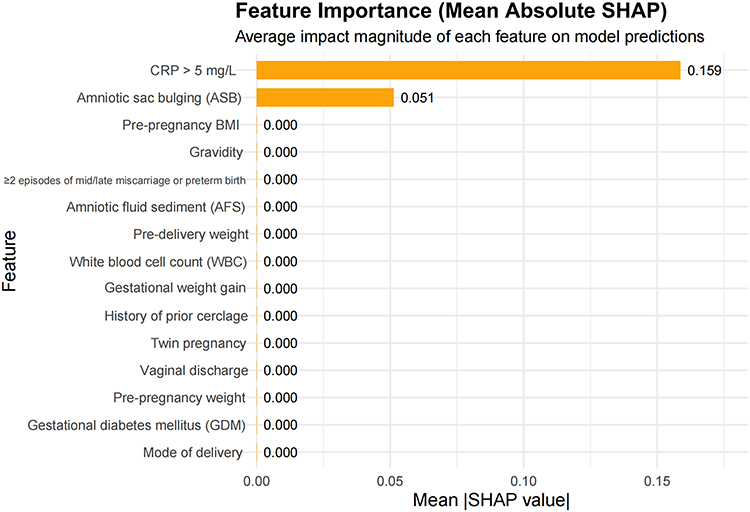 |
Figure 7 SHAP summary plot for the XGBoost model. |
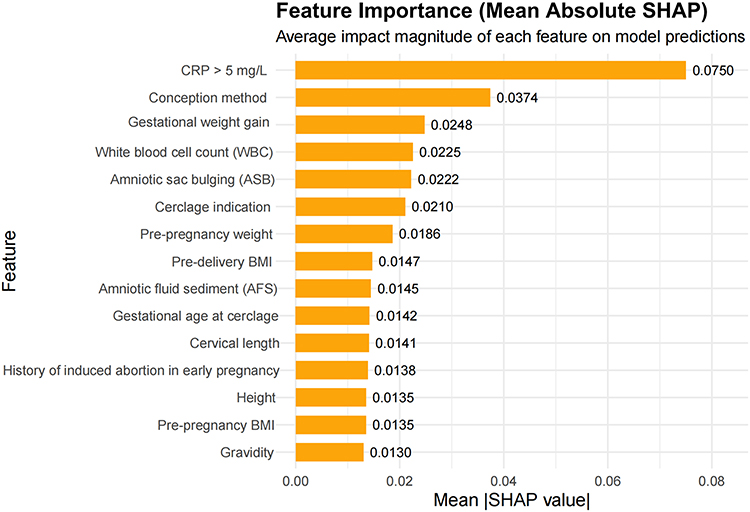 |
Figure 8 SHAP summary plot for the Random Forest (RF) model. |
Web-Based Calculator
To facilitate the clinical translation of the optimal prediction model, the final Random Forest model was deployed as an intuitive, web-based calculator using the R Shiny framework. This application allows clinicians to input easily obtainable patient-specific clinical variables. Upon submission, the platform returns a personalized probability of an adverse pregnancy outcome following McDonald cerclage, providing immediate decision support at the point of care.The web application can be accessed online at the following link: https://breakingdawn.shinyapps.io/rfmodel/.
Discussion
Cervical cerclage remains a fundamental intervention for managing cervical insufficiency, significantly reducing the risk of mid-trimester miscarriage and spontaneous preterm birth.7 In this retrospective analysis involving 462 patients undergoing cerclage, the overall incidence of preterm birth was 27.7%, with a comparable rate of 26.6% observed in those receiving prophylactic cerclage. These findings are consistent with previously published data, including a retrospective study reporting a 30.1% preterm birth rate in patients undergoing prophylactic transvaginal cerclage.8 Multiple machine learning (ML) models were developed to predict post-cerclage pregnancy outcomes. Logistic regression demonstrated the highest overall discrimination (AUC = 0.796), while XGBoost achieved the best balance between precision and recall (F1 = 0.712). Nevertheless, when considering predictive accuracy, clinical utility, interpretability, and reliability together, the Random Forest (RF) model showed the most balanced performance, supporting its application as a clinical decision-support tool.
SHAP analysis of the RF model highlighted the relative contributions of individual predictors for post-cerclage pregnancy outcomes. C-reactive protein (CRP >5 mg/L) emerged as the most prominent predictor (SHAP value = 0.075). Elevated CRP, together with increased white blood cell (WBC) count, underscore the critical role of maternal inflammatory status in determining pregnancy outcomes. Amniotic fluid sludge (AFS) has also been reported as an independent predictor of preterm birth,9 and its predictive value, along with CRP and WBC, supports a central role of intrauterine infection or inflammation. AFS positivity generally indicates more advanced or severe infection, whereas serum markers such as CRP may rise earlier and be more sensitive, suggesting that CRP can provide predictive value at an earlier stage and in a broader range of patients. Although the utility of CRP for predicting intra-amniotic infection remains debated, prior studies indicate that elevated maternal serum CRP may serve as a non-invasive surrogate for occult infection in selected cases.10,11 Early postoperative elevations in CRP and procalcitonin have also been associated with developing infections after cerclage.12 Interestingly, abnormal vaginal discharge was not significantly correlated with outcomes, likely due to standardized postoperative antibiotic prophylaxis, consistent with previous studies showing that vaginal microbial status after cerclage is not independently predictive of gestational duration.13,14
Assisted reproductive or induced ovulation technologies were notably more prevalent among patients who experienced preterm birth, reinforcing the mechanical and hormonal stressors implicated in cervical insufficiency.15 Conception method,pre-pregnancy weight, and gestational weight gain. Although traditional high-risk factors such as gestational diabetes mellitus (GDM) and hypertensive disorders of pregnancy (HDP) did not differ significantly between groups, both were associated with maternal weight16 and conception method.17 This suggests that isolated metabolic disorders may not be the primary drivers of early preterm birth following cervical cerclage, while baseline maternal characteristics and conception method provide stronger independent predictive signals.
Regarding cerclage subtype, particularly U-cerclage and abdominal cerclage (ABS), these were associated with poorer pregnancy outcomes, reflecting greater cervical compromise at the time of intervention. Xiao et al18 classified cerclage into four subtypes based on cervical dilation and membrane prolapse at surgery, corresponding in our study to V-, Y-, U-type cervix, and ABS. U-type cervix and ABS are typically performed as emergency procedures in the presence of cervical dilation or membrane prolapse. Cervical shortening and funneling indicate impaired structural integrity, with thinning and reduced elasticity of cervical tissue, which increases the risk of post-cerclage preterm birth and adverse pregnancy outcomes. This clinical observation was supported by our Random Forest model, in which cerclage indication—a variable reflecting the severity of cervical compromise—emerged as a significant predictor (SHAP value = 0.021). These findings highlight the importance of considering cerclage subtype and indication when assessing post-procedure risk and planning individualized management for high-risk patients.
While transvaginal ultrasound remains the primary method for assessing cervical length, its predictive value beyond 24 weeks in singleton pregnancies may be limited.19 In our cohort, cervical length still significantly distinguished term from preterm outcomes, underscoring its relevance in risk stratification.20 SHAP analysis indicated that cervical length (SHAP value = 0.014), though less influential than inflammatory markers, contributed meaningfully to the RF model, supporting its role as part of a multifactorial assessment rather than a standalone predictor. Importantly, recent advances using deep learning–based ultrasound models have demonstrated superior predictive performance for preterm birth compared with conventional cervical length measurements.21 These findings reinforce that machine learning approaches can provide a more precise, integrative evaluation of prognosis following cervical cerclage, highlighting the potential of AI-assisted risk stratification in clinical practice.
Limitations and Future Directions
This study has several limitations. First, it was a retrospective, single-center study, which may restrict the generalizability of the findings to broader populations and different clinical settings. Second, although we applied SMOTE oversampling to mitigate the issue of class imbalance between favorable and adverse pregnancy outcomes, residual imbalance may still have influenced model stability and limited its predictive accuracy. Third, external validation was not conducted, further constraining the applicability of the model to diverse populations. To partially address this gap, we developed an online prediction tool that enables real-time assessment of preterm birth risk and provides a platform for future external validation. In addition, continuous cervical parameters, such as elastography or dynamic length changes, were not available in this dataset, which may have reduced the precision of risk estimation. Future multicenter, prospective studies with larger and more balanced datasets, integrating comprehensive cervical function measures and inflammatory biomarkers, are warranted to improve model robustness, enhance interpretability, and ensure broader clinical utility.
Conclusion
In summary, this study developed and evaluated multiple machine learning models to predict pregnancy outcomes in women with cervical insufficiency undergoing McDonald cerclage. Among the models, the random forest (RF) model demonstrated the most balanced overall performance, combining high specificity, reasonable sensitivity, and robust interpretability, making it particularly suitable for clinical risk stratification. Logistic regression and XGBoost also showed strong predictive capability, but RF offered the advantage of capturing complex nonlinear relationships and interactions among predictors.
SHAP analysis highlighted that maternal inflammatory status, particularly elevated CRP and WBC, along with amniotic fluid sludge, conception method, maternal weight, and cerclage type, are key determinants of post-cerclage pregnancy outcomes. These findings support the central role of intrauterine infection and maternal baseline characteristics in preterm birth risk. Traditional indicators such as cervical length and gestational age at cerclage remain relevant but provide complementary information within a multifactorial risk assessment framework.
Despite the study’s retrospective, single-center design and lack of external validation, the development of an online prediction tool offers practical guidance for individualized risk assessment. Future multicenter, prospective studies incorporating dynamic cervical parameters and additional inflammatory biomarkers are warranted to further validate and refine predictive models. Overall, our findings provide a robust, interpretable framework, with RF modeling offering particular advantage, to support personalized clinical decision-making and optimize pregnancy outcomes following cervical cerclage.
Abbreviations
LR, logistic regression; RF, random forest; SVM, support vector machine; DT, decision tree; XGboost, extreme gradient boosting; DCA, decision curve analysis; SHAP, shapley additive explanations; CIC, cervical insufficiency; ML, machine learning; GDM, gestational diabetes mellitus; BMI, body mass index; HDP, hypertensive disorders of pregnancy; PCOS, polycystic ovary syndrome; AFS, amniotic fluid sludge; ASB, amniotic sac bulging; PROM, premature rupture of membranes; NICU, neonatal intensive care unit.
Data Sharing Statement
The codes and original datasets used in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Ethical approval for this study was granted by the Ethics Committee of General Hospital of the Northern Theater of Operations of the Chinese People’s Liberation Army (also called by: General Hospital of Northern Theater Command), (No. Y [2024] 299). Informed consent was waived by our Institutional Review Board because of the retrospective nature of our study. All procedures were performed in accordance with the relevant ethical standards.”
Ethical approval for this study was granted by Ethics Committee of General Hospital of the Northern Theater of Operations of the Chinese People’s Liberation Army (No. Y [2024] 299). Informed consent was waived by our Institutional Review Board because of the retrospective nature of our study. All procedures were performed in accordance with the relevant ethical standards.
Consent for Publication
The manuscript is approved by all authors for publication.
Author Contributions
All authors have made substantial contributions to this study, including the conception, study design, data acquisition, analysis, and interpretation. All authors were involved in drafting, revising, or critically reviewing the manuscript, and approved the final version. They have agreed on the target journal, reviewed all versions prior to submission, during revision, and at the proof stage, and consented to any significant changes introduced. All authors accept responsibility and accountability for the content of the article.
Funding
This work was supported by the Shenyang Science and Technology Research Funding Program (22-321-33-31).
Disclosure
The authors declare no competing interests.
References
1. American College of Obstetricians and Gynecologists. Cerclage for the management of cervical insufficiency. acog practice bulletin No. 142. Obstet & Gynecol. 2014;123(2):372–379. doi:10.1097/01.AOG.0000443276.68274.cc
2. Harger JH. Cerclage and cervical insufficiency: an evidence-based analysis. Obstetrics Gynecol. 2002;100(6):1313–1327. doi:10.1016/s0029-7844(02)02365-7
3. Mcdonald SD, Murphy KE. Suture choice for cervical cerclage. Lancet. 2022;400(10361):1385–1387. doi:10.1016/S0140-6736(22)01973-0
4. Kang BS, Lee SU, Hong S, et al. Prediction of gestational diabetes mellitus in Asian women using machine learning algorithms. Scientific Rep. 2023;13(1):13356. doi:10.1038/s41598-023-39680-8
5. Ranjbar A, Montazeri F, Ghamsari SR, et al. Machine learning models for predicting preeclampsia: a systematic review[J/OL]. BMC Pregnanc Childbirth. 2024;24(1):6. doi:10.1186/s12884-023-06220-1
6. Lee SJ, Garcia GGP, Stanhope KK, et al. Interpretable machine learning to predict adverse perinatal outcomes: examining marginal predictive value of risk factors during pregnancy. Am J Obstetrics Gynecol MFM. 2023;5(10):101096. doi:10.1016/j.ajogmf.2023.101096
7. Althuisius SM, Dekker GA, Van Geijn HP, et al. Cervical incompetence prevention randomized cerclage trial (CIPRACT): study design and preliminary results. Am J Obstetrics Gynecol. 2000;183(4):823–829. doi:10.1067/mob.2000.108874
8. Huang G, Deng C, Liao H, et al. Comparison of transvaginal cervical cerclage versus laparoscopic abdominal cervical cerclage in cervical insufficiency: a retrospective study from a single centre. BMC Pregnancy Childbirth. 2022;22:773. doi:10.1186/s12884-022-05108-w
9. Pergialiotis V, Bellos I, Antsaklis A, et al. Presence of amniotic fluid sludge and pregnancy outcomes: a systematic review. Acta Obstetricia Et Gynecologica Scandinavica. 2020;99(11):1434–1443. doi:10.1111/aogs.13893
10. Park H, Park KH, Kim YM, et al. Plasma inflammatory and immune proteins as predictors of intra-amniotic infection and spontaneous preterm delivery in women with preterm labor: a retrospective study. BMC Pregnancy Childbirth. 2018;18(1):146. doi:10.1186/s12884-018-1780-7
11. Jung EY, Park KH, Lee SY, et al. Non-invasive prediction of intra-amniotic infection and/or inflammation in patients with cervical insufficiency or an asymptomatic short cervix (≤15 mm). Archiv Gynecol Obstetrics. 2015;292(3):579–587. doi:10.1007/s00404-015-3684-3
12. Fan X, Ma Y, Zhu Y, et al. The potential presence of infection may be indicated through non-invasive prediction of procalcitonin and C-reactive protein levels within the initial three days after cervical cerclage: a retrospective case-control study. BMC Pregnanc Childbirth. 2024;24(1):474. doi:10.1186/s12884-024-06668-9
13. Seys E, Page AS, Deprest J, et al. Urogenital cultures and preterm birth in women with cervical cerclage: a single center retrospective cohort study. BMC Pregnanc Childbirth. 2024;24(1):324. doi:10.1186/s12884-024-06509-9
14. Steetskamp J, Zander M, Laufs V, et al. Does vaginal bacterial colonization contribute to preterm birth in women with asymptomatic shortened cervix?. Archiv Gynecol Obstetrics. 2024;310(1):121–127. doi:10.1007/s00404-024-07397-2
15. Liu Y, Chen M, Cao T, et al. Cervical cerclage in twin pregnancies: an updated systematic review and meta-analysis[J/OL]. Eur J Obstetrics, Gynecol Reproduct Biol. 2021;260:137–149. doi:10.1016/j.ejogrb.2021.03.013
16. Sun Y, Shen Z, Zhan Y, et al. Effects of pre-pregnancy body mass index and gestational weight gain on maternal and infant complications. BMC Pregnancy Childbirth. 2020;20(1):390. doi:10.1186/s12884-020-03071-y
17. Wang YP, Ray JG, Pudwell J, et al. Mode of conception and risk of spontaneous vs. provider-initiated preterm birth: population-based cohort study. Fertility Sterility. 2022;118(5):926–935. doi:10.1016/j.fertnstert.2022.07.028
18. Xiao H, Xing X, Zhang C, et al. Association between clinical subtypes and pregnancy outcome of cervical incompetence: a retrospective cohort study. BMC Pregnancy Childbirth. 2025;25:348. doi:10.1186/s12884-025-07465-8
19. Gulersen M, Lenchner E, Nicolaides KH, et al. Cervical cerclage for short cervix at 24 to 26 weeks of gestation: systematic review and meta-analysis of randomized controlled trials using individual patient-level data[J/OL]. Am J Obstetrics Gynecol MFM. 2023;5(6):100930. doi:10.1016/j.ajogmf.2023.100930
20. Da Fonseca EB, Vasconcelos De Castro TB, Dias T, et al. Cervical assessment. Best Practice Res. 2025;99:102590. doi:10.1016/j.bpobgyn.2025.102590
21. Sejer EPF, Pegios P, Lin M, et al. The combined use of cervical ultrasound and deep learning improves the detection of patients at risk for spontaneous preterm delivery. Am J Obstetrics Gynecol. 2025:S0002–9378(25)00665–9. doi10.1016/j.ajog.2025.09.012
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Explainable Machine Learning Model to Predict Acute Kidney Injury After Cardiac Surgery: A Retrospective Cohort Study
Gao Y, Wang C, Dong W, Li B, Wang J, Li J, Tian Y, Liu J, Wang Y
Clinical Epidemiology 2023, 15:1145-1157
Published Date: 4 December 2023
Analysis of Health-Related Quality of Life in Elderly Patients with Stroke Complicated by Hypertension in China Using the EQ-5D-3L Scale
Wang S, Shen C, Yang S
Journal of Multidisciplinary Healthcare 2024, 17:1981-1997
Published Date: 30 April 2024
Integrating Machine Learning and the SHapley Additive exPlanations (SHAP) Framework to Predict Lymph Node Metastasis in Gastric Cancer Patients Based on Inflammation Indices and Peripheral Lymphocyte Subpopulations
Zhu Z, Wang C, Shi L, Li M, Li J, Liang S, Yin Z, Xue Y
Journal of Inflammation Research 2024, 17:9551-9566
Published Date: 23 November 2024
Explainable Prediction of Long-Term Glycated Hemoglobin Response Change in Finnish Patients with Type 2 Diabetes Following Drug Initiation Using Evidence-Based Machine Learning Approaches
Chandra G, Lavikainen P, Siirtola P, Tamminen S, Ihalapathirana A, Laatikainen T, Martikainen J, Röning J
Clinical Epidemiology 2025, 17:225-240
Published Date: 8 March 2025
Construction and Validation of a Machine Learning-Based Risk Prediction Model for Sleep Quality in Patients with OSA
Tong Y, Wen K, Li E, Ai F, Tang P, Wen H, Guo B
Nature and Science of Sleep 2025, 17:1271-1289
Published Date: 12 June 2025