Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Development of a Lasso-Nomogram-Based Risk Prediction Model for Cognitive Frailty in Elderly MHD Patients
Authors Xia NN ![]() , Liu J
, Liu J ![]() , Wang H
, Wang H
Received 5 May 2025
Accepted for publication 28 July 2025
Published 12 August 2025 Volume 2025:21 Pages 1637—1650
DOI https://doi.org/10.2147/NDT.S533696
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Ning-ning Xia, Jing Liu, Hongying Wang
Blood Purification Center, Nanjing BenQ Medical Center, the Affiliated BenQ Hospital of Nanjing Medical University, Nanjing, Jiangsu Province, People’s Republic of China
Correspondence: Jing Liu, Email [email protected] Ning-ning Xia, Email [email protected]
Introduction: Cognitive frailty is increasingly recognized among older adults receiving maintenance hemodialysis (MHD), yet effective screening tools tailored for this population are lacking. This study aimed to develop a predictive model to identify MHD patients of advanced age who are at high risk for cognitive frailty, thereby facilitating early detection and intervention.
Methods: A cross-sectional study was conducted between February and December 2024, enrolling 223 older individuals undergoing MHD at a tertiary hospital in Nanjing, China. Data on demographic and clinical characteristics were collected, along with assessments using standardized instruments, including the Kidney Disease Quality of Life Instrument, Geriatric Depression Scale-5, Subjective Cognitive Decline Questionnaire-9, Montreal Cognitive Assessment, Clinical Dementia Rating, Fried Frailty Phenotype, and Cognitive Reserve Index Questionnaire. Least absolute shrinkage and selection operator (LASSO) regression was used to identify relevant variables, which were subsequently entered into multivariate logistic regression to determine independent risk factors. A nomogram was constructed based on the final model.
Results: Cognitive frailty was identified in 85 patients, indicating a prevalence of 38.1%. Eight variables were found to be independent risk factors: serum phosphorus, hemoglobin level, depression score, cognitive reserve, age, dialysis duration, dialysis adequacy (Kt/V), and intradialytic hypotension. The predictive nomogram showed excellent discriminative performance, with an area under the receiver operating characteristic curve of 0.986 (95% confidence interval: 0.970– 0.999), sensitivity of 94.9%, and specificity of 97.6%. Decision curve analysis demonstrated favorable clinical utility.
Conclusion: Cognitive frailty is prevalent among older patients receiving MHD. The nomogram incorporating eight key variables provides a practical tool for early screening and personalized intervention in this high-risk population.
Keywords: cognitive frailty, CF, cognitive reserve, maintenance hemodialysis, MHD, prediction model
Introduction
Maintenance hemodialysis (MHD)1 serves as the primary therapeutic modality for patients with end-stage renal disease (ESRD), a condition resulting from the progression of chronic kidney disease (CKD) to stage 5. At this advanced stage, renal function undergoes progressive, structural, functional, and irreversible deterioration due to multifactorial nephron injury, accompanied by a sustained decline in glomerular filtration rate (GFR). When GFR falls below 15 mL/(min·1.73 m²), renal replacement therapy (RRT) becomes clinically imperative.2,3 While kidney transplantation remains the optimal treatment for ESRD, its widespread application is hindered by limited organ availability and prohibitive costs.4 Peritoneal dialysis, another RRT modality, is less commonly utilized due to inherent risks such as intra-abdominal infections.3 Consequently, hemodialysis has emerged as the predominant therapeutic approach for ESRD patients. MHD is formally defined as hemodialysis administered regularly for a duration exceeding three months. The escalating global burden of CKD has precipitated a parallel rise in the hemodialysis-dependent population in recent years.
While MHD extends the lifespan of ESRD patients, both the treatment modality and the disease itself contribute to multisystem dysfunction, resulting in unavoidable clinical sequelae, such as malnutrition, hypotension, interdialytic weight gain, hypoalbuminemia, depression, and anxiety. These complications not only exacerbate frailty in patients5 but also impair cognitive function.6 Frailty, a prevalent syndrome among MHD patients with an overall incidence of approximately 35%,7 manifests clinically as multisystem dysregulation and diminished physiological resilience. This compromised homeostatic capacity elevates susceptibility to adverse events, including falls, hospital readmissions, and cognitive decline.8 Furthermore, cognitive impairment is disproportionately prevalent in the MHD population due to compounded physiological and psychological stressors. Studies have indicated that 71.1% of MHD patients exhibit deficits in at least one cognitive domain.9 Progressive cognitive deterioration impairs memory, reasoning, linguistic abilities, and visuospatial skills, ultimately disrupting daily functioning and imposing substantial burdens on healthcare resources. Historically, frailty and cognitive impairment were investigated as independent risk factors.9,13 Emerging evidence, however, underscores their bidirectional interdependence.14 Frailty accelerates cognitive decline,15 while cognitive enhancement plays a pivotal role in mitigating frailty.16 Consequently, researchers have shifted focus to the cumulative adverse outcomes arising from their co-occurrence, termed cognitive frailty. This syndrome is operationally defined as the coexistence of physical frailty and cognitive impairment (Clinical Dementia Rating [CDR] = 0.5), excluding Alzheimer’s disease and other dementia subtypes.17 Current epidemiological studies on cognitive frailty predominantly target community-dwelling older adults, with reported prevalence rates of 2.6–2.9% in China,18,19 2.1% in Japan,20 1% in Italy,15 and 5.4% and 12.1% in the United States and Canada, respectively.21,22 Notably, the prevalence among MHD patients exceeds that of the general population due to disease- and dialysis-related factors. A study by Qin et al identified a 17.5% incidence of cognitive frailty in MHD recipients.23 Compared to isolated frailty or cognitive impairment, cognitive frailty exacerbates health deterioration. However, research on cognitive frailty in elderly MHD patients remains scarce. Additional evidence links cognitive frailty to elevated fall risk,18,20 reduced mobility, prolonged hospitalization, and increased susceptibility to dementia and mortality.24 These findings underscore the imperative for clinicians to prioritize early identification of high-risk MHD patients and implement targeted interventions to mitigate cognitive frailty incidence and improve clinical outcomes.
Research on cognitive frailty in MHD patients remains nascent globally, with even fewer studies addressing the development of risk prediction models for these patients. Luo et al25 collected data on activities of daily living, sleep quality, social support, depressive symptoms, sociodemographic characteristics, and clinical parameters from 425 elderly chronic kidney disease (CKD) patients to construct a classification and regression tree (CART) model, providing a preliminary tool for identifying high-risk individuals with cognitive frailty in this cohort. Similarly, Yang et al26 developed a nomogram model incorporating general demographic data, nutritional status, and depression levels from 674 community-dwelling elderly patients with chronic diseases, demonstrating robust calibration and discriminative performance for predicting cognitive frailty. Parallel efforts by Chen et al27 utilized variables including nutritional status, physical activity, multimorbidity burden, mental health, functional independence, and age to design a nomogram for early screening of cognitively frail older adults in community settings. Additionally, Song28 and Wen29 established nomogram-based risk prediction models for cognitive frailty in elderly patients with chronic obstructive pulmonary disease and stable coronary artery disease, respectively, offering practical frameworks for clinical risk stratification. To sum up, in spite of these advances, current tools for identifying cognitive frailty in elderly MHD patients exhibit critical limitations. Existing models inadequately account for disease-specific risk factors inherent to MHD populations, resulting in suboptimal specificity and sensitivity that fail to reflect the unique pathophysiological profile of this group. This study aims to address these gaps through a comprehensive investigation of cognitive frailty prevalence and its multifactorial determinants in elderly MHD patients. By integrating clinical, biochemical, and psychosocial predictors, we seek to establish a tailored risk prediction model that enhances early diagnostic precision and informs targeted therapeutic strategies, ultimately improving prognostic outcomes and quality of life in this vulnerable population.
Methods
Human Ethics and Consent to Participate Declarations
This study complies with the Declaration of Helsinki. Ethical approval was obtained from the institutional Ethics Committee at BenQ Hospital Affiliated to Nanjing Medical University (Grant 2022-KL010). All participants in this study provided written informed consent.
Study Design and Population
This cross-sectional study was carried out at the hemodialysis unit of a tertiary Class A general hospital in Nanjing, Jiangsu Province, China, from February to December 2024. Sample size estimation was performed using the SSizeLogisticCon function from the powerMediation package in R (version 4.2.0), following the methodology proposed by Vittinghoff et al.30 This approach requires specification of four parameters: the proportion of participants in the reference group (pl), the anticipated odds ratio (OR), the significance level (alpha), and the desired statistical power. Based on prior literature, we set pl = 0.180, OR = 4.385, alpha = 0.050, and power = 0.900, resulting in a minimum sample size of 79.71. After adjusting for an estimated 20% attrition rate, the target sample size was set at 100 participants. However, to enhance the robustness of the analysis and accommodate the availability of eligible individuals, we ultimately enrolled a total of 237 participants, exceeding the minimum requirement.
Participants were recruited using a convenience sampling method.Eligible participants met the following criteria: (1) undergoing maintenance hemodialysis for at least three months with clinical stability; (2) aged 65 years or older; and (3) possessing adequate communication abilities to complete assessments. Individuals were excluded if they had (1) a clinical diagnosis of Alzheimer’s disease or other neurocognitive disorders, or (2) experienced acute medical deterioration. A total of 237 maintenance hemodialysis patients were initially enrolled. Due to incomplete data in 14 cases, these participants were excluded, resulting in 223 patients with complete data included in the final analysis.
Measures and Data Collection
The questionnaires were distributed by the members of the team after uniform training. The purpose of the research was explained to the respondents first, and then a face-to-face survey was adopted. Afterwards, researchers eliminated the invalid questionnaires with incomplete answers by checking the completeness of the questionnaires one by one. Two-person input method was used to ensure the accuracy of data input.
General Data Questionnaire
Researchers designed a general data questionnaire. Main indicators included gender, age, living conditions, marital status, body mass index, monthly income, education level, Smoking status and physical activity were assessed as life style factors. Dialysis treatment factors included dialysis method, weight gain during dialysis, vascular access, blood calcium, blood phosphorus, Kt/V and dialysis age, which were obtained from the participants’ electronic medical records and hospital admissions during the previous six months, supplemented by patient self-report.
Health-Related Quality of Life (KDQOL-36) Scale
KDQOL-3631 contains five subscales: symptoms and the problem of kidney disease (SPKD subscale), effects of kidney disease (EKD) subscale, the burden of kidney disease (BKD) subscale, SF-12 physical component summary (PCS) subscale, SF-12 mental component summary (MCS) subscale. There was no total score for the KDQOL-36 scale. Each subscale score was separately calculated, ranging from 0 to 100. A higher score indicates a better quality of life. KDQOL-36 scale was scored using an Excel rating template at the website of Rand Corporation in the United States (www.rand.org/health/surveys_tools/kdqol). This scale has been widely used to evaluate Quality of Life status in China.
Definition of Intradialytic Hypotension
In alignment with the Kidney Disease Outcomes Quality Initiative (K/DOQI) established by the National Kidney Foundation(NKF), intradialytic hypotension (IDH)32 is clinically defined as a systolic blood pressure reduction ≥20 mmHg or a mean arterial pressure decrease >10 mmHg during hemodialysis sessions, concurrent with symptomatic manifestations necessitating immediate therapeutic countermeasures.
The Five-Item Geriatric Depression Scale (GDS-5)
GDS-5 refers to a concise depression assessment scale simplified by Hoyl MT et al33 through the Geriatric Depression Scale. It was applied to screen for depression in the elderly. There are 5 items on the scale, with a scoring range of 0–5 points. A total score of ≥ 2 points indicates symptoms of depression. The total Cronbach’s α coefficient of the scale is 0.88, and the test-retest reliability is 0.84.34
The Subjective Cognitive Decline Questionnaire 9 (SCD-Q9)
SCD-Q9 was used to evaluate the degree of subjective cognitive decline. Developed by Gifford et al35 in 2015, it includes 2 dimensions and 9 items. The questionnaire, including overall memory function and time comparison (4 items) and daily activity ability (5 items), was translated into Chinese by Hao LX et al.36 The higher the score is, the higher the degree of SCD. The Cronbach’s α coefficient of the Chinese-version SCD-Q9 is 0.87–0.88.
The Montreal Cognitive Assessment (MoCA)
MoCA was compiled by Nasreddine et al37 and then translated and revised by Wen HB et al38 to form a Chinese version of MoCA for evaluating cognitive function. In this scale, there are 8 aspects, including visual space and executive function, naming, memory, attention, language, abstract thinking, delayed memory, and orientation. The scoring range is 0–30 points, with ≤ 25 points indicating cognitive impairment. The Cronbach’s α coefficient of this scale is 0.858.
The Clinical Dementia Rating (CDR)
CDR is a tool used by clinical professionals to assess the degree of cognitive impairment in patients by obtaining effective information through conversations with patients and their families.39 The rating content mainly includes memory, orientation, ability to judge and solve problems, social activity ability, family and interests, and personal self-care ability. The evaluation criteria can be listed as follows: “0 for normal, 0.5 points for suspected dementia, 1 point for mild dementia, 2 points for moderate dementia, and 3 points for severe dementia”. The CDR of 0.5 points is considered as one of the recommended diagnostic criteria for cognitive impairment in the guidelines.
The Frailty Phenotype (Fried)
Frailty Phenotype has been widely used to evaluate both frailty and physical frailty in CF,40 including five items: involuntary unexplained weight loss, self-reported fatigue, low physical activity, decreased ability of walking, and decreased grip strength. Satisfaction of any of these items earns 1 point on a scale ranging from 0–5, 0 for non-frailty, 1–2 for pre-frailty, and 3 for frailty.
The Cognitive Reserve Index Questionnaire (CRIq)
CRIq was compiled by Nucci et al41 in 2012, was used to assess the levels of cognitive reserve, including three dimensions: education, work activities, and leisure activities, with a total of 20 items. At last, the CRIq, provided by Nucci et al (https://www.cognitivereserveindex.org), was utilized to calculate the cognitive reserve index and divide it into five levels: low (≤ 70 points), medium low (71–84 points), medium (85–114 points), medium high (115–130 points), and high (>130 points). The higher the score is, the higher the level of cognitive reserve. The Chinese version was directly translated by He Y42 in 2014, with a Cronbach’s α coefficient of 0.62.
Assessment of CF
SCD-Q9 meets the criteria of “self-perceived persistent cognitive dysfunction compared to previous normal state, unrelated to acute events”. FFP ≥ 1, MoCA ≥ 26; or FFP ≥ 1 point, CDR=0.5, MoCA ≤ 25 points indicates CF.
Data Analysis
All data analyses were conducted using SPSS version 25.0 and R software version 4.2.0. Categorical variables were summarized as frequencies and percentages, while continuous variables were tested for normality using the Kolmogorov–Smirnov test. Normally distributed data were expressed as mean ± standard deviation (SD); non-normally distributed data were presented as median with interquartile range (IQR).To address potential multicollinearity and identify the most predictive features, Least Absolute Shrinkage and Selection Operator (LASSO) regression was employed. This method introduces a penalty term to the standard least squares regression, shrinking coefficients of less relevant variables toward zero, thereby achieving variable selection and regularization simultaneously.43 Variables retained through LASSO regression were subsequently included in a multivariate binary logistic regression model to determine independent risk factors associated with cognitive frailty among maintenance hemodialysis (MHD) patients.Based on the significant predictors identified from the logistic regression model, a nomogram was developed using the “rms” package in R. The model’s discrimination ability was evaluated using the concordance index (C-index) and the area under the receiver operating characteristic curve (AUC). Model calibration was assessed by plotting a calibration curve, comparing predicted and observed probabilities. Furthermore, decision curve analysis (DCA) was conducted to estimate the clinical net benefit and practical utility of the prediction model across a range of threshold probabilities.All statistical tests were two-tailed, and a p-value < 0.05 was considered statistically significant.
Results
Participants’ Socio-Demographic Characteristics and General Health
CF occurred in 85 out of 223 elderly MHD patients with an incidence of 38.1%.A comparison of the characteristics of patients with and without CF is shown in Table 1. Male patients had a higher prevalence of CF than female patients (56.5% vs 43.5%). Patients with CF had a higher mean age than those without CF (79.66 years (SD 7.92) vs 72.22 years (SD 5.96)). A higher prevalence of CF was observed in patients with lower education (61.2% vs 50.0%). The proportion of patients who never exercised and had CF was significantly higher (54.1% vs 37.1%). In addition, the CF group had a higher proportion of patients without a spouse than the non-CF group (24.4% vs 17.1%). Of the 85 patients with CF,54.1% (n = 46) had been hospitalised in the previous six months. In the CF group, patients with MHD had a higher proportion of lower monthly household income, more weight gain between dialyses, less autologous vascular access, higher blood phosphorus levels, were older on dialysis and had higher GDS-5 scores compared to those in the non-CF group.
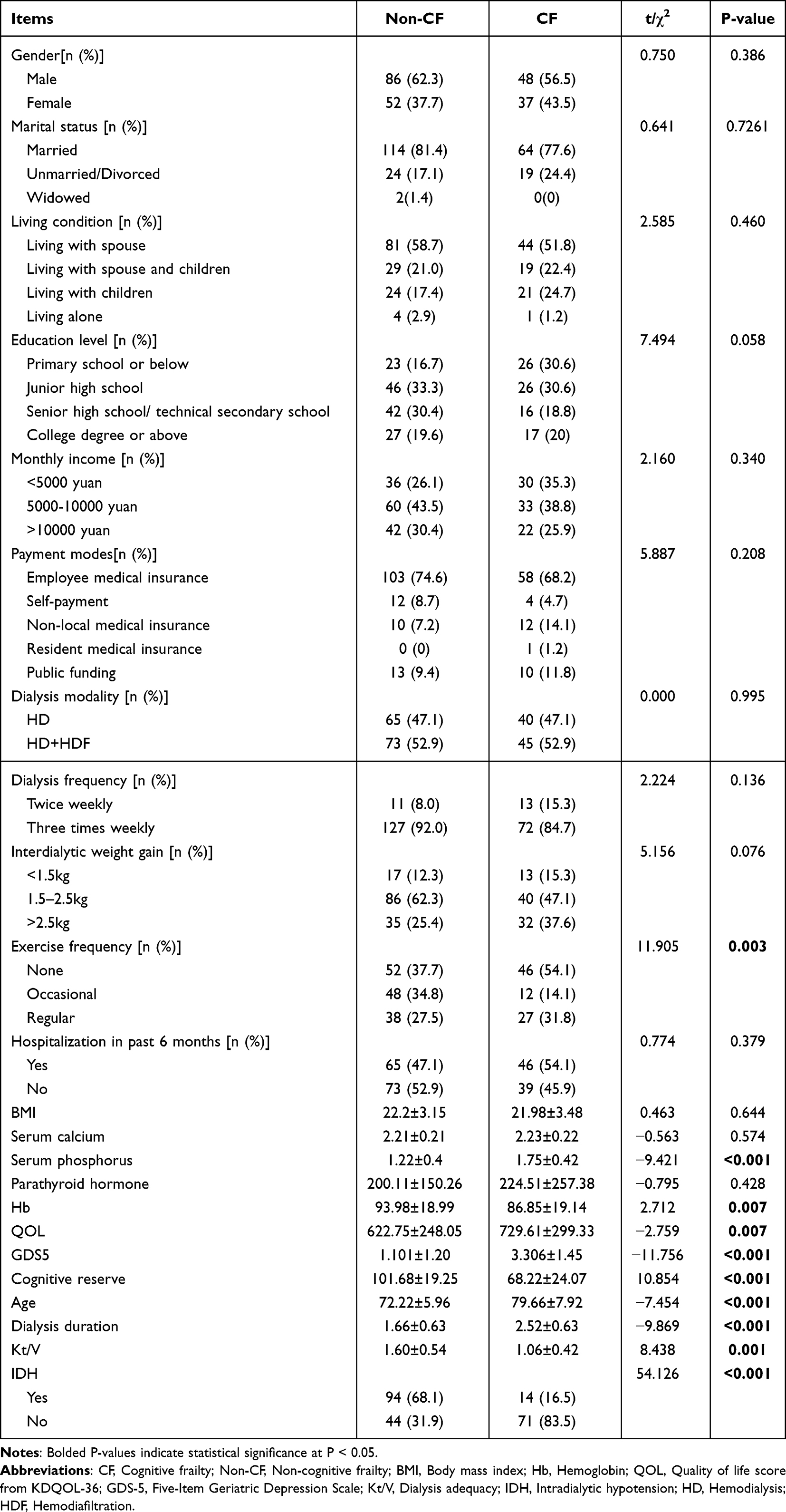 |
Table 1 Comparative Analysis of Clinical Characteristics Between Non-CF and CF Groups |
In this study, statistical comparisons between non-CF and CF groups were conducted through chi-square tests for categorical variables and independent sample t-tests for continuous measures, with results summarized in Table 1. The analysis revealed statistically significant intergroup disparities in exercise frequency, serum phosphorus, hemoglobin (Hb), quality of life (QOL), GDS-5, cognitive reserve, age, dialysis duration, Kt/V, and IDH incidence. Conversely, no significant differences were observed across demographic variables (gender, marital status, living conditions), socioeconomic factors (education level, monthly income, payment modes), dialysis protocol parameters (modality, frequency, interdialytic weight gain), clinical outcomes (hospitalization in past 6 months, depressive symptoms), body mass index (BMI), or biochemical indices (serum calcium, parathyroid hormone).
LASSO Regression Analysis of Risk Factors for Cognitive Frailty
In this study, cognitive frailty status was designated as the dependent variable, with statistically significant predictors identified in Table 1, including exercise frequency, serum phosphorus, Hb, QOL, GDS-5, cognitive reserve, age, dialysis duration, Kt/V, and IDH incidence, which served as independent variables for constructing a LASSO regression model. The analytical framework incorporated two critical visualizations: a variable selection trajectory plot demonstrating coefficient evolution during LASSO regression (see Figure 1), and a cross-validation plot identifying the optimal parameter λ (see Figure 2). Model optimization revealed superior performance at penalty coefficient λ=0.030, achieving optimal balance between model parsimony and predictive accuracy. This parameter selection resulted in eight key predictors of cognitive frailty: serum phosphorus, Hb, GDS5, cognitive reserve, age, dialysis duration, Kt/V, and IDH.
 |
Figure 1 Variable selection trajectory plot demonstrating coefficient evolution during LASSO Regression. Abbreviations: LASSO, Least Absolute Shrinkage and Selection Operator; λ, Regularization parameter. |
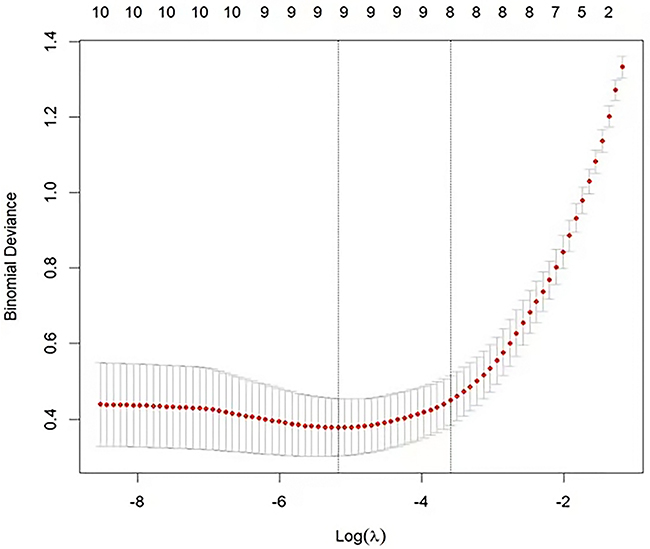 |
Figure 2 Cross-validation plot identifying the optimal parameter λ. Abbreviations: λ, Regularization parameter; LASSO, Least Absolute Shrinkage and Selection Operator. |
Logistic Regression Analysis of Risk Factors for Cognitive Frailty
This study employed cognitive frailty status as the dependent variable, and incorporated these predictors selected through LASSO regression: serum phosphorus, Hb, GDS5, cognitive reserve, age, dialysis duration, Kt/V, and IDH, as independent variables. Multivariate logistic regression analysis identified serum phosphorus, Hb, GDS5, Cognitive reserve, age, dialysis duration, Kt/V, and IDH as significant risk factors for cognitive frailty (P<0.05). Detailed results are presented in Table 2.
 |
Table 2 Logistic Regression Analysis of Factors Influencing Cognitive Frailty |
Development of the Nomogram for Cognitive Frailty Among Patients on MHD
Based on 8 predictors identified through LASSO and logistic regression: serum phosphorus, Hb, GDS5,age, cognitive reserve, dialysis duration, Kt/V, and IDH, a nomogram prediction model for cognitive frailty was developed (see Figure 3). The model utilized cognitive frailty occurrence among the MHD patients as the predictive endpoint.
 |
Figure 3 Nomogram prediction model for cognitive frailty. |
Evaluation of the Nomogram Model
The Nomogram model was drawn to predict the ROC curve of cognitive frailty in the experimental subjects, as shown in Figure 4. The ROC curve demonstrated an area under the curve 0.986 (95% CI:0.970–0.999), with sensitivity and specificity values of 94.9% and 97.6%, respectively, indicating robust predictive performance.
 |
Figure 4 ROC curve of the Nomogram model. Abbreviations: ROC, Receiver Operating Characteristic; AUC, Area Under the Curve. |
Discussion
Elderly MHD patients have demonstrated a significantly higher susceptibility to cognitive frailty than the general community-dwelling older adults. This study enrolled 223 elderly MHD patients, among whom 85 cases of cognitive frailty were identified, with a prevalence rate of 38.1%. This rate markedly exceeds the 17.5% reported in the study by Qin et al,23 a disparity potentially attributable to the exclusive inclusion of elderly individuals in our cohort. Empirical evidence indicates a positive correlation between advancing age and the likelihood of cognitive frailty development in MHD patients, underscoring the imperative for targeted screening initiatives in elderly MHD patients. Although existing assessment tools address cognitive frailty in broader populations, risk stratification tools tailored to elderly MHD patients remain scarce. By integrating multidimensional data encompassing physiological and psychological parameters specific to elderly MHD patients, this study establishes a novel risk prediction model for cognitive frailty in this population, bearing substantial clinical and methodological significance.
Cognitive reserve score can be an important factor influencing the CF in elderly MHD patients, with an adjusted OR of 0.966 (95% CI: −0.060~-0.010). Cognitive reserve refers to a new concept proposed by Stern,44 reflecting the ability to make full use of different brain networks and optimize their functions, thereby being differentiated from brain reserve. The level of cognitive reserve is mainly related to an individual’s educational level, intelligence, professional experience, and the complexity of professional life, and both lifestyle and leisure activities can influence an individual’s level of cognitive reserve.45 Current studies have indicated that cognitive reserve can protect against cognitive disorder caused by pathological brain injury in elderly people, and it can reduce the risk of cognitive impairment independently of the mechanisms of pathological brain changes associated with Alzheimer’s disease (the pathological mechanisms of tau protein and amyloid protein).46 Hence, cognitive reserve is an important protective factor not only for cognitive impairment-related diseases, but also for other neuro-degenerative diseases.47 A further finding of this study showed that older MHD patients with high cognitive reserve seemed less susceptible to be diagnosed with CF than older MHD patients with low cognitive reserve. Recent studies demonstrated6,23 that the CF issue was becoming increasingly prominent in elderly MHD patients, and has been an important reason for affecting the quality of life of elderly MHD patients through severely influencing their mental health and life independence. Cognitive reserve has shown great prospects in reducing the disease burden of elderly MHD patients. Yet few studies have focused on the predictive value of cognitive reserve in elderly MHD patients with CF at present. Therefore, cognitive reserve score can be used to identify the high-risk groups for developing targeted evidence-based cognitive stimulation for elderly MHD patients. This can improve their cognitive reserve, reducing the cognitive impairment caused by hemodialysis, lower the burden of symptoms in such patients, and further improve the quality of life of such patients.
It was found in this study that hyperphosphatemia can be a significant risk factor for cognitive frailty in elderly MHD patients, with an adjusted OR of 37.518 (95% CI: 1.243~6.007). In recent years, emerging evidence has established serum phosphorus levels as an independent determinant of cognitive impairment.48 The underlying pathophysiology may involve dysregulated cerebral calcium-phosphorus homeostasis where elevated serum phosphorus induces endothelial dysfunction, subsequently reducing regional cerebral perfusion and promoting β-amyloid deposition, ultimately contributing to cognitive dysfunction. However, the precise mechanisms linking phosphorus dysregulation to dialysis-associated cognitive deficits remain incompletely elucidated. In elderly MHD patients, age-related metabolic decline and prolonged dialysis duration synergistically exacerbate phosphorus retention. Hence, these findings suggest the clinical imperative for regular serum phosphorus monitoring and targeted interventions to mitigate cognitive frailty risk.
This study demonstrated that decreased Hb levels constitute a significant risk factor for cognitive frailty in MHD patients, with an OR of 0.907 (95% CI: −0.146~-0.049). Contemporary investigations into post-dialysis cognitive dysfunction among chronic renal failure patients have similarly identified reduced Hb levels as contributing to impaired oxygen-carrying capacity, resulting in cerebral hypoxia, disrupted neurometabolic processes, and consequent cognitive deterioration. Corroborating these findings, Guo et al49 revealed that elevated Hb levels serve as a protective factor for cognitive function in elderly hemodialysis patients. Frailty, prevalent among elderly MHD patients, frequently coexists with suboptimal Hb levels, underscoring the clinical necessity for healthcare providers to prioritize Hb monitoring and implement early interventions in elderly MHD patients.
According to these findings in this study, depression serves as a significant risk factor for cognitive frailty in elderly MHD patients, with an OR of 2.463 (95% CI: 0.434~1.370). Accumulating evidence suggests that5,50,51 psychological factors, particularly depression, interact with objective physiological mechanisms in the development of cognitive frailty. Shared pathophysiological mechanisms between depression and cognitive decline, including white matter hyperintensities, non-pathological cerebral aging, and neuroinflammation, may underlie this association. As a result, depression has become a pivotal risk factor for cognitive frailty in elderly MHD patients. The chronic symptom burden, treatment-related lifestyle constraints, reduced social engagement, and social isolation inherent to long-term MHD therapy collectively predispose elderly patients to psychological distress. Clinicians must prioritize routine mental health evaluations in these patients, even when patients exhibit diminished expressive capacity, to prevent under-recognition of affective disorders.
Besides, this study identified advanced age as a significant risk factor for cognitive frailty in elderly MHD patients, with an OR of 1.268 (95% CI:0.084~0.391), consistent with existing evidence implicating synergistic interactions between age-related physical frailty and progressive cognitive dysfunction through cumulative detrimental effects. Furthermore, dialysis duration has emerged as an independent risk factor of cognitive frailty, with an OR of 30.737 (95% CI: 0.701~6.149). Extended dialysis exposure not only facilitates systemic toxin accumulation and neurotoxic damage, but also induces pathological alterations in cerebral vascular endothelium, culminating in irreversible cognitive impairment.16 Additionally, prolonged dialysis contributes to persistent amino acid and protein and protein malnutrition. The sustained catabolic state induced by dialysis-related nutrient losses, particularly critical amino acids essential for neuronal regeneration, exacerbates age-related cognitive decline.19 Consequently, elderly MHD patients with advanced age and extended dialysis histories necessitate regular nutritional assessments and timely therapeutic adjustments to mitigate these compounding risks.
This study also revealed that Kt/V constitutes a protective factor against cognitive frailty in elderly MHD patients, with an OR of 0.180 (95% CI: −3.267~-0.162). In contrast, Guo et al52 demonstrated that reduced Kt/V (OR = 0.008; 95% CI: 0.002–0.035; P< 0.001) serves as a significant risk factor for cognitive impairment in middle-aged and elderly MHD patients. The precise pathophysiological mechanisms linking suboptimal dialysis adequacy to cognitive deterioration remain incompletely characterized. Prior studies hypothesized that uremic toxin accumulation, chronic microinflammation, and acid-base imbalances may synergistically disrupt neuronal homeostasis, thereby exacerbating cognitive dysfunction through multifactorial pathways. Given these collective findings, the factors related to cognitive impairment in HD patients should be highly valued in clinical practice, especially in maintaining adequate dialysis, in order to attenuate the incidence and progression of dialysis-associated cognitive impairment.
This study demonstrated that IDH refers to a significant risk factor for cognitive frailty in elderly MHD patients, with an OR of 6.4922 (95% CI:0.192~3.549). As defined by the NFK’s Kidney Disease Outcomes Quality Initiative (K/DOQI), IDH is characterized by either a ≥20 mmHg reduction in systolic blood pressure or >10 mmHg decrease in mean arterial pressure during hemodialysis, accompanied by clinical symptoms necessitating therapeutic intervention. IDH occurs in 20%–30% of hemodialysis sessions and frequently compromises dialysis adequacy, with severe cases potentially progressing to fatal outcomes. Furthermore, IDH exacerbates MCI through multiple pathways: impaired urea clearance, elevated calcium-phosphate product, and dialysis inefficiency. In addition, recurrent IDH may trigger systemic inflammation, endotoxemia, renin-angiotensin system activation, and oxidative stress, all contributing to MCI pathogenesis. The occurrence of IDH primarily stems from excessive and rapid ultrafiltration rates during dialysis sessions, which acutely reduce effective circulating volume, diminish cardiac output, and overwhelm compensatory mechanisms, culminating in hypoperfusion. The stringent management of IDH, as a controllable risk factor, holds substantial potential to stabilize or ameliorate MCI in elderly MHD patients.
Based on the conceptual framework of cognitive frailty established by Kelaiditi E,17 it can be categorized into reversible cognitive frailty (RCF) and potentially reversible cognitive frailty (PRCF). Cognitive frailty may be positioned as a critical window for reversing cognitive impairment, rendering the early identification and risk mitigation of cognitive frailty in elderly MHD patients a clinical priority. Currently, targeted research remains scarce in spite of the escalating prevalence of cognitive frailty in these patients. To address this gap, the cognitive frailty risk prediction model developed in this study synthesizes both validated risk factors and weighted scoring metrics specific to elderly MHD patients. This model can not only generate personalized predictions based on patient-specific clinical and biochemical profiles, aligning with precision medicine objectives and individualized care protocols, but also provide a user-friendly graphical format to facilitate clinical operations by medical staff.
Strength and Limitations
The present study has the following innovations. First, few study has focused on constructing risk prediction model for cognitive frailty among elderly patients on MHD. The study offers the possibility of early screening and intervention for elderly patients on MHD with cognitive frailty. Second, the study synthesized multi-dimensional factors of physiology, psychology and treatment to make the assessment more comprehensive. Third, the final nomogram is visual and understandable graphic, which facilitates the clinical application. However, several limitations must be acknowledged. The study was conducted at a single center in Nanjing, Jiangsu Province, which may limit the generalizability of the findings to other regions. The predictive model requires external validation in broader geographic and clinical settings. Additionally, although the model included key clinical variables, important vascular-related risk factors such as diabetes mellitus, coronary artery disease (CAD), peripheral vascular disease (PVD), and hypertension—which are known to be associated with cognitive impairment—were not collected or analyzed in this study. This omission may affect the comprehensiveness of the risk prediction. Future studies should incorporate these underlying medical conditions to further refine and improve the predictive model.
Conclusion
The study constructed a nomogram with good discrimination, calibration and clinical utility to predict the risk of cognitive frailty among elderly patients on MHD. The model can be used by healthcare staff to calculate probability of cognitive frailty among elderly patients on MHD and take targeted interventions base on screened risk factors.
Data Sharing Statement
The original contributions presented in the study are included in the article and data analyzed are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
This study complies with the Declaration of Helsinki. Ethical approval was obtained from the institutional Ethics Committee at BenQ Hospital Affiliated to Nanjing Medical University (Grant 2022-KL010). All participants in this study provided written informed consent.
Acknowledgments
In addition to the funding agencies, we would also like to extend our thanks for the invaluable contributions by the study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research was supported by Nanjing Medical Science and Technology Development Fund numbered YKK21255 and 24256, Nanjing Medical University content building special nursing disciplines.
Disclosure
All the authors declare that they have no conflict of interest.
References
1. Ke C, Liang J, Liu M, et al. Correction to: burden of chronic kidney disease and its risk-attributable burden in 137 low-and middle-income countries, 1990-2019: results from the global burden of disease study 2019. BMC Nephrol. 2022;23(1):66. doi:10.1186/s12882-022-02686-x
2. Bikbov B, Purcell CA, Levey AS, GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2020;395(10225):709–733. doi:10.1016/S0140-6736(20)30045-3
3. Thurlow JS, Joshi M, Yan G, et al. Global epidemiology of end-stage kidney disease and disparities in kidney replacement therapy. Am J Nephrol. 2021;52(2):98–107. doi:10.1159/000514550
4. Breton A, Casey D, Arnaoutoglou NA. Cognitive tests for the detection of mild cognitive impairment (MCI), the prodromal stage of dementia: meta-analysis of diagnostic accuracy studies. Int J Geriatr Psychiatry. 2019;34(2):233–242. doi:10.1002/gps.5016
5. Fu W, Zhang A, Ma L, et al. Severity of frailty as a significant predictor of mortality for hemodialysis patients: a prospective study in China. Int J Med Sci. 2021;18(14):3309–3317. doi:10.7150/ijms.51569
6. Chen G, Zhang H, Du X, et al. Comparison of the prevalence and associated factors of cognitive frailty between elderly and middle-young patients receiving maintenance hemodialysis. Int Urol Nephrol. 2022;54(10):2703–2711. doi:10.1007/s11255-022-03188-3
7. Lee HJ, Son YJ. Prevalence and associated factors of frailty and mortality in patients with end-stage renal disease undergoing hemodialysis: a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18(7):3471. doi:10.3390/ijerph18073471
8. Lee SW, Lee A, Yu MY, et al. Is frailty a modifiable risk factor of future adverse outcomes in elderly patients with incident end-stage renal disease? J Korean Med Sci. 2017;32(11):1800–1806. doi:10.3346/jkms.2017.32.11.1800
9. van Zwieten A, Wong G, Ruospo M, et al. COGNITIVE-HD study investigators. Prevalence and patterns of cognitive impairment in adult hemodialysis patients: the COGNITIVE-HD study. Nephrol Dial Transplant. 2018;33(7):1197–1206. doi:10.1093/ndt/gfx314
10. Santos DGMD, Ferreira LGS, Pallone JM, et al. Association between frailty and depression among hemodialysis patients: a cross-sectional study. Sao Paulo Med J. 2022;140(3):406–411. doi:10.1590/1516-3180.2021.0556.r1.14092021
11. Yoneki K, Kitagawa J, Hoshi K, et al. Association between frailty and bone loss in patients undergoing maintenance hemodialysis. J Bone Miner Metab. 2019;37(1):81–89. doi:10.1007/s00774-017-0898-4
12. Takeuchi H, Uchida HA, Kakio Y, et al. The prevalence of frailty and its associated factors in Japanese hemodialysis patients. Aging Dis. 2018;9(2):192–207. doi:10.14336/AD.2017.0429
13. McAdams-DeMarco MA, Tan J, Salter ML, et al. Frailty and cognitive function in incident hemodialysis patients. Clin J Am Soc Nephrol. 2015;10(12):2181–2189. doi:10.2215/CJN.01960215
14. Carini G, Musazzi L, Bolzetta F, et al. The potential role of miRNAs in cognitive frailty. Front Aging Neurosci. 2021;13:763110. doi:10.3389/fnagi.2021.763110
15. Italian Longitudinal Study on Aging Working Group, Solfrizzi V, Scafato E, Lozupone M, et al. Additive role of a potentially reversible cognitive frailty model and inflammatory state on the risk of disability: the Italian longitudinal study on aging. Am J Geriatr Psychiatry. 2017;25(11):1236–1248. doi:10.1016/j.jagp.2017.05.018.
16. Aprahamian I, Suemoto CK, Aliberti MJR, et al. Frailty and cognitive status evaluation can better predict mortality in older adults? Arch Gerontol Geriatr. 2018;77:51–56. doi:10.1016/j.archger.2018.04.005
17. Kelaiditi E, Cesari M, Canevelli M, et al. IANA/IAGG. Cognitive frailty: rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J Nutr Health Aging. 2013;17(9):726–734. doi:10.1007/s12603-013-0367-2
18. Ma Y, Li X, Pan Y, et al. Cognitive frailty and falls in Chinese elderly people: a population-based longitudinal study. Eur J Neurol. 2021;28(2):381–388. doi:10.1111/ene.14572
19. Ma Y, Li X, Pan Y, et al. Cognitive frailty predicting death and disability in Chinese elderly. Neurol Res. 2021;43(10):815–822. doi:10.1080/01616412.2021.1939235
20. Kim H, Awata S, Watanabe Y, et al. Cognitive frailty in community-dwelling older Japanese people: prevalence and its association with falls. Geriatr Gerontol Int. 2019;19(7):647–653. doi:10.1111/ggi.13685
21. Aliberti MJR, Cenzer IS, Smith AK, Lee SJ, Yaffe K, Covinsky KE, Smith AK, et al. Assessing risk for adverse outcomes in older adults: the need to include both physical frailty and cognition. J Am Geriatr Soc. 2019;67(3):477–483. doi:10.1111/jgs.15683
22. St John PD, Tyas SL, Griffith LE, Menec V, Griffith LE, et al. The cumulative effect of frailty and cognition on mortality - results of a prospective cohort study. Int Psychogeriatr. 2017;29(4):535–543. doi:10.1017/S1041610216002088
23. Qin T, Fan C, Liu Q, et al. Development and validation of a nomogram for predicting cognitive frailty in patients on maintenance haemodialysis. J Adv Nurs. 2025;81(2):834–847. doi:10.1111/jan.16253
24. Bu Z, Huang A, Xue M, et al. Cognitive frailty as a predictor of adverse outcomes among older adults: a systematic review and meta-analysis. Brain Behav. 2021;11(1):e01926. doi:10.1002/brb3.1926
25. Luo B, Luo Z, Zhang X, et al. Status of cognitive frailty in elderly patients with chronic kidney disease and construction of a risk prediction model: a cross-sectional study. BMJ Open. 2022;12(12):e060633. doi:10.1136/bmjopen-2021-060633
26. Yang Z, Zhang H. Construction and validation of a risk prediction model for cognitive frailty in elderly patients with chronic diseases in the community. Nurs J. 2021;36(12):4.
27. Chen Y, Zhang Z, Zuo Q, et al. Construction and validation of a risk prediction model for cognitive frailty in elderly individuals in the community. Chin Nurs J. 2022;57(2):7.
28. Song G. Construction and Validation of a Risk Prediction Model for Cognitive Frailty in Elderly Patients with Chronic Obstructive Pulmonary Disease. Shanxi Medical University; 2022.
29. Wen F, Cheng M, Zhao C, et al. Establishment of a risk prediction model for cognitive frailty in elderly patients with stable coronary artery disease. Nurs J. 2021;36(10):6.
30. Vittinghoff E, Sen S, McCulloch CE. Sample size calculations for evaluating mediation. Stat Med. 2009;28(4):541–557. doi:10.1002/sim.3491
31. Tao X, Chow SK, Wong FK. Determining the validity and reliability of the Chinese version of the kidney disease quality of life questionnaire (KDQOL-36™). BMC Nephrol. 2014;15(1):115. doi:10.1186/1471-2369-15-115
32. Sarafidis PA, Persu A, Agarwal R, et al. Hypertension in dialysis patients: a consensus document by the European renal and cardiovascular medicine (EURECA-m) working group of the European renal association-European dialysis and transplant association (ERA-EDTA) and the hypertension and the kidney working group of the European society of hypertension (ESH). Nephrol Dial Transplant. 2017;32(4):620–640. doi:10.1093/ndt/gfw433
33. Hoyl MT, Alessi CA, Harker JO, et al. Development and testing of a five-item version of the Geriatric Depression Scale[J]. J Am Geriatr Soc. 1999;47(7):873–878. doi:10.1111/j.1532-5415.1999.tb03848.x
34. Rinaldi P, Mecocci P, Benedetti C, et al. Validation of the five-item geriatric depression scale in elderly subjects in three different settings[J]. J Am Geriatr Soc. 2003;51(5):694–698. doi:10.1034/j.1600-0579.2003.00216.x
35. Gifford KA, Liu D, Romano RR, et al. Development of a subjective cognitive decline questionnaire using item response theory: a pilot study[J]. Alzheimers Dement. 2015;1(4):429–439. doi:10.1016/j.dadm.2015.09.004
36. Jiang L, Gong L, Sun K. Study on Chinesization, reliability and validity of the English version of subjective cognitive decline questionnaires. Chin General Prac. 2019;22(26):3238–3245.
37. Nasreddine ZS, Phillips NA, Bedirian V, et al. The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
38. Hong-bo W, Zhen-xin Z, Fu-sheng N, et al. The application of Montreal cognitive assessment in urban Chinese residents of Beijing. Chinese J Int Med. 2008;47(1):36–39.
39. Nosheny RL, Yen D, Howell T, et al. Evaluation of the electronic clinical dementia rating for dementia screening. JAMA Network Open. 2023;6(9):e2333786. doi:10.1001/jamanetworkopen.2023.33786
40. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–M156. doi:10.1093/gerona/56.3.M146
41. Nucci M, Mapelli D, Mondini S. Cognitive reserve index questionnaire (CRIq): a new instrument for measuring cognitive reserve. Aging Clin Exp Res. 2012;24(3):218–226. doi:10.1007/BF03654795
42. He Y. Cognitive Reserve and Face Recognition of the Elderly--Mediating Effects of Cognitive Function and Processing Methods. Southwest University; 2015.
43. Daneshvar A, Golalizadeh M. Quantile regression shrinkage and selection via the Lqsso. J Biopharm Stat. 2024;34(3):297–322. doi:10.1080/10543406.2023.2198593
44. Stern Y. Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol. 2012;11(11):1006–1012. doi:10.1016/S1474-4422(12)70191-6
45. Gao Q, Hu K, Yan C, et al. Associated factors of sarcopenia in community-dwelling older adults: a systematic review and meta-analysis. Nutrients. 2021;13(12):4291. doi:10.3390/nu13124291
46. Qiu Y, Li G, Wang X, et al. Prevalence of cognitive frailty among community-dwelling older adults: a systematic review and meta-analysis. Int J Nurs Stud. 2022;125:104112. doi:10.1016/j.ijnurstu.2021.104112
47. C GJ, Hafeeq B, Aziz F, et al. The prevalence of frailty and its association with cognitive dysfunction among elderly patients on maintenance hemodialysis: a cross-sectional study from South India. Saudi J Kidney Dis Transpl. 2020;31(4):767–774. doi:10.4103/1319-2442.292310
48. Shoji T, Mori K, Nagakura Y, Nagakura Y, et al. Associations of cognitive function with serum magnesium and phosphate in hemodialysis patients: a cross-sectional analysis of the Osaka dialysis complication study (ODCS). Nutrients. 2024;16(21):3776. doi:10.3390/nu16213776
49. Guo H, Chen J, Deng J, et al. Analysis of influencing factors of cognitive impairment in middle-aged and elderly patients undergoing maintenance hemodialysis. Chin J Integr Nurs. 2022;8(1):139–141.
50. Anderson BM, Qasim M, Correa G, et al. Cognitive impairment, frailty, and adverse outcomes among prevalent hemodialysis recipients: results from a large prospective cohort study in the United Kingdom. Kidney Med. 2023;5(4):100613. doi:10.1016/j.xkme.2023.100613
51. Jung S, Lee Y-K, Choi SR, et al. Relationship between cognitive impairment and depression in dialysis patients. Yonsei Med J. 2013;54(6):1447–1453. doi:10.3349/ymj.2013.54.6.1447
52. Guo Y, Zhang C, Tian R, et al. A cross-sectional study on characteristics of cognitive impairment in middle-aged and elderly patients undergoing maintenance hemodialysis. Zhonghua Shen Zang Bing Za Zhi. 2021;37(8):632–638.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Easy-to-Use Nomogram Based on SII and SIRI to Predict in-Hospital Mortality Risk in Elderly Patients with Acute Myocardial Infarction
Chen Y, Xie K, Han Y, Xu Q, Zhao X
Journal of Inflammation Research 2023, 16:4061-4071
Published Date: 13 September 2023
Development and Internal Validation of a Nomogram for Predicting Postoperative Cardiac Events in Elderly Hip Fracture Patients
Liu Y, Liu H, Zhang F
Clinical Interventions in Aging 2023, 18:2063-2078
Published Date: 12 December 2023
Development and Validation of a Machine Learning Model for Predicting Medication Adherence Among Home-Dwelling Elderly Patients: A Retrospective Cross-Sectional Study
Zhang Y, Han Y, Yin X, Tian Y, Wu M
Patient Preference and Adherence 2026, 20:611334
Published Date: 19 May 2026