Back to Journals » Journal of Inflammation Research » Volume 19
Development and Validation of an Early Severity Prediction Model for Hypertriglyceridemia-Associated Acute Pancreatitis: A Multicenter Cohort Study
Authors Yao W ![]() , Zhao C, Cao L, Yang H, Liu Y, Li S, Wang L, Zhou J, Wang Z, Ke L, Bu Y
, Zhao C, Cao L, Yang H, Liu Y, Li S, Wang L, Zhou J, Wang Z, Ke L, Bu Y ![]()
Received 24 April 2026
Accepted for publication 11 June 2026
Published 23 June 2026 Volume 2026:19 613698
DOI https://doi.org/10.2147/JIR.S613698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alberto Caminero
Weijie Yao,1,* Chengsi Zhao,1,* Longxiang Cao,2,3 Huijin Yang,1 Yang Liu,2 Shuai Li,2 Lanting Wang,2 Jing Zhou,2 Zuozheng Wang,1 Lu Ke,2,3 Yang Bu1 On behalf of the Chinese Acute Pancreatitis Clinical Trials Group (CAPCTG)
1Department Hepatobiliary Surgery, The General Hospital of Ningxia Medical University, Yinchuan, 750004, People’s Republic of China; 2Department of Critical Care Medicine, Jinling Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, People’s Republic of China; 3National Institute of Healthcare Data Science, Nanjing University, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yang Bu, Department Hepatobiliary Surgery, The General Hospital of Ningxia Medical University, No. 804 Shengli South Street, Yinchuan, 750004, People’s Republic of China, Email [email protected] Lu Ke, Department of Critical Care Medicine, Jinling Hospital, Affiliated Hospital of Medical School, Nanjing University, No. 305 Zhongshan East Road, Nanjing, People’s Republic of China, Email [email protected]
Purpose: Hypertriglyceridemia-associated acute pancreatitis (HTG-AP) has become the second leading cause of acute pancreatitis (AP) in China. Compared with other etiologies, patients with HTG-AP are more likely to develop severe acute pancreatitis (SAP). This study aimed to develop and validate a prediction model for severe HTG-AP.
Patients and Methods: The derivation cohort consisted of 478 HTG-AP patients collected in a multicenter, prospective observational study (PERFORM study, 2020– 2023, involving 36 tertiary hospitals in China). The external validation cohort included 145 prospectively enrolled HTG-AP patients from the General Hospital of Ningxia Medical University (from January 2024 to May 2025). Clinical variables were collected within 24 hours of enrollment. After excluding variables with more than 20% missing data, least absolute shrinkage and selection operator (LASSO) regression was used to select predictors. An XGBoost-based prediction model was constructed. Model performance was evaluated using the area under the receiver operating characteristic curve (AUC), calibration curves, and decision curve analysis (DCA), and compared with traditional scoring systems. SHapley Additive exPlanations (SHAP) analysis was employed to assess model interpretability.
Results: A total of 113 patients (23.6%) in the derivation cohort and 23 patients (15.9%) in the validation cohort developed SAP, respectively. LASSO regression identified seven predictors: serum calcium (Ca2⁺), heart rate (HR), C-reactive protein (CRP), D-dimer (D-D), respiratory rate (RR), serum creatinine (SCr), and pleural effusion. The XGBoost model achieved an AUC of 0.873 in both the derivation and external validation cohorts, thereby significantly outperforming APACHE II (0.708, 0.701), SOFA (0.699, 0.685), SIRS (0.656, 0.649), and CTSI (0.661, 0.658) (all P < 0.05). The model showed good calibration (Hosmer-Lemeshow test P > 0.05) and provided a superior net clinical benefit across a wide range of threshold probabilities in DCA. SHAP analysis revealed that Ca2⁺ was the most influential predictor, followed by HR and CRP. To enhance clinical usability, we developed an interactive web-based calculator using the R Shiny framework.
Conclusion: This study developed and validated an XGBoost-based prediction model that uses seven easily obtained clinical variables for early identification of severe HTG-AP. The model demonstrated favorable discrimination, good calibration, and meaningful clinical utility, and outperformed traditional scoring systems. It offers a promising tool to improve risk stratification in HTG-AP.
Keywords: hypertriglyceridemia, acute pancreatitis, XGBoost, HTG-AP, severity
Introduction
Acute pancreatitis (AP) is a common gastrointestinal emergency worldwide with various etiologies. Over the past decade, the incidence of hypertriglyceridemia-associated acute pancreatitis (HTG-AP) has risen significantly.1 In China, due to lifestyle changes and the rising prevalence of metabolic syndrome, HTG-AP has become the second most frequent cause of AP after gallstone migration, accounting for up to 20–30% of cases.2–4
Beyond this, HTG-AP is characterized by a more severe clinical course.5,6 HTG-AP patients face a significantly higher risk of progressing to severe acute pancreatitis (SAP) and experiencing life-threatening complications compared to AP of other etiologies.7–9 A recent systematic review of 56,617 AP patients worldwide revealed that HTG-AP was associated with higher mortality rates (up to 20.0% vs. 15.2%) and greater severity than non-HTG-AP.10 This clinical variability likely stems from its unique pathophysiology, which involves the cytotoxicity of free fatty acids,11 a more intense systemic inflammatory response,12 and frequent underlying metabolic comorbidities.13,14 Consequently, HTG-AP presents substantial challenges for clinical management, highlighting the importance of early identification of high-risk patients and the implementation of targeted interventions to improve outcomes.
Early identification of SAP is essential in clinical management, as timely and aggressive interventions including fluid resuscitation, lipid-lowering therapy, and intensive care may improve clinical outcomes.15 Traditional multifactorial scoring systems, such as APACHE II, Ranson’s score, BISAP, and the CT severity index (CTSI), are widely used in clinical practice for early severity prediction across the overall AP population.16 However, these systems were not designed to differentiate between etiologies and did not incorporate HTG-specific predictors. Studies have shown that the predictive accuracy of these general scores may underestimate or overestimate patients’ actual risks in the HTG-AP population.17 Although recent investigations have explored single biomarkers or modified scores for predicting HTG-AP severity, most were based on single-center, small-sample retrospective cohorts, and many predictive models did not undergo independent external validation or adequately consider the accessibility of clinical indicators.18–23 A dedicated, well-validated prediction model integrating clinical parameters and etiology-specific factors, derived from prospective multicenter data is still lacking. In light of this clinical need, the present study developed and validated an early prediction model for severe HTG-AP based on a multicenter prospective cohort in China.
Methods
Study Design
This study was a prediction model investigation, designed and reported in strict accordance with the Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD) statement. The research was conducted in two distinct phases. A prediction model for the early identification of severe HTG-AP was developed using data from an existing multicenter, prospective observational cohort (the PERFORM study, Chinese Clinical Trial Registry, ChiCTR2000039541).24 The derived model was subsequently externally validated using an independent, single-center, prospectively collected cohort of HTG-AP patients (Chinese Clinical Trial Registry, ChiCTR2400079742).
The study protocol was approved by the Institutional Review Boards or Ethics Committees of all participating centers. The master protocol for the multicenter study was approved by the Ethics Committee of Jinling Hospital, Nanjing University (No. 2020NZKY-016-01), and the single-center cohort used for validation was separately approved by the Ethics Committee of the General Hospital of Ningxia Medical University (No. KYLL-2023-0533). As this study involved a post-hoc analysis of an existing multicenter cohort, for which written informed consent had already been obtained from all patients at the time of original data collection, the ethics committees granted a waiver of the requirement to obtain additional informed consent for this analysis. For the prospective single-center validation cohort, written informed consent was obtained from each participant prior to enrollment.
Study Participants
The data for the derivation cohort were sourced from the PERFORM study. The PERFORM study is a long-running, prospective, non-blind, observational cohort study designed to assess whether different triglyceride-lowering therapies affect organ function, and to date it has yielded predominantly negative results.24 In this analysis, patients enrolled from November 30, 2020 to June 30, 2023 were included. The validation cohort consisted of an independent, prospectively maintained cohort of HTG-AP patients at the General Hospital of Ningxia Medical University from January 1, 2024 to May 31, 2025.
To ensure homogeneity, consistent patient selection criteria were applied to both cohorts. The diagnosis of AP was based on the Revised Atlanta Classification criteria. The inclusion criteria were: (1) adult patients aged 18–70 years; (2) hospital admission within 72 hours of pain onset; (3) a serum triglyceride level >11.3 mmol/L upon enrollment (or >1000 mg/dL); and (4) the presence of at least one predefined “worrisome feature” described in detail by Gelrud et al on UpToDate25 For this analysis, participants were excluded if they met any of the following conditions: (1) AP attributable to other etiologies. (2) Presence of uncorrectable acidosis (pH < 7.15) or hyperkalemia (≥ 6.5 mmol/L) at enrollment, requiring urgent continuous renal replacement therapy (CRRT). (3) Contraindications to therapeutic plasma exchange. (4) Failure to provide informed consent. (5) Pregnancy, lactation, or intention to conceive within one month following the trial (applies to both female and male participants). (6) Direct affiliation with the trial’s sponsor or investigators, or being an immediate family member thereof. (7) Any other condition that, in the investigator’s judgment, rendered the participant unsuitable for the trial.
Data Collection
The following variables, recorded within 24 hours of enrollment, were collected from electronic medical records including gender, age, body mass index (BMI), history of hyperlipidemia, family history of hyperlipidemia, smoking history, alcohol abuse history, diabetes mellitus, body temperature (T), heart rate (HR), respiratory rate (RR), systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), amylase (AMY), lipase (LIP), white blood cell count (WBC), neutrophil percentage (NEUT%), lymphocyte percentage (LYMPH%), neutrophil-to-lymphocyte ratio (NLR), hematocrit (HCT), coefficient of variation of red blood cell distribution width (RDW-CV), platelet count (PLT), prothrombin time (PT), activated partial thromboplastin time (APTT), thrombin time (TT), fibrinogen (FIB), D-dimer (D-D), aspartate aminotransferase (AST), alanine aminotransferase (ALT), triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), apolipoprotein A1 (APOA1), apolipoprotein B (APOB), total bilirubin (TBIL), serum creatinine (SCr), lactate dehydrogenase (LDH), creatine kinase (CK), creatine kinase-MB isoenzyme (CK-MB), C-reactive protein (CRP), procalcitonin (PCT), pH, lactate (Lac), blood potassium (K+), blood sodium (Na+), calcium (Ca2+), blood glucose (GLU), and presence or absence of fatty liver, pulmonary infection, pleural effusion, or ascites according to the initial abdominal or chest CT scan. Additionally, established clinical severity scores were collected, including the Sequential Organ Failure Assessment score (SOFA, 0–24 scores), Acute Physiology And Chronic Health Evaluation II score (APACHE II, 0–71 scores), Balthazar CT Severity Index (CTSI, 0–10 scores) and Systemic Inflammatory Response Syndrome score (SIRS, 0–32 scores). If multiple measurements were taken within 24 hours of admission, the most abnormal value was recorded.
Primary Outcome
The primary outcome of this prediction model was the development of SAP within 28 days of enrollment. Severe HTG-AP was strictly defined according to the 2012 Revised Atlanta Classification criteria,26 which require the presence of persistent organ failure (affecting the respiratory, cardiovascular, or renal systems for more than 48 hours). All outcome assessments were independently adjudicated by two senior pancreatologists who were blinded to the predictor variables. Any discrepancies were resolved by consensus with a third expert. Patients were divided into SAP and non-SAP groups based on the occurrence of SAP.
Construction of SAP Prediction Model
Missing data were handled prior to model development to ensure data quality and model generalizability. Variables with a missing rate greater than 20% were excluded due to the lack of a reliable basis for imputation.27,28 For predictor variables with a missing rate of ≤ 20%, multiple imputation under a Bayesian framework was performed to generate 10 complete datasets, thereby reducing the risk of variance underestimation associated with single imputation. To assess the robustness of the imputation strategy, a sensitivity analysis was performed using 20 imputations. The Least Absolute Shrinkage and Selection Operator (LASSO) regression algorithm was applied to select clinical features and identify the optimal combination for predicting SAP. Given the superior performance of the eXtreme Gradient Boosting (XGBoost) algorithm in small-sample classification tasks as reported in previous studies,29–31 the XGBoost model was used in this study. Variables identified through LASSO regression were subsequently incorporated into the XGBoost model to capture potential nonlinear relationships and interactions. The model was externally validated in the independent validation cohort.
Performance Evaluation of the Prediction Model
The predictive performance of the model was evaluated in terms of discrimination, calibration, and clinical utility. Discrimination was assessed by plotting the receiver operating characteristic (ROC) curve and calculating the area under the curve (AUC), accuracy (ACC), sensitivity (SEN), specificity (SPE), positive predictive value (PPV), and negative predictive value (NPV). An AUC value closer to 1 indicates better discriminative ability. The nonparametric DeLong test was used to compare the AUC of our model with that of traditional severity scoring systems. Calibration was evaluated by constructing calibration curves and conducting the Hosmer-Lemeshow goodness-of-fit test. A P-value ≥ 0.05 suggests a good consistency between the predicted risk and the actual observed risk. Decision curve analysis (DCA) was applied to assess the clinical net benefit and utility of the model. For external validation, the same evaluation metrics and statistical methods described above were used to verify the external generalizability of the model.
Model Interpretability Analysis
To enhance model interpretability, we employed the SHapley Additive exPlanations (SHAP) framework to analyze the prediction model built using the XGBoost algorithm. By visualizing global feature importance and the contribution of each variable to individual patient predictions, the association between each predictive variable and the outcome of SAP was clarified.
Statistical Analysis
Statistical analyses were performed using Stata 15.0 (StataCorp LLC, College Station, TX, USA) and R 4.2.1 software (R Core Team, Vienna, Austria). Categorical data were presented as frequencies (percentages), and comparisons between groups were conducted using the Pearson’s chi-square test. Normally distributed continuous data were expressed as mean ± standard deviation ( ), and the independent samples t-test was used for between-group comparisons. Non-normally distributed continuous data were described as medians and interquartile range (IQR), and the Mann–Whitney U-test was employed for group comparisons. All hypothesis tests were two-tailed, and a P-value ≤ 0.05 was considered statistically significant.
), and the independent samples t-test was used for between-group comparisons. Non-normally distributed continuous data were described as medians and interquartile range (IQR), and the Mann–Whitney U-test was employed for group comparisons. All hypothesis tests were two-tailed, and a P-value ≤ 0.05 was considered statistically significant.
Results
Comparisons of Baseline Characteristics, Traditional Severity Scores, and Outcomes Between the Derivation Cohort and Validation Cohort
A total of 623 HTG-AP patients were enrolled in this study, including 478 patients in the derivation cohort and 145 patients in the independent external validation cohort (Figure 1). Initially, 53 clinical variables were collected for model development. Among these, six variables (ApoA1, ApoB, LDH, CK, CK-MB, LIP) were excluded due to a missing rate exceeding 20%. The baseline clinical characteristics, traditional severity scores, and outcomes of the two cohorts are summarized in Table 1. Although statistically significant differences were observed in some baseline indicators between the two cohorts, several key clinical variables and outcomes showed no significant differences, including gender, age, BMI, mortality rate, and proportion of SAP (all P > 0.05). Regarding traditional severity scoring systems, there was no statistically significant difference between the two cohorts in most scoring systems (APACHE II, SIRS, SOFA, all P > 0.05), except that the CTSI score was significantly higher in the validation cohort than in the derivation cohort (P < 0.05).
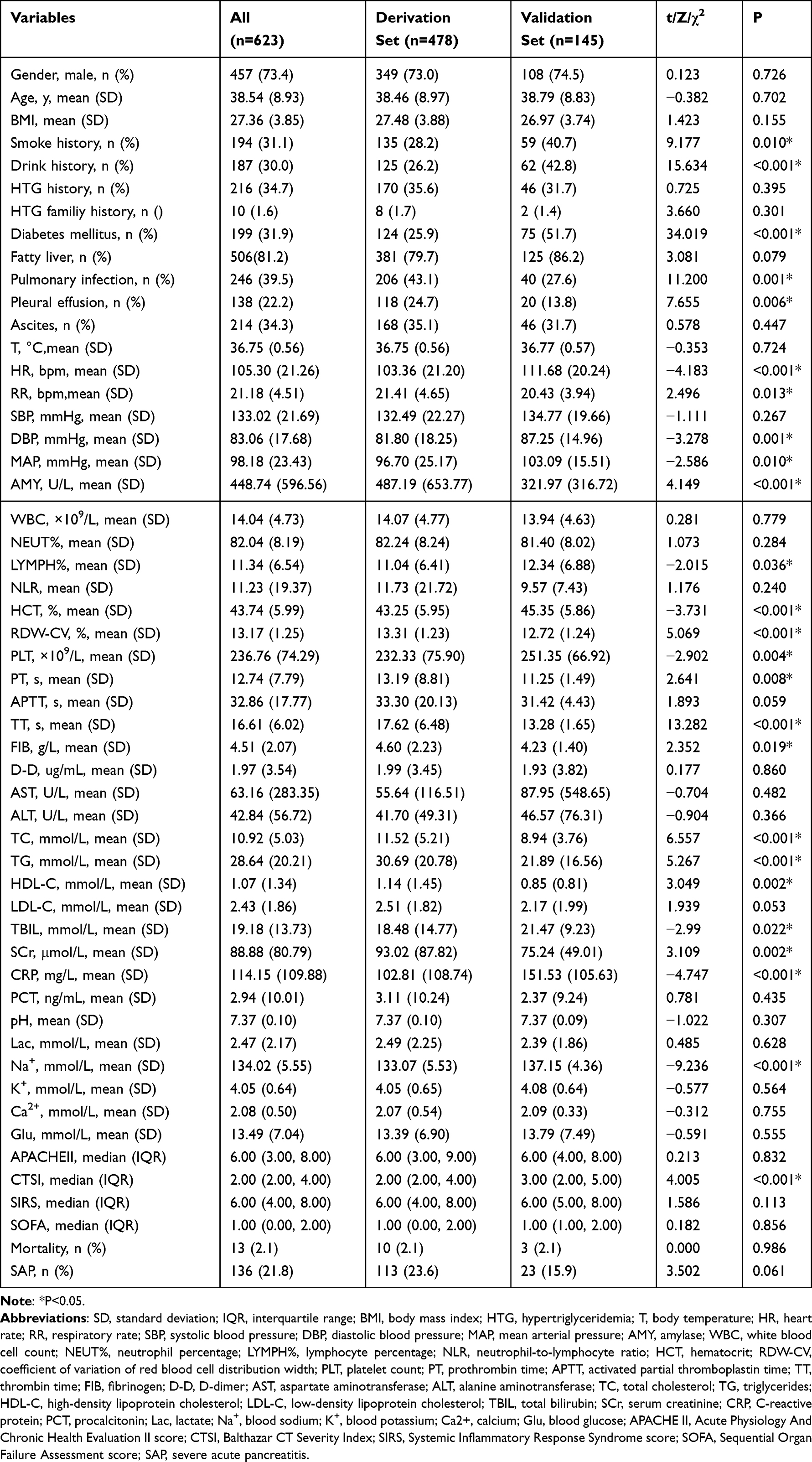 |
Table 1 Comparison of Baseline Clinical Characteristics and Outcomes of HTGAP in the Derivation Set and Validation Set |
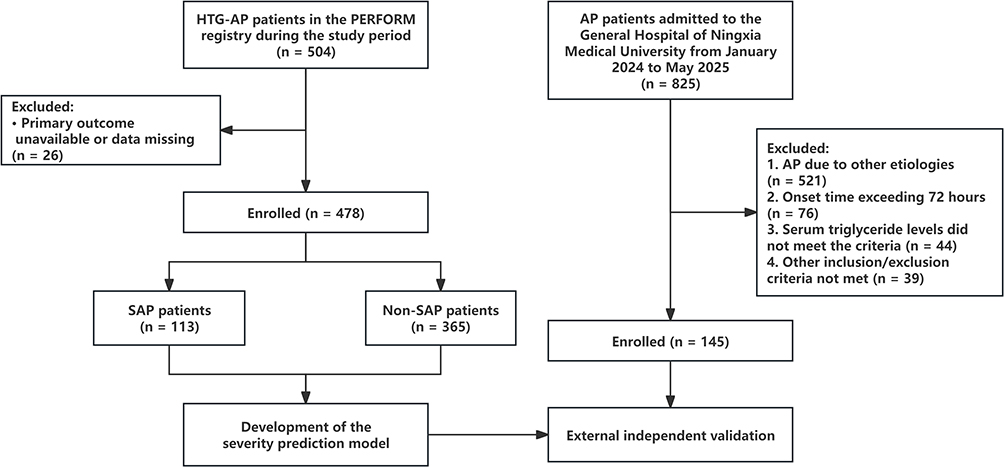 |
Figure 1 The flowchart of participants through this study. |
Comparisons of Clinical Indicators, Traditional Severity Scores and Mortality Between SAP and Non-SAP Patients Within Each Cohort
Baseline clinical characteristics, traditional severity scores, and outcome comparisons between SAP and non-SAP patients are summarized in Table 2. In the derivation cohort, a total of 113 (23.6%) patients were diagnosed with SAP, and 10 (2.1%) cases were fatal. Notably, no deaths were observed in the non-SAP group, compared with a mortality rate of 8.8% in the SAP group. Compared to non-SAP patients, SAP patients in the derivation cohort had significantly higher proportions of smoking history, drinking history, history of HTG-AP, pulmonary infection, pleural effusion and ascites and higher levels of T, HR, RR, AMY, NEUT%, APTT, FIB, D-D,TBIL, SCr, CRP, PCT, Lac, K+, GLU (all P < 0.05). Meanwhile, the levels of LYMPH%, LDL-C, PLT, pH, and Ca2+ were significantly lower in SAP patients than in non-SAP patients (all P < 0.05). Furthermore, SAP patients exhibited significantly higher scores in traditional disease severity scoring systems (all P < 0.05).
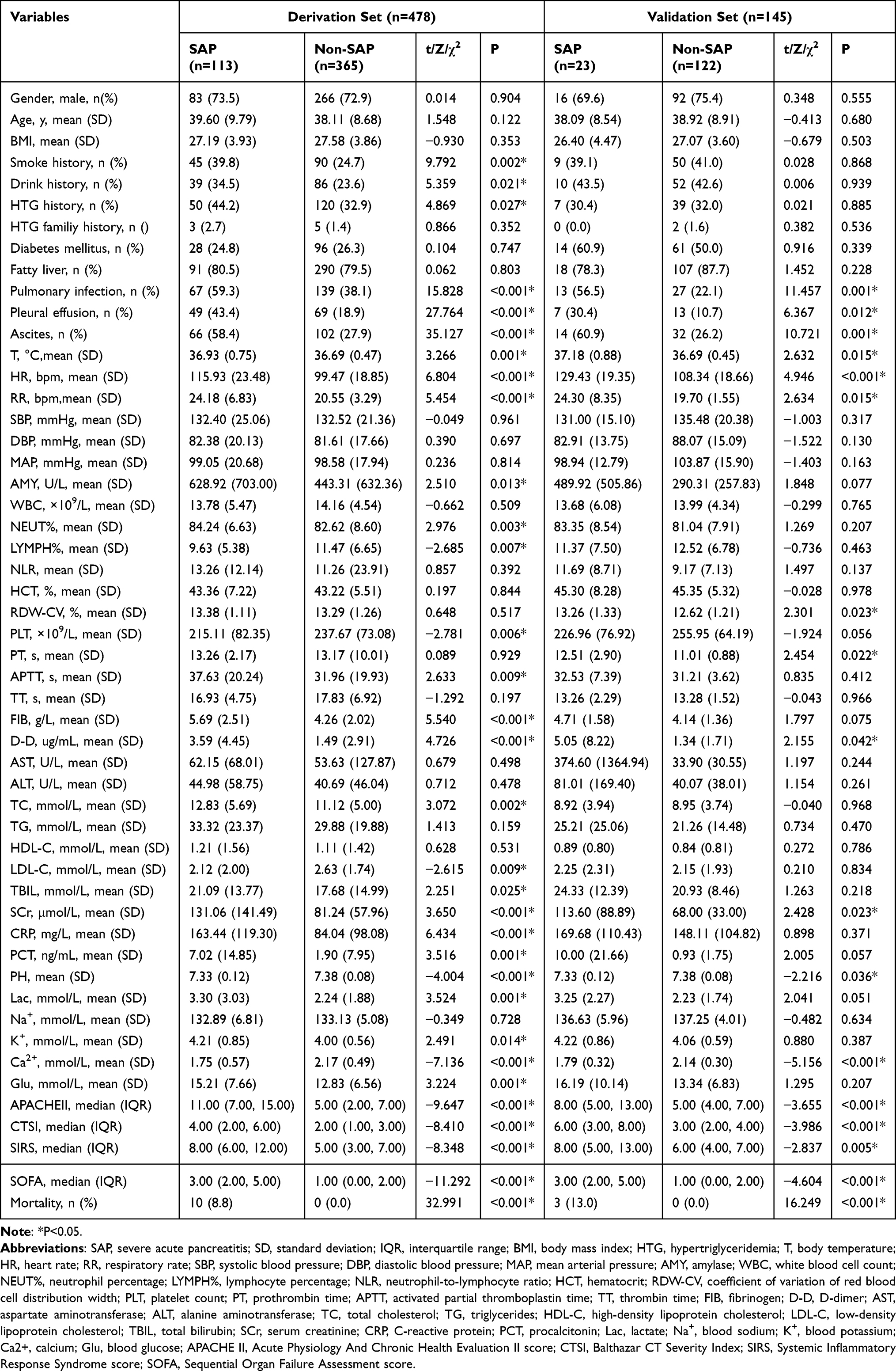 |
Table 2 Comparison of Baseline Clinical Characteristics and Outcomes of SAP and Non-SAP in Two Sets |
Consistent with the derivation cohort, SAP patients in the validation cohort had significantly higher rates of pulmonary infection, pleural effusion, and ascites, higher levels of T, HR, RR, D-D, SCr, and lower levels of pH and Ca2⁺compared to non-SAP patients (all P < 0.05). Similarly, SAP patients scored significantly higher on traditional disease severity scoring systems (all P < 0.05), and no fatalities occurred in the non-SAP group compared with 13.0% in the SAP group. However, unlike in the derivation cohort, SAP patients in the validation cohort also exhibited significantly elevated levels of RDW-CV and PT (both P < 0.05). There were no significant differences in TG levels between the two groups in either cohort (P > 0.05).
LASSO Regression for Variable Selection
LASSO regression was applied to all candidate predictor variables to identify features associated with SAP (Figure 2A). Among the 47 variables included, seven predictive variables were selected using tenfold cross-validation at the optimal penalty parameter lambda (λ) (Figure 2B), including Ca2+, HR, CRP, D-D, RR, SCr and pleural effusion.
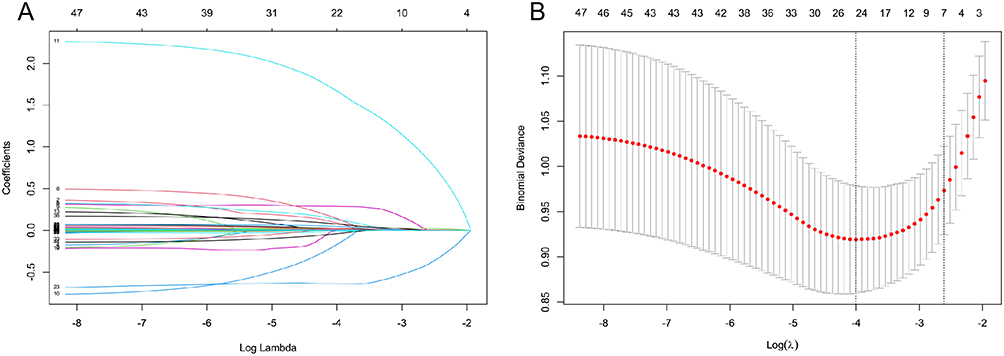 |
Figure 2 Variable selection using the least absolute shrinkage and selection operator (LASSO) regression. (A) LASSO coefficient path plot showing how regression coefficients shrink toward zero as the penalty parameter λ increases; less important variables are eliminated while important predictors are retained. (B) Selection of the optimal λ by cross-validation. Binomial deviance is plotted against log(λ); the vertical lines indicate λ values used to choose a parsimonious model. Based on this, seven predictors were selected for the final model. |
Model Development, External Validation and Evaluation
We constructed an XGBoost prediction model using the XGBoost package in R language, based on the variables screened by LASSO regression. For a comprehensive assessment of the model’s predictive efficacy in practical scenarios, the predictive performance of the constructed model was evaluated by comparing it with existing scoring systems (SOFA, APACHE II, CTSI and SIRS, detailed in Tables 3 and 4). The AUC of our model was 0.873 in the derivation cohort and the validation cohort (Tables 3 and 4), which was superior to that of traditional scoring systems including SOFA (0.841, 0.793), APACHE II (0.799, 0.739), CTSI (0.749, 0.758), and SIRS (0.758, 0.685). The results also showed that the XGBoost model had excellent performance across other evaluation metrics, particularly SEN and NPV in both cohorts. Sensitivity analysis using 20 imputations yielded results consistent with the main analysis, supporting the robustness of the imputation strategy.
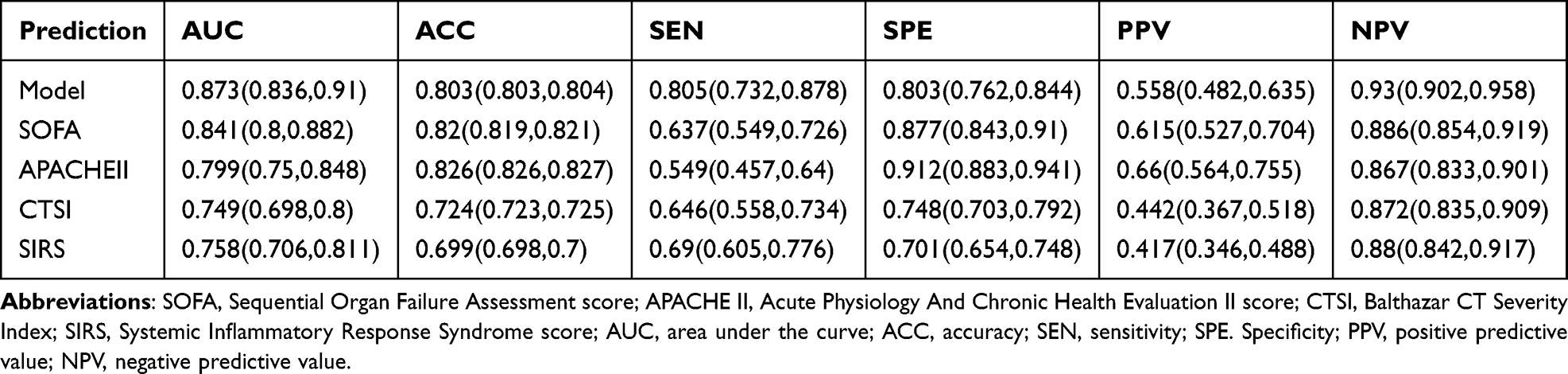 |
Table 3 Prediction Performance of Each Metric in the Derivation Set |
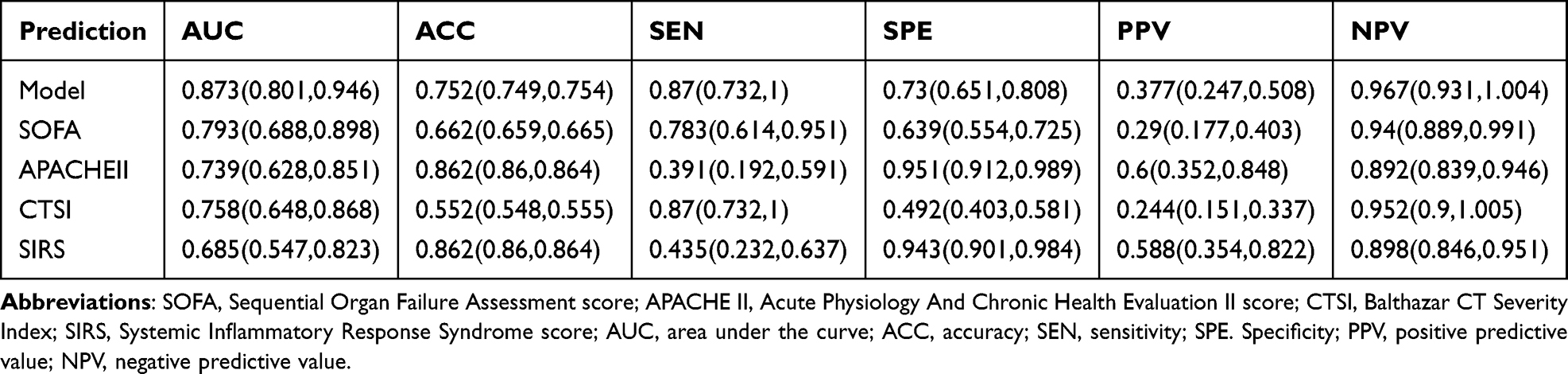 |
Table 4 Prediction Performance of Each Metric in the Validation Set |
The calibration curves for SAP prediction in the derivation and validation cohorts showed excellent agreement between the model-predicted probabilities and the actual observations (Figure 3A and C). To assess the clinical utility of the XGBoost model, decision curve analysis (DCA) was performed in both cohorts. The XGBoost model achieved a higher net clinical benefit than traditional severity scoring systems across a clinically relevant range of threshold probabilities (Figure 3B and D).
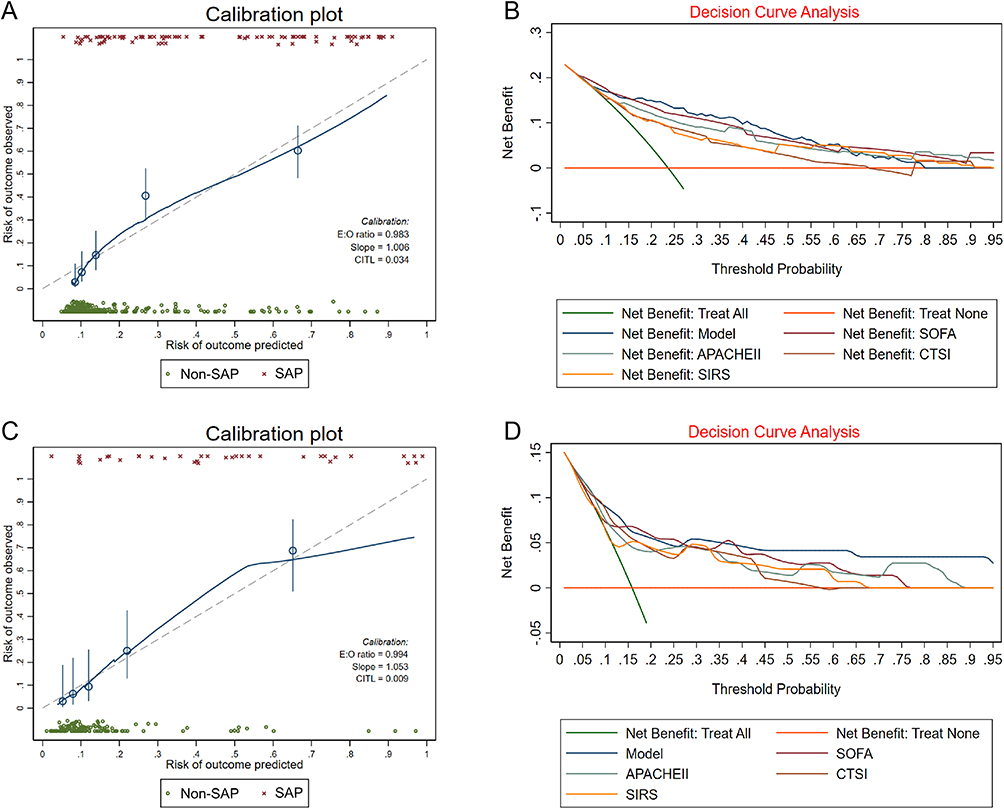 |
Figure 3 Performance evaluation of the XGBoost prediction model in the derivation and validation cohorts. (A and C) Calibration curves for severe acute pancreatitis (SAP) risk prediction. The diagonal dashed line represents perfect prediction, where predicted probabilities exactly match observed outcomes. The solid lines show the calibration performance of the XGBoost model in the derivation cohort (A) and the validation cohort (C). Closer alignment with the diagonal indicates better calibration. (B and D) Decision curve analysis (DCA) for the XGBoost model compared with traditional severity scoring systems. The y-axis represents net benefit, and the x-axis shows the threshold probability for predicting SAP. The XGBoost model (red line) demonstrated superior net clinical benefit across a clinically relevant range of threshold probabilities compared to the SOFA, APACHE II, CTSI, and SIRS scores in both the derivation (B) and validation (D) cohorts. The red horizontal line represents the strategy that no patients are treated, and the green diagonal line represents the strategy that all patients are treated. |
Model Interpretation
The SHAP feature importance plot visually displays the ranked importance of the predictive variables in the XGBoost model. Figure 4A shows that Ca2+ had the greatest influence on model prediction, followed by HR, CRP, D-D, and other variables. The SHAP summary plot (Figure 4B) was employed to interpret the XGBoost model output. It visualizes the contribution of each variable to the SAP risk prediction. The feature value of each variable for individual patients is represented by a color gradient. The SHAP value quantifies the impact of each feature on the model’s output, with positive values indicating a contribution to a higher risk of SAP and negative values indicating a contribution towards a lower risk. Overall, elevated levels of HR, CRP, D-D, RR, and SCr, as well as the presence of pleural effusion, were positively associated with an increased predicted risk of SAP, whereas higher values of Ca2+ contributed negatively to the risk prediction. To illustrate the model interpretability, we presented a typical SAP case predicted using the SHAP waterfall plot (Figure 4C). This plot depicts the contribution of each clinical feature to the individual prediction outcome.
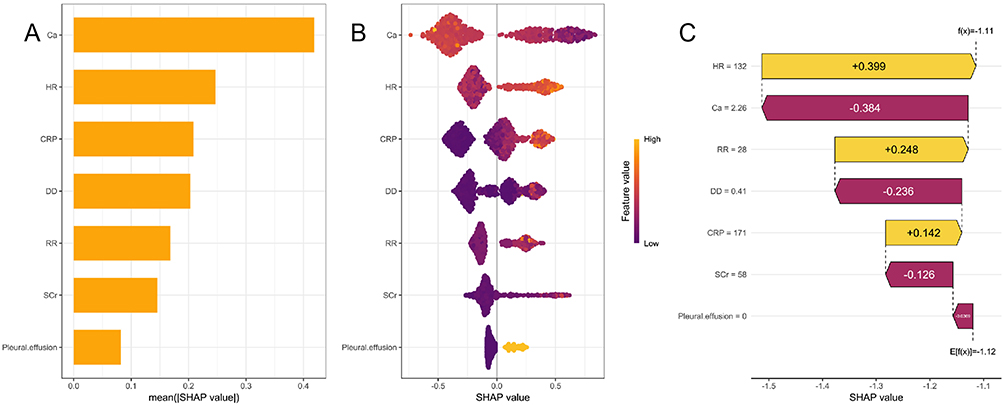 |
Figure 4 SHapley Additive exPlanations (SHAP) analysis of the XGBoost model. (A) SHAP feature importance bar plot. Features are ranked on the y-axis in descending order of importance, with the most influential variable at the top. The x-axis represents the mean absolute SHAP value, indicating the average impact of each feature on the model output magnitude across all patients. (B) SHAP summary plot. Each point represents a single patient’s SHAP value for a given feature. The x-axis shows the SHAP value (impact on model output), where positive values push the prediction toward SAP and negative values toward non-SAP. Feature values are color-coded from low (blue) to high (yellow). (C) SHAP waterfall plot for a representative patient. The y-axis lists features in descending order of contribution to this individual’s prediction. The x-axis shows SHAP values, with yellow bars indicating features that increase the predicted risk of SAP and red bars indicating features that decrease the risk. The length of each bar reflects the magnitude of their contribution. |
To facilitate clinical application of the prediction model, we developed an interactive web-based calculator using the R Shiny framework. The tool requires input of the predictors identified in our final model. Upon entry of these values, the calculator automatically generates the predicted probability of SAP. The web-based calculator is freely accessible at: https://rubyly123.shinyapps.io/HTGSAP_model/.
Discussion
In this study, we developed and validated an early prediction model for severe HTG-AP based on a multicenter prospective cohort in China (the PERFORM study). The results showed that the XGBoost model consistently achieved an AUC of 0.873 in both the derivation and external validation cohorts, significantly outperforming traditional scoring systems (APACHE II, SOFA, SIRS and, CTSI). The model also showed good calibration and provided a superior net clinical benefit across a clinically relevant range of threshold probabilities in decision curve analysis.
Although previous studies have explored single biomarkers or modified scores for predicting HTG-AP severity, these investigations have largely been based on single-center, small-sample retrospective cohorts.20–23 Furthermore, some predictive models did not undergo independent external validation or did not adequately consider the accessibility of clinical indicators. During our model design process, particular attention was paid to both generalizability and clinical practicality. Variables with missing rates exceeding 20% were excluded, indicating that these indicators were not routinely available in all medical centers. In contrast, the included variables were routinely measured after admission in hospitals at various levels, thereby facilitating the model’s clinical implementation. In addition, the model was developed based on multicenter data and externally validated using an independent single-center cohort to assess stability across different populations. Many previous studies on predicting the severity of HTG-AP have used logistic regression to build prediction models.20,22 In our study, we instead applied a machine learning algorithm (XGBoost) to better capture complex nonlinear relationships. We further used SHAP analysis to quantify the contribution of each predictor at both the global and individual-patient levels, thereby improving model interpretability. In addition, we developed a user-friendly web-based calculator (R Shiny) to facilitate bedside clinical application. We also systematically compared our model with conventional scoring systems (SOFA, APACHE II, CTSI, and SIRS) to assess its relative performance. The model demonstrated superior AUC, SEN, and NPV, supporting its use as an early screening tool for severe HTG-AP in the emergency setting to facilitate timely risk alert and intervention.
Given that the PERFORM study reported negative results,24 the potential confounding effect of treatment modalities on patient outcomes was likely minimized. Notably, although statistically significant differences were observed in certain baseline indicators between the multicenter derivation cohort and the single-center validation cohort, key clinical outcomes (SAP incidence, mortality) showed no significant differences. The presence of such baseline discrepancies also supports the stability and generalizability of our model across different centers and populations and suggests that the model was not overfit to the derivation cohort.
In both cohorts of this study, admission TG levels were markedly elevated, yet no significant differences were observed between the SAP and non-SAP groups (P > 0.05). This finding is consistent with previous research and clinical practice.32 Although HTG-AP occurrence requires exceeding a certain TG threshold, once pancreatitis is triggered, subsequent disease progression depends more on the intensity of the individual inflammatory response.33 Similarly, no significant differences were found for other markers of metabolic abnormalities, such as reduced HDL-C levels, elevated BMI, and coexistent fatty liver and diabetes mellitus. This suggests that a state of metabolic disturbance is a common underlying feature in patients with HTG-AP, rather than a specific predictor of disease severity.
The seven predictive indicators included in our model have clear pathophysiological foundations and have been recognized as independent predictors of HTG-AP severity in previous studies.20–22,34–36 These predictors capture distinct yet interconnected pathophysiological domains: systemic inflammation (CRP, HR, RR), coagulation activation and microvascular dysfunction (D-D), organ injury (Ca2⁺, SCr), and local complications (pleural effusion). Their combination provides a multidimensional snapshot from the initial inflammatory insult to downstream organ dysfunction. Among these, serum calcium (Ca2⁺) emerged as the most important predictor in SHAP analysis. Beyond reflecting pancreatic necrosis via calcium-soap formation,37 hypocalcemia directly participates in multiple organ dysfunction by impairing myocardial contractility, neuromuscular excitability, and coagulation.38,39 CRP, HR, and RR collectively represent the inflammatory burden and the body’s compensatory response.40,41 Their inclusion in our prediction model further confirms the central role of inflammation in HTG-AP severity. D-dimer (D-D) is a degradation product of cross-linked fibrin that reflects coagulation activation and hyperfibrinolysis. High concentrations of free fatty acids may damage vascular endothelial cells, activate the extrinsic coagulation pathway, and promote microthrombus formation.42–44 Elevated serum creatinine (SCr) reflects renal impairment and often correlates with poor prognosis. Previous studies have shown that the development of acute kidney injury frequently occurs in conjunction with respiratory or circulatory failure in AP patients,45,46 underscoring its role as a marker of significant escalation in disease severity. The development of pleural effusion is largely attributable to heightened vascular permeability induced by pro-inflammatory factors. It can also exacerbate respiratory dysfunction by restricting lung expansion and affecting gas exchange.47,48 These factors capture the pathophysiological cascade from microvascular injury to overt organ dysfunction. Based on these pathophysiological insights, the SHAP analysis yields several clinically actionable implications for HTG-AP management. Serum calcium (Ca2⁺) emerged as the dominant predictor, supporting a simple and rapid admission-based risk stratification approach. During subsequent management, persistent hypocalcemia or rising D-dimer may indicate treatment failure and should prompt escalation of care. In addition, the waterfall plot helps clarify which specific features drive risk in individual patients, thereby enabling more targeted interventions and facilitating shared decision-making.
This study has several limitations. First, some potentially important predictors were excluded due to missing rates exceeding 20%. Although this approach improved model generalizability, it may have compromised some predictive performance to some extent. Additionally, some potentially useful prognostic factors may not have been included in the original prospective study protocol and therefore could not be evaluated in our model. Future studies incorporating a broader range of predictors may further improve predictive accuracy. Second, while the multicenter design enhances the representativeness of our model, the sample size may still be insufficient to draw definitive conclusions. Additionally, internal validation was not performed due to the limited sample size, as splitting the data would have further reduced the derivation set and potentially led to model instability. Thus, future large-scale studies should incorporate both internal and external validation to confirm these results. Third, although single-center external validation was performed, both validation and derivation cohorts were from China. Future validation in diverse ethnic and geographic populations is warranted to confirm the generalizability of our model.
In conclusion, the XGBoost prediction model developed in this study effectively identifies patients at high risk for severe HTG-AP and outperforms traditional scoring systems. The seven indicators included in the model are routinely measured clinical parameters, which enhances the model’s generalizability and facilitates its clinical translation. With further validation and implementation as a clinical prediction tool, this model may support early risk stratification and guide timely intervention strategies.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to privacy and ethical restrictions but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study protocol was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Boards and/or Ethics Committees of all participating centers. For the multicenter study, the master protocol was approved by the Ethics Committee of Jinling Hospital, Nanjing University (Approval No.: 2020NZKY-016-01). The single-center validation cohort was approved separately by the Ethics Committee of the General Hospital of Ningxia Medical University (Approval No.: KYLL-2023-0533).
Since this study involved a post-hoc analysis of an existing multicenter cohort for which written informed consent had been obtained from all patients at the time of original data collection, the ethics committees granted a waiver of the requirement for additional informed consent specific to this secondary analysis. For the prospective single-center validation cohort, written informed consent was obtained from all individual participants prior to enrollment.
Acknowledgments
Gratitude is extended to all patients and healthcare staff who participated in the study. The authors acknowledge the Chinese Acute Pancreatitis Clinical Trials Group (CAPCTG) for its role in study coordination and data collection. We also thank all members of the CAPCTG for their contributions.
Collaborators
The Chinese Acute Pancreatitis Clinical Trials Group (CAPCTG) includes the following participants (in alphabetical order):
Baiqiang Li, Jinling Hospital, Medical School of Nanjing University, Nanjing, Jiangsu, China; Bing Xue, Shangqiu First People’s Hospital, Shangqiu, Henan, China; Bin Wu, The Third Hospital of Xiamen City, Xiamen, Fujian, China; Chengjian He, Nanhua Hospital, Hengyang, Hunan, China; Dahuan Li, The First Affiliated Hospital and College of Clinical Medicine of Henan University of Science and Technology, Luoyang, Henan, China; Dandan Zhou, Jiangsu Provincial Hospital of Integrated Chinese and Western Medicine, Nanjing, Jiangsu, China; Dongliang Yang, The First Affiliated Hospital of the University of Science and Technology of China, Hefei, Anhui, China; Dongsheng Zhao, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, China; Fang Shao, Nanjing Medical University, Nanjing, Jiangsu, China; Feng Zhou, The First Affiliated Hospital of Wannan Medical College, Wuhu, Anhui, China; Guixian Luo, Qianxinan People’s Hospital, Xingyi, Guizhou, China; Guobing Chen, First People’s Hospital of Yunnan Province, Kunming, Yunnan, China; Guoxiu Zhang, The First Affiliated Hospital and College of Clinical Medicine of Henan University of Science and Technology, Luoyang, Henan, China; Haibin Ni, Jiangsu Provincial Hospital of Integrated Chinese and Western Medicine, Nanjing, Jiangsu, China; Hong Gao, The Qujing NO1 People’s Hospital, Qujing, Yunnan, China; Hong Mei, The Affiliated Hospital of Zunyi Medical University, Zunyi, Guizhou, China; Hongguo Yang, Zhejiang Provincial People’s Hospital, Hangzhou, Zhejiang, China; Honghai Xia, The First Affiliated Hospital of the University of Science and Technology of China, Hefei, Anhui, China; Hongyi Yao, Nanhua Hospital, Hengyang, Hunan, China; Huaguang Ye, The Third Hospital of Xiamen City, Xiamen, Fujian, China; Jianfeng Tu, Zhejiang Provincial People’s Hospital, Hangzhou, Zhejiang, China; Jiajia Lin, Jinling Hospital, Medical School of Nanjing University, Nanjing, Jiangsu, China; Jingchun Song, 94th Hospital of PLA, Nanchang, Jiangxi, China; Jingyi Wu, The First Affiliated Hospital of Wannan Medical College, Wuhu, Anhui, China; Jiyan Lin, The First Affiliated Hospital of Xiamen University, Xiamen, Fujian, China; Junli Sun, Luoyang Central Hospital, Luoyang, Henan, China; Kang Li, The Affiliated Hospital of Zunyi Medical University, Zunyi, Guizhou, China; Keke Xin, Luoyang Central Hospital, Luoyang, Henan, China; Lei Yu, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, China; Lening Ren, The First Affiliated Hospital and College of Clinical Medicine of Henan University of Science and Technology, Luoyang, Henan, China; Liang Xia, The First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, China; Lijuan Zhao, First People’s Hospital of Yunnan Province, Kunming, Yunnan, China; Long Fu, Shangqiu First People’s Hospital, Shangqiu, Henan, China; Mei Yang, The Qujing NO1 People’s Hospital, Qujing, Yunnan, China; Mengjie Lu, Jinling Hospital, Medical School of Nanjing University, Nanjing, Jiangsu, China; Miao Chen, The Affiliated Hospital of Zunyi Medical University, Zunyi, Guizhou, China; Min Shao, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, China; Mingfeng Huang, Jinling Hospital, Medical School of Nanjing University, Nanjing, Jiangsu, China; Mingzhi Chen, Jinjiang Hospital of Traditional Chinese Medicine, Quanzhou, Fujian, China; Nonghua Lv, The First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, China; Qiang Li, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, China; Qingbo Zeng, 94th Hospital of PLA, Nanchang, Jiangxi, China; Qingcheng Xu, Clinical Medical College of Yangzhou University, Yangzhou, Jiangsu, China; Qingyun Zhu, The Affiliated Hospital of Qingdao University, Qingdao, Shandong, China; Quanxing Feng, The Fourth Military Medical University, Xian, Shanxi, China; Shan Xu, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, China; Shumin Tu, Shangqiu First People’s Hospital, Shangqiu, Henan, China; Shusheng Zhou, The First Affiliated Hospital of the University of Science and Technology of China, Hefei, Anhui, China; Songjing Shi, Fujian Province Hospital, Fuzhou, Fujian, China; Wei Zhao, Qilu Hospital of Shandong University, Jinan, Shandong, China; Weihua Lu, The First Affiliated Hospital of Wannan Medical College, Wuhu, Anhui, China; Weili Gu, Affiliated Hospital 2 of Nantong University, Nantong, Jiangsu, China; Weiwei Chen, Clinical Medical College of Yangzhou University, Yangzhou, Jiangsu, China; Wenhua He, The First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, China; Xiaofei Huang, Jiangsu Provincial Hospital of Integrated Chinese and Western Medicine, Nanjing, Jiangsu, China; Xiaomei Chen, Qilu Hospital of Shandong University, Jinan, Shandong, China; Xiangyang Zhao, Qilu Hospital of Shandong University, Jinan, Shandong, China; Xinting Pan, The Affiliated Hospital of Qingdao University, Qingdao, Shandong, China; Yafei Li, First People’s Hospital of Yunnan Province, Kunming, Yunnan, China; Yan Chen, Jinling Hospital, Medical School of Nanjing University, Nanjing, Jiangsu, China; Yin Zhu, The First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, China; Yongjun Lin, Sir Run Run Shaw Hospital of Zhejiang University, Hangzhou, Zhejiang, China; Youdong Wan, The Affiliated Hospital of Qingdao University, Qingdao, Shandong, China; Yun Zhou, Pingxiang People’s Hospital, Pingxiang, Jiangxi, China; Zhenping Chen, The First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, China; Zhiyong Liu, Xiangya Hospital, Changsha, Hunan, China; Zigui Zhu, Nanhua Hospital, Hengyang, Hunan, China.
Author Contributions
Weijie Yao: Conceptualization, Methodology, Investigation, Writing – Original Draft. Chengsi Zhao: Data Curation, Formal Analysis, Writing – Original Draft. Longxiang Cao: Methodology, Data Curation, Writing – Review & Editing. Huijin Yang: Investigation, Data Curation, Writing – Review & Editing. Yang Liu: Methodology, Formal Analysis, Writing – Review & Editing. Shuai Li: Formal Analysis, Data Curation, Writing – Review & Editing. Lanting Wang: Investigation, Project Administration, Writing – Review & Editing. Jing Zhou: Resources, Validation, Writing – Review & Editing. Zuozheng Wang: Conceptualization, Funding Acquisition, Writing – Review & Editing. Lu Ke: Conceptualization, Supervision, Writing – Review & Editing. Yang Bu: Conceptualization, Supervision, Funding Acquisition, Writing – Review & Editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by 1. Key Program of Ningxia Key Research and Development Program (Grant No.: 2026BEG02011); 2. Ningxia Science and Technology Innovation Leading Talents Program (Grant No.: 2025GKLRLX15, 2021GKLRLX04); 3. Ningxia Natural Science Foundation (Grant No.: 2024AAC03714).
Disclosure
Dr Lu Ke reports Consulting fees from NESTLE; Honoraria from Nutricia; Data safety/advisory board participation from Zhengda Group, outside the submitted work.
Dr Yang Bu reports Support for the manuscript from Ningxia Science and Technology Innovation Leading Talents Program, Key Program of Ningxia Key Research and Development Program, during the conduct of the study, outside the submitted work. All other authors report no conflicts of interest in this work.
References
1. Iannuzzi JP, King JA, Leong JH, et al. Global incidence of acute pancreatitis is increasing over time: a systematic review and meta-analysis. Gastroenterology. 2022;162(1):122–16. doi:10.1053/j.gastro.2021.09.043
2. He W, Wang G, Yu B, et al. Elevated hypertriglyceridemia and decreased gallstones in the etiological composition ratio of acute pancreatitis as affected by seasons and festivals: a two-center real-world study from China. Front Cell Infect Microbiol. 2022;12:976816. doi:10.3389/fcimb.2022.976816
3. Jin M, Bai X, Chen X, et al. A 16-year trend of etiology in acute pancreatitis: the increasing proportion of hypertriglyceridemia-associated acute pancreatitis and its adverse effect on prognosis. J Clin Lipidol. 2019;13(6):947–953.e1. doi:10.1016/j.jacl.2019.09.005
4. Fan Z, Li J, Wu D. Hypertriglyceridemic pancreatitis: perspectives from China. Curr Opin Gastroenterol. 2025;41(5):348–354. doi:10.1097/MOG.0000000000001123
5. Deng H, Peng K, Zhang L, et al. Clinical outcomes in a multicenter cohort involving 919 patients with hypertriglyceridemia-associated acute pancreatitis. Am J Gastroenterol. 2025;120(10):2405–2414. doi:10.14309/ajg.0000000000003319
6. Hu X, Gong L, Zhou R, et al. Variations in gut microbiome are associated with prognosis of hypertriglyceridemia-associated acute pancreatitis. Biomolecules. 2021;11(5):695. doi:10.3390/biom11050695
7. Gu RJ, Zhang YR. Predictive utility of the triglyceride-glucose index and visceral adiposity-related indices for severe progression in hypertriglyceridemic pancreatitis. J Clin Lipidol. 2025;S1933-2874(25):00418. doi:10.1016/j.jacl.2025.09.032
8. Fan Z, Zhang Y, Li J, et al. Global burden and characterization of hypertriglyceridemia-induced acute pancreatitis: results from a systematic review and a multi-center cohort study. Sci China Life Sci. 2025;68(10):3010–3020. doi:10.1007/s11427-024-2900-6
9. Lin XY, Zeng Y, Zhang ZC, Lin ZH, Chen LC, Ye ZS. Incidence and clinical characteristics of hypertriglyceridemic acute pancreatitis: a retrospective single-center study. World J Gastroenterol. 2022;28(29):3946–3959. doi:10.3748/wjg.v28.i29.3946
10. Lu J, Wang Z, Mei W, et al. A systematic review of the epidemiology and risk factors for severity and recurrence of hypertriglyceridemia-induced acute pancreatitis. BMC Gastroenterol. 2025;25(1):374. doi:10.1186/s12876-025-03954-4
11. Zádori N, Gede N, Antal J, et al. EarLy elimination of fatty acids iN hypertriglyceridemia-induced acuTe pancreatitis (ELEFANT trial): protocol of an open-label, multicenter, adaptive randomized clinical trial. Pancreatology. 2020;20(3):369–376. doi:10.1016/j.pan.2019.12.018
12. Wang J, Xia Y, Cao Y, et al. Evaluating the efficacy and timing of blood purification modalities in early-stage hyperlipidemic acute pancreatitis treatment. Lipids Health Dis. 2023;22(1):208. doi:10.1186/s12944-023-01968-z
13. Li Q, Hou C, Peng Y, et al. Diabetes and younger age are vital and independent risk factors for acute pancreatitis in patients with severe hypertriglyceridemia. Biomed Res Int. 2019;2019:2620750. doi:10.1155/2019/2620750
14. Fu ZH, Zhao ZY, Liang YB, et al. Impact of metabolic syndrome components on clinical outcomes in hypertriglyceridemia-induced acute pancreatitis. World J Gastroenterol. 2024;30(35):3996–4010. doi:10.3748/wjg.v30.i35.3996
15. Guilabert L, Cárdenas-Jaén K, Buxbaum JL, et al. Evaluation of the PAN-PROMISE symptom scale in a randomized controlled trial of fluid resuscitation in acute pancreatitis. Am J Gastroenterol. 2025;120(8):1852–1859. doi:10.14309/ajg.0000000000003570
16. Wang CH, Zhai YQ. Additional considerations on a combination of inflammatory markers and scoring systems for early severity stratification of acute pancreatitis. World J Gastroenterol. 2025;31(25):108943. doi:10.3748/wjg.v31.i25.108943
17. Li M, Xing XK, Lu ZH, et al. Comparison of scoring systems in predicting severity and prognosis of hypertriglyceridemia-induced acute pancreatitis. Dig Dis Sci. 2020;65(4):1206–1211. doi:10.1007/s10620-019-05827-9
18. Shuanglian Y, Huiling Z, Xunting L, et al. Establishment and validation of early prediction model for hypertriglyceridemic severe acute pancreatitis. Lipids Health Dis. 2023;22(1):218. doi:10.1186/s12944-023-01984-z
19. Cai W, Bhattacharya P, Li Y, et al. Circulating cyclophilin A levels elevate in animal models and can predict mortality in patients with acute pancreatitis. Pancreatology. 2025;25(3):301–306. doi:10.1016/j.pan.2025.02.012
20. Liu ZY, Tian L, Sun XY, et al. Development and validation of a risk prediction score for the severity of acute hypertriglyceridemic pancreatitis in Chinese patients. World J Gastroenterol. 2022;28(33):4846–4860. doi:10.3748/wjg.v28.i33.4846
21. Wu J, Liang Y, Tang X, et al. Ultra-early indicators of acute hypertriglyceridemic pancreatitis may influence treatment decision-making. Sci Rep. 2025;15(1):1572. doi:10.1038/s41598-025-85847-w
22. Wang Z, Liu Y, Zhang X, et al. Construction of a nomogram for hypertriglyceridemic severe acute pancreatitis that includes metabolic indexes. Lipids Health Dis. 2025;24(1):279. doi:10.1186/s12944-025-02702-7
23. Zhong L, Ding J, Chen M, et al. Novel inflammatory markers and their association with the severity of hypertriglyceridemia-associated acute pancreatitis. J Inflamm Res. 2025;18:14771–14790. doi:10.2147/JIR.S549115
24. Zhou J, Wang Z, Liu Q, et al. Triglyceride-lowering therapies in hypertriglyceridemia-associated acute pancreatitis in China: a multicentre prospective cohort study. BMC Med. 2024;22(1):535. doi:10.1186/s12916-024-03755-8
25. Gelrud A, Whitcomb DC. Hypertriglyceridemia-induced acute pancreatitis. 2021. Available from: https://www.uptodate.com/contents/hypertriglyceridemia-induced-acute-pancreatitis.
26. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–111. doi:10.1136/gutjnl-2012-302779
27. Duflot T, Fayette L, Konecki C, et al. Assessing the impact of multiple imputation algorithms on pharmacokinetic model performance: a Simulation-Based Study. AAPS J. 2025;27(4):77. doi:10.1208/s12248-025-01066-1
28. Stavseth MR, Clausen T, Røislien J. How handling missing data may impact conclusions: a comparison of six different imputation methods for categorical questionnaire data. SAGE Open Med. 2019;7:2050312118822912. doi:10.1177/2050312118822912
29. Shi J, Chen L, Yuan X, et al. A potential XGBoost diagnostic score for staphylococcus aureus bloodstream infection. Front Immunol. 2025;16:1574003. doi:10.3389/fimmu.2025.1574003
30. Zhu H, Zhou Y, Shen D, et al. An interpretable machine learning model for predicting early liver metastasis after pancreatic cancer surgery. BMC Cancer. 2025;25(1):1117. doi:10.1186/s12885-025-14503-3
31. Cisnal A, Ruiz Rebollo ML, Flórez-Pardo C, Matesanz-Isabel J, Pérez Turiel J, Fraile JC. Improved early prediction of acute pancreatitis severity using SHAP-based XGBoost model: beyond traditional scoring systems. Dig Liver Dis. 2026;58(1):104–112. doi:10.1016/j.dld.2025.10.017
32. Liu Y, Cheng JP, Zhao XL. The effect of serum triglyceride levels and different lipid-lowering methods on the prognosis of hypertriglyceridemic acute pancreatitis: a single-center 12-year retrospective study by propensity score matching. Scand J Gastroenterol. 2024;59(7):843–851. doi:10.1080/00365521.2024.2342406
33. Wang L, Ren Y, Xu T, Geng J, Yang N, Wang R. Triglycerides: a sensitizer but not a trigger for hypertriglyceridemic acute pancreatitis. Dig Dis Sci. 2024;69(6):2123–2131. doi:10.1007/s10620-024-08412-x
34. Kim SJ, Kang H, Kim EJ, Kim YS, Cho JH. Clinical features and outcomes of hypertriglyceridemia-induced acute pancreatitis: propensity score matching analysis from a prospective acute pancreatitis registry. Pancreatology. 2020;20(4):617–621. doi:10.1016/j.pan.2020.03.013
35. Hao Y, Feng J, He W, Wu Y, Ma Y, Xu H. A clinical and imaging-based model for distinguishing mild from moderately severe/severe hypertriglyceridemic acute pancreatitis: development and validation. J Comput Assist Tomogr. 2026;50(1):81–90. doi:10.1097/RCT.0000000000001791
36. Xinyu X, Jiang Z, Qing A, Lihua L, Xiehong L, Lin Z. Clinical significance of PCT, CRP, IL-6, NLR, and TyG Index in early diagnosis and severity assessment of acute pancreatitis: a retrospective analysis. Sci Rep. 2025;15(1):2924. doi:10.1038/s41598-025-86664-x
37. Khatua B, Yaron JR, El-Kurdi B, Kostenko S, Papachristou GI, Singh VP. Ringer’s lactate prevents early organ failure by providing extracellular calcium. J Clin Med. 2020;9(1):263. doi:10.3390/jcm9010263
38. Carlstedt F, Lind L. Hypocalcemic syndromes. Crit Care Clin. 2001;17(1):
39. Chhabra P, Rana SS, Sharma V, Sharma R, Bhasin DK. Hypocalcemic tetany: a simple bedside marker of poor outcome in acute pancreatitis. Ann Gastroenterol. 2016;29(2):214–220. doi:10.20524/aog.2016.0015
40. Qiu M, Zhou X, Zippi M, et al. Comprehensive review on the pathogenesis of hypertriglyceridaemia-associated acute pancreatitis. Ann Med. 2023;55(2):2265939. doi:10.1080/07853890.2023.2265939
41. Morandotti C, Wikner M, Li Q, et al. Decreased cardio-respiratory information transfer is associated with deterioration and a poor prognosis in critically ill patients with sepsis. J Appl Physiol. 2025;138(1):289–300. doi:10.1152/japplphysiol.00642.2024
42. Bai B, Xiang W, Chen X, et al. Oleic acid promotes lung injury in hypertriglyceridaemia-associated acute pancreatitis via the PIEZO1/NR4A1/CPT1A axis impairing endothelial fatty acid oxidation. Gut. 2026. doi:10.1136/gutjnl-2025-336441
43. Lagrange J, Didelot M, Mohamadi A, et al. Implication of free fatty acids in thrombin generation and fibrinolysis in vascular inflammation in zucker rats and evolution with aging. Front Physiol. 2017;8:949. doi:10.3389/fphys.2017.00949
44. Gui M, Zhao B, Huang J, Chen E, Qu H, Mao E. Pathogenesis and therapy of coagulation disorders in severe acute pancreatitis. J Inflamm Res. 2023;16:57–67. doi:10.2147/JIR.S388216
45. Nassar TI, Qunibi WY. AKI associated with acute pancreatitis. Clin J Am Soc Nephrol. 2019;14(7):1106–1115. doi:10.2215/CJN.13191118
46. Siddiqui SS. Serum cystatin C in early identification of acute kidney injury in acute pancreatitis: is it an old wine in a new bottle? Indian J Crit Care Med. 2020;24(9):744–745. doi:10.5005/jp-journals-10071-23579
47. Luiken I, Eisenmann S, Garbe J, et al. Pleuropulmonary pathologies in the early phase of acute pancreatitis correlate with disease severity. PLoS One. 2022;17(2):e0263739. doi:10.1371/journal.pone.0263739
48. Sánchez-Maure M, Rendón-Ramírez EJ, Jáquez Quintana JO, et al. Association of pleural effusion on thoracic ultrasound with severe acute pancreatitis and mortality. BMC Gastroenterol. 2025;25(1):730. doi:10.1186/s12876-025-04343-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
CT Characteristics of Acute Pancreatitis with Preexisting Fatty Liver and Its Impact on Pancreatitis Severity and Persistent Systemic Inflammatory Response Syndrome
Liu W, Li Z, Zhang X, Du J, Liang R, Ji Y, Tang W, Zhang X
International Journal of General Medicine 2022, 15:7017-7028
Published Date: 5 September 2022
Association Between the Systemic Inflammation Response Index and Severity of Acute Pancreatitis: A Retrospective Cohort Study
Wu W, Zhang Y, Zhang Y, Qu X, Zhang Z, Zhang R
Journal of Inflammation Research 2025, 18:4471-4480
Published Date: 27 March 2025
Nucleotide-Bound Oligomeric Domain-Like Receptor Protein 3 as a Serological Biomarker in Relation to Disease Severity and Delirium After Acute Pancreatitis: A Two-Center Prospective Cohort Study
Tang Z, Zhou X, Rao Y, Wu J
International Journal of General Medicine 2025, 18:3423-3440
Published Date: 26 June 2025
The Predictive Value of Liver/Spleen CT Value, BISAP Score Combined with Serum sPD-L1 for Hyperlipidemic Acute Pancreatitis
Liu T, Peng L, Huo Y, Lu T, Lv X
International Journal of General Medicine 2025, 18:6245-6254
Published Date: 15 October 2025
Utilizing MRI Radiomics and Clinical Features to Predict Severe Acute Pancreatitis in Patients with Metabolic Syndrome
Wang Y, Wan X, Zhang Y, Liu Z, Liu Z, Tang M, Huang X
Journal of Inflammation Research 2025, 18:15959-15971
Published Date: 15 November 2025