Back to Journals » International Journal of General Medicine » Volume 19
Development and Validation of a Nomogram to Predict Multidrug-Resistant Organism Infection in Severe Pneumonia: A Retrospective Cohort Study
Received 17 October 2025
Accepted for publication 28 January 2026
Published 6 February 2026 Volume 2026:19 575149
DOI https://doi.org/10.2147/IJGM.S575149
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Wei Zhang, Jianlong Zhu
Department of Intensive Care Medicine, Ganzhou People’s Hospital, Ganzhou, 341000, People’s Republic of China
Correspondence: Jianlong Zhu, Department of Intensive Care Medicine, Ganzhou People’s Hospital, No. 16 Meiguan Avenue, Zhanggong District, Ganzhou, Jiangxi, 341000, People’s Republic of China, Tel +8615216136394, Email [email protected]
Objective: The purpose of this study was to explore the etiological characteristics of multidrug-resistant bacteria (MDRO) infection in patients with severe pneumonia (SP) and to construct a nomogram model based on their risk factors.
Methods: A total of 214 severe pneumonia (SP) patients admitted from November 2022 to January 2024 were retrospectively assigned to the modeling group, and 92 patients admitted from February 2024 to March 2025 formed the validation group. Patients were categorized into MDRO and non-MDRO groups based on multidrug-resistant organism infection status. The distribution of pathogens in the MDRO group was analyzed. Logistic regression was performed to analyze the influencing factors. R software was performed to construct nomogram models. Decision curve analysis(DCA) was performed to evaluate the clinical application value of nomogram models.
Results: A total of 93 strains of pathogenic bacteria were isolated from 72 MDRO-infected patients. Gram-negative bacteria showed the highest resistance to piperacillin-tazobactam and piperacillin, while Gram-positive bacteria exhibited a high resistance rate to penicillin.Logistic analysis showed types of pneumonia, chronic obstructive pulmonary disease(COPD), invasive examination,intensive care unit(ICU) admission, antimicrobial drug combination, use of carbapenems, and hypoalbuminemia were risk factors (P< 0.05). The modeling group achieved an area under curve(AUC) of 0.910, with the Hosmer–Lemeshow (H-L) test showing χ2 = 7.423. DCA indicated that the nomogram model had high clinical utility for predicted probabilities between 0.07 and 0.94. In the validation group, the AUC was 0.953, with H-L test χ2 = 7.032. DCA showed that the nomogram model had high clinical value for predicted probabilities between 0.07 and 0.89.
Conclusion: The types of pneumonia, COPD, invasive examination, ICU admission, combination of antimicrobial drugs, carbapenems use, and hypoalbuminemia are influencing factors for MDRO infection in SP patients. The nomogram constructed based on this can better evaluate the risk of MDRO infection.
Keywords: severe pneumonia, multidrug resistant organism, risk factors, nomogram
Introduction
Pneumonia is an inflammatory response in the lungs caused by multiple factors, including pathogen-induced infection, impaired immune system, and medication. While ordinary pneumonia can achieve a good therapeutic effect after anti-inflammatory treatment. Severe pneumonia (SP) is a relatively special type of pneumonia mostly caused by pathogenic bacteria infection, which reduces pulmonary ventilation function and thus induces respiratory failure or even multiple organ dysfunction, posing a serious threat to patients’ lives.1,2 Currently, clinical treatment of SP with antibacterial drugs can control the disease and effectively improve patient prognosis. However, during hospitalization, the irrational use of antibiotics may lead to the body’s automatic selection of multiple drug-resistant organisms (MDRO), forming MDRO colonization and infection. In addition, most of these patients are elderly with low immunity and weak resistance to infection, making them prone to MDRO infection.3,4 Worldwide, the incidence of multidrug-resistant organism (MDRO) infections in ICU patients is significantly higher than in general wards, with severe pneumonia being one of the main reservoirs for MDROs. During infection, bacteria can breach the host defense barriers, invade tissues or the bloodstream, and trigger local inflammation or systemic infection, requiring comprehensive assessment through pathogen detection combined with clinical symptoms. The pathogenesis of MDROs remains unclear; some studies suggest that it may be related to bacterial genetic mutations and the acquisition of exogenous resistance genes, leading to resistance to multiple antimicrobial agents. Moreover, resistance genes can be horizontally transmitted between bacteria via plasmids and other mechanisms, thereby exacerbating the spread of MDROs.5 Once MDRO appears in SP patients, it can aggravate the condition, prolong hospital stays, and increase treatment difficulties, thereby affecting patient prognosis.6 Therefore, it is crucial to analyze the distribution and drug resistance of pathogens causing MDRO infection in SP patients and to identify as early as possible the factors influencing MDRO infection so as to improve patient outcomes.
Nomograms can quantify the screened results, integrate the total risk scores of hazardous factors, and calculate the corresponding probability, thereby identifying high-risk groups in the predictive model and assessing the risk of this event. Compared with traditional risk scores such as APACHE II and SOFA, nomograms have obvious advantages, mainly including higher predictive accuracy, greater clinical applicability, and higher degree of individualization: traditional risk scores are mostly population-level risk assessments, whereas nomograms can provide personalized risk predictions based on the characteristics of individual patients, facilitating the development of individualized intervention strategies. Nomograms can also evaluate stability through internal validation (modeling cohort) and external validation (validation cohort), and quantify predictive performance using calibration curves, ROC curves, and other indicators, making them more scientific than the subjective assessments of traditional scores.7,8 A study found that constructing a nomogram risk prediction model for MDRO infections in the neonatal intensive care unit (NICU) demonstrated good goodness-of-fit and calibration. This model can be used in the NICU to develop targeted prevention and control strategies for each individual risk factor (including low birth weight, maternal age, antibiotic use for more than 7 days, and MDRO colonization).9 Based on this, there are few reports on MDRO infection in SP patients using nomograms. Hence, this study aims to investigate the etiology and identify the risk factors associated with MDRO infections in patients with SP, and to construct a nomogram-based predictive model.
Data and Methods
General Data
A total of 214 patients with severe pneumonia (SP) admitted to our hospital from November 2022 to January 2024 were retrospectively included as the training cohort, and 92 patients admitted from February 2024 to March 2025 were included as the validation group. Patients were classified into MDRO and non-MDRO groups based on multidrug-resistant organism infection status. The flowchart of case selection is shown in Figure 1. Inclusion criteria: (1) meeting the standards for SP,10 and confirmed by clinical manifestations and imaging, with all included cases being infectious pneumonia; (2) age ≥18 years; (3) first-time treatment; (4) positive sputum culture; (5) complete clinical data. Exclusion criteria: (1) other infectious diseases (infectious diseases of the digestive, urinary, and other systems); (2) malignant tumors; (3) other lung diseases (tuberculosis, asthma); (4) major organ dysfunction; (5) pregnant or lactating women; (5) psychiatric disorders; (6) non-infectious pneumonia; (7) immune dysfunction. This study was approved by the Ethics Committee of Ganzhou People’s Hospital.
 |
Figure 1 Case flow collection diagram. |
Methods
MDRO Determination Criteria
A fully automated microbial analysis system (VITEK 2 Compact, bioMérieux, France) and a drug susceptibility analysis system were used to detect pathogens. When the bacteria cultured from a specimen exhibit resistance to three or more types of antimicrobial drugs simultaneously, and if the same strain is continuously cultured for three times to be MDRO-positive, it is determined to be MDRO.11
Pathogen Detection and Drug Susceptibility Testing
Early-morning sputum samples were collected after cleaning the oral cavity with normal saline. The strains were cultured, and the pathogens were detected using a fully automated microbial analyzer. Drug susceptibility testing was performed on the isolated strains using a drug susceptibility instrument and drug susceptibility cards (ATB Fungus2 susceptibility card).Quality control strains (Klebsiella pneumoniae ATCC 700603, Pseudomonas aeruginosa ATCC 27853, and Staphylococcus aureus ATCC 29213) were used simultaneously for culture quality control; antimicrobial susceptibility testing was performed using an automated microbial analysis system (VITEK 2 Compact, bioMérieux, France), and the identification of MDROs in this study was strictly conducted according to the definition of multidrug resistance in the corresponding standard.12
Clinical Data Collection
Clinical data were collected from the electronic medical record system (all personnel responsible for data collection had undergone professional training; the study data were entered independently by two individuals into the database, and cross-checked after entry to correct any errors and ensure accuracy). Main variables included age, sex, BMI, length of hospital stay, duration of fever, duration of antibiotic use, diabetes, hypertension, hyperlipidemia,coronary heart disease (CHD),smoking history, alcohol use, pneumonia type (community-acquired pneumonia [CAP]:It is an infectious parenchymal inflammation of the lungs acquired outside the hospital, hospital-acquired pneumonia [HAP]:It refers to pneumonia that was neither present nor incubating at the time of hospital admission but developed 48 hours or more after hospitalization), chronic obstructive pulmonary disease (COPD), invasive procedures, indwelling urinary catheter, admission to ICU, combination antibiotic therapy, use of carbapenems antibiotics, disturbance of consciousness, hypoproteinemia,deep venous catheterization,GCS score, coma, body temperature, endotracheal intubation, central venous catheter, mechanical ventilation time, white blood cell count (WBC), platelet count (PLT), fasting blood glucose (FBG), triglycerides (TG), total cholesterol (TC), hemoglobin (Hb), and APACHE II score. Variables with a missing rate exceeding 5% were excluded to ensure the reliability and rigor of the results.
Statistical Analysis
Data were analyzed using SPSS 25.0. Count data were tested by χ2-test and expressed as cases (%). Measurement data that met normality according to the Shapiro–Wilk test were tested by t test and expressed as ( ).For non-normally distributed data, values were expressed as median (quartiles) [M (Q1, Q3)], and comparisons between groups were performed using the nonparametric Mann–Whitney U-test.Logistic regression analysis was used to identify risk factors for MDRO infection in SP patients (forward stepwise method with entry criteria of 0.05 and removal criteria of 0.1). A nomogram prediction model was constructed using R software (R version 4.5.1 and the rms package). The discrimination and calibration of the nomogram were evaluated by ROC curves and calibration plots, respectively. Internal validation was performed using the bootstrap method. Decision curve analysis (DCA) was conducted to assess the clinical utility of the model. A P-value <0.05 was considered statistically significant.
).For non-normally distributed data, values were expressed as median (quartiles) [M (Q1, Q3)], and comparisons between groups were performed using the nonparametric Mann–Whitney U-test.Logistic regression analysis was used to identify risk factors for MDRO infection in SP patients (forward stepwise method with entry criteria of 0.05 and removal criteria of 0.1). A nomogram prediction model was constructed using R software (R version 4.5.1 and the rms package). The discrimination and calibration of the nomogram were evaluated by ROC curves and calibration plots, respectively. Internal validation was performed using the bootstrap method. Decision curve analysis (DCA) was conducted to assess the clinical utility of the model. A P-value <0.05 was considered statistically significant.
Results
Distribution and Composition of Pathogens in MDRO Infected Patients
A total of 72 patients yielded 93 strains of pathogens. Among these, 53 strains (56.99%) were Gram-negative bacteria, primarily Acinetobacter baumannii (23 strains,24.73%) and Klebsiella pneumoniae (14 strains, 15.05%); 36 strains (38.71%) were Gram-positive bacteria, mainly Staphylococcus aureus (17 strains,18.28%) and Staphylococcus epidermidis (13 strains, 13.98%); and 4 strains (4.30%) were fungi, Candida spp. See Table 1.
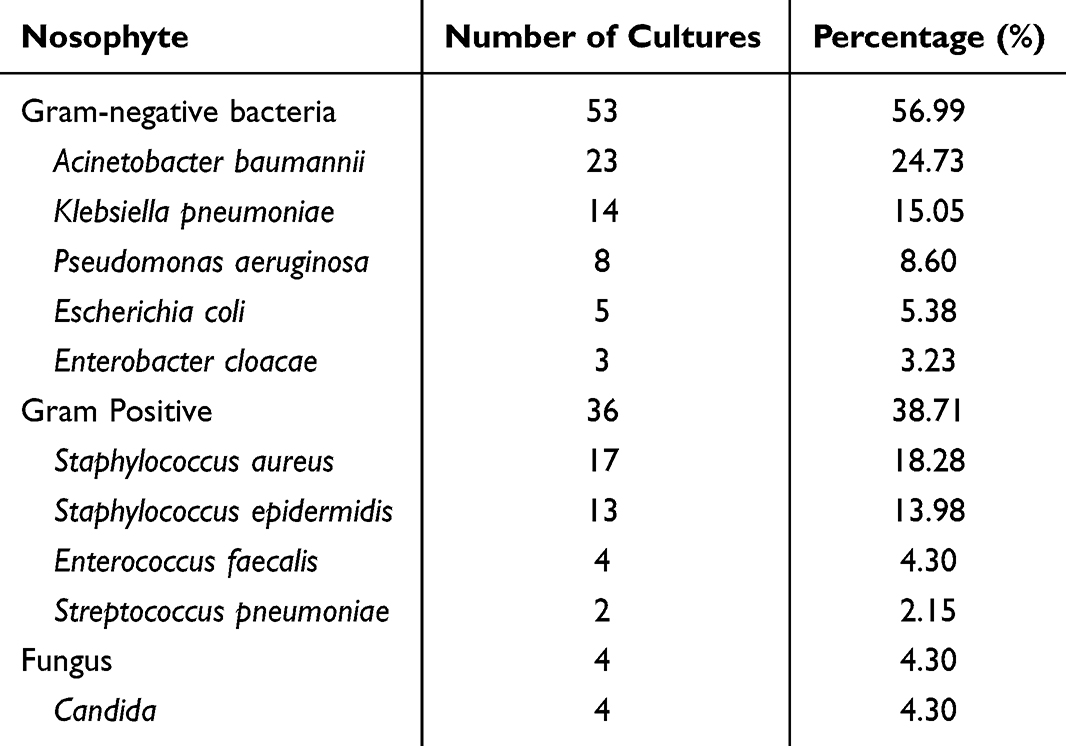 |
Table 1 Distribution and Composition of Pathogenic Bacteria in MDRO Infected Patients |
Analysis of Drug Resistance of Gram-Negative Bacteria
Gram-negative bacteria showed the highest resistance to piperacillin-tazobactam and piperacillin, both at 100%, but was more sensitive to cefiderocol and colistin. See Table 2.
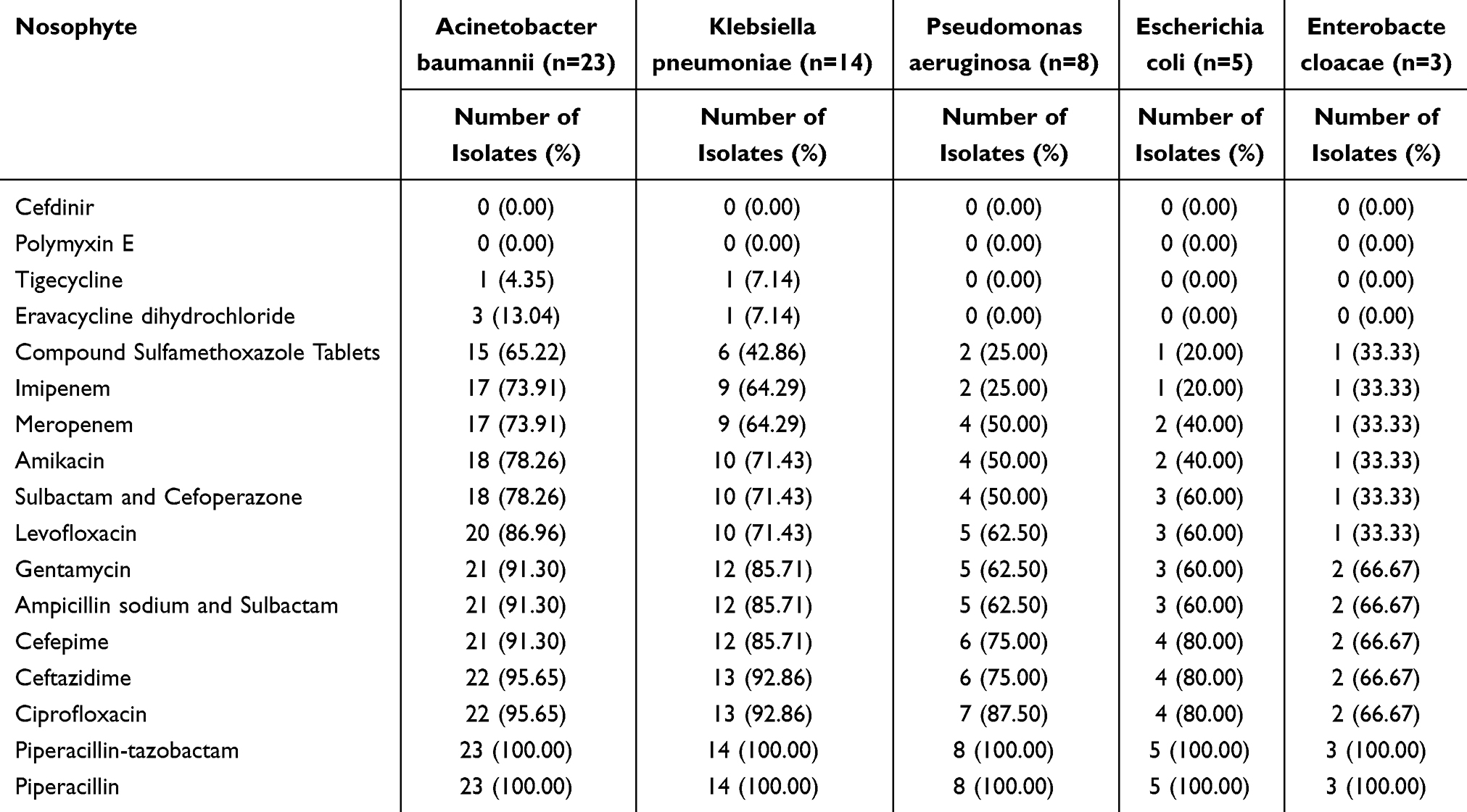 |
Table 2 Analysis of Drug Resistance in Gram-Negative Bacteria |
Analysis of Drug Resistance of Gram-Positive Bacteria
Gram-positive bacteria had a relatively high resistance rate (82.35%) to penicillin but was more sensitive to oxacillin, norvancomycin, vancomycin, fosfomycin, rifampin, teicoplanin, and tigecycline. See Table 3.
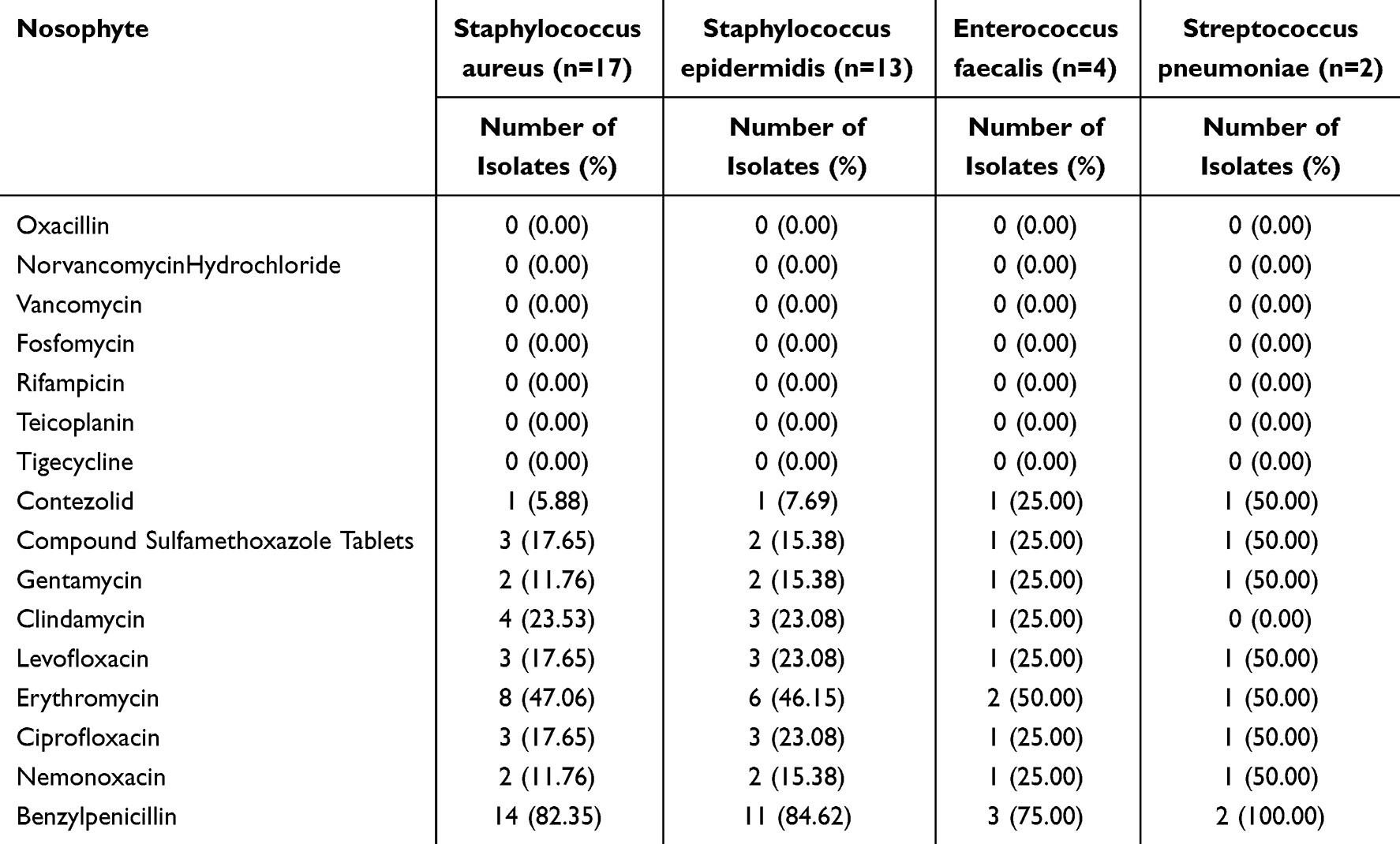 |
Table 3 Analysis of Drug Resistance in Gram-Positive Bacteria |
Comparison of Clinical Data Between the MDRO and Non-MDRO Groups in the Modeling Group
Among the 214 patients, 72 developed MDRO infection, with an incidence rate of 33.64%. There were significant differences in pneumonia type, COPD, invasive procedures, ICU admission, combination antibiotic therapy, use of carbapenems antibiotics, and hypoproteinemia between the MDRO Group and Non-MDRO Groups (P<0.05). There were no significant differences in other clinical data (P>0.05). See Table 4.
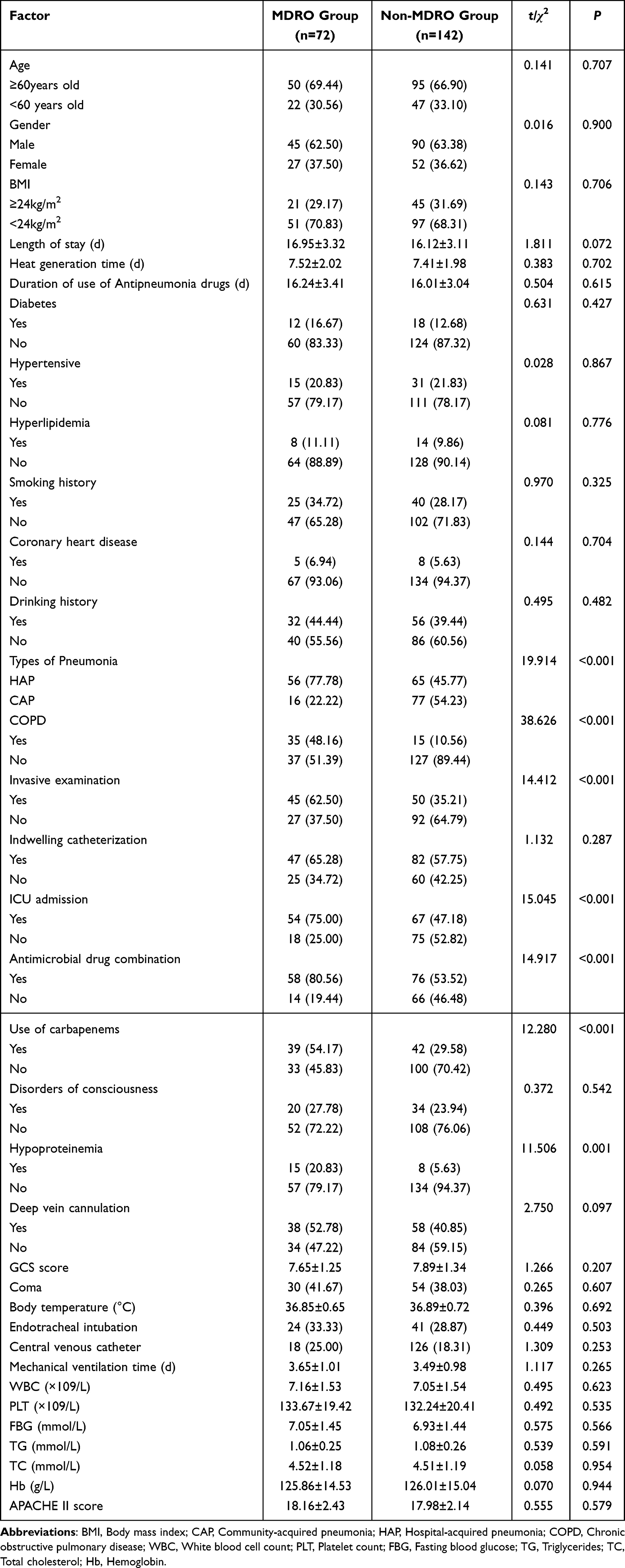 |
Table 4 Comparison of Clinical Data Between MDRO and Non-MDRO Groups in the Modeling Group |
Multifactor Analysis of Influencing Factors for MDRO Infection in SP Patients
The dependent variable was defined as follows: occurrence of MDRO infection in SP patients = 1, otherwise = 0. The assignments for the independent variables are shown in Table 5. After multicollinearity testing, the variance inflation factor (VIF) was less than 10, indicating no multicollinearity. Logistic regression analysis showed that pneumonia type, COPD, invasive procedures, ICU admission, combination antibiotic therapy, use of carbapenems antibiotics, and hypoproteinemia were risk factors for MDRO infection in SP patients (P<0.05). See Table 6.
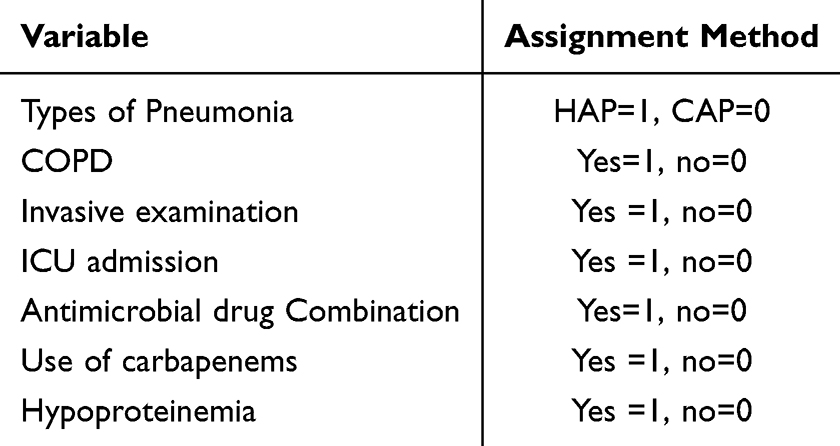 |
Table 5 Assignment methods of Argument Variables |
 |
Table 6 Multifactorial Analysis of Factors Influencing MDRO Infection in SP Patients |
Construction of a Nomogram Model for MDRO Infection in SP Patients
The nomogram model was constructed as follows: P=ex/(1+ex), x = −4.268+2.026 × pneumonia type + 1.529 × COPD + 1.111 × invasive procedures +1.513 × ICU admission + 1.061 × combination antibiotic therapy + 1.147 × use of carbapenems + 1.133 × hypoproteinemia. For example, for a patient with CAP (0 points), COPD (76.5 points), invasive procedures (56.5 points), ICU admission (75.0 points), no combination antibiotic therapy (0 points), use of carbapenems (57.5 points), and hypoproteinemia (21.5 points), the total score would be 287.0 points. Drawing a vertical line from the total score indicates that the predicted probability is 81%. See Figure 2.
 |
Figure 2 The nomogram model for MDRO infection in SP patients. Abbreviations: CAP, Community-acquired pneumonia; HAP, Hospital-acquired pneumonia; COPD, Chronic obstructive pulmonary disease. |
Internal Validation of the Nomogram Model for MDRO Infection in SP Patients
The ROC curve was plotted, with an internal validation AUC of 0.910 (95% CI = 0.65–0.955) in the modeling group, as shown in Figure 3A. The Hosmer-Lemeshow test yielded χ2 = 7.423 (P = 0.751), as shown in Figure 3B.
 |
Figure 3 Internal validation of the nomogram model for MDRO infection in SP patients (A) ROC curve of modeling group; (B) Calibration curve of modeling group. |
Decision Curve Analysis of the Nomogram Model
Decision curve analysis (DCA) showed that the nomogram model had a positive net benefit and good clinical utility when the predicted probability was between 0.07 and 0.94,as shown in Figure 4.
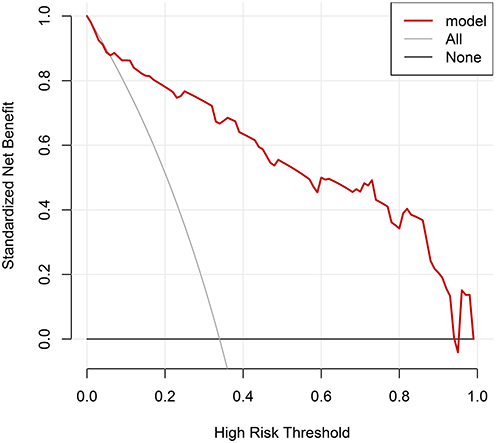 |
Figure 4 DCA curve for the nomogram. |
Comparison of Clinical Data Between MDRO and Non-MDRO Groups in the Validation Group
Significant differences were observed between the MDRO and non-MDRO groups in terms of pneumonia type, COPD, invasive procedures, ICU admission, combination antibiotic therapy, carbapenems use, and hypoproteinemia (P < 0.05). No significant differences were found in other clinical data (P > 0.05). See Table 7.
 |
Table 7 Comparison of Clinical Data Between MDRO and Non-MDRO Groups in the Validation Group |
External Validation of the Nomogram Model for MDRO Infection in SP Patients
The ROC curve was plotted, with an external validation AUC of 0.953 (95% CI = 0.914–0.992) in the validation group, as shown in Figure 5A. The Hosmer-Lemeshow test yielded χ2 = 7.032 (P = 0.741), as shown in Figure 5B.
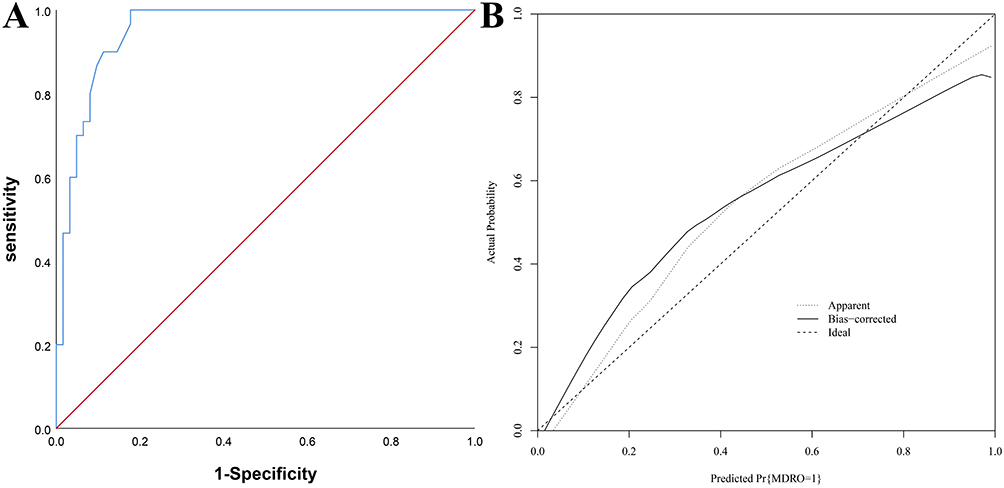 |
Figure 5 External validation of the nomogram model for MDRO infection in SP patients (A) ROC curve of validation group; (B): Calibration curve of modeling group. |
External Validation of the Nomogram Model by Decision Curve Analysis
As shown in the DCA curve, when the probability ranged from 0.07 to 0.89, the nomogram model had a positive net benefit and good clinical utility in evaluating MDRO infection in SP patients. See Figure 6.
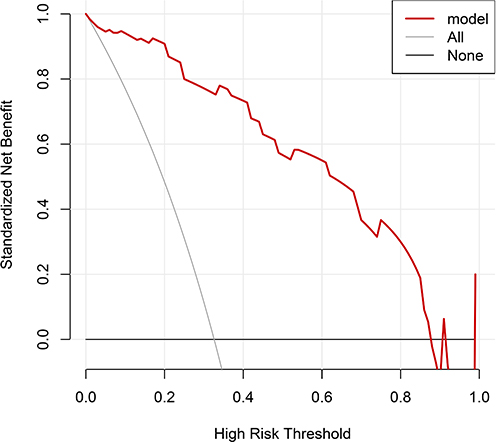 |
Figure 6 External validation of the nomogram model by DCA. |
Discussion
SP progresses relatively rapidly. During disease progression, patients may develop complications such as respiratory failure and disturbance of consciousness. Moreover, when SP patients develop MDRO infection, it exacerbates the disease and increases the difficulty of treatment. The reasons for MDRO infection in SP patients are relatively complex and may be influenced by disease status, antibacterial drugs, and other factors.13,14 This study found that among 306 patients, 101 developed MDRO (33.01%), and among the 214 patients in the modeling group, 72 developed MDRO (33.64%), indicating a relatively high infection rate. The pathogens isolated from MDRO infected patients were mainly Gram-negative bacteria, with Acinetobacter baumannii accounting for the highest proportion. This may be because it is an opportunistic pathogen that is widely distributed in hospitals, can resist ultraviolet radiation, and is therefore difficult to eradicate.15 Through analyzing the drug resistance of the main Gram-negative and Gram-positive bacteria, it was found that Gram-negative bacteria had the highest resistance to piperacillin-tazobactam and piperacillin, while being more sensitive to cefiderocol and colistin, indicating relatively good sensitivity to cefiderocol and colistin, which can be prioritized for clinical treatment.Gram-positive bacteria showed a high resistance rate to penicillin but was more sensitive to oxacillin, norvancomycin, vancomycin, fosfomycin, rifampin, teicoplanin, and tigecycline. Therefore, penicillin should be avoided as much as possible in these patients.16
This study identified seven factors influencing MDRO infection in SP patients, and the reasons are as follows: (1) Studies have shown that among different types of pneumonia, hospital-acquired pneumonia (HAP) is more prone to infection. Patients often develop pulmonary parenchymal inflammation and mixed infections after 48 hours of hospitalization, placing them at a higher risk of infection with MDRO.17 This finding is consistent with the results of the present study. The reason may be that pathogens are more densely distributed in the hospital environment. Patients who are hospitalized for prolonged periods may experience reduced immune function due to steroid use, invasive procedures, etc., thereby increasing the risk of MDRO infection.18 (2) Among SP patients with COPD, there may be other underlying conditions, and they tend to experience repeated infections, requiring multiple types of medication, thus increasing the infection risk.19 Furthermore, patients with acute exacerbations of COPD often need endotracheal intubation, which affects the ciliary function of the respiratory tract, damages the airways, and may increase the risk of infection,20 which is similar to the results of this study. Therefore, for such patients, it is advisable to make a comprehensive assessment of pathogen drug resistance, choose appropriate antimicrobial agents, and use steroids judiciously to reduce the risk of infection. (3) This study found that invasive procedures are a factor influencing MDRO infection in patients with SP. Because,SP patients undergoing invasive procedures face varying degrees of risk and potential injury to the body, which compromises the integrity and defense functions of the body, allowing pathogens to invade, increasing the burden on the body, and thereby raising the risk of infection.21 (4) The ICU is also a high-risk area for MDRO. When patients are admitted to the ICU for surgery and medication, the risk of MDRO infection increases. Thus, it is necessary to emphasize disinfection among healthcare professionals, isolate and manage patients with MDRO, and strengthen the supervision of antimicrobial drug use to minimize MDRO transmission.22 Similar to the findings of this study. (5) Although combination antibiotic therapy can alleviate infection to some extent and inhibit pathogen proliferation, it can also promote the abnormal growth of multidrug-resistant bacteria, increasing drug tolerance. Moreover, the expanded use of antibacterial agents can amplify the suppression of non-pathogenic flora, affect the structure of the oropharyngeal microbiota, facilitate pathogen colonization, and elevate the risk of infection.23 (6) Carbapenems are broad-spectrum antibiotics with strong antibacterial activity; however, they can alter the body’s microbiological ecology and cause an imbalance in the flora. Under pharmacological pressure, this may increase the risk of resistant strains and thereby raise the risk of MDRO infection.11 Therefore, carbapenems can be used initially for SP infection, followed later by rational drug selection based on pathogen detection results to reduce the risk of infection. (7) Albumin, synthesized by hepatocytes, plays a crucial role in maintaining plasma osmotic pressure and nutritional functions. A decrease in albumin levels indicates hepatic dysfunction and compromised immunity.In patients with hypoproteinemia, immune function is diminished, leaving them unable to resist external pathogens, thus increasing the risk of pathogen invasion.24,25
Based on the results of Logistic analysis, this study constructed a nomogram model that can help medical staff intuitively understand the various risk factors. The nomogram constructed in this study yielded AUC values of 0.910 and 0.953 for the two groups, and the H-L test indicated a good fit, suggesting strong predictive ability. When the DCA curve probability ranged from 0.07 to 0.94 and 0.07 to 0.89, the nomogram model for assessing MDRO infection in SP patients showed high clinical applicability, which can help clinicians select high-risk groups based on identified influencing factors and carry out targeted interventions,effectively improving patients’ quality of life.
Conclusions
In summary, pneumonia type, COPD, invasive procedures, ICU admission, combination antibiotic therapy, carbapenems use, and hypoproteinemia are factors influencing MDRO infection in SP patients. The nomogram based on these factors can effectively evaluate the risk of MDRO infection, with good discrimination and clinical applicability. However, there are limitations to this study as it is retrospective, single-center in design, and has a small sample size, possibly introducing bias into the findings,and did not further address potential confounding effects of disease severity and treatment indications. Further verification through multi-center prospective studies with expanded sample sizes is warranted.
Research Involving Human Participants
The study was approved by the Ethics Committee of Ganzhou People’s Hospital (No.GZSRMYY2025010018) and with the 1964 Helsinki Declaration. Written informed consent to participate in this study was provided by the participants.
Data Sharing Statement
The datasets in this study are available from the corresponding author.
Consent for Publication
All authors give consent for publication.
Disclosure
The authors declared no conflicts of interest in this work.
References
1. Eckerle M, Mvalo T, Smith AG, et al. Identifying modifiable risk factors for mortality in children aged 1-59 months admitted with WHO-defined severe pneumonia: a single-centre observational cohort study from rural Malawi. BMJ Paediatr Open. 2022;6(1):e001330. doi:10.1136/bmjpo-2021-001330
2. He L, He A, Qian Y. Imipenem-resistant Pseudomonas aeruginosa treated with piperacillin/tazobactam in a patient with severe pneumonia: a case report and related literature review. Ann Palliat Med. 2021;10(1):810–15. doi:10.21037/apm-20-2495
3. Prendki V, Garin N, Stirnemann J, et al. LOw-dose CT Or Lung UltraSonography versus standard of care based-strategies for the diagnosis of pneumonia in the elderly: protocol for a multicentre randomised controlled trial (OCTOPLUS). BMJ Open. 2022;12(5):e055869. doi:10.1136/bmjopen-2021-055869
4. Sfeir MM. Diagnosis of multidrug-resistant pathogens of pneumonia. Diagnostics. 2021;11(12):2287. doi:10.3390/diagnostics11122287
5. Ling L, Wong W-T, Lipman J, et al. A narrative review on the approach to antimicrobial use in ventilated patients with multidrug resistant organisms in respiratory samples-to treat or not to treat? that is the question. Antibiotics. 2022;11(4):452. doi:10.3390/antibiotics11040452
6. Niu B-Y, Wang G, LI B, et al. Sequential treatment of severe pneumonia with respiratory failure and its influence on respiratory mechanical parameters and hemodynamics. World J Clin Cases. 2022;10(21):7314–7323. doi:10.12998/wjcc.v10.i21.7314
7. Zhang J, Xu C, Yan S, et al. A nomogram for predicting severe adenovirus pneumonia in children. Front Pediatr. 2023;11:1122589. doi:10.3389/fped.2023.1122589
8. Xu C-B, Su -S-S, Yu J, et al. Risk factors and predicting nomogram for the clinical deterioration of non-severe community-acquired pneumonia. BMC Pulm Med. 2024;24(1):57. doi:10.1186/s12890-023-02813-w
9. Zhou J, Luo F, Liang J, et al. Construction and validation of a predictive risk model for nosocomial infections with MDRO in NICUs: a multicenter observational study. Front Med. 2023;10:1193935. doi:10.3389/fmed.2023.1193935
10. Wang S, Tang J, Tan Y, et al. Prevalence of atypical pathogens in patients with severe pneumonia: a systematic review and meta-analysis. BMJ Open. 2023;13(4):e066721. doi:10.1136/bmjopen-2022-066721
11. Paul M, Carrara E, Retamar P, et al. European society of clinical microbiology and infectious diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European society of intensive care medicine. Clin Microbiol Infect. 2022;28(4):521–547. doi:10.1016/j.cmi.2021.11.025
12. Cillóniz C, Torres A, Niederman MS. Management of pneumonia in critically ill patients. BMJ. 2021;375:e065871. doi:10.1136/bmj-2021-065871
13. Sharma A, Rodriguez-Morales AJ, Traore T, et al. Globalisation of antibiotic-resistant bacteria at recurring mass gathering events. Lancet. 2023;402(10398):e5–e7. doi:10.1016/S0140-6736(22)01995-X
14. Fursova NK, Astashkin EI, Ershova ON, et al. Multidrug-resistant klebsiella pneumoniae causing severe infections in the neuro-ICU. Antibiotics. 2021;10(8):979. doi:10.3390/antibiotics10080979
15. Kim C-J, Song K-H, Choi N-K, et al. Socioeconomic burden of pneumonia due to multidrug-resistant Acinetobacter baumannii and Pseudomonas aeruginosa in Korea. Sci Rep. 2022;12(1):13934. doi:10.1038/s41598-022-18189-6
16. Yoneda A, Thänert R, Burnham C-A, et al. In vitro activity of meropenem/piperacillin/tazobactam triple combination therapy against clinical isolates of Staphylococcus aureus, Staphylococcus epidermidis, Staphylococcus pseudintermedius and vancomycin-resistant Enterococcus spp. Int J Antimicrob Agents. 2020;55(2):105864. doi:10.1016/j.ijantimicag.2019.105864
17. Yang L, lu G, Diao H, et al. Predicting infections with multidrug-resistant organisms (MDROs) in neurocritical care patients with hospital-acquired pneumonia (HAP): development of a novel multivariate prediction model. Microbiol Spectr. 2025;13(6):e0246024. doi:10.1128/spectrum.02460-24
18. Fois M, Vito DE, Cherchi A, et al. Efficacy and safety of ceftazidime-avibactam alone versus ceftazidime-avibactam plus fosfomycin for the treatment of hospital-acquired pneumonia and ventilator-associated pneumonia: a multicentric retrospective study from the SUSANA Cohort. Antibiotics. 2024;13(7):616. doi:10.3390/antibiotics13070616
19. Uluç K, Özçelik KUTBAY, Akkütük Öngel E, et al. The prevalence of multidrug-resistant and extensively drug-resistant infections in respiratory intensive care unit, causative microorganisms and mortality. Infect Drug Resist. 2024;17:4913–4919. doi:10.2147/IDR.S480829
20. IDIGO AJ, Wells JM, ML B, et al. Clinical risk factors for admission with Pseudomonas and multidrug-resistant Pseudomonas community-acquired pneumonia. Antimicrob Resist Infect Control. 2022;11(1):95. doi:10.1186/s13756-022-01137-4
21. Mandoli GE, De Carli G, Pastore MC, et al. Right cardiac involvement in lung diseases: a multimodality approach from diagnosis to prognostication. J Intern Med. 2021;289(4):440–449. doi:10.1111/joim.13179
22. Viasus D, Gudiol C, Carratalà J. Treatment of multidrug-resistant Gram-negative bloodstream infections in critically ill patients: an update. Curr Opin Crit Care. 2024;30(5):448–455. doi:10.1097/MCC.0000000000001190
23. Karakonstantis S, Kritsotakis EI, Gikas A. Treatment options for K. pneumoniae, P. aeruginosa and A. baumannii co-resistant to carbapenems, aminoglycosides, polymyxins and tigecycline: an approach based on the mechanisms of resistance to carbapenems. Infection. 2020;48(6):835–851. doi:10.1007/s15010-020-01520-6
24. Jiang A-M, N L, Said ALI, et al. nosocomial infections in gastrointestinal cancer patients: bacterial profile, antibiotic resistance pattern, and prognostic factors. Cancer Manag Res. 2020;12:4969–4979. doi:10.2147/CMAR.S258774
25. Ao H, Song H, Li J. A nomogram for predicting the effectiveness of consultations on multi-drug resistant infections: an exploration for clinical pharmacy services. Infect Drug Resist. 2024;17:3439–3450. doi:10.2147/IDR.S470883
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Model That Predicts the Risk of Diabetic Nephropathy in Type 2 Diabetes Mellitus Patients: A Cross-Sectional Study
Yang J, Jiang S
International Journal of General Medicine 2022, 15:5089-5101
Published Date: 20 May 2022
Development of Risk Prediction Model for Muscular Calf Vein Thrombosis with Acute Exacerbation of Chronic Obstructive Pulmonary Disease
Hu X, Li X, Xu H, Zheng W, Wang J, Wang W, Li S, Zhang N, Wang Y, Han K
International Journal of General Medicine 2022, 15:6549-6560
Published Date: 10 August 2022
Paraspinal Muscle Degeneration: A Potential Risk Factor for New Vertebral Compression Fractures After Percutaneous Kyphoplasty
Si F, Yuan S, Zang L, Fan N, Wu Q, Wang T, Wang A
Clinical Interventions in Aging 2022, 17:1237-1248
Published Date: 13 August 2022
Tracking Epidemiological Characteristics and Risk Factors of Multi-Drug Resistant Bacteria in Intensive Care Units
Wu C, Lu J, Ruan L, Yao J
Infection and Drug Resistance 2023, 16:1499-1509
Published Date: 15 March 2023
Construction and Validation of a Novel Nomogram for Predicting the Recurrence of Diffuse Large B Cell Lymphoma Treated with R-CHOP
Gong Y, Yan H, Yang Y, Zhai B, Huang Z, Zhang Z
Pharmacogenomics and Personalized Medicine 2023, 16:291-301
Published Date: 1 April 2023