Back to Journals » International Journal of Women's Health » Volume 18
Development and Validation of a Nomogram Model for Predicting Chorioamnionitis in Patients with Term Premature Rupture of Membranes
Authors Gao H, Gong L, Li Y, Huang W, Zhao J, Ren Z, Huang X, Lu J
Received 16 October 2025
Accepted for publication 12 February 2026
Published 6 March 2026 Volume 2026:18 570474
DOI https://doi.org/10.2147/IJWH.S570474
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Huiqiao Gao, Liyun Gong, Yanfang Li, Wenyang Huang, Jing Zhao, Zhuo Ren, Xin Huang, Junli Lu
Department of Obstetrics and Gynecology, Beijing Chao-Yang Hospital Affiliated to Capital Medical University, Beijing, 100020, People’s Republic of China
Correspondence: Junli Lu, Department of Obstetrics and Gynecology, Beijing Chao-Yang Hospital Affiliated to Capital Medical University, Beijing, 100020, People’s Republic of China, Email [email protected]
Objective: This study aims to construct and validate a nomogram model based on clinical and laboratory indicators to predict the risk of histological chorioamnionitis in patients with premature rupture of membranes at term, and to evaluate its predictive efficacy and effectiveness.
Methods: A total of 319 PROM patients admitted between May 2023 and December 2024 were randomly divided into a modeling group (n=221) and a validation group (n=98) at a 7:3 ratio. Based on placental and fetal membrane histopathology, the modeling group was classified into a non-HCA group (grade 0, n=138) and an HCA group (grades I–II, n=83).
Results: Compared with the non-HCA group, patients in the HCA group had significantly higher rates of body temperature ≥ 37.3 °C, baseline fetal heart rate ≥ 160 beats/min, rupture-to-delivery time ≥ 12 h, cesarean delivery, WBC ≥ 15× 109/L, neutrophil percentage ≥ 75%, and PCT ≥ 0.05 mg/L (all P< 0.05). Multivariate logistic regression identified body temperature ≥ 37.3 °C, cesarean delivery, WBC ≥ 15× 109/L, neutrophil percentage ≥ 75%, and PCT ≥ 0.05 mg/L as independent risk factors for HCA (P< 0.05). The AUC of the nomogram was 0.890 (95% CI: 0.805– 0.913) in the modeling group and 0.885 (95% CI: 0.776– 0.918) in the validation group. Calibration curves and the Hosmer–Lemeshow test demonstrated good model fit (P> 0.05). Decision curve analysis showed that within risk thresholds of 0.1– 0.8 (modeling group) and 0.1– 0.7 (validation group), the nomogram provided greater net clinical benefit than “treat-all” or “treat-none” strategies.
Conclusion: Body temperature, delivery mode, WBC, neutrophil percentage, and PCT are significantly associated with HCA in PROM patients. The nomogram model shows good discrimination, calibration, and stability, and may assist in predicting HCA risk in clinical practice.
Keywords: premature rupture of membranes, histological chorioamnionitis, nomogram, risk factors
Introduction
Premature rupture of membranes (PROM) refers to the spontaneous rupture of the fetal membranes before delivery, and histological chorioamnionitis (HCA) is its main infectious complication, with an incidence rate of up to 40%-70%.1 HCA can not only lead to maternal uterine atony and postpartum hemorrhage, but also significantly increase the risk of adverse outcomes such as neonatal sepsis and respiratory distress syndrome, seriously threatening maternal and fetal safety.2 The relationship between PROM and HCA is relatively complex. It is currently believed that they may be mutually causal. The incidence of prolapsed PROM and PPROM varies considerably across different countries and populations. The overall incidence of PROM is reported to be approximately 5–10% of all pregnancies, while PPROM accounts for about 2–4% in most developed countries. However, the incidence of PPROM is higher in low- and middle-income regions. For example, a recent hospital-based study in Egypt reported a PPROM prevalence of 10.8% among pregnant women, highlighting the heavy disease burden in the region and suggesting that differences in infection prevalence and levels of obstetric care may contribute to this disparity.3 It may be because chorioamnionitis causes defects in the local defense function of the fetal membranes, and factors such as increased amniotic cavity pressure can lead to rupture of the fetal membranes. After the fetal membranes rupture, the retrograde migration of reproductive tract microorganisms leads to the occurrence of HCA.4,5 However, prenatal diagnosis of HCA has obvious limitations: its clinical manifestations (such as fever and fetal heart rate) lack specificity and are easily confused with other obstetric emergencies; the gold standard relies on postpartum placental and fetal membrane pathological examination, which has a lag and is difficult to meet the needs of early intervention. Currently, there is no unified HCA prediction indicator in clinical practice, which leads to missed diagnosis of some high-risk patients and delayed treatment.
The physiological response to intrauterine infection involves complex inflammatory pathways and is manifested through a variety of clinical and laboratory indicators. When pathogens invade the amniotic cavity, they activate the maternal immune system, triggering the release of endogenous pyrogens (interleukin-1 (IL-1), interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α)). These cytokines act on the hypothalamic thermoregulatory center, leading to an increase in body temperature. Simultaneously, the inflammatory cascade stimulates the bone marrow to accelerate the production and release of granulocytes, resulting in an increased white blood cell count (WBC) and neutrophil percentage. Furthermore, procalcitonin (PCT), as a precursor peptide of calcitonin, is significantly upregulated under the stimulation of bacterial endotoxins and pro-inflammatory cytokines, making it a sensitive biomarker for systemic bacterial infection. Understanding these pathophysiological mechanisms provides a theoretical basis for using these indicators to predict HCA at an early stage.6
The nomogram prediction model is a statistical prediction tool that can integrate multiple predictive indicators through multivariate regression analysis, visualize complex prediction models, and intuitively present the risk of related events, thereby improving the convenience of clinical application. It has been widely used in disease identification and prediction.7,8 However, there are few studies on specific prediction models for HCA in patients with PROM, and most existing studies have not incorporated joint analysis of infection markers and obstetric characteristics. Therefore, this study aimed to identify independent risk factors for HCA and construct and validate a personalized nomogram model, hoping to provide a reliable tool for early clinical identification of high-risk patients and the development of precise intervention strategies, thereby reducing the incidence of maternal and fetal infection-related complications.
Materials and Methods
General Information
This study is a single-center retrospective study. During the study, a total of 415 patients with premature rupture of membranes at term were admitted. Random assignment was performed using SPSS 26.0 software to ensure comparability between the two groups in terms of enrollment time, baseline clinical characteristics, and diagnostic and treatment skills. This study was reviewed and approved by Beijing Chao-yang Hospital Affliated to Capital Medical University ethics committee (approval number: 2025-KE-856). Given the retrospective nature of this study, the requirement for informed consent was waived by the ethics committee. All patient data were anonymized and treated with strict confidentiality.
Inclusion criteria: ① Meet the diagnostic criteria for PROM:9 Spontaneous rupture of membranes before delivery, confirmed by vaginal examination, ultrasound examination (amniotic fluid index <5 cm or maximum amniotic fluid dark area <2 cm) and pH test paper test (vaginal secretion pH ≥6.5); ② Gestational age ≥37 weeks; ③ Complete clinical data (including medical history, laboratory tests, delivery records and pathological results, etc).; ④ Singleton pregnancy. Exclusion criteria included: ① patients with severe cardiac, hepatic, or renal dysfunction; ② patients with malignant tumors, immune system disorders, or hematologic diseases; ③ patients with a history of uterine surgery (eg, cesarean section, myomectomy); ④ patients with a confirmed prenatal diagnosis of intrauterine infection (eg, clinical chorioamnionitis) and receiving anti-infective treatment; and ⑤ patients with incomplete data, transfer to another hospital, or loss to follow-up.
After screening, 96 patients were excluded due to pre-defined exclusion criteria, including severe systemic diseases, prenatally diagnosed intrauterine infection, history of uterine surgery, and incomplete clinical or pathological data. Ultimately, 319 patients with complete clinical and pathological data were included in the final analysis. The screening process is shown in Figure 1.
 |
Figure 1 Flowchart. |
Grouping Criteria
All full-term PROM patients meeting the inclusion and exclusion criteria were included in the study. Enrolled patients were randomly assigned to the modeling group (n=221) and the validation group (n=98) in a 7:3 ratio. Patients in the modeling group were further categorized based on histopathological findings to construct the model, while the validation group was specifically used for external validation of the model.
According to the results of postoperative placental and fetal membrane histopathological examination, patients were divided into two groups according to the HCA grading standard:10 non-HCA group (grade 0): placental and fetal membrane histopathological examination showed no inflammatory cell infiltration in the chorion, amnion and decidua, and no evidence of chorioamnionitis. HCA group (grade I + grade II): grade I: a small amount of inflammatory cell infiltration (5–10 inflammatory cells per high-power field) was seen in the chorion, amnion or decidua, and the inflammation was limited to local tissues; grade II: moderate to large amounts of inflammatory cell infiltration (>10 inflammatory cells per high-power field) was seen in the chorion, amnion and decidua, and the inflammation was widespread, and may be accompanied by choriovilli or decidualitis.
All patients included in the study underwent routine placental and fetal membrane specimen collection and histological examination after delivery. All relevant pathological results were fully traceable within the hospital’s pathology information system. Pathological specimens were all placental and fetal membrane tissues routinely collected immediately after delivery, fixed in 10% neutral formaldehyde, and sent to the pathology department for processing; no live samples were involved. The grouping was determined by two experienced pathologists in a double-blind manner. If the judgment results were inconsistent, the third senior pathologist reviewed and determined the final grouping.
Data Collection
Clinical data of all included patients were retrospectively collected through the hospital electronic medical record system and laboratory information system, including:
- General information: age, body mass index, maternal and childbirth history;
- Underlying diseases: hypertension, diabetes, anemia, vaginitis;
- Infection-related indicators: Group B Streptococcus (GBS): vaginal secretion culture results; Body temperature: axillary temperature at admission; Blood routine: WBC, neutrophil percentage; Inflammatory markers: C-reactive protein (CRP), procalcitonin (PCT); WBC with a cutoff value of 15×109/L, which is the clinical critical reference value for intrauterine infection according to the Manual of Standard Diagnosis and Treatment of Gynecological and Obstetric Infectious Diseases.
- Obstetric indicators: Fetal heart rate: baseline fetal heart rate; Amniotic fluid characteristics and volume; Time from rupture of membranes to delivery;
- Delivery mode: Vaginal delivery (VD)/Cesarean section (CS).
To facilitate modeling, continuous clinical indicators were dichotomized based on clinically accepted thresholds or guideline-recommended cutoff values to enhance clinical interpretation and subsequent scoring in predictive models.
Statistical Methods
Data processing and statistical analysis were performed using SPSS 26.0 and R software (version 4.3.0). Univariate analysis was performed on the collected data. Continuous data were expressed as mean ± standard deviation ( ), and intergroup comparisons were performed using the independent sample t-test. Enumeration data were expressed as number of cases (constituent ratio, %), and intergroup comparisons were performed using the chi-square test. Variables with a P < 0.1 in the univariate analysis were included in a multivariate logistic regression analysis using stepwise regression (forward method, α in = 0.05, α out = 0.10) to identify independent risk factors for HCA (P < 0.05). To ensure sufficient statistical power and model stability, we calculated the event-to-variable ratio (EPV) for the multivariate logistic regression analysis. In the modeling group, 83 patients presented with histological chorioamnionitis, and the multivariate model included 7 variables, with an EPV of approximately 11.9. This value exceeds the generally recommended minimum EPV threshold of 10, indicating that the multivariate logistic regression model has sufficient statistical power and is unlikely to overfit. Based on the independent risk factors, a nomogram model was constructed using the “rms” package in R software. The regression coefficients of each factor were converted into scores, and the total score was used to calculate the risk probability of HCA in patients with PROM. The model was validated using the following methods: Bootstrap self-sampling (number of samples = 1000) to assess stability; C-index and receiver operating characteristic (ROC) curves were calculated to assess discriminatory ability (a C-index closer to 1 and an area under the curve (AUC) greater than 0.7 indicated good discrimination); calibration curves were drawn and the Hosmer-Lemeshow test was used to assess the consistency between predicted and actual risk (P > 0.05 indicated good calibration). Decision curve analysis (DCA) was used to assess the clinical utility of the model. Using net benefit as the metric, the nomogram model was compared with two extreme strategies: “treat all patients” and “do not treat all patients” at different risk thresholds to clarify the model’s clinical applicability. P < 0.05 was considered statistically significant.
), and intergroup comparisons were performed using the independent sample t-test. Enumeration data were expressed as number of cases (constituent ratio, %), and intergroup comparisons were performed using the chi-square test. Variables with a P < 0.1 in the univariate analysis were included in a multivariate logistic regression analysis using stepwise regression (forward method, α in = 0.05, α out = 0.10) to identify independent risk factors for HCA (P < 0.05). To ensure sufficient statistical power and model stability, we calculated the event-to-variable ratio (EPV) for the multivariate logistic regression analysis. In the modeling group, 83 patients presented with histological chorioamnionitis, and the multivariate model included 7 variables, with an EPV of approximately 11.9. This value exceeds the generally recommended minimum EPV threshold of 10, indicating that the multivariate logistic regression model has sufficient statistical power and is unlikely to overfit. Based on the independent risk factors, a nomogram model was constructed using the “rms” package in R software. The regression coefficients of each factor were converted into scores, and the total score was used to calculate the risk probability of HCA in patients with PROM. The model was validated using the following methods: Bootstrap self-sampling (number of samples = 1000) to assess stability; C-index and receiver operating characteristic (ROC) curves were calculated to assess discriminatory ability (a C-index closer to 1 and an area under the curve (AUC) greater than 0.7 indicated good discrimination); calibration curves were drawn and the Hosmer-Lemeshow test was used to assess the consistency between predicted and actual risk (P > 0.05 indicated good calibration). Decision curve analysis (DCA) was used to assess the clinical utility of the model. Using net benefit as the metric, the nomogram model was compared with two extreme strategies: “treat all patients” and “do not treat all patients” at different risk thresholds to clarify the model’s clinical applicability. P < 0.05 was considered statistically significant.
Results
Comparison of Baseline Data Between the Modeling Group and the Validation Group
There were no statistically significant differences in the distribution of inclusion time periods and baseline data (age, BMI, GBS positivity rate, diagnostic, treatment techniques and HCA, etc.) between the modeling group and the validation group (all P>0.05), suggesting that randomization effectively balanced potential confounding factors (including medical technology advances that change over time) and that the two groups were comparable. See Table 1.
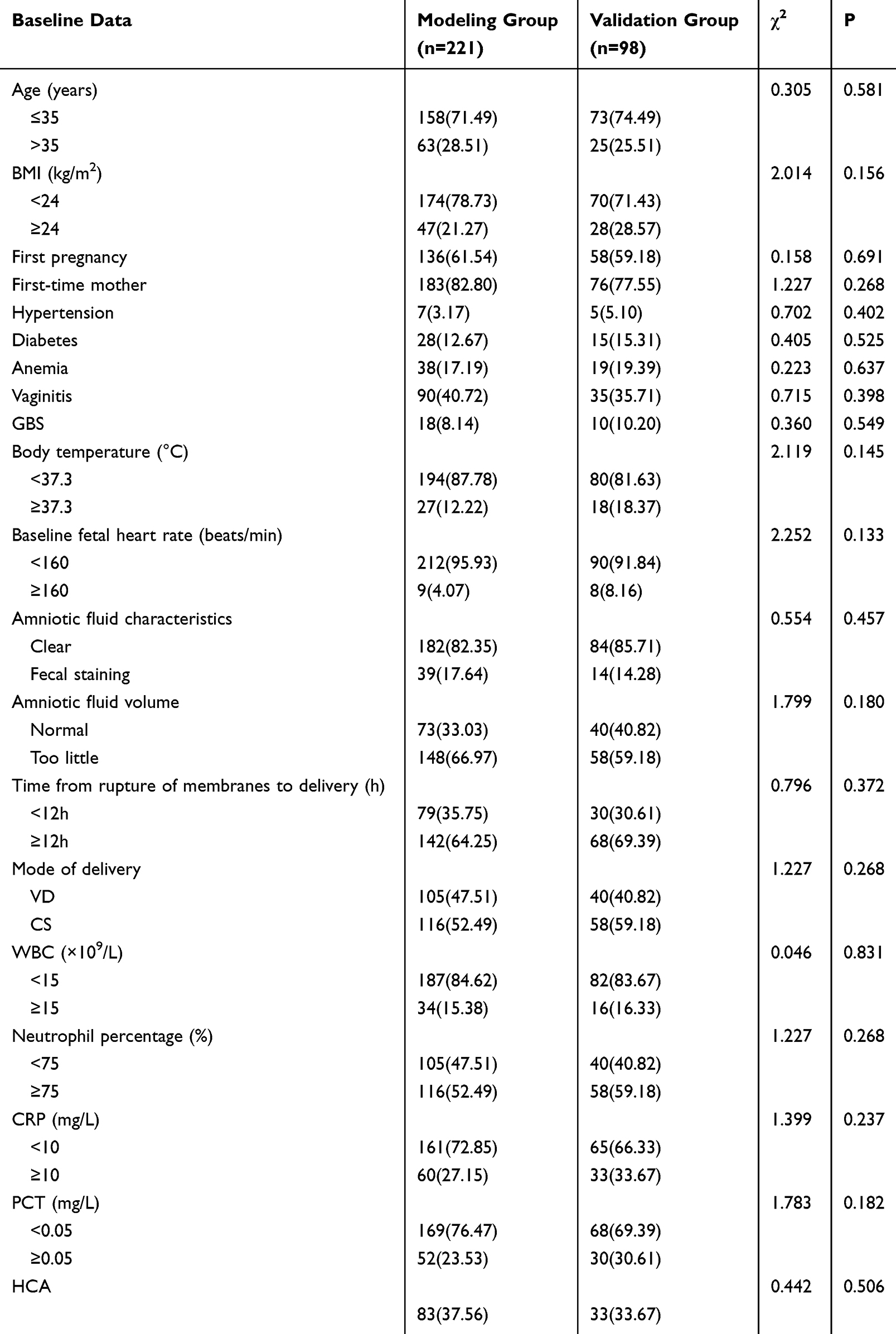 |
Table 1 Baseline Data |
Comparison of Baseline Data of HCA Patients in the Modeling Group and Whether They Were Combined
Compared with the non HCA group, the proportion of HCA group patients with body temperature ≥ 37.3 °C, baseline fetal heart rate ≥ 160 beats/min, rupture to delivery time ≥ 12 hours, cesarean section, WBC ≥ 15×10 9/L, neutrophil percentage ≥ 75%, and PCT ≥ 0.05 mg/L were significantly higher, and the differences were statistically significant (P<0.05), as shown in Table 2.
 |
Table 2 Comparison of Baseline Data of HCA Patients in the Modeling Group and Whether They Were Combined |
Results of Multivariate Logistic Regression Analysis of the Modeling Group
Taking the occurrence of HCA as the dependent variable (no =0, yes =1), and taking the statistically significant indicators in single factor analysis in Table 2 as the independent variables, the assignment situation is as follows: body temperature: < 37.3°C = 0, ≥ 37.3°C = 1; Baseline fetal heart rate: < 160 beats/min = 0, ≥160 beats/min = 1; Time from rupture of fetal membrane to delivery: < 12h = 0, ≥ 12h = 1; Mode of delivery: vaginal delivery (VD)= 0, cesarean section (CS)= 1; WBC: <15×109/L = 0, ≥15×109/L = 1; Percentage of neutrophils: < 75% = 0, ≥ 75% = 1; PCT: <0.05 mg/L = 0, ≥0.05 mg/L = 1; Multivariate logistic regression analysis showed that body temperature ≥37.3°C, cesarean delivery, WBC ≥ 15×109/L, neutrophil percentage ≥75% and PCT ≥0.05 mg/L were independent risk factors for HCA (P < 0.05). (See Table 3).
 |
Table 3 Logistic Regression Analysis |
Construction of the Nomogram Model of the Modeling Group
Based on five independent influencing factors identified by multivariate logistic regression analysis (body temperature, mode of delivery, WBC, and neutrophil percentage), a nomogram model for predicting HCA in patients with PROM was successfully constructed (Figure 2). Based on the predefined scoring rules described in the Methods section, the regression coefficients of each independent predictor were proportionally converted into corresponding point values in the nomogram (eg, body temperature ≥37.3 °C was assigned a higher score relative to other predictors). The sum of these scores yields a total score (ranging from 0 to 220). This total score can then be used to directly determine the patient’s risk of HCA (eg, a total score of 150 corresponds to an approximately 70% risk). The model’s visual design allows clinicians to quickly input the patient’s five indicators and intuitively obtain personalized risk assessment results.
 |
Figure 2 Nomogram model. Notes: The sum of the corresponding scores of each indicator in the nomogram is the total score, which can be used to directly read the risk probability of HCA (for example, a total score of 150 points corresponds to a risk of approximately 70%). |
Verification of the Nomogram Model
ROC Curves
The model was internally validated using the bootstrap self-sampling method (number of samplings = 1000 times). The C index of the model was 0.875 (95% CI: 0.821–0.929), indicating a strong ability to distinguish HCA. Receiver operating characteristic (ROC) curve analysis showed that the area under the curve (AUC) was 0.890 (95% CI: 0.805–0.913, P < 0.001), with a sensitivity of 83.7% and a specificity of 81.6%, indicating that the model had a high predictive accuracy for HCA (Figure 3A).
 |
Figure 3 ROC curves of the modeling group (A) and validation group (B). |
The nomogram model was applied to the validation group (98 cases) for external validation. The results showed that the C index of the model was 0.852 (95% CI: 0.783–0.921), indicating that it still had good discriminatory ability in independent samples. ROC curve analysis showed that the AUC was 0.885 (95% CI: 0.776–0.918, P < 0.001), the sensitivity was 81.2%, and the specificity was 73.5%, which were close to the results of the modeling group (Figure 3B).
Calibration Curves
The calibration curve showed a good fit between the HCA risk predicted by the nomogram and the actual probability of occurrence (Figure 4A). The Hosmer-Lemeshow test showed a x2 = 5.236, P = 0.732 (>0.05), indicating good consistency and calibration between the model-predicted and actual risks.
 |
Figure 4 Calibration curves of the modeling group (A) and the validation group (B). |
The calibration curve showed a good fit between the nomogram-predicted and actual probability of occurrence in the validation group (Figure 4B). The Hosmer-Lemeshow test showed a x2 = 6.102, P = 0.636 (>0.05), indicating that the model maintained good calibration in external samples and exhibited good predictive stability.
DCA Curves
DCA results showed that within a wide range of risk thresholds (modeling group: 0.1–0.8; validation group: 0.1–0.7), the net benefit of the nomogram model constructed in this study was higher than the two extreme strategies of “treating all patients” or “not treating all patients” (Figure 5A and B).
 |
Figure 5 DCA curves of the modeling group (A) and the validation group (B). |
Discussion
PROM is a common perinatal complication, the incidence of which increases with gestational age and is closely related to premature birth, infection, and adverse pregnancy outcomes. Among them, HCA is one of the important complications of PROM, with an incidence as high as 40%-70%, significantly increasing the risk of premature birth, infection, and adverse neonatal outcomes.11 However, the clinical manifestations of HCA are often atypical, making early diagnosis difficult, leading to delayed treatment and further increasing the risk of maternal and infant health. Currently, the diagnosis of HCA mainly relies on histological examination, but there is a lag, which makes it difficult to meet the needs of early clinical intervention.12 Although studies have explored the predictive factors and biomarkers of HCA, there is a lack of a unified prediction model and standardized clinical guidelines. Therefore, further research on the predictive factors of HCA and optimization of the prediction model are of great significance for improving the maternal and infant outcomes of PROM patients.
The results of multivariate logistic regression analysis in this study showed that body temperature, mode of delivery, WBC count, and neutrophil percentage,PCT were independent risk factors for HCA in patients with PROM. Elevated body temperature is a typical immune response to infection. After membrane rupture in patients with PROM, pathogens retrogradely invade the uterine cavity, activating the Toll-like receptor (TLR) signaling pathway and releasing proinflammatory cytokines. These cytokines then act on the hypothalamic thermoregulatory center, leading to increased heat production and decreased heat dissipation, manifesting as an elevated body temperature (≥37.3°C).13,14 Cesarean section (CS) is an invasive method of delivery. It can destroy the amniotic membrane barrier through surgical operation, increasing the chance of infection. In addition, surgical trauma can activate the sympathetic nerve-adrenal axis, release hormones such as cortisol, inhibit the phagocytic function of neutrophils and the secretion of cytokines, reduce the body’s ability to clear intrauterine infection, and indirectly promote the occurrence of HCA.15,16 Increased WBC and neutrophil counts reflect the degree of inflammatory response and infection. When pathogenic microorganisms invade the uterine cavity and cause HCA, bacterial lipopolysaccharide can stimulate the proliferation and differentiation of bone marrow hematopoietic stem cells, release a large number of neutrophils into the blood circulation, and at the same time promote the migration of neutrophils to the inflammatory site, which is manifested as increased WBC and neutrophil counts.17,18 Studies have shown19 that PROM duration >18 hours and increased WBC are independent risk factors for HCA, indicating an increased risk of inflammatory response and infection. PCT is a kind of peptide precursor produced in large quantities by thyroid C cells, liver, lung and other tissue cells during bacterial infection, which generally does not increase in viral infection, so it has high specificity for bacterial infection. In PROM patients, pathogenic microorganisms invade the uterine cavity after the rupture of fetal membranes, which can cause local and even systemic inflammatory reactions and stimulate various cells to release PCT. The increase of PCT level not only reflects the severity of infection, but also may promote leukocyte infiltration and cytokine storm by amplifying inflammatory cascade, and aggravate the inflammatory damage of chorioamnion tissue.20,21
Compared with previous studies, the findings of this research demonstrate better consistency in overall trends.Wang et al11 found in a study involving late preterm and full-term PROM populations that elevated maternal body temperature, increased WBC, and elevated neutrophil proportion were significantly associated with the occurrence of HCA, with a model AUC of 0.82.In this study, the predictive model constructed based on the inclusion of only full-term PROM participants achieved an AUC of 0.890, demonstrating superior discriminative performance. This suggests that the model’s predictive efficacy may be further enhanced in relatively homogeneous populations.Previous studies have predominantly focused on traditional inflammatory markers (eg, WBC, CRP), while attention to PCT has been relatively limited.Studies by Jalkanen et al20 and Horinouchi et al21 suggest that procalcitonin (PCT) has certain value in predicting HCA and adverse neonatal outcomes.This study incorporated PCT into multivariate analysis and confirmed it as an independent risk factor, further supporting its potential clinical significance in the early risk assessment of PROM combined with HCA. In terms of model construction, while some studies used single indicators or scoring systems for risk stratification, this study integrated body temperature, mode of delivery, and multiple inflammatory markers through a column chart format, making the predictive results more intuitive and facilitating rapid clinical decision-making.
The core value of the nomogram lies in visualizing the complex results of multivariate regression analysis. The five indicators incorporated into this model are all closely related to the pathophysiology of HCA. Results showed that the model had a C index of 0.875, indicating strong discrimination for HCA. The receiver operating characteristic (ROC) curve demonstrated high predictive accuracy for HCA. The calibration curve showed a high degree of fit between the nomogram-predicted HCA risk and the actual probability of occurrence, indicating good consistency and ideal calibration between the model-predicted and actual risks. Meanwhile, DCA is used to evaluate the clinical net benefit of the predictive model across different threshold probability ranges, thereby determining whether the model has practical clinical application value. The DCA results of this study show that, within a wider threshold probability range, the net benefit of the predictive model is higher than the extreme strategies of “intervention for all patients” or “no intervention for all patients,” suggesting the model’s potential utility in clinical risk decision-making. For clinicians, DCA provides a visual tool to translate predicted probabilities into a basis for clinical action. When physicians set acceptable risk thresholds based on their own experience or guidelines, if the model shows a positive net benefit within that threshold range, using the model for risk stratification helps optimize intervention timing, reduce unnecessary treatment, and avoid delays in managing high-risk patients. This nomogram’s visual design allows physicians to input five common indicators to obtain a personalized HCA risk score (eg, >30% indicates high risk), guiding early intervention. Through personalized intervention, the incidence of maternal and fetal infection-related complications can be reduced, thereby improving long-term pregnancy outcomes.22–24 From a clinical perspective, the nomogram developed in this study provides a practical and intuitive tool for early risk stratification of HCA in PROM patients. The five predictors included in the nomogram—maternal body temperature, mode of delivery, WBC, neutrophil percentage, and procalcitonin are all routinely available clinical or laboratory indicators during hospital admission or intrapartum monitoring. This allows clinicians to quickly assess an individual patient’s HCA risk without requiring additional examinations or complex calculations. In clinical practice, clinicians can input these five variables into the nomogram to obtain a total score and the corresponding predicted probability of HCA. For example, patients with a high total score (eg, predicted risk >30–40%) may be considered to have an increased potential risk of intrauterine infection. In this case, the nomogram can help clinicians enhance maternal and infant monitoring, optimize the timing of antibiotic treatment, and carefully evaluate delivery management strategies. Conversely, patients with low predicted risk can avoid unnecessary interventions, thereby reducing overtreatment and the resulting burden on the mother and baby.
To improve the interpretability and applicability of this model in clinical practice, this study further clarifies potential clinical management strategies that can be considered at different predicted risk levels. It is important to emphasize that the predictive model developed in this study is intended to assist in risk stratification, not replace clinical decision-making. When the predicted risk is low, patients can continue to receive routine obstetric monitoring and follow-up. When the predicted risk reaches an intermediate level, clinicians may consider enhancing maternal temperature monitoring, inflammatory marker assessment, and fetal heart rate monitoring, and assess the need for prophylactic antibiotic treatment based on clinical presentation. When the predicted risk is high, the model results may suggest that clinicians increase their vigilance for potential histological chorioamnionitis. In this case, clinicians may consider early anti-infective therapy and carefully evaluate the timing and mode of delivery according to established clinical guidelines, based on a comprehensive assessment of gestational age, maternal and infant condition, and evidence of infection.
This study has several limitations that need to be addressed. As a single-center retrospective study, the sample size was relatively small, inevitably leading to selection bias. The generalizability of the predictive model needs further validation in multicenter prospective cohort studies. Furthermore, some clinically relevant factors, such as the time from rupture of membranes to delivery and prior antibiotic use, were not included in the analysis, which may have affected the model’s comprehensiveness. Some continuous variables were categorized rather than modeled as continuous predictors. While this approach may aid clinical interpretation and application, it may also lead to some information loss and reduced statistical power, which should be considered a methodological limitation. Additionally, despite internal validation procedures, stepwise regression methods still carry an inherent risk of overfitting, and this limitation should be considered when interpreting model performance. Although DCA was performed to assess the model’s clinical applicability, the optimal clinical decision threshold was not clearly defined. Therefore, the net benefit at a specific risk threshold and its practical application in different clinical scenarios warrant further investigation.
Conclusion
Body temperature, delivery mode, WBC, neutrophil percentage, and PCT are significantly associated with HCA in PROM patients. The nomogram model shows good discrimination, calibration, and stability, and may assist in predicting HCA risk in clinical practice.
This nomogram provides a simple and practical tool for early risk stratification of histological chorioamnionitis in full-term PROM patients using routine clinical data. It helps clinicians identify high-risk patients requiring close monitoring or timely intervention, while avoiding unnecessary treatment of low-risk cases. This model is intended to complement, not replace, clinical judgment.
Data Sharing Statement
The experimental data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
This study was reviewed and approved by Beijing Chao-yang Hospital Affliated to Capital Medical University ethics committee (approval number: 2025-KE-856). This study was a retrospective observational study, and the requirement for informed consent was waived by the Beijing Chao-yang Hospital Affliated to Capital Medical University Ethics Committee due to the nature of the research. All methods were carried out in accordance with Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was not funded by any funding.
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Lanzarone V, Polkinghorne A, Eslick G, Branley J. Diagnostic tests for the prediction of histological chorioamnionitis and funisitis in pregnant women with preterm premature rupture of membranes: a systematic review. Australian New Zealand J Obstetric Gynaecol. 2025;65(1):13–13. doi:10.1111/ajo.13864
2. Shi H, Sun L, Wang Z, et al. Non-invasive prediction of histologic chorioamnionitis using maternal serum markers in women with preterm prelabour rupture of membranes. Am J Reproduct Immunol. 2022;88(3):e13594. doi:10.1111/aji.13594
3. Gouda ADK, Aboushady RMN, Elhoufey A, Badia TS. Prevalence of preterm premature rupture of membranes and its correlated risk factors among pregnant women attending Women Health Hospital, Assiut University, Egypt. Malaysian J Nurs. 2025;16(3):148–159. doi:10.31674/mjn.2025.v16i03.015
4. Kovács K, Kovács ŐZ, Bajzát D, et al. The histologic fetal inflammatory response and neonatal outcomes: systematic review and meta-analysis. Am J Obstetric Gynecol. 2024;230(5):493–511.e3. doi:10.1016/j.ajog.2023.11.1223
5. Sarno L, Della Corte L, Saccone G, et al. Histological chorioamnionitis and risk of pulmonary complications in preterm births: a systematic review and meta-analysis. J Maternal Fetal Neonatal Med. 2021;34(22):3803–3812. doi:10.1080/14767058.2019.1689945
6. Beck C, Gallagher K, Taylor LA, Goldstein JA, Mithal LB, Gernand AD. Chorioamnionitis and risk for maternal and neonatal sepsis: a systematic review and meta-analysis. Obstetric Gynecol. 2021;137(6):1007–1022. doi:10.1097/AOG.0000000000004377
7. Shi Z, Chen Y, Liu A, et al. ‘Application of random survival forest to establish a nomogram combining clinlabomics-score and clinical data for predicting brain metastasis in primary lung cancer’. Clin Translat Oncol. 2025;27(4):1472–1483. doi:10.1007/s12094-024-03688-x
8. Soveral I, Crispi F, Guirado L, et al. ‘Fetal cardiac filling and ejection time fractions by pulsed-wave Doppler: reference ranges and potential clinical application’. Ultrasound Obstetri Gynecol. 2021;58(1):83–91. doi:10.1002/uog.22152
9. Sénat MV, Schmitz T, Bouchghoul H, et al. Term prelabor rupture of membranes: guidelines for clinical practice from the French College of Gynaecologists and Obstetricians (CNGOF)’. J Maternal Fetal Neonatal Med. 2022;35(16):3105–3109. doi:10.1080/14767058.2020.1810230
10. Ajayi SO, Morris J, Aleem S, et al. Association of clinical signs of chorioamnionitis with histological chorioamnionitis and neonatal outcomes. J Maternal Fetal Neonatal Med. 2022;35(26):10337–10347. doi:10.1080/14767058.2022.2128648
11. Wang X, Huang Z, Ma Y. Development and validation of a multivariable predictive model for the risk of histologic chorioamnionitis in patients with premature rupture of membranes in the late preterm and term. Int J Gen Med. 2024;17:141–152. doi:10.2147/IJGM.S445374
12. Shahshahan Z, Zarean E, Jahanfar S, Hedayat P. Comparison of histological chorioamnionitis in pre-term delivery with and without pre-term rupture of membrane. Advanc Biomed Res. 2024;13:33. doi:10.4103/abr.abr_300_21
13. Abu Shqara R, Glikman D, Jad S, Rechnitzer H, Lowenstein L, Frank Wolf M. Antibiotic treatment of women with isolated intrapartum fever vs clinical chorioamnionitis: maternal and neonatal outcomes. Am J Obstetri Gynecol. 2023;229(5):
14. Rottenstreich A, Levin G, Tsur A, Shai D, Meyer R. Chorioamnionitis at latent phase more than doubles the risk for cesarean delivery compared to chorioamnionitis at active phase. Archiv Gynecol Obstetric. 2021;303(4):905–910. doi:10.1007/s00404-020-05815-9
15. Katakura Y, Nagamine Y, Goto T, Sumikura H. Association of chorioamnionitis with failed conversion of epidural labor analgesia to cesarean delivery anesthesia: a retrospective cohort study. PLoS One. 2021;16(5):e0250596. doi:10.1371/journal.pone.0250596
16. Tanabe S, Yoshimoto A, Sugino S, Ichida K, Niiya K, Morishima S. A case of sudden multiple hematomas during cesarean section due to amniotic fluid embolism. Int J Surg Case Rep. 2023;107:108342. doi:10.1016/j.ijscr.2023.108342
17. Balciuniene G, Kvederaite-Budre G, Gulbiniene V, et al. Neutrophil–lymphocyte ratio for the prediction of histological chorioamnionitis in cases of preterm premature rupture of membranes: a case-control study. BMC Pregnanc Childbirth. 2021;21(1):656. doi:10.1186/s12884-021-04101-z
18. Lv Y, Huang Z, Ma Y. Association analysis between maternal neutrophil ratio and the risk of histological chorioamnionitis in pregnant women with premature rupture of membranes in late pregnancy. Int J Gen Med. 2024;17:1499–1508. doi:10.2147/IJGM.S457645
19. Qiu L, Pan M, Zhang R, Ren K. Maternal peripheral blood platelet-to-white blood cell ratio and platelet count as potential diagnostic markers of histological chorioamnionitis-related spontaneous preterm birth. J Clin Laborat Analys. 2019;33(4):e22840. doi:10.1002/jcla.22840
20. Jalkanen K, Virtanen A, Aittoniemi J, et al. Novel biomarkers: soluble urokinase-type plasminogen activator receptor and procalcitonin and histological chorioamnionitis after preterm premature rupture of membranes. Reproduct Sci. 2024;31(10):3175–3182. doi:10.1007/s43032-024-01678-6
21. Horinouchi T, Yoshizato T, Kozuma Y, et al. Prediction of histological chorioamnionitis and neonatal and infantile outcomes using procalcitonin in the umbilical cord blood and amniotic fluid at birth. J Obstetric Gynaecol Res. 2018;44(4):630–636. doi:10.1111/jog.13573
22. Choi SR, Choi SJ. Afterbirth oral fluid secretory leukocyte protease inhibitor decreased in acute histologic chorioamnionitis in preterm birth. Am J Reproduct Immunol. 2023;90(1):e13733. doi:10.1111/aji.13733
23. Bademkiran MH, Bademkiran C, Ege S, et al. Explanatory variables and nomogram of a clinical prediction model to estimate the risk of caesarean section after term induction. J Obstetric Gynaecol. 2021;41(3):367–373. doi:10.1080/01443615.2020.1798902
24. Xiu Y, Lin Z, Pan M. ‘Establishment and validation of a prognostic model for premature rupture of membranes and preterm delivery in pregnant women after cervical conization’. Am J Translat Res. 2024;16(10):5923–5932. doi:10.62347/VNQF3805
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Model That Predicts the Risk of Diabetic Nephropathy in Type 2 Diabetes Mellitus Patients: A Cross-Sectional Study
Yang J, Jiang S
International Journal of General Medicine 2022, 15:5089-5101
Published Date: 20 May 2022
Development of Risk Prediction Model for Muscular Calf Vein Thrombosis with Acute Exacerbation of Chronic Obstructive Pulmonary Disease
Hu X, Li X, Xu H, Zheng W, Wang J, Wang W, Li S, Zhang N, Wang Y, Han K
International Journal of General Medicine 2022, 15:6549-6560
Published Date: 10 August 2022
Paraspinal Muscle Degeneration: A Potential Risk Factor for New Vertebral Compression Fractures After Percutaneous Kyphoplasty
Si F, Yuan S, Zang L, Fan N, Wu Q, Wang T, Wang A
Clinical Interventions in Aging 2022, 17:1237-1248
Published Date: 13 August 2022
Tracking Epidemiological Characteristics and Risk Factors of Multi-Drug Resistant Bacteria in Intensive Care Units
Wu C, Lu J, Ruan L, Yao J
Infection and Drug Resistance 2023, 16:1499-1509
Published Date: 15 March 2023
Construction and Validation of a Novel Nomogram for Predicting the Recurrence of Diffuse Large B Cell Lymphoma Treated with R-CHOP
Gong Y, Yan H, Yang Y, Zhai B, Huang Z, Zhang Z
Pharmacogenomics and Personalized Medicine 2023, 16:291-301
Published Date: 1 April 2023