Back to Journals » Journal of Pain Research » Volume 18
Determining the Effective Dose of Oliceridine Compounded with Propofol for Painless Hysteroscopy: A Prospective Modified Dixon Sequential Dose-Finding Study
Authors Yang K ![]() , Yuan Q, Huang H, Wang L, You J, Liu Q, Zhou Y, Luo Y, Liu Q
, Yuan Q, Huang H, Wang L, You J, Liu Q, Zhou Y, Luo Y, Liu Q
Received 20 August 2025
Accepted for publication 10 December 2025
Published 18 December 2025 Volume 2025:18 Pages 6903—6910
DOI https://doi.org/10.2147/JPR.S557764
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Ke Yang,1 Qian Yuan,1 Hao Huang,1 Lina Wang,1 Jingyu You,1 Qiaojie Liu,1 Yulin Zhou,2 Yi Luo,3 Qin Liu1
1Department of Anesthesiology, Zigong Maternal and Child Health Care Hospital, Zigong, People’s Republic of China; 2Department of Central Operating Room, Zigong Maternal and Child Health Care Hospital, Zigong, People’s Republic of China; 3Department of Gynecology, Zigong Maternal and Child Health Care Hospital, Zigong, People’s Republic of China
Correspondence: Qin Liu, Email [email protected]
Background: Oliceridine combined with propofol is suitable for intravenous anesthesia in painless hysteroscopy. This study aimed to determine the 50% effective dose (ED50) and 95% effective dose (ED95) of oliceridine compounded with propofol for painless hysteroscopy.
Methods: In all, 29 patients aged 18– 60 years who were scheduled for painless hysteroscopy under intravenous anesthesia were recruited, and a total of 26 patients were enrolled in the final analysis. The trial was conducted using the modified Dixon sequential method, with an initial dose of 1.5 mg of oliceridine, followed by 2.0– 2.5 mg/kg of propofol administered 1 minute later. Whether the dose of oliceridine was increased or decreased depends on the prior operation. If the hysteroscopy failed (positive response), which was defined as inadequate cervical dilatation, patient body movements, frowning, heart rate (HR), or mean arterial pressure (MAP) greater than 20% of the baseline value, or a MOAA/S score ≥ 2, the subsequent dosage of oliceridine was increased by 0.1 mg. Conversely, the dose was decreased by 0.1 mg. At least seven crossover waves had to occur before the formal test was stopped. The probit regression method was used to determine the ED50 and ED95 with 95% confidence intervals (CIs).
Results: The ED50 and ED95 of oliceridine in patients were 1.583 (95% CIs: 1.444– 1.857) mg and 1.848 (95% CIs: 1.701– 4.409) mg, respectively.
Conclusion: A dose of 1.848 mg oliceridine compounded with propofol provides an effective anesthesia approach for painless hysteroscopy. Future larger, multicenter studies will help to expand the population range of oliceridine use and explore its potential benefits and risks.
Keywords: ED50, ED95, oliceridine, painless hysteroscopy
Introduction
Hysteroscopy has gained widespread application in gynecological procedures, while surgical operations such as cervical dilatation and uterine distension are strongly stimulated, frequently causing patients considerable discomfort and even making it difficult for the gynecologist to operate due to the patient’s struggle and twisting movements.1–3 Previous research has indicated that severe pain and discomfort in women was a potential risk within hysteroscopy.4 With the proposal and development of the concept of enhanced recovery after surgery (ERAS), painless hysteroscopy has become a crucial choice for gynecological diagnosis and treatment based on its advantages of safety and tolerance. Propofol combined with opioids is a commonly used sedation and analgesia scheme at present, which can inhibit the severe pain caused by cervical dilatation and provide a satisfactory anesthetic effect for hysteroscopy.5,6 However, the incidence of respiratory and circulatory depression in classical opioids during operation is high, so it is necessary to further explore an anesthesia scheme that is more suitable for hysteroscopy.
As a selective G protein signal transduction pathway, oliceridine is an opioid receptor agonist with low effect on β inhibitory protein recruitment, with rapid onset and short half-life.7,8 According to its unique partial ligand mechanism, it can effectively relieve pain and reduce adverse reactions such as respiratory depression, nausea and vomiting.8–10 The pharmacodynamic characteristics of rapid onset and short-acting duration of oliceridine make it more suitable for situations where procedural sedation and recovery are needed than classical opioids. Although current research and studies have highlighted the potential of oliceridine in the field of sedation and analgesia,9–11 the optimal effective dose of oliceridine for painless hysteroscopy and its safety and efficacy remain to be determined. In order to determine the 50% effective dose (ED50) and 95% effective dose (ED95) of oliceridine combined with propofol during painless hysteroscopy, we designed this prospective dose-finding study so as to provide a reference for future clinical application.
Methods
Study Design
This prospective dose-finding study was conducted from March 2025 to June 2025 at the Zigong Maternal and Child Health Care Hospital and was approved by the ethical committee (2024-IRB-017). The protocol was registered with the Chinese Clinical Trials Registry on 17 March 2025 (ChiCTR2500098967), and all experiments were conducted following the principles of the Helsinki Declaration and the CONSORT guidelines. Informed consent forms were signed by all participants before enrollment in this study.
Patients
Patients who were scheduled for painless hysteroscopy under intravenous anesthesia in our hospital were recruited. Inclusion criteria: (1) age of 18–60 years; (2) BMI index of 18–25 kg/m2; (3) American Society of Anesthesiologists (ASA) physical status of I–II. Exclusion criteria were as follows: (1) Patients who refuse to participate in this trial; (2) Patients with hypertension or other abnormal functions such as heart, lung, liver, and kidney; (3) Patients with obstructive sleep apnea syndrome or difficult airways; (4) Patients with respiratory infections in the recent 2 weeks; (5) Patients with psychiatric diseases or long-term history of taking sedative and analgesic drugs; (6) Those who were allergic to general anesthesia drugs.
Anesthesia Protocol
Before surgery, all patients were required to fast for at least 8h and had imbibed no clear liquids for 2h before intravenous anesthesia. Routine monitoring, including electrocardiogram (ECG), blood pressure (BP), and pulse oxygen saturation (SpO2), was performed as soon as the patient entered the operation room, and oxygen was delivered at 5 L/min with a mask. After the peripheral venous channel was established in the left hand, anesthesia induction was started by the same anesthesiologist according to the experimental scheme. The initial dose of oliceridine was determined to be 1.5 mg based on the previous published research,7,9 and followed by 2.0–2.5 mg/kg of propofol at a constant speed for more than 30s, and then pumped intravenously at 2.0 mg/kg/h. After the patient lost consciousness and the modified observer’s assessment of alertness and sedation (MOAA/S) score achieved 0 points, the hysteroscopy was performed by a skilled gynecologist.
The modified Dixon sequential method is recognized as one of the simple and efficient approaches for the determination of the effective dose of drugs and therefore was used to conduct this study.12,13 The next sequential oliceridine dose depended on whether prior hysteroscopy had failed, which was defined as inadequate cervical dilatation and patient body movement, frowning, heart rate (HR) or mean arterial pressure (MAP) greater than 20% of the baseline value, or a MOAA/S score ≥ 2.5,14 If the operation failed (positive response), the subsequent dose of oliceridine was adjusted up by 0.1 mg. Conversely, the dose was adjusted down by 0.1 mg if the examination was successful (negative response). The formal trial starts with the first crossover wave and stops after seven crossovers are observed. Patients were divided into the positive group or the negative group according to their response during hysteroscopy.
An additional 0.5–1.0 mg/kg propofol was added when there was an occurrence of a positive reaction during the operation and then continued after the anesthesia was satisfactory. The vital signs and respiratory status of patients were closely monitored. If the SpO2 drops below 90%, lift the mandible to open the airway first and provide oxygen assistance. Ephedrine (6 mg) was given to raise BP when MAP is below 60 mmHg or basic BP is lower than 20%. Atropine (0.5 mg) was used to treat bradycardia (HR<50) if needed.
The MOAA/S score was chosen to evaluate the sedation scale of patients:14 sensitive to name calls in a normal tone is 5 points; unresponsive to name calls in a normal tone is 4 points; only responsive to loud or repeated name calls is 3 points; responsive to slight stimulation or shaking is 2 points; responsive to painful stimulation is 1 point and have no response is 0 point.
Observation Indicators
The primary outcome was the 50% effective dose (ED50) and 95% effective dose (ED95) of oliceridine compounded with propofol for hysteroscopy. The secondary outcome included the vital signs and visual analog scale (VAS) scores at different time points, consumption of drugs, surgical duration, recovery time, and adverse events. The vital signs (HR, SpO2, MAP, and RR) were measured before analgesia (T0), after injection of propofol (T1), and at the moment of cervix dilation (T2). Pain evaluation using the VAS scores at postoperative 2h, 6h, and 24h. The incidence of adverse events such as nausea and vomiting, dizziness, respiratory depression, and hypotension during the 24 h postoperatively was calculated.
Statistical Analysis
All of the individual participant data were analyzed using SPSSAU (https://spssau.com/indexs.html) and GraphPad Prism version 9.0.0. The normally distributed data were expressed by the mean ± SD, and compared across groups by using the independent samples students’ t-test. Repeated measurement data were analyzed using repeated measures ANOVA. The non-normal distributed data were expressed by the median (interquartile range), and comparison between groups was conducted using the Mann–Whitney U-test. The categorical variables were expressed as percentages and compared using the Chi-square test or Fisher’s exact probability method, where appropriate. The ED50 and ED95 values of oliceridine combined with propofol and their 95% confidence interval were determined utilizing Probit analysis via probability unit regression. The p-value was set lower than 0.05, indicating that the difference is statistically significant.
Results
A total of 29 eligible patients were recruited for this study, and 3 patients were excluded. Consequently, 26 patients were included in the final analysis (Figure 1). The baseline demographic characteristics are presented in Table 1, such as age, height, weight, BMI, and ASA classification, and they were similar among the two groups (p>0.05). Table 2 summarizes the perioperative information of the patients, and there was no significant difference in surgical duration, time of recovery, or initial dose of propofol, except for the total propofol dose and oliceridine dose. We recorded the VAS scores at 2 h, 6 h, and 24 h postoperative, and the comparative analysis indicated that VAS scores at 2 and 6 h after surgery of patients in the negative group were significantly lower than those in the positive group (p<0.05) (Table 2). Only one patient suffered from hypotension, and one patient had nausea and vomiting during the postoperative period. No significant differences were observed in the adverse events among the positive and negative groups (p>0.05) (Table 3).
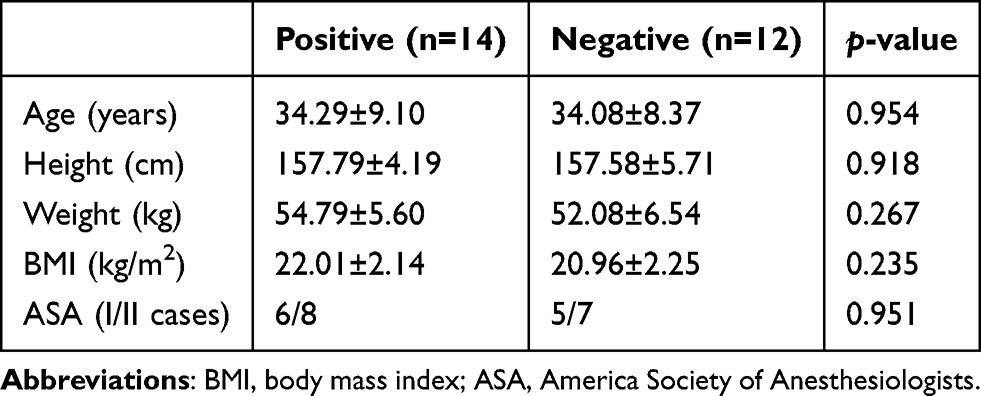 |
Table 1 Demographic Characteristics |
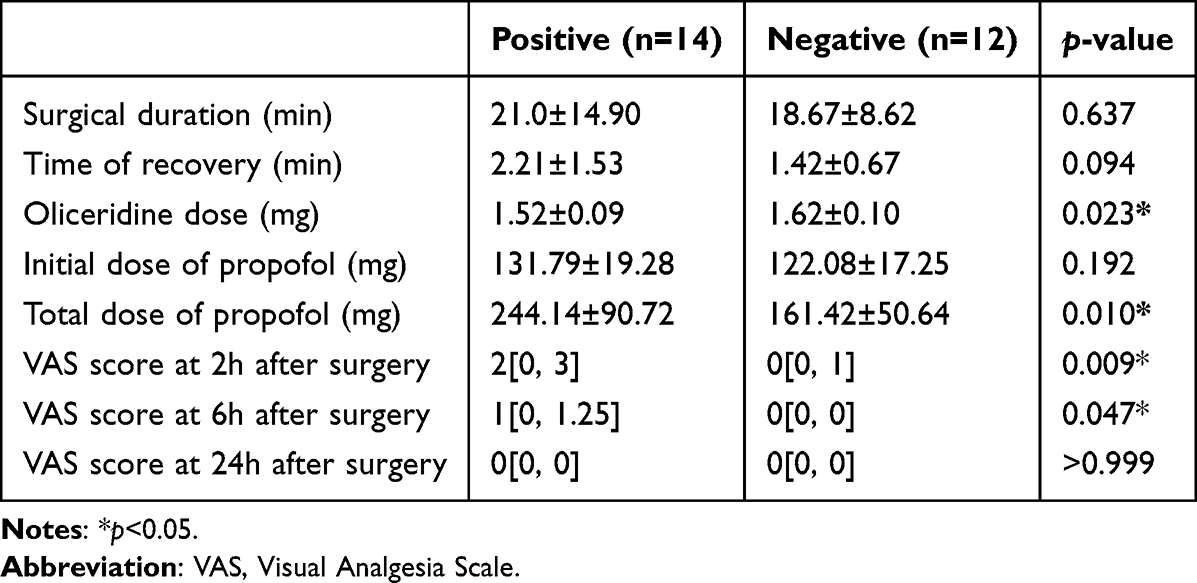 |
Table 2 Comparison of the Perioperative Information of the Patients |
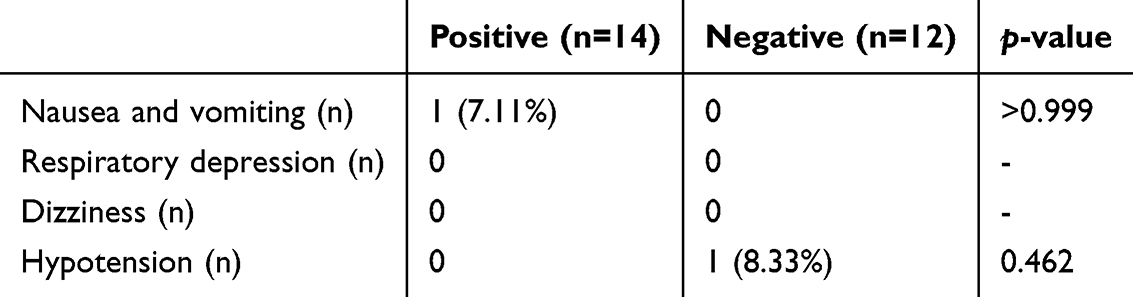 |
Table 3 Incidence of Adverse Events Within 24 h Postoperatively |
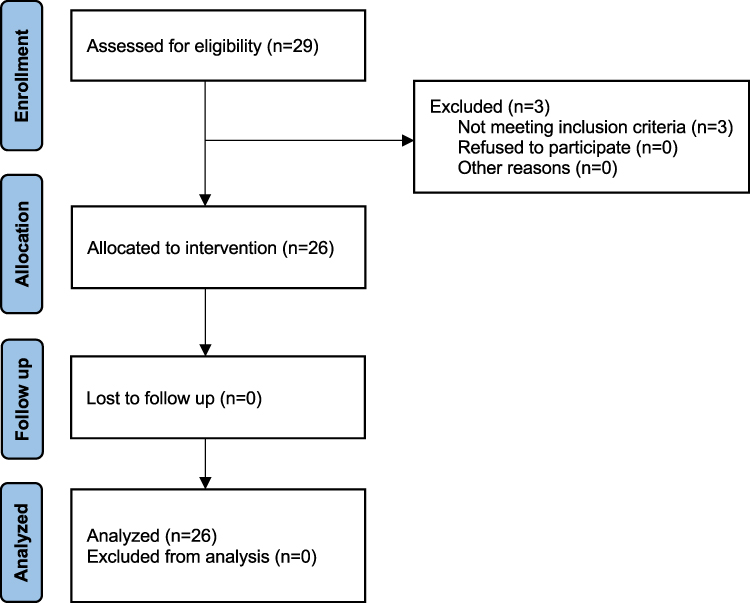 |
Figure 1 Flow chart of this study. |
The sequential dose of oliceridine combined with propofol for painless hysteroscopy is presented in Figure 2. The probit regression analysis yielded the equation probit (P)= −9.805 + 6.195 × oliceridine dose. The Pearson goodness-of-fit test χ2 =5.164 (p=0.160) confirmed that the equation fully fitted the data. According to the modified Dixon sequential method, the values of ED50 and ED95 were 1.583 (1.444–1.857) mg and 1.848 (1.701–4.409) mg, respectively.
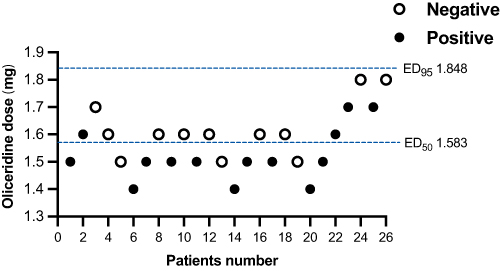 |
Figure 2 Sequence diagram of oliceridine for painless hysteroscopy. A circle indicates a negative response, while a filled circle represents a positive response. |
The results of hemodynamic and respiratory parameters at T0, T1, and T2 are shown in Table 4. Compared to T0, the MAP and RR at both T1 and T2 were considerably lower (p<0.05).
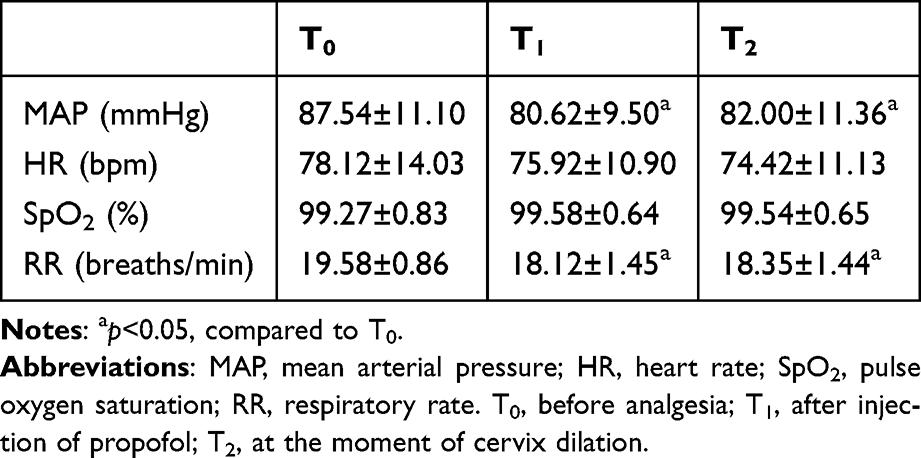 |
Table 4 Hemodynamic and Respiratory Parameters at Different Time Points |
Discussion
Hysteroscopy, as a gynecological procedure, is known to be the gold standard for inspection of uterine pathological conditions and abnormal uterine bleeding.4,15 Although the procedure is thought to be low-pain and well-tolerated, it is reported that almost 25% of patients were experiencing intolerable or even severe pain.16 The cervical length and flexion, intrauterine pressure, and preoperative anxiety are multiple factors related to the pain during hysteroscopy.2,15,17,18 Therefore, a right and appropriate anesthesia scheme is crucial for guaranteeing a smooth hysteroscopy and quick recovery. Intravenous anesthesia based on propofol has been used in clinics for more than 30 years for its stable, clear-headed recovery and antiemetic characteristics.19 When it is co-administered with opioids (such as alfentanil,5 nalbuphine,6 and sufentanil),20 it can inhibit the pain caused by cervical dilatation and provide a satisfactory anesthetic effect for hysteroscopy. However, it is worth noting the risk of respiratory and cardiovascular suppression and gastrointestinal-related adverse events.
As the first G-protein biased μ opioid receptor agonist, Oliceridine selectively activates the G-protein signaling pathways and weakens the effect of β-arrestin recruitment. This partial ligand mechanism enables it to provide equal or even better analgesia while reducing the incidence of opioid-related adverse events.7,21,22 Oliceridine provided comparable analgesia efficacy with superior safety compared to sufentanil in gastrointestinal endoscopy.23 However, there are a few studies that have paid attention to oliceridine in painless hysteroscopy. Therefore, it is imperative to conduct this study to explore the effective dose of oliceridine in hysteroscopy and evaluate its safety.
Oliceridine offers a rapid onset of action that takes effect 1–3 min after administration, and the peak time is obviously faster than morphine (5 min vs 30 min).7,24 Previous research recommended that the initial dose of oliceridine is 1.5 mg, with a maximum single dose not to exceed 3 mg due to safety concerns.7,25,26 Hence, the initial dose of oliceridine in this study was set at 1.5 mg and was given 1 min before the injection of propofol. According to the modified Dixon sequential method, our prospective dose-finding study determined that the ED50 and ED95 values of oliceridine compounded with propofol for painless hysteroscopy were 1.583 (1.444–1.857) mg and 1.848 (1.701–4.409) mg, respectively.
Perioperative opioid use was associated with respiratory depression and postoperative nausea and vomiting (PONV), and this may prolong the hospital stays and cost of patients.27,28 Recent studies have observed a higher incidence of opioid-induced respiratory depression (OIRD) and PONV in the sufentanil group during the hysteroscopy.20,29 In this trial, only one patient experienced respiratory depression during the operation and promptly was relieved by mask ventilation, and one patient had nausea and vomiting within 24 h postoperatively. Our results demonstrated that oliceridine compounded with propofol was safe for painless hysteroscopy. The lower incidence of respiratory depression and gastrointestinal adverse events related to oliceridine may be associated with the decrease of β-arrestin recruitment.21 Propofol has an inhibitory effect on the cardiovascular system, and a significant reduction of MAP was observed at T1 (after propofol injection). Although the MAP and RR at the T1 and T2 time points differed significantly compared to T0, their fluctuating values were still within the range of 20% of the baseline. No serious adverse events were reported with oliceridine at any dose during the intraoperative and postoperative periods in this study. Given the circulatory and respiratory stability, it may encourage anesthesiologists to prefer this combination of oliceridine and propofol in hysteroscopy.
Intravenous injection of propofol stimulates blood vessels to release inflammatory mediators such as histamine, causing injection pain and even becoming the most painful memory of patients before operation.30 A previous study has found that oliceridine can effectively reduce injection pain related to propofol.31 However, our research does not include a direct comparison, and future clinical practice could verify this conclusion. Except for one patient whose VAS scores exceeded 3 at 2 h after hysteroscopy, the other patients had VAS scores below 3, suggesting that oliceridine exhibited a potent analgesic efficacy. Furthermore, patients recovered quickly, and more than 80% of patients woke up within 2 min after surgery. Compared with previous studies on the application of nalbuphine,6 sufentanil,20 and esketamine32 in hysteroscopy, oliceridine showed a shorter recovery time from anesthesia. This rapid recovery may be associated with its short elimination half-life, indicating a more accelerated metabolism that makes it difficult to accumulate8. The attributes of efficient analgesia and rapid recovery demonstrated by these results align with the core principles of ERAS, which support the appropriateness of oliceridine for application in hysteroscopy.
Overall, this study estimated the effective dose of oliceridine compounded with propofol for painless hysteroscopy, and our findings supported that oliceridine is a promising choice for anesthesia management in hysteroscopy. However, several limitations of this study should be acknowledged. Firstly, the estimated effective dose of oliceridine compounded with propofol in our study only applies to patients with ASA I–II classification. In terms of proving the safety and applicability of oliceridine in the population, it is essential to investigate the appropriate dose for the elderly (>60 years), patients with obesity (>25 kg/m2), and other health disorders (ASA III–IV). Secondly, the highest dose of oliceridine in this study was 1.8 mg, and no serious adverse events were observed in any patients. Further research is needed to assess the intraoperative and postoperative safety associated with the effective dose of 1.848 mg. Thirdly, the modified Dixon sequential method was commonly used to determine the median and effective dose of drugs based on its simplicity and effectiveness, whereas a small sample size may introduce selection bias. Hence, a multicenter study with large samples is required to increase the generalizability of the results and comprehensively evaluate the safety and efficacy of oliceridine for hysteroscopy.
Conclusion
In summary, a single dose of oliceridine can effectively inhibit cervical dilatation pain while making rapid recovery from anesthesia in patients undergoing hysteroscopy, and the ED50 and ED95 of oliceridine compounded with propofol were 1.583 and 1.848 mg, respectively. These findings will provide a clinical reference for the appropriate anesthesia approach for painless hysteroscopy. Future larger, multicenter studies will help to expand the population range of oliceridine use and explore its potential benefits and risks.
Data Sharing Statement
The data supporting the conclusions of this study are not public but are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Our study was performed in accordance with the Helsinki Declaration and its later amendments. The ethics committee of Zigong Maternal and Child Health Care Hospital approved this study (2024-IRB-017), and all participants signed informed consent forms.
Acknowledgments
We express our gratitude to the patients in this study for their cooperation and contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, acquisition of data, analysis, or in all these areas, and took part in drafting, revising, or critically reviewing the article. All authors have read the final manuscript and agreed to be accountable for all aspects of the work and then approved this version to be published.
Funding
This study was supported by the Bethune Charity Foundation (J202402E055-16).
Disclosure
The authors declare that they have no competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
References
1. Wahba AH, Hassan AM, Kotb M, et al. Impact of uterine scar on pain experienced during outpatient hysteroscopy: a prospective blinded comparative study. J Minim Invasive Gynecol. 2017;24(4):626–631. doi:10.1016/j.jmig.2017.01.018
2. Vitale SG, Caruso S, Ciebiera M, et al. Management of anxiety and pain perception in women undergoing office hysteroscopy: a systematic review. Arch Gynecol Obstet. 2020;301(4):885–894. doi:10.1007/s00404-020-05460-2
3. Zhang S, Wang J, Ran R, et al. Efficacy and safety of remimazolam tosylate in hysteroscopy: a randomized, single-blind, parallel controlled trial. J Clin Pharm Ther. 2022;47(1):55–60. doi:10.1111/jcpt.13525
4. Harrison R, Kuteesa W, Kapila A, et al. Pain-free day surgery? Evaluating pain and pain assessment during hysteroscopy. Br J Anaesth. 2020;125(6):e468–e470. doi:10.1016/j.bja.2020.08.015
5. Xu C, Peng R, Qian X, et al. Modified Dixon sequential method to determine the effective dose of alfentanil compounded with propofol for day-case hysteroscopy. Ther Adv Drug Saf. 2023;14:20420986231214992. doi:10.1177/20420986231214992
6. Zhong W, Chen C, Tang W. Effective doses of nalbuphine combined with propofol in painless hysteroscopy. Int J Gen Med. 2022;15:5609–5614. doi:10.2147/IJGM.S367449
7. Markham A. Oliceridine: first approval. Drugs. 2020;80(16):1739–1744. doi:10.1007/s40265-020-01414-9
8. Simons P, van der Schrier R, van Lemmen M, et al. Respiratory effects of biased ligand oliceridine in older volunteers: a pharmacokinetic-pharmacodynamic comparison with morphine. Anesthesiology. 2023;138(3):249–263. doi:10.1097/ALN.0000000000004473
9. Niu J, Hu W, Lu Y, et al. Efficacy and safety of oliceridine treatment in patients with postoperative pain: a systematic review and meta-analysis of randomized controlled trials. Expert Rev Clin Pharmacol. 2023;16(6):589–599. doi:10.1080/17512433.2023.2213889
10. Ni Y, Huang R, Yang S, et al. Pharmacokinetics and safety of oliceridine fumarate injection in Chinese patients with chronic non-cancer pain: a phase i, single-ascending-dose, open-label clinical trial. Drug Des Devel Ther. 2024;18:2729–2743. doi:10.2147/DDDT.S461416
11. Daksla N, Wang A, Jin Z, et al. Oliceridine for the management of moderate to severe acute postoperative pain: a narrative review. Drug Des Devel Ther. 2023;17:875–886. doi:10.2147/DDDT.S372612
12. Qiu L, Cao L, Lang Z, et al. Preoperative sedation in children with congenital heart disease: 50% and 95% effective doses, hemodynamic effects, and safety of intranasal dexmedetomidine. J Clin Anesth. 2022;81:110908. doi:10.1016/j.jclinane.2022.110908
13. Oh J, Kim DH, Choi G, et al. The influence of sex on the dosage of remimazolam co-administered with remifentanil for loss of consciousness in adult patients: an up-and-down sequential allocation trial. BMC Anesthesiol. 2024;24(1):292. doi:10.1186/s12871-024-02675-7
14. Pastis NJ, Hill NT, Yarmus LB, et al. Correlation of vital signs and depth of sedation by modified observer’s assessment of alertness and sedation (MOAA/S) scale in bronchoscopy. J Bronchology Interv Pulmonol. 2022;29(1):54–61. doi:10.1097/LBR.0000000000000784
15. Vitale SG, Alonso Pacheco L, Haimovich S, et al. Pain management for in-office hysteroscopy. A practical decalogue for the operator. J Gynecol Obstet Hum Reprod. 2021;50(1):101976. doi:10.1016/j.jogoh.2020.101976
16. Jansen FW, Vredevoogd CB, van Ulzen K, et al. Complications of hysteroscopy: a prospective, multicenter study. Obstet Gynecol. 2000;96(2):266–270. doi:10.1016/s0029-7844(00)00865-6
17. Guraslan H, Senturk MB, Dogan K, et al. Diagnostic office hysteroscopy; why is it still painful procedure despite the surgical experience and mini-hysteroscope? J Obstet Gynaecol Res. 2022;48(6):1418–1425. doi:10.1111/jog.15219
18. Soysal C, Ince O, Taşçı Y. The effect of cervical length on procedure time and VAS pain score in office hysteroscopy. Sci Rep. 2025;15(1):1975. doi:10.1038/s41598-025-85185-x
19. Irwin MG, Chung CKE, Ip KY, et al. Influence of propofol-based total intravenous anaesthesia on peri-operative outcome measures: a narrative review. Anaesthesia. 2020;75(Suppl 1):e90–e100. doi:10.1111/anae.14905
20. Lei X, Zhang T, Huang X. Comparison of a single intravenous infusion of alfentanil or sufentanil combined with target-controlled infusion of propofol for daytime hysteroscopy: a randomized clinical trial. Ther Adv Drug Saf. 2024;15:20420986241292231. doi:10.1177/20420986241292231
21. DeWire SM, Yamashita DS, Rominger DH, et al. A G protein-biased ligand at the μ-opioid receptor is potently analgesic with reduced gastrointestinal and respiratory dysfunction compared with morphine. J Pharmacol Exp Ther. 2013;344(3):708–717. doi:10.1124/jpet.112.201616
22. Kaye AD, Edinoff AN, Babin KC, et al. Pharmacological advances in opioid therapy: a review of the role of oliceridine in pain management. Pain Ther. 2021;10(2):1003–1012. doi:10.1007/s40122-021-00313-5
23. Ma B, Li Y, Leng C, et al. A comparative evaluation of the safety and efficacy of oliceridine and sufentanil in gastrointestinal endoscopy: a single-center, randomized controlled trial. Drug Des Devel Ther. 2025;19:5111–5121. doi:10.2147/DDDT.S512529
24. Viscusi ER, Webster L, Kuss M, et al. A randomized, Phase 2 study investigating TRV130, a biased ligand of the μ-opioid receptor, for the intravenous treatment of acute pain. Pain. 2016;157(1):264–272. doi:10.1097/j.pain.0000000000000363
25. Viscusi ER, Skobieranda F, Soergel DG, et al. APOLLO-1: a randomized placebo and active-controlled Phase III study investigating oliceridine (TRV130), a G protein-biased ligand at the µ-opioid receptor, for management of moderate-to-severe acute pain following bunionectomy. J Pain Res. 2019;12:927–943. doi:10.2147/JPR.S171013
26. Singla NK, Skobieranda F, Soergel DG, et al. APOLLO-2: a randomized, placebo and active-controlled phase III study investigating oliceridine (TRV130), a G Protein-biased ligand at the μ-Opioid receptor, for management of moderate to severe acute pain following abdominoplasty. Pain Pract. 2019;19(7):715–731. doi:10.1111/papr.12801
27. Shanthanna H, Ladha KS, Kehlet H, et al. Perioperative Opioid Administration. Anesthesiology. 2021;134(4):645–659. doi:10.1097/ALN.0000000000003572
28. Cummings Joyner AK, King MR, Safranek C, et al. Health care burden associated with adolescent prolonged opioid use after surgery. Anesth Analg. 2023;136(2):317–326. doi:10.1213/ANE.0000000000006111
29. Cha NH, Hu Y, Zhu GH, et al. Opioid-free anesthesia with lidocaine for improved postoperative recovery in hysteroscopy: a randomized controlled trial. BMC Anesthesiol. 2023;23(1):192. doi:10.1186/s12871-023-02152-7
30. Jalota L, Kalira V, George E, et al. Prevention of pain on injection of propofol: systematic review and meta-analysis. BMJ. 2011;342:d1110. doi:10.1136/bmj.d1110
31. Zhang B, Zhang W, Jia J, et al. Median effective dose of oliceridine combined with propofol for analgesia during induced abortion in patients with different labor histories. Chin J Anesthesiol. 2024;44(12):1437–1440. doi:10.3760/cma.j.cn131073.20240919.01207
32. Sheng Z, Liu X, Lin K, et al. Determining the effective dose of esketamine combined with propofol for painless hysteroscopy: a prospective dose-finding study. Front Pharmacol. 2024;15:1419732. doi:10.3389/fphar.2024.1419732
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effective Doses of Nalbuphine Combined with Propofol in Painless Hysteroscopy
Zhong W, Chen C, Tang W
International Journal of General Medicine 2022, 15:5609-5614
Published Date: 11 June 2022
RETRACTED ARTICLE: Effective Doses of Oliceridine Combined with Propofol for Painless Hysteroscopy: A Prospective Dose-Finding Study
Gao L, Tan A, Wang Z, Wei L, Wang X
International Journal of General Medicine 2025, 18:2651-2657
Published Date: 21 May 2025
Chloroprocaine ED50 and ED95 for Propofol Injection Pain Prevention: Dixon’s Sequential Method
Lai P, Yang X, Yang X, Xuan Q, Fang Y, He Z, Chen B, Yin G
Journal of Pain Research 2025, 18:6699-6709
Published Date: 10 December 2025
Effective Dose of Oliceridine for Inhibiting Hemodynamic Elevation Induced by Tracheal Intubation: An Up-and-Down Sequential Trial
Yu J, Wei S, Ling D, Xin Y, Liu H, Yang Y, Li X, Xiang Z, Liu J
Drug Design, Development and Therapy 2025, 19:11767-11778
Published Date: 26 December 2025