Back to Journals » Journal of Pain Research » Volume 18
Chloroprocaine ED50 and ED95 for Propofol Injection Pain Prevention: Dixon’s Sequential Method
Authors Lai P, Yang X, Yang X, Xuan Q, Fang Y, He Z, Chen B, Yin G
Received 11 July 2025
Accepted for publication 26 November 2025
Published 10 December 2025 Volume 2025:18 Pages 6699—6709
DOI https://doi.org/10.2147/JPR.S553084
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Pengchong Lai,1,* Xiyang Yang,2,* Xuemei Yang,3 Qinghang Xuan,3 Yanwei Fang,3 Zhijiao He,3 Bingjun Chen,3 Guangfen Yin3
1Section One, Department of Anesthesiology, Gaozhou People’s Hospital, Gaozhou, Guangdong Province, 525200, People’s Republic of China; 2Shanghai Institute of Cardiovascular Diseases, Department of Cardiology, Zhongshan Hospital, Fudan University, Shanghai, 200032, People’s Republic of China; 3Department of Anesthesiology, The First Affiliated Hospital of Dali University, Dali, Yunnan Province, 671000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guangfen Yin, Department of Anesthesiology, The First Affiliated Hospital of Dali University, No. 32 of Jiashibo Street, Xiaguan Town, Dali, Yunnan Province, 671000, People’s Republic of China, Tel +860872 2201147, Fax +860872 2201081, Email [email protected]
Objective: This study aimed to estimate the median effective dose (ED50) and the 95% effective dose (ED95) of intravenous chloroprocaine (CP), administered pre-emptively for the prevention of propofol-induced injection pain, using Dixon’s up-and-down sequential allocation method, and to characterize the associated dose–response relationship.
Methods: First, apply a pressure bandage to the elbow of the patient’s arm where the peripheral vein is accessible. Then, administer clonprocaine via intravenous injection into the dorsal hand vein while maintaining local pressure from the bandage to block venous return at the elbow for 30 seconds. The initial clonprocaine dose is set at 30mg with 1mg increments. If no injection pain occurs (negative response), reduce the dose by one step for the next patient until pain develops. If pain occurs (positive response), increase the dose by one step until pain subsides. The trial terminates when seven negative and positive responses are recorded, halting case enrollment. Using Probit probability regression analysis, calculate the median effective dose (ED50) and 95% effective dose (ED95) of clonprocaine for preventing propofol injection pain, along with corresponding 95% confidence intervals (CI).
Results: A total of 35 patients completed the study. Of these, 27 reported no pain upon injection, while 8 experienced pain. Probit analysis yielded an ED50 of 11.554 mg (95% CI: 10.096– 12.740 mg) and an ED95 of 13.085 mg (95% CI: 12.240– 24.151 mg). No vasoactive pharmacologic support was required, and no adverse events related to local anesthetic toxicity were observed.
Conclusion: Intravenous CP, administered at doses of 11.554 mg and 13.085 mg, achieved 50% and 95% efficacy, respectively, in preventing pain associated with propofol injection. These doses were associated with effective attenuation of nociceptive responses, reduced propofol requirements, absence of significant adverse effects, and preservation of hemodynamic stability, thereby supporting the use of CP in enhancing patient comfort during anesthetic induction.
Keywords: chloroprocaine, ED50, ED95, propofol injection pain, sequential method
Introduction
Propofol was introduced into clinical practice in China in 1994 and has since become the most widely used intravenous general anesthetic globally. Its widespread adoption is attributed to its potent sedative-hypnotic properties, rapid onset and recovery profile, and relatively low incidence of postoperative nausea and vomiting.1,2 Clinical studies have reported that propofol-induced injection site pain occurs in approximately 28–90% of adults and 28–85% of pediatric patients.3 As such, effective strategies to prevent or attenuate this pain are essential for improving patient comfort and satisfaction during anesthetic care. At present, various physical techniques and pharmacological interventions have demonstrated differing degrees of efficacy in reducing propofol-induced injection site pain. However, physical intervention measures such as changing to a thinner intravenous injection needle or applying ice to reduce temperature cannot fundamentally block the pain pathway.4 However, the use of drugs such as lidocaine can lead to adverse reactions such as laryngeal spasm, awakening period agitation, gastrointestinal ulcers, pulmonary embolism, delayed effects, tinnitus and dizziness, etc, and it has not consistently achieved complete pain relief.5,6
Chloroprocaine (CP) is a short-acting ester-type local anesthetic and membrane stabilizer, and is widely utilized for neuraxial anesthesia, peripheral nerve blocks, and local infiltration.7 It can exert regional blockage through local blood vessels, change the pH value of propofol, reduce the aqueous phase concentration, and alter the osmotic pressure characteristics to reduce the irritation to the vascular wall. This mechanism temporarily blocks the generation and transmission of pain signals on nerve fibers.4,8,9 Meanwhile, CP binds to the nociceptor receptors located in the vascular endothelium, inhibits voltage-gated sodium channels, reduces sodium influx and potassium efflux, suppresses nerve conduction, stabilizes the nerve cell membrane, and reduces intracellular biochemical reactions. These effects contribute to central analgesia and sedation, and work synergistically with propofol to reduce the required dose of propofol.9 Evidence from studies conducted in China has indicated that pre-emptive intravenous administration of chloroprocaine (CP) may reduce the incidence of propofol injection pain.8,9
CP is metabolized in the body into p-aminobenzoic acid. Excessive use may lead to systemic toxicity, affecting the central nervous system and cardiovascular system.7 Therefore, determining an appropriate CP dose that effectively prevents propofol-induced injection site pain, while minimizing adverse reactions and maintaining hemodynamic stability, remains clinically important. The present investigation expanded upon previous dose-finding research by utilizing Dixon’s up-and-down sequential method to determine the median effective dose (ED50) and 95% effective dose (ED95) of pre-emptively administered CP. The objectives included quantification of the dose-response relationship, evaluation of the preventive efficacy at each dose level, and assessment of perioperative vital signs, and adverse event incidence. These findings were intended to support safer and more evidence-based use of CP in clinical anesthesia practice.
Participants
This study was approved by the Ethics Committee of the First Affiliated Hospital of Dali University. Patients scheduled to undergo tracheal intubation under total intravenous anesthesia between January and September 2023 were recruited.
Inclusion and Exclusion Criteria
Inclusion Criteria
Exclusion Criteria
Methods
Anesthetic Management
Eligible patients were enrolled in a sequential manner. All enrolled patients underwent a preoperative evaluation one day prior to surgery, during which the potential of transient injection site pain associated with propofol administration was discussed. Preoperative fasting protocols were followed, with an eight-hour fasting period for solids and a six-hour abstinence from liquids.
Upon arrival in the operating theatre, patients were placed in the supine position. A 20-gauge intravenous cannula was inserted into a dorsal hand vein for the infusion of compound sodium chloride solution, and a three-way stopcock was connected to facilitate drug administration. Standard monitoring was initiated, comprising non-invasive blood pressure, pulse oxygen saturation (SpO2), electrocardiogram (ECG), systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), heart rate (HR), respiratory rate (RR), end-tidal carbon dioxide (PETCO2), and bispectral index (BIS).
CP was prepared by diluting a 3% stock solution with normal saline to achieve a 1% concentration. The required dose was drawn into a 3-mL syringe prior to induction anesthesia. A tourniquet was applied to the upper arm proximal to the site of venous cannulation to occlude venous return. The predetermined dose of 1% CP was administered via the dorsal hand vein, and the tourniquet was maintained for 30 seconds prior to release.
Subsequently, 1% propofol at a dose of 2 mg/kg was administered at a rate of 0.5 mL/s. Injection site pain was assessed every five seconds until loss of consciousness, defined by the absence of the eyelash reflex; the final verbal or physical response prior to loss of consciousness was recorded. Pain intensity was assessed using the four-point McCrirrick scale.10
Following the onset of unconsciousness, sufentanil at 0.4 μg/kg and rocuronium at 0.6 mg/kg were administered to complete anesthetic induction.
Based on Dixon’s up-and-down sequential allocation method and informed by prior literature, the initial dose of 1% CP was set at 30 mg, with dose adjustments made in 1 mg increments. During induction with propofol, the absence of injection site pain was recorded as a negative response, resulting in a 1 mg dose reduction for the next patient. Conversely, the presence of pain was classified as a positive response, prompting a 1 mg dose increase for the next patient. The study was concluded upon attainment of seven negative-positive crossover points (Figure 1).
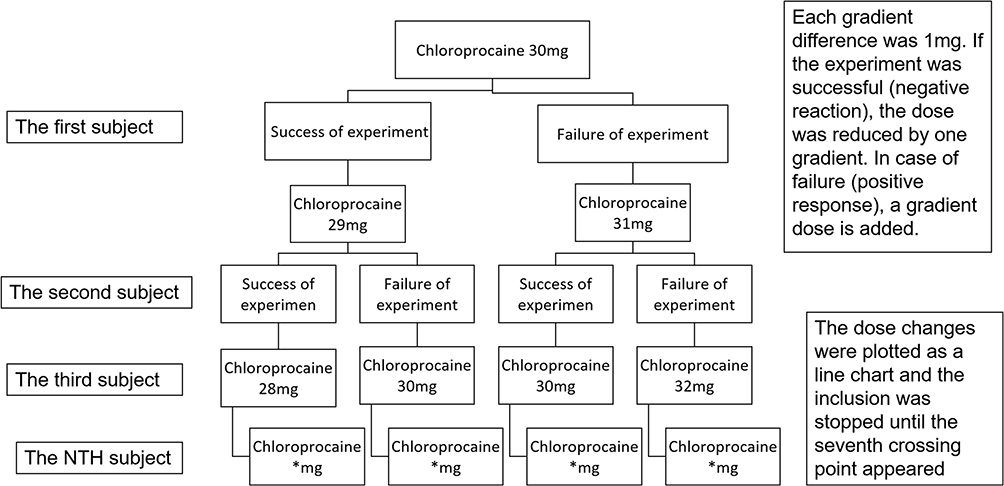 |
Figure 1 Experimental flow diagram of Dixon sequential method. |
Outcome Measures
Baseline characteristics included age, sex, height, weight, body mass index, American Society of Anesthesiologists (ASA) physical status classification, and BIS values. Recorded variables included comprised the administered dose of CP; the presence of adverse events within 30 seconds following CP injection such as pruritus, erythema, or blistering at the injection site, dizziness, tinnitus, perioral numbness, transient loss of consciousness, or convulsions; the predicted induction dose of 1% propofol (2 mg/kg); and the actual dose of 1% propofol required to achieve loss of the eyelash reflex.
Hemodynamic parameters including MAP and HR were documented at baseline (prior to CP injection, T0) and 30 seconds post-injection (T1). Additional outcomes included the requirement for vasoactive drugs during anesthetic induction, grading of propofol injection pain using the McCrirrick four-point pain scale (Table 1), and the number of effective and ineffective responses at each CP dose level.
 |
Table 1 McCrirrick Grade 4 Pain Rating Scale |
The primary calculated outcomes were the ED50, ED95, and their respective 95% confidence intervals for the prevention of propofol-induced injection site pain.
Pain Assessment
Pain intensity associated with propofol injection was evaluated using the four-point McCrirrick scale. The grading criteria and corresponding clinical manifestations are presented in Table 1.
Statistical Analysis
Data analysis was conducted using SPSS version 26.0. The Shapiro–Wilk test was applied to assess the normality of continuous variables. Data with a normal distribution were reported as mean ± standard deviation, while non-normally distributed data were expressed as median (interquartile range) and compared using the Wilcoxon signed-rank test. Categorical variables were compared using the chi-squared (χ2) test. A two-sided p value of less than 0.05 was considered statistically significant.
The ED50, ED95, and their respective 95% confidence intervals were estimated using Probit regression analysis. Sequential allocation data and dose-response curves were generated using GraphPad Prism version 8.
Results
Baseline Characteristics
Based on seven sets of negative-positive crossover results from the Dixon sequential method trial, 35 patients scheduled for elective tracheal intubation under general anesthesia were enrolled in the study. All patients were ASA II grade, with an average age of (45.1±2.5) years, average height of (167.4±5.1) cm, average weight of (64.9±2.4) kg, average BMI of (23.2±1.4) kg/m2, and average BIS of (92.6±1.8). Statistical analysis showed that the general data followed normal distribution, with all P-values>0.05, indicating no statistically significant differences.
Effective Doses
The flow of the sequential dosing trial is presented in Figure 2. Probit regression analysis estimated the ED50 of CP for preventing propofol-induced injection pain at 11.554 mg (95% CI: 10.096–12.740 mg), and the ED95 at 13.085 mg (95% CI: 12.240–24.151 mg) (Figure 3).
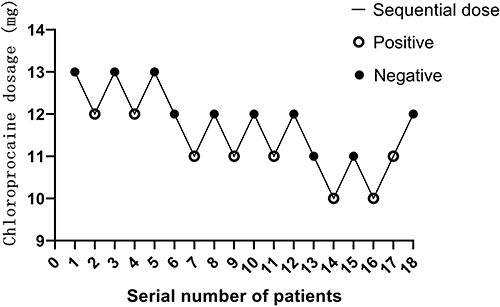 |
Figure 2 Sequential test of chloroprocaine doses. |
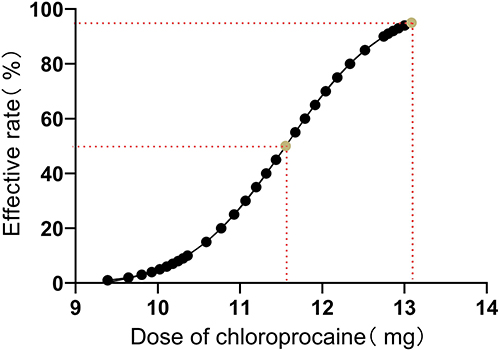 |
Figure 3 Fitting curve of the dose effect of chloroprocaine and propofol intravenous injection. |
Hemodynamic Changes
Assessment of MAP before and after CP administration revealed that MAP data did not follow a normal distribution (p = 0.021 < 0.05), and were therefore analyzed using the paired Wilcoxon signed-rank test. The results indicated a statistically significant reduction in MAP (z = −5.169, p = 0.000 (p < 0.05), with the median of paired differences differing significantly from zero. Although MAP decreased following CP administration, no patient exhibited MAP values below 60 mmHg, and the magnitude of reduction did not exceed 30% of baseline. No vasoactive drugs were required, indicating that the decrease in MAP observed 30 seconds after CP injection did not result in clinically significant hemodynamic instability or hypotension (Table 2).
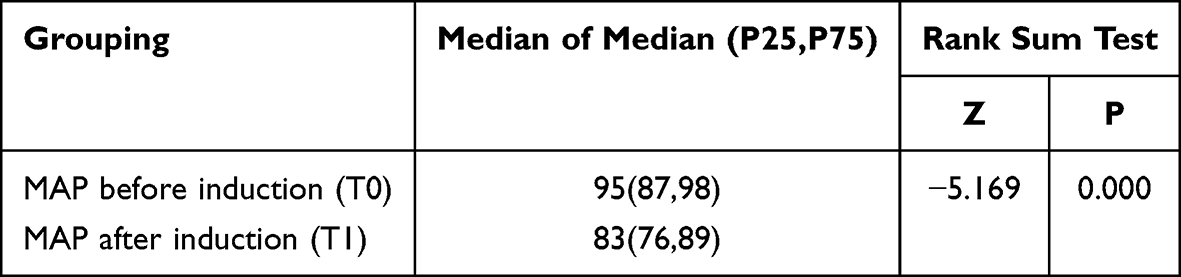 |
Table 2 Mean Pressure (MAP) Changes in the 30s Before and After Induction with Chloroprocaine in Patients (n=35) |
HR data satisfied assumptions of normal distribution (p = 0.318 > 0.05) and were evaluated using a paired t-test. The mean HR increased from 76.14 ± 2.18 beats per minute to 81.23 ± 2.03 beats per minute. The mean difference was −5.09 beats per minute (95% CI: −8.25 to −1.92), with statistical significance (p = 0.003 < 0.05) (Table 3). The increase in HR following CP administration was modest and remained within clinically acceptable limits.
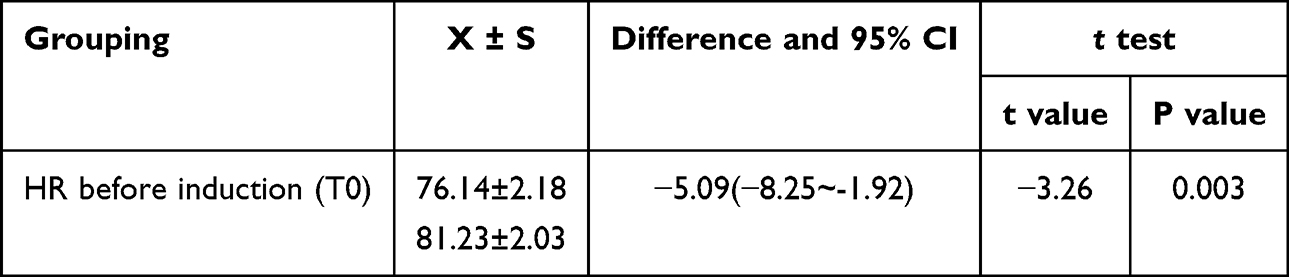 |
Table 3 Heart Rate (HR) Changes in Patients Before and After Induction with Chloroprocaine for 30s (n=35) |
Incidence of Propofol Injection Pain by CP Dose
Among the 35 patients included in the study, 27 did not report injection site pain following propofol administration, corresponding to a pain prevention success rate of 77.14%. The remaining 8 patients experienced pain, yielding an incidence rate of 22.86% (Figure 4). Among those reporting pain, CP doses ranged primarily between 10 and 12 mg. According to the McCrirrick pain scale, six patients reported grade 1 pain and two reported grade 2 pain. The observed distribution indicated a nonlinear, inverse dose-response relationship, wherein higher CP doses were associated with both a reduced incidence and diminished severity of propofol-induced injection site pain (Table 4).
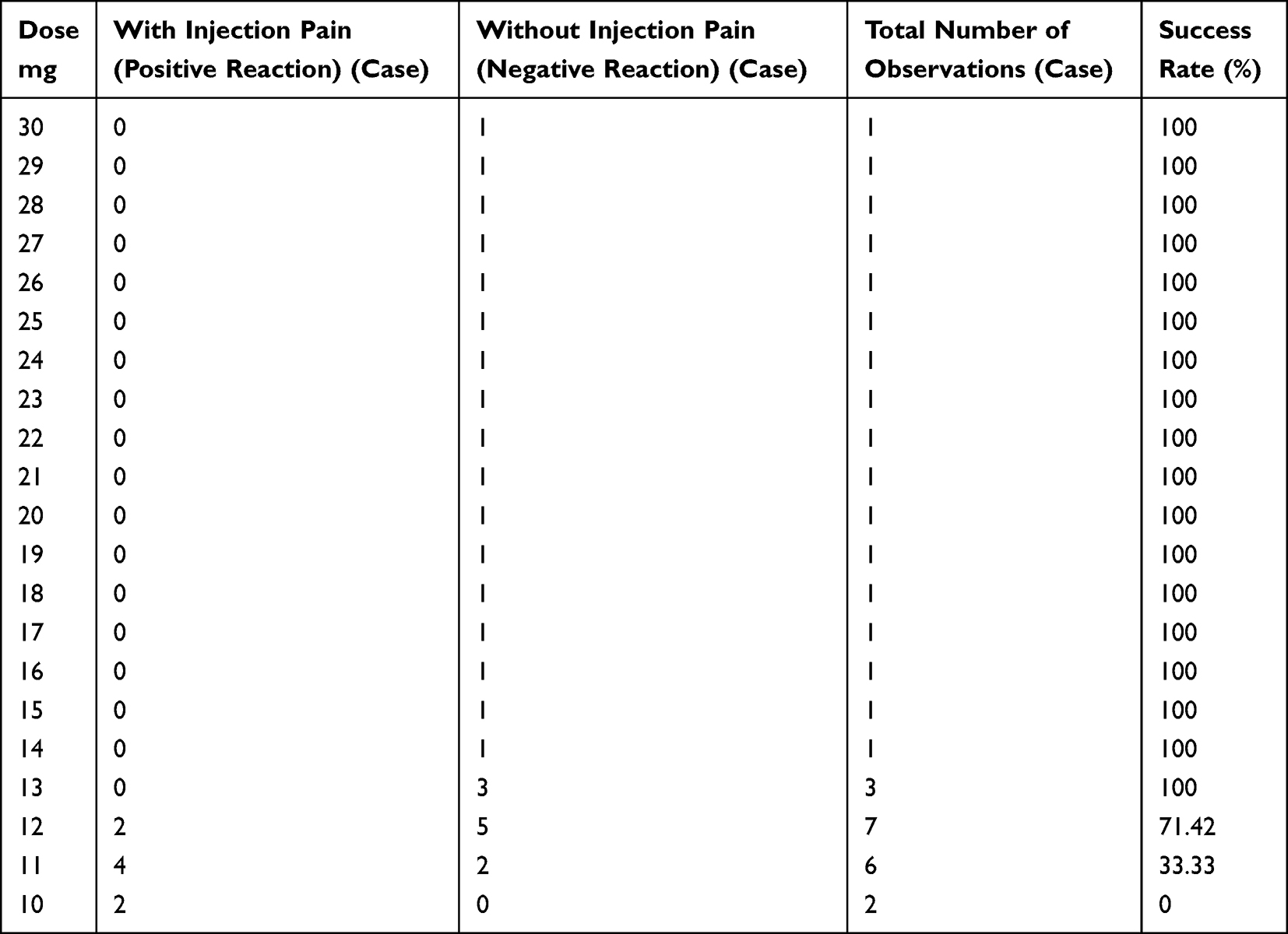 |
Table 4 Success Rates of Different Doses of Chloroprocaine for Prevention of Intravenous Propofol Pain (n=35) |
 |
Figure 4 Proportion of propofol injection pain in all patients. |
Predicted versus Actual Propofol Induction Doses
Both the predicted dose of 1% propofol (2 mg/kg) and the actual dose required to achieve loss of the eyelash reflex demonstrated normal distribution (predicted 1% propofol, p = 0.117 > 0.05; actual 1% propofol, p = 0.063 > 0.05). No statistically significant differences were observed in the actual induction doses across different CP dose groups (Table 5).
 |
Table 5 Analysis of 1% Propofol Dose |
However, the distribution of paired differences between predicted and actual doses was non-normal, necessitating analysis using the Wilcoxon signed-rank test. The results demonstrated a statistically significant reduction in the actual dose compared to the predicted 2 mg/kg dose (z = −5.182, p = 0.000 (p < 0.05)), indicating that pre-emptive administration of CP reduced the total propofol requirement for induction (Table 6).
 |
Table 6 Comparison of Induction Doses of 1% Propofol |
Adverse Events
No patients experienced signs of pruritus, erythema, blistering at the injection site, dizziness, tinnitus, perioral numbness, transient loss of consciousness, convulsions, or other adverse reactions following CP administration.
Discussion
Pain is defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage. In 1995, the American Pain Society advocated for the recognition of pain as the “fifth vital sign,” alongside respiration, pulse, temperature, and blood pressure.11 Accordingly, the provision of pain-free and comfortable care constitutes a fundamental medical obligation. The prevention and management of pain remain key priorities in perioperative care, particularly within the scope of anesthetic practice.
Anesthetic induction has been regarded as one of the most distressing phases of the perioperative period, primarily due to the intravenous administration of hypnotic agents, many of which are associated with injection site pain. Propofol remains the most commonly utilized intravenous hypnotic agent, attributed to its rapid onset, smooth induction profile, swift recovery, and low incidence of postoperative nausea and vomiting. However, its phenolic structure and lipid emulsion formulation have been shown to irritate the vascular endothelium,12 often resulting in a burning sensation during administration.2
Chinese researchers have evaluated the efficacy of CP in preventing propofol-induced injection site pain. In one study, Hongwu et al administered CP at doses of 30 mg, 60 mg, and 90 mg prior to 1% propofol injection and compared the outcomes with a control group.8 In the 90 mg group, venous return was additionally occluded at the elbow for 30 seconds. Visual analogue scale scores demonstrated that the combination of 90 mg CP with venous occlusion reduced the incidence of injection pain by approximately two-thirds compared to the control group and by approximately half compared to the 30 mg and 60 mg groups, along with a decrease in pain intensity. In a separate study, Guozhong et al mixed CP directly with propofol and reported that a 90 mg dose reduced the incidence of pain by 14% compared to a 60 mg dose.13
Chinese researchers including Fu Runqiao14 have conducted comparative studies on the analgesic efficacy of clonprocaine versus lidocaine in propofol injections. In their experimental protocol, participants received 4mL of either 2% clonprocaine, 4mL of 2% lidocaine, or 4mL of saline solution intravenously. Thirty seconds later, 2 mg/kg of propofol was administered intravenously. Results demonstrated that the clonprocaine group achieved a 92.7% incidence rate of no injection pain, significantly higher than the 60.0% in the lidocaine group and 43.6% in the control group. Pain intensity was notably milder in the clonprocaine group compared to both lidocaine and control groups. Furthermore, adverse reaction rates were substantially lower in the clonprocaine group. These findings conclusively indicate that pre-injection clonprocaine provides superior analgesic efficacy against propofol-induced pain compared to lidocaine and saline controls.
These findings supported the existence of an inverse, dose-dependent relationship between CP dosage and the incidence of propofol injection pain.
CP is an ester-type local anesthetic characterized by rapid onset, quick diffusion, and a favorable safety profile.15,16 It has been widely used in clinical practice for epidural anesthesia, local infiltration, and peripheral nerve blocks,7,16 and is particularly employed for postoperative intrathecal analgesia following caesarean delivery17 and for the management of breakthrough pain during labor.15 However, documentation of its use in intravenous regional anesthesia remains limited.
Mechanistically, CP, similar to other local anesthetics, binds to specific sites on the α-subunit of voltage-gated sodium channels. This interaction decreases sodium membrane permeability, blocks sodium influx and potassium efflux, and inhibits neuronal signal conduction, and resulting in reversible nerve blockade. By stabilizing the neuronal membrane, CP also reduces intracellular metabolic activity, elevates the excitation threshold, and slows the propagation of nerve impulses, thereby attenuating nociceptive signaling during propofol injection.16
Based on previously reported dosing regimens, the present study investigated and determined the ED50 and ED95 of pre-emptively administered intravenous CP for the prevention of propofol-induced injection site pain. Concurrently, dose-response relationships for relevant clinical parameters were evaluated within the framework of a sequential allocation trial. These findings contribute to addressing the current paucity of clinical data regarding intravenous CP use and support its safe and rational application in anesthetic practice.
In clinical pharmacology, the ED50 refers to the dose required to achieve the intended therapeutic effect in 50% of a population and serves as a key quantitative parameter for drug development, therapeutic decision-making, and safety evaluation. The up-and-down sequential allocation method, introduced by W.J. Dixon and subsequently refined by K. Brownlee, has been widely adopted for ED50 estimation due to its methodological simplicity, cost-effectiveness, and efficiency.18,19
This method typically begins with an initial dose approximating the anticipated ED50. Subsequent doses are adjusted upward or downward in fixed increments, typically following a 1:1 ratio, based on the response of the preceding participant. Sample sizes generally range between 20 and 40 participants. The protocol is usually terminated after achieving a predefined number of response crossovers, most frequently seven, between successive dose increases and decreases. This approach enables precise estimation of ED50 while minimizing sample size and reducing participant exposure.20,21
As most administered doses tend to cluster near the true ED50, the up-and-down sequential method allows for efficient dose estimation while minimizing participant exposure and conserving resources without compromising precision. Upon completion of data collection, ED50 may be estimated using either the average of crossover doses (“turning-point” method) or binary regression models such as logistic or probit analysis. In the present investigation, probit analysis was used to estimate both ED50 and ED95.
Consistent with prior studies, a 1% CP solution was administered at an initial dose of 30 mg, corresponding to the lowest dose previously reported in the literature. The dose increment was set at 1 mg. A negative response, defined as the absence of propofol-induced injection site pain, resulted in a 1 mg reduction for the subsequent participant. Conversely, a positive response, indicating the presence of pain, prompted a 1 mg dose increase. Participant recruitment was discontinued after seven negative-positive crossover points were recorded, in alignment with the established stopping criteria for Dixon’s method.
Within the sequential trial, the initial 18 patients reported no injection site pain following administration of their assigned 1% CP doses. The first positive response, indicative of pain was observed in the nineteenth patient, who had received 12 mg of 1% CP, thereby establishing the initial negative-positive crossover. The seventh crossover occurred between patient 32, who received 11 mg (negative response), and patient 33, who received 10 mg (positive response). Data-collection concluded with patient 35, who received 12 mg of 1% C and reported no pain. The final sample size of 35 fell within the commonly recommended range of 20 to 40 participants for Dixon’s up-and-down sequential method.
Probit regression analysis estimated the ED50 of CP for the prevention of propofol-induced injection site pain at 11.554 mg (95% CI: 10.096–12.740 mg) and the ED95 at 13.085 mg (95% CI: 12.240–24.151 mg). Among the 35 patients, 27 (77.14%) experienced no pain and were classified as McCrirrick grade 0. Of the eight patients who reported pain, two received 10 mg of 1% CP and exhibited spontaneous discomfort accompanied by minor movement prior to prompting; both were graded as level 2. The remaining six acknowledged mild pain only upon questioning and demonstrated no observable motor response during 1% propofol administration; all were graded as level 1. These findings supported a dose-dependent relationship between CP and the reduction of propofol injection pain, consistent with previous reports indicating increased analgesic efficacy at higher CP doses.13
Hemodynamic assessment demonstrated a mild reduction in MAP and a slight increase in HR within 30 seconds following CP administration, both of which were statistically significant (p < 0.05). However, no MAP values decreased below 60 mmHg, no reductions exceeded 30% of baseline values, and administration of vasoactive agents was not required. Additionally, none of the 35 patients exhibited signs of local anesthetic toxicity, including pruritus, erythema, blistering, dizziness, tinnitus, perioral numbness, transient loss of consciousness, convulsions, or other adverse manifestations.16 While procaine, as a local anesthetic, may exert some suppression on the central nervous system and cardiovascular circulation, the experimental protocols employed low-dose induction with minimal toxicity.16 This ensured stable hemodynamic parameters and prevented theoretical adverse reactions, maintaining overall stability. Therefore, this dosage of procaine effectively prevents pain during propofol intravenous administration while ensuring steady vital signs throughout the induction phase.
Comparison of the actual induction dose of 1% propofol with the predicted dose of 2 mg/kg following CP administration revealed a statistically significant difference (p < 0.05), indicating that pre-emptive intravenous CP reduced the amount of propofol required to achieve loss of consciousness. This finding suggests a potential synergistic interaction, whereby CP may have enhanced the central sedative effects of propofol, contributing to dose reduction. As a result, this interaction may have supported more stable hemodynamic parameters during anesthetic induction.
However, this experimental study still has certain limitations. First, previous literature did not provide dose calculations of clonpropanolol for intravenous administration per kilogram of body weight. Therefore, all participants in this study had a weight range of 60–70 kg. Although statistical analysis showed P>0.05, indicating no statistically significant differences in body weight data among subjects (which justified the study), the calculated ED50 and ED95 values may only be applicable to this specific weight range. Second, age was not stratified as a factor in the study. Although only patients aged 40–50 years were included (with P>0.05 showing no statistically significant age differences), the results may not be generalizable to other age groups. Particularly, the appropriate dosing of clonpropanolol for elderly patients with pain sensitivity or children with heightened pain perception requires further investigation through larger-scale studies across multiple centers. Additionally, gender was not considered in this experiment. Although studies have reported significant differences in pain perception between individuals of the same age but different genders,22 more research is needed to explore the incidence of pain following propofol intravenous injection in patients of different genders. Furthermore, the use of the MCCRIRCK 4-level pain rating scale to assess 1% propofol intravenous injection pain may introduce subjectivity. Traditional methods like using a pressure band to block peripheral veins2 might also interfere with pain perception, necessitating more objective evaluation criteria. Furthermore, this experiment calculated both the median effective dose (ED50) and 95% effective dose (ED95). However, according to relevant literature, for values like ED95 or even ED99 at the extremes of the dose-response curve, Gorges et al recommended using the biased coin method and continuous reassessment method21 for greater accuracy. Due to the biased coin design requiring larger sample sizes and more complex operations, this experiment did not adopt these methods. The ED95 value obtained is a systemically calculated estimate, and its accuracy warrants further evaluation. Finally, the study only included 35 cases, and the failure to report adverse events may be attributed to the relatively small sample size. The safety of clonpropanol has not yet been discussed, and we anticipate further improvements and refinements in future research.
Conclusion
In adults aged 40 to 50 years with body weight between 60 to 70 kg, the ED50 of CP for the prevention of propofol-induced injection site pain was 11.554 mg, and the ED95 was 13.085 mg. At these doses, CP effectively alleviated injection pain, reduced propofol dosage, and maintained hemodynamic stability without adverse events during anesthesia induction. These findings support the use of CP as a clinically valuable agent for enhancing perioperative comfort and offer evidence-based guidance for its safe and rational application in anesthesia practice.
Abbreviations
ED50, The Median Effective Dose; ED95, 95% Effective Dose; 95% CI, 95% Confidence Interval; CP, ChloroProcaine; PIP, Pain from intravenous ProPofol; HR, Heart Rate; MAP, Mean arterial Pressure; SPO2, Pulse oxygen saturation; ECG, Electrocardiogram; ASA, American Society of Anesthesiologists; BMI, Body Mass Index; BIS, BisPectral Index.
Ethics Approval and Consent to Participate
The investigation was sanctioned by the the Ethics Committee of the First Affiliated Hospital of Dali University (Approval No. DYF20221215001). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all patients.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Funding
No external funding received to conduct this study.
Disclosure
The authors declare that they have no competing interests.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
References
1. Tan M, Zhang C, Zeng W, Chen M, Huang Z, Huang D. Determining the effective dose of esketamine for mitigating pain during propofol injection by Dixon’s uP-and-down method: a double-blind, prospective clinical study of drug dose response. BMC Anesthesiol. 2022;22(1):368. doi:10.1186/s12871-022-01914-z
2. Gao H, Tan J. Research progress on the mechanism of propofol injection pain and its preventive drugs. China Med. 2022;17(02):312–315.
3. Ji L, Sun W, Lan Y, et al. Dexmedetomidine for prevention of propofol injection pain upon induction of anesthesia: a meta-analysis. Eur J Clin Pharmacol. 2020;76(8):1103–1110. doi:10.1007/s00228-020-02889-x
4. Ying L, Hongfei X, Xiaoli N, et al. Research progress on propofol injection pain and its prevention. China J Pain Med. 2018;24(09):685–688.
5. Xu C, Wei X, Zhang C, et al. Esketamine prevents propofol-induced injection pain: randomized controlled trial. Front Pharmacol. 2022;13:991559. doi:10.3389/fphar.2022.991559
6. Xuehai G, Ziyin J, Xiaofang G, et al. Efficacy of pre-treatment with remimazolam on prevention of propofol-induced injection pain in patients undergoing abortion or curettage: a prospective, double-blinded, randomized and placebo-controlled clinical trial. Drug Des Devel Ther. 2021;15.
7. Li K, Gu Y, Zhao G, et al. Advances in the use of chloroprocaine for day surgery. Chin J Lab Diagnosis. 2022;26(01):147–149.
8. Chen H, Cai J, Zheng X, et al. Effect of chloroprocaine on pain caused by propofol, injection. J Shanxi Med Univ. 2009;40(06):
9. Fu R, Peng X, Ren H, et al. Comparison of chloroprocaine with lidocaine in preventing propofol injecting pain. Med J Air Force. 2015;31(03):165–167.
10. McCrirrick A, Hunter S. Pain on injection of propofol: the effect of injectate temperature. Anaesthesia. 1990;45(6):443–444. doi:10.1111/j.1365-2044.1990.tb14329.x
11. Christ M. Pain - the fifth vital sign. Swiss Med Wkly. 2020;150:w20215. doi:10.4414/smw.2020.20215
12. Muhammad H, Gauhar A, Muhammad N, et al. Efficacy of intravenous paracetamol in combination with lidocaine pretreatment for reducing pain during injection of propofol. Cureus. 2020;12(2).
13. Chen H, Chen G. Effectiveness of different doses of chloroprocaine mixing in reducing the pain of propofol injection observed. J Taishan Medl Coll. 2011;32(09):708.
14. Runqiao F, Xiaofeng P, Haiqiang R, et al. Comparative study on the analgesic effects of clonprucaine and lidocaine versus propofol intravenous injection. J Air Force Med. 2015;31(03):165–167.
15. Ji T, Jiang C, Liu H, et al. Efficacy and safety of epidural chloroprocaine for breakthrough pain during labor analgesia: a prospective, double-blind, randomized trial. Pain TheraPy. 2024;13:227–239. doi:10.1007/s40122-024-00577-7
16. Tonder S, Togioka BM, Maani CV. ChloroProcaine. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024. PMID: 30422496.
17. Singariya G, Choudhary K, Kamal M, Bihani P, Pahuja H, Saini P. ComParison of analgesic efficacy of intrathecal 1% 2-chloroProcaine with or without fentanyl in elective caesarean section: a ProsPective, double-blind, randomised study. Indian J Anaesth. 2021;65(2):102–107. doi:10.4103/ija.IJA_816_20
18. Oron AP, Souter MJ, Flournoy N. Understanding research methods: UP-and-down designs for dose-finding. Anesthesiology. 2022;137(2):137–150. doi:10.1097/ALN.0000000000004282
19. Dixon WJ. Staircase bioassay: the uP-and-down method. Neurosci BiobehavRev. 1991;15(1):47–50.
20. Baykuş HE, Güç AA, Karabaş Ç, Çalış HT. Efficacy of hypnotherapy in the management of fibromyalgia:Aprospective randomized controlled study. World J Tradit Chin Med. 2023;9:447–453. doi:10.4103/2311-8571.391116
21. Görges M, Zhou G, Brant R, Ansermino JM. Sequential allocation trial design in anesthesia: an introduction to methods, modeling, and clinical applications. Paediatr Anaesth. 2017;27(3):240–247. doi:10.1111/pan.13088
22. Kang HJ, Kwon MY, Choi BM, Koo MS, Jang YJ, Lee MA. Clinical factors affecting the pain on injection of ProPofol Korean. J Anesthesiol. 2010;58(3):239–243.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effective Doses of Nalbuphine Combined with Propofol in Painless Hysteroscopy
Zhong W, Chen C, Tang W
International Journal of General Medicine 2022, 15:5609-5614
Published Date: 11 June 2022
RETRACTED ARTICLE: Effective Doses of Oliceridine Combined with Propofol for Painless Hysteroscopy: A Prospective Dose-Finding Study
Gao L, Tan A, Wang Z, Wei L, Wang X
International Journal of General Medicine 2025, 18:2651-2657
Published Date: 21 May 2025
Determining the Effective Dose of Oliceridine Compounded with Propofol for Painless Hysteroscopy: A Prospective Modified Dixon Sequential Dose-Finding Study
Yang K, Yuan Q, Huang H, Wang L, You J, Liu Q, Zhou Y, Luo Y, Liu Q
Journal of Pain Research 2025, 18:6903-6910
Published Date: 18 December 2025