Back to Journals » Drug Design, Development and Therapy » Volume 19
Effective Dose of Oliceridine for Inhibiting Hemodynamic Elevation Induced by Tracheal Intubation: An Up-and-Down Sequential Trial
Authors Yu J ![]() , Wei S
, Wei S ![]() , Ling D, Xin Y, Liu H, Yang Y, Li X, Xiang Z, Liu J
, Ling D, Xin Y, Liu H, Yang Y, Li X, Xiang Z, Liu J
Received 16 September 2025
Accepted for publication 23 December 2025
Published 26 December 2025 Volume 2025:19 Pages 11767—11778
DOI https://doi.org/10.2147/DDDT.S567868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Jianmang Yu,1,2,* Shiyou Wei,3,4,* Dandan Ling,4,5,* Yuxuan Xin,3 Hang Liu,3 Yiming Yang,3 Xionggang Li,1 Zhixiong Xiang,1 Jianming Liu3
1Department of Anesthesiology, Tianmen First People’s Hospital, Tianmen, Hubei, 431700, People’s Republic of China; 2Hubei Key Laboratory of Occupational Hazard Identification and Control, Wuhan University of Science and Technology, Wuhan, Hubei, 430065, People’s Republic of China; 3Department of Anesthesiology, Shanghai Pulmonary Hospital, School of Medicine, Tongji University, Shanghai, 200433, People’s Republic of China; 4Outcomes Research® Consortium, Houston, TX, 78299, USA; 5Department of Anesthesiology, Fudan University Shanghai Cancer Center, Shanghai, 200032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianming Liu, Department of Anesthesiology, Shanghai Pulmonary Hospital, School of Medicine, Tongji University, No. 507 Zhengmin Road, Shanghai, 200433, People’s Republic of China, Email [email protected] Zhixiong Xiang, Department of Anesthesiology, Tianmen First People’s Hospital, No. 1 East Jingling Renmin Avenue, Tianmen, Hubei, 431700, People’s Republic of China, Email [email protected]
Objective: This study aimed to investigate the effective dose of oliceridine for suppressing hemodynamic responses to tracheal intubation during general anesthesia induction and to evaluate the influence of age on dosing requirements, thereby providing evidence for clinical medication protocols.
Methods: A prospective single-center sequential dosing trial was conducted using a modified Dixon’s up-and-down method. Patients scheduled for elective surgery under general anesthesia with tracheal intubation were enrolled and divided into a young group (18– 65 years) and an elderly group (≥ 65 years). The initial doses were 45 μg/kg for the young group and 39 μg/kg for the elderly, with 3 μg/kg adjustments based on intubation response until seven crossovers occurred. A positive cardiovascular response was defined as an increase in mean arterial pressure or heart rate exceeding 20% from baseline within 3 minutes after intubation initiation. ED50 and ED95 values were estimated using Probit regression. Secondary outcomes included the incidence of injection-related cough, sedation success rate (MOAA/S score ≤ 2), peri-intubation hemodynamic changes, and adverse events.
Results: Fifty-eight patients were enrolled (28 young, 30 elderly). The ED50 of oliceridine was 46.5 μg/kg (95% CI 42.0– 51.19) and ED95 was 55.4 μg/kg (95% CI 43.58– 86.56) in the young group. In the elderly group, ED50 was 39.73 μg/kg (95% CI 34.17– 44.76) and ED95 was 50.11 μg/kg (95% CI 37.31– 77.87). Probit models demonstrated good fit in both groups. No injection-related cough reactions were observed, and the sedation success rate was 100%. Heart rate and blood pressure decreased during induction and normalized after intubation, with no significant intergroup differences. Adverse event incidence was comparable between groups.
Conclusion: Under standardized general anesthesia induction, the ED95 of oliceridine for suppressing tracheal intubation-induced hemodynamic elevation shows age-related differences, being approximately 55 μg/kg in younger patients and 50 μg/kg in the elderly.
Clinical Trial Registration: ClinicalTrials.gov, NCT07134660.
Keywords: oliceridine, tracheal intubation, hemodynamics, ED95, dixon’s up-and-down method
Introduction
Tracheal intubation is an essential technique for administering general anesthesia and facilitating mechanical ventilation. However, as an invasive procedure, it often elicits strong physiological stimulation, most notably significant hemodynamic elevation following intubation.1 Hemodynamic instability can increase the risk of cardiovascular complications, including myocardial ischemia, arrhythmias, and even heart failure, and has been associated with adverse perioperative outcomes.2
An ideal anesthetic induction should achieve unconsciousness, effective analgesia, adequate muscle relaxation, suppression of stress responses, and minimal impact on circulatory function. Currently, no single agent fulfills all these requirements; hence, a combination of drugs is commonly used in clinical practice. Standard regimens often include intravenous anesthetics, opioids, neuromuscular blocking agents, and other adjunct medications.
Opioids not only provide analgesia but are also highly effective in attenuating hemodynamic fluctuations induced by intubation.3,4 However, conventional opioids are associated with adverse effects such as nausea, vomiting, and respiratory depression.5,6 Most clinically used opioids act as agonists at the μ-, δ-, and κ-opioid receptor subtypes, non-selectively activating both G protein and β-arrestin signaling pathways. The latter is generally considered the primary mechanism underlying opioid-related adverse effects.7
Oliceridine is the first approved biased μ-opioid receptor agonist. Its analgesic effect is primarily mediated through G protein activation. It exhibits rapid onset and reliable analgesia, as it selectively activates G protein-coupled receptor (GPCR) signaling without engaging the β-arrestin pathway.8 Studies have shown that oliceridine has a favorable tolerability and safety profile in patients with acute pain, significantly reducing the incidence of various adverse events compared to morphine.7 Nevertheless, its clinical use remains relatively recent, with limited data available—especially in the context of tracheal intubation. The effective dose for suppressing intubation-induced hemodynamic elevation remains to be established.
Age is a critical factor influencing physiological function, drug metabolism, and dose-response relationships.9 Compared to younger patients, elderly individuals—particularly those with underlying cardiovascular and cerebrovascular diseases—are more susceptible to severe and potentially irreversible consequences resulting from pronounced hemodynamic fluctuations during intubation.10,11 This study aims to determine the effective dose of oliceridine for suppressing hemodynamic responses to tracheal intubation in patients of different age groups during general anesthesia induction, thereby providing a scientific basis for rational clinical medication use.
Methods
This trial was approved by the Ethics Committee of Tianmen Hospital Affiliated to Wuhan University of Science and Technology (Approval No. 20250250; Date: May 20, 2025) and registered on ClinicalTrials.gov (NCT07154979) on August 6, 2025, prior to the enrollment of the first patient. The study was conducted in accordance with the principles of the Declaration of Helsinki, and all participants provided written informed consent.
Inclusion and Exclusion Criteria
Inclusion criteria: Patients aged ≥18 years, body mass index (BMI) <25 kg/m2, American Society of Anesthesiologists (ASA) physical status I–III, scheduled for elective surgery requiring general anesthesia with tracheal intubation. Exclusion criteria: Preoperative resting systolic blood pressure (SBP) ≥160 mmHg or diastolic blood pressure (DBP) ≥110 mmHg or heart rate ≥110 beats/min; long-term use of analgesic or sedative medications; pregnancy, lactation, potential or planned pregnancy; history of allergy to the study drug; psychiatric disorders or communication barriers.
Termination criteria: Intubation failure (more than two attempts or intubation time exceeding one minute); incomplete data collection preventing evaluation of efficacy or adverse reactions; occurrence of perioperative cardiovascular or cerebrovascular accidents.
Study Design
This was a prospective, single-center, dose-finding clinical trial using a modified Dixon’s up-and-down sequential method. According to a recent study,12 the ED90 and ED99 of oliceridine in combination with propofol for suppressing responses during gastroscopy are 22.5 and 23.8μg/kg, respectively, with a dose adjustment of 2 μg/kg. Considering that tracheal intubation is more stimulating than gastroscope insertion, we selected 30 μg/kg as the initial dose and a step size of 3 μg/kg for both age groups in the present study to provide an appropriately higher starting level. During the subsequent Dixon up-and-down sequence, the first negative responses to tracheal intubation occurred at 45 μg/kg in the young group and 39 μg/kg in the elderly group. Subsequent doses were adjusted based on the patient’s response to tracheal intubation.
A positive cardiovascular response (CR) was defined as an increase in maximum mean arterial pressure or heart rate exceeding 20% above baseline values within 3 minutes after intubation. If a positive CR occurred, the dose for the next patient was increased by 3 μg/kg; if negative, the dose was decreased by 3 μg/kg. This process was repeated until seven sequential crossovers between positive and negative responses were observed, thereby determining the final sample size. A blinding procedure was implemented: both the anesthesiologist performing the procedure and the patient were unaware of the oliceridine concentration. Only the anesthesia nurse responsible for drug preparation was unblinded.
Grouping
Given that elderly patients generally require lower drug doses to achieve equivalent anesthetic effects,9,13 patients were divided into two age-based groups for determining population-specific effective doses: Young group (Y group), 18–65 years; Old group (O group), ≥65 years.This age cutoff is consistent with commonly accepted criteria in perioperative outcome studies14 and geriatric research,15 and is consistent with standards in both anesthetic pharmacology and geriatric medicine.
General Anesthesia and Perioperative Management
All patients fasted for 8 hours and abstained from clear fluids for 3 hours preoperatively. Standard anesthesia monitoring was applied intraoperatively. Both groups received intravenous flurbiprofen axetil (50 mg) and tropisetron (5 mg) 20 minutes before the end of surgery.
The anesthesia induction protocol was as follows: intravenous oliceridine (Jiangsu Enhua Pharmaceutical) was administered first, followed 2 minutes later by propofol (Sichuan Kelun Pharmaceutical) at 2.0 mg/kg. After loss of consciousness, rocuronium bromide (Jiangsu Hengrui Pharmaceuticals) was given at 0.6 mg/kg. Upon jaw relaxation, tracheal intubation was performed using a video laryngoscope with a single-lumen tube (size ID 6.5 for females and ID 7.0 for males), followed by initiation of mechanical ventilation.
Outcome Measures
The primary outcomes were the ED50 and ED95 of oliceridine for suppressing intubation-induced hemodynamic elevation. A positive cardiovascular response (CR) was defined as an increase in either the maximum mean arterial pressure or heart rate exceeding 20% above baseline values within 3 minutes from the start of intubation. Data obtained via the modified Dixon’s sequential method were analyzed using Probit regression to calculate ED50 and ED95.
The secondary outcome was the number of cough episodes. Coughing occurring during intravenous opioid injection was recorded.
Other Outcome Measures
Sedation success rate was assessed using the Modified Observer’s Assessment of Alertness/Sedation Scale (MOAA/S). This scoring system is a commonly used clinical tool for evaluating sedation depth.13 It grades responsiveness to varying levels of stimulation as follows: a score of 5 indicates responsiveness to name called in normal tone; 4 indicates lethargic response to name called in normal tone; 3 indicates response only after name is called loudly or repeatedly; 2 indicates response to mild prodding or shaking; 1 indicates response only to painful stimulus (trapezius squeeze); and 0 indicates no response to painful stimulus. A MOAA/S score ≤2 signifies loss of consciousness, assisting healthcare providers in objectively determining the patient’s level of sedation and consciousness.16
Blood pressure (systolic and diastolic) and heart rate were recorded at the following time points: upon entering the operating room (Tbase), immediately before intubation (Tbegin), and 3 minutes after intubation (T3min). The baseline value (Tbase) was defined as the average of three consecutive measurements of heart rate and blood pressure taken within 10 minutes after the patient entered the operating room. The pre-intubation time point (Tbegin) was defined as when the patient was under anesthesia and ready for tracheal intubation. The 3-minute post-intubation time point (T3min) referred to the period immediately following completion of the intubation procedure.
Adverse events including arrhythmias, body movement, airway spasm, allergic reactions, as well as subjective symptoms such as palpitations and dyspnea were documented.
Sample Size
Due to the sequential nature of the study design, a conventional precise sample size calculation was not feasible. However, literature indicates that a sample size of 20–40 subjects is sufficient to achieve stable estimates of the target dose using this methodology.16–18 Dixon suggested that the trial could be terminated after a fixed number of crossovers (transitions between positive and negative responses), with the results providing adequate stability for estimation.19 It is widely accepted that six crossovers meet statistical requirements.20 In this study, each age group was followed until seven crossovers occurred, which is generally considered adequate for a stable ED50 estimate.
Statistical Analysis
All statistical analyses were performed using R software (version 4.4.1). Normally distributed continuous data are presented as mean ± standard deviation, non-normally distributed data as median (interquartile range), and categorical data as number (percentage). The half-maximal effective dose of the drug was calculated using the classical Dixon sequential method. A Probit regression model was employed to fit the experimental data, from which the ED50, ED95, and their corresponding 95% confidence intervals (CI) were derived for each group. A P-value <0.05 was considered statistically significant.
Results
A total of 59 patients were enrolled in this study. One patient was excluded due to suspected rocuronium allergy, and the remaining 58 patients completed the trial and were included in the final analysis, comprising 28 in the young group and 30 in the elderly group (Figure 1). Baseline characteristics of all patients are presented in Table 1.
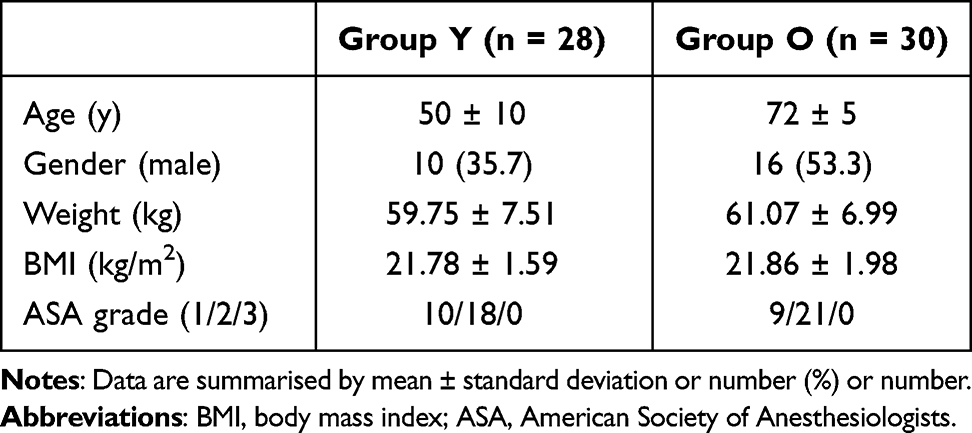 |
Table 1 Baseline Characteristics of Two Groups |
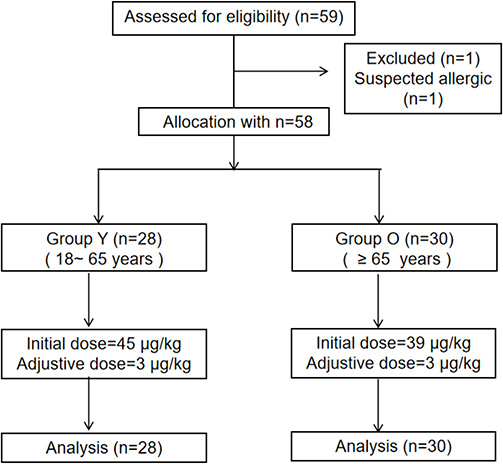 |
Figure 1 Trial flow diagram. |
The primary outcomes were the ED50 and ED95 of oliceridine for suppressing intubation-induced hemodynamic responses. In the young group, the ED50 (95% CI) of oliceridine for suppressing tracheal intubation responses was 46.5 (42.0–51.19) μg/kg, and the ED95 (95% CI) was 55.4 (43.58–86.56) μg/kg. The up-and-down sequential dosing sequence is illustrated in Figure 2A, the dose-response curves is in Figure 3A. Dose-response analysis based on Probit regression yielded the following model: Probit(P) = −7.929 + 0.171 × dose (μg/kg). The goodness-of-fit χ2-test indicated no significant deviation between the model and observed data (χ2 = 1.172, P = 0.883), suggesting good model fit.
 |
Figure 2 The up-and-down sequential plots of oliceridine dose and patient response (μg/kg). (A) Young group (Group Y, n=28) and (B) Elderly group (Group O, n=30). The X-axis represents patient number, the Y-axis represents oliceridine dose, solid circles represent negative cardiovascular responses (no increase in mean arterial pressure or heart rate exceeding 20% of baseline within 3 minutes after intubation), whereas solid triangles denote positive cardiovascular responses. |
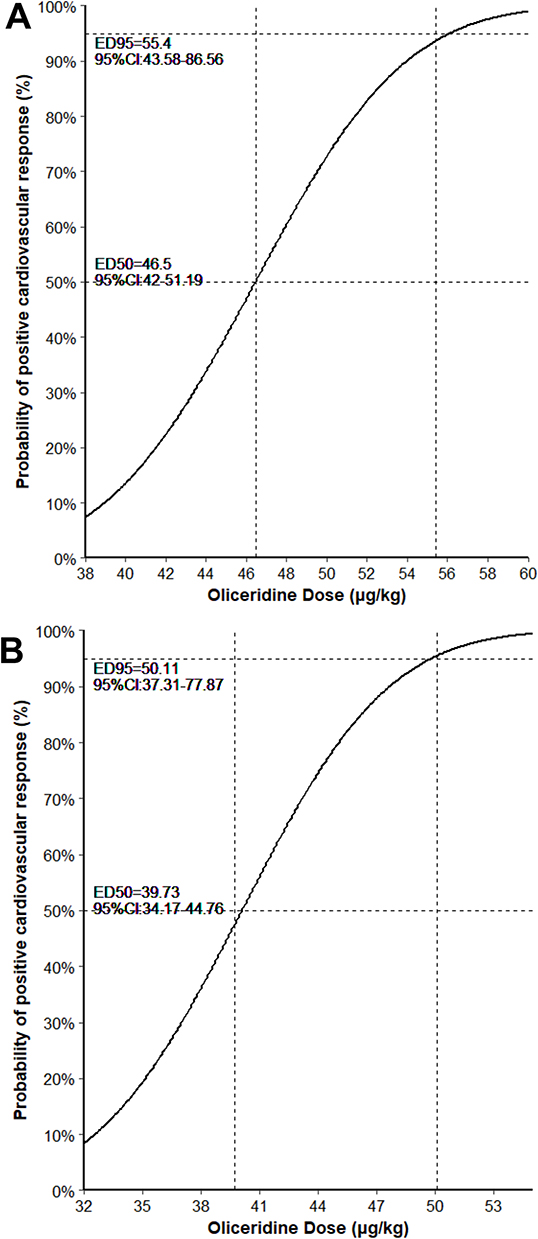 |
Figure 3 Dose-response curves for intravenous oliceridine. Dose-response curves for intravenous oliceridine for tracheal intubation plotted according to the relationship between the effective response probability derived from Probit regression analysis and the initial bolus dose, (A) Young group (Group Y, n=28) and (B) Elderly group (Group O, n=30). Probability of a positive cardiovascular response vs dose, with Probit-estimated ED50, ED95, and 95% CIs (dashed lines). |
In the elderly group, for positive patients (n = 15), 3 had both MAP and HR increased by 20%-30%, and in 12 at least one increased by >30%. For negative patients (n = 13), 2 had both increased by <10%, and 13 had at least one increased by 10%-20%.In the elderly group, the ED50 (95% CI) of oliceridine for suppressing intubation responses was 39.73 (34.17–44.76) μg/kg, and the ED95 (95% CI) was 50.11 (37.31–77.87) μg/kg. The up-and-down sequence is shown in Figure 2B. Probit regression analysis produced the model: Probit(P) = −6.807 + 0.170 × dose (μg/kg). The goodness-of-fit test showed no significant misfit (χ2 = 1.709, P = 0.789), indicating that the model adequately described the data. The dose-response curves is in Figure 3B.
We have examined potential sex-related differences in dose-response. In the young group (n = 28), the most frequent dose was 45 (n = 10); Fisher’s exact tests based on sex and response type showed no significant differences (P > 0.05). In the elderly group (n = 30), the most frequent doses were 39 (n = 9) and 42 (n = 9); similarly, Fisher’s exact tests revealed no significant sex-related differences in response type at these doses (P > 0.05).
Secondary Outcomes
The incidence of coughing is presented in Table 2. No coughing episodes were observed during oliceridine administration in this study.
 |
Table 2 Incidence of Coughing and Sedation Success Rate in Two Groups |
Other Outcomes
The sedation success rate was 100% (Table 2). During anesthesia induction, both groups exhibited reductions in blood pressure and heart rate. In the young group, heart rate decreased from 73 ± 14 bpm to 62 ± 11 bpm, and mean arterial pressure decreased from 98 ± 12 mmHg to 80 ± 13 mmHg. In the elderly group, heart rate decreased from 72 ± 11 bpm to 62 ± 10 bpm, and mean arterial pressure decreased from 103 ± 11 mmHg to 79 ± 13 mmHg. The magnitude of reduction showed no significant differences between groups (Table 3).
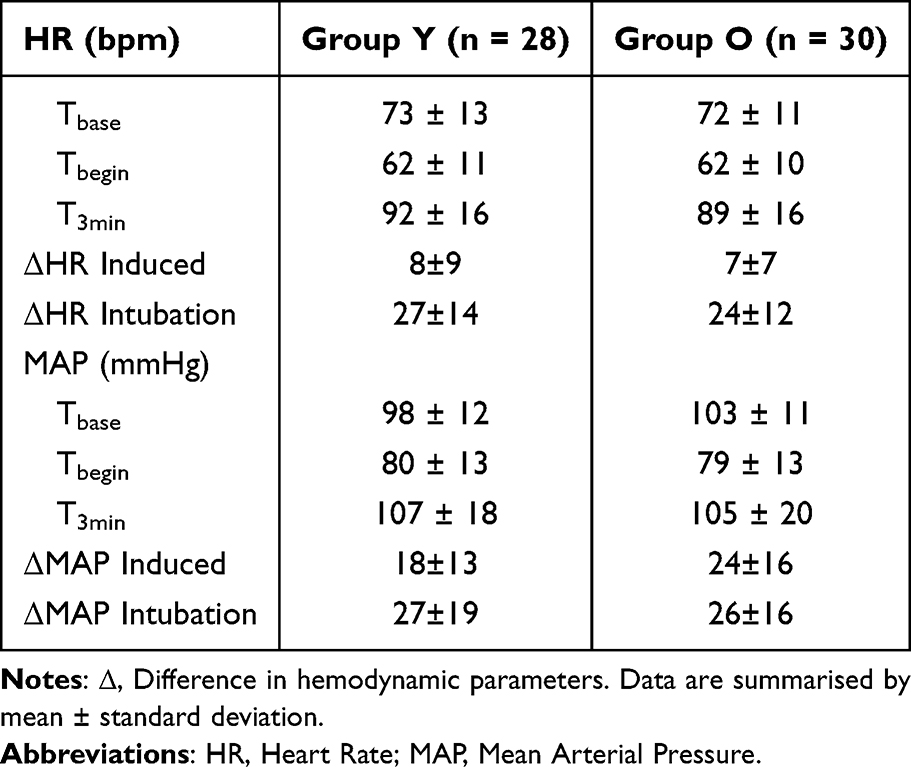 |
Table 3 Comparison of Hemodynamic Parameters Between Two Groups |
Following intubation, both groups demonstrated increases in heart rate and blood pressure, with no statistically significant differences in the magnitude of increase between groups (Table 3).
In the young group, for positive patients (n = 15), 3 had both MAP and HR increased by 20%-30%, and in 12 at least one of MAP or HR increased by >30%. For negative patients (n = 13), 2 had both MAP and HR increased by <10%, and 11 had at least one increased by 10%-20%.In the elderly group, for positive patients (n = 15), 3 had both MAP and HR increased by 20%-30%, and in 12 at least one increased by >30%. For negative patients (n = 15), 2 had both increased by <10%, and 13 had at least one increased >10%.
Throughout the anesthesia induction period and the 3-minute observation period after intubation, the young group experienced 2 cases of bradycardia, 1 case of tachycardia, 3 cases of hypertension, 1 case of arrhythmia (atrial premature contraction), and 1 case of palpitation. The elderly group experienced 1 case of bradycardia, 1 case of tachycardia, 4 cases of hypertension, 3 cases of hypotension, and 3 cases of arrhythmia (including ventricular premature contraction, atrial premature contraction, and irregular rhythm), with no reported palpitations. The overall incidence of adverse reactions did not differ significantly between groups (Table 4).
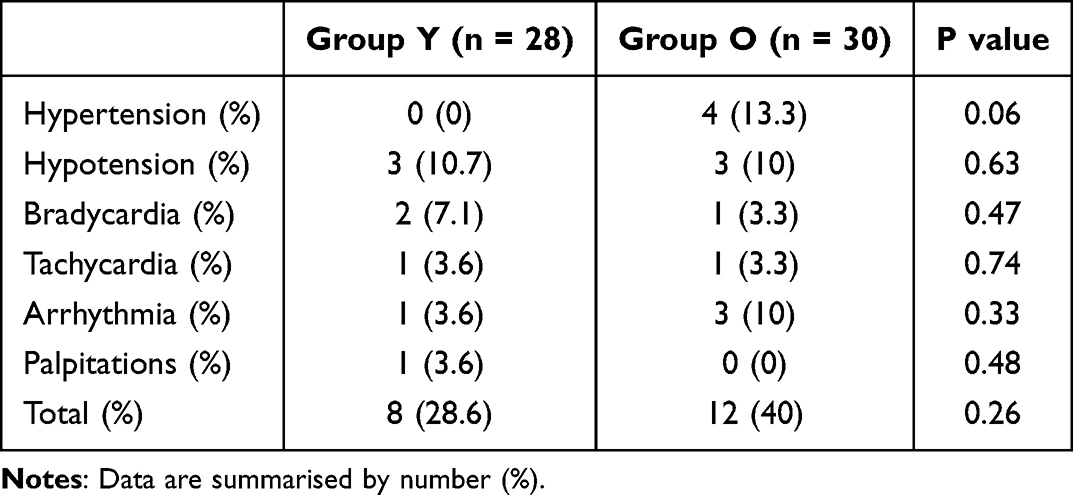 |
Table 4 Cases of Adverse Reactions In the Two Groups |
Discussion
This study employed a modified Dixon’s sequential method to evaluate the effective dose of oliceridine for suppressing intubation-induced hemodynamic responses in both young and elderly patients under a standardized anesthesia induction protocol. The primary results demonstrated that when using a 20% increase in either mean arterial pressure or heart rate from baseline within 3 minutes after intubation as the criterion for a positive cardiovascular response (CR), the ED50 values were 46.5 (42.0–51.19) μg/kg in the young group and 39.73 (34.17–44.76) μg/kg in the elderly group, while the ED95 values were 55.4 (43.58–86.56) μg/kg and 50.11 (37.31–77.87) μg/kg, respectively. Both groups showed good goodness-of-fit in the Probit regression models. Notably, the approximately 10% difference in ED95 values between groups suggests that age significantly influences the dose requirement of oliceridine needed to suppress intubation stress responses under the induction protocol used in this study.
Elderly patients typically exhibit increased pharmacokinetic and pharmacodynamic sensitivity to centrally sedating drugs.21,22 Drug metabolism occurs primarily through hepatic enzyme systems, transforming compounds into inactive or active metabolites. These metabolic enzymes are categorized into Phase I (oxidation and degradation reactions) and Phase II (synthetic reactions) pathways. Phase I metabolism is predominantly mediated by cytochrome P450 (CYP) enzymes, while Phase II metabolism involves enzymes such as glucuronosyltransferases, sulfotransferases, and acetyltransferases.23 Sedative-hypnotics, anxiolytics (eg, chlordiazepoxide), and benzodiazepines used for conscious sedation (eg, midazolam) undergo biotransformation primarily via Phase I enzymes.24,25 The clearance of these drugs is reduced in elderly patients, resulting in prolonged elimination half-lives and increased drug exposure. Consequently, dosage reduction of sedative-hypnotic medications is necessary for elderly patients.16 Fentanyl is a key analgesic agent used during anesthesia, primarily metabolized to norfentanyl through CYP3A4-mediated N-dealkylation.26 As fentanyl binds to plasma proteins, clinical conditions affecting protein levels may alter its plasma concentration.27 The absence of active metabolite accumulation may contribute to fentanyl’s potentially superior tolerability profile compared to morphine. Liver function status and use of CYP3A4 inducers can significantly influence serum fentanyl concentrations, while age demonstrates no substantial effect on its pharmacokinetics.26,28 Research indicates that the concentration producing 50% of maximal EEG suppression (C50) is reduced by 50% in elderly subjects.29 This suggests that pharmacodynamic rather than pharmacokinetic mechanisms explain why dose reduction of approximately 50% is required in elderly patients to achieve similar recovery profiles as younger patients 30 Oliceridine is metabolized in the liver by cytochrome P450 enzymes CYP3A4 and CYP2D6 to inactive metabolites,31,32 with drug efficacy directly correlating with plasma concentrations. CYP3A4 enzyme capacity shows an inverse relationship with age,33 providing a mechanistic explanation for the need to reduce oliceridine dosage in elderly patients.
In addition, based on the data from this study, we analyzed sex-related differences in the effective dose of oliceridine. The results showed that the difference in effective dose between male and female patients was not statistically significant. Existing studiesare still insufficient to determine whether there are true sex differences in opioid analgesia.34,35 Further research is needed to elucidate the nature of sex differences in opioid-induced pain relief and to clarify their underlying mechanisms.
Opioids frequently induce cough reactions, previous studies have reported cough incidences as high as 55% during induction with sufentanil at 0.5 μg/kg.36 Although typically short-lived and self-limiting, severe coughing can lead to abrupt increases in blood pressure, intraocular pressure, intracranial pressure, and intra-abdominal pressure. These hemodynamic changes may pose life-threatening risks, particularly in elderly patients, those with severe cardiopulmonary diseases, or individuals at high risk of aspiration.37 In this study, no injection-related cough was observed during intravenous administration of oliceridine, suggesting a potentially lower propensity of this agent to elicit airway reflexes. The precise mechanism underlying opioid-induced cough remains incompletely understood. Several theories are widely accepted: (1) Dualistic action on opioid receptors: Opioids exert analgesic effects primarily through G protein-coupled μ-receptor activation, but can also bias toward β-arrestin signaling pathways, leading to adverse effects such as respiratory depression, nausea, vomiting, constipation, and dependence.38 Variations in binding affinity to μ-receptors may influence interactions with downstream signaling proteins (eg, G proteins or β-arrestin), thereby modulating signal transduction.39 For instance, low-dose sufentanil activates μ-receptors and suppresses cough, whereas high doses may provoke coughing.40 This may relate to dose-dependent differences in receptor binding patterns and coupling protein selectivity. (2) Histamine release: Activation of opioid receptors can trigger the release of histamine and neuropeptides, resulting in bronchoconstriction and increased vascular permeability, which contribute to cough reflex.41 (3) Enhanced vagal nerve excitability: Opioids suppress sympathetic activity and augment vagal tone, reducing chest wall compliance and causing muscle rigidity and vocal cord adduction, thereby eliciting cough.42(4) Effects of drug excipients: Certain formulation components, such as citric acid in sufentanil preparations, may stimulate airway C-fibers and induce coughing.43
The sedation success rate was 100% in both groups. During anesthesia induction, heart rate and blood pressure decreased in both groups, followed by an increase after intubation. The magnitudes of these changes showed no significant differences between groups, suggesting that appropriate dosing regimens tailored to different populations can promote hemodynamic stability during induction. The overall incidence of perioperative adverse events was similar between groups, with no new safety signals identified. However, due to the limited observation window, the true spectrum of adverse reactions such as respiratory depression and postoperative nausea and vomiting requires further systematic evaluation.
Respiratory depression and nausea/vomiting are clinically significant adverse events associated with opioid medications, for which oliceridine may offer potential advantages.44 As a novel selective modulator of the μ-receptor G protein signaling pathway, oliceridine is designed to preferentially activate G protein signaling while minimizing recruitment of the β-arrestin pathway. In contrast to conventional opioids that non-selectively activate both G protein and β-arrestin signaling pathways, oliceridine’s low β-arrestin recruitment profile is associated with a significantly lower incidence of adverse reactions compared to morphine. It demonstrates particular advantages in reducing nausea, vomiting, and respiratory complications.44,45
Methodologically, this study’s strengths include the use of a sequential design to improve the efficiency of ED50 estimation, blinded drug allocation to reduce implementation bias, and application of Probit regression to extrapolate ED95 values. The definition of cardiovascular response (CR), based on either mean arterial pressure or heart rate increasing >20% from baseline during the high-risk 3-minute post-intubation window, effectively balances clinical relevance and operational feasibility.
However, several limitations should be considered: This was a single-center study with a limited sample size, which may limit the generalizability of our findings. Enrollment was restricted to elective surgery patients with a BMI less than 25 kg/m2, and patients with an ASA physical status greater than III were excluded. These restrictions limit the applicability of the results to higher-risk populations., the absence of a comparator opioid (such as remifentanil, fentanyl, or sufentanil), which prevents direct comparisons with other commonly used agents, and the relatively short observation window, which may not capture longer-term hemodynamic or clinical outcomes. At the same time, the secondary outcomes (cough incidence and sedation success rate) involved very few events and thus offer limited clinical information. Moreover, the sequential dose-finding design was neither intended nor powered to accurately estimate the incidence of these endpoints. Consequently, these findings should be viewed as descriptive observations rather than definitive conclusions, and further adequately powered randomized controlled trials are required to clarify their true incidence and clinical relevance. In addition, it should be noted that ED95 in both age groups was extrapolated from Probit regression applied to data from a design primarily optimized for ED50. Consequently, the 95% confidence intervals for ED95 were relatively wide, reflecting an inherent limitation of Dixon-type sequential designs, which concentrate information around the 50% response level and provide less precision in the upper tail of the dose-response curve. Despite these limitations, this method is still widely used in clinical practice and research to estimate the ED95, and the resulting values remain of considerable reference value.46,47
In conclusion, under a standardized general anesthesia induction protocol, the ED95 of oliceridine for suppressing intubation-induced hemodynamic responses was influenced by age. The ED95 was approximately 55 μg/kg in young patients and 50 μg/kg in elderly patients.
Data Sharing Statement
All data is included in the article. Further inquiries can be made to the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Review Committee of Tianmen Hospital Affiliated to Wuhan University of Science and Technology (Approval No. 20250250; Date: May 20, 2025). All patients have signed the informed consent form.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Shanghai Medical Innovation & Development Foundation (SMIDF2024-128-13) and China Red Cross Foundation Medical Empowerment Special Public Welfare Fund 2024 Analgesia Initiative Clinical Research Project (CRCF-YXFN-202401009). Joint Fund of Hubei Key Laboratory of Occupational Hazard Identification and Control (JF2023-Y12).
Disclosure
All authors have declared that they have no potential conflicts of interest for this work.
References
1. Foz C, Staffa SJ, Park R, et al. Difficult tracheal intubation and perioperative outcomes in patients with congenital heart disease: a retrospective study. J Clin Anesth. 2022;76:110565. doi:10.1016/j.jclinane.2021.110565
2. El-Shmaa NS, El-Baradey GF. The efficacy of labetalol vs dexmedetomidine for attenuation of hemodynamic stress response to laryngoscopy and endotracheal intubation. J Clin Anesth. 2016;31:267–273. doi:10.1016/j.jclinane.2016.01.037
3. Amin SM, Hasanin A, ElSayed OS, et al. Comparison of the hemodynamic effects of opioid-based versus lidocaine-based induction of anesthesia with propofol in older adults: a randomized controlled trial. Anaesth Crit Care Pain Med. 2023;42(4):101225. doi:10.1016/j.accpm.2023.101225
4. Grillot N, Lebuffe G, Huet O, et al. Effect of remifentanil vs neuromuscular blockers during rapid sequence intubation on successful intubation without major complications among patients at risk of aspiration: a randomized clinical trial. JAMA. 2023;329(1):28–38. doi:10.1001/jama.2022.23550
5. Nam SW, Do S-H, Hwang J-W, et al. Effects of opioid-sparing general anesthesia on postoperative nausea and vomiting in laparoscopic gynecological surgery. Korean J Anesthesiol. 2024;77(6):605–613. doi:10.4097/kja.24336
6. Meissner K, Kharasch ED. What’s old is new again: opioid and benzodiazepine actions on ventilation, a reminder of the importance of knowing one’s drugs. Br J Anaesth. 2025;134(4):903–905. doi:10.1016/j.bja.2025.01.014
7. Urits I, Viswanath O, Orhurhu V, et al. The utilization of mu-opioid receptor biased agonists: oliceridine, an opioid analgesic with reduced adverse effects. Curr Pain Headache Rep. 2019;23(5):31. doi:10.1007/s11916-019-0773-1
8. Ok HG, Kim SY, Lee SJ, et al. Can oliceridine (TRV130), an ideal novel µ receptor G protein pathway selective (µ-GPS) modulator, provide analgesia without opioid-related adverse reactions? Korean J Pain. 2018;31(2):73–79. doi:10.3344/kjp.2018.31.2.73
9. Chau DL, Walker V, Pai L, et al. Opiates and elderly: use and side effects. Clin Interv Aging. 2008;3(2):273–278. doi:10.2147/CIA.S1847
10. Khan FA, Ullah H. Pharmacological agents for preventing morbidity associated with the haemodynamic response to tracheal intubation. Cochrane Database Syst Rev. 2013;2013(7):Cd004087. doi:10.1002/14651858.CD004087.pub2
11. Russotto V, Myatra SN, Laffey JG, et al. Intubation practices and adverse peri-intubation events in critically ill patients from 29 countries. JAMA. 2021;325(12):1164–1172. doi:10.1001/jama.2021.1727
12. Tang Z, Yin G, Yu Y, et al. Determination of ED(90) and ED(99) of oliceridine combined with propofol in inhibiting responses to gastroscope insertion: a biased coin up-and-down design. BMC Anesthesiol. 2025;25(1):175. doi:10.1186/s12871-025-03052-8
13. Kowalski R, Mahon P, Boylan G, et al. Validity of the modified observer’s assessment of alertness/sedation scale (MOAA/S) during low dose propofol sedation: 3AP6-3. Eur J Anaesthesiol. 2007;24.
14. Chen JH, Chang -S-S, Liu JJ, et al. Comparison of clinical characteristics and performance of pneumonia severity score and CURB-65 among younger adults, elderly and very old subjects. Thorax. 2010;65(11):971–977. doi:10.1136/thx.2009.129627
15. Zizzo MG, Cicio A, Raimondo S, et al. Age-related differences of γ-aminobutyric acid (GABA)ergic transmission in human colonic smooth muscle. Neurogastroenterol Motil. 2022;34(3):e14248. doi:10.1111/nmo.14248
16. Wei S, Liu X, Chang R, et al. Effect of pre-use of dexmedetomidine on the effective inhibitory dose of remimazolam tosilate on positive cardiovascular response in double-lumen endobronchial intubation: a clinical study. BMC Anesthesiol. 2023;23(1):382. doi:10.1186/s12871-023-02305-8
17. Stylianou M, Flournoy N. Dose finding using the biased coin up-and-down design and isotonic regression. Biometrics. 2002;58(1):171–177. doi:10.1111/j.0006-341X.2002.00171.x
18. Pace NL, Stylianou MP, Warltier DC. Advances in and limitations of up-and-down methodology: a précis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107(1):144–152. doi:10.1097/01.anes.0000267514.42592.2a
19. Dixon WJ. Staircase bioassay: the up-and-down method. Neurosci Biobehav Rev. 1991;15(1):47–50. doi:10.1016/S0149-7634(05)80090-9
20. Paul M, Fisher DM. Are estimates of MAC reliable? Anesthesiology. 2001;95(6):1362–1370. doi:10.1097/00000542-200112000-00014
21. Gronich N. Central nervous system medications: pharmacokinetic and pharmacodynamic considerations for older adults. Drugs Aging. 2024;41(6):507–519. doi:10.1007/s40266-024-01117-w
22. Ngcobo NN. Influence of ageing on the pharmacodynamics and pharmacokinetics of chronically administered medicines in geriatric patients: a review. Clin Pharmacokinet. 2025;64(3):335–367. doi:10.1007/s40262-025-01494-4
23. Garza AZ, Park SB, Kocz R. Drug Elimination. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
24. Greenblatt DJ, Shader RI, Abernethy DR, Abernethy DR. Drug therapy. Current status of benzodiazepines. N Engl J Med. 1983;309(7):410–416. doi:10.1056/NEJM198308183090705
25. Greenblatt DJ, Abernethy DR, Locniskar A, et al. Effect of age, gender, and obesity on midazolam kinetics. Anesthesiology. 1984;61(1):27–35. doi:10.1097/00000542-198461010-00006
26. Mercadante S. Influence of aging on opioid dosing for perioperative pain management: a focus on pharmacokinetics. J Anesthesia Analgesia Critical Care. 2024;4(1):51. doi:10.1186/s44158-024-00182-2
27. Mercadante S. Opioid metabolism and clinical aspects. Eur J Pharmacol. 2015;769:71–78. doi:10.1016/j.ejphar.2015.10.049
28. Ekstein M, Gavish D, Ezri T, et al. Monitored anaesthesia care in the elderly: guidelines and recommendations. Drugs Aging. 2008;25(6):477–500. doi:10.2165/00002512-200825060-00003
29. Scott JC, Stanski DR. Decreased fentanyl and alfentanil dose requirements with age. A simultaneous pharmacokinetic and pharmacodynamic evaluation. J Pharmacol Exp Ther. 1987;240(1):159–166. doi:10.1016/S0022-3565(25)22695-7
30. Das S, Forrest K, Howell S. General anaesthesia in elderly patients with cardiovascular disorders: choice of anaesthetic agent. Drugs Aging. 2010;27(4):265–282. doi:10.2165/11534990-000000000-00000
31. Singla NK, Skobieranda F, Soergel DG, et al. APOLLO-2: a randomized, placebo and active-controlled phase iii study investigating oliceridine (TRV 130), a G Protein–Biased ligand at the μ-opioid receptor, for management of moderate to severe acute pain following abdominoplasty. Pain Pract. 2019;19(7):715–731. doi:10.1111/papr.12801
32. Fossler MJ, Sadler BM, Farrell C, et al. Oliceridine, a novel G protein-biased ligand at the μ-opioid receptor, demonstrates a predictable relationship between plasma concentrations and pain relief. ii: simulation of potential phase 3 study designs using a pharmacokinetic/pharmacodynamic model. J Clin Pharmacol. 2018;58(6):762–770. doi:10.1002/jcph.1075
33. Han J, Zhang Z, Liu X, et al. Prediction of pharmacokinetics for CYP3A4-metabolized drugs in pediatrics and geriatrics using dynamic age-dependent physiologically based pharmacokinetic models. Pharmaceutics. 2025;17(2):214. doi:10.3390/pharmaceutics17020214
34. Fillingim RB, Ness TJ, Glover TL, et al. Morphine responses and experimental pain: sex differences in side effects and cardiovascular responses but not analgesia. J Pain. 2005;6(2):116–124. doi:10.1016/j.jpain.2004.11.005
35. Fillingim RB, Gear RW. Sex differences in opioid analgesia: clinical and experimental findings. Eur J Pain. 2004;8(5):413–425. doi:10.1016/j.ejpain.2004.01.007
36. Chen P, Zeng P, Gong Y, et al. Recommended dose of sufentanil during induction of general anesthesia to avoid coughing and drastic hemodynamic fluctuations in patients undergoing surgery. J Int Med Res. 2021;49(3):300060521996143. doi:10.1177/0300060521996143
37. Irwin RS, Baumann MH, Bolser DC, et al. Diagnosis and management of cough executive summary: ACCP evidence-based clinical practice guidelines. Chest. 2006;129(1 Suppl):1s–23s. doi:10.1378/chest.129.1_suppl.1S
38. Manglik A, Lin H, Aryal DK, et al. Structure-based discovery of opioid analgesics with reduced side effects. Nature. 2016;537(7619):185–190. doi:10.1038/nature19112
39. Raehal KM, Schmid CL, Groer CE, et al. Functional selectivity at the μ-opioid receptor: implications for understanding opioid analgesia and tolerance. Pharmacol Rev. 2011;63(4):1001–1019. doi:10.1124/pr.111.004598
40. Kamei J, Iwamoto Y, Misawa M, et al. Antitussive effect of beta-endorphin is mediated by mu-opioid receptors, but not by kappa- or epsilon-opioid receptors. Eur J Pharmacol. 1993;233(2–3):251–254. doi:10.1016/0014-2999(93)90057-O
41. Ambesh SP, Singh N, Gupta D, et al. A huffing manoeuvre, immediately before induction of anaesthesia, prevents fentanyl-induced coughing: a prospective, randomized, and controlled study. Br J Anaesth. 2010;104(1):40–43. doi:10.1093/bja/aep333
42. Wang J, Duan J, Wang Q, et al. Pretreatment with nalbuphine prevents sufentanil-induced cough during the anesthesia induction: a randomized controlled trial. Ther Clin Risk Manag. 2020;16:281–286. doi:10.2147/TCRM.S247437
43. Kamei J, Nakanishi Y, Asato M, et al. Fentanyl enhances the excitability of rapidly adapting receptors to cause cough via the enhancement of histamine release in the airways. Cough. 2013;9(1):3. doi:10.1186/1745-9974-9-3
44. Singla N, Minkowitz H, Soergel D, et al. A randomized,Phase IIb study investigating oliceridine (TRV130), a novel µ-receptor G-protein pathway selective (µ-GPS) modulator, for the management of moderate to severe acute pain following abdominoplasty. J Pain Res. 2017;10:2413–2424. doi:10.2147/JPR.S137952
45. Viscusi ER, Webster L, Kuss M, et al. A randomized, phase 2 study investigating TRV130, a biased ligand of the μ-opioid receptor, for the intravenous treatment of acute pain. Pain. 2016;157(1):264–272. doi:10.1097/j.pain.0000000000000363
46. Zhou X, Zhao L, Mao W, et al. The median effective dose of ciprofol combined with sufentanil in suppressing the laryngeal mask airway insertion response in both young and older adult patients. BMC Anesthesiol. 2024;24(1):464. doi:10.1186/s12871-024-02855-5
47. Shi X, Yi F, Xiao H, et al. Low-dose alfentanil effectively reduces the ED50 of remimazolam for loss of consciousness in pediatric patients undergoing general anesthesia: a study using up-and-down sequential allocation method. Drug Des Devel Ther. 2025;19:7459–7466. doi:10.2147/DDDT.S532565
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
RETRACTED ARTICLE: Effective Doses of Oliceridine Combined with Propofol for Painless Hysteroscopy: A Prospective Dose-Finding Study
Gao L, Tan A, Wang Z, Wei L, Wang X
International Journal of General Medicine 2025, 18:2651-2657
Published Date: 21 May 2025
Determining the Effective Dose of Oliceridine Compounded with Propofol for Painless Hysteroscopy: A Prospective Modified Dixon Sequential Dose-Finding Study
Yang K, Yuan Q, Huang H, Wang L, You J, Liu Q, Zhou Y, Luo Y, Liu Q
Journal of Pain Research 2025, 18:6903-6910
Published Date: 18 December 2025
The ED90 of Oliceridine for Tracheal Intubation in Children: A Biased-Coin Up-and-Down Parallel Dose-Finding Study
Cheng L, Jiang J, Li M, Dan Y, Zheng J, Huang Y, Zhang K
Drug Design, Development and Therapy 2026, 20:601178
Published Date: 19 May 2026