Back to Journals » Psychology Research and Behavior Management » Volume 16
Depression, Perceived Risk of COVID-19, Loneliness, and Perceived Social Support from Friends Among University Students in Poland, UK, and India
Authors Bokszczanin A ![]() , Palace M, Brown W, Gladysh O, Tripathi R, Shree D
, Palace M, Brown W, Gladysh O, Tripathi R, Shree D
Received 29 June 2022
Accepted for publication 17 October 2022
Published 9 March 2023 Volume 2023:16 Pages 651—663
DOI https://doi.org/10.2147/PRBM.S380318
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Anna Bokszczanin,1 Marek Palace,2 William Brown,3 Olga Gladysh,4 Rakhi Tripathi,5 Divya Shree6
1Institute of Psychology, University of Opole, Opole, Poland; 2School of Psychology, Liverpool John Moores University, Liverpool, UK; 3School of Psychology, University of Bedfordshire, Luton, UK; 4Institute of Psychology, Polish Academy of Sciences, Warsaw, Poland; 5Information Technology Area, FORE School of Management, New Delhi, India; 6School of Criminology and Behavioural Sciences, Rashtriya Raksha University Lavad, Dahegam, India
Correspondence: Anna Bokszczanin, University of Opole, Institute of Psychology, 45-052 Opole, Plac Staszica 1, Opole, Poland, Email [email protected]
Background: The study examines the prevalence of depression among university students in Poland, the UK and India in the face of the second pandemic wave of COVID-19. The paper also examines the protective role of perceived social support, the hypothesis being that social support from friends would reduce depression.
Methods: The data from university students (N=732) in Poland (N=335), UK (N= 198), and India (N=199) were collected online during of the fall/winter 2021. Participants completed measures of depression (CES-D), COVID-19 risk perception index, loneliness (DJGLS), and perceived social support (MSPSS).
Results: Almost 52% of all participants (58.5% in Poland, 62.6% in the UK, and 29.1% in India) met the criteria for major depression. The higher levels of depression symptoms were associated with a higher perceived risk of COVID-19, greater loneliness, female gender, younger students’ age, and the lower levels of perceived social support. The greater family support predicted lower levels of depression symptoms in the Polish and Indian samples. Structural equation analyses (SEM) revealed the indirect effect of perceived social support from friends on the association between social loneliness and depression and between age and depression. This result shows that the support from friends significantly reduced depression, regardless of age, the level of social loneliness, and the perceived risk of COVID-19.
Conclusion: Our conclusions link to university specialists’ enhancement of psychological help for students with depression. We also recommend information campaigns on depression and treatment options.
Keywords: depression, perceived risk of COVID-19, loneliness, perceived social support, university students
Introduction
Ample empirical evidence shows that the COVID-19 pandemic (announced in March 2020 by the WHO) took a substantial toll on the mental health of university students around the world.1–5 The pandemic completely changed the lives of students. However, a consistent pattern emerged with the transition to remote learning, campus closures, self-isolation, physical distancing rules, closed public spaces, travel restrictions, job losses, and financial strain.6–8
Depression is one of the main threats to the mental health of university students because its consequences can be hazardous and lead to self-harm, suicidal thoughts, or suicide itself.9 More specifically, students showed higher levels of depression at the beginning of the pandemic than before.4 The negative impact of the pandemic on depression levels has transcended cross-cultural and Gross Domestic Product (GDP) differences.
For example, in the UK sample, one-third of the surveyed students met the criteria for clinical depression, whereas, before lockdown, this was the case for 15% of the sample.2 Similarly, in an online US study of college students, nearly 50% reported moderate and severe symptoms of depression.1 In Poland, longitudinal studies during the lockdown time also showed high scores of depression in students.11 Such increased scores observed in many studies are characterized by a persistent trend called elevated depression.12,13 Thus, the data collected during the lockdown periods lend weight to the importance of the question about the short and long-term impact of the pandemic on students’ depression levels, justifying the examination of both risk and protective factors.12,14
The pandemic’s stress can profoundly affect high rates of depression and anxiety.15–17 Studies in the US have shown that factors related to the COVID-19 epidemic were significantly associated with the risk of depression for university students, especially the social proximity of COVID-19 cases.18 In a Chinese study, the risk of developing depression symptoms in students with confirmed COVID-19 cases in family members and relatives was three times higher than in those without the confirmed infection.10 It was also shown that knowing a person infected with COVID-19 can increase the likelihood of distress.1 This relationship has also been found in international studies.19 Students’ concerns about the coronavirus, as their own and family and friends’ health, and missing out on social life during the lockdown15 were also identified.
Loneliness is the substantial factor responsible for student depression during the pandemic that emerges from many studies.15,20 In a Dutch study, for example, students’ depression was positively correlated with high levels of loneliness.20 In Poland, young adults’ loneliness was also positively associated with depression symptoms.21 The rate of loneliness among young people during the lockdowns was high in the UK and Germany,22 particularly among women in Spain and Finland.23 The increased loneliness during the pandemic arose from the drastic and sudden limit on students’ social activities.12 In the US, for example, loneliness was exacerbated by social distancing, online learning, uncertainty, and lack of social support.7,24 The limited access to required study materials and national lockdowns hurt students’ self-discipline in China,8 further compounded by the stress of physical distancing and a sudden stop to social interactions and activities associated with student life. According to Weiss,25 there are two types of loneliness: emotional, resulting from the lack of close and intimate relationships) and social (resulting from the lack of a social network). Given the imposed social distancing rules, distance learning, and the critical role that college friends play in protecting against mental health issues,26 our main interest lies in examining social loneliness.
Several studies with college student populations report that during the COVID-19 outbreak, a higher level of depression was observed in women than in men.1,27 In turn, some studies found that younger students experienced higher levels of depression than older age groups in Ethiopia and Spain. These findings suggest that gender and age remain essential factors to be considered in mental health interventions.2
One way of staving off depression and loneliness and its repercussions is to rely on the social resources offered by family and friends.28 The available literature on people’s reactions to natural and health disasters shows that social support is one of the most important factors protecting mental health and buffering against psychopathology.29,30 The social support theory by Lakey and Cohen31 suggests that social support acts as a stress buffer (ie, reduces the effects of stressful life events on health) through either the supportive actions of others (eg, advice, reassurance) or the belief that their support is available. Whereas supportive activities enhance coping performance, the perception of available support leads to assessing of potentially threatening situations as less stressful.32 This was also identified during the COVID-19 pandemic, with resilience, coping behaviors, and social support protecting students against loneliness,33 depression,34,35 and pandemic-related stressful experiences.36
Researchers usually focus on perceived social support, namely how individuals perceive family members and friends in terms of delivering emotional, material, psychological, and overall support during times of stress.28 The positive role of perceived social support manifests in both individualist and collectivist cultures. Whereas US students with more symptoms of depression and anxiety reported greater increases in alcohol consumption, those with more perceived social support reported less alcohol intake following the campus closure.37 In China, the degree of students’ perceived social support during the pandemic was directly proportional to their adoption of active coping strategies38 and fewer depression symptoms.39 Also, low social support and being male was associated with higher depression, anxiety, and stress levels among Chinese undergraduates.3 In the Philippines, perceived social support reduced a sense of loneliness among students.33 Support from family and friends has a significant, positive impact on university students’ social and academic achievements. When a young person enters university, peer support can become more important than their parents’ support, significantly reducing the risk of depression.40
As the above-covered study identifies young adults’ mental health as particularly vulnerable, and given the apparent differences in depression levels between the countries during the pandemic, the current paper answers the call for intercultural comparisons41–43 by focusing on university students in countries with different rules of social support – individualist UK, mixed-culture Poland and collectivist India where closer family bonds have been identified.44 Whereas Poland and the UK are officially high-income countries, India has been classified as a lower-middle-income country. The cultural and social differences between the three countries are vast. Some of such differences, for example, can be found in how their respective universities operate, their curricula, student life, and drinking age, to name a few.43
Based on the above-covered literature, we would like to examine the prevalence of depression among university students in Poland, the UK, and India in the face of the second wave of the COVID-19 pandemic. It was hypothesized that higher depression symptoms would be associated with a greater perceived risk of COVID-19, a greater sense of loneliness, female gender, younger students’ age, and less perceived social support. Finally, we hypothesized that social support from friends would reduce the symptoms of depression regardless of cultural settings.
Methodology
Study Design and Procedure
This study utilized a cross-sectional research design, and the online surveys were prepared using Google Forms. The data were collected in each country in the fall/ winter of 2020/2021 in Poland (October 27 to November 26, 2020), the UK (November 23 to January 30, 2021), and India (November 29 to February 2, 2021). The study procedure was identical in all three countries at universities in Poland (University of Opole), the UK (Liverpool John Moores University), and India (Fore School of Management and Rashtriya Raksha University). The snowball sampling technique was used to recruit respondents. To obtain a medium effect size (Cohen’s coefficient, χ²-test, p < 0.05, 95% confidence), the minimum sample size is 159 people per group. Whereas Poland-based participants completed the survey in Polish, the UK and India-based participants completed it in English. We used a structured questionnaire including a set of measurement tools with proven psychometric properties, appropriately validated in Polish46,49,50 and widely used by researchers in English and Polish.
A pilot study was carried out before starting, in which several students filled in the questionnaire and then provided feedback. Researchers discussed all their comments to improve the questionnaire towards unambiguousness and simplicity and sent the link with the online survey to a group of student-helpers from a research club, requesting to disseminate the link on student forums and social media. At the end of the questionnaire, the participant requested to send the questionnaire to friends via email. All participants were informed about voluntary participation and their right to withdraw without consequences. Their informed consent was obtained by clicking on the “agree” button. Only those who gave their consent had access to other parts of the survey.
All students who completed the survey were qualified (N = 732); twenty-one persons did not complete the survey and were therefore excluded from the later calculations. Information on participants’ depression, loneliness, perceived COVID-19 risk, social support, and sociodemographic data, including age, gender, study year, study subject, and employment, were collected. Depression symptom level was an explained (dependent) variable and perception of COVID-19 risk, loneliness, perceived social support, gender, and age were independent variables.
Following the lead author’s ethics board clearance (University of Opole, Poland, No 9/2020), which was accepted by the authors’ ethics boards from the UK and India as compliant with their respective institutional ethics requirements, we proceeded with the data collection.
The study was carried out following the Declaration of Helsinki. No information identifying the respondents was collected.
Participants
The data from university students (N = 732) in Poland (N = 335), UK (N = 198), and India (N = 199) were collected using an opportunity sample. Participants’ age was primarily in the range of 18–24 (86%), and most of them (71%) were women. Whereas in Poland and the UK, most participants studied social sciences (33% and 82%, respectively), in India, economics was predominant (88%). Most participants were undergraduates (Poland 75%; the UK 97%; India, 56%), and were not currently employed (61% in Poland; 45% in the UK and 93% in India).
Measures
The reliability indicators of each scale by country showing good values ranging from 0.71 to 0.95.
Depression (CES-D)
Depression was measured by the Centre for Epidemiological Studies Depression scale (CES-D;)45,46 CES-D consists of 20 items with scores ranging from 0 to 60. Using a Likert-type scale, participants reported the frequency of symptoms, such as restless sleep and poor appetite over the past week. The scale features four possible answers: never or rarely (less than one day), some of the time (1–2 days), occasionally (3–4 days), and most or all of the time (5–7 days). The severity of depression symptoms is then estimated using the score total: 0–15 no depression, 16–21 experiencing mild to moderate depression, 22–60 a major depression.
COVID-19 Risk Perception
COVID-19 Risk perception is a holistic measure of risk perception featuring six items measuring participants’ perceived severity of the pandemic over the next six months.47 The COVID-19 risk perception was measured as an index that included participants’ perceived likelihood of contracting the COVID-19 virus, their current worry about the virus, and the perceived likelihood of their family and friends catching it. The total risk perception measure was calculated as the mean value of all six items ranging from 0 to 36.
De Jong Gierveld Loneliness Scale
Loneliness was measured with the eleven-item De Jong Gierveld Loneliness Scale (DJGLS), covering both emotional and social loneliness.48,49 Each item has five possible answers: definitely yes = 1, yes = 2, more or less = 3, no = 4, definitely no= 5. The scale consists of 6 negatively formulated items responding to emotional loneliness and five positively formulated items responding to social loneliness. Before the total score was calculated, the negatively formulated items were reversed, meaning that the higher the final summarized value was, the higher the sense of loneliness (ranging from 11 to 55) was.
The Multidimensional Scale of Perceived Social Support (MSPSS)
Social Support was measured with the Multidimensional Scale of Perceived Social Support (MSPSS),50 which captures perceived social support across different cultures.51 It is a 12-item scale comprising three subscales: perceived social support from family, friends, and the significant other, with each of the subscales comprising four items on a Likert-type scale ranging from 1 to 7 (1 = very strongly disagree and 7 = very strongly agree). Each subscale item is related to practical help, emotional support, availability to discuss problems, and help in decision-making. The range of each scale was from 3 to 21; for the whole scale was 12 to 84, showing that the higher the score, the higher the perceived social support.
Statistical Analysis
In the beginning, the means (M), standard deviations (SD) and Pearson’s bivariate correlations (r) were examined. Next, percentage proportions of depression between the countries were estimated using the following criteria: 0–15 (no depression), 16–21 (mild to moderate depression), and 22–60 (major depression). A one-way ANOVA with the Bonferroni post hoc test was used to assess the differences in the level of depression between Poland, the UK, and India. Then four hierarchical regression analyses were performed, the aim being to isolate of significant predictors of depression symptoms severity. Finally, Structural Equation Modeling (SEM) was run using the AMOS software. Four SEM analyses were performed (for the total sample and per country). The SEM was meant to show the predictors of depression using the pathway technique to examine the variables’ causal order, answering the question about social support potentially buffering against risk factors (eg, COVID-19 risk perception and loneliness) for depression.
Results
Means, Standard Deviations, and Correlations
Table 1 shows the variables’ means, standard deviations, and correlation matrix. The correlation analysis examined the association between depression severity and other variables. Many statistically significant correlations were observed (p <0.01). Table 1 shows that higher levels of depression symptoms were observed in females and younger students. The level of depression symptoms was positively and significantly associated with the perceived risk of COVID-19, general loneliness, and emotional and social loneliness. In turn, the severity of depression symptoms was negatively correlated with the overall score on the perceived social support scale, support from family, friends, and the significant other.
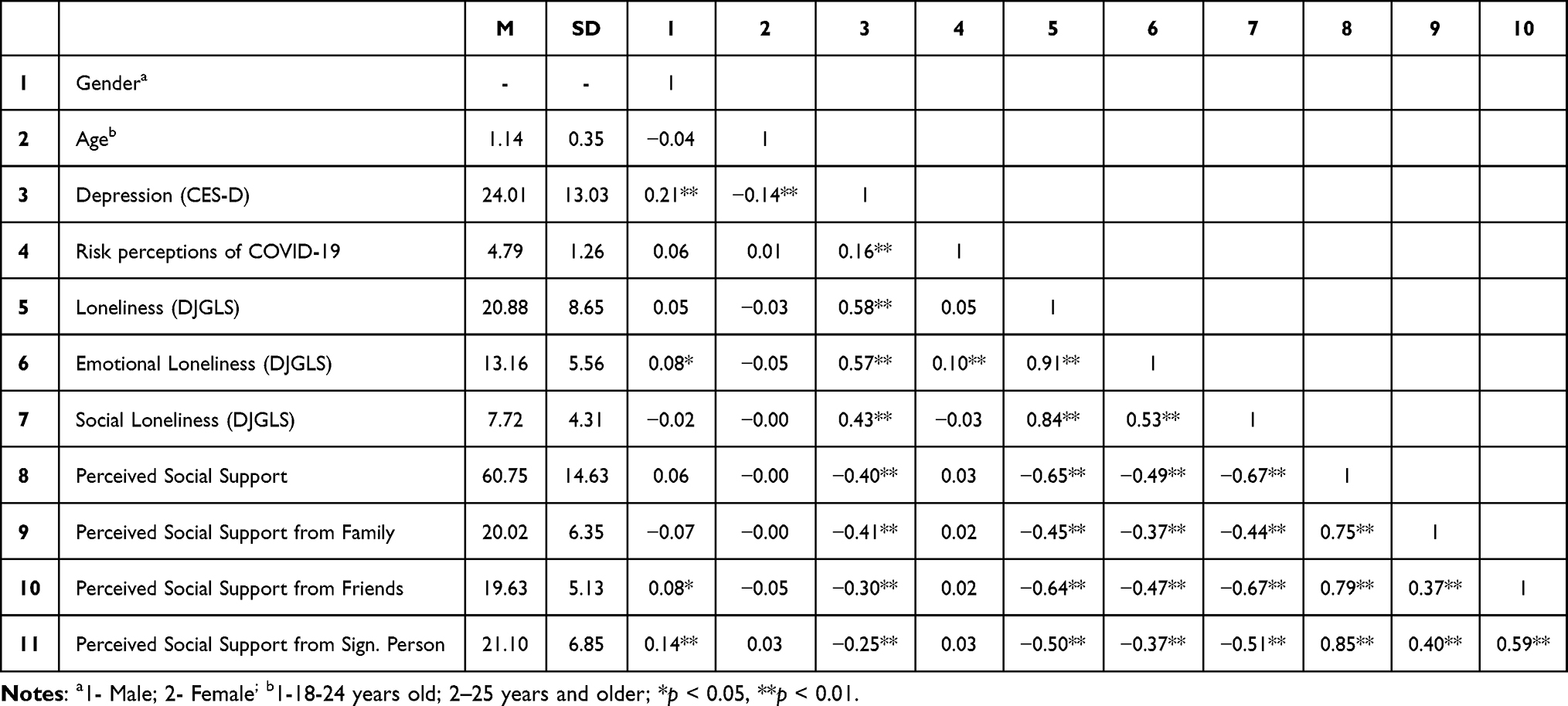 |
Table 1 Means (M), Standard Deviations (SD), and Correlation of the Variables |
Prevalence of Depression
Table 2 shows that 51.6% of the total sample reported major depression symptoms, 17.1% reported mild to moderate symptoms, and 31.3% reported no symptoms. Most Polish sample (58.5%) reported major symptoms, 13.7% reported mild to moderate symptoms, and 27.8% reported no symptoms. About sixty-three percent of the UK sample (62.6%) reported major depression symptoms, 16.2% reported mild and moderate symptoms, and 21.2% reported no symptoms. The sample reporting the lowest major depression symptoms was Indian (29.1%), with 23.6% reporting mild to moderate symptoms and 47.3% reporting no depression symptoms.
 |
Table 2 Prevalence and Severity of Depression Symptoms by Country |
The Severity of Depression Symptoms
A one-way ANOVA with the Bonferroni post hoc tests was used to compare the results. Means and standard deviations of the study variables and differences between the countries are presented in Table 2. Higher and statistically significant differences in the level of depression symptoms were found in the Polish and UK samples than in the Indian sample: F (2,731) = 31.05, p <0.001.
Hierarchical Regression Analyses
Four hierarchical regression equations were performed to examine the effects of gender, age, loneliness, perceived risk of COVID-19, and perceived social support on depression symptoms in the whole group of participants and separately for each country. Gender and age were introduced in the first step, followed by the perception of COVID-19 risk and social and emotional loneliness in the second step. In the last third step, they perceived social support from family, friends, and their significant other. All independent variables entered into the equations explained the statistically significant part of the variance in all the four dependent variables. As for the total sample, the model explained 45% of the total variance of depression symptoms, R2=0.45, p<0.001, F=72.35, p<0.001; R2 = 0.45, p<0.001, F= 32.26, p<0.001 (the Polish sample); R2=0.44, p<0.001, F=12.13, p<0.001 (the UK sample); and R2 = 0.45, p<0.001, F = 18.85, p<0.001 (the Indian sample). The results are presented in Table 3.
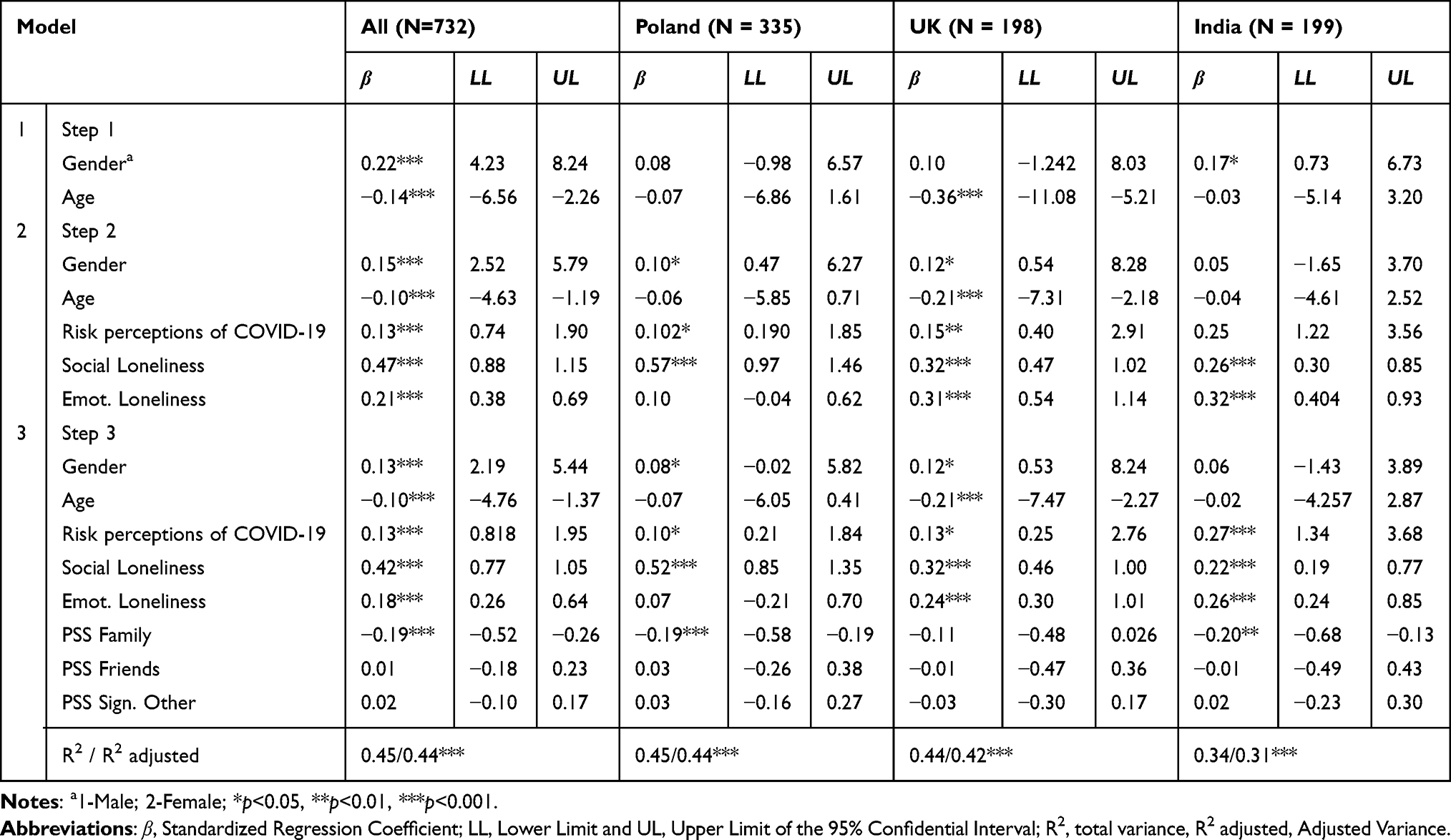 |
Table 3 Hierarchical Regression Analyses for All Participants |
Introduced in the first step, the female gender was a statistically significant predictor of greater depression in the total sample, Poland and the UK (β =0.13***p<0.001; β =0.08* p<0.05; β =0.12*p<0.05, respectively). The younger age of students was a statistically significant predictor in the total sample (β=−0.10***p<0.001 and in the UK sample (β=−0.21***p<0.001) only.
In all four regression equations (ie, for the total, UK, Polish and Indian samples), the perception of a greater COVID-19 risk was associated with greater severity of depression symptoms (β=0.13***p<0.001; β=0.10***p<0.001); β =0.15***p<0.001; β =0.25***p<0.001, respectively). Similarly, a higher sense of social loneliness increased the risk of depression in all the samples (β =0.42***p<0.001; β =0.52***p<0.001); β =0.32***p<0.001; β =0.22*** p<0.001, respectively). In contrast, the feeling of emotional loneliness was a statistically significant predictor of depression symptoms in the total sample (β =0.18***p<0.001), UK sample (β=0.24***p<0.001), and Indian sample (β =0.26***p<0.001). Apart from the UK sample, greater perceived social support from the family predicted lower severity of depression (in the total sample β=−0.19***p<0.001; in the Polish sample β=−0.19***p<0.001; in the Indian sample β=−0.20***p<0.001). The support of friends and the significant other did not affect the level of depression symptoms.
Structural Equation Modeling (SEM)
Depression Structural Equation Model for the Total Sample
SEM was conducted to examine the hypothesis that social support from friends would reduce the symptoms of depression regardless of participants’ current country of residence.26
A non-kin social support approach to depression was adapted over a strictly mood-based approach. Specifically, it was anticipated that COVID-19 lockdown restrictions could increase social isolation in both sexes, which could lead to depressive symptoms without adequate social support buffering from friends. Thus, five independent variables were entered into the model, ie, age, risk perceptions of COVID-19, social loneliness, and perceived social support from friends. The first model was developed using the total number of participants. The model showed a good fit: χ2=2.24, df = 1; comparative fit index [CFI] =0.99; root mean square error of approximation [RMSEA] =0.04; Akaike information criteria [AIC] =30.23. The resulting model (Figure 1) found small and large associations between intercept and slope factors. Age (standardized coefficient = −0.09, p=0.002), COVID-19 risk perception (standardized coefficient=0.15, p<0.001), social loneliness (standardized coefficient =0.53, p<0.001), and social support from friends (standardized coefficient = −0.11, p=0.003) all directly predicted depression severity. There was no statistically significant indirect effect on COVID-19 risk perception. However, there was an indirect effect of age (indirect standardized coefficient=0.69) on depression via its relation to social support from friends (standardized coefficient=0.02, p=0.04).
 |
Figure 1 Depression structural equation model for the total sample (India, Poland and the United Kingdom). Notes: A(1 = 18–24; 2 = 25 and older); Fitting of the model: RMSEA = 0.04; χ2 = 2.24, df = 1; CFI = 0.99; AIC = 30.23. |
Depression Structural Equation Model for the Polish Sample
The same set of independent variables was introduced into the SEM model with depression symptoms as an outcome. The results from the structural equation suggest a good fit: χ2=0.001, df = 1; comparative fit index [CFI]=1.00; root mean square error of approximation [RMSEA] = 0.00; Akaike information criteria [AIC]=28.00. The resulting model (Figure 2) found small to large associations between intercept and slope factors. Only COVID-19 risk perception (standardized coefficient=0.10, p=0.015) and social loneliness (standardized coefficient=0.62, p<0.001) directly predicted depression. There were no statistically significant indirect effects on depression.
 |
Figure 2 Depression structural equation model for the Polish sample. Notes: A(1 = 18–24; 2 = 25 and older); Fitting of the model: RMSEA = 0.00; χ2 = 2.24 df = 1; CFI = 1.00; AIC = 28.00. |
Depression Structural Equation Model for the UK Sample
The results from the structural equation suggest a good fit: χ2 = 10.09, df =1; comparative fit index [CFI]= 0.93; root mean square error of approximation [RMSEA] = 0.21; Akaike information criteria [AIC]=38.09. The resulting model (Figure 3) found small to large associations between intercept and slope factors. Age (standardized coefficient=−.24, p<0.001), COVID-19 risk perception (standardized coefficient =0.14, p=0.01), social loneliness (standardized coefficient =0.38, p<0.001), and perceived social support from friends (standardized coefficient =−.21, p<0.001) all directly predicted depression. There was no statistically significant indirect effect on COVID-19 risk perception. However, there was an indirect effect of age (indirect standardized coefficient =0.13) on depression via its relation with social support from friends (standardized coefficient =0.61, p=0.02).
 |
Figure 3 Depression structural equation model for the United Kingdom sample. Notes: A(1 = 18–24; 2 = 25 and older); Fitting of the model: RMSEA = 0.21; χ2=10.09, df = 1; CFI = 0.93; AIC = 38.09. |
Depression Structural Equation Model for the Indian Sample
The results from the structural equation suggest a good fit: χ2= 1.99, df = 1; comparative fit index [CFI] =0.99; root mean square error of approximation [RMSEA] =0.07; Akaike information criteria [AIC] =29.99. The resulting model (Figure 4) found small and large associations between intercept and slope factors. COVID-19 risk perception (standardized coefficient =0.27, p<0.001), social loneliness (standardized coefficient =0.31, p<0.001), and perceived social support from friends (standardized coefficient =−.19, p=0.003) all directly predicted depression severity. There were no statistically significant indirect effects.
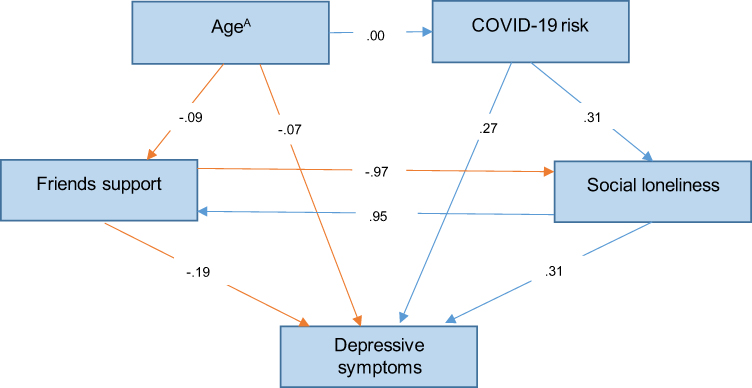 |
Figure 4 Depression structural equation model for the Indian sample. Notes: A(1= 18–24; 2=25 and older); Fitting of the model: RMSEA = 0.07; χ2 = 1.99; CFI = 0.99; AIC = 29.99. |
Discussion
We examined the depression symptoms among university students in Poland, the UK, and India in the face of the second wave of the COVID-19 pandemic. Our cross-sectional study of 732 students resident in the three countries revealed a significant prevalence and increased in symptoms of depression compared to the early lockdown studies.2,4 Almost 52% of students from the total sample had potentially major depression (58,5% in Poland, 63.6% in the UK, and 29.1% in India). It suggests that more than half of them could suffer from depression symptoms after about a year of lockdown. These results are alarming and surpass data from the beginning of the pandemic. Depending on the sample, the percentage of students at risk of depression ranged from 30 to 50%.2,10 Thus, it can be concluded that students’ mental health deteriorated significantly in the face of the second wave of the pandemic, which is consistent with the observed trend defined as elevated depression.11–13
Such high student scores on the depression scale can be attributed to the dangers of the pandemic situation. The second wave of the COVID-19 epidemic swept through Europe from the beginning of September 2020,52 through India from November,53 and during our data collection period. During the second wave of the pandemic, the morbidity and mortality rate was much higher than at the beginning of the first wave of the pandemic (March-May 2020). For example, the official pandemic death toll (from September 2020 to December 2021) was 17,326 in Poland54 and 19,118 in the UK. In India, the coronavirus cases amounted to over 10 million new cases (from November 2020 to February 2021) and over 155,000 deaths within one month. These figures demonstrate that the second wave was more severe than the first one and could directly affect students’ levels of depression in the form of negative mood, sadness, downheartedness, hopelessness, and a lack of joy in life.
The Polish and UK students had higher scores of depression than the Indian students. This difference may be put down to the differences between our samples. The Polish sample had more women than the UK and Indian samples, respectively, 82%, 85%, and 37%. Relatedly, during the pandemic, women were found to admit to being depressed more than men.1,27 The meta-analysis of data from studies during the COVID-19 pandemic confirmed that women had a 1.77 higher risk of experiencing depression than men.55 There was also a difference related to the student’s work and study subject that could help explain the observed differences in levels of depression. While 30% of Polish and 37% of UK students were in gainful employment during the pandemic, only 3.5% of Indian students reported being employed. It can be speculated that the combination of work and study obligations might have increased the burden and stress, negatively affecting mental health. Furthermore, a related Polish study showed that the studied course subject (ie, sports science) was crucial in facilitating better mental health.5 Thus, some of the identified differences in the current study could be down to the studied course. In contrast, the primary major of the Polish and UK student samples was social sciences. The dominant major in the Indian sample was economics.
We hypothesized that higher levels of depression symptoms would be associated with a greater perceived risk of COVID-19, a greater sense of loneliness, female gender, and younger students’ age. The results of our study confirmed these expectations. The perceived risk of COVID-19 was understood and measured in our study as a subjective sense of threat to one’s own life and health and the threat to other people.47 This variable turned out to be a significant predictor of greater intensity of depression symptoms, independently explaining a significant part of the variance in the total and three separate samples. This result means that the greater the subjective sense of being in danger of COVID-19, the greater the severity of depression symptoms. Similar results were found in studies where factors related to the COVID-19 epidemic were significantly associated with the risk of depression.1,10,17,18 This result is also in line with the latest understanding of the risk related to COVID-19, defined as a new type of psychological trauma that can damage mental health, well-being, social status, and income.56
Loneliness is a subsequent factor that was associated with greater severity of depression symptoms in students. Both emotional and social types of loneliness were significant predictors of greater severity of depression symptoms, beyond and above demographic factors, and the perceived risk of COVID-19. These findings are consistent with the current study reports.15,20,21 High depression symptoms in students may be conditioned by the lack of people around, belonging to a specific group (social loneliness), and breaking and/or the lack of close ties with the significant other (emotional loneliness). The lack of social activity caused by distance learning likely contributed to students’ loneliness7,12,24 by hampering social interaction, which is worth examining in further studies.
Correlation and regression analyses support the expectation that female and younger students would have more symptoms of depression than older students. Similar results have been noticed in studies in Poland11 and other countries, like Ethiopia and Spain. Overall, younger students seem to have dealt with the pandemic’s stress more poorly, partly due to their less developed academic skills and greater need for social contact.57
As anticipated, perceived social support had significant inverse associations with the severity of depression symptoms. The hierarchical regression analyses revealed that perceived social support from family, friends, and the “significant other” explained a significant part of the variance of depression over demographic variables (gender, age) and risk factors (perceived risk of COVID-19, social and emotional loneliness). Our results suggest that social support during the pandemic alleviated depression symptoms. Similar results were observed by researchers in other countries.3,37,38 All in all, our results align with the knowledge that a sense of support from others can improve coping performance and reduce perceived stress and negative mood.32
Due to the lockdown, most students probably continued their studies online in their family homes and depended on their parents. However, in our study, the greater family support predicted less severe depressive symptoms only in the Polish and Indian samples. According to our expectations, this may be partially due to collectivist cultures having stronger social support networks58 that appear to reduce symptoms of depression.59 It also aligns with the existing study on collectivist cultures having stronger family bonds.44
Our last hypothesis about social support from friends reducing the symptoms of depression regardless of cultural settings28,40,45 has been supported. Regarding structural equation modelling, there was an indirect pathway for the association between age and depression, meaning that students who perceived more social support from friends had lower depression scores. Similarly, there was an indirect pathway between social loneliness and depression symptoms severity, whereby socially lonely people perceived less social support from friends and became more depressed. These indirect associations do not nullify or minimize the direct associations between age-depression and loneliness-depression, which is consistent with the social support buffering model. The indirect negative association between age and symptoms of depression shows that the older students had fewer symptoms of depression because they could access social support from their friends more than the younger ones. These indirect pathways between age and depression and social loneliness seem primarily driven by the UK sample. As COVID-19 directly predicted depression in all three cultures, it appears that young people have been particularly affected regardless of individualist or collectivist settings. Nonetheless, the SEM clearly shows that friends’ social support can help reduce depression.
Some limitations of the current study must be acknowledged. In the cross-sectional study design, the larger number of female participants, most of whom belong to the young adult age group, limits the data generalizability. It is also plausible that the online survey attracted a disproportionate number of participants suffering from depression who sought to share their responses more than those less depressed. This study used self-reported questionnaires to measure psychiatric symptoms and did not make a clinical diagnosis. A structured clinical interview is a gold standard for establishing psychiatric and psychological diagnoses. Functional neuroimaging should be applied in the future face-to-face study after COVID-19 restrictions are removed.60,61
Despite such limitations, the current paper suggests that depression symptoms among university students in Poland, the UK, and India, were prevalent during the second pandemic wave. These findings, then, invite universities to provide much more support for students facing lockdown restrictions as the current support does not seem to adequately buffer against depression symptoms in the face of the unprecedented crisis. The most evidence-based treatment is Cognitive Behavior Therapy (CBT), especially Internet CBT.62
However, social support from parents and friends appeared to play a protective role and was associated with a lower risk of depression.63 Parents should create an atmosphere of support and encourage young people to continue their education despite the pandemic and difficulties. Creating an atmosphere of close social support should thus help improve their well-being and study performance. Our findings invite more campaigns about depression among university students, stressing the need to facilitate conditions that help them maintain close online social relations with their close contacts during times of distress, especially when offline physical contact is severely limited. Such conditions could be fostered by organizing online social meetings, well-being sessions, and online therapeutic support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Browning MH, Larson LR, Sharaievska I, et al. Psychological impacts from COVID-19 among university students: risk factors across seven states in the United States. PLoS One. 2021;16(1):e0245327. doi:10.1371/journal.pone.0245327.
2. Evans S, Alkan E, Bhangoo JK, Tenenbaum H, Ng-Knight T. Effects of the COVID-19 lockdown on mental health, wellbeing, sleep, and alcohol use in a UK student sample. Psychiatry Res. 2021;298:113819. doi:10.1016/j.psychres.2021.113819
3. Xiong J, Lipsitz O, Nasri F, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. 2020;277:55–64. doi:10.1016/j.jad.2020.08.001
4. Werner AM, Tibubos AN, Mülder LM, et al. The impact of lockdown stress and loneliness during the COVID-19 pandemic on mental health among university students in Germany. Sci Rep. 2021;11(1):22637. doi:10.1038/s41598-021-02024-5
5. Rogowska AM, Kuśnierz C, Bokszczanin A. Examining anxiety, life satisfaction, general health, stress and coping styles during COVID-19 pandemic in Polish sample of university students. Psychol Res Behav Manag. 2020;13:797–811. doi:10.2147/PRBM.S266511
6. Bu F, Steptoe A, Fancourt D. Who is lonely in lockdown? Cross-cohort analyses of predictors of loneliness before and during the COVID-19 pandemic. Public Health. 2020;186:31–34. doi:10.1016/j.puhe.2020.06.036
7. Almarzooq ZI, Lopes M, Kochar A. Virtual learning during the COVID-19 pandemic: a disruptive technology in graduate medical education. Journal of the American College of Cardiology. 2020;75(20):2635–2638. doi:10.1016/j.jacc.2020.04.015
8. Bao W. COVID ‐19 and online teaching in higher education: a case study of Peking University. Human Behav Em Technol. 2020;2(2):113–115. doi:10.1002/hbe2.191
9. Iob E, Steptoe A, Fancourt D. Abuse, self-harm and suicidal ideation in the UK during the COVID-19 pandemic. Br J Psychiatry. 2020;217(4):543–546. doi:10.1192/bjp.2020.130
10. Ren Z. Psychological Impact of COVID-19 on College Students After School Reopening: a Cross-Sectional Study Based on Machine Learning. Front Psychol. 2021;12:641806. doi:10.3389/fpsyg.2021.641806
11. Debowska A, Horeczy B, Boduszek D, Dolinski D. A repeated cross-sectional survey assessing university students’ stress, depression, anxiety, and suicidality in the early stages of the COVID-19 pandemic in Poland. Psychol Med. 2020;2:1–4. doi:10.1017/S003329172000392X
12. Hager NM, Judah MR, Milam AL. Loneliness and Depression in College Students during the COVID-19 Pandemic: boredom and Repetitive Negative Thinking as Mediators. Res Square. 2021. doi:10.21203/rs.3.rs-101533/v1
13. Ettman CK, Abdalla SM, Cohen GH, Sampson L, Vivier PM, Galea S. Prevalence of Depression Symptoms in US Adults Before and During the COVID-19 Pandemic. JAMA Network Open. 2020;3(9):1–12. doi:10.1001/jamanetworkopen.2020.19686
14. Rudenstine S, McNeal K, Schulder T, et al. Depression and anxiety during the covid‐19 pandemic in an urban, low‐income public university sample. J Trauma Stress. 2021;34(1):12–22. doi:10.1002/jts.22600
15. Elmer T, Mepham K, Stadtfeld C. Students under lockdown: comparisons of students’ social networks and mental health before and during the COVID-19 crisis in Switzerland. PLoS One. 2020;15(7):e0236337. doi:10.1371/journal.pone.0236337
16. Oh H, Marinovich C, Rajkumar R, et al. COVID-19 dimensions are related to depression and anxiety among US college students: findings from the Healthy Minds Survey 2020. J Affect Disord. 2021;292:270–275. doi:10.1016/j.jad.2021.05.121
17. Kujawa A, Green H, Compas BE, Dickey L, Pegg S. Exposure to COVID‐19 pandemic stress: associations with depression and anxiety in emerging adults in the United States. Depress Anxiety. 2020;37(12):1280–1288. doi:10.1002/da.23109
18. Vigo D, Jones L, Munthali R, et al. Investigating the effect of COVID-19 dissemination on symptoms of anxiety and depression among university students. BJPsych Open. 2021;7(2):e69. doi:10.1192/bjo.2021.24
19. Wang C, Chudzicka-Czupała A, Tee ML, et al. A chain mediation model on COVID-19 symptoms and mental health outcomes in Americans, Asians and Europeans. Sci Rep. 2021;11:6481. doi:10.1038/s41598-021-85943-7
20. Misirlis N, Zwaan M, Sotiriou A, Weber D. International Students’ Loneliness, Depression and Stress Levels in COVID-19 Crisis: the Role of Social Media and the Host University. J Contemporary Edu Theory Res. 2020;4(2):20–25. doi:10.5281/zenodo.4256624
21. Okruszek Ł, Aniszewska-Stańczuk A, Piejka A, Wiśniewska M, Żurek K. Safe but lonely? Loneliness, anxiety, and depression symptoms and COVID-19. Front Psychol. 2020;11:
22. Rauschenberg C, Schick A, Goetzl C, Roehr S, Riedel-Heller SG, Koppe G. Social isolation, mental health, and use of digital interventions in youth during the COVID-19 pandemic: a nationally representative survey. Eur Psychiatry. 2021;64(1):e20. doi:10.1192/j.eurpsy.2021.17
23. Salo AE, Junttila N, Vauras M. Social and emotional loneliness: longitudinal stability, interdependence, and intergenerational transmission among boys and girls. Fam Relat. 2020;69(1):151–165. doi:10.1111/fare.12398
24. Deng J, Zhou F, Hou W, et al. The prevalence of depressive symptoms, anxiety symptoms and sleep disturbance in higher education students during the COVID-19 pandemic: a systematic review and meta-analysis. Psychiatry Res. 2021;301:113863. doi:10.1016/j.psychres.2021.113863
25. Weiss RS. Loneliness: The Experience of Emotional and Social Isolation. Cambridge, MA, USA: The MIT Press; 1973.
26. McIntyre JC, Worsley J, Corcoran R, Harrison Woods P, Bentall RP. Academic and non-academic predictors of student psychological distress: the role of social identity and loneliness. J Mental Health. 2018;27(3):230–239. doi:10.1080/09638237.2018.1437608
27. da Silva ML, Rocha RSB, Buheji M, Jahrami H, Cunha KDC. A systematic review of the prevalence of anxiety symptoms during coronavirus epidemics. J Health Psychol. 2021;26(1):115–125. doi:10.1177/1359105320951620
28. Grey I, Arora T, Thomas J, Saneh A, Tohme P, Abi-Habib R. The role of perceived social support on depression and sleep during the COVID-19 pandemic. Psychiatry Res. 2020;293:113452. doi:10.1016/j.psychres.2020.113452
29. Kaniasty K. Social support, interpersonal, and community dynamics following disasters caused by natural hazards. Curr Opinion Psychol. 2020;32:105–109. doi:10.1016/j.copsyc.2019.07.026
30. Xu J, Ou J, Luo S, et al. Perceived Social Support Protects Lonely People Against COVID-19 Anxiety: a Three-Wave Longitudinal Study in China. Front Psychol. 2020;11:566965. doi:10.3389/fpsyg.2020.566965
31. Lakey B, Cohen S. Social support theory and measurement. In: Cohen S, Underwood LG, Gottlieb BH editors. Social Support Measurement and Intervention: A Guide for Health and Social Scientists. Oxford University Press; 2020:29–52. doi:10.1093/med:psych/9780195126709.001.0001.
32. Lakey B, Cronin A. Low Social Support and Major Depression: Research, Theory and Methodological Issues. Risk Factors in Depression. Elsevier Academic Press; 2008:385–408. doi:10.1016/B978-0-08-045078-0.00017-4
33. Labrague LJ, De Los Santos JAA, Falguera CC. Social and emotional loneliness among college students during the COVID-19 pandemic: the predictive role of coping behaviours, social support, and personal resilience. Perspectives in Psychiatric Care. 2021;57(4):1578–1584. doi:10.1111/ppc.12721
34. Basak R, Sinha D. Association between Interpersonal Social Support and Perceived Depression among Undergraduate College Students of Kolkata during Unlock Phase of COVID-19 Lockdown. EAS J PsycholBehavSci. 2020;2(6). doi:10.36349/easjpbs.2020.v02i06.003
35. Liu CH, Zhang E, Wong G, Hyun S, Hahm HC. Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: clinical implications for US young adult mental health. Psychiatry Res. 2020;290:113172. doi:10.1016/j.psychres.2020.113172
36. Ye Z, Yang X, Zeng C, et al. Resilience, social support, and coping as mediators between COVID‐19‐related stressful experiences and acute stress disorder among college students in China. Appl Psychol. 2020;12(4):1074–1094. doi:10.1111/aphw.12211
37. Lechner WV, Laurene KR, Patel S, Anderson M, Grega C, Kenne DR. Changes in alcohol use as a function of psychological distress and social support following COVID-19 related University closings. Addict Behav. 2020;110:106527. doi:10.1016/j.addbeh.2020.106527
38. Mai Y, Wu YJ, Huang Y. What Type of Social Support Is Important for Student Resilience During COVID-19? A Latent Profile Analysis. Front Psychol. 2021;12:2463. doi:10.3389/fpsyg.2021.646145
39. Li X, Wu H, Meng F, Li L, Wang Y, Zhou M. Relations of COVID-19-related stressors and social support to Chinese college students’ psychological response during the COVID-19 epidemic. Front Psychiatry. 2020;11:1084. doi:10.3389/fpsyt.2020.551315
40. Wörfel F, Gusy B, Lohmann K, Töpritz K, Kleiber D. Mental health problems among university students and the impact of structural conditions. J Public Health (Bangkok). 2016;24(2):125–133. doi:10.1007/s10389-015-0703-6
41. Goodwin R, Hou WK, Sun S, Ben-Ezra M. Psychological and behavioural responses to COVID-19: a China–Britain comparison. J Epidemiol Community Health. 2021;75(2):189–192. doi:10.1136/jech-2020-214453
42. Holmes EA, O’Connor RC, Perry VH, et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry. 2020;7(6):547–560. doi:10.1016/S2215-0366(20)30168-1
43. Ishida M, Montagni I, Matsuzaki K, et al. The association between depressive symptoms and self-rated health among university students: a cross-sectional study in France and Japan. BMC Psychiatry. 2020;20(1):549. doi:10.1186/s12888-020-02948-8
44. Kalmijn M, Saraceno C. A comparative perspective on intergenerational support: responsiveness to parental needs in individualistic and familialistic countries. Eur Soc. 2008;10(3):479–508. doi:10.1080/14616690701744364
45. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401. doi:10.1177/014662167700100306
46. Jankowski KS. Morningness-eveningness and depressive symptoms: test on the components level with CES-D in Polish students. J Affect Disord. 2016;196:47–53. doi:10.1016/j.jad.2016.02.015
47. Dryhurst S, Schneider CR, Kerr J, et al. Risk perceptions of COVID-19 around the world. J Risk Res. 2020;23(7–8):994–1006. doi:10.1080/13669877.2020.1758193
48. Gierveld JDJ, Van Tilburg T. The De Jong Gierveld short scales for emotional and social loneliness: tested on data from 7 countries in the UN generations and gender surveys. Eur J Ageing. 2010;7(2):121–130. doi:10.1007/s10433-010-0144-6
49. Grygiel P, Humenny G, Rebisz S, Świtaj P, Sikorska J. Validating the Polish adaptation of the 11-item de Jong Gierveld Loneliness Scale. Eur J Psychol Assessment. 2013;29(2):129–139. doi:10.1027/1015-5759/a000130
50. Zimet GD, Powell SS, Farley GK, Werkman S, Berkoff KA. Psychometric characteristics of the multidimensional scale of perceived social support. J Pers Assess. 1990;55(3–4):610–617. doi:10.1080/00223891.1990.9674095
51. Dambi JM, Corten L, Chiwaridzo M, Jack H, Mlambo T, Jelsma J. A systematic review of the psychometric properties of the cross-cultural translations and adaptations of the Multidimensional Perceived Social Support Scale (MSPSS). Health Qual Life Outcomes. 2018;16(1):1–19. doi:10.1186/s12955-018-0912-0
52. Cohen J. Second Wave of Coronavirus Intensifies Across Europe. Forbes; 2020. Available from: https://www.forbes.com/sites/joshuacohen/2020/10/19/second-wave-of-coronavirus-hits-europe-major-differences-in-impact-across-countries/?sh=60cf528c1542.
53. Wallen J Fears of COVID-19 second wave in India as daily cases increase again. The Telegraph; 2020. Available from: https://www.telegraph.co.uk/global-health/science-and-disease/fears-covid-19-second-wave-india-daily-cases-increase/.
54. Ważna M Druga fala epidemii uderzyła w Polskę silniej niż w Hiszpanię czy Niemcy. Medonet; 2020. Available from: https://www.medonet.pl/koronawirus/koronawirus-na-swiecie,druga-fala-epidemii-uderzyla-w-polske-silniej-niz-w-hiszpanie-czy-niemcy,artykul,41721440.html.
55. Suminanto S, Widiyanto A, Tri Darmayanti A, Arradini D, Tri Handayani R, Atmojo JT. Meta Analysis: potential Age and Gender Factors Against Depression Events in the Pandemic Time COVID-19. J Ilmu Keperawatan Jiwa. 2021;1(2):281–288.
56. Kira IA, Shuwiekh HA, Alhuwailah A, Ashby JS. The effects of COVID-19 and collective identity trauma (intersectional discrimination) on social status and well-being. Traumatology. 2021;27(1):29–39. doi:10.1037/trm0000289
57. Arnett JJ. Emerging adulthood: the winding road from the late teens through the twenties. Oxford University Press. 2004. doi:10.1093/acprof:
58. Goodwin R, Hernandez Plaza S. Perceived and received social support in two cultures: collectivism and support among British and Spanish students. J Soc Pers Relat. 2000;17(2):282–291. doi:10.1177/0265407500172007
59. Jibeen T. Perceived social support and mental health problems among Pakistani university students. Community Ment Health J. 2016;52(8):1004–1008. doi:10.1007/s10597-015-9943-8
60. Ho CSH, Lim LJH, Lim AQ, et al. Diagnostic and Predictive Applications of Functional Near-Infrared Spectroscopy for Major Depressive Disorder: a Systematic Review. Front Psychiatry. 2020;11:378. doi:10.3389/fpsyt.2020.00378
61. Ho CSH, Cornelia Yi C, Roger Cm H. Mental health strategies to combat the psychological impact of COVID-19 beyond paranoia and panic. Ann Acad Med Singapore. 2020;49(1):1–3.
62. Ho CS. Use of Cognitive Behavior Therapy (CBT) to treat psychiatric symptoms during COVID-19: mental Health Strategies to Combat the Psychological Impact of COVID-19. Beyond Paranoia and Panic. Ann Acad Med Singapore. 2020;49(3):155160.
63. Islam MA, Barna SD, Raihan H, Khan MNA, Hossain MT. Depression and anxiety among university students during the COVID-19 pandemic in Bangladesh: a web-based cross-sectional survey. PLoS One. 2020;15(8):e0238162. doi:10.1371/journal.pone.0238162
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Loneliness and Pain Catastrophizing Among Individuals with Chronic Pain: The Mediating Role of Depression
Wilson JM, Colebaugh CA, Meints SM, Flowers KM, Edwards RR, Schreiber KL
Journal of Pain Research 2022, 15:2939-2948
Published Date: 16 September 2022
Relationship Between Negative Life Events and Depressive Symptoms for Chinese College Students: The Mediating Role of Rumination and Moderating Role of Perceived Social Support and Psychological Capital
Chen G, Zhang G, Yang Y, Zhang J, Hu Y
Psychology Research and Behavior Management 2023, 16:271-282
Published Date: 2 February 2023
Improved Mental Health, Social Connections and Sense of Self: A Mixed Methods Systematic Review Exploring the Impact and Experience of Community Reminiscence Programs
Laidlaw RJ, McGrath R, Adams C, Kumar S, Murray CM
Journal of Multidisciplinary Healthcare 2023, 16:4111-4132
Published Date: 15 December 2023
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024
The Impact of Problematic Internet Use on Adolescent Loneliness-Chain Mediation Effects of Social Support and Family Communication
Gong F, Gong Z, Liu H, Yi P, Jia Y, Zhuang J, Shu J, Huang X, Wu Y
Psychology Research and Behavior Management 2024, 17:1903-1916
Published Date: 6 May 2024