Back to Journals » Psychology Research and Behavior Management » Volume 16
Relationship Between Negative Life Events and Depressive Symptoms for Chinese College Students: The Mediating Role of Rumination and Moderating Role of Perceived Social Support and Psychological Capital
Authors Chen G ![]() , Zhang G, Yang Y, Zhang J, Hu Y
, Zhang G, Yang Y, Zhang J, Hu Y
Received 14 November 2022
Accepted for publication 27 January 2023
Published 2 February 2023 Volume 2023:16 Pages 271—282
DOI https://doi.org/10.2147/PRBM.S395551
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Gongxing Chen,1,2 Guiyuan Zhang,2 Yingsi Yang,3,4 Jiamiao Zhang,2,5 Yingying Hu2
1College of Education for the Future, Beijing Normal University at Zhuhai, Zhuhai, People’s Republic of China; 2Center for Mental Health, Guangxi Vocational College of Water Resources and Electric Power, Nanning, People’s Republic of China; 3School of Economics and Management, Beijing University of Posts and Telecommunications, Beijing, People’s Republic of China; 4School of Management, Guilin University of Aerospace Technology, Guilin, People’s Republic of China; 5School of Psychology, Central China Normal University, Wuhan, People’s Republic of China
Correspondence: Yingsi Yang, Beijing University of Posts and Telecommunications, Xitucheng Road 10, Haidian District, Beijing, 100876, People’s Republic of China, Email [email protected]
Objective: External events affect individuals through their cognitive process, a model on how and when negative life events are associated with depressive symptoms was tested by considering individuals’ internal and external factors based on the conservation of resource theory (COR).
Methods: We conducted a survey to test our hypotheses. Participants were college students who were selected with the cluster sampling method and were asked to complete the scales measuring negative life events, perceived social support, psychological capital (PsyCap), rumination, and depressive symptoms in the classroom with a unit of class. A total of 764 questionnaires were distributed and returned, and 703 valid data were obtained finally.
Results: The present study found that (1) the relationship between negative life events and depressive symptoms was moderated by perceived social support negatively, such that the relationship was stronger with low perceived social support; (2) the relationship between negative life events and depressive symptoms was mediated by rumination; (3) the relationship between rumination and depressive symptoms was moderated by PsyCap negatively, such that the relationship was stronger with low PsyCap; (4) the indirect relationship between negative life events and depressive symptoms through rumination was moderated by PsyCap negatively, such that the indirect relationship got stronger with low PsyCap.
Conclusion: Rumination is an essential process for negative life events to affect depressive symptoms, PsyCap and perceived social support help alleviate the detrimental effect of negative life events from internal and external perspectives, respectively. Our research conclusion has a theoretical and practical implementation for reducing depressive symptoms in college students.
Keywords: depressive symptoms, perceived social support, rumination, psychological capital, negative life events
Introduction
The detection rate of depression among college students in China is 21.6%~37.6%,1 normal college students frequently experience depressive symptoms as well.2 College students face many negative events such as failure in academic exams, family conflicts, and disputes with friends.3 Therefore, it is necessary to examine how and when negative life events elicit depressive symptoms from both internal and external factors.
Negative Life Events and Depressive Symptoms: The Moderating Role of Perceived Social Support
Some researchers found that negative life events caused depressive symptoms,4,5 while others found that the relationship between negative life events and depressive symptomatology is not significant.6 The inconsistency reminds us that there may exist a moderator between negative life events and depressive symptoms. The stress-buffering model of social support proposed that social support can buffer the detrimental effect of negative life events on an individual’s mental health condition.7 Perceived social support was defined as the belief that help is available if needed (p.47).8 Indeed, many researchers provided evidence for the buffering effect of perceived social support in the relationship between stressful events and the negative outcomes.9,10 Therefore, our first goal is to address the inconsistency of the relationship between negative life events and depressive symptoms by considering the moderating role of perceived social support.
According to COR,11 perceived social support provides external resources for individuals to cope with negative life events by not only perceiving the events as less stressful but also responding to the events with more adjustive behavior such as asking for help with more ease,7 as they know that someone is always there to provide support and help when they are in trouble.8 Though negative life events consume an individual’s energy, perceived social support injects resources into them and thus weakens the detrimental effect of negative life events on depressive symptoms. On the contrary, individuals with lower perceived social support did not think they can get resource replenishment from external support or help when negative life events bringing them into an exhausted state,11 they are more likely to appraise the events as stressful because they need to face the negative events alone, in their opinion, no one is available to help them, the sense of helplessness lead to more depressive symptoms. Furthermore, they are more likely to adopt maladaptive behaviors to cope with negative life events, for example, they are less likely to ask for help, the maladaptive behavior is invalid which is useless for solving the problem, thus making them experience more depressive symptoms.7
Negative Life Events and Depressive Symptoms: The Mediating Role of Rumination
The causal relationship between rumination and depressive symptoms is confusing so far, for example, some researchers did not distinguish depression from rumination,12 they believed that depressive symptoms make an individual ruminate, that is, they may measure rumination using scales including items overlapping with items measuring depressive symptoms;13 some researchers used depression to predict rumination,14 while other researchers showed that rumination predicts depression15 or causes depression,16 which is mainstream in the literature of depression.17 Researchers even found a reciprocal causal relationship between rumination and depression.18 As a result, our second goal is to provide empirical evidence for the relationship between rumination and depressive symptoms by examining the mediating role of rumination in the relationship between negative life events and depressive symptoms.
When encountering negative life events, individuals may experience negative emotions and even depressive symptoms which can have a destructive effect on their everyday life.4,19 In terms of the mechanism of life events’ effect on depressive symptoms, the cognitive process has long been identified.20–22 Rumination, which is defined as a method of coping with negative moods that involve a repetitive and passive focus on one’s negative emotions,23 is such a cognitive coping strategy. Rumination has been found to play a mediating role between additional stressors one month after one’s family member’s death and depressive symptoms 5 months later.24
Our reasoning is as follows: firstly, rumination can be elicited by negative life events.25 Individuals are equipped with a tendency to think about the causes of negative life events to comprehend the world,26 the degree of rumination was highest one week after the happening of a stressful event and decreased gradually and then become lowest 6 months later. It was proposed that rumination was more easily elicited under stressful conditions such as a mid-session exam regardless of trait ruminative tendencies.27 Secondly, rumination may lead to depressive symptoms because rumination is a common coping strategy for depressed individuals.28 Researchers found that rumination positively predicted depressive symptoms for both adolescents and adults6,21 or even caused depression.29,30
Rumination and Depressive Symptoms: The Moderating Role of PsyCap
When facing a stressful situation, individuals may react very differently because of their different personal characteristics, and then lead to very different outcomes. Psychological capital (PsyCap) is such a kind of personal characteristic that we should consider when testing the relationship between rumination and depressive symptoms. Individual who possesses high PsyCap is better equipped for coping with stress from the external environment or internal psychological process31 and enjoying a more satisfied life.32,33 From the perspective of COR,34 the four types of resources help individuals buffer the detrimental effect of stress from the internal psychological process. Several researchers provided evidence for personal characteristics’ buffering effect.35,36 PsyCap is a kind of personal characteristic as well which can be treated as a resource. As a result, we reason that PsyCap may moderate the relationship between individuals’ internal cognitive process (rumination) and its outcome (depressive symptoms).
PsyCap is composed of self-efficacy, optimism, hope, and resilience which help individuals bounce back to attain success even when they are faced with challenging tasks.37 Individuals with high levels of self-efficacy are more likely to believe themselves to complete a challenging task successfully by mobilizing the motivation, cognitive resources and necessary action.38 Hope is a state which motivates individuals with goal-oriented energy and planning to meet goals, that is, individuals with a high level of hope will leave no effort to find means to meet their goals.39 The third dimension of PsyCap, optimism, involves attributing negative events to temporary factors while attributing positive events to permanent factors.38 Resilience means the ability to “bounce back” and even beyond to attain success when facing problems and adversity.40 The four dimensions make PsyCap a unique theoretical and measurable contribution to a higher-order core construct and represent one’s positive appraisal of circumstances and probability for success based on motivated effort and perseverance (p.549–550).37
We expect that the positive relationship between rumination and depressive symptoms becomes weaker when PsyCap gets higher. First, rumination makes individuals immerse in negative thoughts, and engage in self-critical activities which belong to depressive symptoms,41 however, their high PsyCap makes them more confident in the ability to cope with stressful events,38 as a result, the sense of mastery help counteracting the negative effect of rumination on depressive symptoms by helping them adopt a more positive view on their situation.42 Second, though rumination makes individuals experience repetitive and passive thoughts about negative events or goal pursuit failure,29,43 high PsyCap individual’s hope, featured with goal-directed and determined to find pathways to achieve the goals, can help them find solutions to relieve their depressive symptoms and feel better, thus buffers the effect of rumination on depressive symptoms.39 Their resilience involves finding constructive meaning and then bouncing back from setbacks or failures,44 which can not only help individuals go through the negative events but also the negative thoughts of rumination, thus reducing the individual’s depressive symptoms elicited by rumination. Third, though rumination makes individuals more self-centered and pay more attention to their negative thoughts,45 high PsyCap individual’s optimism, featured with positive attribution, helps counteracts the negative effect of rumination by paying more attention to their positive thoughts, attributing more to temporary, external, and situational factors.31
On the contrary, individuals with low PsyCap are less confident, which makes them more difficult to deal with internal stress, that is, rumination is more likely to make them experience depressive symptoms.42 Low PsyCap individuals are less optimistic and less hopeful about their future, which makes them pay more attention to the negative aspects and ignore the positive aspects, thus rumination leads to more serious depressive symptoms for them.31,39 Furthermore, low PsyCap individuals are also less resilient, which prevents them from bouncing back against failure, in such a situation, rumination is more likely to lead to more serious depressive symptoms.44
Based on what was discussed above, we propose an integrated conceptual model (see Figure 1) which aims at examining how and when negative life events influence depressive symptoms by simultaneously considering both internal and external factors based on COR (our third goal), our hypotheses are as follow:
H1: Perceived social support negatively moderates the relationship between negative life events and depressive symptoms, thus the relationship between negative life events and depressive symptoms gets stronger when perceived social support gets lower. H2: Rumination mediates the positive effect of negative life events on depressive symptoms. H3: PsyCap negatively moderates the relationship between rumination and depressive symptoms, thus the relationship between rumination and depressive symptoms gets stronger when PsyCap gets lower. H4: PsyCap moderates the indirect relationship between negative life events and depressive symptoms through rumination, thus the mediating effect of rumination between life events and depressive symptoms gets stronger when PsyCap gets lower.
 |
Figure 1 Hypothesized model. |
Methods
Participants
Participants were selected with cluster sampling method with the class as a sampling unit from five universities in a southwest province. A total of 764 questionnaires were distributed and returned. After deleting 61 data who answered the same number on the entire questionnaires, we obtained 703 (92.02%) valid responses, whose ages ranged from 17 to 25 years old (M = 19.05, SD = 1.29), other characteristics of participants are played in Table 1. All procedures performed in studies involving human participants were approved by the ethical standards of the institutional research committee of Guangxi Vocational College of Water Resources and Electric Power and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consents were obtained from the study participants.
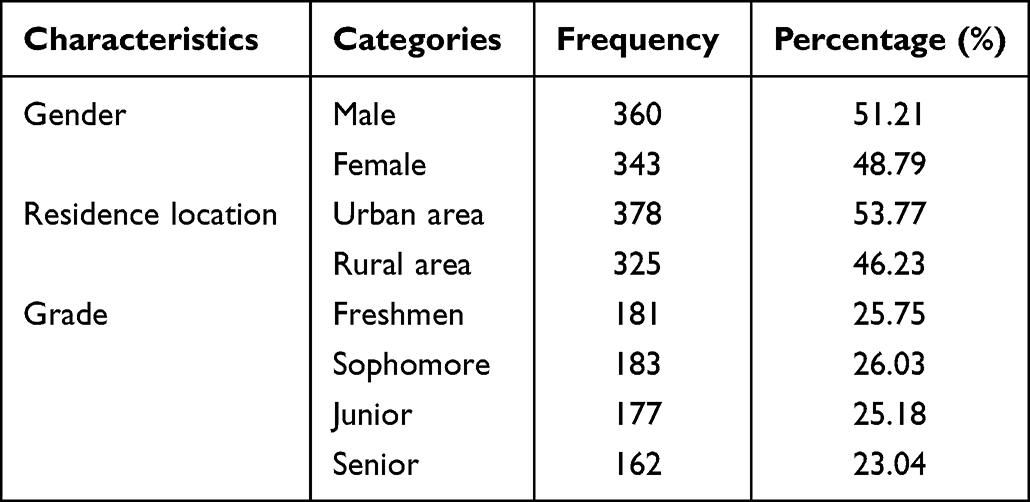 |
Table 1 Characteristics of Participants |
Procedure
Psychological researchers who had been trained before administering the survey collected data with a unit of the class. Upon arriving at the classroom, psychological researchers read the instruction and requirements to participants, then participants scanned the QR code which was shown on the screen in front of the classroom to complete the measurement with their mobile phones anonymously. Uniform instruction was applied for all participants to rule out confounding effect, the duration of survey was set as no less than 20 minutes to make sure that participants answered carefully, and those whose duration of answering was less than 10 minutes were dropped.
Measurements
Negative Life Events
The 27-item Adolescent Self-Rating Life Events Checklist (ASLEC) developed by Liu et al46 was used to assess 13~20-year-old participants’ stress. Researchers showed that the scale can also be applied to participants who are more than 20 years old.3,47 It is a 6-point Likert scale. Sample items (events) are “Being misunderstood by others” and “Failure in examination”.
Rumination
A 10-item Chinese version of the Ruminative Responses Scale (RRS) developed by Treynor et al13 was used to measure the participants’ tendency to ruminate in response to their symptoms of negative emotion. It is a 4-point Likert scale. The 10-item version includes two dimensions: reflective pondering and brooding, and 5 items for each dimension. Sample items are “Think about a recent situation, wishing it had gone better” and “Go someplace alone to think about my feelings”.
PsyCap
A 26-item Positive Psychological-Capital Questionnaire (PPQ) developed by Luthans et al37 was used to assess participants’ PsyCap. It is a 7-point Likert scale. The scale includes four dimensions: self-efficacy (7 items), resilience (7 items), hope (6 items), and optimism (7 items). Sample items are “I always finish my task very well” and “I’m full of hope for my future”.
Perceived Social Support
A 12-item Multidimensional Scale of Perceived Social Support (MSPSS) developed by Zimet et al48 was used to assess participants’ perceived social support. It is a 7-point Likert scale. The scale includes three subscales: family, friends, and significant other. Sample items are “My family tries to help me” and “I can count on my friends when things go wrong”.
Depressive Symptoms
A 20-item Center for Epidemiologic Studies Depression Scale (CES-D) was developed by Radloff49 to measure participants’ depressive symptomatology. It is a 4-point Likert scale. The total score is 0 to 60. The higher the score, the higher the level of depression. A score of 28 was used as the cut-off point for depression.50 Sample items are “I thought my life had been a failure” and “I felt sad”.
Results
Common Method Variance Testing
Our data were all self-reported by college students, it is necessary to estimate the effects of common method variance. Firstly, participants completed the measurements anonymously to minimize the effects of common method variance.51 Secondly, Harman’s single-factor test was employed.51 We performed a factor analysis on all items, extracted eighteen factors with eigenvalues greater than one. Furthermore, no general factor was apparent in the unrotated factor structure, with Factor 1 accounting for 18.54% of the variance. Thus, common method variance is not of great concern in the present study.
Test of Confirmatory Factor Analysis (CFA) of Measurements
We used Mplus 8.3 to perform a confirmatory factor analysis (CFA) for all variables. The fit index of measurements in Table 2 were all acceptable.
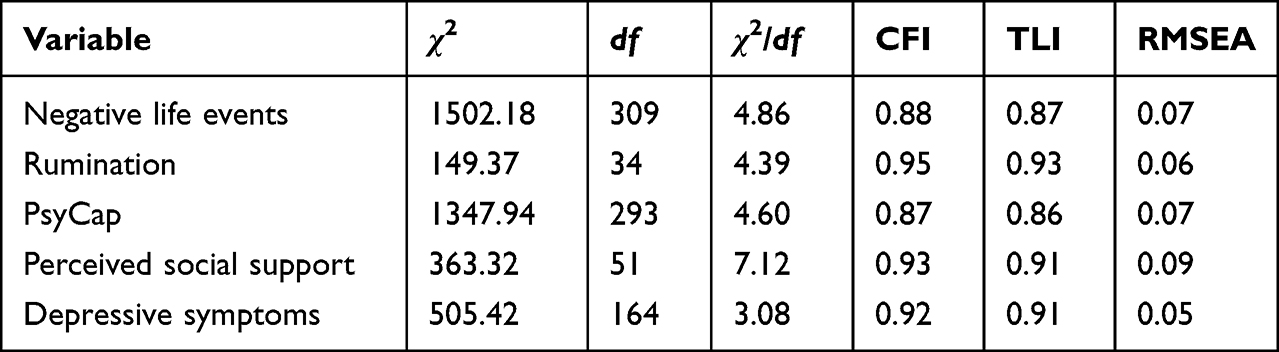 |
Table 2 Results of CFA |
Descriptive Statistics Analysis
We used SPSS 24.0 to perform descriptive statistics on variables. Table 3 presents all variables’ means, standard deviations, correlations, and reliability estimates. The average score of CES-D of the participants was 14.44, which was significantly less than the depression cut-off point of 28 (t = - 41.52, p < 0.001), suggesting that the depression level of our participants of college students was different from clinical clients.50 Negative life events were positively related to rumination (r = 0.29, p < 0.001), and rumination was positively related to depressive symptoms (r = 0.29, p < 0.001), these results provided preliminary support for H2.
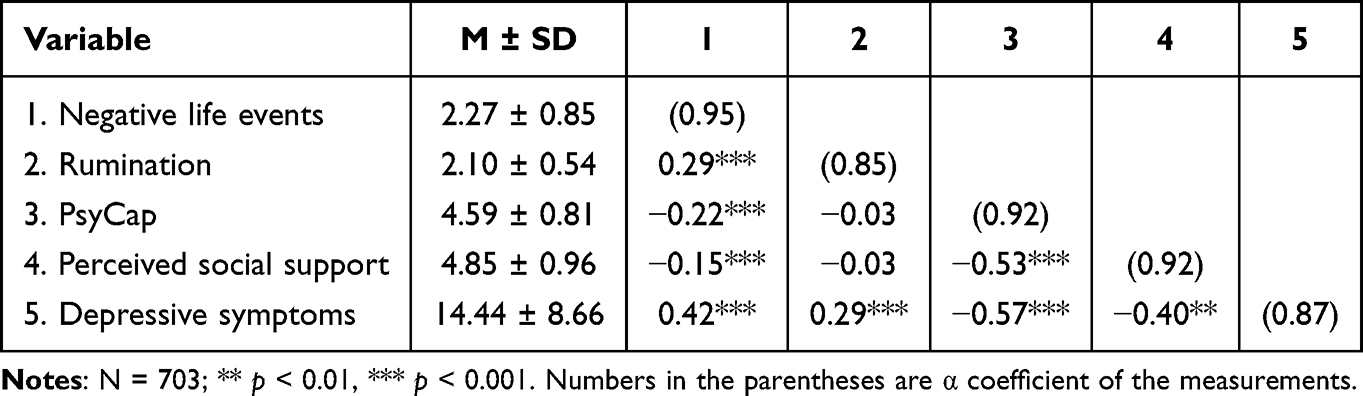 |
Table 3 Descriptive Statistics, Correlations, and Reliabilities |
Hypotheses Testing
We Used Mplus 8.3 to Test the Hypotheses
Hypothesis 1 predicted that perceived social support moderates the relationship between negative life events and depressive symptoms. The interaction term of negative life events and perceived social support was negative and significant (B = - 0.11, SE = 0.04, p <0.01) in predicting depressive symptoms, thus H1 was supported. As illustrated in Figure 2, the simple slope test results indicated that, when perceived social support was low, the relationship between negative life events and depressive symptoms was stronger (B = 0.48, SE = 0.05, p<0.001, 95% CI = [0.38, 0.58]); whereas when perceived social support was high, the relationship between negative life events and depressive symptoms was weaker (B = 0.26, SE = 0.06, p<0.001, 95% CI = [0.14, 0.39]). Furthermore, the difference between the two effects of negative life events on depressive symptoms in conditions of high and low perceived social support was significant (difference = 0.22, SE = 0.09, p <0.01, 95% CI = [0.05, 0.39]).
 |
Figure 2 Interaction effect of negative life events and perceived social support on depressive symptoms. |
Hypothesis 2 predicted that rumination mediates the relationship between negative life events and depressive symptoms. We used bootstrapping to test the indirect effect of negative life events on depressive symptoms through rumination. The results showed that the indirect effect was significant (Indirect effect = 0.05, SE = 0.02, 95% CI= [0.03, 0.09]), suggesting that rumination mediated the relationship between negative life events and depressive symptoms, thus H2 was supported.
Hypothesis 3 predicted that PsyCap moderates the relationship between rumination and depressive symptoms. The interaction term of rumination and PsyCap was negative and significant (B = - 0.12, SE = 0.04, p <0.01) in predicting depressive symptoms, thus H3 was supported. As illustrated in Figure 3, the simple slope test results indicated that, when PsyCap was low, the relationship between rumination and depressive symptoms was stronger (B = 0.45, SE = 0.06, p<0.001, 95% CI = [0.33, 0.58]), whereas when PsyCap was high, the relationship between rumination and depressive symptoms was weaker (B = 0.20, SE = 0.05, p<0.001, 95% CI = [0.12, 0.30]). Furthermore, the difference between the two effects of rumination on depressive symptoms in conditions of high and low PsyCap was significant (difference = 0.25, SE = 0.08, p <0.01, 95% CI = [0.09, 0.40]).
 |
Figure 3 Interaction effect of rumination and PsyCap on depressive symptoms. |
Hypothesis 4 predicted that PsyCap negatively moderates the indirect effect of negative life events on depressive symptoms through rumination. We used bootstrapping to test this hypothesis. As shown in Table 4, when PsyCap was low, the indirect effect was stronger (estimate = 0.11, 95% CI = [0.07, 0.16]), whereas when PsyCap was high, the indirect effect was weaker (estimate = 0.04, 95% CI = [0.02, 0.07]). Furthermore, the difference between the two indirect effects was significant (difference = 0.07, 95% CI = [0.03, 0.12]). Thus, H4 was supported.
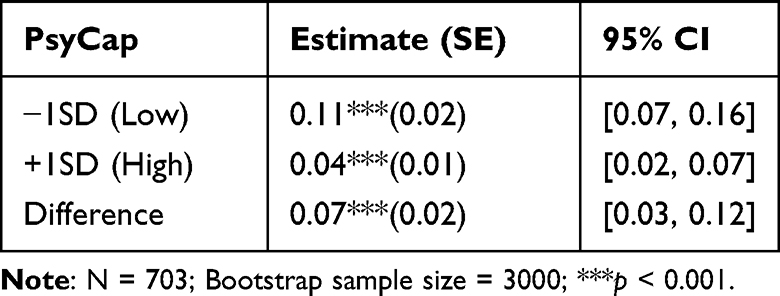 |
Table 4 Bootstrapped 95% CI for the Conditional Indirect Effect of Life Events on Depressive Symptoms Through Rumination at Low and High PsyCap |
Discussion
Whether negative life events predict depressive symptoms positively or not is still unclear yet. Several studies provided evidence for a positive relationship between negative life events and depression,4,52 while Garnefski et al did not find a significant relationship between them.6 To address this inconsistency, we considered perceived social support as a moderator between them and found that perceived social support helped inject resources from the external environment and buffered the detrimental effect of negative life events based on COR, thus the relationship between negative life events and depressive symptoms became weaker when perceived social support got high rather than low. As a result, we provided evidence to address the inconsistency of the relationship between negative life events and depressive symptoms, we contributed to perceived social support literature as well.
Researchers have long proved that negative life events can lead to depression4,19 and have proposed several mechanisms for how negative life events influence depressive symptoms through the cognitive process.20,21,53 The results of the present study confirmed the opinion that cognition played an important role in the relationship between environmental stimuli and outcomes.20,21,53 Furthermore, we proposed a new mechanism by considering the mediating role of rumination which is different from cognitive appraisal20 or automatic thought.53 Cognitive appraisal and automatic thought can be positive or negative;20,53 automatic thought can generate more positive effects when intervened appropriately. Beck proved that cognitive therapy decreased depression significantly by instructing clients to transfer their automatic thought from negative to positive.53 While rumination, which is featured repetitive thoughts of a bad situation, is merely negative that can lead to depressive symptoms more straightforwardly. The present study was consistent with the findings of the study which found that rumination mediated the relationship between additional stress and depressive symptoms as well.24 Generally, we made contribution to negative life events and depression literature by providing a new mechanism in which we consider the mediating role of rumination. We also provide empirical evidence for addressing the confusing causal relationship between rumination and depressive symptoms.
Rumination had long been considered in depression literature in depressive samples.21,29,41 While we proposed that rumination, as a cognitive process, was not exclusive in depressive samples, it can also be experienced by ordinary people which was supported by our results from college students. For ordinary people, rumination is associated with depressive symptoms though it does not reach the diagnostic standard of depression disorder54 and our finding is consistent with it. In summary, we contributed to rumination literature by testing its negative effect on ordinary people.
Individuals are faced with lots of stressors in their environment and they must cope with them successfully to survive, as a result, positive personal characteristics which can be treated as an internal resource are of extreme importance. According to COR, personal characteristics resources may buffer the negative effect of stress34 and several empirical studies found that PsyCap played a buffering role between the relationship of stress and its negative outcomes,55–58 our findings were consistent with them. Specially, we found that PsyCap buffered the negative effect of rumination on depressive symptoms and the indirect effect of negative life events on depressive symptoms through rumination. Individuals with higher PsyCap experience fewer depressive symptoms than those with lower PsyCap when they ruminate, rumination also generated less negative mediating effect on depressive symptoms for them when encountering negative life events. As a result, we contributed to COR literature by providing evidence of personal characteristics resources like PsyCap which helped buffer the negative effect of environmental and cognitive stimuli, we also contributed to depression literature by considering enhancing individuals’ PsyCap which buffered negative variables’ effect on depressive symptoms. By considering the moderating effect of perceived social support and PsyCap, our integrated model investigated both the external and internal boundary conditions simultaneously.
Beck made a great contribution to depression therapy with cognitive therapy by training clients to form more positive automatic thinking because depressive individuals always have a negative automatic thought when they encounter life events no matter positive, neutral, or negative.53 Following his steps, we found that rumination plays a significant role between negative life events and depressive symptoms and we proved that individuals’ depressive symptoms may be relieved by learning to ruminate less or divide attention to other things when encountering negative life events. Studies showed that individuals experienced fewer depressive symptoms when they were asked to perform a distracted task after negative life events than those who were asked to ruminate.29,30 As a result, we contributed to depression literature by considering changing individuals’ ruminations.
Implications
The present study made three theoretical contributions. Firstly, we tried to address the inconsistency of the relationship between negative life events and depressive symptoms by considering an external factor, that is, perceived social support as a moderator; secondly, we explored the “black box” between objective environment and depressive symptoms by considering a different cognitive construct (ie, rumination) which allowed us to better understand the mechanism of how negative life events influence depressive symptoms; thirdly, we sought to provide new insights into the relationship between negative life events and depressive symptoms through rumination by adopting COR theory in which PsyCap served as a personal characteristics resource and buffered the negative effect of life events and rumination on depressive symptoms. In doing so, we contributed to the literature on life events, rumination, and depressive symptoms by identifying internal (ie PsyCap) and external factors (ie perceived social support) as boundary conditions.
Limitations and Future Directions
Though we made several contributions, we acknowledge limits existed in our study. Our data were all collected in the form of self-report which put us at risk of suffering the interference of common method biases. Though we performed Harman’s single-factor test which showed that we were free of the interference of common method biases, we still suggest researchers measure the variables by more objective means like multi-source measurement (ie rated by subjects’ teachers or parents) in the future. We collected data from the variables at the same time which made it unable to generate causal conclusions encountering negative life events, ruminating, and then experiencing depressive symptoms, this should be a process in time series, researchers can design longitudinal research to test it in the future. Negative life events do not always lead to rumination, future research should explore conditions in which negative life events do not lead to rumination by considering personal characteristics (ie, competence and need for achievement) and external environment factors (ie, social support and academic stress).
Conclusion
The present study tested how and when negative life events lead to depressive symptoms, results supported all of our hypotheses. Firstly, perceived social support moderated the relationship between negative life events and depressive symptoms negatively, which provided empirical evidence for addressing the inconsistency of the relationship between negative life events and depressive symptoms; secondly, we found that rumination mediated the relationship between negative life events and depressive symptoms, which provided empirical evidence for addressing the confusing conclusion about the relationship between rumination and depressive symptoms; thirdly, PsyCap moderated both the direct effect of rumination on depressive symptoms and the indirect effect of negative life events on depressive symptoms through rumination, with perceived social support moderating the relationship between negative life events and depressive symptoms at the same time, which provided insight for buffering the negative effect of negative life events on depressive symptoms from both the internal and external factors.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Compliance with Ethical Standards
All procedures performed in studies involving human participants were by the ethical standards of the institutional research committee of Guangxi Vocational College of Water Resources and Electric Power and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual adult participants included in the study.
Funding
This project was funded and supported by the Theoretical and Practical Research on Ideological and Political Education for College Students in Guangxi Province (2021SZ061); Funding Program of Guilin University of Aerospace Technology (XJ22KT12); Guangxi University Young and Middle-aged Teachers’ Scientific Research Basic Ability Promotion Project (2022KY1083); Teaching Reform and Scientific Research Project of Guangxi Vocational College of Water Resources and Electric Power (2021yb34).
Disclosure
The authors declare that they have no conflict of interest.
References
1. Tang H, Ding L-L, Song X-L, et al. Meta-analysis of detection rate of depressed mood among Chinese college students from 2002 to 2011. J Jilin Univ. 2013;39(5):965–969.
2. Liu H, Ye B, Hu Y. Stressful life events and depression during the recurrent outbreak of COVID-19 in China: the mediating role of grit and the moderating role of gratitude. Psychol Res Behav Manag. 2022;15:1359–1370. doi:10.2147/PRBM.S360455
3. Sun J-W, Xue J-M, Bai H-Y, Zhang -H-H, Lin P-Z, Cao F-L. The association between negative life events, neuroticism and aggression in early adulthood. Pers Individ Dif. 2016;102:139–144.
4. Friis RH, Wittchen H-U, Pfister H, Lieb R. Life events and changes in the course of depression in young adults. Eur Psychiatry. 2002;17:241–253.
5. Marazziti D, Avella MT, Mucci N, et al. Impact of economic crisis on mental health: a 10-year challenge. CNS Spectr. 2021;26(1):7–13.
6. Garnefski N, Boon S, Kraaij V. Relationships between cognitive strategies of adolescents and depressive symptomatology across different types of life event. J Youth Adolesc. 2003;32(6):401–408.
7. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310–357.
8. Calvete E, Connor-Smith JK. Perceived social support, coping, and symptoms of distress in American and Spanish students. Anxiety Stress Coping. 2006;19(1):47–65.
9. Shi B. Perceived social support as a moderator of depression and stress in college students. Soc Behav Pers. 2021;49(1):1–9.
10. Zhao S, Peng L. Feeling matters: perceived social support moderates the relationship between personal relative deprivation and depressive symptoms. BMC Psychiatry. 2021;345(21):1–10.
11. Halbesleben JRB, Neveu J-P, Paustian-Underdahl SC, Westman M. Getting to the “COR”: understanding the role of resources in conservation of resources theory. J Manage. 2014;40(5):1334–1364. doi:10.1177/0149206314527130
12. Zhou HX, Chen X, Shen YQ, et al. Rumination and the default mode network: meta-analysis of brain imaging studies and implications for depression. Neuroimage. 2020;206:1–43. doi:10.1016/j.neuroimage.2019.116287
13. Treynor W, Gonzalez R, Nolen-Hoeksema S. Rumination reconsidered: a psychometric analysis. Cognit Ther Res. 2003;27(3):247–259. doi:10.1023/A:1023910315561
14. Liu D, Liu S, Deng H, et al. Depression and suicide attempts in Chinese adolescents with mood disorders: the mediating role of rumination. Eur Arch Psychiatry Clin Neurosci. 2022;2022:1.
15. Rodenas-Perea G, Velasco-Barbancho E, Perona-Garcelan S, et al. Childhood and adolescent trauma and dissociation: the mediating role of rumination, intrusive thoughts and negative affect. Scand J Psychol. 2022;2022:1.
16. Kong T, He Y, Auerbach RP, McWhinnie CM, Xiao J. Rumination and depression in Chinese university students: the mediating role of overgeneral autobiographical memory. Pers Individ Dif. 2015;77:221–224. doi:10.1016/j.paid.2014.09.035
17. Olatunji BO, Naragon-Gainey K, Wolitzky-Taylor KB. Specificity of rumination in anxiety and depression: a multimodal meta-analysis. Clin Psychol Sci Pract. 2013;20(3):225–257.
18. Moberly NJ, Watkins ER. Ruminative self-focus and negative affect: an experience sampling study. J Abnorm Psychol. 2008;117(2):314–323. doi:10.1037/0021-843X.117.2.314
19. Stroud CB, Davila J, Moyer A. The relationship between stress and depression in first onsets versus recurrences: a meta-analytic review. J Abnorm Psychol. 2008;117(1):206–213. doi:10.1037/0021-843X.117.1.206
20. Lazarus RS. On the primacy of cognition. Am Psychol. 1984;39:124–129. doi:10.1037/0003-066X.39.2.124
21. Kraaij V, Garnefski N, Wilde EJD, et al. Negative life events and depressive symptoms in late adolescence: bonding and cognitive coping as vulnerability factors? J Youth Adolesc. 2003;32(3):185–193. doi:10.1023/A:1022543419747
22. Hjartarson KH, Snorrason I, Bringmann LF, Olafsson RP. Automaticity and depression: daily mood-reactive rumination in people with and without depression history. J Psychopathol Clin Sci. 2022;131(4):327–340. doi:10.1037/abn0000752
23. Nolen-Hoeksema S, Wisco BE, Lyubomirsky S. Rethinking Rumination. Perspect Psychol Sci. 2008;3(5):400–424. doi:10.1111/j.1745-6924.2008.00088.x
24. Nolen-Hoeksema S, Parker LE, Larson J. Ruminative coping with depressed mood following loss. J Pers Soc Psychol. 1994;67(1):92–104. doi:10.1037/0022-3514.67.1.92
25. Watkins ER, Roberts H. Reflecting on rumination: consequences, causes, mechanisms and treatment of rumination. Behav Res Ther. 2020;127:1–28.
26. Garnefski N, Kraaij V, Spinhoven P. Negative life events, cognitive emotion regulation and emotional problems. Pers Individ Dif. 2001;30:1311–1327. doi:10.1016/S0191-8869(00)00113-6
27. Guastella AJ, Moulds ML. The impact of rumination on sleep quality following a stressful life event. Pers Individ Dif. 2007;42(6):1151–1162. doi:10.1016/j.paid.2006.04.028
28. Nolen-Hoeksema S. Responses to depression and their effects on the duration of depressive episodes. J Abnorm Psychol. 1991;100(4):569–582. doi:10.1037/0021-843X.100.4.569
29. Nolen-Hoeksema S, Morrow J. Effects of rumination and distraction on naturally occurring depressed mood. Cogn Emot. 1993;7(6):561–570.
30. Morrow J, Nolen-Hoeksema S. Effects of responses to depression on the remediation of depressive affect. J Pers Soc Psychol. 1990;58(3):519–527.
31. Luthans F, Avey JB, Patera JL. Experimental analysis of a Web-based training intervention to develop positive psychological capital. Acad Manag Learn Educ. 2008;7(2):209–221.
32. Luthans F, Avolio BJ, Walumbwa FO, Li W. The psychological capital of Chinese workers: exploring the relationship with performance. Manag Organ Rev. 2005;1(2):249–271.
33. Larson M, Luthans F. Potential added value of psychological capital in predicting work attitudes. J Leadersh Organ Stud. 2006;13(2):75–92.
34. Hobfoll SE. The influence of culture, community, and the nested-self in the stress process: advancing conservation of resources theory. Appl Psychol. 2001;50(3):337–421.
35. Van Yperen NW, Snijders TA. A multilevel analysis of the demands--control model: is stress at work determined by factors at the group level or the individual level? J Occup Health Psychol. 2000;5(1):182–190.
36. Pierce JL, Gardner DG. Self-esteem within the work and organizational context: a review of the organization-based self-esteem literature. J Manage. 2004;30(5):591–622.
37. Luthans F, Avolio BJ, Avey JB, Norman SM. Positive psychological capital: measurement and relationship with performance and satisfaction. Pers Psychol. 2007;60(3):541–572.
38. Luthans F, Luthans KW, Luthans BC. Positive psychological capital: beyond human and social capital. Bus Horiz. 2004;47(1):45–50.
39. Snyder CR, Harris C, Anderson JR, et al. The will and the ways: development and validation of an individual-differences measure of hope. J Pers Soc Psychol. 1991;60(4):570–585.
40. Luthans F, Vogelgesang GR, Lester PB. Developing the psychological capital of resiliency. Hum Resour Dev Rev. 2006;5(1):25–44.
41. Lyubomirsky S, Tucker KL, Caldwell ND, Berg K. Why ruminators are poor problem solvers: clues from the phenomenology of dysphoric rumination. J Pers Soc Psychol. 1999;77(5):1041–1060.
42. Shen YE. Relationships between self-efficacy, social support and stress coping strategies in Chinese primary and secondary school teachers. Stress Health. 2009;25(2):129–138.
43. Liang LH, Hanig S, Evans R, Brown DJ, Lian H. Why is your boss making you sick? A longitudinal investigation modeling time-lagged relations between abusive supervision and employee physical health. J Organ Behav. 2018;39(9):1050–1065.
44. Tugade MM, Fredrickson BL. Resilient individuals use positive emotions to bounce back from negative emotional experiences. J Pers Soc Psychol. 2004;86(2):320–333.
45. Pingel R, Fay D, Urbach T. A resources perspective on when and how proactive work behaviour leads to employee withdrawal. J Occup Organ Psychol. 2019;92(2):410–435.
46. Liu X, Liu L, Yang J, Chai F, Wang A. Development and reliability-validity testing of adolescent self-rating life events checklist. Shandong Psychiatry. 1997;10(1):15–19.
47. Xia L-X, Ding C, Hollon SD, Wan L. Self-supporting personality and psychological symptoms: the mediating effects of stress and social support. Pers Individ Dif. 2013;54(3):408–413.
48. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. 1988;52(1):30–41.
49. Radloff LS. The CES-D Scale. Appl Psychol Meas. 1977;1(3):385–401.
50. Radloff LS. The use of the center for epidemiologic studies depression scale in adolescents and young adults. J Youth Adolesc. 1991;20(2):149–166.
51. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903.
52. Nazroo JY, Edwards AC, Brown GW. Gender differences in the onset of depression following a shared life event: a study of couples. Psychol Med. 1997;27:9–19.
53. Beck JS. Cognitive Therapy: Basic and Beyond. New York: Guilford Press; 1995.
54. Garnefski N, Legerstee J, Kraaij VV, Van Den Kommer T, Teerds J. Cognitive coping strategies and symptoms of depression and anxiety: a comparison between adolescents and adults. J Adolesc. 2002;25(6):603–611.
55. Roberts SJ, Scherer LL, Bowyer CJ. Job stress and incivility. J Leadersh Organ Stud. 2011;18(4):449–458.
56. Zhou Y, Gao J, Chen Y. Psychological Capital Moderate the Influence of Job Satisfaction on Performance. International Conference on Computer Science and Service System. IEEE; 2012.
57. Valdersnes KB, Eid J, Hystad SW, Nielsen MB. Does psychological capital moderate the relationship between worries about accidents and sleepiness? Int Marit Health. 2017;68(4):245–251.
58. Megeirhi HA, Kilic H, Avci T, Afsar B, Abubakar AM. Does team psychological capital moderate the relationship between authentic leadership and negative outcomes: an investigation in the hospitality industry. Econ Res Ekon Istraz. 2018;31(1):927–945.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Depression, Perceived Risk of COVID-19, Loneliness, and Perceived Social Support from Friends Among University Students in Poland, UK, and India
Bokszczanin A, Palace M, Brown W, Gladysh O, Tripathi R, Shree D
Psychology Research and Behavior Management 2023, 16:651-663
Published Date: 9 March 2023
Quality of Life Status and Its Influencing Factors Among Lung Cancer Chemotherapy Patients in China: A Cross-Sectional Study
Xu F, Zhong X, Li Q, Luo X, Wang N, Wang J, Xie S, Zhang J
Cancer Management and Research 2025, 17:603-615
Published Date: 17 March 2025