Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 15
Depression in Saudi Patients with Rheumatoid Arthritis
Authors Alharbi S ![]()
Received 20 November 2022
Accepted for publication 21 January 2023
Published 26 January 2023 Volume 2023:15 Pages 1—9
DOI https://doi.org/10.2147/OARRR.S397489
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Samar Alharbi
Department of Medicine, College of Medicine, Taibah University, Medina, Saudi Arabia
Correspondence: Samar Alharbi, Department of Medicine, Taibah University, Medina, 42312-3779, Saudi Arabia, Tel +96 6553018777, Fax +96 648461172, Email [email protected]
Purpose: Depression is the most common psychiatric disorder associated with rheumatoid arthritis (RA). However, little is known about its prevalence and risk factors among Saudi patients, specifically. Therefore, this study sought to determine the prevalence and predictors of depression in patients with RA in Saudi Arabia.
Patients and Methods: A cross-sectional study was conducted with patients registered at the Saudi Charitable Association for Rheumatic Diseases. Inclusion criteria were that the patients either met the American College of Rheumatology 1987 revised criteria for the classification of RA or the 2010 RA classification criteria. Demographic data and clinical variables were collected, and Beck’s 21-item Depression Inventory was used to assess for depression.
Results: Of the 210 participants with RA, 171 were women (81.4%), and 39 were men (18.6%). The prevalence of depression was 68%. There were significant relationships between age, gender, marital status, and having depression. Rheumatoid factor (RF) was positive in 144 participants (68.6%), which positively correlated with the risk of having depression (P value < 0.001). Moreover, depression severity correlated with age, gender, marital status, RF positivity, and prolonged disease duration.
Conclusion: Based on the results, depression is highly prevalent in Saudi patients with RA, especially those with positive RF and those who are female, middle-aged, and divorced. Early detection and treatment of depression in patients with RA is highly recommended to improve their quality of life and avoid unfavorable effects on RA clinical progression.
Keywords: rheumatoid arthritis, depression, rheumatoid factor, Beck’s 21-item depression inventory
Introduction
Depression is one of the most common complications of chronic illnesses. Rheumatoid arthritis (RA) is a chronic, systemic autoimmune disease of unknown etiology, which is three times more likely to affect women than men. It typically commences between the ages of 30 and 50 years.
The prevalence of RA worldwide is 0.2–1.2%, and according to one study conducted in the Qassim region, 2.2 per 1000 individuals are affected in Saudi Arabia.1,2 Furthermore, depression is more common in patients with RA than in the general population.3 Previous studies have reported a wide range in the prevalence of depression among patients with RA, with estimates between 9.5% and 41.5%.4,5 One study (conducted in a single center) estimated the prevalence of depression in Saudi Arabia to be 18%, which was more prevalent in patients with high disease activity.6
Among patients with RA who received inadequate treatment, 20% became severely disabled, and 35% died within 20 years. Additionally, patients with RA and coexisting depression have poor long-term prognoses and engage in increased health services utilization. Having both RA and depression is also associated with more comorbidities.7–10 In addition, it is well known that the combination of depression and RA is associated with increased mortality rates.9,11
This study investigated the prevalence of depression in Saudi patients with RA and determined the demographic and clinical characteristics associated with depression. Understanding the prevalence of depression is key to early diagnosis and intervention to improve the quality of life for patients with RA in Saudi Arabia.
Patients and Methods
Study Design and Setting
A cross-sectional study was conducted among patients with RA who were registered at the Saudi Charitable Association for Rheumatic Diseases between January and June 2021. The Saudi Charitable Association for Rheumatic Diseases is considered the first of its kind in Saudi Arabia, and its services are available in all regions of the country. It is registered with the Ministry of Human Resources and Social Affairs and is a member of the United Nations Program, the NCD, and the regional network. Additionally, it provides health assistance to patients with rheumatological diseases, and provides permanent assistance to patients (and their families) in need of financial support. Moreover, the Saudi Charitable Association for Rheumatic Diseases purchases, provides, and distributes medication, in addition to supporting further research in the field.
Inclusion criteria were patients aged 18 years or older and who were diagnosed with RA. A requirement was also that diagnoses were made according to either the American College of Rheumatology 1987 revised criteria for the classification of RA or the 2010 RA classification criteria.12,13 Exclusion criteria included patients diagnosed with depression or other psychiatric illnesses before their RA diagnosis and patients with hypothyroidism or malignancies.
Sample Size
The sample size was calculated using the prevalence of depression among patients with RA from a previous study (18%).6 Using Epi Info version 7.2.5.0, the sample size was calculated to be at least 227 at a confidence level of 95% and an acceptable margin of error of 5%.
Data Collection
Data on patients were gathered using a standardized data collection form that was developed and administered using Google Forms. The form included questions on demographic information, clinical characteristics, and relevant variables such as gender, age, occupation, marital status, education, disease duration (defined from RA diagnosis) (≤2 years for early disease or >2 years for established disease), age at RA diagnosis, and the presence of rheumatoid factor (RF). The online survey was made available to the Saudi Charitable Association for Rheumatic Diseases and completed by accessible patients (who met the inclusion criteria) until the target sample size was met. Participants completed the questionnaires, and the responses were transferred to the final database and downloaded as a Microsoft Excel sheet.
Assessment of Depression
To assess depression, we used the Arabic version of Beck’s 21-item Depression Inventory (BDI), which is a well-known self-reported rating system. The original 21-item version was introduced in 1961,14 and its reliability and validity have been established across a broad spectrum of clinical and non-clinical populations.15 The tool consists of 21 questions (for a total of 63 points) with score categories of “No depression” (0 to 13), as well as “Mild” (14 to 19), “Moderate” (20 to 28), and “Severe depression” (29 to 63). The Arabic version of the BDI has been tested and validated on Arabic-speaking patients.16
Ethical and Administrative Considerations
The study was conducted in accordance with the Declaration of Helsinki of 1975 and was approved by the Institutional Review Board of the Ministry of Health, General Directorate of Health Affairs in Madinah (protocol code IRB 566, approved on November 17, 2020). All participants were informed about the purpose of the questionnaire, and consent was obtained through their voluntary completion of the questionnaire.
Statistical Analysis
All analyses were conducted using the IBM SPSS Statistics software version 25.0 (Armonk, NY, USA). Quantitative data were presented as means and standard deviations, and qualitative data were presented as frequencies and proportions. Normality was tested using the Kolmogorov–Smirnov test and if there was statistically significant deviation from the norm, then data were non-normally distributed. Pearson’s Chi-squared test was used to analyze the qualitative variables. Odds ratios (ORs) and 95% confidence intervals were used to assess the risk of patient characteristics being independent determinants of depression. Binary logistic regression was used to assess significant predictors via multivariate analysis, and Spearman correlation coefficient was used to assess the relationship between duration and total depression score. A P value of ˂0.05 was accepted as statistically significant.
Results
This study comprised 210 participants with RA, and had a response rate of 92.5% (210/227). The mean age (± standard deviation, SD) of the participants was 46.29 (±11.44) years old with 171 patients being women (81.4%) and 39 being men (18.6%). Of all the patients, 136 (64.8%) were married, 103 (49.0%) had completed higher education, and 151 (71.9%) were working. Disease duration was less than two years in 78 (37.1%) patients and more than two years in 132 (62.9%) patients. RF was positive in 144 (68.6%) of the participants. Participants’ demographic and clinical characteristics are summarized in Table 1. The prevalence of depressive symptoms among the participants was 68%. As assessed by the BDI, the numbers of participants that experienced mild, moderate, and severe depression were 37 (17.6%), 61 (29.0%), and 45 (21.4%), respectively (Table 2).
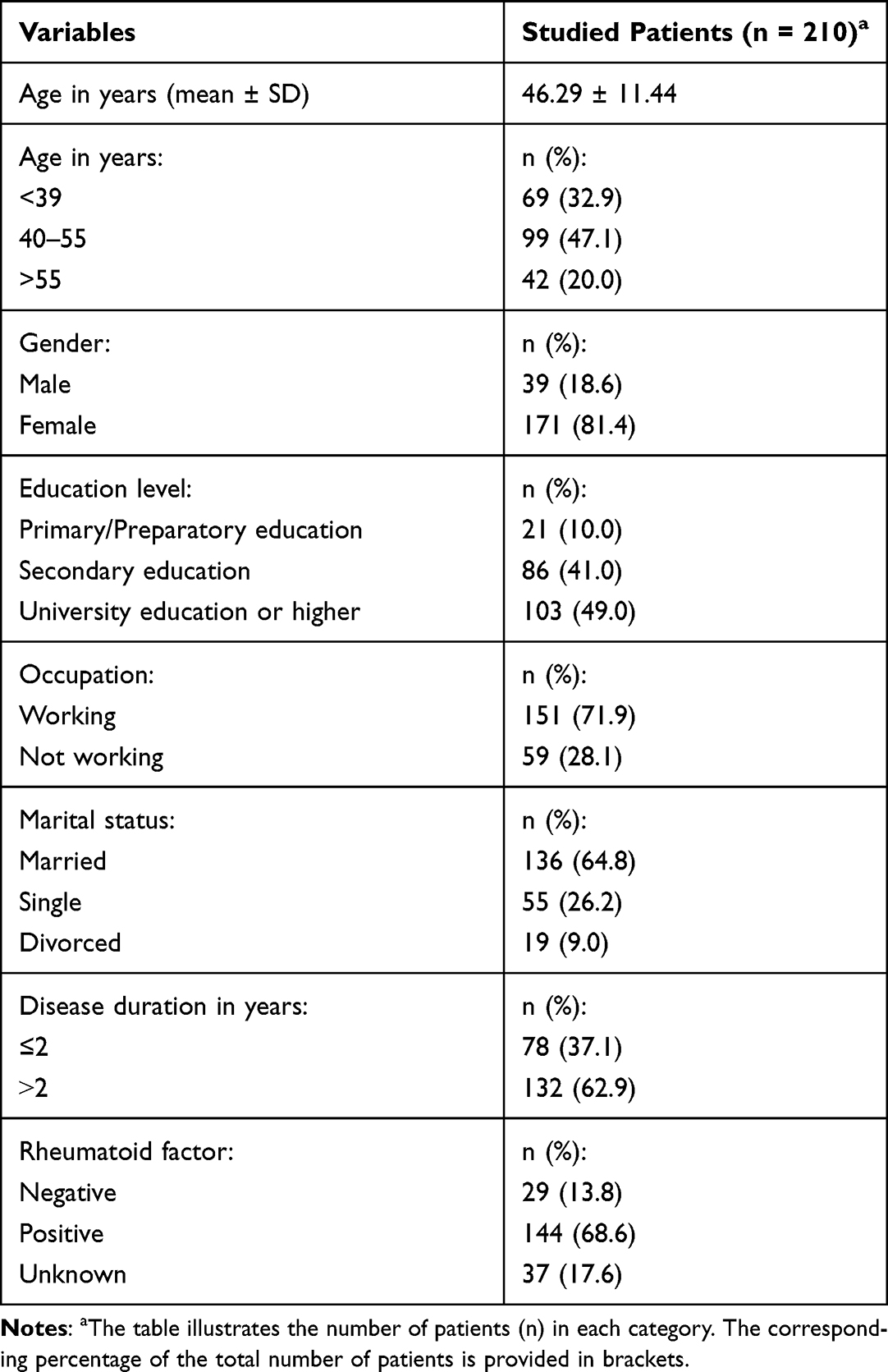 |
Table 1 Sociodemographic Characteristics of Participants |
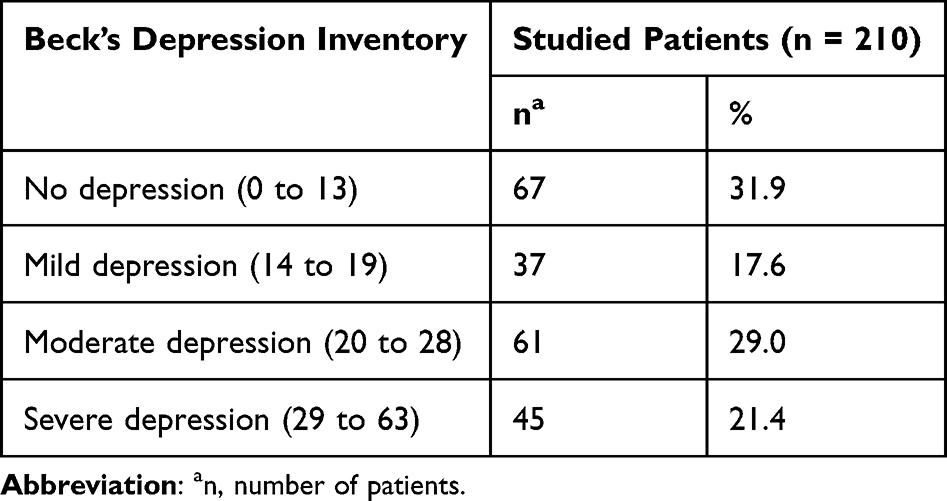 |
Table 2 Prevalence of Depression Among Patients with RA |
A statistically significant association was detected between the presence of depressive symptoms and the following factors: age, gender, marital status, and RF. Among those aged 40 to 55 years, 77.8% were depressed (OR = 2.63). Women were more likely to be depressed than men (75.4% versus 35.9%; OR = 5.48). Divorced participants, 89.5% of whom had depression, were 4.34 times more likely to develop depression than married participants. Furthermore, among participants with positive RF, 72.9% were depressed (OR = 3.81). Multivariate analysis revealed that the following predictors affected 74% of depression cases: being aged 40–55 years, being female, divorced, and RF-positive (Table 3). Statistically significant relationships were found between depression severity and sociodemographic characteristics including age, gender, marital status, disease duration, and RF. More severe cases of depression were detected among women, those aged 40–54 years, those who were divorced, and those with a disease duration of over two years and a positive RF (Table 4).
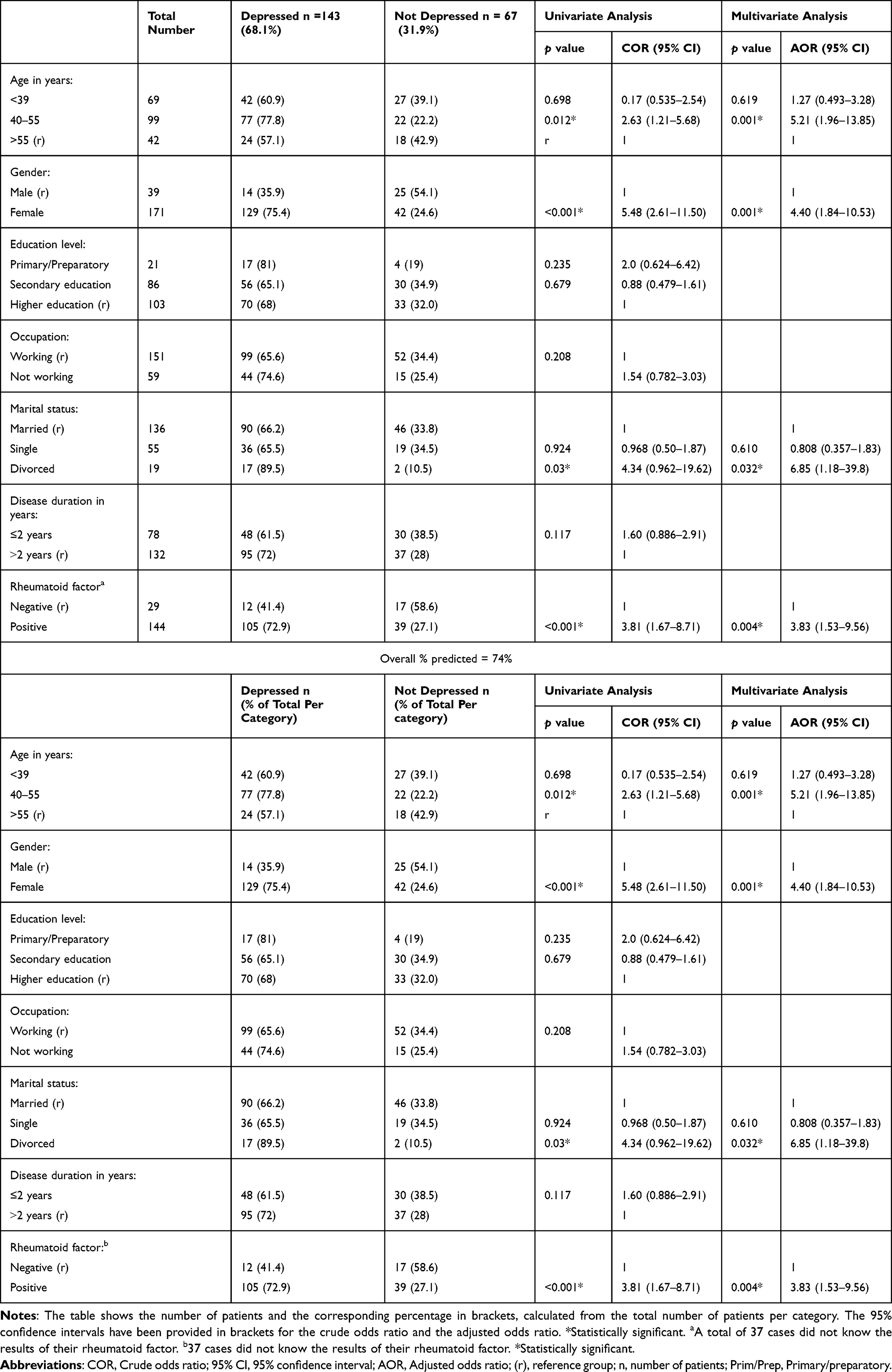 |
Table 3 Association Between Depression and Patient Sociodemographic Characteristics |
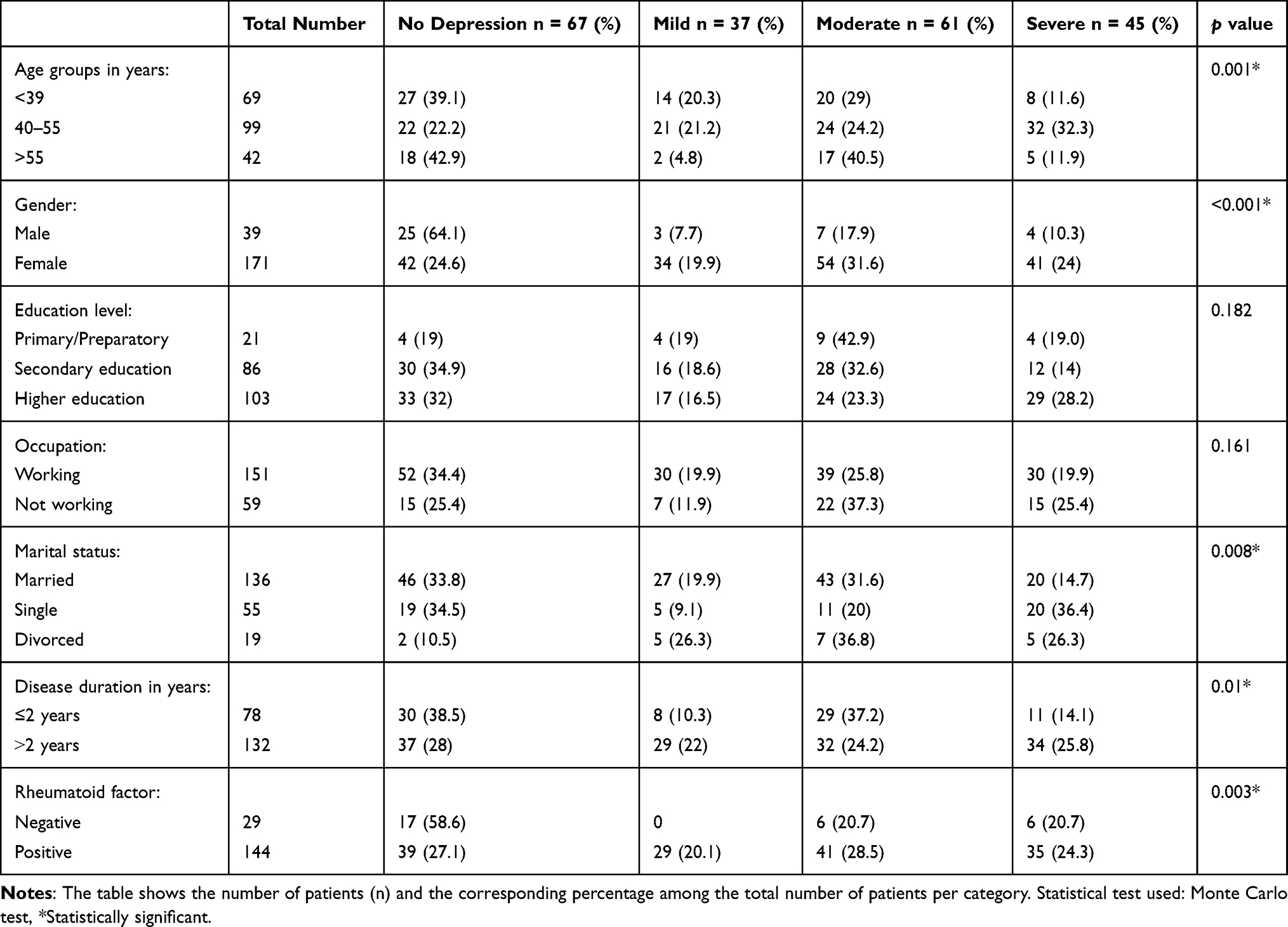 |
Table 4 Association Between Depression Severity and Sociodemographic or Clinical Characteristics of Patients with RA |
Discussion
Depressive symptoms are highly prevalent in individuals with RA compared to those without RA.17 Previous studies have also shown that depression is more common in individuals with RA than in those with other chronic illnesses.17–19 Additionally, depression in individuals with RA has been found to be an independent risk factor for myocardial infarction and cardiovascular disease.20,21
Even after adjusting for RA disease duration, disease activity, disability, and pain, RA was found to be associated with suicidal ideation22,23 and increased risk of mortality.11 Furthermore, a recent study has shown depression to be a significant risk factor for the development of RA as well.24
The primary objective of this study was to assess the prevalence of depression among Saudi patients with RA and to determine its predictors. In this study, 68% of the participants experienced some degree of depression. This figure was higher than what was observed in a previous Saudi study, in which the prevalence of depression was 18%.6 However, it was comparable to the prevalence of depression reported in previous studies from Egypt and Pakistan at 66.2% and 71.5%, respectively.25,26 The variation in the prevalence of depression among patients with RA could be explained by different disease definitions used across studies, as well as different study designs. However, the primary reason for this high percentage is the fact that the study was conducted during the COVID-19 pandemic. According to a cross-sectional study conducted in Saudi Arabia during the pandemic to assess the fear of 637 patients with rheumatic diseases, the majority of the participants (42.7%) were RA patients who were fearful of contracting COVID-19 (33.4%) or experiencing a disease flare-up as a result of COVID-19 infection (51.8%).27 The psychological impact (including anxiety and depression) of the COVID-19 pandemic on RA patients was tested and validated in several studies conducted in different communities.28–30
The nature of RA, which is associated with continuous pain, functional disability, inability to work, and side effects from medication, could contribute to the development of depression.31 Based on available psychometric evidence, BDI-II is valid and reliable screening questionnaires that can be viewed as a cost-effective questionnaire for detecting the presence of depressive symptoms, in addition to measuring the severity of depression, with broad applicability for research and clinical practice worldwide.32,33 The 21 items included reflect a variety of symptoms and attitudes commonly found among clinically depressed individuals (eg, mood, self-dislike, social withdrawal, and sleep disturbance). BDI-II demonstrated reliable, internally consistent and valid scores in a primary care medical setting and it was thus concluded that the inclusion of somatic items was appropriate for the medical sample.34 Moreover, it can monitor changes over time and provide an objective measure for measuring improvement and the effectiveness of treatment methods.35
In this study, we also analyzed the variables that correlated with an increased risk of depressive symptoms in patients with RA. Regarding sociodemographic features and risk of depression, there were positively correlating relationships between the prevalence of depression and factors like gender, age, and marital status. Women with RA were more likely to have depression, which is consistent with previous studies.36,37 Middle-aged patients were also at higher risk of having depression, consistent with previous reports that identified a positive correlation between age and risk of developing depression in patients with RA.36,38,39
Data concerning marital status was limited and contradictory. We observed that depression was more common among divorced participants than married participants. Similar findings were observed in Iranian populations.40 A previous study also found that a higher rate of depression was associated with being unmarried.41 However, another study published in 2001 indicated no significant association between marital status and depression in patients with RA.42 Additionally, our study found no association between depression and the level of education or occupational status.
We observed a positive correlation between the severity of depression and disease duration. However, there was no statistically significant correlation between disease duration and the risk of depression, which is consistent with previous findings.7,43,44 We also observed a significant positive correlation between the presence of RF and the risk of developing depression. Additionally, a study published in 2011 highlighted the association between high RF and depression.38 However, the data on the role of serological factors such as RF in predicting depression is still limited. One report from 1968 by Oreskes et al observed that patients with high RF titers exhibited depressive symptoms.45
Another important predictor of depression in patients with RA, reported in several previous studies but not assessed in this one, is high disease activity.2,6,31,45,46 Depression has also been reported to enhance disease activity in patients with RA, and therapy for concomitant psychiatric illnesses can reduce disease activity.46 Moreover, depression may also increase the risk of an RA flare-up. Yilmaz et al demonstrated that psychological stress and mood disorders were the most common factors associated with such flare-ups.47
As a cross-sectional study, this research is limited in its ability to fully explain the interplay of depression symptoms through the chronic course of RA. Furthermore, several variables such as disease activity, health-related quality of life, medications such as glucocorticoids, and associated comorbidities were not assessed in this study. Future prospective studies should investigate this relationship, as depression presumably influences the course of RA and its therapy over time.
Conclusion
In conclusion, depressive symptoms are highly prevalent in Saudi patients with RA, especially those with positive RF and who are female, middle-aged, and divorced. Therefore, screening, early diagnosis, and treatment of depression in patients with RA are highly recommended to avoid unfavorable effects on RA clinical progression.
Abbreviations
BDI, Beck’s 21-item Depression Inventory; NCD, Noncommunicable disease; OR, Odds ratio; RA, Rheumatoid arthritis; RF, Rheumatoid factor; SD, Standard deviation.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy/ethical restrictions.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki of 1975 and was approved by the Institutional Review Board of the Ministry of Health in Medina (protocol code IRB 566, approved on November 17, 2020). Informed consent was obtained from all participants involved in the study.
Author Contributions
The author made a significant contribution to the work reported, whether that is, in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Alamanos Y, Voulgari PV, Drosos AA. Incidence and prevalence of rheumatoid arthritis, based on the 1987 American College of Rheumatology criteria: a systematic review. Semin Arthritis Rheum. 2006;36(3):182–188. doi:10.1016/j.semarthrit.2006.08.006
2. Al-Dalaan A, Al Ballaa S, Bahabri S, Biyari T, Al Sukait M, Mousa M. The prevalence of rheumatoid arthritis in the Qassim region of Saudi Arabia. Ann Saudi Med. 1998;18(5):396–397. doi:10.5144/0256-4947.1998.396
3. Waraich P, Goldner EM, Somers JM, Hsu L. Prevalence and incidence studies of mood disorders: a systematic review of the literature. Can J Psychiatry. 2004;49(2):124–138. doi:10.1177/070674370404900208
4. Lok EYC, Mok CC, Cheng CW, Cheung EFC. Prevalence and determinants of psychiatric disorders in patients with rheumatoid arthritis. Psychosomatics. 2010;51(4):338–338.e8. doi:10.1176/appi.psy.51.4.338
5. Isik A, Koca SS, Ozturk A, Mermi O. Anxiety and depression in patients with rheumatoid arthritis. Clin Rheumatol. 2007;26(6):872–878. doi:10.1007/s10067-006-0407-y
6. Attar SM. Can we predict depression in patients with rheumatoid arthritis. Kuwait Med J. 2014;46(3):219–224.
7. Matcham F, Rayner L, Steer S, Hotopf M. The prevalence of depression in rheumatoid arthritis: a systematic review and meta-analysis. Rheumatology. 2013;52(12):2136–2148. doi:10.1093/rheumatology/ket169
8. Spicer JG Health-related quality of life: covariance structural equation modeling in the evaluation of symptom status and support in persons with rheumatoid arthritis [dissertation]. San Francisco: University of California; 1998.
9. Katz PP, Yelin EH. Prevalence and correlates of depressive symptoms among persons with rheumatoid arthritis. J Rheumatol. 1993;20(5):790–796.
10. Michelsen B, Kristianslund EK, Sexton J, et al. Do depression and anxiety reduce the likelihood of remission in rheumatoid arthritis and psoriatic arthritis? Data from the prospective multicentre NOR-DMARD study. Ann Rheum Dis. 2017;76(11):1906–1910. doi:10.1136/annrheumdis-2017-211284
11. Ang DC, Choi H, Kroenke K, Wolfe F. Comorbid depression is an independent risk factor for mortality in patients with rheumatoid arthritis. J Rheumatol. 2005;32(6):1013–1019.
12. Arnett FC, Edworthy SM, Bloch DA, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31(3):315–324. doi:10.1002/art.1780310302
13. Aletaha D, Neogi T, Silman AJ, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569–2581. doi:10.1002/art.27584
14. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561–571. doi:10.1001/archpsyc.1961.01710120031004
15. Beck AT, Steer RA, Carbin MG. Psychometric properties of the Beck depression inventory: twenty-five years of evaluation. Clin Psychol Rev. 1988;8(1):77–100. doi:10.1016/0272-7358(88)90050-5
16. Abdel-Khalek AM. Internal consistency of an Arabic adaptation of the Beck depression inventory in four Arab countries. Psychol Rep. 1998;82(1):264–266. doi:10.2466/pr0.1998.82.1.264
17. Dickens C, McGowan L, Clark-Carter D, Creed F. Depression in rheumatoid arthritis: a systematic review of the literature with meta-analysis. Psychosom Med. 2002;64(1):52–60. doi:10.1097/00006842-200201000-00008
18. Ghaemmohamadi MS, Behzadifar M, Ghashghaee A, et al. Prevalence of depression in cardiovascular patients in Iran: a systematic review and meta-analysis from 2000 to 2017. J Affect Disord. 2018;227:149–155. doi:10.1016/j.jad.2017.10.026
19. Ravaghi H, Behzadifar M, Behzadifar M, et al. Prevalence of depression in hemodialysis patients in Iran: a systematic review and meta-analysis. Iran J Kidney Dis. 2017;11(2):90–98.
20. Scherrer JF, Virgo KS, Zeringue A, et al. Depression increases risk of incident myocardial infarction among Veterans Administration patients with rheumatoid arthritis. Gen Hosp Psychiatry. 2009;31(4):353–359. doi:10.1016/j.genhosppsych.2009.04.001
21. Treharne GJ, Hale ED, Lyons AC, et al. Cardiovascular disease and psychological morbidity among rheumatoid arthritis patients. Rheumatology. 2005;44(2):241–246. doi:10.1093/rheumatology/keh441
22. Timonen M, Viilo K, Hakko H, et al. Suicides in persons suffering from rheumatoid arthritis. Rheumatology. 2003;42(2):287–291. doi:10.1093/rheumatology/keg082
23. Tektonidou MG, Dasgupta A, Ward MM. Suicidal ideation among adults with arthritis: prevalence and subgroups at highest risk. Data from the 2007–2008 national health and nutrition examination survey. Arthritis Care Res (Hoboken). 2011;63(9):1322–1333. doi:10.1002/acr.20516
24. Vallerand IA, Patten SB, Barnabe C. Depression and the risk of rheumatoid arthritis. Curr Opin Rheumatol. 2019;31(3):279–284. doi:10.1097/BOR.0000000000000597
25. Imran MY, Saira Khan EA, Ahmad NM, Farman Raja S, Saeed MA, Ijaz Haider I. Depression in rheumatoid arthritis and its relation to disease activity. Pak J Med Sci. 2015;31(2):393–397. doi:10.12669/pjms.312.6589
26. el-Miedany YM, el-Rasheed AH. Is anxiety a more common disorder than depression in rheumatoid arthritis? Joint Bone Spine. 2002;69(3):300–306. doi:10.1016/S1297-319X(02)00368-8
27. Hassen LM, Almaghlouth IA, Hassen IM, et al. Impact of COVID-19 outbreak on rheumatic patients’ perceptions and behaviors: a cross-sectional study. Int J Rheum Dis. 2020;23:1541–1549. doi:10.1111/1756-185X.13959
28. Tee CA, Salido EO, Reyes PW, Ho RC, Tee ML. Psychological state and associated factors during the 2019 coronavirus disease (COVID-19) pandemic among Filipinos with rheumatoid arthritis or systemic lupus erythematosus. Open Access Rheumatol. 2020;12:215–222. doi:10.2147/OARRR.S269889
29. Itaya T, Torii M, Hashimoto M, et al. Prevalence of anxiety and depression in patients with rheumatoid arthritis before and during the COVID-19 pandemic. Rheumatology. 2021;60:2023–2024. doi:10.1093/rheumatology/keab065
30. Ş G, Akkubak Y, Aksoy ZK, Küçük A, Cüre E. Effects of the COVID-19 pandemic on psychology and disease activity in patients with Ankylosing spondylitis and rheumatoid arthritis. Turk J Med Sci. 2021;51:1631–1639. doi:10.3906/sag-2011-188
31. Mella LFB, Bértolo MB, Dalgalarrondo P. Depressive symptoms in rheumatoid arthritis. Braz J Psychiatry. 2010;32(3):257–263. doi:10.1590/S1516-44462010005000021
32. Subica AM, Fowler JC, Elhai JD, et al. Factor structure and diagnostic validity of the Beck depression inventory–II with adult clinical inpatients: comparison to a gold-standard diagnostic interview. Psychol Assess. 2014;26(4):1106–1115. doi:10.1037/a0036998
33. Bifftu BB, Dachew BA, Tiruneh BT, Tebeje NB. Depression among people with epilepsy in Northwest Ethiopia: a cross-sectional institution based study. BMC Res Notes. 2015;8(1):585. doi:10.1186/s13104-015-1515-z
34. Warmenhoven F, van Rijswijk E, Engels Y, et al. The Beck Depression Inventory (BDI-II) and a single screening question as screening tools for depressive disorder in Dutch advanced cancer patients. Support Care Cancer. 2011;20(2):319–324. doi:10.1007/s00520-010-1082-8
35. Arnau RC, Meagher MW, Norris MP, Bramson R. Psychometric evaluation of the Beck depression inventory-II with primary care medical patients. Health Psychol. 2001;20(2):112–119. doi:10.1037/0278-6133.20.2.112
36. Wolfe F, Michaud K. Predicting depression in rheumatoid arthritis: the signal importance of pain extent and fatigue, and comorbidity. Arthritis Rheum. 2009;61(5):667–673. doi:10.1002/art.24428
37. Pezzato S, Bonetto C, Caimmi C, et al. Depression is associated with increased disease activity and higher disability in a large Italian cohort of patients with rheumatoid arthritis. Adv Rheumatol. 2021;61(1):57. doi:10.1186/s42358-021-00214-3
38. Ho RCM, Fu EHY, Chua ANC, Cheak AAC, Mak A. Clinical and psychosocial factors associated with depression and anxiety in Singaporean patients with rheumatoid arthritis. Int J Rheum Dis. 2011;14(1):37–47. doi:10.1111/j.1756-185X.2010.01591.x
39. Sariyildiz MA, Batmaz I, Bozkurt M, et al. Sleep quality in rheumatoid arthritis: relationship between the disease severity, depression, functional status and the quality of life. J Clin Med Res. 2014;6(1):44–52. doi:10.4021/jocmr1648w
40. Jamshidi AR, Banihashemi AT, Paragomi P, Hasanzadeh M, Barghamdi M, Ghoroghi S. Anxiety and depression in rheumatoid arthritis: an epidemiologic survey and investigation of clinical correlates in Iranian population. Rheumatol Int. 2016;36(8):1119–1125. doi:10.1007/s00296-016-3493-4
41. Rivero-Carrera NN, Serra-Bonett N, Snih SA, Duque-Criollo JV, Rodríguez MA. Risk factors associated with depressive symptoms in Venezuelan patients with rheumatoid arthritis. J Clin Rheumatol. 2011;17(4):218–219. doi:10.1097/RHU.0b013e31821c7af3
42. Sharpe L, Sensky T, Allard S. The course of depression in recent onset rheumatoid arthritis: the predictive role of disability, illness perceptions, pain and coping. J Psychosom Res. 2001;51(6):713–719. doi:10.1016/S0022-3999(01)00266-5
43. Strating MM, Suurmeijer TP, van Schuur WH. Disability, social support, and distress in rheumatoid arthritis: results from a thirteen‐year prospective study. Arthritis Rheum. 2006;55(5):736–744. doi:10.1002/art.22231
44. Barlow JH, Cullen LA, Rowe IF. Comparison of knowledge and psychological well-being between patients with a short disease duration (≤ 1 year) and patients with more established rheumatoid arthritis (≥ 10 years duration). Patient Educ Couns. 1999;38(3):195–203. doi:10.1016/S0738-3991(98)00144-X
45. Oreskes I, Rosenblatt S, Spiera H, Meadow H. Rheumatoid factors in an acute psychiatric population. Ann Rheum Dis. 1968;27(1):60–63. doi:10.1136/ard.27.1.60
46. Crotty M, McFarlane AC, Brooks PM, Hopper JL, Bieri D, Taylor SJ. The psychosocial and clinical status of younger women with early rheumatoid arthritis: a longitudinal study with frequent measures. Br J Rheumatol. 1994;33(8):754–760. doi:10.1093/rheumatology/33.8.754
47. Yılmaz V, Umay E, Gündoğdu I, Karaahmet ZÖ, Öztürk AE. Rheumatoid Arthritis: are psychological factors effective in disease flare? Eur J Rheumatol. 2017;4(2):127–132. doi:10.5152/eurjrheum.2017.16100
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Comparative Analysis of Cognitive Deficits in Rheumatoid Arthritis and Fibromyalgia: Impact of Symptoms Severity and Its Clinical Implications
Galvez-Sánchez CM, Duschek S, Reyes del Paso GA
Psychology Research and Behavior Management 2024, 17:1399-1415
Published Date: 28 March 2024
Research Trends of Rheumatoid Arthritis and Depression from 2019 to 2023: A Bibliometric Analysis
Zhao Y, Chen GY, Fang M
Journal of Multidisciplinary Healthcare 2024, 17:4465-4474
Published Date: 17 September 2024
Advances in the Diagnosis and Treatment of Rheumatoid Arthritis: From Pathological Mechanisms to Integrated Chinese and Western Medicine Therapeutic Strategies
Wang M, Pan L, Guan R
International Journal of General Medicine 2026, 19:575521
Published Date: 5 February 2026