Back to Journals » Clinical Ophthalmology » Volume 17
Idiopathic Epiretinal Membrane Surgery in Patients Aged Over 80 Years: Efficacy and Safety
Authors Li Q, Yang K, Ji Q, Jiang J, Zong R, Zhang Y, Qian Y, Che X, Suo J, Wang Z ![]()
Received 30 August 2023
Accepted for publication 27 October 2023
Published 3 November 2023 Volume 2023:17 Pages 3365—3372
DOI https://doi.org/10.2147/OPTH.S437815
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Qingjian Li,1,* Kunhuan Yang,2– 5,* Qianlin Ji,1,* Jing Jiang,1 Rongrong Zong,2– 5 Yu Zhang,1 Yiwen Qian,1 Xin Che,1 Jinshan Suo,1 Zhiliang Wang1
1Department of Ophthalmology, Huashan Hospital, Fudan University, Shanghai, People’s Republic of China; 2Fujian Provincial Key Laboratory of Ophthalmology and Visual Science, Xiamen, Fujian, People’s Republic of China; 3Fujian Engineering and Research Center of Eye Regenerative Medicine, Xiamen, Fujian, People’s Republic of China; 4Eye Institute of Xiamen University, Xiamen, Fujian, People’s Republic of China; 5Xiamen University School of Medicine, Xiamen, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinshan Suo; Zhiliang Wang, Email [email protected]; [email protected]
Purpose: To evaluate the efficacy and safety of idiopathic epiretinal membrane (ERM) surgery in patients aged over 80 years.
Methods: Consecutive patients who underwent pars plana vitrectomy (PPV) combined with ERM and internal limiting membrane (ILM) peeling with retrobulbar anesthesia were recruited. Based on age, the patients were divided into the elderly group (≥ 80 years of age) and the control group (< 80 years of age). The best-corrected visual acuity (BCVA) and surgical complications were regarded as the main measurement indicators.
Results: This study included 43 eyes from 43 patients aged 80 to 91 years and 86 eyes from 86 patients aged 54 to 79 years. Surgical intervention substantially improved BCVA both in the elderly and control groups (p = 0.005 and p < 0.001, respectively). Statistical analyses showed no significant difference in the incidence of surgical complications between the two groups (p = 0.631). The operations in either group were not delayed or canceled for the reason of complications of retrobulbar anesthesia, severe anxiety, or physical discomfort in the perioperative period. Moreover, no patient required a second operation. Also, no stroke, myocardial infarction, or death occurred during the follow-up period. All the surgical complications were treated satisfactorily.
Conclusion: Our outcomes indicate that PPV combined with ERM and ILM peeling with retrobulbar anesthesia is effective and safe in elderly patients aged 80 years or older. Based on age alone, we believe that advancing age should not be the risk factor for idiopathic ERM surgery.
Keywords: idiopathic epiretinal membrane, elderly, pars plana vitrectomy, complication, safety
Introduction
Idiopathic epiretinal membrane (ERM) is a prevalent vitreoretinal disease, with population-based research demonstrating a prevalence of 9.6 per 100 adults and an average annual incidence of 3.2 per 100,000.1 The prevalence of ERM increases dramatically with age, from less than 1% among adults under 50 years to more than 11% among those over 80 years of age.2 ERM often causes metamorphopsia and visual impairment in the elderly population. For most patients with idiopathic ERM, the standard clinical therapy is pars plana vitrectomy (PPV) with ERM peeling, combined with internal limiting membrane (ILM) peeling,3,4 with about 70% of patients improving visual acuity two lines or more.5,6 A study by Jackson et al1 has shown that 9.8% of the patients undergoing ERM surgeries have surgical complications, including lens touch, iatrogenic retinal trauma, posterior capsular rupture, and corneal edema.
Several studies have demonstrated a remarkable improvement in vision and life quality after ERM surgeries.7–10 Therefore, ERM surgeries are essential for elderly patients. However, for some elders, advanced age remains a barrier to undergo ERM surgery. Several researches have shown that age is an independent risk factor for the majority of operations.11–17 and the increased surgical risk in elderly patients is also present for ophthalmic procedures.18–21 It is especially true for idiopathic ERM, which is usually associated with mild or moderate visual impairment, while surgery may be related to the risk of serious complications, such as endophthalmitis, vitreous hemorrhage, or retinal detachment. Also, a study has proved that final best-corrected visual acuity (BCVA) after ERM surgery is inversely correlated to age.22
As far as we know, no published study has evaluated the results of idiopathic ERM surgery in a subset of the subjects aged ≥ 80 years. Therefore, it is necessary to assess surgery’s efficacy and safety among patients aged 80 years or older.
Methods
Patients
This research recruited consecutive subjects who underwent PPV combined with peeling of ERM and ILM with retrobulbar anesthesia at Huashan Hospital affiliated to Fudan University. The Institutional Review Board of Huashan Hospital of Fudan University approved the research (No. KY2021-837), which was conducted in accordance with the Declaration of Helsinki. The informed consent form was signed by all subjects recruited for this study.
Inclusion Criteria
Consecutive subjects undergoing PPV combined with peeling of ERM and ILM under retrobulbar anesthesia were eligible for inclusion in this research. Based on age, the patients were divided into the elderly group (≥ 80 years of age) and the control group (< 80 years of age). To improve this research’s reliability, one patient in the elderly group was paired with two patients in the control group. The subjects with a history of ocular trauma, ophthalmic surgery, uveitis, diabetic retinopathy, retinal vascular disease, high myopia, or age-related macular degeneration were excluded from the research, except those with a history of cataract surgery. The subjects with serious systemic diseases, including congestive heart failure, decompensated cirrhosis, severe chronic obstructive pulmonary disease and so on, were also ruled out. However, this research still enrolled the participants with underlying chronic conditions, such as diabetes mellitus, hypertension, asthma, or cardiovascular disease, and the participants receiving antiplatelet or anticoagulant medications. The systemic drugs taken by the patients before surgery were not discontinued during the perioperative period.
Data Collection
Preoperative data including the patient’s sex, age, disease duration, surgical eye, surgeon, BCVA, intraocular pressure (IOP), lens status, foveal thickness, antiplatelet medications, anticoagulant medications, and common comorbidity (history of diabetes mellitus and hypertension) were recorded. For all statistical analyses, BCVA was presented as logarithm of the minimum angle of resolution (logMAR) value.23,24 IOP > 30 mmHg or < 6 mmHg was considered as ocular hypertension or hypotension, respectively.24–26 The postoperative BCVA and surgical complications were used as the main measurement indicators. Other indicators included postoperative IOP, foveal thickness, and vitreous tamponading agent.
Surgical Technique
One of two skilled surgeons in the same institution performed standard three-port trocar-based 23-gauge PPV combined with ERM and ILM peeling with retrobulbar anesthesia. The standard phacoemulsification technique combined with posterior chamber intraocular lens (IOL) implantation was performed in all phakic eyes. Compound tropicamide eye drops containing tropicamide (0.5%) and phenylephrine hydrochloride (0.5%) served as preoperative mydriatic as a routine. The anesthetic contained 2.5ml bupivacaine hydrochloride (0.75%) and 2.5ml lidocaine hydrochloride (2%) without epinephrine. Triamcinolone acetonide was employed to optimize visualization during ERM peeling, while indocyanine green was used for ILM peeling.
Statistical Analysis
SPSS statistical analysis software (SPSS, Version 24.0, IBM Inc., Chicago, IL, USA) was used for statistical analyses. Continuous data were presented as mean ± standard deviation. Categorical data were presented as absolute numbers and percentages. The Student t-test or Wilcoxon test was used for continuous variable comparisons. The Chi-square test or Fisher’s exact test was used to compare categorical variables. Statistical difference was defined as a two-sided p value < 0.05.
Results
This study included 43 eyes from 43 patients aged 80–91 years and 86 eyes from 86 patients aged 54–79 years. The average age was 83.44 ± 2.35 years in the elderly group and 69.29 ± 5.23 years in the control group. PPV combined with ERM and ILM peeling with retrobulbar anesthesia was performed in all 129 patients (129 eyes). Ninety-three (93 eyes) of them experienced standard phacoemulsification combined with IOL implantation. The follow-up time was 5–7 months after the ERM surgery. The patient’s general characteristics are shown in Table 1. The sex, disease duration, surgical eye, surgeon, preoperative BCVA, IOP, lens status, nuclear hardness, foveal thickness, antiplatelet therapy, anticoagulant therapy, and common comorbidity between the two groups showed no significant difference (all p > 0.05).
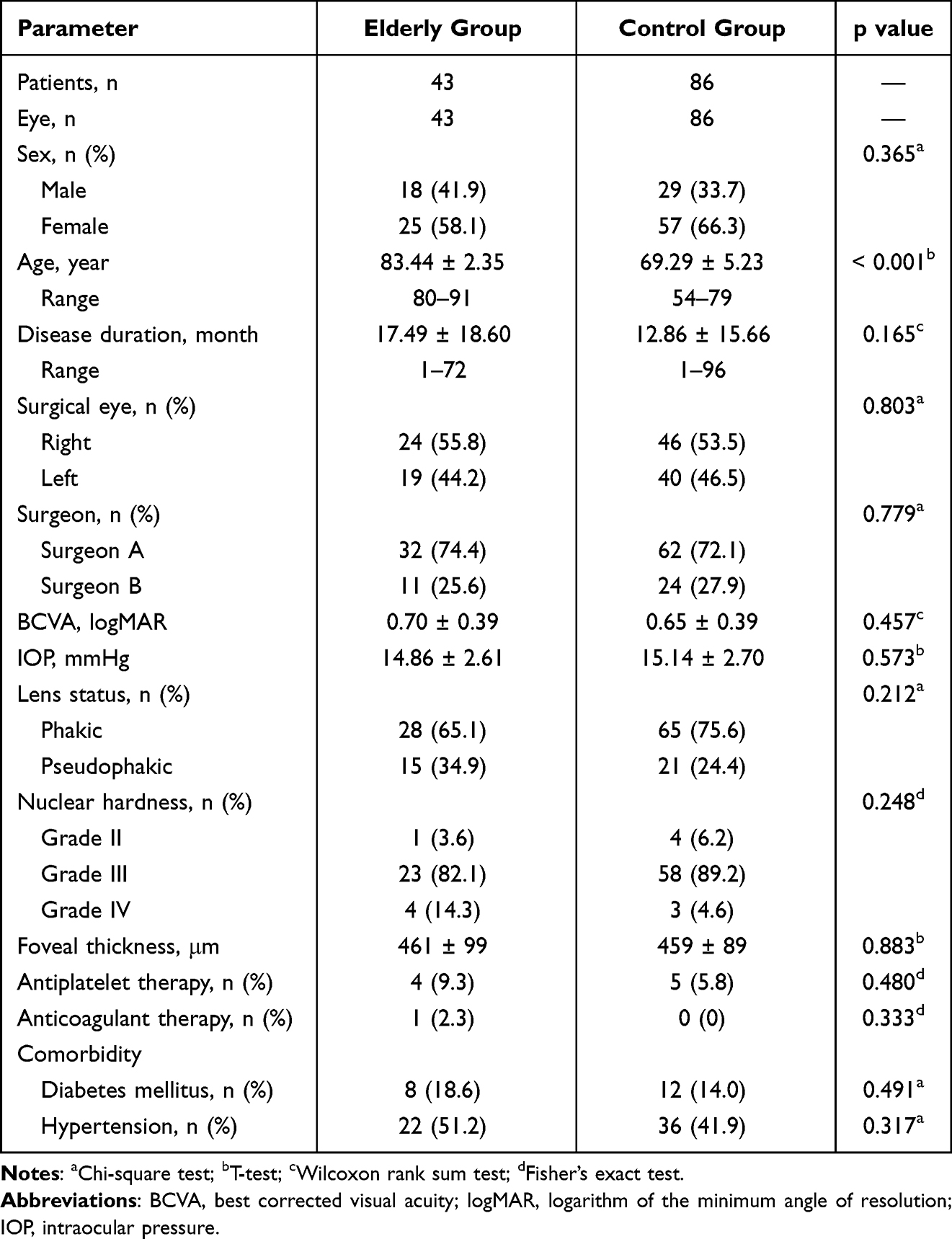 |
Table 1 Patient’s General Characteristics |
Representative optical coherence tomography images before and after ERM surgery are shown in Figure 1. The postoperative results at the last follow-up are shown in Table 2. Surgical intervention substantially improved BCVA both in the elderly and control groups (p = 0.005 and p < 0.001, respectively). The visual acuity improved from 0.70 ± 0.39 to 0.49 ± 0.30 logMAR in the elderly group and from 0.65 ± 0.39 to 0.41 ± 0.23 logMAR in the control group. The postoperative BCVA in the elderly group was worse than that in the control group, but the difference was not statistically significant (0.49 ± 0.30 versus 0.41 ± 0.23 logMAR, p = 0.217). The two groups were equally distributed in terms of the postoperative IOP, visual acuity improvement, vitreous substitute used, and foveal thickness (p = 0.573, p = 0.824, p = 0.516, and p = 0.613, respectively).
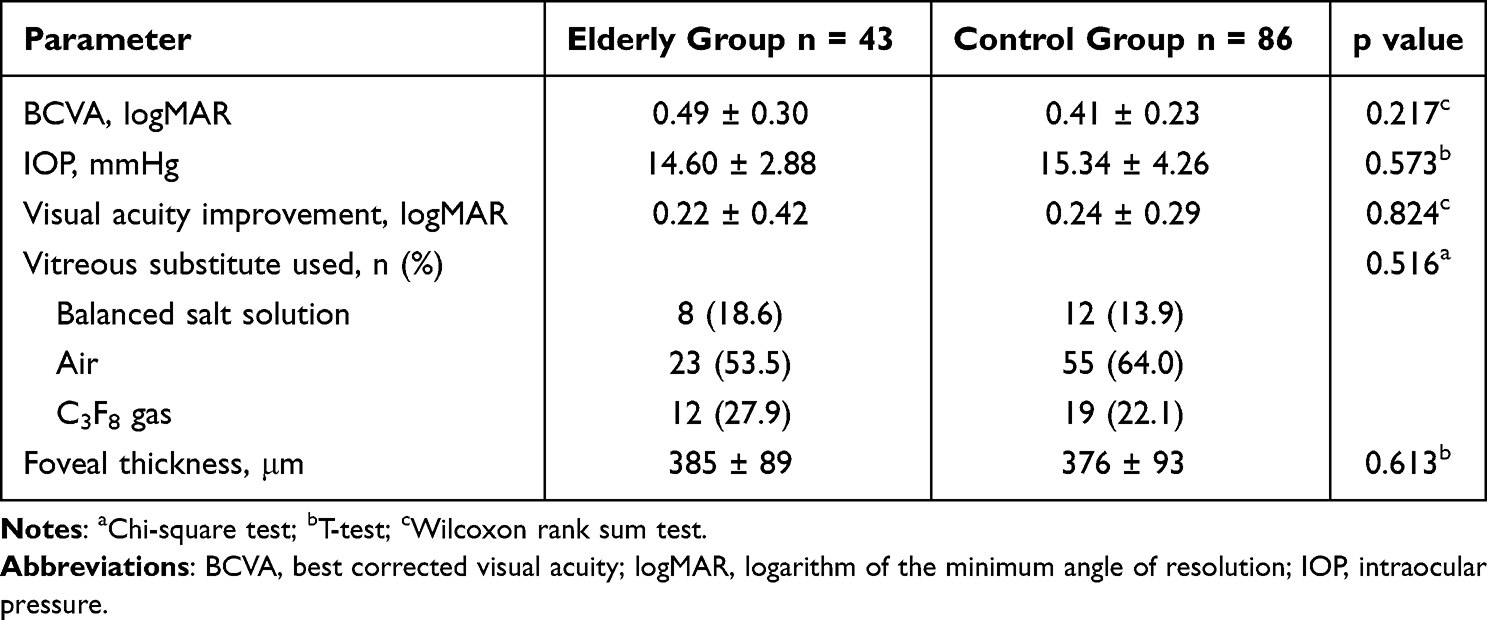 |
Table 2 Postoperative Results |
 |
Figure 1 Representative optical coherence tomography images from an 83-year-old male patient with ERM in the right eye. (A) Pre-operation. (B) Post-operation. |
The surgical complications are shown in Table 3. Statistical analyses showed no significant difference between the elderly and control groups in terms of the incidence of surgical complications, including iatrogenic retinal trauma, hyphema, ocular hypertension, and hypotension (p = 0.718, p = 1.000, p = 0.730, and p = 0.333, respectively). Within the elderly group, all two iatrogenic retinal traumas were located in the posterior pole. In the control group, five iatrogenic retinal traumas were observed in the posterior pole, with one additional trauma occurring in the periphery. Given that the procedure of ERM and ILM peeling had produced mechanical traction on the retina, resulting in damage to the retinal pigment epithelium or Bruch’s membrane in some cases, 27.9% of eyes in the elderly group were treated with C3F8 compared to 22.1% in the control group. One patient in the elderly group experienced temporary ocular hypotonia after surgery, while a total of 10 cases developed transient ocular hypertension that could be effectively controlled with eye drops. The operations in either group were not delayed or canceled because of complications of retrobulbar anesthesia, severe anxiety, or physical discomfort in the perioperative period. Moreover, no patient required a second operation. Also, no stroke, myocardial infarction, or death occurred during the follow-up period. Ten subjects took antiplatelet or anticoagulant medications, and none of them suffered from hyphema. All the surgical complications were treated satisfactorily.
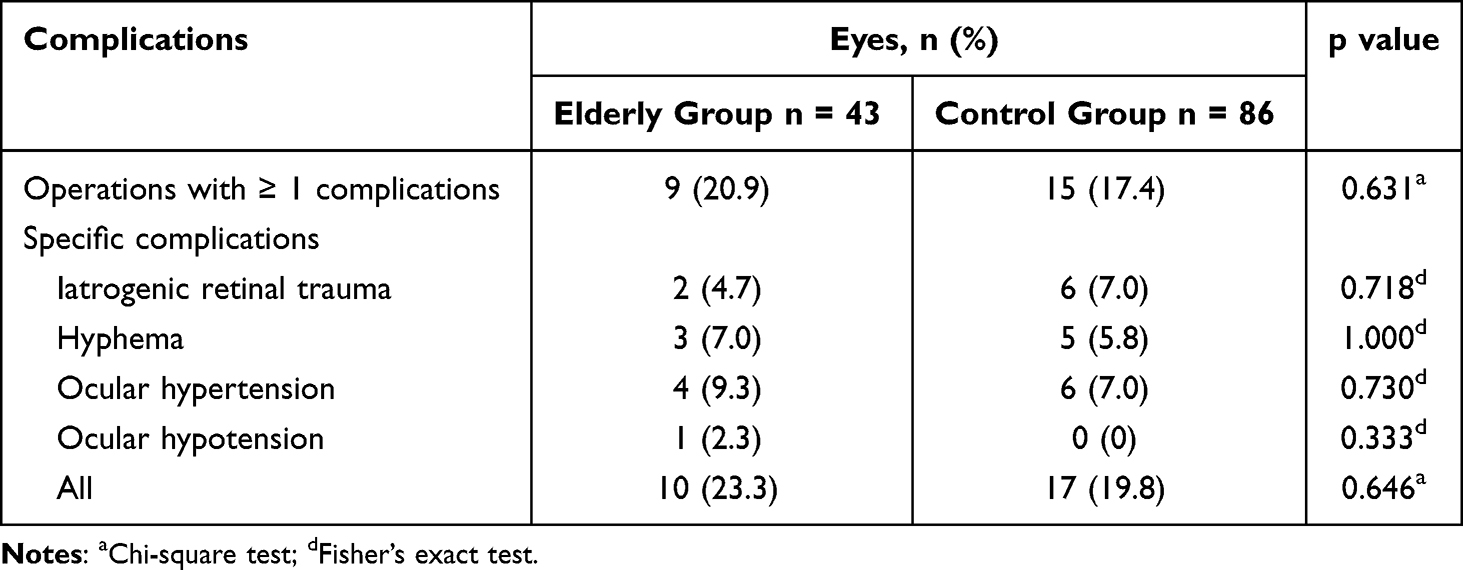 |
Table 3 Surgical Complications |
Discussion
With the aging of the population, it is necessary for us to understand the impact of age on idiopathic ERM surgery. In our study, surgical intervention substantially improved BCVA both in the elderly and control groups. Statistical analyses showed no significant difference between the two groups in terms of the incidence of surgical complications. Thus, the outcomes of our study indicate that idiopathic ERM surgery with retrobulbar anesthesia is effective and safe for elders who are ≥ 80 years old.
Compared to the young group, the elderly population faces more health problems. Poor baseline functional status and systemic comorbidity increase the risk of postoperative complications in senile subjects. Previous studies have demonstrated that the old population has higher morbidity and mortality than the young population after surgeries.27–32 In a study by Chandra et al21 surgical risk factors were compared between 56 subjects with suprachoroidal hemorrhagic and 5403 subjects in the control group after PPV. The outcomes showed that an increase in age was a risk factor for suprachoroidal hemorrhagic. However, some investigators discovered that no independent association between advancing age and worse postoperative results, as in some nonocular surgeries like coronary artery bypass graft surgery,33 carotid endarterectomy,34 abdominal surgery,35 and colorectal cancer.36 Moisseiev et al6 reported the outcomes of idiopathic ERM surgery among 29 subjects aged 75–92 years and concluded that the operation was safe for the aged population. But the sample size was relatively small, with 10 participants over 80 years of age. So far, it is hard to decide whether older subjects are suitable to undergo idiopathic ERM surgery.
In our study, all 43 patients were more than 80 years old, with an average age of 83.44 ± 2.35 years (80–91 years of age). We also enrolled the subjects with underlying chronic conditions, such as diabetes mellitus, hypertension, asthma, or cardiovascular disease, and the subjects receiving antiplatelet or anticoagulant drugs. Our study showed no significant difference in visual acuity improvement between the old and young populations. The improved visual function after ERM surgery significantly enhanced their quality of life. We even detected that the idiopathic ERM surgery was still effective and safe for the elderly population who did not discontinue antiplatelet or anticoagulant medications.
Our study showed no significant difference between the elderly and control groups in terms of the incidence of postoperative complications. No patient suffered from serious surgical complications, such as retinal detachment, vitreous hemorrhage, or endophthalmitis, resulting in reoperation. The outcomes of this study demonstrate that idiopathic ERM surgery among the elderly population aged 80 years or older is as safe as among young people.
For phakic eyes, the majority of surgeons recommend ERM surgery combined with phacoemulsification cataract surgery. In this way, the patient can avoid a second operation to treat complicated cataract, which usually takes place within a year.37,38 We performed phacoemulsification and IOL implantation combined with PPV in phakic eyes and concluded that it was effective and safe for older patients.
Our previous study has demonstrated the efficacy and safety of vitrectomy for idiopathic macular hole (MH) in individuals aged over 80 years.26 In comparison to patients with MH, those with ERM experience less visual impairment. Consequently, the need for improving visual acuity in patients with ERM is more likely to be overlooked. Therefore, it is crucial to assess the safety and effectiveness of ERM surgery.
This research has several limitations. First, our sample size was relatively small due to the limited number of older adults aged 80 or older. Second, despite the presence of underlying chronic conditions such as diabetes mellitus, hypertension, asthma, or cardiovascular disease, the subjects with serious systemic diseases were excluded from this study. These attributes require special attention and understanding by surgeons.
Conclusion
Our outcomes indicate that PPV combined with ERM and ILM peeling with retrobulbar anesthesia is effective and safe among patients aged ≥ 80 years. We believe age should not represent a barrier for patients and surgeons, notably for patients with underlying chronic diseases.
Abbreviations
ERM, Epiretinal membrane; PPV, Pars plana vitrectomy; ILM, Internal limiting membrane; BCVA, Best-corrected visual acuity; IOP, Intraocular pressure; logMAR, logarithm of the minimum angle of resolution; IOL, Intraocular lens; MH, Macular hole.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Institutional Review Board of Huashan Hospital of Fudan University (No. KY2021-837). The informed consent form was signed by all subjects recruited for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from the Science and Technology Commission of Shanghai Municipality (No. 20Y11910800).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Jackson TL, Donachie PH, Williamson TH, Sparrow JM, Johnston RL The royal college of ophthalmologists’ national ophthalmology database study of vitreoretinal surgery: report 4, epiretinal membrane. Retina-J Ret Vit Dis. 2015, 35:1615–1621. doi:10.1097/IAE.0000000000000523
2. McCarty DJ, Mukesh BN, Chikani V, et al. Prevalence and associations of epiretinal membranes in the visual impairment project. Am J Ophthalmol. 2005;140(2):288–294. doi:10.1016/j.ajo.2005.03.032
3. Mieno H, Kojima K, Yoneda K, et al. Evaluation of pre- and post-surgery reading ability in patients with epiretinal membrane: a prospective observational study. BMC Ophthalmol. 2020;20(1):95. doi:10.1186/s12886-020-01364-6
4. Piccirillo V, Sbordone S, Sorgente F, et al. Evaluation of efficacy and safety of new high-density dyes for chromovitrectomy. Sci Rep-Uk. 2021;11:15171. doi:10.1038/s41598-021-94770-9
5. Wong JG, Sachdev N, Beaumont PE, Chang AA. Visual outcomes following vitrectomy and peeling of epiretinal membrane. Clin Exp Ophthalmol. 2005;33:373–378. doi:10.1111/j.1442-9071.2005.01025.x
6. Moisseiev E, Davidovitch Z, Kinori M, Loewenstein A, Moisseiev J, Barak A. Vitrectomy for idiopathic epiretinal membrane in elderly patients: surgical outcomes and visual prognosis. Curr Eye Res. 2012;37(1):50–54. doi:10.3109/02713683.2011.614373
7. Yusuf AM, Bizrah M, Bunce C, Bainbridge JW. Surgery for idiopathic epiretinal membrane. Cochrane Db Syst Rev. 2021;3:D13297. doi:10.1002/14651858.CD013297.pub2
8. Minami S, Shinoda H, Shigeno Y, et al. Effect of axial length and age on the visual outcome of patients with idiopathic epiretinal membrane after pars plana vitrectomy. Sci Rep-Uk. 2019;9(1):19056. doi:10.1038/s41598-019-55544-6
9. Hashemi H, Mehravar F, Asgari S, Emamian MH, Fotouhi A. Visual functions and disability in Iranian adults: a population-based study. BMC Ophthalmol. 2022;22(1):30. doi:10.1186/s12886-022-02262-9
10. Mukkamala LK, Avaylon J, Welch RJ, et al. Intraoperative Retinal Changes May Predict Surgical Outcomes After Epiretinal Membrane Peeling. Transl Vis Sci Techn. 2021;10(2):36. doi:10.1167/tvst.10.2.36
11. Story DA. Postoperative complications in elderly patients and their significance for long-term prognosis. Curr Opin Anesthesio. 2008;21:375–379. doi:10.1097/ACO.0b013e3282f889f8
12. Turrentine FE, Wang H, Simpson VB, Jones RS. Surgical risk factors, morbidity, and mortality in elderly patients. J Am Coll Surgeons. 2006;203(6):865–877. doi:10.1016/j.jamcollsurg.2006.08.026
13. Hamel MB, Henderson WG, Khuri SF, Daley J. Surgical outcomes for patients aged 80 and older: morbidity and mortality from major noncardiac surgery. J Am Geriatr Soc. 2005;53(3):424–429. doi:10.1111/j.1532-5415.2005.53159.x
14. Bischoff P, Kramer TS, Schroder C, et al. Age as a risk factor for surgical site infections: German surveillance data on total Hip replacement and total knee replacement procedures 2009 to 2018. Eurosurveillance. 2023;28. doi:10.2807/1560-7917.ES.2023.28.9.2200535
15. Ji Q, Zhao Y, Shen J, et al. Elderly Patients with Moderate Chronic Ischemic Mitral Regurgitation: coronary Artery Bypass Grafting Alone or Concomitant Mitral Annuloplasty?. Cardiol Res Pract. 2019;2019:1846904. doi:10.1155/2019/1846904
16. Ouyang X, Ding Y, Yu L, et al. Effects of Hip replacement combined with alendronate sodium on postoperative healing of osteoporotic femoral neck fracture and levels of CTX-1 and BALP in patients. Exp Ther Med. 2019;18(6):4583–4590. doi:10.3892/etm.2019.8158
17. Liu X, Zheng G, Ye B, Chen W, Xie H, Zhang T. Risk factors for surgical opportunity in patients with femoral hernia: a retrospective cohort study. Medicine. 2018;
18. Tooley AA, Klingler KN, Bartley GB, et al. Dacryocystorhinostomy for Acquired Nasolacrimal Duct Stenosis in the Elderly (≥80 Years of Age). Ophthalmology. 2017;124(2):263–267. doi:10.1016/j.ophtha.2016.10.018
19. Greenberg PB, Liu J, Wu WC, et al. Predictors of mortality within 90 days of cataract surgery. Ophthalmology. 2010;117:1894–1899, 1891–1899. doi:10.1016/j.ophtha.2010.02.009
20. Chen PP, Thompson JT. Risk factors for elevated intraocular pressure after the use of intraocular gases in vitreoretinal surgery. Ophthalmic Surg Lasers. 1997;28(1):37–42. doi:10.3928/1542-8877-19970101-08
21. Chandra A, Xing W, Kadhim MR, Williamson TH. Suprachoroidal hemorrhage in pars plana vitrectomy: risk factors and outcomes over 10 years. Ophthalmology. 2014;121(1):311–317. doi:10.1016/j.ophtha.2013.06.021
22. Kumagai K, Ogino N. Results of epiretinal membrane removal combined with PEA and IOL. Semin Ophthalmol. 2001;16(3):151–157. doi:10.1076/soph.16.3.151.4198
23. Li Q, Qian Y, Zhang Y, Sun G, Zhou X, Wang Z. Continuation of Aspirin Therapy before Cataract Surgery with Different Incisions: safe or Not?. J Ophthalmol. 2018;2018:6543937. doi:10.1155/2018/6543937
24. Li Q, Shen X, Wang S, et al. Combined aspirin and clopidogrel therapy in phacoemulsification cataract surgery: a risk factor for ocular hemorrhage?. Int Ophthalmol. 2020;40(8):2023–2029. doi:10.1007/s10792-020-01378-5
25. Wang J, Li Q, Zhang Y, et al. Continuation of aspirin therapy before pars plana vitrectomy: safe or not?. Eur J Ophthalmol. 2020;810696462. doi:10.1177/1120672120946930
26. Wang J, Li Q, Jiang J, et al. Vitrectomy for Idiopathic Macular Hole in Patients Aged 80 Years or Older: efficacy and Safety. Curr Eye Res. 2020;45(6):733–736. doi:10.1080/02713683.2019.1695842
27. Moon SY, Kim S, Lee SY, et al. Laparoscopic surgery for patients with colorectal cancer produces better short-term outcomes with similar survival outcomes in elderly patients compared to open surgery. Cancer Med-Us. 2016;5(6):1047–1054. doi:10.1002/cam4.671
28. Zhu Q, Huang Y, Zhu X, et al. Mannose-coated superparamagnetic iron oxide nanozyme for preventing postoperative cognitive dysfunction. Mater Today Bio. 2023;19:100568. doi:10.1016/j.mtbio.2023.100568
29. Trojnar A, Domagala-Kulawik J, Sienkiewicz-Ulita A, et al. The clinico-pathological characteristics of surgically treated young women with NSCLC. Transl Lung Cancer R. 2022;11(12):2382–2394. doi:10.21037/tlcr-22-443
30. Maillard J, Elia N, Ris F, et al. Changes of health-related quality of life 6 months after high-risk oncological upper gastrointestinal and hepatobiliary surgery: a single-centre prospective observational study (ChangeQol Study). BMJ Open. 2023;
31. Okamoto J, Kubokura H, Usuda J. Factors Determining the Choice of Surgical Procedure in Elderly Patients with Non-Small Cell Lung Cancer. Ann Thorac Cardiovasc Surg. 2016;22:131–138. doi:10.5761/atcs.oa.15-00365
32. Ahiko Y, Shida D, Horie T, et al. Controlling nutritional status (CONUT) score as a preoperative risk assessment index for older patients with colorectal cancer. BMC Cancer. 2019;19:946. doi:10.1186/s12885-019-6218-8
33. Smith KM, Lamy A, Arthur HM, Gafni A, Kent R. Outcomes and costs of coronary artery bypass grafting: comparison between octogenarians and septuagenarians at a tertiary care centre. Can Med Assoc J. 2001;165:759–764.
34. Lau D, Granke K, Olabisi R, Basson MD, Vouyouka A. Carotid endarterectomy in octogenarian veterans: does age affect outcome? A single-center experience. Am J Surg. 2005;190:795–799. doi:10.1016/j.amjsurg.2005.07.022
35. El-Haddawi F, Abu-Zidan FM, Jones W. Factors affecting surgical outcome in the elderly at Auckland Hospital. Anz J Surg. 2002;72(8):537–541. doi:10.1046/j.1445-2197.2002.02484.x
36. Latkauskas T, Rudinskaite G, Kurtinaitis J, et al. The impact of age on post-operative outcomes of colorectal cancer patients undergoing surgical treatment. BMC Cancer. 2005;5(1):153. doi:10.1186/1471-2407-5-153
37. Jackson TL, Donachie PH, Sparrow JM, Johnston RL. United Kingdom National Ophthalmology Database Study of Vitreoretinal Surgery: report 1; case mix, complications, and cataract. Eye. 2013;27(5):644–651. doi:10.1038/eye.2013.12
38. Dugas B, Ouled-Moussa R, Lafontaine PO, et al. Idiopathic epiretinal macular membrane and cataract extraction: combined versus consecutive surgery. Am J Ophthalmol. 2010;149(2):302–306. doi:10.1016/j.ajo.2009.09.011
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of TKI Plus PD-1 Inhibitors in Elderly uHCC Patients: A Retrospective Study
Chen B, Lei J, Zhao H, Dong J, Zeng Z, Li Y, Yu L, Zhou L, Jia A, Lu Y, Cheng J
Journal of Hepatocellular Carcinoma 2022, 9:1171-1185
Published Date: 8 November 2022
Current Insights into the Risks of Using Melatonin as a Treatment for Sleep Disorders in Older Adults
Tuft C, Matar E, Menczel Schrire Z, Grunstein RR, Yee BJ, Hoyos CM
Clinical Interventions in Aging 2023, 18:49-59
Published Date: 12 January 2023
Safety and Performance of OptiVantage, a CT Contrast Media Injector, in Multi-Patient Mode
Tirri A, Iannelli FN, Sequeira A, Hebert F
Medical Devices: Evidence and Research 2025, 18:233-240
Published Date: 12 April 2025
Real-World Experience of Guselkumab in the Elderly Population
Fratton Z, Bighetti S, Bettolini L, Maione V, Rossi M, Venturini M, Mazzoletti V, Zelin E, Stinco G, Errichetti E
Psoriasis: Targets and Therapy 2025, 15:581-601
Published Date: 26 December 2025
Anlotinib Plus Immune Checkpoint Inhibitors versus Chemotherapy in Elderly Patients with Extensive-Stage Small-Cell Lung Cancer: A Real World, Exploratory Study
Lu BW, Zhao C, Wang DZ, Wang W
Drug Design, Development and Therapy 2026, 20:608659
Published Date: 27 May 2026