Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Cost-Utility Analysis of Renal Replacement Therapy Modalities in the Management of Severe Acute Kidney Injury in US Critically Ill Patients
Authors Martins R ![]() , Koyner J, Wald R, Harenski K, Echeverri J
, Koyner J, Wald R, Harenski K, Echeverri J
Received 13 June 2025
Accepted for publication 26 November 2025
Published 15 December 2025 Volume 2025:17 Pages 931—944
DOI https://doi.org/10.2147/CEOR.S546850
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xing Lin Feng
Rui Martins,1,2 Jay Koyner,3 Ron Wald,4– 6 Kai Harenski,7 Jorge Echeverri8
1Health Economics Unit, Global Market Access Solutions, Chardonne, Switzerland; 2GZW Global Health Department, University of Groningen, University Medical Center Groningen, Groningen, the Netherlands; 3Section of Nephrology, University of Chicago, Chicago, IL, USA; 4Division of Nephrology, St. Michael’s Hospital, University of Toronto, Toronto, ON, Canada; 5Li Ka Shing Knowledge Institute, Toronto, ON, Canada; 6Department of Nephrology and Hypertension, Tel Aviv Medical Center, Tel Aviv, Israel; 7Global Medical Affairs, Vantive Health LLC, Unterschleissheim, Germany; 8Global Medical Affairs, Vantive Health LLC, Deerfield, IL, USA
Correspondence: Rui Martins, Health Economics Unit, Global Market Access Solutions, Chardonne, Switzerland, Email [email protected]
Background: Acute kidney injury (AKI) is common among patients admitted to the intensive care unit (ICU), with 5– 15% receiving renal replacement therapy (RRT). Continuous renal replacement therapy (CRRT) and intermittent hemodialysis (IHD) are well-established treatments for severe AKI, but renal recovery is variable and often incomplete, leading to long-term morbidity and mortality. The clinical and cost-effectiveness of either therapy are under active debate. This analysis aims to strengthen the evidence on the cost-utility of CRRT compared with IHD to manage severe AKI in ICU using a US third-party costing perspective.
Methods: The analysis used a 90-day decision tree simulating hospital admission and a semi-Markov process with annual cycles and half-cycle correction to capture lifetime costs and outcomes, discounted at 3% annually. Survivors at 90 days either progressed to ESKD on dialysis (ESKD-D), with some receiving transplants, or became dialysis-independent. In the case of transplant failure, patients returned to ESKD-D. Tunnel states addressed Markov memoryless properties. A US-representative analysis of real-world data applying propensity score matching to control for selection bias informed the probability of lifetime dialysis dependence. Costs and utilities were sourced from peer-reviewed publications or national data. Uncertainty was investigated using deterministic and probabilistic sensitivity analyses.
Results: In the base case, lifetime costs and quality-adjusted life-years (QALYs) were $273,314 and 5.681 for CRRT compared to $268,449 and 5.457 for IHD. CRRT had an 89.6% probability of being cost-effective ($23,860/QALY gained), being associated with 0.269 additional life-years. Long-term CKD management costs, accounting for 50% of CRRT’s excess costs, significantly influenced results and were examined in scenario analyses.
Conclusion: CRRT is likely a cost-effective option for managing severe AKI in the ICU compared with IHD. This study builds on existing economic evaluations by incorporating large comparative studies and exploring clinical uncertainty. The model highlights the need to clarify RRT’s role in CKD progression and enhance post-AKI care to improve patient outcomes.
Keywords: continuous renal replacement therapy, intermittent hemodialysis, acute kidney injury, intensive care unit, cost-effectiveness
Background
Acute kidney injury is common in hospitalized patients worldwide.1 The incidence of AKI is particularly high in individuals admitted to the intensive care unit (ICU).2 It is thought that 5–15% of critically ill admissions experiencing AKI will require renal replacement therapy (RRT).3,4 Patients with AKI suffer significant short- and long-term morbidity and mortality.5
Renal replacement therapies are well-established interventions to manage life-threatening fluid and electrolyte imbalance in the context of severe AKI in the ICU.6 In theory, because CRRT applies slower fluid and electrolyte exchange compared to intermittent hemodialysis, it is thought to be better tolerated by critically ill patients, particularly those who are hemodynamically unstable or fluid overloaded,7,8 compared with IHD. Nonetheless, there is controversy about RRT modalities’ true effect on long-term dialysis requirements, resource utilization and mortality.9
In developed countries, CRRT is the standard therapy for managing AKI in critically ill patients requiring acute dialysis.3,10 Despite CRRT being the most commonly used RRT modality for AKI in the ICU,3 the choice of modality does vary across geographies, according to clinician preference (intensivist vs nephrologist-led care), local expertise, and resource availability.10,11
Randomized controlled studies (RCTs) comparing CRRT with IHD in the management of AKI in the ICU are clinically heterogeneous and not without weaknesses. Issues related to reduced statistical power, allocation/concealment, selection bias, and lack of representativeness of current RRT practices have been documented in the literature.11 Conducting such trials faces significant challenges due to heterogeneity in the etiology of AKI, geographic variation in clinical practice, resource availability, and financial implications associated with the numbers needed to recruit to produce powered comparisons.9,12
Independent research groups have used real-world data and data from a large international RCT to assess the clinical efficacy of CRRT and IHD for AKI in ICU.13,14 Both publications have adjusted for bias in modality allocation at baseline by applying a propensity score methodology, and their results align in proposing that CRRT is associated with a lower likelihood of 90-day dialysis dependence (DD). Skepticism around the perceived higher upfront costs of CRRT has motivated previous analyses assessing the cost-effectiveness of CRRT compared with IHD in the presence or absence of fluid overload.15,16
This study aims to clarify the cost-utility of CRRT, as compared to IHD, in critically ill individuals experiencing AKI in the ICU, using a US third party perspective of costs. The analysis will incorporate recent clinically relevant evidence comparing CRRT with IHD and will expand on published analyses by exploring the long-term impact of CKD progression and transplantation.
Methods
Model Structure
A decision analytic model implemented in Microsoft Excel and Visual Basic for Applications (VBA) was used to simulate the pathway of 60-year-old individuals13 presenting with severe AKI and requiring CRRT or IHD as the initial RRT modality in the ICU (Figure 1). The reporting of this health economic evaluation follows the CHEERS 2022 checklist guidelines.17 The analysis combined a 90-day decision tree covering the period after RRT initiation, and a semi-Markov model with annual cycles and half-cycle correction modeling lifetime costs and outcomes. At 90 days, AKI survivors were modelled to either recover from AKI (ie, be RRT independent) or develop persistent RRT requirement, progressing to the dialysis independence (DI) or ESKD on dialysis (ESKD-D) health states, respectively. Some individuals with ESKD-D were modeled to receive a renal transplant. In the event of graft failure, individuals transitioned to ESKD-D for their lifetime. To overcome the memoryless properties of Markov traces, time to graft failure in deceased or living donor transplant recipients were modelled using tunnel states.
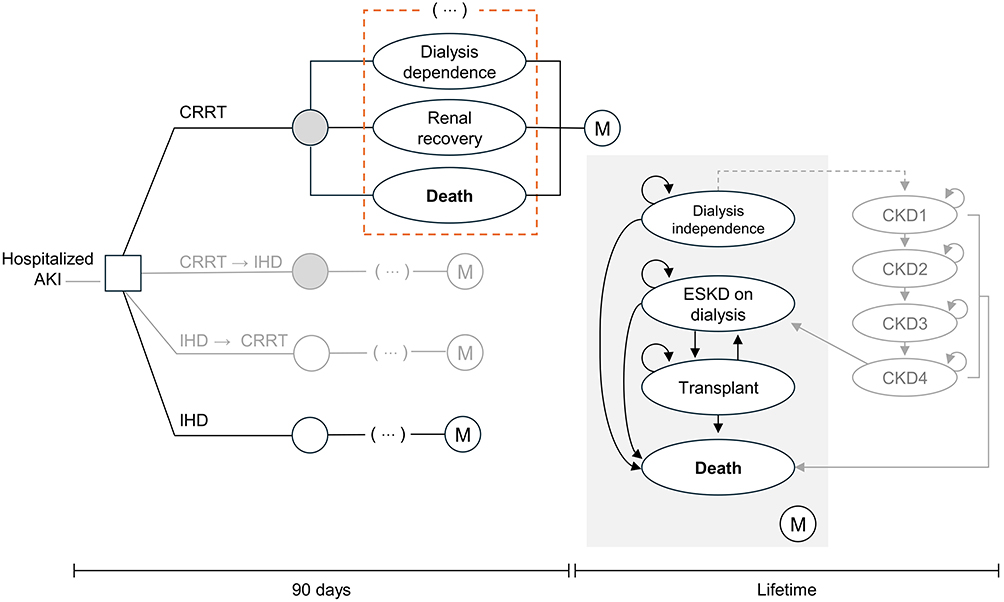 |
Figure 1 Representation of the model structure. Light grey elements of the diagram represent structural variations explored in scenario analyses. To avoid repetition, the health states enclosed in the dashed rectangle (ie Dialysis dependence, Renal recovery, and Death) preceding the semi-Markov process (i.e. “M”) in each branch of the decision tree were replaced by “(…)”. Abbreviations: AKI, acute kidney injury; CKD, chronic kidney disease; ESKD, end-stage kidney disease; IHD, intermittent hemodialysis; M, Markov process. |
Model Inputs
Published systematic literature reviews (SLRs) were scoped to identify existing randomized controlled studies (RCTs) informing the effect of RRT modality on clinical outcomes. Details of the PICOS criteria, literature search strategy, key data extracted, and overlap between published systematic reviews are documented in Supplemental Tables 1,2,3,4, and 5, respectively. Eleven SLRs were identified reporting on 11 RCTs. Overall, RCT quality was low, with most studies lacking statistical power and suffering from treatment crossover or clinical constraints, with unclear impact on the results (Supplemental Table 5).
Consequently, a literature search was conducted in PubMed (Supplemental Table 6), Embase (Supplemental Table 7) and Web of Science (Supplemental Table 8) to identify relevant non-randomized comparative studies (NRCS) with 17 being included for data extraction (Supplemental Figure 1). Details of the outcomes reported by each NRCS are shown in Supplemental Table 9. Several meta-analyses were conducted grouping studies by follow-up duration (Supplemental Figures 2, 3, 4, and 5), method of statistical adjustment for confounding (Supplemental Figure 6), and endpoint statistical measure (Supplemental Figure 7). A final meta-analysis also pooled NRCS and RCTs (Supplemental Figure 8).
RRT Modality and Short-Term Clinical Outcomes
The base case was defined using model parameters/settings perceived to be more robust and generalizable to the US setting. Consequently, in addition, the base case assumed that the RRT modality impacted 90-day dialysis requirements and therapy costs but had no impact on hospital/ICU length-of-stay (LOS) or mortality.4,14 Individuals remaining on RRT at 90 days were assumed not to recover and to become ESKD-D indefinitely.18
Continuous RRT was modeled to reduce 90-day DD, with an odds ratio (OR) of 0.680 (95% confidence interval [CI]: 0.470–0.970). This estimate was based on a study considered representative of the US ICU population with AKI.13 Alternative inputs, including the summary estimate of the ad hoc meta-analysis of NRCS, were explored in scenario analyses.
Treatment switching was modeled as a scenario with 90-day DD being conditional to the initial RRT modality (ie, switching affected solely hospital costs).
Long-Term Clinical Outcomes
USRDS data suggest that 6 to 12 months post discharge, 41% to 43% of DI individuals who survived an episode of in-hospital AKI requiring dialysis present with CKD 3–5.19 Although not specific to the patient population under analysis, this does align with post-ICU CKD prevalence values reported internationally.20 Consequently, in the base case, 60% of the DI individuals were modeled to have completely recovered renal function, with 40% only partially recovering (20% CKD 3, 20% CKD 4). Long-term transitions between CKD severity categories were excluded from base case results.
A sequence of scenarios was implemented to explore the impact of modeling CKD progression. In the absence of specific US data, the distribution of CKD severity in survivors was informed by a nationwide Taiwanese study, following survivors of AKI requiring RRT for more than a year.21 Transitions between CKD severity states used probabilities reported by a systematic review targeting long-term modeling of CKD.22
The probabilities of receiving a renal transplant and graft failure used age-specific data from the US Renal Data System (USRDS).23,24
Mortality
Base case settings assumed no difference in 90-day mortality between comparators. Background mortality was implemented using US lifetables.25 Excess mortality in dialysis-independent individuals was applied in the long-term model according to CKD severity.26 Mortality for ESKD-D and transplanted individuals used USRDS data with extrapolation over 10 years assuming an exponential distribution.27,28 The effect of differential RRT-related mortality was explored in a scenario.14
Costs and Resource Use
Daily costs of hospital and ICU admissions did not differ between comparators.29,30 The daily costs of CRRT and IHD were $919 and $285, respectively.31 Upon discharge, ESKD-D costs were informed by national averages for individuals on hemodialysis or peritoneal dialysis.32 The costs associated with the DI cohort were based on USRDS data33 and weighted using the distribution of CKD severity. Individuals with no CKD were assigned the same healthcare costs as the general US population.34 The costs of transplantation and graft failure were also informed by USRDS.35 All costs were reported as 2024 US dollars. When required, cost was inflated using the US consumer price index.36
Measures of Health Gain
Published utilities derived using preference-based methods were assigned to each modeled health state. RRT modality was assumed not to affect quality of life during ICU stay37 or the remaining hospital admission.38 Survivors experienced reduced utility for up to 90 days post-discharge due to recovery from a critical illness.38 Over the same period, a disutility was applied to those remaining dialysis dependent.39
For the long term, a weighted average utility was calculated using the utility values for hemodialysis and peritoneal dialysis,40 assuming 13.1% of patients were on peritoneal dialysis.41 Because the dialysis independence (DI) cohort was composed of individuals with different levels of kidney impairment, utilities were conditional on CKD distribution. In the absence of CKD, individuals were assigned the age and sex-specific utility of the US general population.42 The impact of kidney impairment on quality of life was informed by a US study applying the EQ-5D to assess quality of life in 205 individuals with CKD.43 The study reported utility estimates above the US population norms for some age groups, so disutilities were calculated as a percentage reduction from the lower severity category (CKD 1) (ie, CKD 3 disutility = (0.90–0.87)/0.90 = 3.3%). These were applied to age- and sex-specific general population utilities, weighted by CKD severity distribution, to estimate the average utility of the cohort with DI. It was assumed that no disutility was associated with CKD 1 and CKD 2 severities. A description of all model inputs and associated uncertainty are described in Table 10 of the Supplemental Materials.
Model Outcomes
Total costs and effects for each comparator were used to calculate incremental cost-effectiveness ratios (ICER). Separate ICERs were calculated using quality-adjusted life-years QALYs and equal value life-years (evLYs) as denominators and presented in parallel. This follows the Inflation Reduction Act requirements of valuing life extension using the same weight, regardless of treatment and population characteristics.44 Steps involved in estimating these metrics were detailed in Section 2.1 of the Supplemental Materials.
Cost-effectiveness was assessed at the usual US threshold of $50,000 to $100,000 per QALY gained.45,46 Costs and life-years were discounted at 3% annually.45,46
Acronyms: C, costs; CRRT, continuous renal replacement therapy; E, effects; ICER, incremental cost-effectiveness ratio; IHD, intermittent hemodialysis.
Acknowledging restrictions to the use of the QALY imposed by the US government results incorporating equal value of life-years gained were reported alongside.44
Sensitivity Analyses
One-way sensitivity analyses (OSA) were conducted using the lower and upper bounds of the 95% CI of all deterministic inputs to examine the impact of the most influential parameters on the results of the model. These findings were summarized in a tornado diagram.
As part of the analysis of uncertainty, scenario analyses were implemented to investigate structural and input-related base case assumptions. Scenarios were implemented using alternative sources for the effect of RRT on 90-day DD, mortality, hospital and ICU LOS, discount rate, time horizon, and modality switching. Additional scenarios investigated the impact of long-term CKD management by modeling CKD progression and the hypothetical effect of RRT modality in reducing CKD severity post discharge.
A Monte Carlo simulation was used to account for parameter uncertainty by sampling 20,000 times from distributions assigned to all model inputs. Results of the probabilistic sensitivity analysis (PSA) were plotted in a cost-effectiveness acceptability curve and cost-effectiveness plane. A complete list of inputs, distributions, and probabilistic parameterization is included in Table 10 of the Supplemental Materials.
Results
Base Case
Base case results suggest that for every 100 individuals requiring RRT for AKI in ICU, IHD was associated with an excess of 2.2 cases of dialysis dependence and 2.1 ESKD-related deaths compared to CRRT. Over the initial 90 days, CRRT was more expensive ($3740) but led to community dialysis savings ($436). In the long term, CRRT was associated with higher CKD management costs ($6738), lower costs from ESKD-D management ($4451), and lower transplantation ($680) and graft failure costs ($104). The breakdown of clinical and cost outcomes is included in Table 11 of the Supplemental Materials.
The model predicted that 99.9% of individuals would be dead within 44 years of the model start. Over this period, CRRT was more expensive ($4864) and more effective, producing 0.269 additional life-years, and higher quality of life (0.223 QALYs, 0.236 evLYs) compared with IHD. Base case results estimated CRRT to be cost-effective at $21,755 per QALY or $20,590 per evLY gained (Table 1).
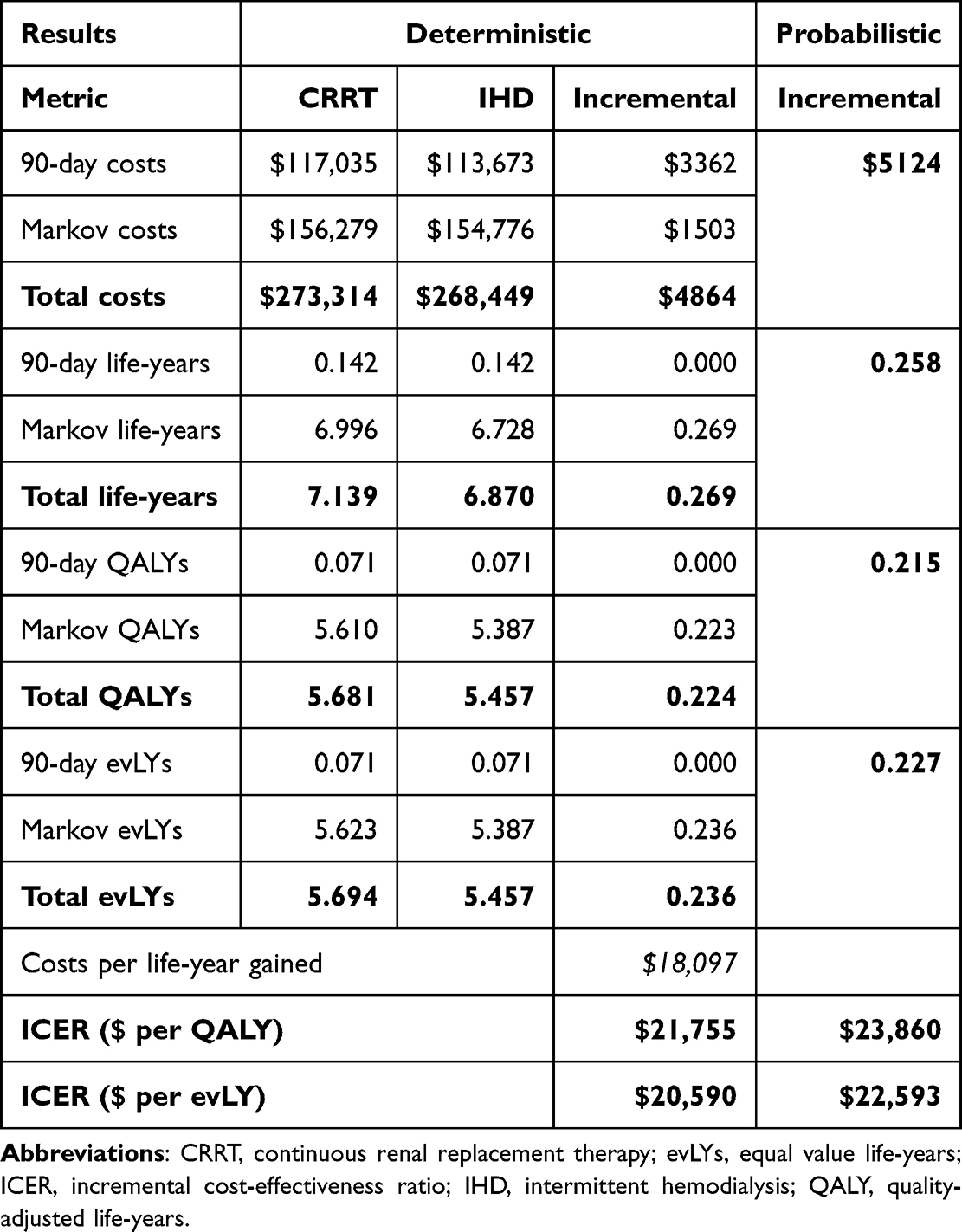 |
Table 1 Base Case Deterministic and Probabilistic Results |
One-Way Sensitivity Analysis
Figure 2 compiles the results of the OSA, highlighting the magnitude of base case result variation driven by the ten most influential model inputs. Among these, the effect of CRRT on dialysis dependence had the greatest impact on the ICER, while the remaining inputs did not alter the overall conclusions of the analysis.
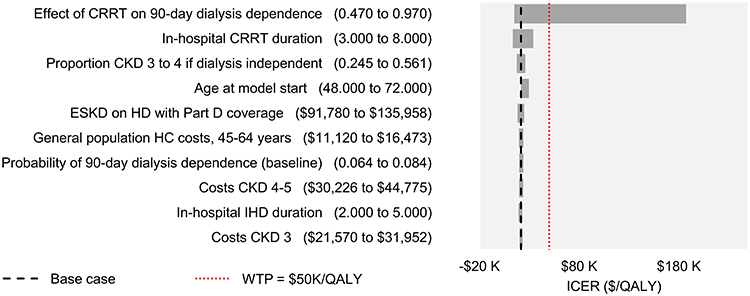 |
Figure 2 Tornado diagram. The bold dashed line represents the base case value of the ICER. The red dotted line represents the $50,000/QALY cost-effectiveness threshold. Horizontal bars crossing the dotted line suggest that varying the associated input affects base case conclusions. Abbreviations: CKD, chronic kidney disease; CRRT, continuous renal replacement therapy; ESKD, end-stage kidney disease; ICER, incremental cost-effectiveness ratio; HC, healthcare costs; HD, hemodialysis; IHD, intermittent hemodialysis; QALY, quality-adjusted life-year; WTP, willingness to pay. |
Scenario Analyses
Table 2 summarizes the deterministic scenarios implemented to challenge the base case model assumptions. Changing the source of the effect of CRRT on DD to a secondary analysis of the STARRT-AKI trial and the meta-analysis of non-randomized comparative studies conducted by the authors did not change the overall conclusions, decreasing the ICER by 14.1% or increasing it by 20.4%, respectively. Switching RRT modalities, changing the discount rate, and reducing the risk of death in those initially treated with CRRT also had modest effects on the ICER. The results were extremely sensitive to hospital/ICU length of stay variations, with CRRT becoming dominant (cheaper and more effective than IHD). Altering the analytical time horizon revealed that a substantial proportion of the costs were incurred within the initial 10 years. Scenarios altering the composition of the DI cohort also had an important effect on results due to their effect on mortality and long-term costs of managing CKD. Assuming that the entire DI cohort was free from CKD halved the base case ICER. Modelling CKD progression more than doubled the value of the ICER, reaching values around the lower bound of the $50,000 to $100,000 cost-effectiveness threshold. Modelling CKD progression also reduced the cohort’s overall longevity, with 99.9% of individuals dying within 39 years of model onset. Assuming CRRT would avoid 5% of CKD progression across severities more than halved the value of the ICER ($20,407/QALY, $18,660/evLY).
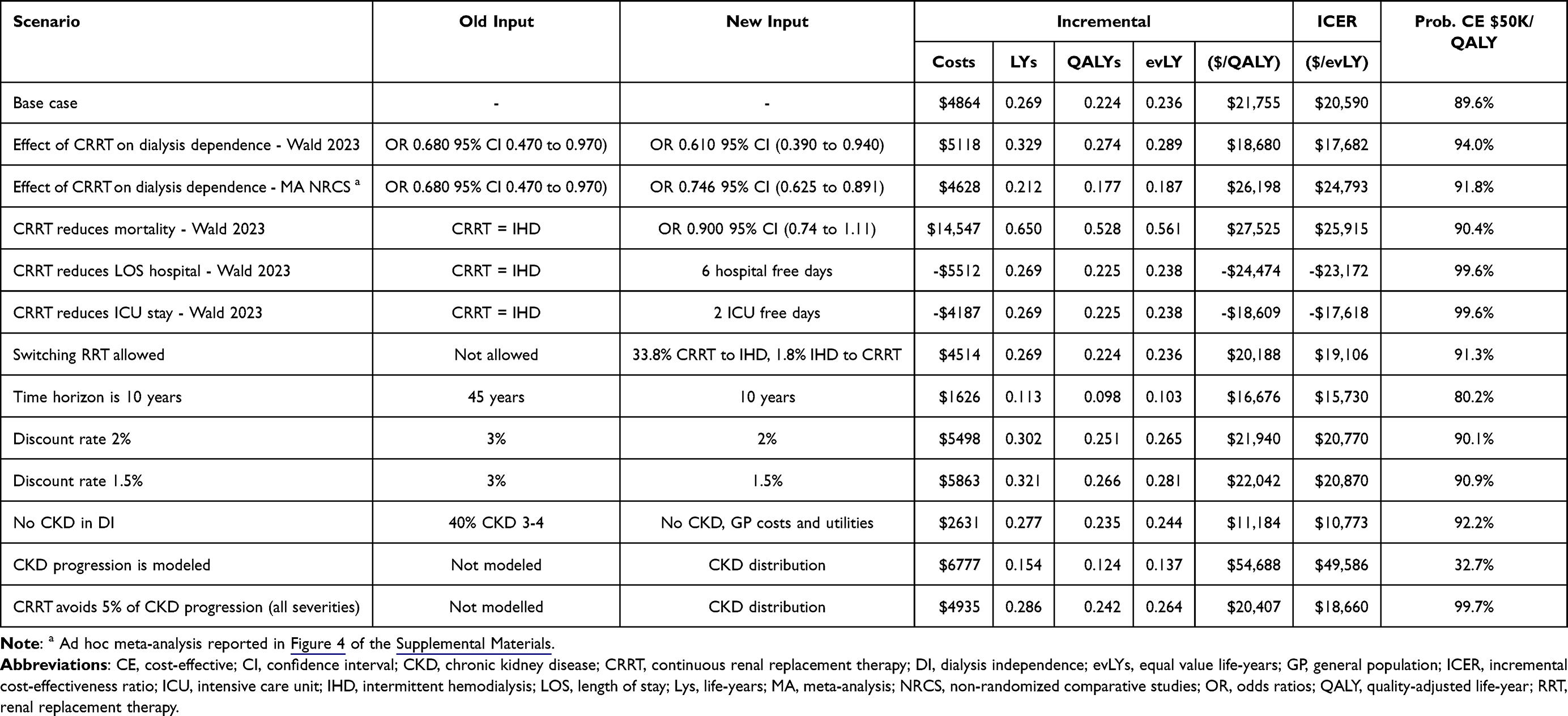 |
Table 2 Scenario Analyses |
The characteristics of the DI cohort greatly impacted the results, warranting further exploration. The protective effect of CRRT in reducing DD in critically ill individuals requiring RRT for AKI may also contribute to delaying or preventing escalation of CKD severity. Despite being physiologically plausible, this has not been assessed in clinical trials and was investigated in a series of scenarios depicted in Figure 3. A less conservative scenario assumed that a proportion of all CKD was avoided (bold line). An intermediate scenario assumed a proportion stepdown to less severe CKD/no-CKD (all severities, grey line). A more conservative scenario assumed a proportion stepdown in CKD 3 and 4 to less severe CKD (dotted line).
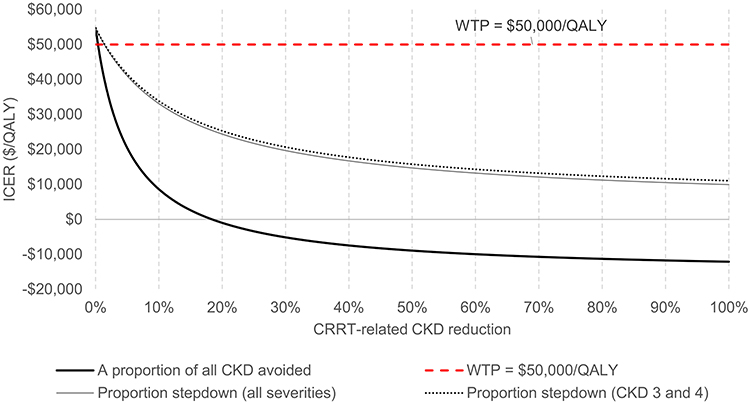 |
Figure 3 Scenario analysis exploring CKD progression. Abbreviations: CKD, chronic kidney disease; ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life-year; WTP, willingness to pay. |
Probabilistic Sensitivity Analysis
The result of 20,000 Monte Carlo simulations comparing CRRT with IHD was plotted in the cost-effectiveness plane (Figure 4). Mean PSA results (Table 1) suggest that CRRT was associated with an 89.6% probability of being cost-effective according to base case settings. The probability of cost-effectiveness over a range of willingness to pay values is represented graphically in Figure 5.
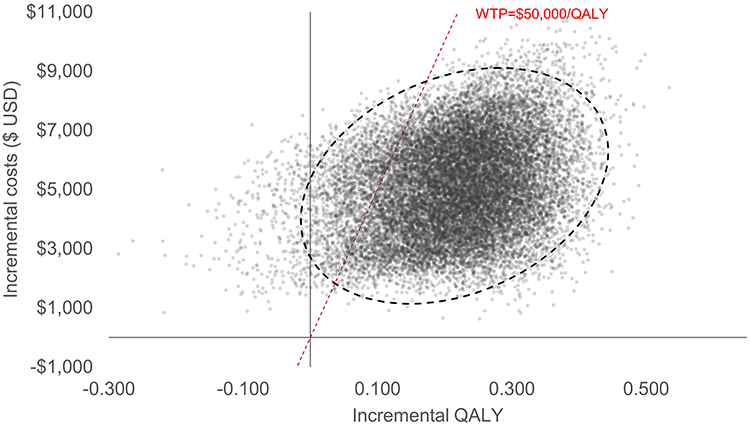 |
Figure 4 Cost-effectiveness plane. The confidence ellipse circumscribes 95% of the sampled mean ICERs. Abbreviations: QALY, quality-adjusted life-years; USD, United States dollars. |
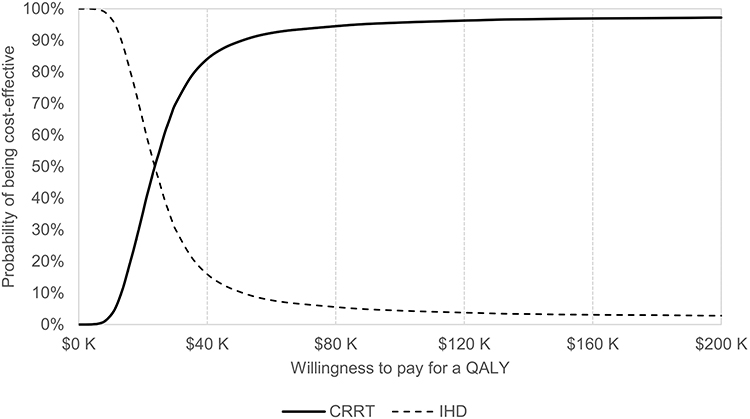 |
Figure 5 Cost-effectiveness acceptability curves of CRRT vs IHD. Abbreviations: CRRT, continuous renal replacement therapy; IHD, intermittent hemodialysis; QALY, quality-adjusted life-years. |
Discussion
This cost-utility analysis estimated that CRRT is associated with a higher probability of being cost-effective in the management of severe AKI in the ICU compared with IHD. Individuals receiving CRRT were predicted to survive 0.269 additional life-years and to have a better quality of life, an excess of 0.224 QALYs or 0.236 evLYs. The model has shown that for every 100 individuals with severe AKI, initial treatment with CRRT led to the avoidance of approximately two deaths and two cases of permanent dialysis dependence. Over a lifetime, CRRT was $4864 more expensive than IHD. Whilst some of this difference in cost was related to the initial costs of therapy, close to 30% was linked to the management of dialysis independent CKD. Further, in the scenarios exploring long-term CKD progression, worsening CKD, potentially leading to ESKD-D and renal transplantation, accounted for 50% of the incremental cost difference.
In general, our results support the findings of previous economic evaluations comparing CRRT with IHD in US settings15,16 and elsewhere.47,48 Nonetheless, significant differences in the summary ICERS can be found between our study and the analogous publication by Ethgen et al 2015.16 Higher ICERs reported in the present study were likely driven by a more conservative effect of CRRT on DD, a lower number of IHD days in ICU relative to CRRT,49 and conservative (CKD-adjusted) utility and cost values assigned to the dialysis independence health state.
Our research addresses concerns about data quality raised by previous studies that found CRRT to be cost-ineffective.50 This was achieved by extensively reviewing both randomized and non-randomized studies comparing CRRT and IHD, prioritizing data perceived to be more robust, representative of the US context, and reflective of current RRT practices. While randomized trials are the gold standard for assessing intervention efficacy, challenges such as clinical heterogeneity, lack of clinician blinding, the tendency to assign sicker patients to CRRT (selection bias), and variations in RRT dose and practices have complicated RCT implementation and led to inconsistent findings (Ye et al, 2021). Further, assuming a baseline mortality probability of 46.9%14 and a 7.4% probability of DD13 for individuals on IHD, a RCT capable of detecting a 5–10% variation in mortality and a 2–5% difference in DD with an 80% power using a two-sided alpha of 5% would require sample sizes of 1549 (5% difference mortality) to 381 (10% difference in mortality), and 2350 (2% difference in DD) to 291 (5% difference in DD).51 It becomes clear that very few RCTs were set up to detect such differences and that doing so would involve substantial funds and coordination. Published analyses of large datasets13,14,52,53 avoid some of the obstacles to implementing such a trial, whilst making use of techniques such as propensity matching and inverse probability treatment weighting to account for biases inherent to observational data. This analysis used a reproducible methodology and is compliant with national and international standards for economic evaluation.45,46,54 The model framework is aligned with published economic evaluations of treatments for acute and chronic kidney diseases.15,16,55,56 The selection of model inputs and settings was discussed thoroughly and validated by experts in critical care and clinical research.
Base case results were subject to extensive sensitivity analysis, which contributed to mapping and communicating the uncertainty surrounding inputs and model settings. The results were robust to the deterministic and probabilistic sensitivity analyses. The OSA has demonstrated the extreme sensitivity of the ICER to the effect of CRRT on DD. This input is core to the incremental difference between CRRT and IHD, so this effect was anticipated. It is not expected that all patients would present levels of DD at the extremes set by a 95% confidence interval. Conversely, PSA results incorporating all parameter uncertainty agreed with the deterministic base case.
In sum, our results expand on previous publications by providing compelling evidence of CRRT cost-effectiveness,15,16 incorporating robust evidence of the effect of CRRT on DD13,14 whilst addressing longstanding data quality concerns, and finally by exploring the important role of long-term CKD costs.
There are several limitations to this analysis. Whilst we aim to generalize our conclusions to the US population of individuals with severe AKI, the model does not account for local variation in RRT practice, built-in expertise, or geographical availability of either therapy. These factors may limit the applicability of these results to specific jurisdictions.
Though some patients do become dialysis-independent after 90 days this is unlikely, dialysis dependence at 90 days was used as a proxy for lifetime dialysis dependence.18,20 The implemented 90-day duration of the decision tree was deemed appropriate as it is a follow-up commonly reported by key clinical studies assessing the role of RRT on AKI progression.11,13,14,49,57–59 In addition, 90-days marks the ends of the acute phase of AKI in survivors.60 The analysis focused on the CRRT vs IHD comparison, with other RRT modalities being excluded. This was done deliberately, based on the rationale that CRRT and IHD are most commonly utilized for critically ill individuals.6,11 Modalities such as sustained low efficiency dialysis (SLED) are used in a few centers.3,9
Another limitation is that the costs of RRT were based on estimates reported by a Canadian study.31 We were unable to identify a publication reporting alternative US-specific inputs. Although not identical, the Canadian data shares a similar socio-economic context and medical practices to the US. Cost inflation and currency conversion were transparently conducted using standard methods. In addition, the base case assumes a $634 cost difference (higher for CRRT) which is conservative when compared with the $290 excess CRRT costs reported in the literature.61 Varying the costs of CRRT in OSA seemed not to impact the conclusions of the analysis. Specifically, CRRT and IHD duration (proxies for total modality cost) were identified as influential parameters, but one-way variation of the deterministic base case inputs did not cross the threshold for cost-effectiveness (Figure 2).
Readmission to hospital was not modeled as no published evidence was found of a CRRT/IHD incremental difference. For simplicity, it was assumed that severity-specific CKD costs would account for direct medical costs from readmission and other inherent complications.
Additional uncertainty may have been introduced by inputs obtained from studies with relatively small sample sizes43 (ie, CKD utilities). Uncertainty around these inputs was assessed deterministically and probabilistically and did not seem to affect base case results.
This study only accounted for direct medical costs of severe AKI and CKD and did not capture direct non-medical costs or indirect costs associated with kidney impairment. It is likely that including direct non-medical and indirect costs of CKD would increase the costs of CRRT, as this strategy was associated with a larger number of survivors, lower proportion of dialysis dependence, and consequently a higher absolute number of people living with CKD. Nonetheless, there is uncertainty surrounding the role of RRT modality on the distribution of CKD severity. It is therefore difficult to conclude the direction of effect of including such costs if CKD severity post-discharge is differential between comparators, as higher severity implies significantly higher costs, but also additional mortality.
The model accounted for the change in therapy costs associated with treatment switching, but this had a negligible impact on results. A more comprehensive assessment of the clinical and economic implications of RRT modality switching would require information about the circumstances of switching (duration of therapy, reason for switching) and its consequences (mortality, dialysis requirements) which, to the best of our knowledge, is currently unsupported by clinical evidence.
Finally, the authors would also like to draw attention to the important impact of prevalent CKD on long-term morbidity, mortality, and costs in individuals partially recovering from AKI who require RRT. Future research should investigate the impact of RRT modality on non-dialysis-requiring CKD in survivors of severe AKI in the ICU.
Conclusion
This cost-utility analysis supports the cost-effectiveness of CRRT compared with IHD in managing severe AKI in the ICU setting. CRRT was associated with an extension of life and quality of life. However, CRRT incurred higher lifetime costs, largely driven by CKD progression and subsequent management.
Given the challenges of conducting RCTs to detect small but meaningful differences in mortality and dialysis dependence, large observational datasets remain valuable for informing economic models.
Future research should explore the role of acute RRT modality on CKD prevention and refine estimates of renal impairment in AKI survivors. Addressing these uncertainties is critical for optimizing resource allocation and improving long-term outcomes for critically ill patients receiving RRT.
Abbreviations
AKI, acute kidney injury; CKD, chronic kidney disease; CMS, Centers for Medicare and Medicaid Services; CRRT, continuous renal replacement therapy; DD, dialysis dependence; DI, dialysis independence; ESKD, end-stage kidney disease; ESKD-D, dialysis dependent end-stage kidney disease; evLYs, equal value life-years; HD, hemodialysis; ICER, incremental cost-effectiveness ratio; ICU, intensive care unit; IHD, intermittent hemodialysis; IQR, interquartile range; LOS, length of stay; MA, meta-analysis; NRCS, non-randomized comparative studies; OR, odds ratios; OSA, one-way sensitivity analysis; PD, peritoneal dialysis; PSA, probabilistic sensitivity analysis; QALY, quality-adjusted life-year; RCTS, randomized controlled studies; RR, relative risk; RRT, renal replacement therapy; SE, standard error; STARRT-AKI, standard versus accelerated initiation of renal replacement therapy in acute kidney injury study; US, United States; USRDS, United States Renal Data System; WTP, willingness to pay.
Disclosure
This analysis was funded by Vantive Health LLC (formerly the Baxter Kidney Care segment). This publication was subject to review by internal employees from Vantive Health LLC prior to submission for protection of Confidential Information. However, the Authors retain full responsibility for the content of this publication.
RM is an employee for Global Market Access Solutions and has received consulting fees from Vantive Health LLC (formerly Baxter Healthcare Corporation) for developing the present economic model.
JE and KH are full-time employees of Vantive Health LLC.
JK and RW have received consulting fees from Vantive Health LLC.
Dr Jay Koyner reports grants, personal fees from biomerieux, grants, personal fees from fresenius, personal fees from alexion, personal fees from novartis, personal fees from guard therapeutics, grants, personal fees from bioporto, outside the submitted work.
Dr Ron Wald reports personal fees from Baxter, during the conduct of the study.
The authors report no other conflicts of interest in his work.
References
1. Susantitaphong P, Cruz DN, Cerda J, et al. World incidence of AKI: a meta-analysis. Clin J Am Soc Nephrol. 2013;8(9):1482–1493. doi:10.2215/CJN.00710113
2. Case J, Khan S, Khalid R, Khan A. Epidemiology of acute kidney injury in the intensive care unit. Crit Care Res Pract. 2013;2013:479730. doi:10.1155/2013/479730
3. Hoste EA, Bagshaw SM, Bellomo R, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41(8):1411–1423. doi:10.1007/s00134-015-3934-7
4. Nash DM, Przech S, Wald R, O’Reilly D. Systematic review and meta-analysis of renal replacement therapy modalities for acute kidney injury in the intensive care unit. J Crit Care. 2017;41:138–144. doi:10.1016/j.jcrc.2017.05.002
5. Hoste EAJ, Kellum JA, Selby NM, et al. Global epidemiology and outcomes of acute kidney injury. Nat Rev Nephrol. 2018;14(10):607–625. doi:10.1038/s41581-018-0052-0
6. International Society of Nephrology. KDIGO clinical practice guideline for acute kidney injury. Injury Kidney Int Suppl. 2012;120(4):c179–84
7. Bell M, Granath, Swing S, et al. Continuous renal replacement therapy is associated with less chronic renal failure than intermittent haemodialysis after acute renal failure. Intensive Care Med. 2007;33(5):773–780. doi:10.1007/s00134-007-0590-6
8. Schneider AG, Bellomo R, Bagshaw SM, et al. Choice of renal replacement therapy modality and dialysis dependence after acute kidney injury: a systematic review and meta-analysis. Intensive Care Med. 2013;39(6):987–997. doi:10.1007/s00134-013-2864-5
9. Wang AY, Bellomo R. Renal replacement therapy in the ICU: intermittent hemodialysis, sustained low-efficiency dialysis or continuous renal replacement therapy? Curr Opin Crit Care. 2018;24(6):437–442. doi:10.1097/MCC.0000000000000541
10. Vaara ST, Serpa Neto A, Bellomo R, et al. Regional practice variation and outcomes in the standard versus accelerated initiation of renal replacement therapy in acute kidney injury (STARRT-AKI) trial: a post hoc secondary analysis. Crit Care Explor. 2024;6(2):e1053. doi:10.1097/CCE.0000000000001053
11. Ye Z, Wang Y, Ge L, et al. Comparing renal replacement therapy modalities in critically ill patients with acute kidney injury: a systematic review and network meta-analysis. Crit Care Explor. 2021;3(5):e0399. doi:10.1097/CCE.0000000000000399
12. Pannu N, Gibney RN. Renal replacement therapy in the intensive care unit. Ther Clin Risk Manag. 2005;1(2):141–150. doi:10.2147/tcrm.1.2.141.62908
13. Koyner JL, Mackey RH, Echeverri J, et al. Initial renal replacement therapy (RRT) modality associates with 90-day postdischarge RRT dependence in critically ill AKI survivors. J Crit Care. 2024;82:154764. doi:10.1016/j.jcrc.2024.154764
14. Wald R, Gaudry S, da Costa BR, et al. Initiation of continuous renal replacement therapy versus intermittent hemodialysis in critically ill patients with severe acute kidney injury: a secondary analysis of STARRT-AKI trial. Intensive Care Med. 2023;49(11):1305–1316. doi:10.1007/s00134-023-07211-8
15. Ethgen O, Murugan R, Echeverri J, Blackowicz M, Harenski K, Ostermann M. Economic analysis of renal replacement therapy modality in acute kidney injury patients with fluid overload. Crit Care Explor. 2023;5(6):e0921.
16. Ethgen O, Schneider AG, Bagshaw SM, Bellomo R, Kellum JA. Economics of dialysis dependence following renal replacement therapy for critically ill acute kidney injury patients. Nephrol Dial Transplant. 2015;30(1):54–61. doi:10.1093/ndt/gfu314
17. Husereau D, Drummond M, Augustovski F, et al. Consolidated health economic evaluation reporting standards 2022 (CHEERS 2022) statement: updated reporting guidance for health economic evaluations. BMC Med. 2022;20(1):23. doi:10.1186/s12916-021-02204-0
18. Cerdá J, Liu KD, Cruz DN, et al. Promoting kidney function recovery in patients with AKI requiring RRT. Clin J Am Soc Nephrol. 2015;10(10):1859–1867. doi:10.2215/CJN.01170215
19. USRDS. 4.1 AKI - Chronic kidney disease status during 24 months following live discharge from first hospitalization with acute kidney injury in older adults without pre-existing CKD, 2017-2019. 2023. Available from: https://usrds-adr.niddk.nih.gov/2023/chronic-kidney-disease/4-acute-kidney-injury.
20. De Corte W, Dhondt A, Vanholder R, et al. Long-term outcome in ICU patients with acute kidney injury treated with renal replacement therapy: a prospective cohort study. Critical Care. 2016;20(1):256. doi:10.1186/s13054-016-1409-z
21. Pan H-C, Chen H-Y, Teng N-C, et al. Recovery dynamics and prognosis after dialysis for acute kidney injury. JAMA Network Open. 2024;7(3):e240351–e240351. doi:10.1001/jamanetworkopen.2024.0351
22. Sugrue DM, Ward T, Rai S, McEwan P, van Haalen HGM. Economic modelling of chronic kidney disease: a systematic literature review to inform conceptual model design. Pharmacoeconomics. 2019;37(12):1451–1468. doi:10.1007/s40273-019-00835-z
23. USRDS. Annual Data Report: epidemiology of kidney disease in the United States. Table E.10 - Renal transplant rates, by donor type; All donor types: by age, sex, race/ethnicity, primary diagnosis, per 100 dialysis patient years, unadjusted. 2023. Available from: https://adr.usrds.org/2023.
24. USRDS. Annual Data Report: epidemiology of kidney disease in the United States. Reference tables - F: transplantation outcomes, Probability of graft failure necessitating dialysis or retransplantation. 2023. Available from: https://adr.usrds.org/2023.
25. Arias E, Jiaquan X, Kochanek K. United States Life Tables, 2021. Hyattsville: National Center for Health Statistics; 2023.
26. CKD Prognosis Consortium. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375(9731):2073–2081. doi:10.1016/S0140-6736(10)60674-5
27. USRDS. Annual Data Report: epidemiology of kidney disease in the United States. Reference tables - Survival, Probability of death with a functioning graft. 2023. Available from: https://adr.usrds.org/2023.
28. USRDS. Annual Data Report: epidemiology of kidney disease in the United States. Reference tables - I: survival, Survival probabilities: incident dialysis patients, adjusted for age, sex, race/ethnicity, and primary cause of ESRD. 2023. Available from: https://adr.usrds.org/2023.
29. Dasta JF, McLaughlin TP, Mody SH, Piech CT. Daily cost of an intensive care unit day: the contribution of mechanical ventilation. Crit Care Med. 2005;33(6):1266–1271. doi:10.1097/01.CCM.0000164543.14619.00
30. Foundation KF. Hospital Adjusted Expenses per Inpatient Day. 2022. Available from: https://www.kff.org/health-costs/state-indicator/expenses-per-inpatient-day/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D.
31. Manns B, Doig CJ, Lee H, et al. Cost of acute renal failure requiring dialysis in the intensive care unit: clinical and resource implications of renal recovery. Crit Care Med. 2003;31(2):449–455. doi:10.1097/01.CCM.0000045182.90302.B3
32. USRDS. Annual Data Report: epidemiology of kidney disease in the United States. Section K: medicare Costs for ESRD patients. Tables K.7.1 and K.8.1. 2023. Available from: https://adr.usrds.org/2023.
33. USRDS. Annual Data Report: epidemiology of kidney disease in the United States. Tables 6.3 and 6.4 - Per person per year spending among adults with CKD (ESRD excluded), by CKD stage overall and by patient characteristics, 2020, Medicare FFS. 2022. Available from: https://www.niddk.nih.gov/about-niddk/strategic-plans-reports/usrds/prior-data-reports.
34. CMS. Total Personal Health Care Per-capita Spending by Sex and Age Group, Calendar Years 2002, 2004, 2006, 2008, 2010, 2012, 2014, 2016, 2018, 2020. 2020. Available from: https://www.cms.gov/data-research/statistics-trends-and-reports/national-health-expenditure-data/age-and-sex.
35. USRDS. Annual Data Report: epidemiology of kidney disease in the United States. Section K: healthcare Expenditures for CKD - Tables Table K.11.1, K.12.1, and K.13.1. 2023. Available from: https://adr.usrds.org/2023.
36. US Bureau of Labor Statistics. Consumer Price Index for All Urban Consumers (CPI-U) - Medical care in U.S. city average, all urban consumers, not seasonally adjusted. 2025. Available from: https://data.bls.gov/toppicks?survey=cu.
37. De Smedt DM, Elseviers MM, Lins RL, Annemans L. Economic evaluation of different treatment modalities in acute kidney injury. Nephrol Dial Transplant. 2012;27(11):4095–4101. doi:10.1093/ndt/gfs410
38. Hernández RA, Jenkinson D, Vale L, Cuthbertson BH. Economic evaluation of nurse-led intensive care follow-up programmes compared with standard care: the PRaCTICaL trial. Eur J Health Econ. 2014;15(3):243–252. doi:10.1007/s10198-013-0470-7
39. Wyld M, Morton RL, Hayen A, Howard K, Webster AC. A systematic review and meta-analysis of utility-based quality of life in chronic kidney disease treatments. PLoS Med. 2012;9(9):e1001307. doi:10.1371/journal.pmed.1001307
40. Manns B, Johnson JA, Taub K, Mortis G, Ghali WA, Donaldson C. Quality of life in patients treated with hemodialysis or peritoneal dialysis: what are the important determinants? Clin Nephrol. 2003;60(5):341–351. doi:10.5414/CNP60341
41. USRDS. Annual Data Report: epidemiology of kidney disease in the United States. Section D: modality - Percentages and counts of reported ESRD patients: by treatment modalityTables K.7.1 and K.8.1. 2023. Available from: https://adr.usrds.org/2023.
42. Jiang R, Janssen MFB, Pickard AS. US population norms for the EQ-5D-5L and comparison of norms from face-to-face and online samples. Qual Life Res. 2021;30(3):803–816. doi:10.1007/s11136-020-02650-y
43. Gorodetskaya I, Zenios S, McCulloch CE, et al. Health-related quality of life and estimates of utility in chronic kidney disease. Kidney Int. 2005;68(6):2801–2808. doi:10.1111/j.1523-1755.2005.00752.x
44. Campbell JD, Whittington MD, Pearson SD. An alternative measure of health for value assessment: the equal value life-year. Pharmacoeconomics. 2023;41(10):1175–1182. doi:10.1007/s40273-023-01302-6
45. Institute for Clinical and Economic Review. Value Assessment Framework. 2023. Available from: https://icer.org/wp-content/uploads/2023/10/ICER_2023_VAF_For-Publication_101723.pdf.
46. Sanders GD, Neumann PJ, Basu A, et al. Recommendations for conduct, methodological practices, and reporting of cost-effectiveness analyses: second panel on cost-effectiveness in health and medicine. JAMA. 2016;316(10):1093–1103. doi:10.1001/jama.2016.12195
47. Phongphithakchai A, Liabsuetrakul T, Boonsrirat U. Cost-utility analysis of separated continuous renal replacement therapy systems versus intermittent hemodialysis in critically ill patients with acute kidney injury in a low-resource setting. Artificial Organs. 2023;47(9):1522–1530. doi:10.1111/aor.14557
48. Ramirez MG, Costa MD, Costa Carvalho M. Cost-effectiveness analysis of continuous versus intermittent renal replacement therapy for critically ILL acute kidney injury patients under the perspective of the brazilian private healthcare system. Value Health. 2017;20(9):A867. doi:10.1016/j.jval.2017.08.2528
49. STARRT-AKI Investigators. timing of initiation of renal-replacement therapy in acute kidney injury. New Engl J Med. 2020;383(3):240–251. doi:10.1056/NEJMoa2000741
50. Klarenbach S, Manns B, Pannu N, Clement FM, Wiebe N, Tonelli M. Economic evaluation of continuous renal replacement therapy in acute renal failure. Int J Technol Assessment Health Care. 2009;25(3):331–338. doi:10.1017/S0266462309990134
51. Kirkwood BR, Sterne JAC. Essential Medical Statistics. Wiley; 2010.
52. Liang KV, Sileanu FE, Clermont G, et al. Modality of RRT and recovery of kidney function after aki in patients surviving to hospital discharge. Clin J Am Soc Nephrol. 2016;11(1):30–38. doi:10.2215/CJN.01290215
53. Naorungroj T, Neto AS, Wang A, Gallagher M, Bellomo R. Renal outcomes according to renal replacement therapy modality and treatment protocol in the ATN and RENAL trials. Critical Care. 2022;26(1). doi:10.1186/s13054-022-04151-5
54. National Institute for Health and Care Excellence. NICE health technology evaluations: the manual. 2023. Available from: https://www.nice.org.uk/process/pmg36.
55. Hall PS, Mitchell ED, Smith AF, et al. The future for diagnostic tests of acute kidney injury in critical care: evidence synthesis, care pathway analysis and research prioritisation. Health Technol Assess. 2018;22(32):1–274. doi:10.3310/hta22320
56. Jacobsen E, Sawhney S, Brazzelli M, et al. Cost-effectiveness and value of information analysis of NephroCheck and NGAL tests compared to standard care for the diagnosis of acute kidney injury. BMC Nephrol. 2021;22(1):399. doi:10.1186/s12882-021-02610-9
57. Bagshaw SM, Berthiaume LR, Delaney A, Bellomo R. Continuous versus intermittent renal replacement therapy for critically ill patients with acute kidney injury: a meta-analysis. Crit Care Med. 2008;36(2):610–617. doi:10.1097/01.CCM.0B013E3181611F552
58. Ma H, Liu H, Wang Y, Liu Y, He J, Yang Q. Efficacy of continuous renal replacement therapy and intermittent hemodialysis in patients with renal failure in intensive care unit: a systemic review and meta-analysis. Evid Based Complement Alternat Med. 2023;2023:8688974. doi:10.1155/2023/8688974
59. Wald R, Shariff SZ, Adhikari NKJ, et al. The association between renal replacement therapy modality and long-term outcomes among critically ill adults with acute kidney injury: a retrospective cohort study*. Crit Care Med. 2014;42(4):868–877. doi:10.1097/CCM.0000000000000042
60. Improving Global Outcomes (KDIGO) CKD Work Group. Clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2024;105(4S):S117–S314.
61. Srisawat N, Lawsin L, Uchino S, Bellomo R, Kellum JA. Cost of acute renal replacement therapy in the intensive care unit: results from the beginning and ending supportive therapy for the kidney (BEST Kidney) study. Crit Care. 2010;14(2):R46. doi:10.1186/cc8933
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nomogram Prediction Model of Serum Chloride and Sodium Ions on the Risk of Acute Kidney Injury in Critically Ill Patients
Lu J, Qi Z, Liu J, Liu P, Li T, Duan M, Li A
Infection and Drug Resistance 2022, 15:4785-4798
Published Date: 24 August 2022
Exploring the Cost-Utility of a Biomarker Predicting Persistent Severe Acute Kidney Injury: The Case of C-C Motif Chemokine Ligand 14 (CCL14)
Echeverri J, Martins R, Harenski K, Kampf JP, McPherson P, Textoris J, Koyner JL
ClinicoEconomics and Outcomes Research 2024, 16:1-12
Published Date: 12 January 2024
Neutrophil Gelatinase-Associated Lipocalin and Interleukin-18 in the Prediction of Acute Kidney Injury in Sepsis Patients
Liu Y, Li C, Yang X, Guo S, Cui Z, Kang H, Ma Z, Wang H
International Journal of General Medicine 2024, 17:6335-6341
Published Date: 18 December 2024