Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Cost-Effectiveness of Triple Therapy with Budesonide/Glycopyrronium/Formoterol Fumarate Dihydrate versus Dual Therapies in Moderate-to-Very Severe Chronic Obstructive Pulmonary Disease: United Kingdom Analysis Using the ETHOS Study
Authors de Nigris E, Treharne C, Brighton N, Holmgren U ![]() , Walker A, Haughney J
, Walker A, Haughney J
Received 4 July 2022
Accepted for publication 9 November 2022
Published 22 November 2022 Volume 2022:17 Pages 2987—3000
DOI https://doi.org/10.2147/COPD.S381138
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Richard Russell
Enrico de Nigris,1 Catrin Treharne,2 Nick Brighton,2 Ulf Holmgren,3 Andrew Walker,4 John Haughney5
1Formerly of Global Product and Portfolio Strategy, AstraZeneca, Cambridge, UK; 2Formerly of Health Economic Modelling, Regulatory and Access, Parexel International, London, UK; 3Real World Science and Digital, BioPharmaceuticals Medical, AstraZeneca, Gothenburg, Sweden; 4Salus Alba, Glasgow, UK; 5Clinical Research Facility, Queen Elizabeth University Hospital, Glasgow, UK
Correspondence: Ulf Holmgren, AstraZeneca, Pepparedsleden 1, Gothenburg, SE-431 83, Sweden, Tel +46 0 317 761 424, Email [email protected]
Background: In the 52-week ETHOS study (NCT02465567), fixed-dose triple therapy with budesonide/glycopyrronium/formoterol fumarate dihydrate (BGF) reduced moderate or severe chronic obstructive pulmonary disease (COPD) exacerbations versus fixed-dose long-acting muscarinic antagonist (LAMA)/long-acting β2-agonist (LABA) or inhaled corticosteroid (ICS)/LABA dual therapies. Here, ETHOS data were used to estimate the long-term cost-effectiveness of BGF versus LAMA/LABA and ICS/LABA dual therapies in the United Kingdom.
Methods: Costs, exacerbations, quality-adjusted life-years (QALYs), and LYs were extrapolated using a Markov model that considered disease severity progression, risk of moderate and severe exacerbations, adverse events, and treatment discontinuation in patients with moderate-to-very severe COPD receiving BGF 320/14.4/10 μg, the LAMA/LABA glycopyrronium/formoterol fumarate dihydrate 14.4/10 μg (GFF), or the ICS/LABA budesonide/formoterol fumarate dihydrate 320/10 μg (BFF). Utilities for COPD severity states were estimated using EuroQol 5-dimension 5-level data from ETHOS. Exacerbation disutilities were sourced from published literature. Healthcare resource utilization was based on ETHOS data, published literature, key external experts’ input, and informed assumptions. Unit costs came from the UK National Health Service Schedule of Reference Costs, Unit Costs of Health and Social Care from the Personal Social Services Research Unit, and published literature. A lifetime horizon was considered, with costs, QALYs, and LYs discounted at 3.5% per annum.
Results: The incremental cost–utility ratio (ICUR; per QALY gained) was £ 9901 for BGF versus GFF and £ 2164 for BGF versus BFF. The probability of treatments being cost-effective at the conventional UK-adopted willingness-to-pay threshold of ICUR <£ 20,000 was 85.1% for BGF, 14.3% for GFF, and 0.6% for BFF.
Conclusion: Based on ETHOS data, BGF was demonstrated to be cost-effective versus LAMA/LABA and ICS/LABA dual therapies at the conventional UK-adopted willingness-to-pay threshold (ICUR <£ 20,000). The main cost-effectiveness driver for BGF versus LAMA/LABA and ICS/LABA therapies was reduction in rate of exacerbations, which reduced costs and preserved quality of life.
Keywords: budesonide/glycopyrronium/formoterol fumarate dihydrate, chronic obstructive pulmonary disease, COPD, cost-effectiveness, Markov model, triple therapy
Plain Language Summary
Treatment costs for chronic obstructive pulmonary disease (COPD) are high. Many patients with COPD have times when their symptoms suddenly worsen, called exacerbations or flare-ups. These exacerbations make a patient’s day-to-day life difficult. They are also one of the main reasons why managing COPD is expensive.
To control their symptoms, patients may take one or more types of daily “maintenance” medicines. If patients keep having exacerbations, their doctor may suggest taking a combination of medicines that include an inhaled corticosteroid (ICS), a long-acting muscarinic antagonist (LAMA), and a long-acting β2-agonist (LABA).
In this cost-effectiveness analysis, we compared treatments to see which one gives the best value over the lifetime of patients with moderate-to-very severe COPD in terms of healthcare costs and improved quality of life. We looked at an inhaler that includes all three medicines (ICS, LAMA, and LABA), called budesonide/glycopyrronium/formoterol fumarate dihydrate or BGF. The treatments we compared BGF with included two of three medicines. One inhaler had a LAMA and a LABA and was called glycopyrronium/formoterol fumarate dihydrate or GFF. The other inhaler had an ICS and a LABA and was called budesonide/formoterol fumarate dihydrate or BFF. The analysis used data from a large clinical trial called ETHOS.
The total cost of BGF was more than that of GFF or BFF, but BGF was the most cost-effective over a patient’s lifetime. Mainly, this was because BGF is better than the other treatments at reducing how often patients experience COPD exacerbations, which reduces the associated healthcare costs and improves daily living.
Introduction
Chronic obstructive pulmonary disease (COPD) is a major contributor to morbidity and mortality worldwide,1,2 with mortality rates being substantially increased in patients with COPD compared with individuals of the same age without COPD.3 COPD is associated with a decline in lung function4 and is also characterized by periods of symptom exacerbations.5
COPD incurs a substantial economic burden,5,6 with higher costs observed as COPD severity increases7 and exacerbations being a major contributor to the estimated annual economic burden of COPD.8 In 2010, the projected cost of COPD in the United States was approximately $50 billion ($20 billion indirect costs; $30 billion direct costs),9 and in 2011, the cost of COPD in the European Union was over €48 billion (€25 billion indirect costs; €23 billion direct costs).10 The annual economic burden of COPD for the United Kingdom (UK) National Health Service (NHS) in 2014 was estimated to be £1.9 billion (£61 million indirect costs; £1.8 billion direct costs).6 The cost of managing COPD increases substantially with increasing frequency of exacerbations. In a retrospective cohort study in the UK, annual costs (2010‒2011) of managing COPD (excluding medications) were £1523, £2405, and £3396 for patients experiencing 0, 1, or ≥ 2 moderate-to-severe exacerbations, respectively.11 Therefore, reducing the risk and severity of exacerbations may be a key driver of the cost-effectiveness of COPD treatments.12
Triple therapy with an inhaled corticosteroid (ICS), a long-acting muscarinic antagonist (LAMA), and a long-acting β2-agonist (LABA) has demonstrated improvements in lung function, exacerbations, and patient-reported outcomes, and reductions in all-cause mortality, compared with LAMA/LABA and ICS/LABA dual therapies.5,13 Thus, in patients with COPD who have persistent COPD exacerbations despite dual therapy with a LAMA/LABA or ICS/LABA, treatment with ICS/LAMA/LABA triple therapy is recommended by the Global Initiative for Chronic Obstructive Lung Disease (GOLD).5 Guidelines from the UK National Institute for Health and Care Excellence (NICE) recommend ICS/LAMA/LABA triple therapy in patients receiving LAMA/LABA dual therapy who experience one severe or two moderate exacerbations within a year, and in patients receiving ICS/LABA dual therapy who have day-to-day symptoms that adversely impact quality of life (QoL), or have one severe or two moderate exacerbations within a year.14
To support reimbursement of triple therapy, there is a need to demonstrate value for money compared with dual therapies. Using data from the IMPACT study, ICS/LAMA/LABA triple therapy with fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI) was shown to be cost-effective versus ICS/LABA therapy with FF/VI in patients with symptomatic COPD and a history of exacerbations in the UK.15 In a separate analysis using data from the IMPACT study, FF/UMEC/VI was also demonstrated to be cost-effective versus LAMA/LABA therapy with UMEC/VI in the UK.16
The 52-week ETHOS study (NCT02465567) showed that triple therapy with a budesonide/glycopyrronium/formoterol fumarate dihydrate (BGF) metered-dose inhaler at two ICS dose levels (320/14.4/10 μg and 160/14.4/10 μg) reduced moderate or severe COPD exacerbations versus fixed-dose LAMA/LABA or ICS/LABA dual therapy in patients with moderate-to-very severe COPD and at least one exacerbation in the previous year.17 Triple therapy with BGF 320/14.4/10 μg is approved as maintenance treatment in patients with COPD in several regions and countries, including the United States, the European Union, the UK, China, Japan, Canada, and Australia.18–24
Here, we developed an economic model using ETHOS data to assess the long-term cost-effectiveness of single inhaler triple therapy with BGF 320/14.4/10 μg (the approved dose of BGF) versus LAMA/LABA and ICS/LABA dual therapies in the UK. The economic model was developed in accordance with guidance from health technology assessment agencies, including the Scottish Medicines Consortium and NICE.
Methods
Setting and Patient Population
ETHOS was a randomized, double-blind, parallel-group, Phase III study conducted in 26 countries. Full details of the ETHOS study design, including patient inclusion and exclusion criteria, have been previously published.17,25 Patients were aged 40−80 years with moderate-to-very severe COPD, were symptomatic, and had a prior history of moderate or severe COPD exacerbations. All patients were required to be taking ≥2 inhaled maintenance therapies for the management of their COPD for ≥6 weeks prior to screening. Patients were randomly assigned 1:1:1:1 to receive one of the following treatments, twice daily over 52 weeks, via a single metered-dose inhaler: BGF 320/14.4/10 μg, BGF 160/14.4/10 μg, the LAMA/LABA glycopyrronium/formoterol fumarate dihydrate 14.4/10 μg (GFF), or the ICS/LABA budesonide/formoterol fumarate dihydrate 320/10 μg (BFF).
This analysis used clinical data from the modified intent-to-treat population in the ETHOS study to extrapolate the long-term cost-effectiveness of BGF 320/14.4/10 μg (the approved dose of BGF) versus GFF and BFF. A third-party payer perspective (NHS Scotland) was adopted.
Model Structure and Clinical Parameters
A Markov model was developed that accounts for progression in disease severity (lung function decline), the occurrence of moderate and severe exacerbations, adverse events, and treatment discontinuation, based on data from ETHOS. The model consists of health states reflecting various stages that follow the natural progression of COPD (Figure 1). Health state-specific costs (ie, disease management and societal costs), treatment-related costs, and utilities were assigned to each health state.
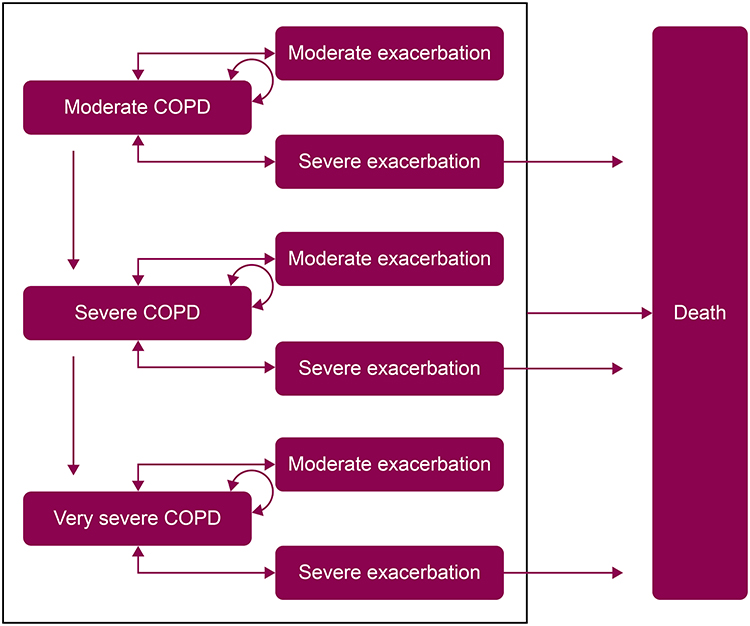 |
Figure 1 Health state transitions in the Markov model. Abbreviations: COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; GOLD, Global Initiative for Chronic Obstructive Lung Disease. Notes: COPD health states were defined by lung function, as determined by FEV1.5 Moderate COPD: FEV1 ≥50 to <80% predicted (based on GOLD 2). Severe COPD: FEV1 ≥30 to <50% predicted (based on GOLD 3). Very severe COPD: FEV1, <30% predicted (based on GOLD 4). |
Health states in the model were defined by lung function, as determined by forced expiratory volume in 1 second (FEV1): a moderate COPD health state was defined as FEV1 ≥50 to <80% predicted (based on GOLD 2); a severe COPD health state was defined as FEV1, ≥30 to <50% predicted (based on GOLD 3); and a very severe COPD health state was defined as FEV1, <30% predicted (based on GOLD 4).5 A patient cohort entered the model in the no exacerbation health states (moderate, severe, and very severe COPD) and was distributed across health states according to the ETHOS study population at baseline: moderate COPD, 28.5%; severe COPD, 60.6%; and very severe COPD, 10.9%. On entering the model, patients received treatment with BGF, GFF, or BFF. At each monthly cycle, patients were permitted to transition to a more severe COPD health state without experiencing an exacerbation; transition to a moderate or severe exacerbation health state; remain within the current COPD health state; or die. Moderate exacerbations were defined as those requiring use of systemic glucocorticoids, antibiotics, or both, for at least 3 days. Severe exacerbations were defined as those resulting in hospitalization or death. Exacerbation states were treated as discrete events that patients entered for one monthly cycle then exited, thus being at risk of further exacerbations in subsequent monthly cycles. Since COPD is considered a progressive disease, patients were not able to experience an improvement in lung function and transition back to a less severe COPD health state.
Outcomes and Treatment Comparisons
Quality-adjusted life-years (QALYs), LYs, exacerbations, and costs were extrapolated from the model and compared for BGF, GFF, and BFF as mean values per patient. The incremental cost–utility ratio (ICUR; [total cost for BGF – total cost for comparator] / [total QALYs for BGF – total QALYs for comparator]) was calculated for BGF versus GFF and BGF versus BFF. All output costs are presented in 2019 British pounds (£).
Data Sources
Clinical Efficacy
Clinical efficacy data were derived from ETHOS. Probabilities for transitions between health states are presented in Table 1. Based on ETHOS data, the monthly risk of discontinuation was 1.85% for BGF, 1.31% for GFF, and 1.16% for BFF.
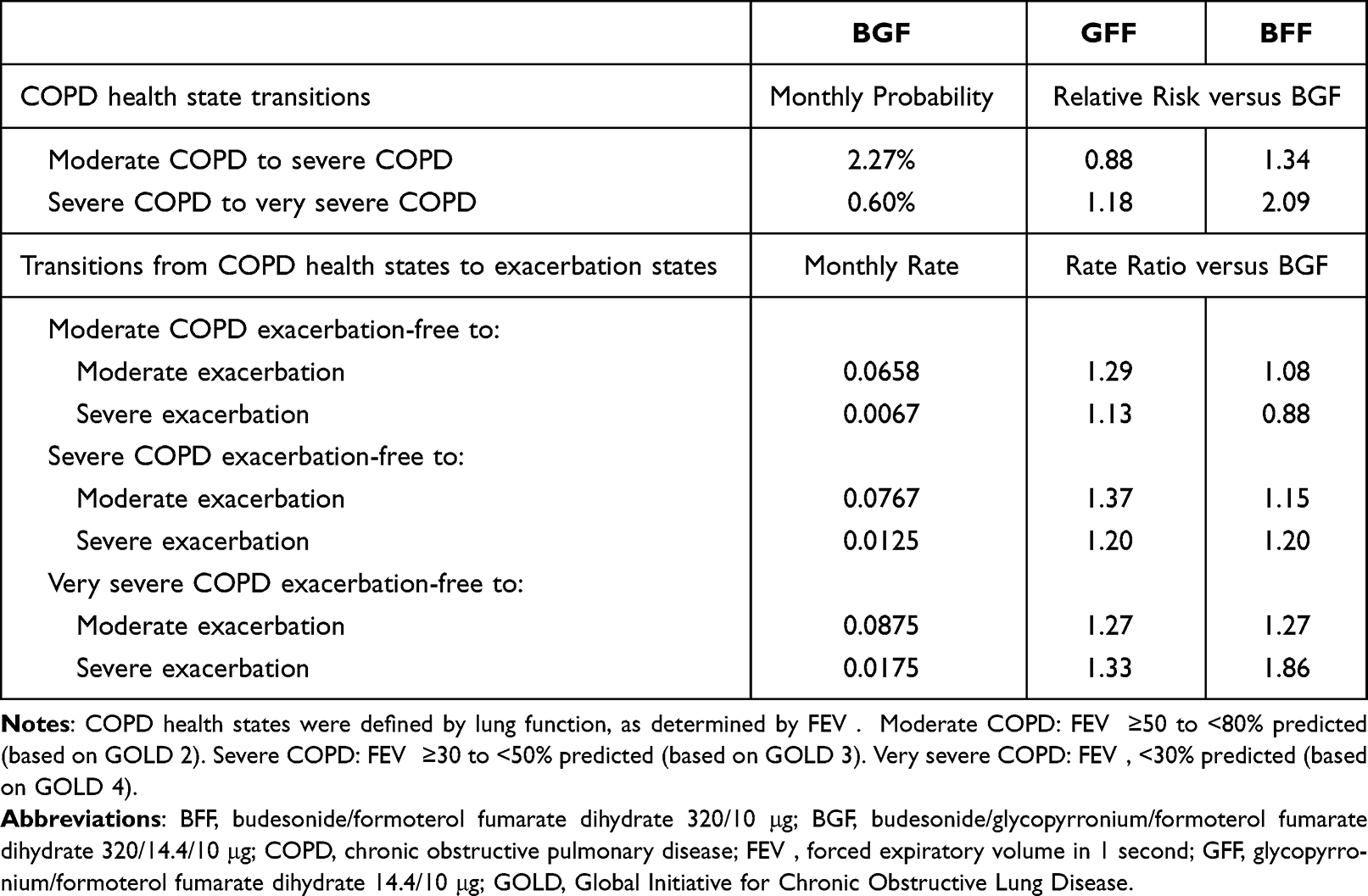 |
Table 1 Health State Transitions Based on ETHOS Data (Model Input) |
Mortality
Mortality data from the ETHOS study were used for the first 52 weeks of the analysis, with mortality probabilities applied across this period as constant monthly probabilities of 0.118% for BGF, 0.223% for GFF, and 0.158% for BFF. These values reflect the lower mortality rate seen in patients treated with BGF versus GFF and BFF during the 52-week ETHOS study. Thereafter, mortality was calculated based on health state occupancy, with general population mortality data from the literature adjusted to reflect the increased risk of mortality for patients with moderate, severe, and very severe COPD, respectively.
Relative risks of COPD-related mortality by COPD health states from the published literature26 were applied to all-cause mortality rates in the Scottish general population27 to derive overall mortality rates for UK patients with COPD by disease severity: moderate COPD, relative risk 1.40; severe and very severe COPD, relative risk 2.60.
Utilities
Utility values from the EuroQol 5-dimension 5-level (EQ-5D-5L) questionnaire and from St George’s Respiratory Questionnaire data mapped to the EQ-5D-5L were estimated from ETHOS data. Health state-related utilities were 0.79 for moderate COPD, 0.76 for severe COPD, and 0.72 for very severe COPD. Utility decrements due to exacerbations (0.010 for moderate exacerbations and 0.042 for severe exacerbations) were sourced from published literature.28 Disutilities due to adverse events were set to 0 to avoid double counting in the base case analysis; these disutilities were assumed to be captured in the underlying EQ-5D-5L analysis of the ETHOS data.
Healthcare Resource Utilization
Resource use per month for COPD management by COPD severity was derived from ETHOS data.
Costs
Disease management costs are presented in Table 2. Monthly disease management costs by COPD health state were derived from resource consumption using ETHOS data and costs from the UK NHS Schedule of Reference Costs (2017−2018),29 the Information Services Division (ISD) Scotland (2018−2019),30 Unit Costs of Health and Social Care from the Personal Social Services Research Unit (PSSRU; 2015 and 2018),31,32 and the British National Formulary (BNF; 2021).33 Unit costs of resources related to COPD health states are presented in Supplementary Table 1. Costs per exacerbation event were derived from resource consumption using ETHOS data, assumptions, and unit costs from the BNF (2021),33 the ISD Scotland (2018−2019),34 and Unit Costs of Health and Social Care from the PSSRU (2020).35 The distribution of healthcare resource utilization for moderate and severe exacerbations is presented in Supplementary Table 2.
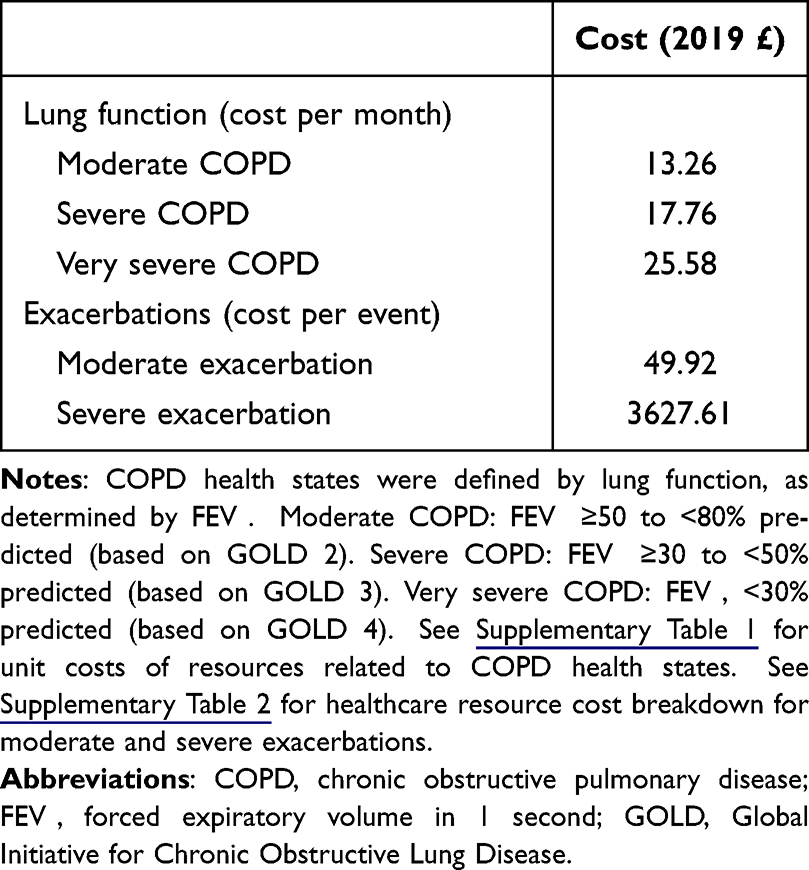 |
Table 2 Disease Management Costs Across All Treatments (Model Input) |
Treatment-related costs are presented in Table 3. Treatment acquisition costs were sourced from the BNF (2021).33 Subsequent treatment costs (treatment acquisition costs for patients who discontinued initial treatment) were derived from key external experts’ input and costs from the BNF (2021).33 Rescue medication costs were derived from resource consumption in ETHOS and costs from the BNF (2021) (Supplementary Table 3).33 Treatment-related adverse-event costs were derived from the UK NHS Schedule of Reference Costs (2017−2018).29
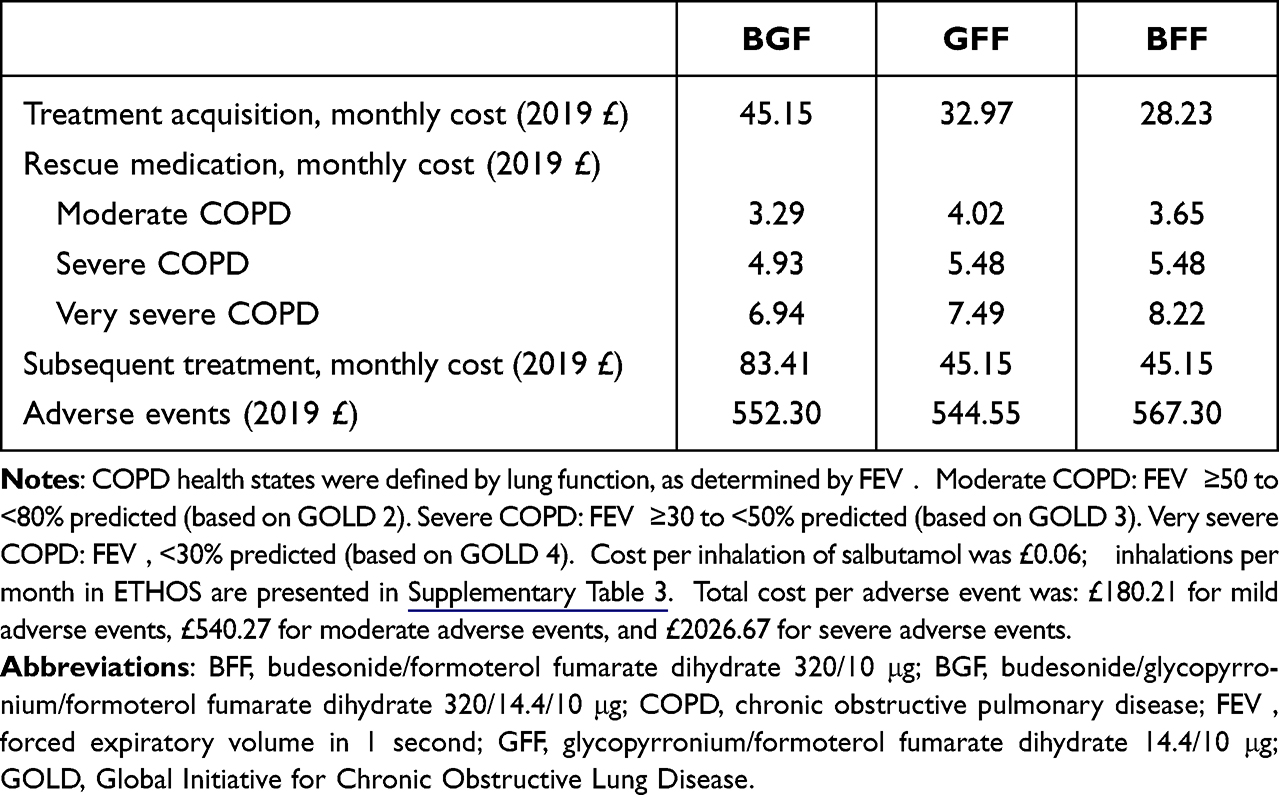 |
Table 3 Treatment-Related Costs (Model Input) |
All input costs are presented in 2019 British pounds (£).
Model Assumptions
Transition Probabilities
Patients were stratified into subgroups according to their COPD severity at ETHOS study baseline, and the proportion of patients whose lung function declined over the study duration was calculated. Similarly, moderate and severe exacerbation rates were analyzed over the course of the ETHOS study for the overall patient population stratified by COPD severity at study baseline. These 52-week probabilities were transformed to monthly probabilities. For exacerbation probabilities, exacerbations were considered separate events provided that ≥7 days elapsed between the recorded stop date of the earlier event and start date of the latter.
Adverse Events
The incidence of serious adverse events was very low in ETHOS, so only incidence and relative risks of mild, moderate, and severe adverse events were included in the model. The costs and disutilities associated with adverse events were ascribed at the beginning of the model when the entire cohort was at risk of treatment-related adverse events, to ensure that the full impact of adverse events was captured.
Treatment Discontinuation and Subsequent Treatment
After treatment discontinuation, patients were considered to have received subsequent treatment as described by key external experts and supported by GOLD recommendations. For patients initially treated with GFF or BFF, it was assumed that the subsequent treatment was BGF. Patients initially treated with BGF were assumed to receive subsequent treatment with BGF plus roflumilast.
Time Horizon and Discounting
The base case analysis considered a lifetime horizon, defined as a maximum of 30 years, however with most patients dying sooner considering the application of COPD mortality rates. Costs, QALYs, and LYs were discounted at 3.5% per annum.
Fully Incremental Analysis
Treatments were compared sequentially by ascending cost, with costs and QALYs for each treatment compared with those for the next non-dominated alternative in ranking.
Uncertainty
Model inputs and assumptions were subject to probabilistic sensitivity analyses (PSA) and deterministic sensitivity analyses (DSA). A PSA assessed the joint uncertainty surrounding each and all of the parameters in the model by assigning predetermined probabilistic distributions and randomly sampling input parameter values from these distributions (ie, a second-order Monte Carlo simulation). The choice of probabilistic distribution for each parameter was based on the nature of the data and its constraints, as well as recommendations from the literature.36 Distributions ascribed to parameters based on the PSA are presented in Supplementary Table 4. Where data to incorporate uncertainty around parameters were not available (eg, values elicited from expert opinion surveys), assumptions regarding the variance were made. Outcomes from the PSA are presented graphically in the form of a cost-effectiveness acceptability curve for all treatments.
A DSA tool assessed the impact of changing a parameter using a ±20% variation of the deterministic value to establish the impact on the results. Tornado diagrams for the ICUR were generated to visualize the results.
Results
Base Case Analysis
Costs, QALYs, and LYs were higher for BGF versus GFF and BFF, with BGF having an ICUR per QALY gained of £9901 versus GFF and £2164 versus BFF (Table 4). The main reduction in costs for BGF versus GFF, and BGF versus BFF, was associated with exacerbation-related costs (Table 5).
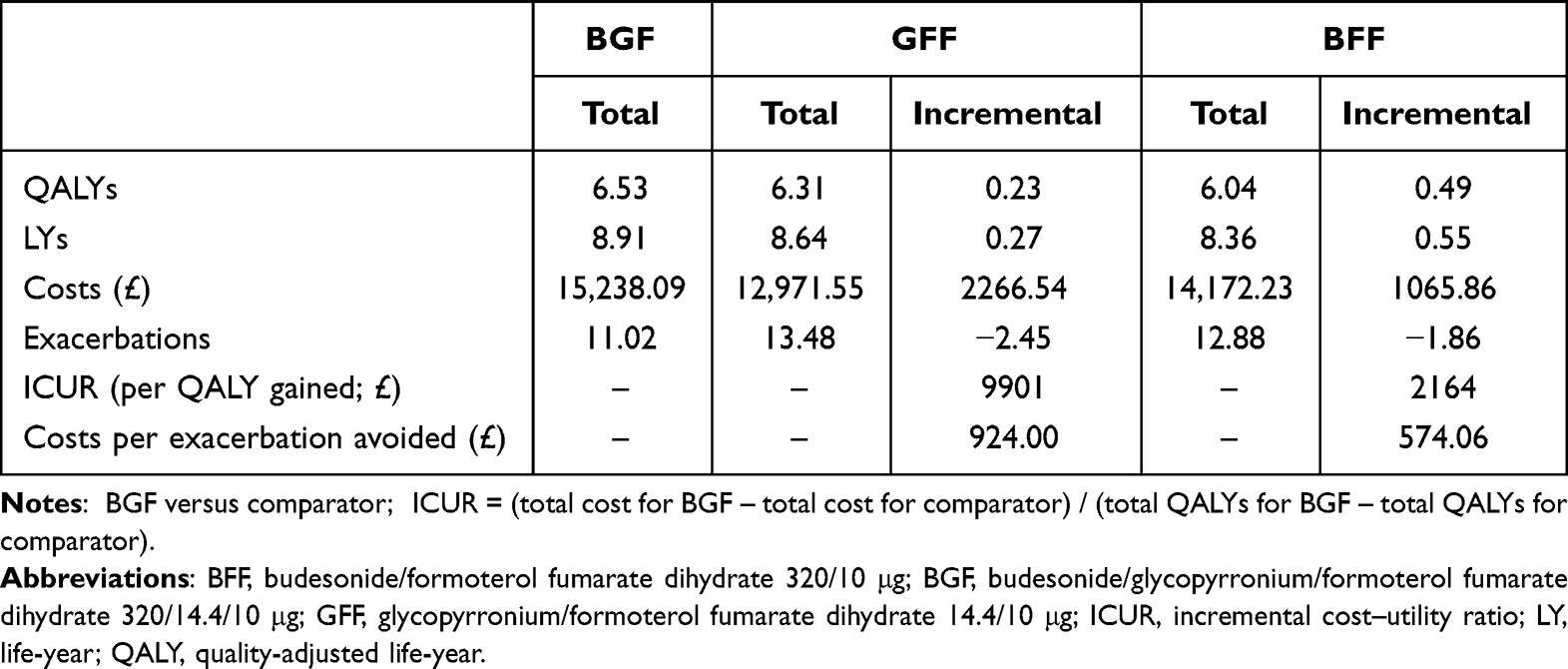 |
Table 4 Base Case Analysis (Model Output) |
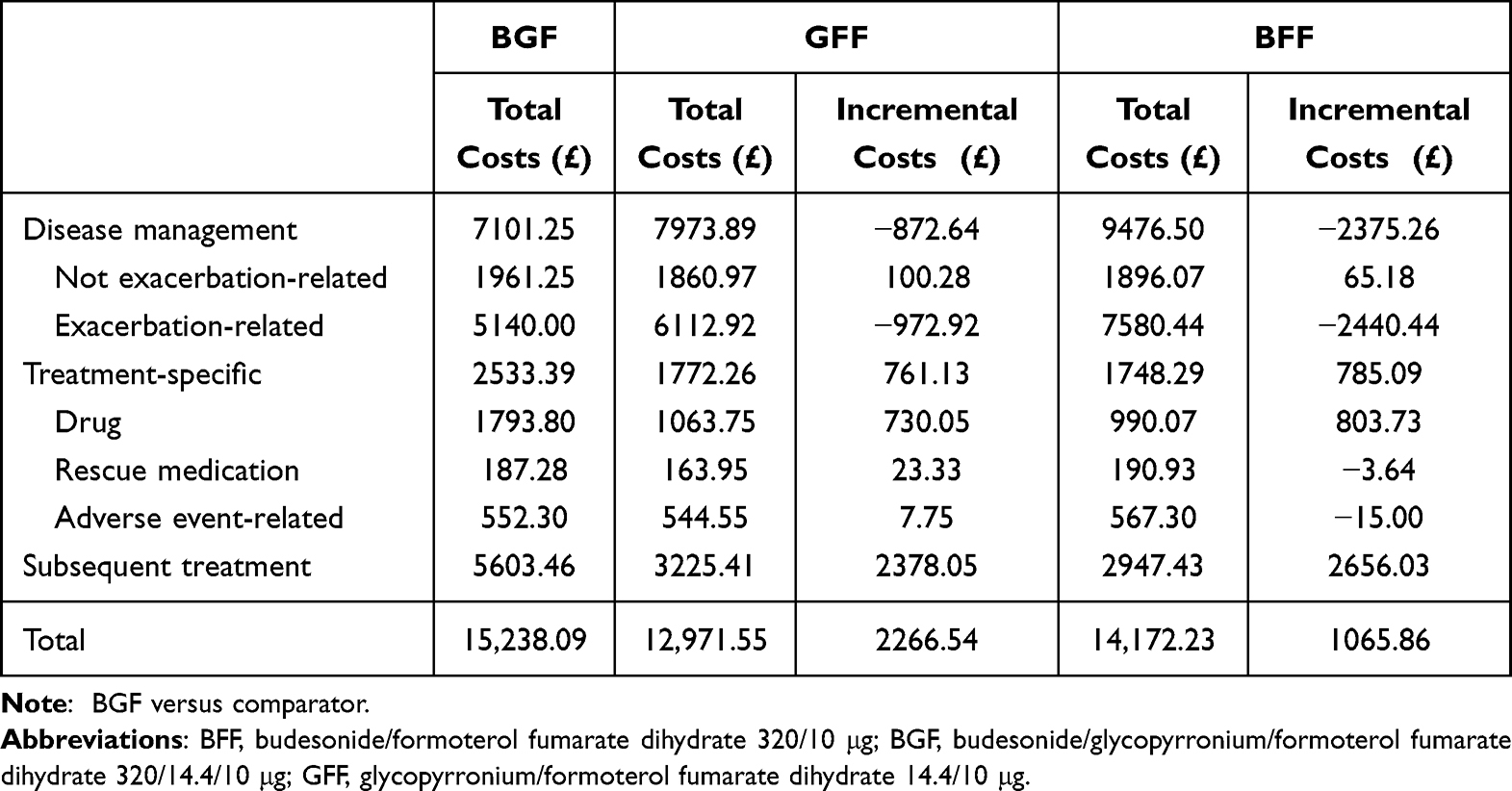 |
Table 5 Cost Breakdown for Base Case Analysis (Model Output) |
Fully Incremental Analysis
BFF was dominated by GFF in terms of higher costs and lower QALYs (Figure 2).
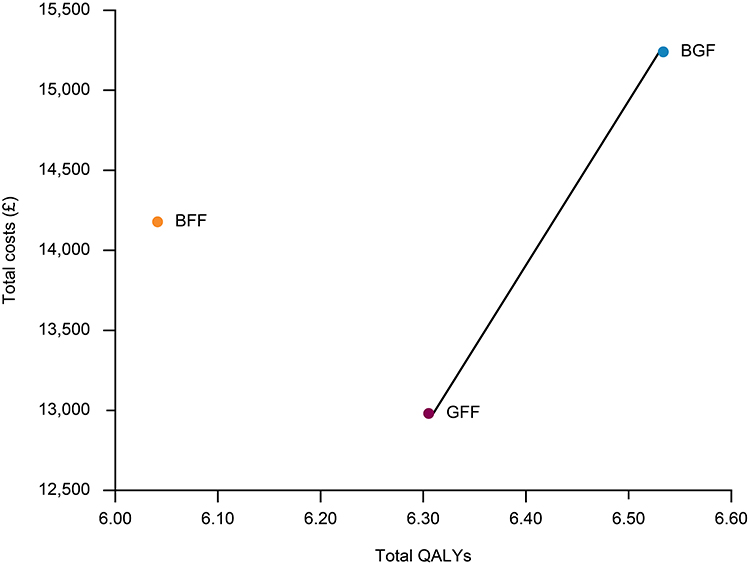 |
Figure 2 Cost-effectiveness frontier (fully incremental analysis; model output). Abbreviations: BFF, budesonide/formoterol fumarate dihydrate 320/10 μg; BGF, budesonide/glycopyrronium/formoterol fumarate dihydrate 320/14.4/10 μg; GFF, glycopyrronium/formoterol fumarate dihydrate 14.4/10 μg; QALY, quality-adjusted life-year. |
Probabilistic Sensitivity Analysis
The probability of each treatment being cost-effective at various ICUR willingness-to-pay thresholds is shown in Figure 3. At the conventional UK-adopted willingness-to-pay threshold of ICUR £20,000 per QALY gained,37 the probability of each treatment being cost-effective was 85.1% for BGF, 14.3% for GFF, and 0.6% for BFF. At a willingness-to-pay threshold of ICUR £30,000 per QALY gained, the probability of each treatment being cost-effective was 93.3% for BGF, 6.3% for GFF, and 0.4% for BFF.
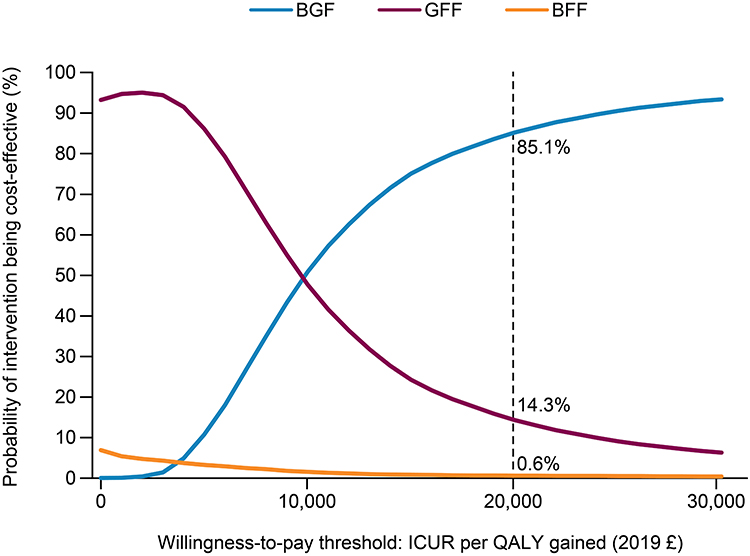 |
Figure 3 Cost-effectiveness acceptability curve (probabilistic sensitivity analysis; model output). Abbreviations: BFF, budesonide/formoterol fumarate dihydrate 320/10 μg; BGF, budesonide/glycopyrronium/formoterol fumarate dihydrate 320/14.4/10 μg; GFF, glycopyrronium/formoterol fumarate dihydrate 14.4/10 μg; ICUR, incremental cost–utility ratio; QALY, quality-adjusted life-year; UK, United Kingdom. Note: Dashed vertical line represents conventional UK-adopted willingness-to-paythreshold.37 |
Deterministic Sensitivity Analysis
For BGF versus GFF, the DSA showed that the frequency of exacerbations following BGF and GFF treatment discontinuation and the GFF risk of severe exacerbations were key drivers (most sensitive) of cost-effectiveness (Figure 4A), with changes in these variables resulting in the greatest changes in ICUR per QALY gained.
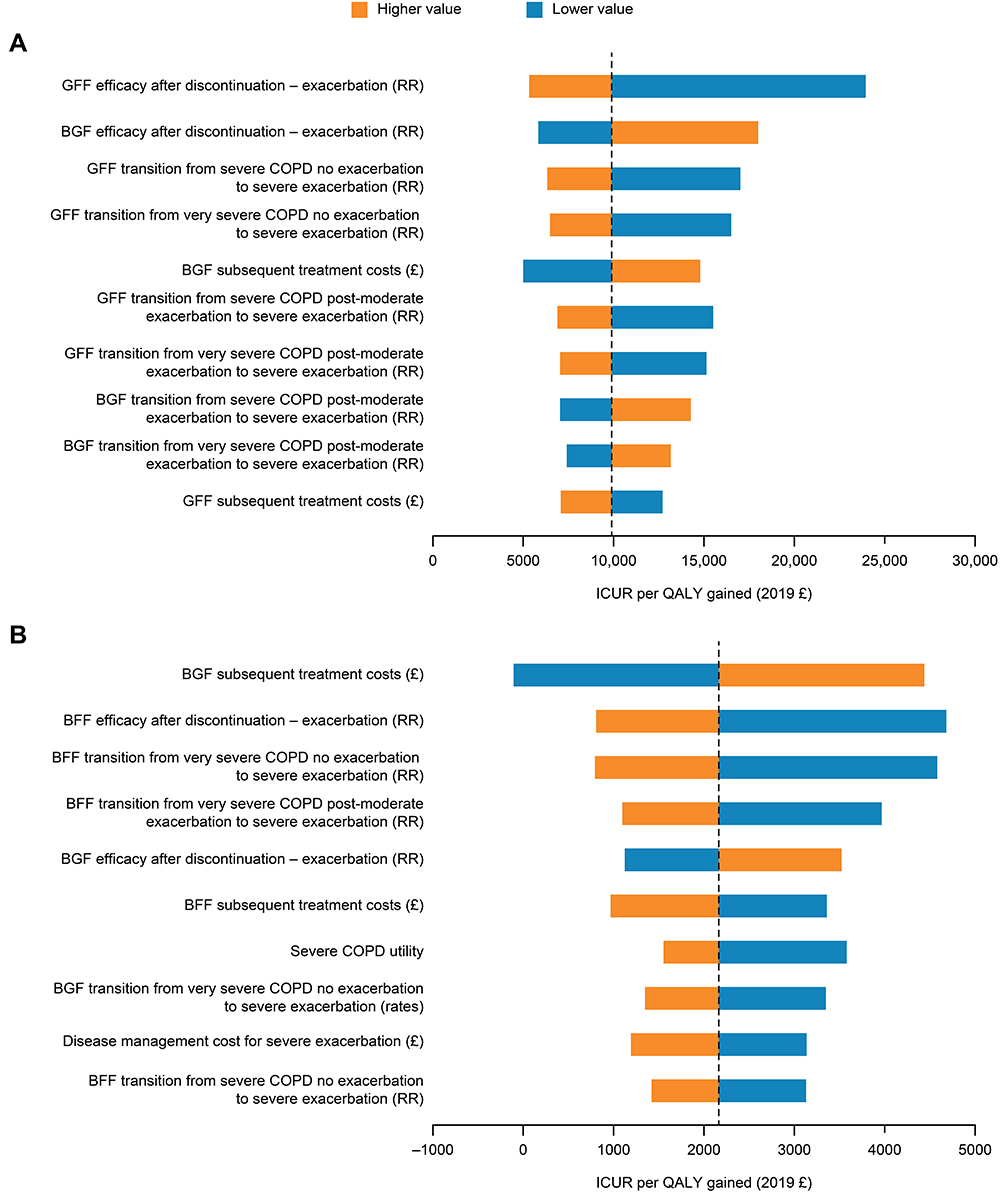 |
Figure 4 Tornado diagrams for ICUR with (A) BGF versus GFF and (B) BGF versus BFF (deterministic sensitivity analysis; model output). Abbreviations: BFF, budesonide/formoterol fumarate dihydrate 320/10 μg; BGF, budesonide/glycopyrronium/formoterol fumarate dihydrate 320/14.4/10 μg; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; GFF, glycopyrronium/formoterol fumarate dihydrate 14.4/10 μg; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICUR, incremental cost–utility ratio; QALY, quality-adjusted life-year; RR, rate ratio. Notes: COPD health states were defined by lung function, as determined by FEV1.5 Moderate COPD: FEV1 ≥50 to <80% predicted (based on GOLD 2). Severe COPD: FEV1 ≥30 to <50% predicted (based on GOLD 3). Very severe COPD: FEV1, <30% predicted (based on GOLD 4). The diagrams have been truncated to show the 10 parameters with the greatest impact on the results. The vertical dashed lines represent the ICUR per QALY gained in the base case analysis: (A) £9901 (BGF vs GFF) and (B) £2164 (BGF vs BFF). |
For BGF versus BFF, the DSA showed that BGF subsequent treatment costs, the frequency of exacerbations following BFF treatment discontinuation, and the BFF risk of severe exacerbations were key drivers (most sensitive) of cost-effectiveness (Figure 4B), with changes in these variables resulting in the greatest changes in ICUR per QALY gained.
Discussion
The aim of this analysis was to assess the cost-effectiveness of single inhaler triple therapy with BGF compared with LAMA/LABA (as measured using GFF) and ICS/LABA (as measured using BFF) dual therapies in patients with moderate-to-very severe COPD in the UK. The key finding was that BGF was cost-effective versus both LAMA/LABA and ICS/LABA dual therapy at the conventional UK-adopted willingness-to-pay threshold (ICUR <£20,000 per QALY gained) over a lifetime horizon from the UK healthcare payer perspective. BGF had an ICUR per QALY gained of £9901 and £2164 versus LAMA/LABA and ICS/LABA dual therapies, respectively. Reducing exacerbation rates has been previously reported to be a key driver of the cost-effectiveness of COPD treatments.12 Indeed, reduction in the rate of exacerbations was the main cost-effectiveness driver in the current analysis. With BGF versus LAMA/LABA and ICS/LABA therapies, exacerbation-related costs were reduced by £973 and £2440, respectively, and the reduction in exacerbations helped to preserve QoL.
Markov models have been widely used in the economic assessment of COPD treatment,15,16,38–44 and the overall strengths of this modeling approach merited its selection in the current analysis. The health state structure aims to capture stages in COPD progression that represent differences in healthcare costs and patient health-related QoL, and costs and health-related QoL decrements associated with moderate and severe exacerbations are captured.
The current cost-effectiveness analysis compared dual therapies with ICS/LAMA/LABA triple therapy (BGF) via a single metered-dose inhaler. “Open triple therapy” (OTT) involves combination treatment with an ICS/LABA and a LAMA in multiple inhalers.45 A cost-minimization analysis that compared the 1-year costs of BGF versus OTT in patients with moderate-to-very severe COPD in the UK has also been conducted.46 This cost-minimization analysis, which also utilized ETHOS data and a Markov model, estimated total 1-year costs of £1822 for BGF and £1961 for OTT, resulting in a cost saving with BGF of £139 per patient per year.46 With an estimated 222,000 UK patients receiving OTT in 2021, annual cost savings with BGF versus OTT were predicted to be approximately £30.9 million.46 Taken together, these complementary analyses demonstrate an economic benefit of BGF compared with both dual therapies and OTT.
Limitations of the current analysis include that it did not fully capture the link between exacerbations, symptoms, and lung function to the extent of a patient-level simulation model. Furthermore, the model did not capture exacerbation history and its impact on future exacerbation risk. The choice of employing a more complex model with patient-level data would have to be weighed against the availability of data (eg, risks of events) for patient-specific profiles and validated risk equations. Also, the increasing mortality risk associated with repeated exacerbations47–49 is not fully captured by the current model structure. In addition, the analysis was based on the ETHOS study population of patients with moderate-to-very severe COPD who were symptomatic and had a prior history of moderate or severe COPD exacerbations. Therefore, the findings may not be generalizable to the general population of patients with COPD, including those with less severe disease who are well controlled on their current therapy. We also recognize that assumptions in the model, for example regarding treatment escalation, may vary depending on local guidelines. Lastly, although the model considered a lifetime horizon, the duration of the ETHOS study was 52 weeks. The model assumed that treatment efficacy did not decrease over time, but more long-term data on the efficacy of triple therapy beyond 52 weeks are needed.
Conclusions
Using data from the ETHOS study, single inhaler triple therapy with BGF was found to be cost-effective versus LAMA/LABA and ICS/LABA dual therapy at the conventional UK-adopted willingness-to-pay threshold (ICUR <£20,000 per QALY gained) using a Markov model. The main cost-effectiveness driver was the reduced exacerbation rate, which lowered costs and preserved QoL for BGF versus LAMA/LABA and ICS/LABA therapies. Ultimately, it will be important to observe the long-term efficacy of BGF in clinical practice to validate the findings of this model.
Abbreviations
BFF, budesonide/formoterol fumarate dihydrate; BGF, budesonide/glycopyrronium/formoterol fumarate dihydrate; BNF, British National Formulary; COPD, chronic obstructive pulmonary disease; DSA, deterministic sensitivity analyses; EQ-5D-5L, EuroQol 5-dimension 5-level; FEV1, forced expiratory volume in 1 second; FF/UMEC/VI, fluticasone furoate/umeclidinium/vilanterol; FF/VI, fluticasone furoate/vilanterol; GFF, glycopyrronium/formoterol fumarate dihydrate; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroid; ICUR, incremental cost–utility ratio; ISD, Information Services Division; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; LY, life-year; NHS, National Health Service; NICE, National Institute for Health and Care Excellence; OTT, open triple therapy; PSA, probabilistic sensitivity analyses; PSSRU, Personal Social Services Research Unit; QALY, quality-adjusted life-year; QoL, quality of life; RR, rate ratio; UK, United Kingdom; UMEC/VI, umeclidinium/vilanterol.
Ethics Approval and Informed Consent
For the ETHOS study, the protocol and informed consent form were approved by the appropriate Institutional Review Board, independent ethics committee, or health authority (Supplementary Table 5); written informed consent was obtained from all patients before screening.
Data Sharing Statement
Data underlying the findings described in this manuscript may be obtained in accordance with AstraZeneca’s data-sharing policy described at https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure.
Acknowledgments
Portions of the data reported in this manuscript have been previously presented at the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Europe Conference 2021: de Nigris E et al. Cost-effectiveness of triple therapy with budesonide/glycopyrronium/formoterol fumarate versus dual therapies in moderate-to-very severe COPD: United Kingdom analysis using the ETHOS study. Value Health. 2022;25 (Suppl 1):S46. The authors thank Martin Jenkins for his contributions to the study and to the development of the ISPOR EU abstract and poster, and Danny Gibson for his technical support in validating the model. The authors also thank Colin Bonner, Linda Stotsky, Mario Marinazzo, and Philomena Britto for their review of the plain language summary as people living with COPD. Medical writing support, under the direction of the authors, was provided by Sarah Piggott, MChem, CMC Connect, a division of IPG Health Medical Communications, funded by AstraZeneca, in accordance with Good Publication Practice (GPP 2022) guidelines.50
Author Contributions
All authors made a significant contribution to the work reported. Enrico de Nigris and Ulf Holmgren contributed to study conception or design, data acquisition, data analysis, and data interpretation. Catrin Treharne and Nick Brighton contributed to study conception or design, data analysis, and data interpretation. Andrew Walker and John Haughney contributed to study conception or design, and data interpretation. All authors took part in drafting, revising, or critically reviewing the article, gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
Both the ETHOS study and the current analyses were sponsored by AstraZeneca. The study sponsor was involved in the design and conduct of the study, in the data analysis and interpretation, and in the review of the manuscript for accuracy. Decisions on final content were made by the authors. Medical writing support for development of this manuscript was funded by AstraZeneca.
Disclosure
Enrico de Nigris is a former employee of AstraZeneca and previously held stock and/or stock options in the company. Catrin Treharne and Nick Brighton are former employees of Parexel International. Ulf Holmgren is an employee of AstraZeneca and holds stock and/or stock options in the company. Andrew Walker is the Director of Salus Alba, was funded for this work by AstraZeneca, and has earned consultancy income in the last 3 years from AbbVie, Aesara, Akcea, Albireo, Alexion, Allergan, Almirall, Amarin, Arena, Apsara, Astellas, AstraZeneca, Autolus, Avexis, Bayer, BioCryst, Biogen, BioMarin, Bristol-Myers Squibb, Boehringer Ingelheim, Calico, Celgene, Chiesi, Daiichi-Sankyo, Deciphera, Diurnal, Eisai, Eli Lilly, Ferring, Galapagos, Gedeon Richter, Gilead, GlaxoSmithKline, GW Pharma, Intercept, Idorsia, Incyte, Ionis, Ipsen, Janssen, Jazz, Jcyte, Kite, LEK, LEO, Les Laboratoires Servier, Lundbeck, Merck Serono, Miltenyi, Mundi Biopharma, Mylan, Myovant, Norgine, Novartis, Novo Nordisk, Orchard, Paion, Pfizer, Pierre Fabre, PTC, RegenXBio, Rhythm, Sarepta, Sanofi, Santen, Seagen, Shionogi, Sigmatec, SOBI, Takeda, Tanaya, UCB, and Vertex. John Haughney has received personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, Circassia, and Teva, unrelated to the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. World Health Organization. Global health estimates: life expectancy and leading causes of death and disability; 2020. Available from: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates.
2. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1789–1858. doi:10.1016/S0140-6736(18)32279-7
3. Afonso ASM, Verhamme KMC, Sturkenboom MC, Brusselle GG. COPD in the general population: prevalence, incidence and survival. Respir Med. 2011;105(12):1872–1884. doi:10.1016/j.rmed.2011.06.012
4. Tantucci C, Modina D. Lung function decline in COPD. Int J Chron Obstruct Pulmon Dis. 2012;7:95–99. doi:10.2147/COPD.S27480
5. Global Initiative for Chronic Obstructive Lung Disease. 2022 GOLD Report. Global strategy for the diagnosis, management and prevention of COPD. 2022. Available from: https://goldcopd.org/2022-gold-reports-2/.
6. Trueman D, Woodcock F, Hancock E. Estimating the economic burden of respiratory illness in the UK; 2017. Available from: https://cdn.shopify.com/s/files/1/0221/4446/files/PC-1601_-_Economic_burden_report_FINAL_8cdaba2a-589a-4a49-bd14-f45d66167795.pdf?1309501094450848169&_ga=2.11091697.435115983.1642422068-1593090845.1642422068.
7. Hilleman DE, Dewan N, Malesker M, Friedman M. Pharmacoeconomic evaluation of COPD. Chest. 2000;118(5):1278–1285. doi:10.1378/chest.118.5.1278
8. Celli BR, MacNee W, Agusti A; ATS/ERS Task Force. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932–946. doi:10.1183/09031936.04.00014304
9. Guarascio AJ, Ray SM, Finch CK, Self TH. The clinical and economic burden of chronic obstructive pulmonary disease in the USA. Clinicoecon Outcomes Res. 2013;5:235–245. doi:10.2147/CEOR.S34321
10. European Respiratory Society. European lung white book; 2013. Available from: https://www.erswhitebook.org/.
11. Punekar YS, Shukla A, Müllerova H. COPD management costs according to the frequency of COPD exacerbations in UK primary care. Int J Chron Obstruct Pulmon Dis. 2014;9(1):65–73. doi:10.2147/COPD.S54417
12. Mapel DW, Schum M, Lydick E, Marton JP. A new method for examining the cost savings of reducing COPD exacerbations. Pharmacoeconomics. 2010;28(9):733–749. doi:10.2165/11535600-000000000-00000
13. Long H, Xu H, Janssens JP, Guo Y. Single-inhaler triple vs single-inhaler dual therapy in patients with chronic obstructive pulmonary disease: a meta-analysis of randomized control trials. Respir Res. 2021;22(1):209. doi:10.1186/s12931-021-01794-w
14. National Institute for Health and Care Excellence. Visual summary: treatment algorithm; 2019. Available from: https://www.nice.org.uk/guidance/ng115/resources/visual-summary-treatment-algorithm-pdf-6604261741.
15. Martin A, Shah D, Schroeder M, et al. Informing the pathway of COPD treatment (the IMPACT study): single inhaler triple therapy (FF/UMEC/VI) versus FF/VI in patients with COPD – cost-effectiveness in the UK. Thorax. 2018;73(Suppl 4):P250.
16. Anley G, Shah D, Schroeder M, et al. Informing the pathway of COPD treatment (the IMPACT study): single inhaler triple therapy (FF/UMEC/VI) versus dual bronchodilator therapy (UMEC/VI) in patients with COPD – cost-effectiveness in the UK. Thorax. 2018;73(Suppl 4):P249.
17. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N Engl J Med. 2020;383(1):35–48. doi:10.1056/NEJMoa1916046
18. Specialist Pharmacy Service. Budesonide + formoterol + glycopyrronium. Available from: https://www.sps.nhs.uk/medicines/budesonide-formoterol-glycopyrronium/.
19. European Medicines Agency. Trixeo Aerosphere. Summary of product characteristics; 2021. Available from: https://www.ema.europa.eu/en/documents/product-information/trixeo-aerosphere-epar-product-information_en.pdf.
20. US Food and Drug Administration. Breztri Aerosphere™: highlights of prescribing information; 2020. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/212122s000lbl.pdf.
21. AstraZeneca. Breztri Aerosphere (PT010) approved in Japan for patients with chronic obstructive pulmonary disease; 2019. Available from: https://www.astrazeneca.com/media-centre/press-releases/2019/breztri-aerosphere-pt010-approved-in-japan-for-patients-with-chronic-obstructive-pulmonary-disease-19062019.html.
22. AstraZeneca. AstraZeneca’s triple-combination therapy approved in China for patients with COPD; 2019. Available from: https://www.astrazeneca.com/media-centre/press-releases/2019/astrazenecas-triple-combination-therapy-approved-in-china-for-patients-with-copd-23122019.html.
23. Canadian Agency for Drugs and Technologies in Health. Reimbursement reviews. Budesonide/glycopyrronium/formoterol fumarate; 2021. Available from: https://www.cadth.ca/budesonide-glycopyrronium-formoterol-fumarate.
24. Australian Government Department of Health Therapeutic Goods Administration. Australian product information. Breztri Aerosphere™ 160/7.2/5 (budesonide/glyopyrronium/formoterol (eformoterol) fumarate dihydrate) pressurised metered dose inhaler; 2021. Available from: http://www.guildlink.com.au/gc/ws/astra/pi.cfm?product=appbrezt10721.
25. Rabe KF, Martinez FJ, Ferguson GT, et al. A Phase III study of triple therapy with budesonide/glycopyrrolate/formoterol fumarate metered dose inhaler 320/18/9.6 μg and 160/18/9.6 μg using co-suspension delivery technology in moderate-to-very severe COPD: the ETHOS study protocol. Respir Med. 2019;158:59–66. doi:10.1016/j.rmed.2019.08.010
26. Shavelle RM, Paculdo DR, Kush SJ, Mannino DM, Strauss DJ. Life expectancy and years of life lost in chronic obstructive pulmonary disease: findings from the NHANES III follow-up study. Int J Chron Obstruct Pulmon Dis. 2009;4:137–148. doi:10.2147/COPD.S5237
27. Office for National Statistics. National life tables, Scotland: 2016 to 2018; 2019. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/lifeexpectancies/datasets/nationallifetablesscotlandreferencetables.
28. Rutten-van Mölken MP, Hoogendoorn M, Lamers LM. Holistic preferences for 1-year health profiles describing fluctuations in health: the case of chronic obstructive pulmonary disease. Pharmacoeconomics. 2009;27(6):465–477. doi:10.2165/00019053-200927060-00003
29. UK National Health Service. Reference cost collection: national schedule of reference costs, 2017/18 - NHS trusts and NHS foundation trusts; 2019. Available from: https://webarchive.nationalarchives.gov.uk/ukgwa/20200501111106/https://improvement.nhs.uk/resources/reference-costs/.
30. Information Services Division Scotland. National statistics release - outpatients - specialty costs and activity - nurse led clinics, by specialty, by hospital; 2019. Available from: https://www.isdscotland.org/health-topics/finance/costs/Detailed-Tables/Speciality-Costs/Outpatients.asp.
31. Personal Social Services Research Unit. Unit costs of health and social care 2015; 2015. Available from: https://www.pssru.ac.uk/project-pages/unit-costs/unit-costs-2015/.
32. Personal Social Services Research Unit. Unit costs of health and social care 2018; 2018. Available from: https://www.pssru.ac.uk/project-pages/unit-costs/unit-costs-2018/.
33. National Institute for Health and Care Excellence. British national formulary. Available from: https://bnf.nice.org.uk/.
34. Information Services Division Scotland. National statistics release - acute medical - specialty costs and activity - inpatients in all specialties (exc long stay), by hospital; 2019. Available from: https://www.isdscotland.org/Health-Topics/Finance/Costs/Detailed-Tables/Speciality-Costs/Acute-Medical.asp.
35. Personal Social Services Research Unit. Unit costs of health and social care 2020; 2020. Available from: https://www.pssru.ac.uk/project-pages/unit-costs/unit-costs-2020/.
36. Briggs AH, Baker T, Risebrough NA, et al. Development of the Galaxy chronic obstructive pulmonary disease (COPD) model using data from ECLIPSE: internal validation of a linked-equations cohort model. Med Decis Making. 2017;37(4):469–480. doi:10.1177/0272989X16653118
37. National Institute for Health and Care Excellence. The guidelines manual. Process and methods [PMG6]. 7 Assessing cost effectiveness; 2012. Available from: https://www.nice.org.uk/process/pmg6/chapter/assessing-cost-effectiveness.
38. Fenwick E, Martin A, Schroeder M, et al. Cost-effectiveness analysis of a single-inhaler triple therapy for COPD in the UK. ERJ Open Res. 2021;7(1):480. doi:10.1183/23120541.00480-2020
39. Wilson MR, Patel JG, Coleman A, McDade CL, Stanford RH, Earnshaw SR. Cost-effectiveness analysis of umeclidinium/vilanterol for the management of patients with moderate to very severe COPD using an economic model. Int J Chron Obstruct Pulmon Dis. 2017;12:997–1008. doi:10.2147/COPD.S124420
40. van Boven JF, Kocks JW, Postma MJ. Cost-effectiveness and budget impact of the fixed-dose dual bronchodilator combination tiotropium-olodaterol for patients with COPD in the Netherlands. Int J Chron Obstruct Pulmon Dis. 2016;11:2191–2201. doi:10.2147/COPD.S114738
41. Negro RD, Eandi M, Pradelli L, Iannazzo S. Cost-effectiveness and healthcare budget impact in Italy of inhaled corticosteroids and bronchodilators for severe and very severe COPD patients. Int J Chron Obstruct Pulmon Dis. 2007;2(2):169–176.
42. Hertel N, Kotchie RW, Samyshkin Y, Radford M, Humphreys S, Jameson K. Cost-effectiveness of available treatment options for patients suffering from severe COPD in the UK: a fully incremental analysis. Int J Chron Obstruct Pulmon Dis. 2012;7:183–199. doi:10.2147/COPD.S29820
43. National Institute for Health and Care Excellence. Roflumilast for treating chronic obstructive pulmonary disease. Technology appraisal guidance [ID984]; 2016. Available from: https://www.nice.org.uk/guidance/ta461.
44. Hoogendoorn M, Rutten-van Mölken MP, Hoogenveen RT, Al MJ, Feenstra TL. Developing and applying a stochastic dynamic population model for chronic obstructive pulmonary disease. Value Health. 2011;14(8):1039–1047. doi:10.1016/j.jval.2011.06.008
45. Huang WC, Chen CY, Liao WC, et al. A real world study to assess the effectiveness of switching to once daily closed triple therapy from mono/dual combination or open triple therapy in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2021;16:1555–1568. doi:10.2147/COPD.S308911
46. de Nigris E, Holmgren U, Treharne C, Brighton N, Walker A, Haughney J. Cost minimization analysis of fixed-dose triple therapy with budesonide/glycopyrronium/formoterol fumarate versus open triple therapy for moderate-to-very severe COPD in the United Kingdom. Value Health. 2022;25(Suppl 1):POSA68.
47. Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. doi:10.1136/thx.2005.040527
48. Rothnie KJ, Müllerová H, Smeeth L, Quint JK. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice-based population with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(4):464–471. doi:10.1164/rccm.201710-2029OC
49. Suissa S, Dell’Aniello S, Ernst P. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67(11):957–963. doi:10.1136/thoraxjnl-2011-201518
50. DeTora LM, Toroser D, Sykes A, et al. Good publication practice (GPP) guidelines for company-sponsored biomedical research: 2022 Update. Ann Intern Med. 2022;175(9):1298–1304. doi:10.7326/M22-1460
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cost-Effectiveness Analysis of the TCM “Yupingfeng Granules” in the Treatment of Acute Exacerbations of COPD Based on a Randomized Clinical Trial
Hu M, Ding P, Ma J, Yang N, Zheng J, Zhou N
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2369-2379
Published Date: 23 September 2022
Cost-Effectiveness of Cardioverter-Defibrillator Implantation in Kazakhstan
Begisbayev T, Kosherbayeva L, Gaitova K, Brimzhanova M
Vascular Health and Risk Management 2022, 18:813-821
Published Date: 18 October 2022
Cost-Effectiveness of Single- versus Multiple-Inhaler Triple Therapy in a UK COPD Population: The INTREPID Trial
Halpin DM, Kendall R, Shukla S, Martin A, Shah D, Midwinter D, Beeh KM, Kocks JWH, Jones PW, Compton C, Risebrough NA, Ismaila AS
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2745-2755
Published Date: 25 October 2022