")
Back to Journals » Vascular Health and Risk Management » Volume 18
Cost-Effectiveness of Cardioverter-Defibrillator Implantation in Kazakhstan
Authors Begisbayev T, Kosherbayeva L , Gaitova K, Brimzhanova M
Received 10 April 2022
Accepted for publication 5 October 2022
Published 18 October 2022 Volume 2022:18 Pages 813—821
DOI https://doi.org/10.2147/VHRM.S369953
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mirna N Chahine
Temirkhan Begisbayev,1 Lyazzat Kosherbayeva,2,3 Kamilla Gaitova,4 Marzhan Brimzhanova1
1Kazakhstans Medical University “KSPH”, Almaty, Kazakhstan; 2Asfendiyarov Kazakh National Medical University, Almaty, Kazakhstan; 3Al-Farabi Kazakh National University, Almaty, Kazakhstan; 4Health Technology Assessment Department, Republican Center for Health Development, Nur-Sultan, Kazakhstan
Correspondence: Lyazzat Kosherbayeva, Asfendiyarov Kazakh National Medical University, 88 Tole bi Street, Almaty, Kazakhstan, Tel + 7 705 120 46 52, Email [email protected]; [email protected]
Abstract: Cardiovascular disease is the leading cause of morbidity and mortality worldwide. The implementation of effective technologies such as Implantable cardioverter-defibrillator (ICD) for patients at risk of sudden cardiac death requires additional health system resources.
Objective: To assess the economic effectiveness of ICD in comparison with conservative tactics for preventing life-threatening rhythm disturbances in Kazakhstan.
Methods: A Markov model was built with a time horizon of 35 years. Mortality and utility data were obtained from the available literature. The economic parameters of the model are based on the approved tariffs for medical services in Kazakhstan and clinical protocols. Following WHO recommendations, a willingness to pay threshold of three times gross domestic product per capita was used to assess cost-effectiveness. A discount rate of 3.5% was applied to both costs and benefits. To deal with parameter uncertainties and to provide robust analysis, a probabilistic sensitivity analysis was performed, randomly varying all inputs subject to uncertainty assuming a statistical distribution.
Results: The total costs in the primary prevention (PP) group by ICD implantation and in the control group were 8,903,786 tenges and 3,194,414 tenges, respectively. The discounted total quality-adjusted life-years saved (QALYs) in the ICD and control groups were 6.48 and 4.98, respectively. The indicator of incremental cost-effectiveness ratio amounted to3791604 tenge, which is below the willingness to pay threshold and indicates the cost-effectiveness of using ICD as a PP strategy in patients with sudden cardiac death risk factors in the health care of Kazakhstan.
Conclusion: The ICD for the primary prevention of the development of life-threatening rhythm disturbances and sudden cardiac death is a cost-effective health technology from the position of a payer in the health care system of Kazakhstan.
Keywords: cardioverter-defibrillator implantation, cost-effectiveness, Markov model, reimbursement of ICD in Kazakhstan
Introduction
Implantable cardioverter-defibrillator (ICD) is an effective method of preventing sudden cardiac death (SCD) in patients with mild symptoms of heart failure and decreased systolic function, which has been confirmed by numerous randomized clinical trials.1–3 The method is recommended by clinical guidelines,4,5 and cost-effectiveness has been proven in various health care systems.6–8
Despite compelling evidence, we can observe a disparity between indications for and underutilization of ICD worldwide, partly due to the high cost of the device and lack of reimbursement.9,10 In Kazakhstan the population reimbursed from a guaranteed package of free health services (SGBP) that is funded by the government budget and other forms of health care covered by a mandatory social health insurance system (MSHI). The procedure for implantation of a cardioverter-defibrillator is reimbursed within the framework of the MSHI and the SGBP. However, this procedure uses in Kazakhstan about 44 devices per year per 1 million inhabitants, although it should be noted that before the COVID-19 pandemic, there was an increase in the number of implantations per year. Thus, in 2019, 806 implantations of cardioverter-defibrillators were carried out against 719 in 2017, while in 2020 only 687 procedures were performed. By comparison, the total number of registered implants in Spain in 2019 was 14.9 per million inhabitants, which is generally much lower than the average ICD use in Europe,11 while in South Korea the rate of new implants in 2016 was 1.9 per 100000 populations.12
While the cost-effectiveness of ICD for the primary prevention of sudden cardiac arrest has been well proved in other countries,7,13 there were no studies conducted in Kazakhstan before. The aim of this study was to assess the cost-effectiveness of ICD therapy as primary prevention in patients with heart failure from the position of a payer in the health care system of Kazakhstan.
Methods
A Markov decision-making model was built to assess costs, impact on quality of life, survival rates, and an incremental indicator of the cost-effectiveness of ICD versus no ICD in a population of Kazakhstani patients at risk of SCD.
The simulations were based on previously published research data and did not suggest additional human studies. A group of patients without the use of an ICD was selected as a control group. Conservative drug use was not considered for comparison behavior, as the SCD-HeFT14 study showed no significant difference between amiodarone and placebo treatment in preventing death in patients at risk of developing life-threatening heart rhythm disturbances. The input parameters of the model are shown in Table 1 and are detailed below. The model was built using Microsoft Excel. Discount rates have not yet been determined in Kazakhstan. Since a number of directions in healthcare were previously adapted from United Kingdom (UK)15,16 for our study discount rate of 3.5% was applied to both costs and benefits based on the National Institute for Health and Care Excellence (UK).17
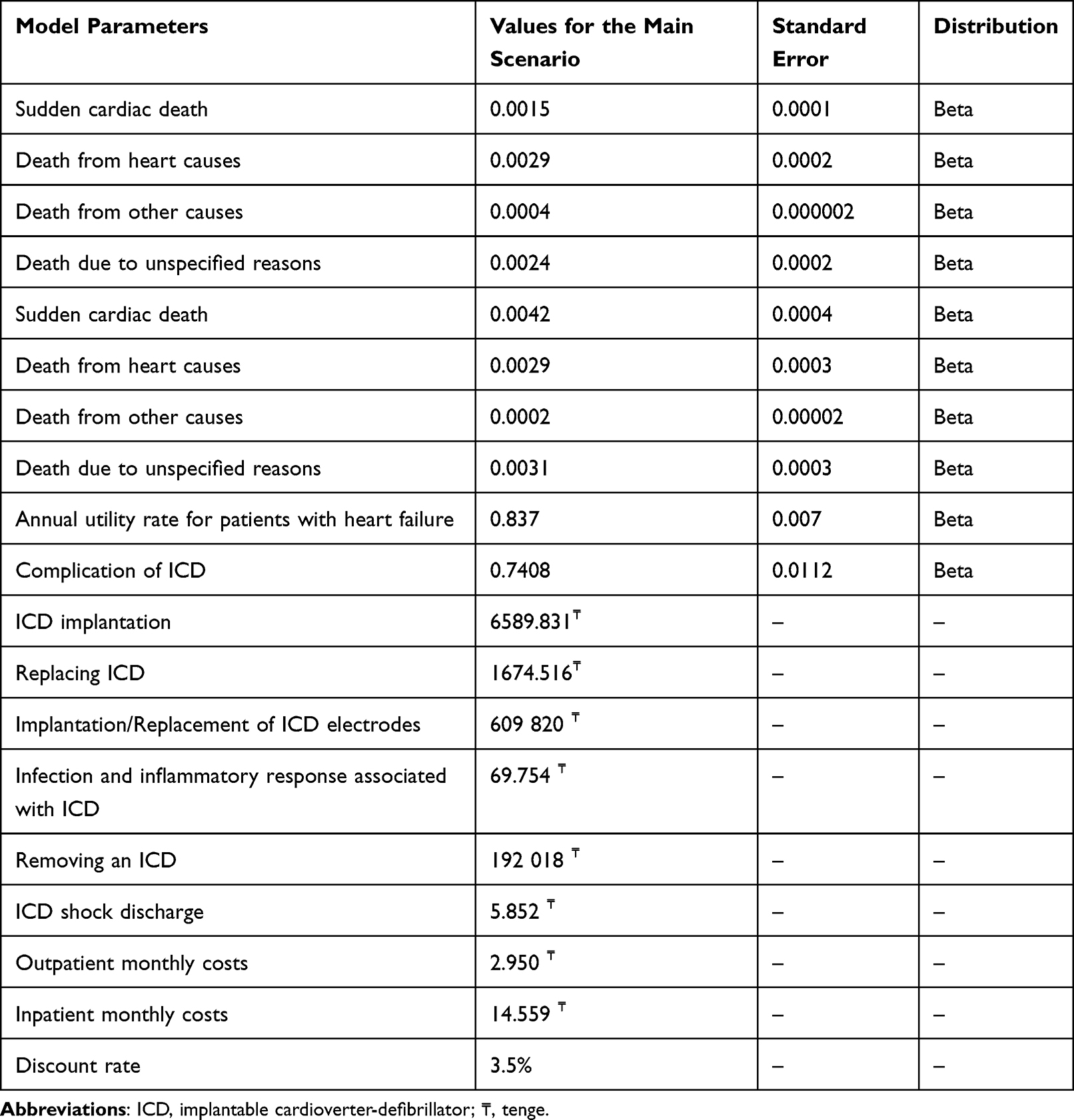 |
Table 1 Input Parameters of the Model |
Model Structure
The model was based on previously published studies8,13 and is constructed as a decision tree with two treatment groups, with or without ICD therapy, followed by successive Markov cycles (Figure 1). The baseline simulation scenario included a cohort of 1000 patients with standard indications for primary prevention by implantation of a cardioverter-defibrillator. Patients in the ICD group were at risk of dying during surgery. Patients who underwent ICD surgery entered the Markov model in a state of “well-being” in which they could remain or go into states of “ICD complications”, “sudden cardiac death”, “death from non-cardiac causes”, and “death from unknown causes.” Patients remained in the same state or transitioned to a different state at the beginning of each cycle, apart from the complication state. Patients who developed a complication after ICD remained in a complication state for only one cycle, then transitioned to “continue ICD therapy” or “discontinue ICD therapy”. After ICD removal, patients may also remain in a “well-being” state or die for one reason or another. Patients in the non- ICD group enter the model in good health and remain healthy or progress to sudden cardiac death, not sudden cardiac death, non-cardiac death, or unknown death.
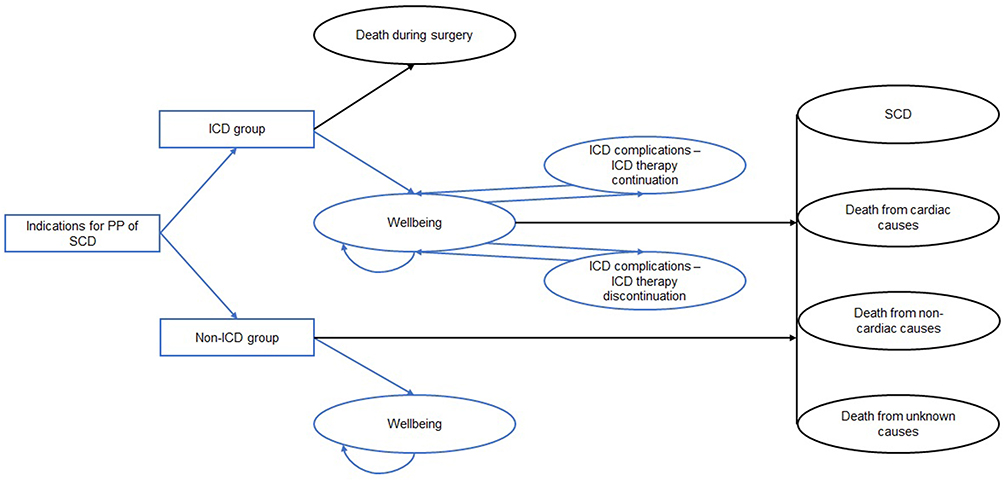 |
Figure 1 Graphic representation of the model. Abbreviations: ICD, implantable cardioverter-defibrillator; PP, primary prevention; SCD, sudden cardiac death. |
Progressing the patient cohort monthly throughout life (35 years) was associated with cost and utility rates for each condition; the time horizon of the model allowed the model to consider all possible costs of the payer in the health care system of the country associated with patients. Patients in both comparison groups were associated with monthly expenses for inpatient and outpatient treatment, which were calculated based on the approved tariffs for medical interventions and the frequency of these procedures per year based on the recommendations of the current clinical treatment protocols. The ICD treatment group also included the cost ICDs the ICD implantation procedure. Patients with ICD who survived long enough to require device replacement incurred additional costs for re-implantation. Patients with ICD may have received shocks that were misconfigured or other ICD -related complications that were costly and affected adherence. After an inadequate shock or other ICD-related complication occurred, patients could remain in the ICD group or go into a state of discontinuation of the ICD. It has been hypothesized that patients with ICD who discontinue use of the ICD have the same risk of death as patients in the non- ICD group.
Clinical Parameters of the Model
Baseline mortality data for patients with indications for primary prevention of SCD were based on previously published meta-analyzes and the Improve SCA18,19 study. The data on perioperative mortality associated with ICD is based on statistics from the Electronic Inpatient Register of the Republican Center for Electronic Health and is applicable only to the ICD therapy group. The likelihood of inadequate electrical discharge was obtained by calculating a weighted average based on previously published studies.20–23 The probability of electrode failure (0.45%) or displacement (1.8%) after initial implantation and the probability of displacement of the ICD generator and its replacement (about 1%) are also taken from the literature.24–26 The potential for infection of an implanted device after initial ICD implantation (1.2%) and after replacement (2.16%) is based on data from a study by Eby EL et al.27
Economic Parameters of the Model
The model calculates the direct medical costs associated with the implantation of an automatic cardioverter-defibrillator and the health care costs associated with cardiovascular disease throughout the patient’s life. The cost of the ICD and implantation procedure, its subsequent revision, complete or partial replacement, as well as the cost of treating complications associated with the ICD (infection, displacement, inadequate discharges), the cost of diagnostic tests and specialist consultations at an outpatient level, were obtained from the tariffs for medical services provided within the SGBP and in the system of MSHI, approved by Minister of Health of the Republic of Kazakhstan.28
Health-Related Quality of Life
Due to the absence of Kazakhstan-specific utility coefficients, the quality-of-life indicators in the model were based on literature data.29 The model suggests that baseline utility different for patients in the ICD group and for the non- ICD group.30 Patients who developed a complication after ICD implantation had a short-term decrease in utility of 0.096, which is equivalent to 3.5 days.31
Incremental Cost-Effectiveness Ratio (ICER), Willingness to Pay Threshold
The incremental cost-effectiveness ratio (ICER) was calculated by correlating the difference in costs in the ICD group and in the non- ICD group to the difference in quality-adjusted life-years (QALYs) obtained. For greater reliability, ICER was calculated both without discounting and considering the application of the discount rate. As a threshold of willingness to pay for one quality year of life, in accordance with the WHO recommendations, three times the average annual GDP per capita in 2020 was taken, which amounted to 27,167.25 US dollars or 3,845,705,36 Kazakh tenge at the weighted average rate at the time of research.32
Sensitivity Analysis
To identify and analyze the influence of model parameters on the result, a one-way deterministic sensitivity analysis was carried out. To determine the reliability of the model and its robustness to the uncertainty of the input parameters, a probabilistic sensitivity analysis was also carried out. The beta distribution was used for both the probabilities of transition of patients from one state to another, and for the parameters of utility.
Results
Main Scenario
The analysis showed that the use of ICD for the primary prevention of SCD would provide 117.8 additional months of life per patient without discounting and 106.6 months with discounting. In the group of patients who did not undergo ICD, this indicator was 88.4 and 81.6 months without discounting and discounted, respectively. In terms of quality-adjusted life years, the following results were obtained: ICD implantation resulted in a retention of 6.5 (7.2 without discounting), while patients in the non-ICD group received 5.0 QALYs (5.4 without discounting). Thus, the difference per patient was 1.5 QALY (1.8 without discounting).
It was calculated that the total direct medical costs, considering discounting, for patients with and without ICD will be 8,903,786 tenges and 3,194,414 tenges, respectively. The cost-effectiveness ratio for ICD implantation was3791604 tenge per 1 QALY, which is below the commonly used willingness to pay threshold. Thus, the implantation of a cardioverter-defibrillator for the primary prevention of sudden cardiac arrest in Kazakhstan’s healthcare environment may be considered cost-effective from the payer’s perspective (Table 2).
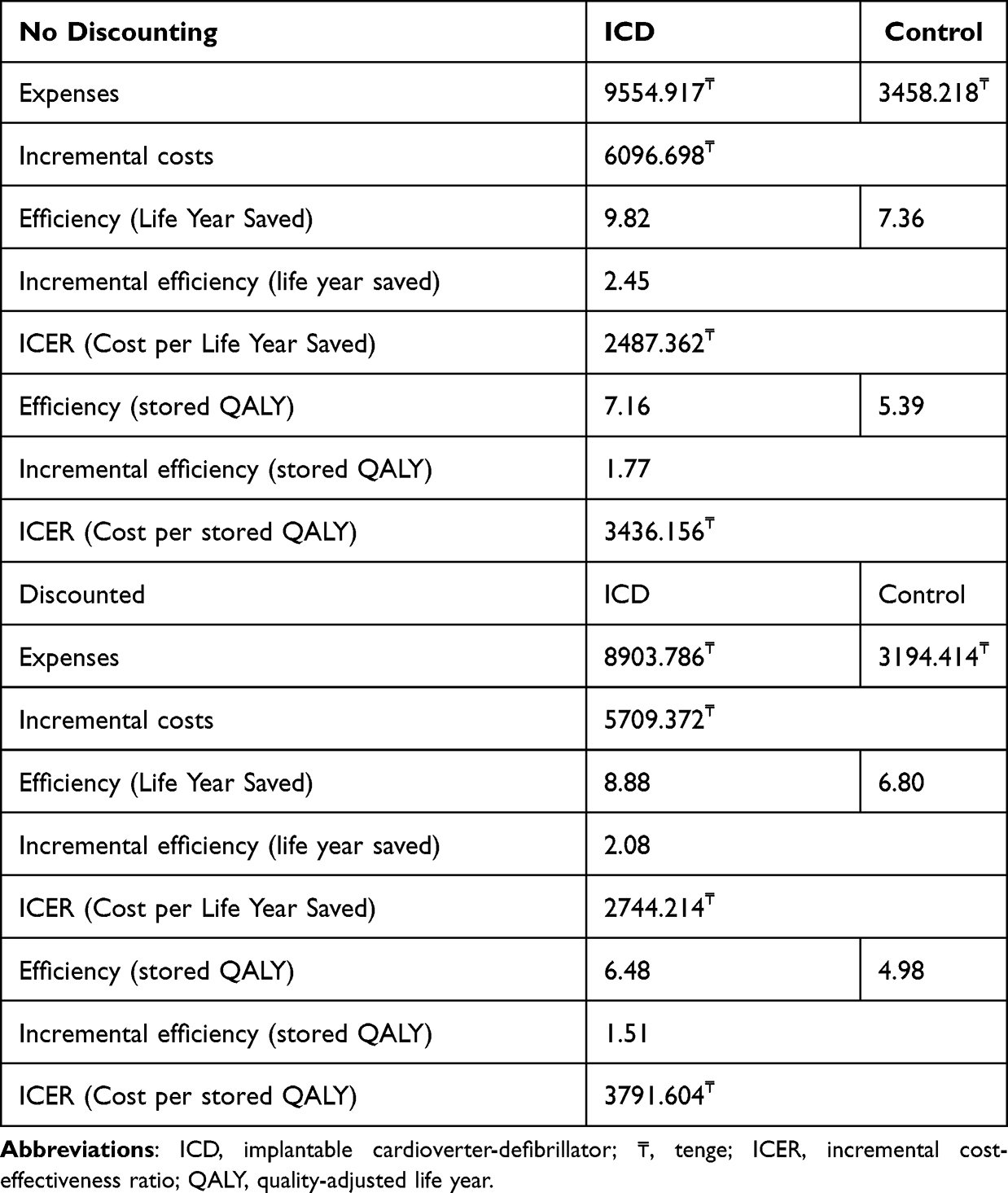 |
Table 2 Results of the Main Scenario |
Sensitivity Analysis
One-sided deterministic sensitivity analysis showed that the quality-adjusted cost-effectiveness ratio (ICER) for 1 added year of life is more dependent on the following parameters: the patient’s age at the time of ICD implantation, the overall mortality rate, and quality of life indicators.
Figure 2 shows the modeled cost per QALY from the probabilistic sensitivity analysis. Based on the results of 1000 simulations, the average costs per 1 QALY amounted to KZT 3,765,770.65 (median costs per 1 QALY amounted to KZT 3,754,881.24, 95% CI [KZT 2,518,234.80 - KZT 14,345,161.99] per 1 QALY) after 1000 iterations. At the same time, 99.5% of simulations showed ICER for 1 QALY below willingness to pay threshold, which indicates a high cost-effectiveness of implantation of a cardioverter-defibrillator for the primary prevention of sudden cardiac arrest in Kazakhstan’s healthcare environment.
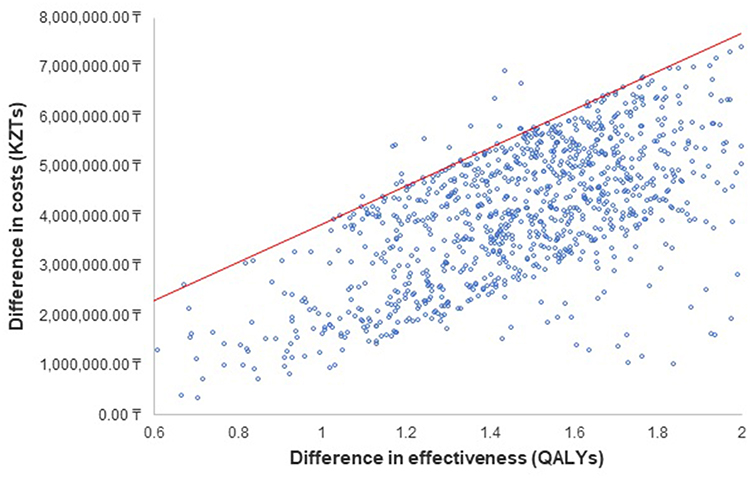 |
Figure 2 Results of sensitivity analysis. Abbreviations: QALYs, quality-adjusted life year; KZT, Kazakh tenge. |
Discussion
Despite compelling evidence from randomized clinical trials and recommendations in international clinical guidelines, the frequency of ICD use in Kazakhstan is relatively low. According to this indicator, Kazakhstan can be compared with the countries of Latin America, such as Argentina (up to 56 implantations per million per year).10 For comparison, in Europe, on average, over 150 ICDs (per million) are implanted per year,33 while in South Korea this figure reaches 200 devices (per 100,000) per year.12
In our study, we found a cost-effectiveness ratio of fewer than 4,000,000.00 tenges per QALY gained. A probabilistic sensitivity analysis of the model confirmed these results. Kazakhstan does not currently have a set willingness-to-pay threshold. If we apply the World Health Organization Choice for Cost-Effective Interventions (WHO-CHOICE) Project, a widely accepted recommendation for setting a willingness-to-pay threshold of fewer than three times the national annual gross domestic product (GDP) per capita, then this intervention can be considered very cost-effective.34
Our results are generally consistent with the available literature on the cost-effectiveness of ICD use. For example, in the United States, it was estimated that the use of ICD is an economically attractive technology with ICER more than 2 times lower than the established willingness to pay threshold.14 Similar results were obtained in studies conducted in the conditions of Europe,13 Taiwan, Brazil, and other Latin American countries.13,18,35,36
The main limitation of this study is the fact that some input parameters for constructing a mathematical model were taken from foreign sources due to the lack of similar available data for Kazakhstan. However, this is a standard approach in economic modeling, and the fact that the authors used real figures from official sources for the country to calculate the costs and likelihood of perioperative mortality makes the results of this study as reliable and close to reality as possible.
Conclusion
The implantation of a cardioverter-defibrillator for the primary prevention of sudden cardiac arrest in Kazakhstan’s healthcare environment is cost-effective. The data obtained can serve as the basis for justifying and stimulating the more frequent use of ICD therapy in this cohort of patients in Kazakhstan. Additional studies to identify the most “cost-effective” subgroups of patients for cardioverter-defibrillator implantation could contribute to better prioritization and, accordingly, better planning of the allocation of the available budget, which is relevant given the limited health care resources of the country.
Data Sharing Statement
Materials and these articles are with the authors.
Ethical Approval
The study was approved by the Local Ethics Committee of Kazakhstans Medical University “KSPH”, Almaty, Kazakhstan.
Consent for Publication
All authors consent for publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare they have no competing interests.
References
1. Moss AJ, Zareba W, Hall WJ, et al.; Multicenter Automatic Defibrillator Implantation Trial II Investigators. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346(12):877–883. doi:10.1056/NEJMoa013474
2. Al-Khatib SM, Hellkamp AS, Lee KL, et al.; scd-heft investigators. Implantable cardioverter defibrillator therapy in patients with prior coronary revascularization in the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT). J Cardiovasc Electrophysiol. 2008;19(10):1059–1065. doi:10.1111/j.1540-8167.2008.01191.x
3. Poole JE, Olshansky B, Mark DB, et al.; SCD-HeFT Investigators. Long-term outcomes of implantable cardioverter-defibrillator therapy in the SCD-HeFT. J Am Coll Cardiol. 2020;76(4):405–415. doi:10.1016/j.jacc.2020.05.061
4. Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2018;138:e210–e271. doi:10.1161/CIR.0000000000000548
5. Priori SG, Blomström-Lundqvist C, Mazzanti A, et al.; ESC Scientific Document Group (2015). ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC). Endorsed by: association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J. 2015;36(41):2793–2867. doi:10.1093/eurheartj/ehv316
6. Sequeira S, Jarvis CI, Benchouche A, Seymour J, Tadmouri A. Cost-effectiveness of remote monitoring of implantable cardioverter-defibrillators in France: a meta-analysis and an integrated economic model derived from randomized controlled trials. Europace. 2020;22(7):1071–1082. doi:10.1093/europace/euaa082
7. Gialama F, Prezerakos P, Maniadakis N. The cost effectiveness of implantable cardioverter defibrillators: a systematic review of economic evaluations. Appl Health Econ Health Policy. 2014;12(1):41–49. doi:10.1007/s40258-013-0069-2
8. Higuera L, Holbrook R, Wherry K, et al. Comparison of cost-effectiveness of implantable cardioverter defibrillator therapy in patients for primary prevention in Latin America: an analysis using the Improve SCA study. J Med Econ. 2021;24(1):173–180. doi:10.1080/13696998.2021.1877451
9. Chia Y, Teng TK, Tan E, et al. Disparity between indications for and utilization of implantable cardioverter defibrillators in Asian patients with heart failure. Circ Cardiovasc Qual Outcomes. 2017;10(11):e003651. doi:10.1161/CIRCOUTCOMES.116.003651
10. Mond HG, Proclemer A. The 11th world survey of cardiac pacing and implantable cardioverter-defibrillators: calendar year 2009–a World Society of Arrhythmia’s project. PACE. 2011;34(8):1013–1027. doi:10.1111/j.1540-8159.2011.03150.x
11. Lozano IF, Asensi JO, Rodríguez JA; Spanish Implantable Cardioverter-defibrillator Registry. 16th official report of the heart rhythm association of the spanish society of cardiology (2019). Rev Esp Cardiol. 2020;73(12):1026–1037.
12. Lee JH, Lee SR, Choi EK, et al. Temporal trends of cardiac implantable electronic device implantations: a nationwide population-based study. Korean Circ J Sep. 2019;49(9):841–852. doi:10.4070/kcj.2018.0444
13. Holbrook R, Higuera L, Wherry K, et al. Implantable cardioverter defibrillator therapy is cost effective for primary prevention patients in Taiwan: an analysis from the Improve SCA trial. PLoS One. 2020;15(11):e0241697. doi:10.1371/journal.pone.0241697
14. Mark DB, Nelson CL, Anstrom KJ, et al.; SCD-HeFT Investigators. Cost-effectiveness of defibrillator therapy or amiodarone in chronic stable heart failure: results from the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT). Circulation. 2006;114(2):135–142. doi:10.1161/CIRCULATIONAHA.105.581884
15. Chanturidze T, Adams O, Tokezhanov B, Naylor M, Richardson E. Building policy-making capacity in the Ministry of Health: the Kazakhstan experience. Hum Resour Health. 2015;13:4. doi:10.1186/1478-4491-13-4
16. Kazakhstan - health sector technology transfer and institutional reform project (english). Washington, D.C: World Bank Group. Available from: http://documents.worldbank.org/curated/en/823341515169244215/Kazakhstan-Health-Sector-Technology-Transfer-and-Institutional-Reform-Projec.
17. Sharma D, Aggarwal AK, Downey LE, Prinja S. National healthcare economic evaluation guidelines: a cross-country comparison. Pharmacoecon Open. 2021;5(3):349–364. doi:10.1007/s41669-020-00250-7
18. Cowie MR, Marshall D, Drummond M, et al. Lifetime cost-effectiveness of prophylactic implantation of a cardioverter defibrillator in patients with reduced left ventricular systolic function: results of Markov modelling in a European population. Europace. 2009;11(6):716–726. doi:10.1093/europace/eup068
19. Zhang S, Ching CK, Huang D, et al.; Improve SCA Investigators. Utilization of implantable cardioverter-defibrillators for the prevention of sudden cardiac death in emerging countries: improve SCA clinical trial. Heart Rhythm. 2020;17(3):468–475. doi:10.1016/j.hrthm.2019.09.023
20. Moss AJ, Schuger C, Beck CA, et al. MADIT-RIT Trial Investigators Reduction in inappropriate therapy and mortality through ICD programming. N Engl J Med. 2012;367(24):2275–2283. doi:10.1056/NEJMoa1211107
21. Gasparini M, Proclemer A, Klersy C, et al. Effect of long-detection interval vs standard-detection interval for implantable cardioverter-defibrillators on antitachycardia pacing and shock delivery: the ADVANCE III randomized clinical trial. JAMA. 2013;309(18):1903–1911. doi:10.1001/jama.2013.4598
22. Saeed M, Hanna I, Robotis D, et al. Programming implantable cardioverter-defibrillators in patients with primary prevention indication to prolong time to first shock: results from the PROVIDE study. J Cardiovasc Electrophysiol. 2014;25(1):52–59. doi:10.1111/jce.12273
23. Auricchio A, Schloss EJ, Kurita T, et al.; PainFree SST Investigators. Low inappropriate shock rates in patients with single- and dual/triple-chamber implantable cardioverter-defibrillators using a novel suite of detection algorithms: painFree SST trial primary results. Heart Rhythm. 2015;12(5):926–936. doi:10.1016/j.hrthm.2015.01.017
24. Ghani A, Delnoy PP, Ramdat Misier AR, et al. Incidence of lead dislodgement, malfunction and perforation during the first year following device implantation. Neth Heart J. 2014;22(6):286–291. doi:10.1007/s12471-014-0556-6
25. Providência R, Kramer DB, Pimenta D, et al. Transvenous Implantable Cardioverter-Defibrillator (ICD) lead performance: a meta-analysis of observational studies. J Am Heart Assoc. 2015;4(11):e002418. doi:10.1161/JAHA.115.002418
26. Poole JE, Gleva MJ, Mela T, et al.; REPLACE Registry Investigators. Complication rates associated with pacemaker or implantable cardioverter-defibrillator generator replacements and upgrade procedures: results from the REPLACE registry. Circulation. 2010;122(16):1553–1561. doi:10.1161/CIRCULATIONAHA.110.976076
27. Eby EL, Bengtson L, Johnson MP, Burton ML, Hinnenthal J. Economic impact of cardiac implantable electronic device infections: cost analysis at one year in a large U.S. health insurer. J Med Econ. 2020;23(7):698–705.
28. Order of the Minister of Health of the Republic of Kazakhstan dated September 5, 2018 No. ҚР ДСМ-10. Registered in the Ministry of Justice of the Republic of Kazakhstan on September 7, 2018 No. 17353. On approval of tariffs for medical services provided within the guaranteed volume of free medical care and in the system of compulsory social health insurance; 2018.
29. Sears SF, Rosman L, Sasaki S, et al. Defibrillator shocks and their effect on objective and subjective patient outcomes: results of the PainFree SST clinical trial. Heart Rhythm. 2018;15(5):734–740. doi:10.1016/j.hrthm.2017.12.026
30. Bundgaard JS, Thune JJ, Nielsen JC, et al. The impact of implantable cardioverter-defibrillator implantation on health-related quality of life in the DANISH trial. Europace. 2019;21(6):900–908. doi:10.1093/europace/euz018
31. Sanders GD, Hlatky MA, Owens DK. Cost-effectiveness of implantable cardioverter-defibrillators. N Engl J Med. 2005;353(14):1471–1480. doi:10.1056/NEJMsa051989
32. Shiroiwa T, Sung YK, Fukuda T, Lang HC, Bae SC, Tsutani K. International survey on willingness-to-pay (WTP) for one additional QALY gained: what is the threshold of cost effectiveness? Health Econ. 2010;19(4):422–437. doi:10.1002/hec.1481
33. Pekka Raatikainen MJ, Arnar DO, Zeppenfeld K, Merino JL, Kuck K-H, Hindricks G. Current trends in the use of cardiac implantable electronic devices and interventional electrophysiological procedures in the European Society of Cardiology member countries: 2015 report from the European Heart Rhythm Association. EP Europace. 2015;17(suppl_4):iv1–iv72. doi:10.1093/europace/euv265
34. World Health Organization. Making Choices in Health: WHO Guide to Cost-Effectiveness Analysis. Tan-Torres Edejer T, Baltussen R, Adam T, et al. Geneva: World Health Organization; 2003.
35. Wherry K. Cost-effectiveness analysis of implantable cardioverter defibrillator therapy for primary prevention patients with additional risk factors in Brazil. Int J Cardiovasc Sci. 2021. doi:10.36660/ijcs.20200016
36. Boriani G, Cimaglia P, Biffi M, et al. Cost-effectiveness of implantable cardioverter-defibrillator in today’s world. Indian Heart J. 2014;66(Suppl1):S101–S104. doi:10.1016/j.ihj.2013.12.034
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.