Back to Journals » Journal of Pain Research » Volume 18
Corticospinal Excitability in Bilateral M1 Hand Areas: Association with Neuropathic Pain After Spinal Cord Injury
Authors Liu X ![]() , Dai C, Gao M, Lin X, Xi X, Wu X, Cheng G, Han T, Li Q, Lu Y
, Dai C, Gao M, Lin X, Xi X, Wu X, Cheng G, Han T, Li Q, Lu Y ![]() , Sun X
, Sun X ![]() , Yuan H
, Yuan H ![]()
Received 30 January 2025
Accepted for publication 22 July 2025
Published 11 August 2025 Volume 2025:18 Pages 4003—4018
DOI https://doi.org/10.2147/JPR.S517353
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor King Hei Stanley Lam
Xinyu Liu,1,2,* Chunqiu Dai,1,3,* Ming Gao,1,* Xiaodong Lin,1 Xiao Xi,1 Xiangbo Wu,1 Guiqing Cheng,1 Tao Han,1 Qiaozhen Li,1 Yixing Lu,1 Xiaolong Sun,1 Hua Yuan1
1Department of Rehabilitation Medicine, The First Affiliated Hospital, Air Force Medical University (Fourth Military Medical University) of Chinese People’s Liberation Army, Xi’an, Shaanxi, People’s Republic of China; 2Department of Rehabilitation Medicine, The 940th Hospital of Joint Logistics Support Force of Chinese People’s Liberation Army, Lanzhou, Gansu, People’s Republic of China; 3Lintong Rehabilitation and Convalescent Centre, Xi’an, Shaanxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hua Yuan; Xiaolong sun, Department of Rehabilitation Medicine, The First Affiliated Hospital, Air Force Medical University (Fourth Military Medical University) of Chinese People’s Liberation Army, No. 127, Changle West Road, Xi’an, Shaanxi, 710032, People’s Republic of China, Tel/Fax +86-29-84775437 ; +86-29-84775439, Email [email protected]; [email protected]
Purpose: Neuropathic pain (NP) is a major and debilitating complication of spinal cord injury (SCI), frequently occurring bilaterally below the injury level. Repetitive transcranial magnetic stimulation (rTMS) targeting the primary motor cortex (M1) is suggested as a treatment for NP following SCI (SCI-NP). However, the specific changes in corticospinal excitability (CSE) within the bilateral M1 remain unclear, hindering the development of optimized rTMS parameters for SCI-NP.
Patients and Methods: This retrospective study analyzed data from 625 SCI patients and 131 healthy controls. Motor-evoked potential (MEP) was used to assess CSE in the bilateral M1 hand areas. The hemispheric asymmetry of bilateral M1 CSE was measured by calculating the natural logarithm of the MEP amplitude ratio between the dominant hemisphere (DH) and non-dominant hemisphere (NDH), expressed as ln(DH/NDH amplitude). The study utilized correlation analysis and multiple linear regression to examine the associations between hemispheric CSE asymmetry and the course, severity, and emotional disturbances of NP.
Results: SCI patients experiencing NP exhibited lower MEP amplitude than those without NP in bilateral M1 hand areas, with a more pronounced decrease in NDH. Hemispheric CSE asymmetry was found to be elevated and positively correlated with NP course (r=0.213, P=0.034), severity (r=0.317, P=0.004), and emotional disturbances (r=0.294, P=0.009). Notably, hemispheric CSE asymmetry was independently associated with NP severity and emotional disturbances, particularly in younger individuals (under 52 years), those with traumatic injuries, and those with non-cervical SCI.
Conclusion: Hemispheric CSE asymmetry shows potential as a biomarker for assessing SCI-NP severity and emotional disturbances in SCI patients. High-frequency rTMS targeting bilateral M1 hand areas may provide improved analgesic effects. This finding could enhance neuropathic pain assessment and guide rTMS optimization, potentially improving the quality of life for individuals with SCI.
Keywords: spinal cord injury, neuropathic pain, corticospinal excitability, MEP, hemispheric CSE asymmetry, rTMS
Graphical Abstract:

Introduction
Spinal cord injury (SCI) predominantly affects individuals in their younger and middle adult years.1 Neuropathic pain (NP), occurring in 84–92% of SCI patients, significantly impedes rehabilitation and exacerbates sleep disturbances, depression, and anxiety, creating a substantial economic burden on society.2,3 Although pharmacological interventions are the mainstay of NP management, their effectiveness is limited, and adverse effects, including increased overdose-related mortality, are concerning.4–6
Repetitive transcranial magnetic stimulation (rTMS) has shown promise as a non-pharmacological treatment for SCI-NP. The analgesic effects are linked to modulating the primary motor cortex (M1) excitability, affecting pain perception and emotional processing through cortico-limbic circuits.7 International guidelines suggest high-frequency rTMS on the contralateral M1 for unilateral NP.8 However, SCI often leads to bilateral NP in the trunk and lower limbs, creating uncertainty about the optimal side of M1 stimulation side.9,10 Furthermore, there is ongoing debate about whether the ideal stimulation site in M1 should be the somatotopic pain region or the more accessible hand area. For example, Jetté et al demonstrated effective SCI-NP relief with high-frequency rTMS targeting the M1 hand or leg area contralateral to the more affected or dominant hand side, while Defrin et al reported no significant difference between sham and active rTMS targeting the M1 lower limb region in SCI-NP patients.11,12 The deeper localization of the lower limb region complicates stimulation, favoring the hand area for its accessibility and clinical practicality.13,14 Our previous studies found that high-frequency rTMS of the left M1 hand area provided analgesic effects for SCI-NP. Nonetheless, these effects were restricted, necessitating a minimum of two weeks of treatment to achieve notable improvement over sham stimulation.15,16 The lack of clarity about excitability changes in the bilateral M1 hand areas adds to the ongoing discussion about rTMS parameters.
TMS-induced motor evoked potentials (MEPs) have been established as a reliable neurophysiological tool for assessing corticospinal excitability (CSE). This technique offers distinct advantages including excellent temporal resolution and non-invasive evaluation of corticospinal pathway integrity.17 As a stable and reproducible measure, MEPs provide valuable insights into the functional state of the corticospinal tract (CST), making them particularly useful for both research applications and clinical assessment. In complex regional pain syndrome (CRPS), Krause et al identified significant hemispheric asymmetry in motor cortical representation (size, MEP, and calculated volumes) in affected versus unaffected muscles.18 Similarly, Barbosa et al found that stroke patients with central neuropathic pain (CNP) exhibited significantly lower MEP amplitudes in both hemispheres compared to those with non-neuropathic pain or no pain.19 Thus, MEPs provide objective and quantifiable metrics for evaluating pain characteristics.
To comprehensively assess neuropathic pain characteristics, we employed the Short-Form McGill Pain Questionnaire-2 (SF-MPQ-2), a validated multidimensional pain assessment tool comprising 22 items across four subscales: continuous pain, intermittent pain, predominantly neuropathic pain, and affective descriptors.20,21 While the full SF-MPQ-2 was used to evaluate overall neuropathic pain severity, we specifically utilized its fourth subscale (SF-MPQ-2-4) to quantify pain-related negative emotional states, as these affective components may independently influence corticospinal excitability in pain conditions.
This retrospective study examined alterations in CSE in the bilateral M1 hand areas of SCI-NP patients and analyzed its correlation with the NP course and severity, with the goal of offering objective evidence for NP assessment and the optimization of rTMS parameters.
Materials and Methods
Study Design
This retrospective cross-sectional study analyzed neurophysiological and pain-related data from patients with SCI who experienced NP or no neuropathic pain (NNP), as well as healthy controls. Data were gathered from January 2018 to April 2024 in the inpatient unit of the Department of Rehabilitation Medicine at the First Affiliated Hospital of Air Force Medical University of Chinese People’s Liberation Army. The Medical Ethics Committee of the First Affiliated Hospital of Air Force Medical University of Chinese People’s Liberation Army approved the study (No. KY20222096-C-1), and the study was registered in the Chinese Clinical Trial Registry (ChiCTR2300073824). Due to the retrospective nature of this study, informed consent was waived as it would not adversely affect the rights and welfare of the subjects, and it was objectively impossible to obtain informed consent from the subjects. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Participants
Inclusion criteria for SCI patients included: a. Age of 18–70 years, right hand dominance (as determined by the Edinburgh Handedness Inventory);22 b. Diagnosed with SCI;23 c. Disease course ≤ 36 months (from SCI onset to clinical assessment and MEP measurement, with recovery from spinal shock); d. No rTMS therapy within the past 2 weeks; e. No cognitive impairment (Mini-Mental State Examination (MMSE) score ≥ 24);24 f. For the NP group, diagnosis of NP following SCI.25 Exclusion criteria included: a. Severe language impairment; b. Presence of conductive, ferromagnetic, or other magnetically sensitive metals in the head or neck, as well as a pacemaker; c. Seizures within the past six months; d. Severe local or systemic diseases that prevent tolerance of relevant tests; e. Other types of pain (eg, musculoskeletal pain, visceral pain, or non-neuropathic pain); f. Use of medications that may affect MEP recordings within the past week, such as baclofen, diazepam, or similar drugs;26 g. MEP measurements of the M1 hand area were not conducted.
Healthy controls included individuals aged 18–70 years, matched with SCI patients, who were right-hand dominant (as determined by the Edinburgh Handedness Inventory) and had stable MEPs in bilateral M1 hand areas. Exclusion criteria encompassed conditions preventing TMS application and individuals with acute or chronic pain.
Motor Evoked Potentials
MEPs were captured using a TMS device (MEP-9404C, Japan) and 10 mm Ag-AgCl surface electrodes on the abductor pollicis brevis muscle, adhering to a standardized protocol.27 The TMS coil was aligned with the M1 hand area’s surface projection, precisely targeting the “hot spot” with single-pulse TMS at 80% of the stimulator’s maximum output.28 MEPs were recorded every 5 seconds. MEPs elicited from both bilateral M1 hand areas were classified as “Bilateral MEP Elicited” (B-MEP), while those elicited unilaterally or not at all were categorized as “Non-Bilateral MEP Elicited” (NB-MEP).
Evaluation of Hemispheric CSE in Bilateral M1 Hand Areas
A previously established method was used to assess hemispheric CSE symmetry in the bilateral M1 hand areas.29 Hemispheric CSE asymmetry was quantified by calculating the natural logarithm of the MEP amplitude ratio between the dominant hemisphere (DH) and non-dominant hemisphere (NDH): ln (DH/NDH amplitude). An asymmetry value of 0 indicates equal excitability between the DH and NDH [ln(1) = 0]; a value greater than 0 indicates greater excitability in the DH compared to the NDH [ln(>1) > 0]; and a value less than 0 suggests lower excitability in the DH than in the NDH [ln(<1) < 0].
NP Assessment
SF-MPQ-2, known for its clinical reliability and validity, was employed to assess the multidimensional aspects of NP.20,21 This tool comprises 22 items distributed across four subscales: continuous pain, intermittent pain, predominantly NP, and affective descriptors. Items are rated on a 0 to 10 scale, where higher scores denote more intense pain or negative emotional states.30
Statistical Analysis
General Data Statistics
Continuous variables are expressed as mean ± standard deviation (SD) for normally distributed data and as median with interquartile range (IQR) for non-normally distributed data. Categorical variables were represented as frequencies and percentages [N (%)]. Statistical analyses included the Kruskal–Wallis test for multiple group comparisons of continuous variables, Fisher’s exact test or the Chi-square test for categorical variables, and the Mann–Whitney U test for two independent groups of continuous or ordinal data. A P-value below 0.05 was deemed statistically significant.
MEPs and CSE Asymmetry
The Shapiro–Wilk test evaluated the normality of data for MEP amplitude, latency, and central motor conduction time (CMCT). The Kruskal–Wallis test was used to compare the variables among the NP, NNP, and control groups due to the non-normal distribution of the data. The Wilcoxon signed-rank test was used for post hoc comparisons. Additionally, a non-parametric paired test was utilized to compare the DH and NDH variables within each group. A one-way ANOVA was conducted on the natural logarithm of the dominant to non-dominant hand amplitude ratio to assess hemispheric CSE asymmetry, followed by post hoc comparisons using the least significant difference (LSD) test. The Kruskal–Wallis test was used to assess hemispheric symmetry of MEP latency and CMCT, followed by the Wilcoxon signed-rank test for post hoc analysis. Statistical significance was considered at a level of P < 0.05.
Analysis of Correlation and Regression
Following confirmation of non-normal distributions via Shapiro–Wilk testing, Spearman correlation analysis assessed the relationship between hemispheric CSE asymmetry and the course and intensity of NP. Subgroup analyses were performed to investigate the effects of age, etiology of SCI, and neurological level of injury (NLI). To assess the impact of age on MEP amplitude in bilateral M1 hand areas, patients were classified into two age groups: <52 years and ≥52 years, using receiver operating characteristic (ROC) curve analysis for optimal cut-off determination.31,32 Additionally, patients were categorized into traumatic (eg, compression by heavy objects, traffic accidents, falls) and non-traumatic (eg, congenital or disease-related factors) SCI groups. Patients were categorized into cervical and non-cervical (thoracic, lumbar, sacral) injury groups to assess the potential influence of cervical injuries on MEP amplitude stability.
Univariate and multivariate linear regression analyses were conducted to assess the effect of MEP hemispheric asymmetry in the M1 hand area on pain outcomes. The study examined MEP hemispheric asymmetry as the independent variable, while the SF-MPQ-2 total scores and its affective subscale (SF-MPQ-2-4) served as the dependent variables. Variables with P-values below 0.10 in the univariate analysis were incorporated into the multivariate model. Statistical significance was determined at a P-value threshold of 0.05.
All analyses were conducted using SPSS 27.0, and data visualizations were generated with GraphPad Prism 9.5 and R 4.4.1.
Results
Basic Characteristics of NP, NNP Patients, and Healthy Controls
Data were collected from 625 SCI patients admitted to the inpatient unit of the Department of Rehabilitation Medicine at the First Affiliated Hospital of Air Force Medical University of Chinese People’s Liberation Army between January 2018 and April 2024. A total of 78 patients were excluded for not meeting the inclusion criteria. A total of 325 patients were excluded due to exclusion criteria: 263 had other types of pain, and 62 lacked MEP measurements in the M1 hand area. The remaining 222 patients were categorized into B-MEP (N = 155) and NB-MEP (N = 67) groups based on whether MEPs were elicited from bilateral or unilateral M1 hand areas. The B-MEP group was further subdivided into the patients with NP (N = 114) and NNP (N = 41) (Figure 1). For comparison, 131 healthy controls matched by age and sex were analyzed alongside the NP and NNP groups.
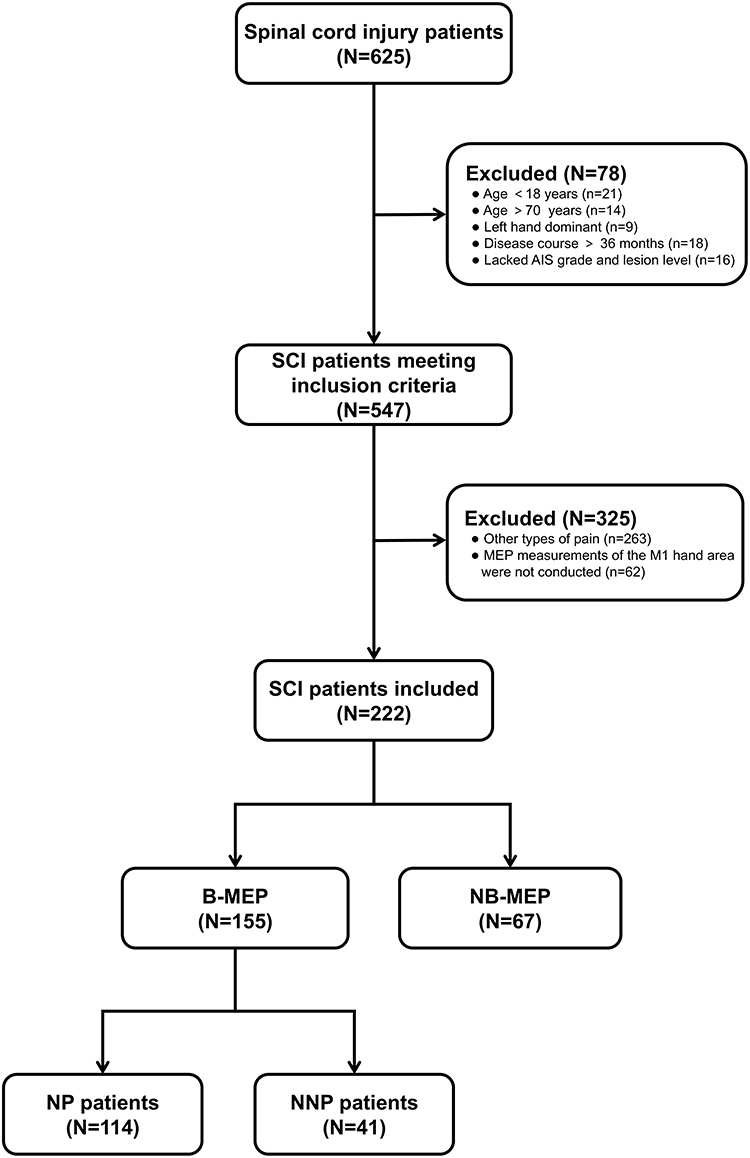 |
Figure 1 Study Flowchart. Data were collected from 625 SCI patients admitted to the inpatient unit of the Department of Rehabilitation Medicine at the First Affiliated Hospital of Air Force Medical University between January 2018 and April 2024. Of these, 78 patients were excluded for failing to meet the inclusion criteria, and 325 patients were excluded based on the exclusion criteria. The remained 222 patients were classified into B-MEP (N = 155) and NB-MEP (N = 67) groups based on MEPs elicited from bilateral or unilateral M1 hand areas. The B-MEP group was further subdivided into patients with NP (N = 114) or NNP (N = 41). For comparison, 131 healthy controls matched by age and sex were analyzed alongside the NP and NNP groups. |
Table 1 outlines the fundamental characteristics of the B-MEP and NB-MEP groups. While no significant disparities were observed in age or gender between the two groups, notable differences emerged in NLI, AIS grade, and the incidence of NP. Patients in the B-MEP group demonstrated a lower NLI, milder injury severity, and a higher incidence of NP. Table 2 presents the basic characteristics of NP, NNP patients, and healthy controls. Although no significant differences were found in age [44.00 (35.00, 54.00) years] or sex distribution [male N(%): 85 (64.89%)] among these groups, 78.95% of NP patients reported lower limb pain, and 87.72% experienced bilateral pain (Table 2). Additionally, NP and NNP patients showed no significant differences in disease course, etiology, NLI, AIS grade, or other baseline characteristics.
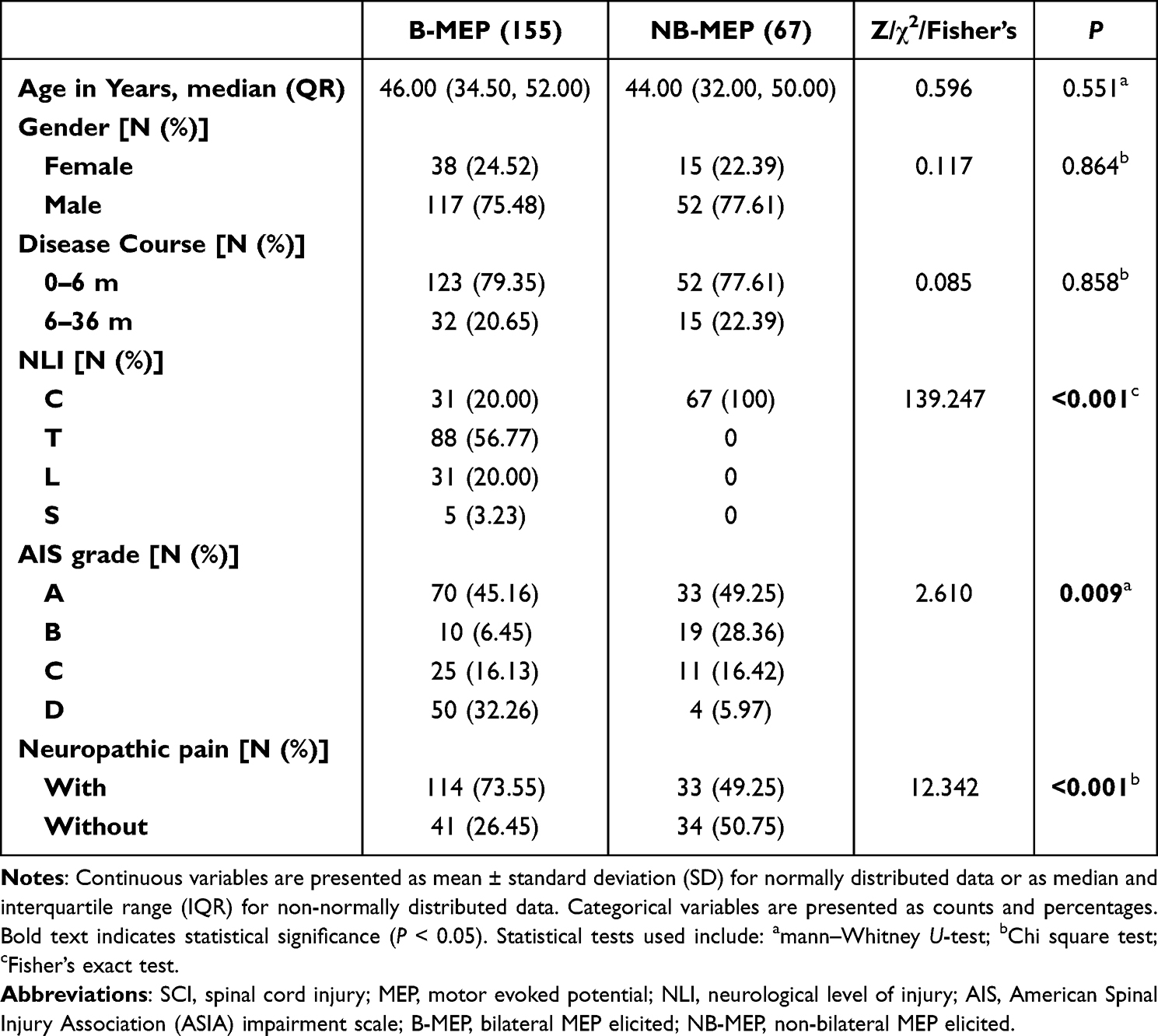 |
Table 1 Basic Characteristics of SCI Subgroup Patients with Tested M1 Hand Area MEP |
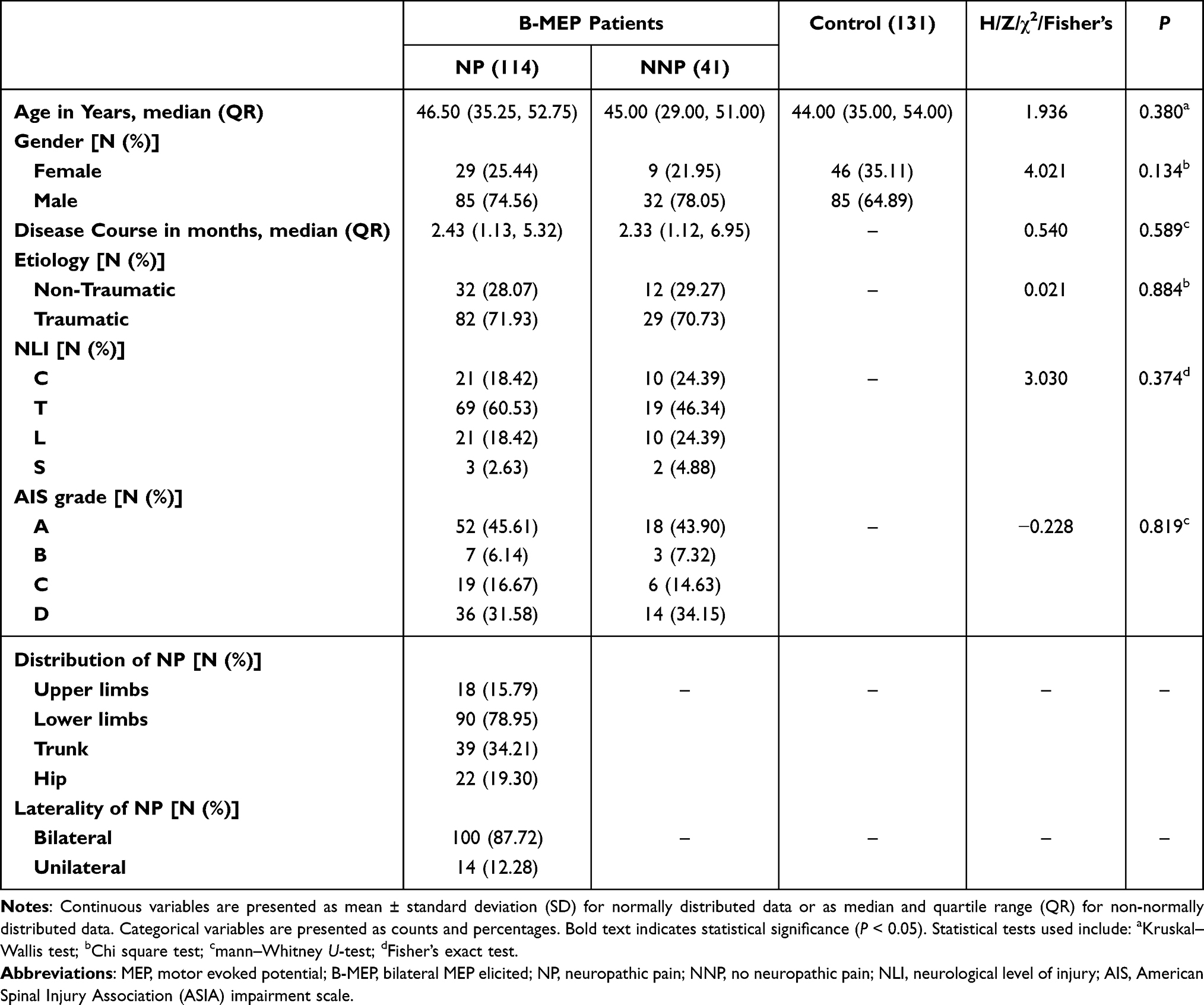 |
Table 2 Basic Characteristics of B-MEP Patients and Healthy Controls |
Comparison of M1 Hand Area MEPs Between Hemispheres in NP, NNP, and Healthy Control Groups
We analyzed MEP recordings to evaluate changes in CSE in the bilateral M1 hand areas of NP patients after SCI. Our study identified a reduction trend in MEP amplitudes from both hemispheres in NP patients relative to healthy controls. In the NP group, the MEP amplitude from the NDH M1 hand area was notably lower than that from the DH M1 hand area (P < 0.05). The NNP group showed no significant difference in MEP amplitude between the DH and NDH M1 hand areas (Figure 2A). Latency analysis revealed a notable delay in MEP onset from both hemispheres in NP patients relative to healthy controls (P < 0.001; Figure 2B). Figure 2C shows that CMCT did not significantly differ among the three groups.
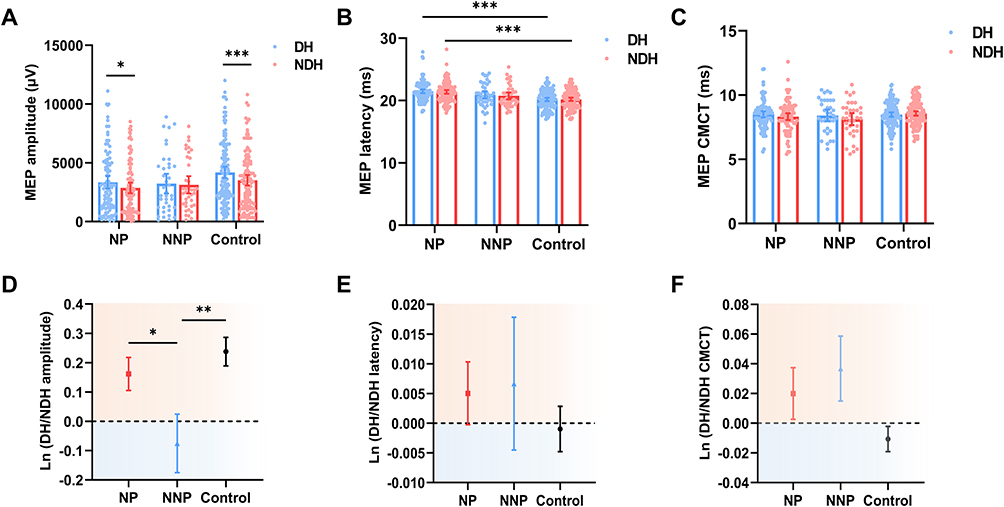 |
Figure 2 MEP Comparison of the M1 Hand Area Across Both Hemispheres in NP, NNP, and Healthy Control Groups. (A) Comparison of MEP amplitude between hemispheres in NP, NNP, and healthy control groups. In both healthy controls and the NP group, the MEP amplitude in the NDH M1 hand area was significantly smaller than in the DH M1 hand area. The NNP group showed no significant difference in MEP amplitude between the DH and NDH M1 hand areas. (B) Comparison of MEP latency between hemispheres in NP, NNP, and healthy control groups. The NP group exhibited a notable delay in bilateral M1 hand area MEP latency relative to healthy controls. (C) Comparison of MEP CMCT between hemispheres in NP, NNP, and healthy control groups. No significant differences were observed in M1 hand area MEP CMCT among the three groups. (D) Hemispheric CSE asymmetry was quantified by calculating the natural logarithm of the MEP amplitude ratio between the DH and NDH. The ln(DH/NDH amplitude) was 0.16±0.56 in NP patients, 0.24±0.55 in the control group, and −0.08±0.62 in NNP patients. The degree of hemispheric asymmetry was greater in the NP group compared to the NNP group. (E) Bilateral hemispheric differences in MEP latency in the M1 hand area were quantified by calculating the natural logarithm of the MEP latency ratio between DH and NDH. No significant differences were found in ln(DH/NDH latency) among the three groups. (F) Bilateral hemispheric differences in MEP CMCT in the M1 hand area were quantified by calculating the natural logarithm of the MEP CMCT ratio between DH and NDH. No significant differences were found in ln(DH/NDH CMCT) among the three groups. * P <0.05, ** P <0.01, *** P <0.001. Abbreviations: NP, neuropathic pain; NNP, no neuropathic pain; M1, primary motor cortex; CSE, corticospinal excitability; MEP, motor evoked potential; DH, dominant hemisphere; NDH, non-dominant hemisphere; CMCT, central motor conduction time. |
In NP patients, MEP amplitudes in the M1 hand area were significantly lower on the NDH side compared to the DH side, a difference not observed in NNP patients. The asymmetry was corroborated by a notable rise in the ln(DH/NDH amplitude), increasing from −0.08 ± 0.62 in NNP patients to 0.16 ± 0.56 in NP patients (Figure 2D). No significant differences were found in hemispheric MEP latency or CMCT (Figure 2E and F).
Correlation Between Hemispheric CSE Asymmetry and NP Course and Severity
Spearman correlation analyses were carried out to examine the connection between hemispheric M1 hand area CSE asymmetry and the progression and intensity of NP. A significant positive correlation was observed between ln(DH/NDH amplitude) and the NP course in NP patients (r = 0.213, P = 0.034; Figure 3A). The ln(DH/NDH amplitude) showed significant positive correlations with both the total SF-MPQ-2 score (SF-MPQ-2, r = 0.317, P = 0.004; Figure 3B) and its affective subscale (SF-MPQ-2-4, r = 0.294, P = 0.009; Figure 3C).
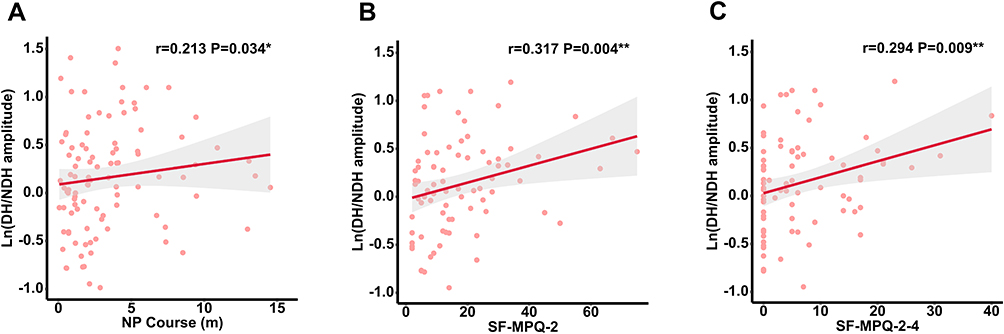 |
Figure 3 Correlation Between Hemispheric CSE Asymmetry and NP Duration and Severity Scores. (A) Correlation of hemispheric CSE asymmetry degree with NP course. A notable positive correlation was identified between the ln(DH/NDH amplitude) and NP duration (r=0.213). (B) Correlation of hemispheric CSE asymmetry degree with SF-MPQ-2 scores. A notable positive correlation was found between the ln(DH/NDH amplitude) and the SF-MPQ-2 score (r=0.317). (C) Correlation of hemispheric CSE asymmetry degree with SF-MPQ-2-4 scores. A notable positive correlation was noted between the ln(DH/NDH amplitude) and SF-MPQ-2-4 (r=0.294).* P <0.05, ** P <0.01. Abbreviations: NP, neuropathic pain; DH, dominant hemisphere; NDH, non-dominant hemisphere; CSE, corticospinal excitability; SF-MPQ-2, short-form McGill pain questionnaire-2; SF-MPQ-2-4, subscale 4 of SF-MPQ-2. |
Age Subgroup Analysis
In patients younger than 52, a positive correlation was found between the ln(DH/NDH amplitude) and NP course (r = 0.306, P = 0.010), SF-MPQ-2 (r = 0.300, P = 0.022), and SF-MPQ-2-4 (r = 0.310, P = 0.019). This trend was not significant in patients aged 52 or above (Figure 4A).
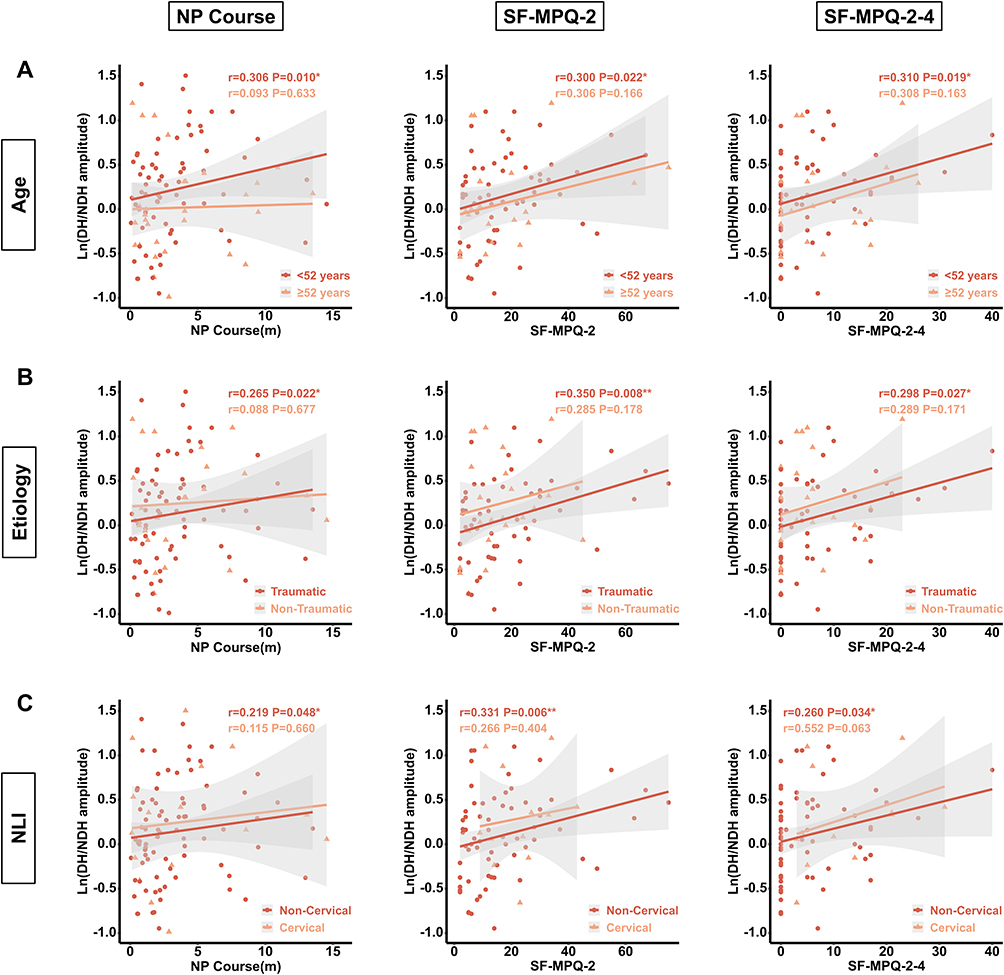 |
Figure 4 Correlation Between Hemispheric CSE Asymmetry and NP Course and Severity Scores in SCI Subgroups. (A) Correlation of hemispheric CSE asymmetry degree with NP course and severity scores in patients under 52 years of age. The ln(DH/NDH amplitude) showed a significant positive correlation with NP course (r = 0.306), SF-MPQ-2 (r = 0.300), and SF-MPQ-2-4 (r = 0.310). For patients aged 52 and above, there was no significant correlation between ln(DH/NDH amplitude) and NP course (r = 0.093), SF-MPQ-2 (r = 0.306), or SF-MPQ-2-4 (r = 0.308). (B) Correlation of hemispheric CSE asymmetry degree with NP course and severity scores in the traumatic SCI group. A significant positive correlation was observed between the ln(DH/NDH amplitude) and NP course (r = 0.265), SF-MPQ-2 (r = 0.350), and SF-MPQ-2-4 (r = 0.298). In the non-traumatic SCI group, no significant correlation was found between the ln(DH/NDH amplitude) and NP course (r = 0.088), SF-MPQ-2 (r = 0.285), or SF-MPQ-2-4 (r = 0.289). (C) Correlation of hemispheric CSE asymmetry degree with NP course and severity in the cervical injury group. The ln(DH/NDH amplitude) showed no significant correlation with NP course (r = 0.115), SF-MPQ-2 (r = 0.266), or SF-MPQ-2-4 (r = 0.552). In the non-cervical injury group, ln(DH/NDH amplitude) showed a significant positive correlation with NP course (r = 0.219), SF-MPQ-2 (r = 0.331), and SF-MPQ-2-4 (r = 0.260).* P <0.05, ** P <0.01. Abbreviations: SCI, spinal cord injury; NP, neuropathic pain; DH, dominant hemisphere; NDH, non-dominant hemisphere; CSE, corticospinal excitability; SF-MPQ-2, short-form McGill pain questionnaire-2; SF-MPQ-2-4, subscale 4 of SF-MPQ-2. |
Etiology Subgroup Analysis
The ln(DH/NDH amplitude) and NP course were significantly positively correlated in the traumatic SCI subgroup (r=0.265, P =0.022) but not in the non-traumatic SCI subgroup. In the traumatic SCI subgroup, ln(DH/NDH amplitude) showed a significant positive correlation with SF-MPQ-2 (r = 0.350, P = 0.008) and SF-MPQ-2-4 (r = 0.298, P = 0.027), whereas no such correlation was observed in the non-traumatic SCI subgroup (Figure 4B).
NLI Subgroup Analysis
A positive correlation was identified between ln(DH/NDH amplitude) and NP course (r = 0.219, P = 0.048), SF-MPQ-2 (r = 0.331, P = 0.006), and SF-MPQ-2-4 (r = 0.260, P = 0.034) in patients with non-cervical SCI. However, these correlations were not observed in the cervical SCI subgroup (Figure 4C).
Contribution of Hemispheric M1 Hand Area CSE Asymmetry to NP Severity
Univariate and multivariate linear regression analyses were performed using SF-MPQ-2 and SF-MPQ-2-4 scores as dependent variables to mitigate potential confounding factors. Univariate analysis revealed that hemispheric M1 hand area CSE asymmetry, NP course, and NLI significantly contributed to both outcomes (P < 0.10). However, multivariate analysis indicated that only hemispheric CSE asymmetry contributed significantly to both SF-MPQ-2 scores (unstandardized β = 7.085, P = 0.049) and SF-MPQ-2-4 scores (unstandardized β = 3.828, P = 0.045) (Table 3).
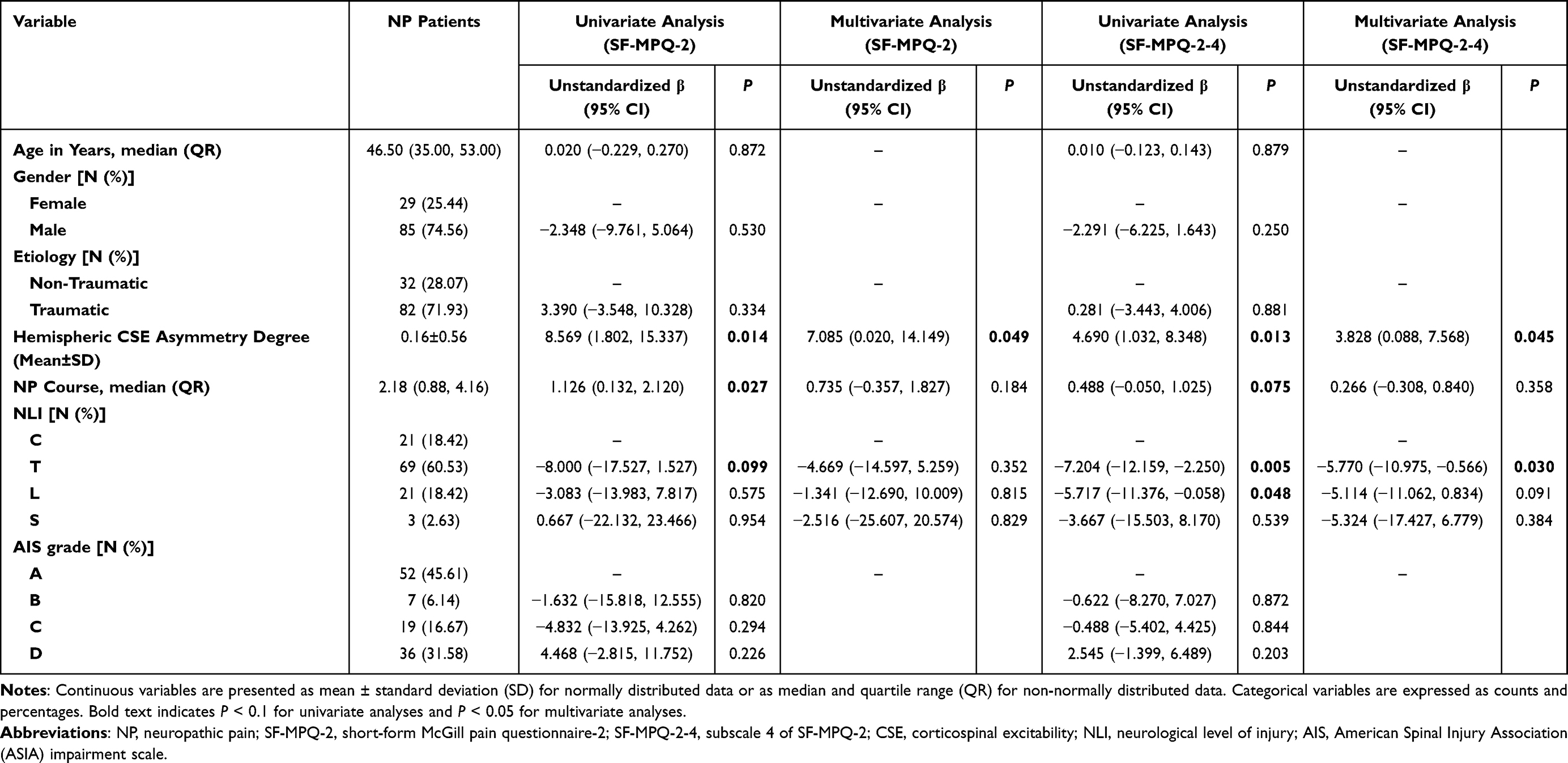 |
Table 3 Linear Regression Analysis of SF-MPQ-2 and SF-MPQ-2-4 |
Additional univariate and multivariate linear regression analyses focused on NP patients younger than 52 years with traumatic SCI occurring outside the cervical region. Univariate analysis within this specific subgroup disclosed a substantial association between the extent of hemispheric CSE asymmetry and scores of the SF-MPQ-2 (unstandardized β = 11.187, P = 0.014) and SF-MPQ-2-4 (unstandardized β = 5.787, P = 0.014) (Table 4). Compared to the broader analyses, the unstandardized β values demonstrated an increase of 2.618 for SF-MPQ-2 and by 1.097 for SF-MPQ-2-4, respectively.
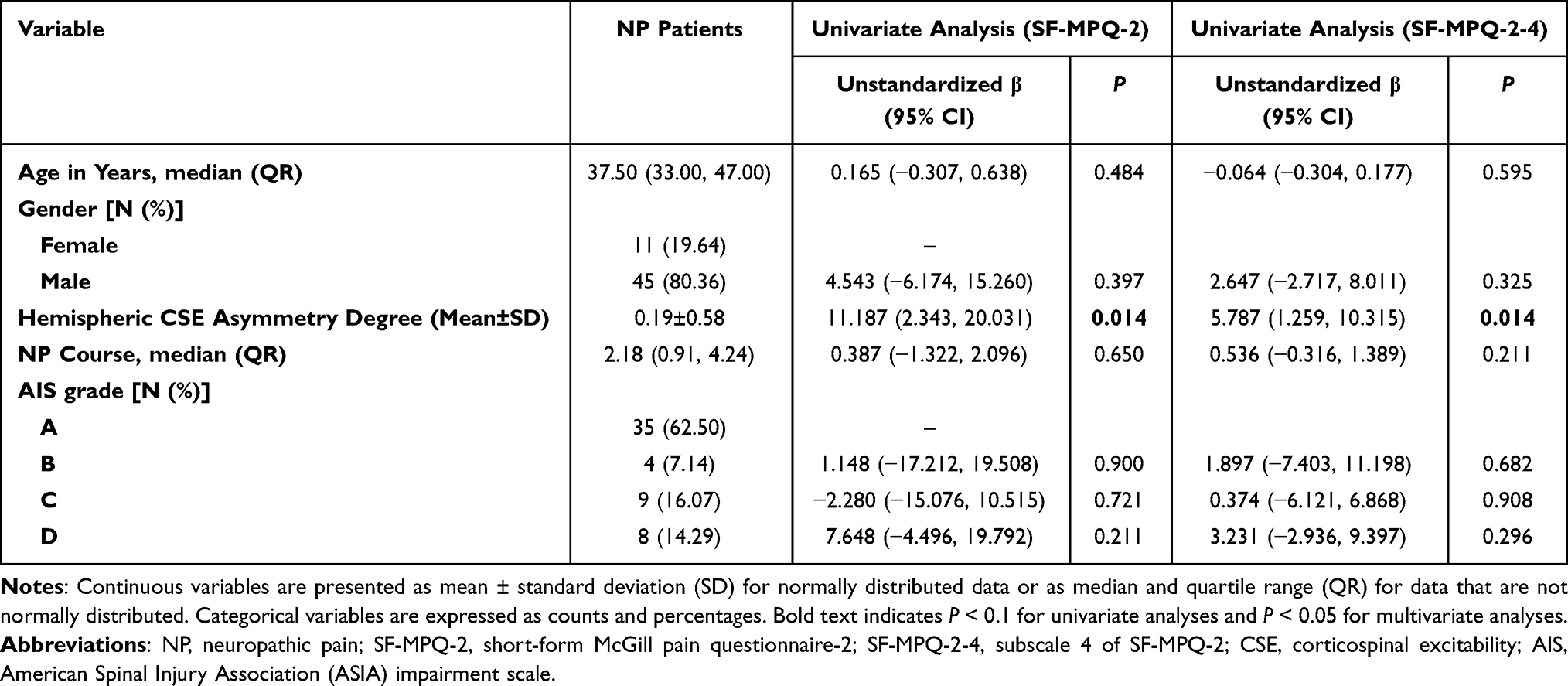 |
Table 4 Linear Regression Analysis of SF-MPQ-2 and SF-MPQ-2-4 in NP Patients Under 52 Years of Age, Traumatic, and Non-Cervical Injury After SCI |
Discussion
The study found that patients with bilateral NP after SCI showed reduced MEP amplitudes in the M1 hand areas compared to NNP patients, especially in the NDH. Additionally, increased hemispheric CSE asymmetry in NP patients correlated positively with NP severity, duration, and emotional disturbances. Multiple regression analysis identified hemispheric CSE asymmetry as an independent factor associated with NP severity and emotional disturbances, particularly in younger (under 52 years) traumatic non-cervical SCI patients. The results indicate that hemispheric CSE asymmetry could be a biomarker for SCI-NP, advocating for high-frequency rTMS targeting of bilateral M1 hand areas, particularly the NDH, as a therapeutic approach.
Our study established a significant link between bilateral M1 hand areas and SCI-NP. Patients with B-MEP exhibited a higher incidence of NP (73.55%) compared to those without (NB-MEP, 49.25%), suggesting a strong association between M1 activity and NP onset (P<0.001). Notably, a greater reduction in CSE was observed in the NDH among NP patients, suggesting that reduced NDH CSE plays a pivotal role in NP development. This finding aligns with Jutzeler et al, who reported that post-SCI NP development was linked to increased gray matter volume in the NDH M1, hypothesizing that this enhanced cortical connectivity may exacerbate pain transmission.33 Similarly, Galhardoni et al reported that patients with persistent idiopathic facial pain (PIFP) exhibited decreased MEP amplitudes and reduced short-interval intracortical inhibition (SICI) in both hemispheres, as noted by Schwenkreis et al found diminished intracortical inhibition (ICI) in both hemispheres in type I CRPS patients.34,35 Our study similarly found prolonged bilateral MEP latencies in patients with SCI-NP, suggesting that bilateral M1 alterations are physiologically linked to SCI-NP.
To account for inter-patient variability, we standardized MEP amplitudes across both hemispheres and introduced a metric for hemispheric CSE asymmetry. This metric was significantly higher in NP patients compared to NNP patients and positively correlated with both the duration and severity of NP. The results suggest that hemispheric CSE asymmetry may be a dependable biomarker for evaluating NP severity in SCI patients. Previous research indicated that high-frequency rTMS targeting the left M1 hand area offered analgesic effects, albeit with limited efficacy.15,16 The current study revealed reduced bilateral MEP amplitudes in SCI-NP patients and a positive correlation between hemispheric CSE asymmetry and SF-MPQ-2 scores. This indicates that diminished hemispheric CSE asymmetry could be associated with decreased NP intensity, emphasizing the potential of high-frequency rTMS targeting bilateral M1 hand areas, especially the NDH, as an innovative treatment for SCI-NP.
Current rTMS guidelines do not agree on the best M1 stimulation target for NP treatment.8 Some studies suggest targeting the cortical representation of the painful area, while others recommend the M1 hand area for its accessibility and broader analgesic effects.36,37 Our findings support the latter, showing significant changes in CSE and hemispheric asymmetry in the M1 hand area, even in SCI patients with lower limb NP. The M1 hand area likely plays a systemic role in pain modulation due to its extensive cortical and subcortical connections.38 Clinically, it is more accessible for targeting than lower-limb motor areas, making it a practical option for rTMS interventions.13
The revised pain definition by the International Association for the Study of Pain (IASP) highlights that neuropathic pain (NP) impacts both sensory and emotional aspects.39 The SF-MPQ-2, a prevalent tool in NP research, evaluates these dimensions comprehensively, offering more robust insights than single-dimension tools like the Numeric Rating Scale (NRS).30 Our study found a significant positive correlation between SF-MPQ-2 scores and hemispheric CSE asymmetry, with the affective subscale (SF-MPQ-2-4) showing the strongest correlation. This highlights the profound emotional burden that NP imposes on patients. This finding supports previous research indicating that NP impairs emotional regulation and stress coping, contributing to anxiety and depression.40 Emotional disturbances may worsen chronic pain via noradrenergic system dysfunction.41 Anxiety and depression prevalence in NP patients can reach 65.6% and 73.7%, respectively, significantly impacting their quality of life.42 The well-documented reciprocal relationship between chronic pain and emotional disorders highlights that emotional distress often intensifies pain perception, further harming emotional well-being.43 This emphasizes the need for early intervention addressing both the physical and emotional aspects of NP. High-frequency rTMS targeting the M1 area has been shown to alleviate both NP and co-occurring depression, reinforcing the need for integrated treatment strategies that address both aspects of SCI-NP.44
In our subgroup analysis, we found that younger patients (under 52 years), those with traumatic SCI, and those with non-cervical SCI exhibited more pronounced positive correlations between hemispheric CSE asymmetry and NP characteristics. This supports previous research indicating that cortical excitability and neuroplasticity decline with age, which may reduce the effectiveness of plasticity-based interventions such as rTMS in older adults.45,46 Moreover, the stronger correlation observed in traumatic SCI patients compared to non-traumatic SCI patients may reflect more predictable recovery patterns and consistent NP mechanisms in traumatic injuries. Notably, we observed a significant correlation between hemispheric CSE asymmetry and NP parameters in patients with non-cervical SCI, but no such relationship was found in those with cervical SCI. Direct damage to the CST in the M1 hand area in cervical SCI may compromise MEP pathway integrity, affecting the reliability of CSE measurements. Further subgroup analysis of younger, traumatic non-cervical SCI patients revealed a stronger correlation between hemispheric CSE asymmetry and both NP severity and emotional disturbances. These results suggest that hemispheric CSE asymmetry may be a particularly robust biomarker for assessing NP in this specific patient population, emphasizing the importance of considering injury location and patient demographics when developing personalized treatment strategies.
Previous studies have explored cortical excitability changes in patients with CNP. Hosomi et al investigated 21 patients with chronic post-stroke CNP and 8 healthy controls, finding higher RMT values in patients but no significant difference in MEP amplitudes.47 Similarly, Barbosa et al examined 93 stroke and 70 neuromyelitis optica (NMO) patients, including 74 with CNP, and found lower MEP amplitudes in brain injury-related CNP compared to non-neuropathic pain and no-pain groups.19 These findings indicate that changes in cortical excitability could serve as neurophysiological markers for the development of CNP. However, their findings are primarily based on stroke populations, limiting generalizability to SCI patients. Our study included 625 SCI patients and 131 healthy controls, representing the largest SCI patient population studied to date. Unlike Barbosa et al’s focus on NMO, our study covered a broader range of etiologies, including trauma, offering more clinical relevance.48 Additionally, our analysis was more comprehensive, incorporating stratified analyses based on age, etiology, and neurological level of injury (NLI). Given that SCI can lead to cortical excitability changes, we investigated differences in cortical excitability among NP, NNP, and healthy control groups, controlling for SCI-induced alterations.49 To address individual variability in SCI outcomes, we further compared excitability between hemispheres.50 This is the first study to conduct such analyses in SCI patients with NP.
This study has certain limitations. While 625 patients were enrolled, only about a quarter had complete and analyzable MEP data for both M1 hand areas. Larger sample sizes of SCI patients with NP and NNP are needed to validate the findings on hemispheric CSE asymmetry. Prospective cohort studies are essential to further explore the relationship between CSE asymmetry and NP severity. Our findings indicate that bilateral high-frequency rTMS applied to M1 hand area may reduce neuropathic pain by correcting imbalances in CSE. Future double-blind randomized controlled trials (RCTs) should compare unilateral and bilateral approaches, using CSE measurements to personalize treatment parameters (eg, targeting specific brain hemispheres or adjusting stimulation frequency). Although MEP measurements assessed hemispheric excitability asymmetry, methods like paired-pulse TMS (ppTMS) and functional near-infrared spectroscopy (fNIRS) could offer a more comprehensive evaluation of cortical excitability changes.15,51
Conclusions
In summary, this study demonstrates that SCI patients with bilateral NP exhibit reduced CSE in the NDH M1 hand area. Hemispheric CSE asymmetry is linked to pain severity and emotional disturbances in NP patients, suggesting it may serve as a candidate biomarker for objective NP assessment. The observed CSE changes in both M1 hand areas also indicate that these regions could be effective therapeutic targets for high-frequency stimulation in SCI patients with NP. Timely identification and intervention for NP, along with suitable psychological support, may alleviate pain and enhance quality of life in specific patient groups. These findings propose new avenues for NP assessment and treatment, with promising clinical implications.
Abbreviations
SCI, spinal cord injury; NP, neuropathic pain; NNP, no neuropathic pain; IASP, International Association for the Study of Pain; TMS, transcranial magnetic stimulation; rTMS, repetitive transcranial magnetic stimulation; M1, primary motor cortex; CSE, corticospinal excitability; CST, corticospinal tract; MEP, motor evoked potential; DH, dominant hemisphere; NDH, non-dominant hemisphere; SF-MPQ-2, short-form McGill pain questionnaire-2; AIS, American Spinal Injury Association (ASIA) impairment scale; NLI, neurological level of injury; CMCT, central motor conduction time; ICI, cortical intracortical inhibition; SICI, short-interval intracortical inhibition; ICF, intracortical facilitation; RMT, resting motor threshold; SD, standard deviation; QR, quartile range; ROC, receiver operating characteristic; PIFP, persistent idiopathic facial pain; CRPS, complex regional pain syndrome; CNP, central neuropathic pain; ppTMS, paired-pulse TMS; fNIRS, functional near-infrared spectroscopy; NRS, Numeric Rating Scale; NMO, neuromyelitis optica.
Data Sharing Statement
For additional details, please reach out to the corresponding author. The datasets analyzed in this study can be obtained from the corresponding author upon reasonable request.
Ethics Statement
The present study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Air Force Medical University of Chinese People’s Liberation Army (No. KY20222096-C-1) and registered in the Chinese Clinical Trial Registry (ChiCTR2300073824). Due to the retrospective nature of this study, informed consent was waived as it would not adversely affect the rights and welfare of the subjects, and it was objectively impossible to obtain informed consent from the subjects.
Acknowledgments
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com). We thank the Home for Researchers (www.home-for-researchers.com) for their help with language.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the National Natural Science Foundation of China (82472593, 82272591, and 82072534), and the Medical Staff Training & Boost Project of Xijing Hospital (XJZT24JC19, XJZT24LY11, XJZT24QN20).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. McDonald JW, Sadowsky C. Spinal-cord injury. Lancet. 2002;359(9304):417–425. doi:10.1016/S0140-6736(02)07603-1
2. Adriaansen JJ, Post MW, de Groot S, et al. Secondary health conditions in persons with spinal cord injury: a longitudinal study from one to five years post-discharge. J Rehabil Med. 2013;45(10):1016–1022. doi:10.2340/16501977-1207
3. Schaefer C, Sadosky A, Mann R, et al. Pain severity and the economic burden of neuropathic pain in the United States: BEAT Neuropathic Pain Observational Study. Clinicoecon Outcomes Res. 2014;6:483–496. doi:10.2147/CEOR.S63323
4. Colloca L, Ludman T, Bouhassira D, et al. Neuropathic pain. Nat Rev Dis Primers. 2017;3:17002. doi:10.1038/nrdp.2017.2
5. Bannister K, Sachau J, Baron R, Dickenson AH. Neuropathic pain: mechanism-based therapeutics. Annu Rev Pharmacol Toxicol. 2020;60:257–274.
6. Evoy KE, Sadrameli S, Contreras J, Covvey JR, Peckham AM, Morrison MD. Abuse and misuse of pregabalin and gabapentin: a systematic review update. Drugs. 2021;81(1):125–156. doi:10.1007/s40265-020-01432-7
7. Chiang MC, Hsueh HW, Yeh TY, et al. Maladaptive motor cortical excitability and connectivity in polyneuropathy with neuropathic pain. Eur J Neurol. 2022;29(5):1465–1476. doi:10.1111/ene.15247
8. Lefaucheur JP, Aleman A, Baeken C, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): an update (2014–2018). Clin Neurophysiol. 2020;131(2):474–528.
9. Rosner J, Lutolf R, Hostettler P, et al. Assessment of neuropathic pain after spinal cord injury using quantitative pain drawings. Spinal Cord. 2021;59(5):529–537. doi:10.1038/s41393-021-00616-6
10. Kong ST, Yeo D, Neo EJ, Chen D. Bilateral upper limb complex regional pain syndrome (Type 2) in cervical spinal cord injury: a case report. Cureus. 2022;14(6):e26440. doi:10.7759/cureus.26440
11. Jette F, Cote I, Meziane HB, Mercier C. Effect of single-session repetitive transcranial magnetic stimulation applied over the hand versus leg motor area on pain after spinal cord injury. Neurorehabil Neural Repair. 2013;27(7):636–643. doi:10.1177/1545968313484810
12. Defrin R, Grunhaus L, Zamir D, Zeilig G. The effect of a series of repetitive transcranial magnetic stimulations of the motor cortex on central pain after spinal cord injury. Arch Phys Med Rehabil. 2007;88(12):1574–1580. doi:10.1016/j.apmr.2007.07.025
13. Kesar TM, Stinear JW, Wolf SL. The use of transcranial magnetic stimulation to evaluate cortical excitability of lower limb musculature: challenges and opportunities. Restor Neurol Neurosci. 2018;36(3):333–348. doi:10.3233/RNN-170801
14. Groppa S, Oliviero A, Eisen A, et al. A practical guide to diagnostic transcranial magnetic stimulation: report of an IFCN committee. Clin Neurophysiol. 2012;123(5):858–882. doi:10.1016/j.clinph.2012.01.010
15. Sun X, Long H, Zhao C, et al. Analgesia-enhancing effects of repetitive transcranial magnetic stimulation on neuropathic pain after spinal cord injury:An fNIRS study. Restor Neurol Neurosci. 2019;37(5):497–507. doi:10.3233/RNN-190934
16. Zhao CG, Sun W, Ju F, et al. Analgesic effects of directed repetitive transcranial magnetic stimulation in acute neuropathic pain after spinal cord injury. Pain Med. 2020;21(6):1216–1223. doi:10.1093/pm/pnz290
17. Pozdniakov I, Vorobiova AN, Galli G, Rossi S, Feurra M. Online and offline effects of transcranial alternating current stimulation of the primary motor cortex. Sci Rep. 2021;11(1):3854. doi:10.1038/s41598-021-83449-w
18. Krause P, Forderreuther S, Straube A. TMS motor cortical brain mapping in patients with complex regional pain syndrome type I. Clin Neurophysiol. 2006;117(1):169–176. doi:10.1016/j.clinph.2005.09.012
19. Barbosa LM, Valerio F, da Silva VA, et al. Corticomotor excitability is altered in central neuropathic pain compared with non-neuropathic pain or pain-free patients. Neurophysiol Clin. 2023;53(3):102845. doi:10.1016/j.neucli.2023.102845
20. Mori N, Hosomi K, Nishi A, Oshino S, Kishima H, Saitoh Y. Analgesic effects of repetitive transcranial magnetic stimulation at different stimulus parameters for neuropathic pain: a randomized study. Neuromodulation. 2022;25(4):520–527. doi:10.1111/ner.13328
21. Matsuoka H, Iwase S, Miyaji T, et al. Predictors of duloxetine response in patients with neuropathic cancer pain: a secondary analysis of a randomized controlled trial-JORTC-PAL08 (DIRECT) study. Support Care Cancer. 2020;28(6):2931–2939. doi:10.1007/s00520-019-05138-9
22. Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia. 1971;9(1):97–113. doi:10.1016/0028-3932(71)90067-4
23. Rupp R, Biering-Sorensen F, Burns SP, et al. International standards for neurological classification of spinal cord injury: revised 2019. Top Spinal Cord Inj Rehabil. 2021;27(2):1–22. doi:10.46292/sci2702-1
24. Oyama K, Hu L, Sakatani K. Prediction of MMSE score using time-resolved near-infrared spectroscopy. Adv Exp Med Biol. 2018;1072:145–150.
25. Bryce TN, Biering-Sorensen F, Finnerup NB, et al. International spinal cord injury pain classification: part I. Background and description. Spinal Cord. 2012;50(6):413–417. doi:10.1038/sc.2011.156
26. Ziemann U, Reis J, Schwenkreis P, et al. TMS and drugs revisited 2014. Clin Neurophysiol. 2015;126(10):1847–1868. doi:10.1016/j.clinph.2014.08.028
27. Dai C, Lin X, Xue B, et al. Correlation of bilateral M1 hand area excitability and overall functional recovery after spinal cord injury: protocol for a prospective cohort study. BMC Neurol. 2024;24(1):213. doi:10.1186/s12883-024-03705-0
28. Long J, Federico P, Perez MA. A novel cortical target to enhance hand motor output in humans with spinal cord injury. Brain. 2017;140(6):1619–1632. doi:10.1093/brain/awx102
29. Dai CQ, Gao M, Lin XD, et al. Primary motor hand area corticospinal excitability indicates overall functional recovery after spinal cord injury. Front Neurol. 2023;14:1175078. doi:10.3389/fneur.2023.1175078
30. Dworkin RH, Turk DC, Revicki DA, et al. Development and initial validation of an expanded and revised version of the Short-form McGill Pain Questionnaire (SF-MPQ-2). Pain. 2009;144(1–2):35–42. doi:10.1016/j.pain.2009.02.007
31. Tang X, Huang P, Li Y, et al. Age-related changes in the plasticity of neural networks assessed by transcranial magnetic stimulation with electromyography: a systematic review and meta-analysis. Front Cell Neurosci. 2019;13:469. doi:10.3389/fncel.2019.00469
32. Gruener H, Zeilig G, Gaidukov E, et al. Biomarkers for predicting central neuropathic pain occurrence and severity after spinal cord injury: results of a long-term longitudinal study. Pain. 2020;161(3):545–556. doi:10.1097/j.pain.0000000000001740
33. Jutzeler CR, Huber E, Callaghan MF, et al. Association of pain and CNS structural changes after spinal cord injury. Sci Rep. 2016;6:18534. doi:10.1038/srep18534
34. Galhardoni R, Ciampi de Andrade D, Puerta MY, et al. Altered cortical excitability in persistent idiopathic facial pain. Cephalalgia. 2019;39(2):219–228. doi:10.1177/0333102418780426
35. Schwenkreis P, Janssen F, Rommel O, et al. Bilateral motor cortex disinhibition in complex regional pain syndrome (CRPS) type I of the hand. Neurology. 2003;61(4):515–519. doi:10.1212/WNL.61.4.515
36. Ayache SS, Ahdab R, Chalah MA, et al. Analgesic effects of navigated motor cortex rTMS in patients with chronic neuropathic pain. Eur J Pain. 2016;20(9):1413–1422. doi:10.1002/ejp.864
37. Andre-Obadia N, Magnin M, Simon E, Garcia-Larrea L. Somatotopic effects of rTMS in neuropathic pain? A comparison between stimulation over hand and face motor areas. Eur J Pain. 2018;22(4):707–715. doi:10.1002/ejp.1156
38. Willett FR, Deo DR, Avansino DT, et al. Hand knob area of premotor cortex represents the whole body in a compositional way. Cell. 2020;181(2):396–409e326. doi:10.1016/j.cell.2020.02.043
39. Raja SN, Carr DB, Cohen M, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
40. Alba-Delgado C, Llorca-Torralba M, Horrillo I, et al. Chronic pain leads to concomitant noradrenergic impairment and mood disorders. Biol Psychiatry. 2013;73(1):54–62. doi:10.1016/j.biopsych.2012.06.033
41. Gonzalez-Sepulveda M, Pozo OJ, Marcos J, Valverde O. Chronic pain causes a persistent anxiety state leading to increased ethanol intake in CD1 mice. J Psychopharmacol. 2016;30(2):188–203. doi:10.1177/0269881115622238
42. Cherif F, Zouari HG, Cherif W, Hadded M, Cheour M, Damak R. Depression prevalence in neuropathic pain and its impact on the quality of life. Pain Res Manag. 2020;2020:7408508. doi:10.1155/2020/7408508
43. Luo A, Wu Z, Li S, et al. The soluble epoxide hydrolase inhibitor TPPU improves comorbidity of chronic pain and depression via the AHR and TSPO signaling. J Transl Med. 2023;21(1):71. doi:10.1186/s12967-023-03917-x
44. Gayduk AJ, Shishkovskaia TI, Cumming P, et al. Association between neuropathic pain and depression: focusing on the transcranial magnetic stimulation as a promising treatment approach. Psychiatry Danub. 2022;34(Suppl 8):105–111.
45. Antonenko D, Nierhaus T, Meinzer M, et al. Age-dependent effects of brain stimulation on network centrality. Neuroimage. 2018;176:71–82. doi:10.1016/j.neuroimage.2018.04.038
46. Ghasemian-Shirvan E, Farnad L, Mosayebi-Samani M, et al. Age-related differences of motor cortex plasticity in adults: a transcranial direct current stimulation study. Brain Stimul. 2020;13(6):1588–1599. doi:10.1016/j.brs.2020.09.004
47. Hosomi K, Kishima H, Oshino S, et al. Cortical excitability changes after high-frequency repetitive transcranial magnetic stimulation for central poststroke pain. Pain. 2013;154(8):1352–1357. doi:10.1016/j.pain.2013.04.017
48. Wu SY, Jiang YH, Jhang JF, Hsu YH, Ho HC, Kuo HC. Inflammation and barrier function deficits in the bladder urothelium of patients with chronic spinal cord injury and recurrent urinary tract infections. Biomedicines. 2022;10(2):220.
49. Nardone R, Holler Y, Brigo F, et al. Descending motor pathways and cortical physiology after spinal cord injury assessed by transcranial magnetic stimulation: a systematic review. Brain Res. 2015;1619:139–154.
50. Ahuja CS, Nori S, Tetreault L, et al. Traumatic spinal cord injury-repair and regeneration. Neurosurgery. 2017;80(3S):S9–S22. doi:10.1093/neuros/nyw080
51. Han T, Dai C, Liang Y, et al. PFC/M1 activation and excitability: a longitudinal cohort study on fatigue symptoms in healthcare workers post-COVID-19. J Transl Med. 2024;22(1):720. doi:10.1186/s12967-024-05319-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Complement Receptor 3 Pathway and NMDA Receptor 2B Subunit Involve Neuropathic Pain Associated with Spinal Cord Injury
Li Y, Fang SC, Zhou L, Mo XM, Guo HD, Deng YB, Yu HH, Gong WY
Journal of Pain Research 2022, 15:1813-1823
Published Date: 25 June 2022
Cerium Oxide Nanoparticles Alleviate Neuropathic Pain by Modulating Macrophage Polarization in a Rat SCI Model
Ban D, Yu H, Xiang Z, Li C, Yu P, Wang J, Liu Y
Journal of Pain Research 2022, 15:3369-3380
Published Date: 25 October 2022
Non-Coding RNAs Regulate Spinal Cord Injury-Related Neuropathic Pain via Neuroinflammation
Zhu J, Huang F, Hu Y, Qiao W, Guan Y, Zhang ZJ, Liu S, Liu Y
Journal of Inflammation Research 2023, 16:2477-2489
Published Date: 13 June 2023
A Silver Lining of Neuropathic Pain: Predicting Favorable Functional Outcome in Spinal Cord Injury
Xu ML, Wu XB, Liang Y, Li N, Hu X, Lin XD, Sun MQ, Dai CQ, Niu D, Zhang YR, Cao H, Zhao CG, Sun XL, Yuan H
Journal of Pain Research 2023, 16:2619-2632
Published Date: 27 July 2023