Back to Journals » Journal of Inflammation Research » Volume 19
Correlation of Omentin-1 with Disease Extent and Therapeutic Response to Infliximab in Ulcerative Colitis
Authors Chen C ![]() , Wang J, Wang T
, Wang J, Wang T ![]() , Zhou Z, Gao C, Pan Y, He C
, Zhou Z, Gao C, Pan Y, He C
Received 15 January 2026
Accepted for publication 26 May 2026
Published 11 June 2026 Volume 2026:19 593807
DOI https://doi.org/10.2147/JIR.S593807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Syed Adeel Hassan
Chen Chen,1,2 Jinxia Wang,1 Tingting Wang,1,2 Zhou Zhou,2 Caiping Gao,1,2 Yan Pan,2 Chong He1,2
1Translational Clinical Immunology Key Laboratory of Sichuan Province, Sichuan Provincial People’s Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, Sichuan, People’s Republic of China; 2Department of Gastroenterology, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu, Sichuan, People’s Republic of China
Correspondence: Chong He, Email [email protected] Yan Pan, Email [email protected]
Background: Ulcerative colitis (UC) is classified by both activity and extent. Accumulating evidence suggests that disease extent is an independent factor in determining poor prognosis. However, there is a significant lack of blood biomarkers that mirror lesion reach, clinicians still rely on repeated endoscopy to determine disease activity and mucosal healing. Omentin-1 is an adipokine secreted mainly by visceral adipose tissue and intestinal goblet cells that has been reported to exert anti-inflammatory and epithelial-barrier-enhancing effects. Therefore, we hypothesized that serum omentin-1 correlates with disease extent and predicts primary response to infliximab (IFX).
Methods: Consecutive UC patients (n = 126) were enrolled and stratified by Montreal classification into distal (E1/E2, n = 84) or extensive (E3, n = 42) disease. Serum omentin-1 was quantified by ELISA. Clinical activity (partial Mayo) and endoscopic activity (MES) were recorded. Among 36 subjects who received standard IFX induction, response was assessed at week 14.
Results: Among the 126 UC patients, serum omentin-1 levels were significantly lower in extensive than distal colitis [median: 48.60 (38.28– 67.35) ng/mL vs 62.70 (58.48– 73.88) ng/mL, p < 0.01]. By controlling for clinical and endoscopic activity scores between groups, we found that serum omentin-1 levels differed between patients with different UC disease extents at the same level of disease activity, suggesting that serum omentin-1 can effectively predict the disease extent of UC independently of disease activity. In the IFX cohort (n = 36), responders (n = 23) exhibited higher baseline serum omentin-1 than non-responders. Extent-stratified analysis revealed that the discriminative capacity was confined to extensive colitis, with no significant predictive value in distal disease.
Conclusion: Serum omentin-1 quantifies UC extent independently of activity and predicts IFX response specifically in extensive colitis, offering a blood-based tool to map disease extent and guide biologic therapy. This finding may reduce the reliance on repeated colonoscopy and support therapeutic stratification in extensive disease.
Keywords: ulcerative colitis, inflammatory bowel disease, omentin-1, disease extent, infliximab
Introduction
Ulcerative colitis (UC) is one of the two major clinical subtypes of inflammatory bowel disease (IBD) and is characterized by continuous, superficial inflammation that begins in the rectum and may extend proximally. The condition follows a relapsing–remitting course and can culminate in life-threatening complications such as massive haemorrhage, toxic megacolon, and colitis-associated cancer.1,2 Over the past two decades its global incidence has risen steeply, yet the etiology remains elusive and curative therapy is still unavailable, prompting intensive efforts to identify biomarkers and therapeutic targets that can modify its natural history.3
UC is traditionally classified by both disease activity—the intensity of mucosal inflammation at a given time point—and disease extent, ie., the continuous segment of colon that is macroscopically involved. UC extent is classified using the Montreal classification: proctitis, left-sided, extensive; and can only be reliably determined by invasive colonoscopy.4 Studies have shown that the extent of UC is not only potentially associated with disease severity and long-term prognosis, but also holds significant clinical importance for identifying high-risk patients and guiding individualized treatment strategies (such as the appropriate selection of biologics).5,6 However, disease activity and extent do not necessarily parallel each other. Accumulating evidence indicates that extent is an independent driver of hard outcomes—hospitalization, colectomy, colorectal neoplasia—yet biomarkers that specifically mirror anatomical spread are lacking.7 Consequently, clinicians still rely on repeated endoscopy to document extension or remission of disease, a practice that is costly, uncomfortable and carries procedural risk.
Biomarkers for IBD can help monitor the clinical activity of the disease. Currently, blood and stool tests, such as C-reactive protein (CRP) and fecal calprotectin, are commonly used in clinical practice to assess inflammation levels and treatment efficacy. Most of the currently available biomarkers actually deliver suboptimal performance. In contrast, endoscopy remains the most effective tool for evaluating inflammatory activity in IBD, with the key advantage of being able to localize the site of disease involvement. However, due to its invasiveness, its clinical application is limited. Therefore, to achieve better management of IBD, there is an urgent need to identify reliable, non-invasive, and cost-effective biomarkers that are also easily accessible. Omentin-1 (also termed intelectin-1) is an adipokine secreted mainly by visceral adipose tissue and intestinal goblet cells that exerts anti-inflammatory and epithelial-barrier–enhancing effects.8 Its serum level is typically reduced in obesity and metabolic syndrome,9 but its behaviour in IBD has been scantily explored. Our earlier case–control study in which serum omentin-1 was already shown to be lower in UC versus controls and to correlate with both clinical and endoscopic disease activity, as well as with mucosal healing.10 However, it remains unknown whether omentin-1 acts as a potential “extent-specific” serum biomarker that could non-invasively map disease distribution and refine risk stratification.
Here, we compared serum omentin-1 between distal (E1/E2) and extensive (E3) colitis in 126 UC patients and tested whether baseline levels predict infliximab response within each extent group. By scanning omentin-1 across the full disease extent, this study aim to provide further insight into the clinical value of serum omentin-1 in UC, thereby offering the prospect of fewer repeat colonoscopies and a more measured path to personalized, burden-matched care.
Methods
Ethical Considerations
The protocol of this study was approved by the Institutional Review Board for Clinical Research of Sichuan Provincial People’s Hospital, which was in accordance with the Declaration of Helsinki. Written informed consent were obtained from all participants enrolled.
Participants
Consecutive adults aged 18–70 years old were recruited from the Gastroenterology department of Sichuan Provincial People’s Hospital. As reported previously,11–13 diagnosis of ulcerative colitis was established by integrating symptom history, laboratory markers, radiological examinations, as well as colonoscopic and histopathological confirmation. Clinical disease intensity was quantified using the Partial Mayo Score (p-Mayo, range 0–9),14 which records stool frequency, rectal bleeding, and physician global assessment; scores were interpreted as remission (≤ 2), mild (3–4), moderate (5–6), or severe (7–9). Disease extent was determined by colonoscopy and classified according to the Montreal system: E1 (proctitis) when erythema, friability, or ulceration was confined to the rectum; E2 (left-sided colitis) when inflammation extended continuously from the rectum to the sigmoid and/or descending colon but stopped distal to the splenic flexure; and E3 (extensive colitis) when mucosal changes continued proximal to the splenic flexure, including the transverse and/or ascending colon. Endoscopic severity within each segment was graded with the four-point Mayo Endoscopic Score (MES, 0–3),15 with 0 indicating normal mucosa and 3 denoting spontaneous bleeding or deep ulceration. Patients starting standard IFX induction (5 mg kg−1, weeks 0-2-6) were followed. Patients with complete, partial response or primary non-response were defined by the physician’s assessment of symptoms at week 12–14 after initial administration.12
Serum Collection and Omentin-1 Measurement
As reported previously,10 venous blood samples from all patients were collected in the morning on the day of colonoscopy, immediately centrifuged, aliquoted into cryotubes, and stored at –80 °C within 30 min. Samples were thawed only once immediately before the assay. Measurement of serum Omentin-1 levels was performed using a commercially available enzyme-linked immunosorbent assay (ELISA) kit (BlueGene Biotech Co., Shanghai, China) according to the manufacturer’s instructions. Technicians were blinded to clinical data and endoscopic reports.
Statistics
The statistical analysis was performed using a Prism software Version 8.4 (Graphpad Software, San Diego, California, USA). Normality was checked by Shapiro–Wilk; Comparisons of participants’ characteristics between the two groups and comparisons of omentin-1 levels between the distal colitis and extensive colitis groups were performed using chi-squared tests for categorical variables and the Mann–Whitney test for continuous variables when the assumptions for the t-test were not met. The efficacy of serum omentin-1 in distinguishing different subgroups was assessed using ROC curves, and the area under the ROC curve (AUC) was used to evaluate the diagnostic accuracy of the test. p < 0.05 was considered statistically significant.
Results
Characteristics of the Participants
The characteristics of this study participants are detailed in Table 1. This study included 126 patients with UC. We categorized patients with UC into subgroups based on the disease extent: proctitis (E1, n = 35), left-sided colitis (E2, n = 49), extensive colitis (E3, n = 42). There were no statistically significant differences in age, gender, or body mass index (BMI) among the three groups. However, disease activity was significantly higher in the extensive colitis (E3) group, with both p-Mayo scores (5.1±3.1) and Mayo endoscopic scores (MES, 2.1±1.2) being significantly elevated compared to the other two groups (p = 0.0031 and p = 0.0057, respectively), indicating more severe disease activity in this subgroup.
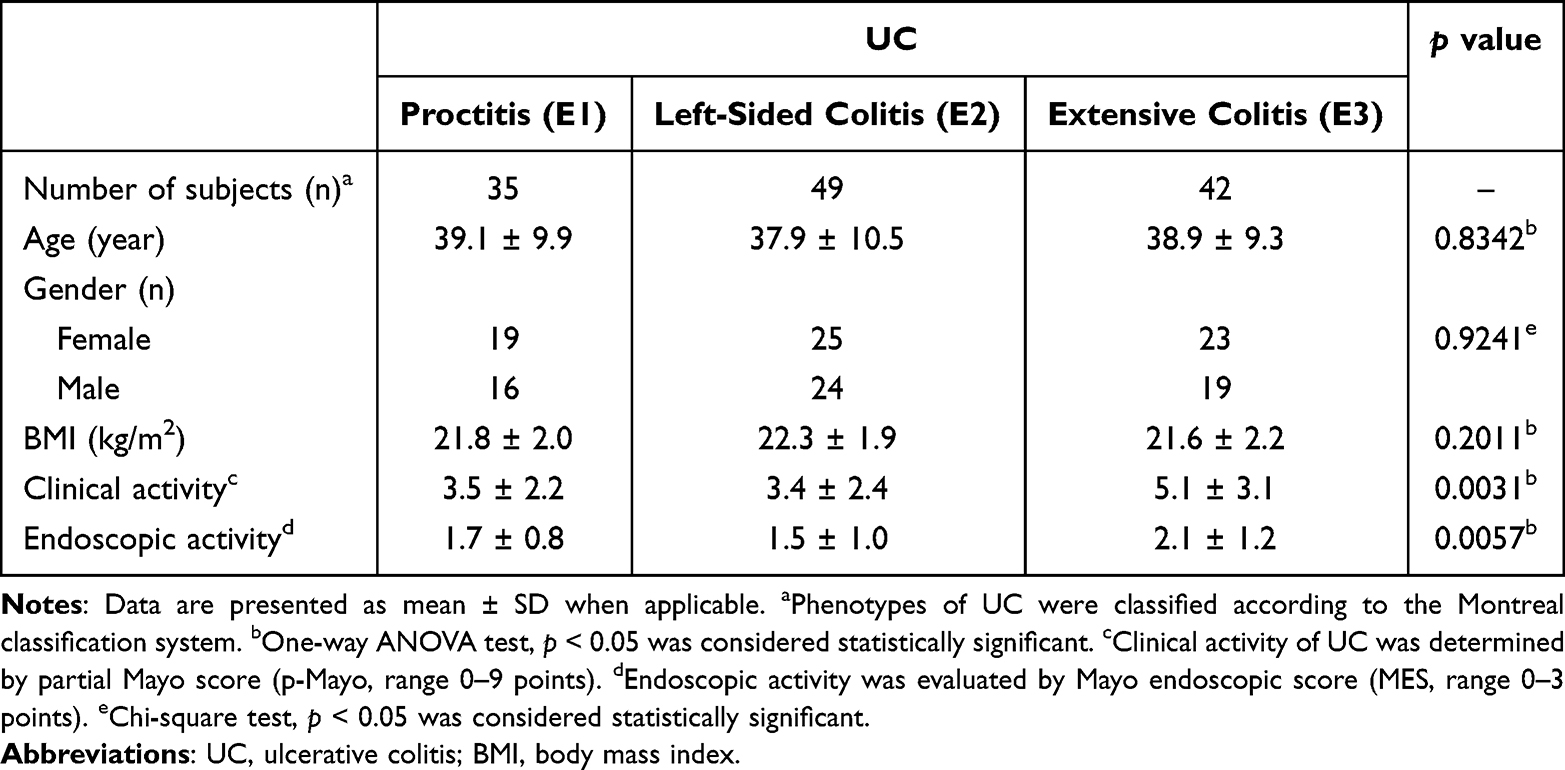 |
Table 1 Clinical Characteristics of UC Patients |
Serum Omentin-1 Levels Differ by Disease Extent
Recently, we confirmed that serum omentin-1 is significantly reduced in UC relative to healthy controls.10 The next question was whether this reduction is linked to disease extent. To address this, we stratified the enrolled patients according to UC lesion location into two groups: distal colitis (Montreal E1/E2) and extensive colitis (E3). Comparison of serum omentin-1 levels between the two groups revealed that the extensive-colitis cohort had significantly lower values than the distal-colitis cohort (Figure 1), hinting that omentin-1 levels reflects the lesion sites rather than simply offering a generic read-out of inflammation intensity.
 |
Figure 1 Serum omentin-1 levels differ by disease extent. Serum omentin-1 was quantified by ELISA. Patients were stratified by lesion location: distal colitis (Montreal E1/E2, n = 84) and extensive colitis (E3, n = 42). Each dot represents an individual subject. The Mann–Whitney test. |
Serum Omentin-1 Differs Between Distal and Extensive Colitis at Matched Clinical Activity
It should be noted that the distal-colitis and extensive-colitis groups in this cohort differed significantly in clinical activity (Supplementary Figure 1A). Because we had previously found serum omentin-1 to be negatively correlated with clinical activity,10 we re-stratified patients by activity grade to remove this potential bias. As shown in Figure 2A, omentin-1 levels in clinically active patients remained markedly lower in the extensive-colitis group than in the distal-colitis group, whereas no such difference was observed in the clinically inactive cohort (Figure 2B). Further subdivision of the clinically active subset into mildly–moderately active (Figure 2C) and severely active (Figure 2D) yielded the same observation, underscoring that omentin-1 levels reflects disease extent rather than symptom intensity alone.
 |
Figure 2 Serum omentin-1 differs between distal and extensive colitis at matched clinical activity. Clinical activity stratification: patients were classified as (A) clinically active (p-Mayo ≥ 3) or (B) clinically inactive (p-Mayo ≤ 2). Active subgroup divided into (C) mildly–moderately active (p-Mayo 3–6) and (D) severely active (p-Mayo ≥ 7). Serum omentin-1 was quantified by ELISA. ns = no significance, The Mann–Whitney test. |
Serum Omentin-1 Differs by Extent at Matched Endoscopic Activity
Similarly, to rule out the influence of endoscopic activity (Supplementary Figure 1B), we compared serum omentin-1 between the distal- and extensive-colitis groups at the same endoscopic stage. In the endoscopically active stratum (MES ≥ 2), omentin-1 levels remained significantly lower in extensive colitis than in distal colitis (Figure 3A). No difference was seen among patients in endoscopic remission (MES 0/1) (Figure 3B). Together with the findings described above, these data indicate that serum omentin-1 levels not only reflect disease severity but also convey information on disease extent.
 |
Figure 3 Serum omentin-1 differs by extent at matched endoscopic activity. Endoscopic activity stratification: patients were classified as (A) endoscopically active (MES = 2/3) or (B) endoscopically inactive (MES = 0/1). Serum omentin-1 was quantified by ELISA. ns = no significance, The Mann–Whitney test. |
Efficacy of Serum Omentin-1 as an Extent Marker for UC Evaluation
We next evaluated the diagnostic performance of serum omentin-1 in distinguishing extensive from distal colitis. ROC analysis yielded different AUC values that indicate different levels of diagnostic accuracy: sufficient (0.6–0.7), good (0.7–0.8), very good (0.8–0.9), and excellent (≥0.9).16 For discriminating distal from extensive UC, we found AUC = 0.7326 and a cut-off value of 56.2 ng/mL in omentin-1 concentration was revealed (sensitivity of 66.67%, specificity of 78.57%, LR (+) of 3.1, LR (-) of 0.4) (Figure 4A). Furthermore, the AUC was 0.8302 (a cut-off value of 50.65 ng/mL, sensitivity of 73.33%, specificity of 88.68%, LR (+) of 6.5, LR (-) of 0.3) in clinically active patients (Figure 4B), and the AUC was 0.8870 (a cut-off value of 51.25 ng/mL, sensitivity of 79.31%, specificity of 89.36%, LR (+) of 7.5, LR (-) of 0.2) in endoscopically active patients (Figure 4C). These results strengthen our evidence that serum omentin-1 can be utilized for detecting UC extent in clinical use.
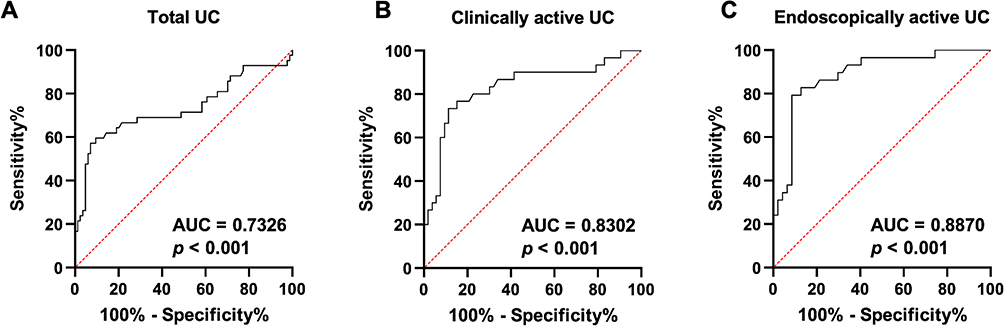 |
Figure 4 Efficacy of serum omentin-1 for UC extent evaluation. Receiver-operating-characteristic (ROC) curves were constructed to assess the ability of serum omentin-1 to discriminate extensive colitis from distal colitis. (A) Total study population (n = 126). (B) Clinically active subgroup (p-Mayo ≥ 3, n = 83). (C) Endoscopically active subgroup (MES ≥ 2, n = 76). |
Omentin-1 Levels Predict Response to IFX in Patients with Extensive UC
Among 36 UC subjects who received standard IFX induction within our cohort, 23 achieved complete or partial response whereas 13 exhibited primary non-response. Figure 5A shows that responders entered therapy with significantly higher omentin-1 levels than eventual non-responders. ROC analysis confirmed that omentin-1 levels discriminated between these outcome categories across the whole IFX subset (Figure 5B). When the same treatment group was further stratified by lesion sites, the predictive power resided exclusively within extensive colitis (Figure 5C, D and Supplementary Figure 2). Collectively, these data indicate that serum omentin-1 may serve as a response-prediction tool specifically for patients with extensive UC.
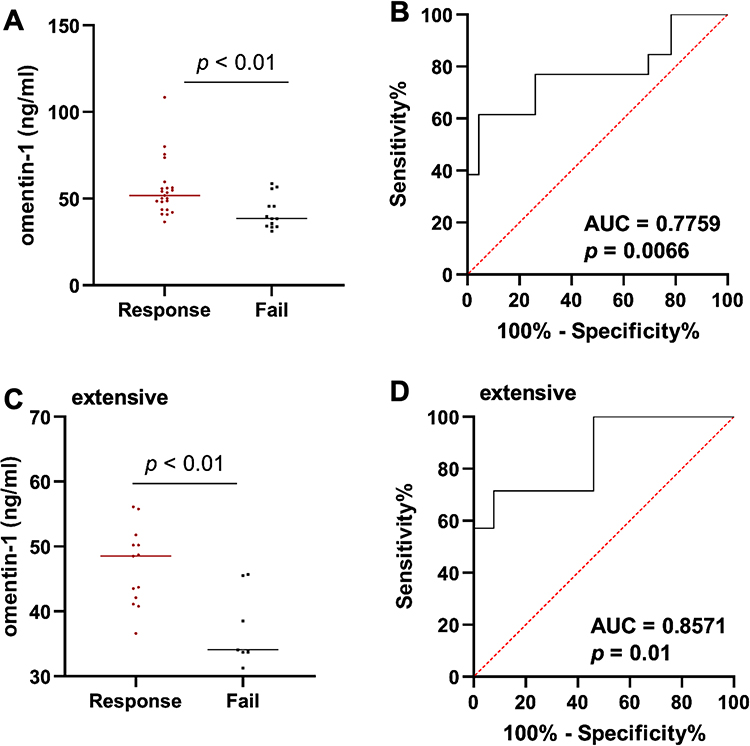 |
Figure 5 Omentin-1 levels Predict Response to infliximab (IFX) in Patients with extensive UC. UC patients (n = 36) received IFX induction therapy including 23 with complete or partial response and 13 with primary non-response. (A) Differences of serum omentin-1 were determined between patients with initial response to IFX and those who had primary non-response (fail). (B) Abilities of serum omentin-1 to discriminate IFX responders from primary non-responders were determined by ROC curve analysis was performed. p < 0.05 was considered significant. (C) Baseline levels of serum omentin-1 and (D) their discriminative abilities between IFX responders and non-responders were determined in patients with extensive UC. The Mann–Whitney test. |
Discussion
UC is judged by both how intense and how far the inflammation spreads, yet most studies have focused on the former, leaving the latter largely overlooked. We asked whether omentin-1—already shown in our earlier work to decrease when UC is active—might also mirror the disease extent.
Unraveling the molecular circuitry of IBD has remained a central theme in gastroenterology for decades. Recent evidence positions adipokines as important regulators of intestinal immunity.17 Among these, leptin, chemerin, and resistin have been linked to disease severity in both Crohn’s disease (CD) and UC,18 yet the contribution of omentin-1 remains less-defined. Omentin-1 is synthesized and secreted by visceral adipocytes and, more relevant to the gut, by goblet and Paneth cells.9 Our group first reported a reduction in circulating omentin-1 in irritable bowel syndrome (IBS), where low concentrations correlated with heightened pro-inflammatory cytokine signatures, worse somatic symptom scores, and impaired quality of life. In an IBS mouse model, exogenous omentin-1 attenuated visceral hyperalgesia and decreased mucosal mast-cell infiltration, establishing a causal link between the adipokine and gut homeostasis.19 Extending these observations to IBD, we recently demonstrated that serum omentin-1 levels were significantly lower in UC patients than in matched healthy controls and that concentrations scale inversely with both clinical and endoscopic activity.10 Collectively, these data situate omentin-1 as a biologically plausible participant in intestinal inflammation and support its utility as an accessible biomarker for monitoring disease activity.
Building on our previous work, the present study set out to examine whether serum omentin-1 carries disease extent information in UC. Management of UC relies on a thorough evaluation of several factors, including the activity scores and extent. Clinically, the intensity of inflammation dictates drug choice and dosing, and persistently high activity predicts hospitalization, colectomy and cancer. Not surprisingly, most trials have therefore concentrated on suppressing symptoms, treating extent as a background note. Recently, mechanistic IBD work—especially genotype analyses mapping CD to distinct gut sites—has driven home the point that, in UC as well, extent is an in-built trait with major clinical significance. A genome-wide association analysis has emphasized that disease extent is partly heritable and serves as the principal determinant of long-term disease behaviour in UC.7 The Montreal classification translates this genetic continuum into practical anatomy: lesions limited to the rectum (E1) or left colon (E2) behave differently from pancolitis (E3), and the boundary is no longer regarded as a mere technical detail. Distal disease (E1/E2) is linked to higher likelihood of clinical remission, whereas extensive disease (E3) predicts poorer response to agents such as vedolizumab and carries a markedly higher lifetime risk of colectomy and colitis-associated neoplasia.20 In this study, among the 126 patients, serum omentin-1 levels decreased progressively as the lesion extent extended beyond the splenic flexure, and patients with extensive colitis had significantly lower serum omentin-1 levels than those with distal colitis. Next, by controlling for clinical and endoscopic activity scores between groups, we show that serum omentin-1 levels differed between patients with different UC disease extents at the same level of disease activity, suggesting that serum omentin-1 can effectively predict the disease extent of UC independently of disease activity.
Anti-TNF therapy has become a cornerstone in the management of IBD, altering the disease course for both CD and UC.21–24 Among these agents, IFX is the most extensively studied and has proven effective in inducing and maintaining clinical remission and mucosal healing.21 However, approximately one-third of patients experience primary non-response—defined as no or limited clinical benefit 12–14 weeks after induction—highlighting a critical unmet need.25,26 Given the high cost, potential for serious adverse effects, and lack of universal efficacy, identifying reliable biomarkers to predict IFX response is essential.27 While several predictive factors have been proposed—including age, body weight, smoking status, disease duration, CRP, and albumin, most of them have not demonstrated utility, and many others remain controversial.27,28 In this study, we found that serum omentin-1 levels significantly discriminated between IFX responders and primary non-responders. Importantly, this discriminative capacity was not uniform across all UC subtypes: it was statistically significant in patients with extensive colitis but absent in those with distal disease. These findings suggest that omentin-1 may serve as a useful predictive biomarker specifically in the context of extensive UC, offering a blood-based tool to guide IFX initiation and avoid futile exposure in this high-risk population.
There are several limitations in the current study. First, the sample size was relatively small.The number of patients receiving biologic therapy was relatively small (36 cases), and further division into responders, partial responders, and non-responders resulted in even more limited sample sizes, which may affect the reliability of assessing the role of omentin-1 in predicting response to biologic therapy. Our study aimed to preliminarily observe the expression trends of omentin-1 across different treatment response groups. Although the subgroup analysis is indeed limited by sample size, we hope that these findings can serve as a valuable reference and provide preliminary data for future larger-scale, multicenter studies. We suggest that subsequent research adopt larger sample sizes and prospective designs to validate our findings. Second, only serum omentin-1 was measured; mucosal omentin-1 levels and their association with extent remain unknown and should be assessed in future work. Third, the underlying mechanisms linking omentin-1 to lesion sites were not explored; functional and pathway studies are needed to clarify this association. Fourth, Fecal calprotectin and C-reactive protein (CRP) are well-established classic biomarkers for IBD and are of great significance in assessing disease activity. Analyzing the correlation between omentin-1 and established biomarkers such as calprotectin or CRP will undoubtedly help clarify the clinical value of omentin-1 as a biomarker in IBD. Therefore, future prospective studies should incorporate comparisons with these biomarkers to better evaluate the potential clinical value of omentin-1.
Conclusions
Across a 126-patient UC cohort, serum omentin-1 exhibited an extent-dependent reduction that persisted after adjustment for clinical and endoscopic activity and retained independent predictive value for primary response to IFX selectively within extensive UC. These data reposition omentin-1 from a generic inflammatory read-out to an disease extent-informative biomarker, providing a non-invasive tool to quantify lesion sites and to stratify extensive-colitis patients for IFX therapy while reducing reliance on serial endoscopic reassessment. Furthermore, the ability of serum omentin-1 to distinguish disease extent may have broader clinical implications beyond guiding intestinal management. Accurate stratification of disease extent is increasingly recognized as important for identifying patients at risk for extraintestinal manifestations, such as enteropathic arthritis.29 Given that extensive colonic involvement is associated with a higher prevalence of these extraintestinal complications, a blood-based biomarker that reliably reflects disease extent could assist in risk stratification and inform multidisciplinary care. Future studies should investigate whether omentin-1 levels correlate with the presence or severity of extraintestinal manifestations in patients with UC.
Data Sharing Statement
All the data included in this study are available upon request by contacting the corresponding author.
Ethics Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board for Clinical Research of Sichuan Provincial People’s Hospital (No.2024.575-1). All subjects were well informed about the study and potential risk and signed an informed consent before participation.
Author Contributions
Chen Chen: conceptualization, methodology, writing-original draft, writing-review and editing, investigation, formal analysis
Jinxia Wang: conceptualization, methodology, writing-original draft, writing-review and editing, investigation, formal analysis
Tingting Wang: writing-original draft, data curation, formal analysis, visualization
Zhou Zhou: writing-review and editing, methodology, resources, investigation
Caiping Gao: writing-review and editing, methodology, resources, investigation
Yan Pan: methodology, validation, writing-review and editing, supervision, project administration
Chong He: conceptualization, methodology, validation, writing-review and editing, supervision, project administration, funding acquisition
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (82571551), Sichuan Science and Technology Program (2025ZNSFSC0056), and Sichuan Academy of Medical Sciences and Sichuan Provincial People’s Hospital (2022QN49).
Disclosure
The authors declare no competing interests.
References
1. Alatab S, Sepanlou SG, Ikuta K. Collaborators GBDIBD. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):17–10. doi:10.1016/S2468-1253(19)30333-4
2. Kaplan GG. The global burden of IBD: from 2015 to 2025. Nat Rev Gastroenterol Hepatol. 2015;12:720–727. doi:10.1038/nrgastro.2015.150
3. Sands BE. Biomarkers of inflammation in inflammatory bowel disease. Gastroenterology. 2015;149:1275–1285e2. doi:10.1053/j.gastro.2015.07.003
4. Satsangi J, Silverberg MS, Vermeire S, Colombel JF. The montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut. 2006;55:749–753. doi:10.1136/gut.2005.082909
5. Scarozza P, Marafini I, Laudisi F, et al. Extent of mucosal inflammation in ulcerative colitis influences the clinical remission induced by vedolizumab. J Clin Med. 2020;9:385. doi:10.3390/jcm9020385
6. Pabla BS, Schwartz DA. Assessing severity of disease in patients with ulcerative colitis. Gastroenterol Clin North Am. 2020;49:671–688. doi:10.1016/j.gtc.2020.08.003
7. Cleynen I, Boucher G, Jostins L, et al. Inherited determinants of Crohn’s disease and ulcerative colitis phenotypes: a genetic association study. Lancet. 2016;387(10014):156–167. doi:10.1016/S0140-6736(15)00465-1
8. Zhao A, Xiao H, Zhu Y, et al. Omentin-1: a newly discovered warrior against metabolic related diseases. Expert Opin Ther Targets. 2022;26:275–289. doi:10.1080/14728222.2022.2037556
9. Watanabe T, Watanabe-Kominato K, Takahashi Y, Kojima M, Watanabe R. Adipose Tissue-derived Omentin-1 function and regulation. Compr Physiol. 2017;7:765–781. doi:10.1002/j.2040-4603.2017.tb00769.x
10. Pan Y, Li A, Huang X, et al. Association between serum omentin-1 and mucosal disease activity in patients with ulcerative colitis. Postgrad Med J. 2024;100:327–333. doi:10.1093/postmj/qgae008
11. He C, Shi Y, Wu R, et al. miR-301a promotes intestinal mucosal inflammation through induction of IL-17A and TNF-alpha in IBD. Gut. 2016;65:1938–1950. doi:10.1136/gutjnl-2015-309389
12. Zhou Z, Zhang Y, Pan Y, et al. A novel neutrophil-based biomarker to monitor disease activity and predict response to infliximab therapy in patients with ulcerative colitis. Front Med. 2022;9:872831. doi:10.3389/fmed.2022.872831
13. He C, Yu T, Shi Y, et al. MicroRNA 301A promotes intestinal inflammation and colitis-associated cancer development by inhibiting BTG1. Gastroenterology. 2017;152:1434–1448e15. doi:10.1053/j.gastro.2017.01.049
14. Lewis JD, Chuai S, Nessel L, et al. Use of the noninvasive components of the Mayo score to assess clinical response in ulcerative colitis. Inflamm Bowel Dis. 2008;14:1660–1666. doi:10.1002/ibd.20520
15. D’Haens G, Sandborn WJ, Feagan BG, et al. A review of activity indices and efficacy end points for clinical trials of medical therapy in adults with ulcerative colitis. Gastroenterology. 2007;132:763–786. doi:10.1053/j.gastro.2006.12.038
16. Simundic AM. Measures of diagnostic accuracy: basic definitions. EJIFCC. 2009;19:203–211.
17. Radzik-Zajac J, Wytrychowski K, Wisniewski A, Barg W. The role of the novel adipokines vaspin and omentin in chronic inflammatory diseases. Pediatr Endocrinol Diabetes Metab. 2023;29:48–52. doi:10.5114/pedm.2022.121371
18. Ren Y, Zhao H, Yin C, et al. Adipokines, hepatokines and myokines: focus on their role and molecular mechanisms in adipose tissue inflammation. Front Endocrinol. 2022;13:873699.
19. Gao Y, Chen C, Huang X, et al. Omentin-1, a protective adipokine for irritable bowel syndrome. J Inflamm Res. 2025;18:1689–1701. doi:10.2147/JIR.S499613
20. Sun Y, Ruan G, Guo M, et al. Progressing or preserving, disease extent evolution in hospitalized patients with ulcerative colitis in China: a real-world study. Therap Adv Gastroenterol. 2025;18:17562848251339878. doi:10.1177/17562848251339878
21. Rutgeerts P, Sandborn WJ, Feagan BG, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2005;353:2462–2476. doi:10.1056/NEJMoa050516
22. Hanauer SB, Feagan BG, Lichtenstein GR, et al. Maintenance infliximab for Crohn’s disease: the ACCENT I randomised trial. Lancet. 2002;359:1541–1549. doi:10.1016/S0140-6736(02)08512-4
23. Louis E, Lofberg R, Reinisch W, et al. Adalimumab improves patient-reported outcomes and reduces indirect costs in patients with moderate to severe Crohn’s disease: results from the CARE trial. J Crohns Colitis. 2013;7:34–43. doi:10.1016/j.crohns.2012.02.017
24. Loftus EV, Feagan BG, Colombel JF, et al. Effects of Adalimumab maintenance therapy on health-related quality of life of patients with Crohn’s disease: patient-reported outcomes of the CHARM trial. Am J Gastroenterol. 2008;103:3132–3141. doi:10.1111/j.1572-0241.2008.02175.x
25. Rutgeerts P, D’Haens G, Targan S, et al. Efficacy and safety of retreatment with anti-tumor necrosis factor antibody (infliximab) to maintain remission in Crohn’s disease. Gastroenterology. 1999;117:761–769. doi:10.1016/S0016-5085(99)70332-X
26. Santora LC, Krull IS, Grant K. Characterization of recombinant human monoclonal tissue necrosis factor-alpha antibody using cation-exchange HPLC and capillary isoelectric focusing. Anal Biochem. 1999;275:98–108. doi:10.1006/abio.1999.4275
27. Gisbert JP, Chaparro M. Predictors of primary response to biologic treatment [Anti-TNF, Vedolizumab, and Ustekinumab] in patients with inflammatory bowel disease: from basic science to clinical practice. J Crohns Colitis. 2020;14:694–709. doi:10.1093/ecco-jcc/jjz195
28. Beltran B, Iborra M, Saez-Gonzalez E, et al. Fecal calprotectin pretreatment and induction infliximab levels for prediction of primary nonresponse to infliximab therapy in Crohn’s disease. Dig Dis. 2019;37:108–115. doi:10.1159/000492626
29. Çabuk B, Bulut Gökten D, Solakoğlu T, Mete R, Türkel Küçükmetin N, Mercan R. A single-center experience: enteropathic arthritis in inflammatory bowel diseases. Egypt Rheumatol. 2024;46:171–174. doi:10.1016/j.ejr.2024.07.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Literature Review of Ozanimod Therapy in Inflammatory Bowel Disease: From Concept to Practical Application
Becher N, Swaminath A, Sultan K
Therapeutics and Clinical Risk Management 2022, 18:913-927
Published Date: 8 September 2022
A Review on Inflammatory Bowel Diseases: Recent Molecular Pathophysiology Advances
Abdulla M, Mohammed N
Biologics: Targets and Therapy 2022, 16:129-140
Published Date: 12 September 2022
The Association Between Inflammatory Bowel Disease and Exposure to Tobacco Smoking: A Case-Control Study in Qatar
Abdallah B, Arif M, Al-Malki M, Hourani R, Al-Maadeed T, Khodr N, Al-Kuwari G, Al-Siddiqi M, Kane T, Chivese T
International Journal of General Medicine 2023, 16:233-242
Published Date: 21 January 2023
Stem Cell Therapy in Inflammatory Bowel Disease: A Review of Achievements and Challenges

Tian CM, Zhang Y, Yang MF, Xu HM, Zhu MZ, Yao J, Wang LS, Liang YJ, Li DF
Journal of Inflammation Research 2023, 16:2089-2119
Published Date: 16 May 2023
Emerging Therapies for Ulcerative Colitis: Updates from Recent Clinical Trials
AlAmeel T, AlMutairdi A, Al-Bawardy B
Clinical and Experimental Gastroenterology 2023, 16:147-167
Published Date: 17 August 2023