Back to Journals » International Journal of Women's Health » Volume 18
Correlation Between Superoxide Dismutase and Very-Low-Density Lipoprotein Cholesterol in the Blood of Patients with Uterine Fibroids
Authors Dai J, Man Y, Zhang L, Bo C, Chen C, Wang Y
Received 12 March 2026
Accepted for publication 29 June 2026
Published 9 July 2026 Volume 2026:18 608011
DOI https://doi.org/10.2147/IJWH.S608011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marta Barba
Jiahui Dai,1– 3 Yin Man,4 Liuqing Zhang,2 Caixia Bo,2 Chao Chen,5 Yunfei Wang3
1Department of Obstetrics and Gynecology, the First Affiliated Hospital of Guangzhou Medical University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Gynecologic Oncology, Affiliated Hospital of Jining Medical University, Jining, Shandong, People’s Republic of China; 3Center of Obstetrics and Gynecology, Peking University Shenzhen Hospital, Shenzhen, Guangdong, People’s Republic of China; 4Department of Gynecologic Oncology, Zhongnan Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China; 5Department of Neurosurgery, Qingdao Central Hospital, University of Health and Rehabilitation Sciences, Qingdao, Shandong, People’s Republic of China
Correspondence: Yunfei Wang, Email [email protected]
Introduction: Abnormal lipid metabolism and oxidative stress have both been implicated in uterine fibroids (UFs), but the relationship between these processes in patients with UFs remains unclear. The present study examined the correlation between serum levels of very-low-density lipoprotein cholesterol (VLDL-C) and superoxide dismutase (SOD) in patients with UFs.
Methods: This retrospective cross-sectional study included 1435 patients with UFs hospitalized at the Affiliated Hospital of Jining Medical University from January 2016 to December 2022. The correlation between SOD and VLDL-C was examined using baseline VLDL-C as the independent variable and SOD as the dependent variable. Age, body mass index (BMI), maximum fibroid diameter, and menstrual characteristics were considered covariates. The study population was divided into single-fibroid and multiple-fibroid groups based on the number of fibroids.
Results: A significant negative correlation between VLDL-C and SOD was observed in the overall study population and in both the single-fibroid and multiple-fibroid groups.
Conclusion: This study demonstrated a significant negative correlation between VLDL-C and SOD levels in patients with UFs. These findings support further prospective studies to determine whether the combined assessment of VLDL-C and SOD could aid the evaluation of lipid-related oxidative stress in this population.
Keywords: uterine fibroids, superoxide dismutase, very-low-density lipoprotein cholesterol, lipid metabolism, oxidative stress
Introduction
Uterine fibroids (UFs) are the most common benign neoplasms of the uterus, with a cumulative incidence approaching 70% by 50 years of age.1–4 Although many patients remain asymptomatic, UFs can cause abnormal uterine bleeding, pelvic pain, and anemia, substantially impair quality of life, and, in some cases, contribute to infertility.4–6 Despite their high prevalence and considerable clinical burden, UF pathophysiology remains incompletely understood. Metabolic and vascular abnormalities have recently received increasing attention as potential factors involved in UF development.
UFs and atherosclerotic lesions share several pathological features, including smooth muscle cell dysregulation and extracellular matrix remodeling.7,8 Dyslipidemia, particularly elevated triglyceride levels, has also been associated with the presence of UFs, suggesting a possible link between lipid metabolism and UF pathophysiology.8,9 Very-low-density lipoprotein cholesterol (VLDL-C) represents the cholesterol carried by triglyceride-rich VLDL particles and has been widely studied in relation to atherosclerotic cardiovascular disease (ASCVD).10,11 In atherosclerosis, VLDL and other triglyceride-rich lipoproteins have been linked to oxidative stress, vascular inflammation, and endothelial dysfunction, indicating a close relationship between triglyceride-rich lipoprotein metabolism and redox imbalance.10,12 These observations suggest that oxidative stress may also be relevant to the relationship between lipid metabolic abnormalities and UFs.
Oxidative stress has also been implicated in UF pathophysiology. An imbalance between reactive oxygen species production and antioxidant defenses may contribute to leiomyoma cell proliferation, extracellular matrix remodeling, and fibrotic changes in leiomyoma tissue.13–15 Superoxide dismutase (SOD) is a key enzymatic antioxidant that catalyzes the dismutation of superoxide anions into hydrogen peroxide and molecular oxygen, thereby limiting superoxide-mediated cellular injury.13,16,17 Cellular and clinical studies suggest that SOD-mediated antioxidant defenses are impaired in UFs. Reduced SOD expression and enzymatic activity have been reported in human leiomyoma cells, together with lower circulating SOD activity in women with UFs.13,18 Increased acetylation of manganese superoxide dismutase (MnSOD) at lysine 122, a post-translational modification associated with reduced enzymatic activity, has also been detected in leiomyoma tissues and primary leiomyoma cells compared with matched myometrial controls.19 Taken together, these findings support a link between impaired SOD-mediated antioxidant defenses and redox imbalance in UFs.
Despite growing evidence linking dysregulated lipid metabolism and impaired antioxidant defenses to UFs, it remains unclear whether circulating VLDL-C is correlated with SOD levels in patients with UFs. Defining this relationship may help clarify the relationship between lipid metabolism and antioxidant status in this population. We therefore conducted a retrospective cross-sectional study to examine the correlation between serum VLDL-C and SOD levels after adjustment for relevant demographic, menstrual, and fibroid-related factors. We also performed subgroup analyses in patients with single and multiple fibroids to assess the consistency of this correlation across groups.
Materials and Methods
Study Design
This was a retrospective cross-sectional study based on electronic medical records from the Department of Gynecology, Affiliated Hospital of Jining Medical University. VLDL-C, SOD, and relevant covariates were obtained from baseline preoperative records during the same hospitalization, and no longitudinal follow-up data were used. Baseline VLDL-C was considered the independent variable, and SOD was considered the dependent variable for the analysis of their correlation.
Study Population
This retrospective cross-sectional study included patients with UFs whose relevant clinical information was collected from the Department of Gynecology at the Affiliated Hospital of Jining Medical University. Data were extracted from the hospital’s electronic medical record system and de-identified to protect patient privacy. The study was approved by the Ethics Committee of the Affiliated Hospital of Jining Medical University (approval number: 2022C114). The requirement for informed consent was waived by the Ethics Committee in accordance with the institutional ethical review policy for retrospective studies using de-identified existing clinical data. The study was conducted in accordance with the Declaration of Helsinki.
The study population comprised patients who visited the Department of Gynecology, Affiliated Hospital of Jining Medical University from January 2016 to December 2022. Inclusion criteria: (1) UFs determined by postoperative pathology or (2) UFs determined by auxiliary examination and preoperative clinical manifestations. Exclusion criteria: (1) use of antibiotics or lipid-lowering drugs within 3 months before surgery; (2) the presence of hematological diseases, malignant tumors, autoimmune diseases, metabolic diseases, hypersplenism, or active infections; (3) use of glucocorticoids, long-term immunomodulatory drugs, or anti-inflammatory drugs; (4) age <18 years old; (5) pregnancy or lactation; and (6) previous use of drugs or surgery to treat UFs. No formal a priori sample size calculation was performed because this was a retrospective analysis of an existing clinical database, and the final sample size was determined by the number of eligible patients during the predefined study period. After application of the inclusion and exclusion criteria, 1435 patients were included in the final analysis. Based on the number of UFs, the 1435 research subjects were divided into a single-fibroid group comprising 658 individuals and a multiple-fibroid group comprising 777 individuals.
Variables
Patient data, including age, body mass index (BMI), menstrual status, the number and size of lesions, and blood indicators, such as triglycerides (TGs), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), VLDL-C, and SOD, were retrospectively collected. The patient’s medical history was used to obtain information concerning regular menstruation, heavy menstrual flow, and absence of dysmenorrhea. The standard for regular menstruation is a menstrual cycle of 21 to 35 days and a menstrual period lasting from 4 to 6 days. Individuals who met the standards were considered regular, whereas those who did not meet the standards were considered irregular. Menstrual blood loss of ≥80 mL was considered excessive. During hospitalization, fasting peripheral venous blood samples were collected after at least 8 h of fasting for liver function testing and other biochemical measurements. Laboratory tests were typically performed approximately 2 days before surgery. The lipid-related parameters and SOD included in the present analysis were extracted from these baseline laboratory records. All laboratory measurements were performed by trained laboratory personnel at our hospital. TGs, TC, HDL-C, LDL-C, VLDL-C, and SOD were determined using a Cobas 8000 C702 fully automatic biochemical immunoanalyzer.20
Covariates were selected based on clinical relevance, previously reported factors related to the study variables, and data availability. Model I was adjusted for age, menstrual regularity, menstrual flow, and dysmenorrhea. Model II was further adjusted for BMI and maximum fibroid diameter. The number of fibroids was used for subgroup analyses rather than as a covariate in the final regression models. All covariates were collected at baseline.
Statistical Analysis
Continuous variables were expressed in two ways: normally distributed continuous variables were expressed as mean ± standard deviation (SD), and non-normally distributed continuous variables were expressed as median (interquartile range, IQR). Categorical variables were expressed as frequencies or percentages. Continuous variables were compared between the single-fibroid and multiple-fibroid groups using the independent-samples t test or Mann–Whitney U-test, as appropriate. Categorical variables were compared using the χ2-test or Fisher’s exact test, as appropriate.
Pearson correlation coefficients (r) and corresponding P-values were calculated to assess the unadjusted linear correlation between VLDL-C and SOD in the overall study population and in the single-fibroid and multiple-fibroid subgroups.
The entire data analysis process can be divided into two steps. In the first step, multivariable linear regression models were generated to examine the correlation between VLDL-C and SOD after adjustment for relevant covariates. Model I was adjusted for age, menstrual regularity, menstrual flow, and dysmenorrhea. Model II was further adjusted for BMI and maximum fibroid diameter. Model II used complete-case data because maximum fibroid diameter was missing in some patients. Multicollinearity was assessed using variance inflation factors (VIFs).
In the second step, generalized additive models with penalized spline smoothing were used to explore potential nonlinear correlations between VLDL-C and SOD. If nonlinearity was detected, a recursive algorithm was used to compute the inflection point, followed by the construction of a two-part linear regression model on both sides of the inflection point. The fit of the one-linear and two-piecewise linear regression models was compared using the likelihood-ratio test.
The R statistical software package was used to perform all statistical analyses (http://www.R-project.org R Foundation). A two-sided P < 0.05 was considered statistically significant.
Results
Baseline Characteristics of the Study Population
A total of 1435 participants were included in the final analysis (Figure 1). Table 1 displays the baseline characteristics of the selected study subjects. Participants were categorized into single-fibroid and multiple-fibroid groups according to the number of fibroids. The average age of all participants was 45.89 ± 7.78 years. Among them, multiple UFs accounted for approximately 54.15%, and the remainder had single UFs. No statistically significant differences were observed in HDL-C, LDL-C, TGs, TC, and SOD between the single-fibroid and multiple-fibroid groups (all P > 0.05). However, statistically significant differences were observed in age, BMI, maximum fibroid diameter, VLDL-C, menstrual pattern, menstrual volume, and dysmenorrhea (all P < 0.05).
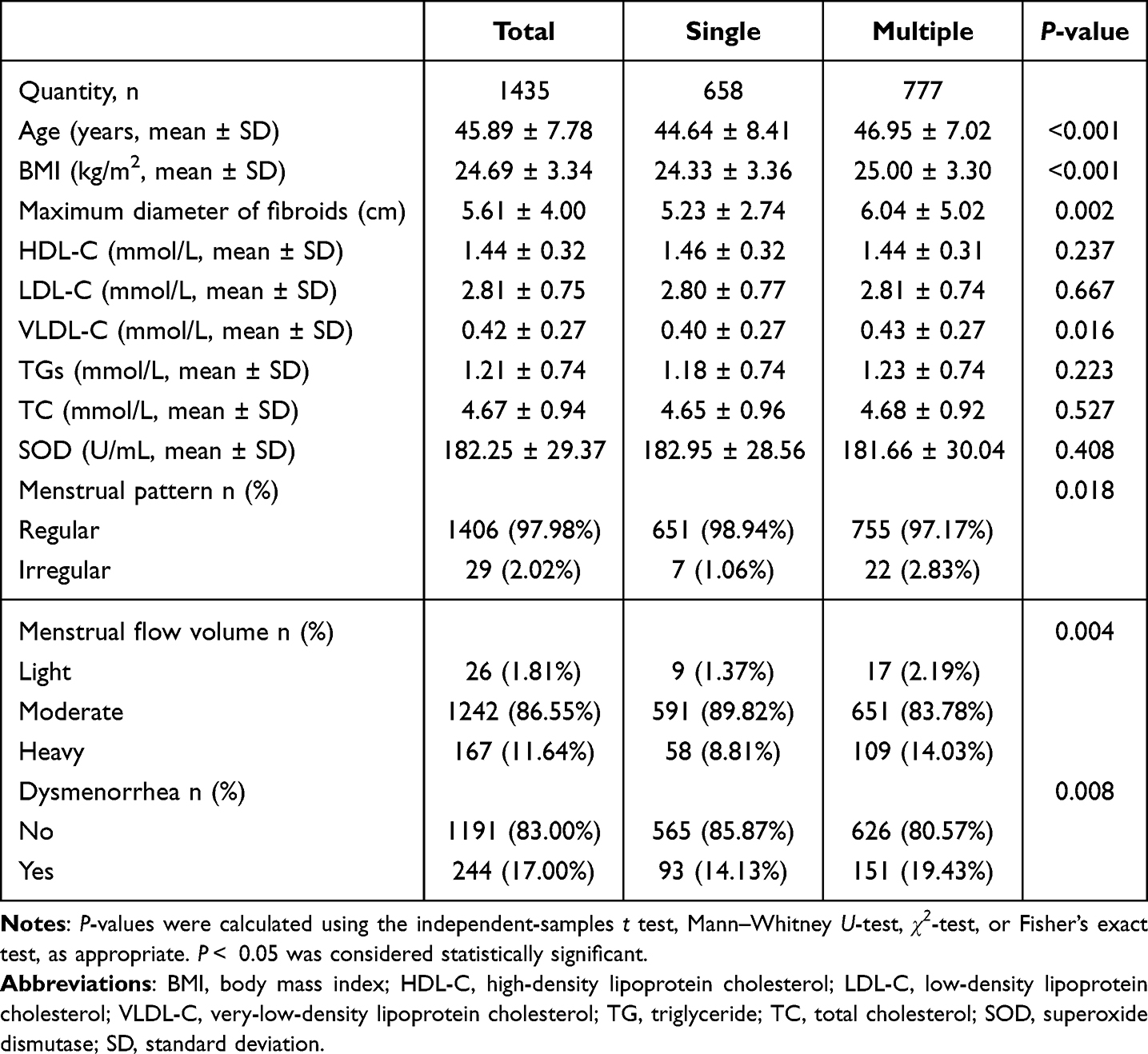 |
Table 1 Baseline Characteristics of the Study Population |
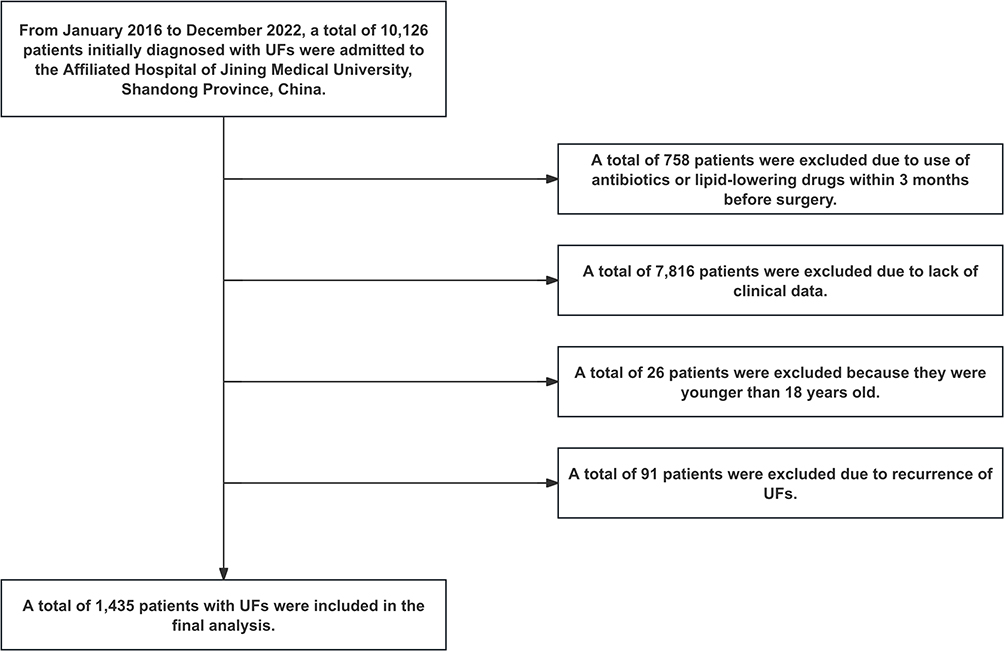 |
Figure 1 Inclusion and exclusion criteria process. Eligible patients with uterine fibroids (UFs) were screened according to the inclusion and exclusion criteria. A total of 1435 patients were included in the final analysis and categorized into the single-fibroid group (n = 658) and multiple-fibroid group (n = 777) according to the number of fibroids. |
Univariate Analysis of Superoxide Dismutase
In the overall study population, HDL-C was positively correlated with SOD (β = 7.28, 95% CI = 2.45, 12.08), whereas VLDL-C was negatively correlated with SOD (β = −13.09, 95% CI = −18.64, −7.55), as shown in Table 2. Interestingly, separate analyses of the study population by the single-fibroid and multiple-fibroid groups indicated that in the single-fibroid group, a negative correlation was observed between TGs and SOD (β = −3.23, 95% CI = −6.19, −0.27). However, this phenomenon was not observed in the multiple-fibroid group or in the overall population. The remaining results were generally consistent with those observed in the overall study population.
 |
Table 2 Univariate Analysis of SOD (U/mL) |
Results of Unadjusted and Adjusted Linear Regression
Pearson correlation analysis showed weak negative correlations between VLDL-C and SOD in the overall study population (r = −0.122, P < 0.001), the single-fibroid group (r = −0.086, P = 0.028), and the multiple-fibroid group (r = −0.150, P < 0.001), as shown in Supplementary Table S1. Multivariable linear regression analysis was then performed to examine the correlation between VLDL-C and SOD after adjustment for relevant covariates. As demonstrated in Table 3, three models were established: unadjusted model, model I (adjusted variables: age, menstrual period regularity, menstrual volume, and dysmenorrhea), and model II (adjusted variables: age, BMI, maximum fibroid diameter, menstrual regularity, menstrual flow, and dysmenorrhea). In addition, the effect sizes (β) and 95% confidence intervals (CI) were presented. In the entire study population, under the unadjusted model, a negative correlation was observed between VLDL-C (β = −13.09, 95% CI = −18.64, −7.55) and SOD. Similarly, in adjusted model I, a negative correlation between VLDL-C (β = −13.81, 95% CI = −19.41, −8.21) and SOD was also identified. Additionally, in adjusted model II, a negative correlation between VLDL-C (β = −15.76, 95% CI = −22.96, −8.53) and SOD was observed. Subsequently, subgroup analysis was conducted on the study population based on the number of UFs. The findings of the single-fibroid and multiple-fibroid groups were generally consistent with those of the overall study population. The inverse association between VLDL-C and SOD remained statistically significant after adjustment in both Model I and Model II. No evidence of problematic multicollinearity was observed in Model II, with VIFs ≤1.09.
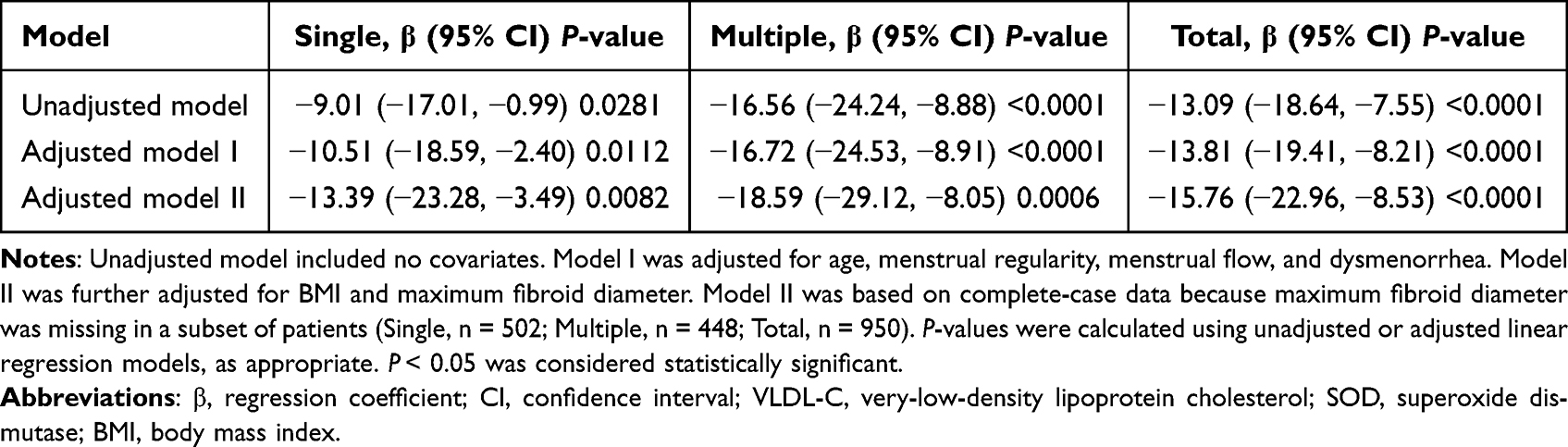 |
Table 3 Relationship Between VLDL-C (mmol/L) and SOD (U/mL) in Different Models |
Relationship Between Very-Low-Density Lipoprotein Cholesterol and Superoxide Dismutase
In this study, the relationship between VLDL-C and SOD was investigated not only in the entire study population but also in the single-fibroid and multiple-fibroid groups. After adjustment for age, menstrual regularity, menstrual flow, and dysmenorrhea, smooth curve fitting suggested an inverse pattern between VLDL-C and SOD in the overall study population. Similar visual patterns were observed in the single-fibroid and multiple-fibroid groups, as shown in Figures 2–4.
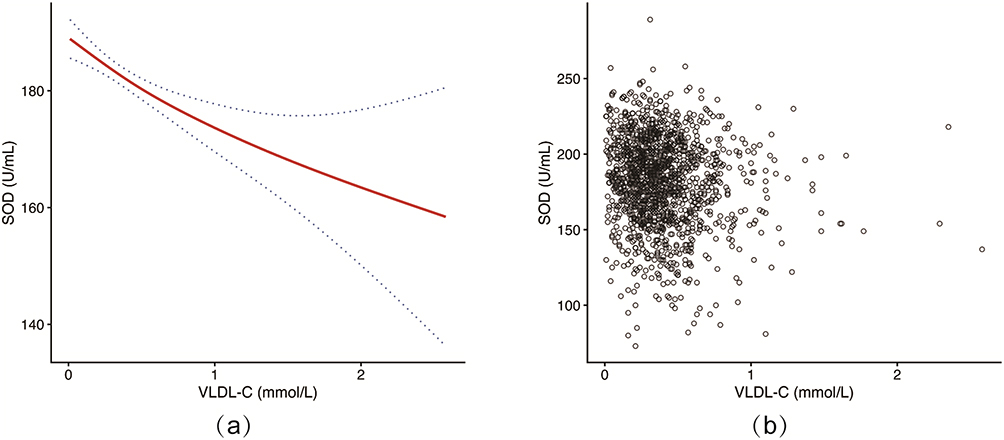 |
Figure 2 Relationship between VLDL-C and SOD in the overall study population. (a) Smooth curve illustrating the association between VLDL-C and SOD. (b) Scatter plot of VLDL-C and SOD values. The solid red line represents the fitted smooth curve, and the blue dotted lines represent the 95% confidence interval around the fitted curve. |
 |
Figure 3 Relationship between VLDL-C and SOD in the single-fibroid group. (a) Smooth curve illustrating the association between VLDL-C and SOD. (b) Scatter plot of VLDL-C and SOD values. The solid red line represents the fitted smooth curve, and the blue dotted lines represent the 95% confidence interval around the fitted curve. |
 |
Figure 4 Relationship between VLDL-C and SOD in the multiple-fibroid group. (a) Smooth curve illustrating the association between VLDL-C and SOD. (b) Scatter plot of VLDL-C and SOD values. The solid red line represents the fitted smooth curve, and the blue dotted lines represent the 95% confidence interval around the fitted curve. |
As shown in Table 4, exploratory segmented regression analyses were performed after adjustment for age, menstrual regularity, menstrual flow, and dysmenorrhea. In the overall study population, the candidate breakpoint was 0.50 mmol/L. VLDL-C was inversely associated with SOD below this value (β = −24.13, 95% CI = −35.84, −12.40), whereas the association was attenuated and no longer statistically significant above the candidate breakpoint. A similar pattern was observed in the multiple-fibroid group, with a candidate breakpoint of 0.61 mmol/L, and the two-piecewise linear model showed a better fit than the one-linear model (P = 0.020). In the single-fibroid group, an inverse association was observed below the candidate breakpoint of 0.09 mmol/L, but the difference between the two slopes was not statistically significant. Therefore, the segmented patterns and estimated candidate breakpoints should be interpreted as exploratory.
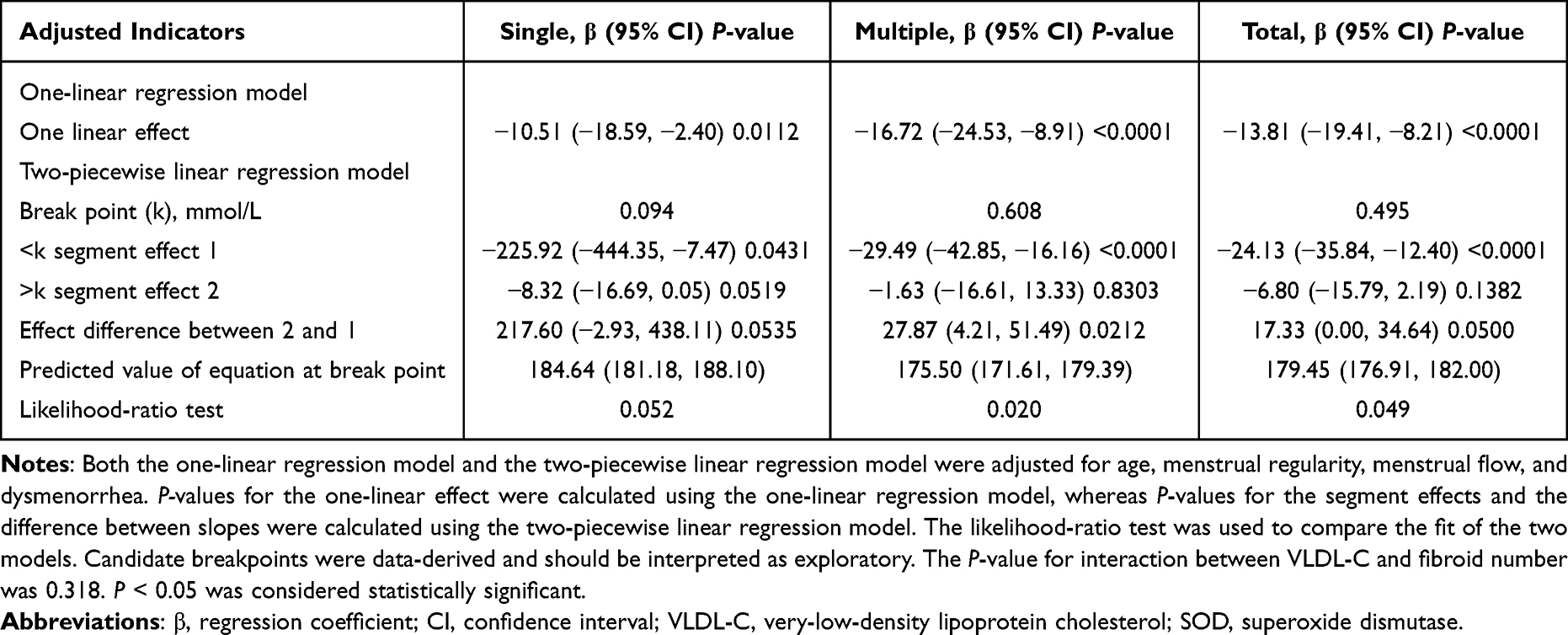 |
Table 4 Threshold Effect Analysis of the Relationship Between VLDL-C (mmol/L) and SOD (U/mL) Levels |
Discussion
UFs are one of the most common gynecological tumors in women. Although UFs are highly prevalent, their pathophysiology and risk factors remain incompletely understood.21 SOD is an important antioxidant enzyme, and previous studies have shown that UFs are characterized by impairment of the intracellular antioxidant system, including reduced SOD activity compared with normal myometrium.13 Elevated circulating lipid levels have also been associated with UFs, and altered lipid profiles have been reported in recurrent UF tissues.21–23 Although the correlation between oxidative stress and lipid metabolism has been widely investigated in various diseases, it has not been fully characterized in patients with UFs.23–26
In this study, univariate analysis, multivariable linear regression, and threshold-effect analysis were used to comprehensively examine the correlation between SOD and lipid metabolism-related indicators. The findings indicated that both HDL-C and VLDL-C were correlated with SOD in the overall study population. Specifically, a positive correlation was observed between HDL-C and SOD, whereas a negative correlation was observed between VLDL-C and SOD. The study population was further analyzed according to the number of fibroids. In the single-fibroid group, a negative correlation was observed between TG and SOD, whereas this correlation was not observed in the multiple-fibroid group or the overall population. The remaining findings were generally consistent with those in the overall study population. These results suggest that abnormalities in lipid metabolism may coexist with altered antioxidant status in patients with UFs.
Subsequent analyses focused on the correlation between VLDL-C and SOD. VLDL-C, a component of non-HDL cholesterol, is considered an atherogenic lipid indicator associated with the risk of ASCVD.27 The formation of UFs has been proposed to share certain injury-response mechanisms with the formation of atherosclerotic plaques.7,8,22 Our study demonstrated a significant inverse correlation between VLDL-C and SOD in the overall study population and in both the single-fibroid and multiple-fibroid groups. Exploratory segmented regression analyses, adjusted for age, menstrual regularity, menstrual flow, and dysmenorrhea, suggested that the inverse correlation may be more apparent at lower VLDL-C levels. In the overall study population, the candidate breakpoint was 0.50 mmol/L. VLDL-C was inversely correlated with SOD below this value, whereas the correlation was attenuated and was no longer statistically significant above the candidate breakpoint. A similar pattern was observed in the multiple-fibroid group, with a candidate breakpoint of 0.61 mmol/L. In this subgroup, the difference between the slopes below and above the candidate breakpoint was statistically significant, and the two-piecewise linear model showed a better fit than the one-linear model according to the likelihood-ratio test. In the single-fibroid group, the candidate breakpoint was 0.09 mmol/L. Although an inverse correlation was observed below this value and was attenuated above it, neither the difference between the two slopes nor the likelihood-ratio test reached statistical significance.
Therefore, the evidence for a segmented correlation in the single-fibroid group was limited. Several explanations may account for the attenuation of the inverse correlation at higher VLDL-C levels. First, the relationship may follow a saturable pattern, such that further increases in VLDL-C are accompanied by progressively smaller changes in SOD after antioxidant defenses have already been substantially altered. Second, other metabolic or inflammatory processes may become more influential at higher VLDL-C levels and attenuate the observed correlation. Third, the relatively limited number of observations at the upper end of the VLDL-C distribution may have reduced the precision of the estimates. These explanations remain speculative and cannot be distinguished using the present cross-sectional data. Because the candidate breakpoints were data-derived, they should not be interpreted as definitive biological or clinical thresholds and require validation in independent populations.
These exploratory observations should be regarded as hypothesis-generating and do not support the clinical application of the identified breakpoints. The potential clinical relevance of the observed VLDL-C–SOD association should therefore be interpreted cautiously within the broader context of gynecological assessment. Obesity, diabetes mellitus, and hypertension have been reported as risk factors for endometrial cancer,28 highlighting the importance of metabolic health in women with uterine conditions. However, VLDL-C and SOD are not specific markers of UFs and cannot replace established diagnostic approaches. The evaluation of uterine masses continues to rely on clinical assessment, imaging, and, when indicated, histopathological examination. Expert ultrasonography and magnetic resonance imaging may provide additional information when atypical features raise concern for uterine sarcoma.29
To the best of our knowledge, this is the first study to examine the independent correlation between serum VLDL-C and SOD levels in patients with UFs. The inverse association observed in this study suggests that altered lipid metabolism and antioxidant status may coexist in this population. Prospective studies are needed to clarify the temporal relationship and underlying biological mechanisms and to determine whether the combined assessment of VLDL-C and SOD may help characterize lipid-related oxidative stress in patients with UFs.
However, this study has several limitations. First, the study subjects were patients with confirmed UFs in southwestern Shandong, China. Thus, additional multicenter studies are essential to validate these findings. Second, patients with a history of pharmacological or surgical treatment for UFs were excluded. Therefore, the findings may not be generalizable to previously treated populations. Finally, due to the exclusion criteria, the findings of this study may not be generalizable to patients who had used lipid-lowering drugs within the previous 3 months, individuals aged < 18 years, or other excluded populations.
Conclusions
In this retrospective cross-sectional study, serum VLDL-C levels were inversely correlated with SOD levels in patients with UFs. This inverse correlation remained evident after adjustment for relevant covariates and in analyses stratified by fibroid number. These findings do not establish a causal relationship but support further prospective studies to clarify the temporal relationship and potential biological mechanisms linking lipid metabolism and oxidative stress in patients with UFs.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
Ethical approval for this retrospective study was obtained from the Ethics Committee of the Affiliated Hospital of Jining Medical University (Approval No. 2022C114). The requirement for written informed consent was waived by the Ethics Committee in accordance with the institutional ethical review policy for retrospective studies using de-identified existing clinical data. All patient information was handled in a de-identified and confidential manner. The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors thank all the healthcare technicians in the Department of Gynecology, Affiliated Hospital of Jining Medical University.
Funding
This work was supported by Shenzhen High-level Hospital Construction Fund (YBH2019-260), Shenzhen Key Medical Discipline Construction Fund (No.SZXK027) & Sanming Project of Medicine in Shenzhen (No.SZSM202011016).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bulun SE. Uterine fibroids. N Engl J Med. 2013;369(14):1344–11. doi:10.1056/NEJMra1209993
2. Machado-Lopez A, Simón C, Mas A. Molecular and cellular insights into the development of uterine fibroids. Int J Mol Sci. 2021;22(16):8483. doi:10.3390/ijms22168483
3. Marsh EE, Al-Hendy A, Kappus D, Galitsky A, Stewart EA, Kerolous M. Burden, prevalence, and treatment of uterine fibroids: a survey of US women. J Womens Health. 2018;27(11):1359–1367. doi:10.1089/jwh.2018.7076
4. Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol. 2003;188(1):100–107. doi:10.1067/mob.2003.99
5. Donnez J, Tomaszewski J, Vázquez F, et al. Ulipristal acetate versus leuprolide acetate for uterine fibroids. N Engl J Med. 2012;366(5):421–432. doi:10.1056/NEJMoa1103180
6. Giuliani E, As-Sanie S, Marsh EE. Epidemiology and management of uterine fibroids. Int J Gynaecol Obstet. 2020;149(1):3–9. doi:10.1002/ijgo.13102
7. Kirschen GW, AlAshqar A, Miyashita-Ishiwata M, Reschke L, El Sabeh M, Borahay MA. Vascular biology of uterine fibroids: connecting fibroids and vascular disorders. Reproduction. 2021;162(2):R1–R18. doi:10.1530/REP-21-0087
8. Uimari O, Auvinen J, Jokelainen J, et al. Uterine fibroids and cardiovascular risk. Hum Reprod. 2016;31(12):2689–2703. doi:10.1093/humrep/dew249
9. Takeda T, Sakata M, Isobe A, et al. Relationship between metabolic syndrome and uterine leiomyomas: a case-control study. Gynecol Obstet Invest. 2008;66(1):14–17. doi:10.1159/000114250
10. Ginsberg HN, Packard CJ, Chapman MJ, et al. Triglyceride-rich lipoproteins and their remnants: metabolic insights, role in atherosclerotic cardiovascular disease, and emerging therapeutic strategies-a consensus statement from the European Atherosclerosis Society. Eur Heart J. 2021;42(47):4791–4806. doi:10.1093/eurheartj/ehab551
11. Vallejo-Vaz AJ, Fayyad R, Boekholdt SM, et al. Triglyceride-rich lipoprotein cholesterol and risk of cardiovascular events among patients receiving statin therapy in the TNT trial. Circulation. 2018;138(8):770–781. doi:10.1161/CIRCULATIONAHA.117.032318
12. Anderson RA, Evans ML, Ellis GR, et al. The relationships between post-prandial lipaemia, endothelial function and oxidative stress in healthy individuals and patients with type 2 diabetes. Atherosclerosis. 2001;154(2):475–483. doi:10.1016/S0021-9150(00)00499-8
13. Fletcher NM, Saed MG, Abu-Soud HM, Al-Hendy A, Diamond MP, Saed GM. Uterine fibroids are characterized by an impaired antioxidant cellular system: potential role of hypoxia in the pathophysiology of uterine fibroids. J Assist Reprod Genet. 2013;30(7):969–974. doi:10.1007/s10815-013-0029-7
14. Olson SL, Akbar RJ, Gorniak A, Fuhr LI, Borahay MA. Hypoxia in uterine fibroids: role in pathobiology and therapeutic opportunities. Oxygen. 2024;4(2):236–252. doi:10.3390/oxygen4020013
15. Nayki C, Nayki U, Gunay M, et al. Oxidative and antioxidative status in the endometrium of patients with benign gynecological disorders. J Gynecol Obstet Hum Reprod. 2017;46(3):243–247. doi:10.1016/j.jogoh.2017.02.002
16. Jomova K, Alomar SY, Alwasel SH, Nepovimova E, Kuca K, Valko M. Several lines of antioxidant defense against oxidative stress: antioxidant enzymes, nanomaterials with multiple enzyme-mimicking activities, and low-molecular-weight antioxidants. Arch Toxicol. 2024;98(5):1323–1367. doi:10.1007/s00204-024-03696-4
17. Valko M, Leibfritz D, Moncol J, Cronin MT, Mazur M, Telser J. Free radicals and antioxidants in normal physiological functions and human disease. Int J Biochem Cell Biol. 2007;39(1):44–84. doi:10.1016/j.biocel.2006.07.001
18. Vignini A, Sabbatinelli J, Clemente N, et al. Preperitoneal fat thicknesses, lipid profile, and oxidative status in women with uterine fibroids. Reprod Sci. 2017;24(10):1419–1425. doi:10.1177/1933719116689598
19. Vidimar V, Gius D, Chakravarti D, Bulun SE, Wei JJ, Kim JJ. Dysfunctional MnSOD leads to redox dysregulation and activation of prosurvival AKT signaling in uterine leiomyomas. Sci Adv. 2016;2(11):e1601132. doi:10.1126/sciadv.1601132
20. Coucke W, Charlier C, Croes K, et al. Analytical performance of eight enzymatic assays for ethanol in serum evaluated by data from the Belgian external quality assessment scheme. Clin Chem Lab Med. 2022;60(8):1211–1217. doi:10.1515/cclm-2022-0285
21. Duan Y, Guo L, Peng Y, et al. Correlation between inflammatory marker and lipid metabolism in patients with uterine leiomyomas. Front Med. 2023;10:1124697. doi:10.3389/fmed.2023.1124697
22. Korkmaz V, Ozkaya E, Özer Kadife S, Kara F, Kucukozkan T. Investigation of cardiovascular disease risk in women with uterine leiomyomas. Ir J Med Sci. 2016;185(3):689–693. doi:10.1007/s11845-015-1343-0
23. Zabłocka-Słowińska K, Płaczkowska S, Skórska K, et al. Oxidative stress in lung cancer patients is associated with altered serum markers of lipid metabolism. PLoS One. 2019;14(4):e0215246. doi:10.1371/journal.pone.0215246
24. Zarrouk A, Hammouda S, Ghzaiel I, et al. Association between oxidative stress and altered cholesterol metabolism in Alzheimer’s disease patients. Curr Alzheimer Res. 2020;17(9):823–834. doi:10.2174/1567205017666201203123046
25. Cruz-Gregorio A, Aranda-Rivera AK, Ortega-Lozano AJ, Pedraza-Chaverri J, Mendoza-Hoffmann F. Lipid metabolism and oxidative stress in HPV-related cancers. Free Radic Biol Med. 2021;172:226–236. doi:10.1016/j.freeradbiomed.2021.06.009
26. Wang H, Ruan X, Li Y, Cheng J, Mueck AO. Oxidative stress indicators in Chinese women with PCOS and correlation with features of metabolic syndrome and dependency on lipid patterns. Arch Gynecol Obstet. 2019;300(5):1413–1421. doi:10.1007/s00404-019-05305-7
27. Zhao F, Qi Y, Liu J, et al. Low very low-density lipoprotein cholesterol but high very low-density lipoprotein receptor mRNA expression in peripheral white blood cells: an atherogenic phenotype for atherosclerosis in a community-based population. EBioMedicine. 2017;25:136–142. doi:10.1016/j.ebiom.2017.08.019
28. Nguyen PN, Nguyen VT. Evaluating clinical features in intracavitary uterine pathologies among vietnamese women presenting with peri-and postmenopausal bleeding: a bicentric observational descriptive analysis. J Midlife Health. 2022;13(3):225–232. doi:10.4103/jmh.jmh_81_22
29. Nguyen XL, Huynh QH, Nguyen PN. Assessing the clinical characteristics and the role of imaging modalities in uterine sarcoma: a single-center retrospective study from vietnam. J Clin Ultrasound. 2025;53(7):1527–1537. doi:10.1002/jcu.24046
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Superoxide Dismutase and Glutathione Reductase as Indicators of Oxidative Stress Levels May Relate to Geriatric Hip Fractures’ Survival and Walking Ability: A Propensity Score Matching Study
Liu M, Yang C, Chu Q, Fu X, Zhang Y, Sun G
Clinical Interventions in Aging 2022, 17:1081-1090
Published Date: 12 July 2022
Antioxidant Mitoquinone Alleviates Chronic Pancreatitis via Anti-Fibrotic and Antioxidant Effects
Li M, Yuan Y, Han X, Liu X, Zhang W, Hao J
Journal of Inflammation Research 2022, 15:4409-4420
Published Date: 3 August 2022
Effects of Semaglutide on Cardiac Protein Expression and Cardiac Function of Obese Mice
Pan X, Yue L, Ban J, Ren L, Chen S
Journal of Inflammation Research 2022, 15:6409-6425
Published Date: 24 November 2022
The Lipid-Oxidative Stress Axis: Novel Therapeutic Targets for Podocytopathy

Liu Y, Zou M, Wang Y
Journal of Inflammation Research 2025, 18:12505-12532
Published Date: 11 September 2025
Biomaterials Promote the Regression of Atherosclerotic Plaque by Regulating Cell Behavior
Wang C, Sun C, Wu X, Ding Z, Liu K, Cao J
International Journal of Nanomedicine 2026, 21:574592
Published Date: 2 May 2026