Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
COPD–Lung Cancer Comorbidity: Mechanistic Insights and Precision Oncology Implications
Authors He Y ![]() , Liu B, Li W, Zhou X, Tao H
, Liu B, Li W, Zhou X, Tao H
Received 4 March 2026
Accepted for publication 9 May 2026
Published 18 May 2026 Volume 2026:21 606647
DOI https://doi.org/10.2147/COPD.S606647
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Zijing Zhou
Yajuan He, Beili Liu, Wenjun Li, Xinyi Zhou, Hongyan Tao
Department of Pulmonary and Critical Care Medicine, The Second Hospital & Clinical Medical School, Lanzhou University, Lanzhou, 730000, People’s Republic of China
Correspondence: Hongyan Tao, Department of Pulmonary and Critical Care Medicine, The Second Hospital & Clinical Medical School, Lanzhou University, 82 Cuiyingmen Street, Chengguan District, Lanzhou, 730000, People’s Republic of China, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) and lung cancer frequently coexist, constituting a clinically consequential comorbidity with major implications for precision medicine.
Mechanistic Insights: Beyond shared environmental exposures such as tobacco smoke and air pollution, COPD has emerged as an independent driver of pulmonary carcinogenesis, mediated through persistent inflammation, genomic instability, epigenetic remodeling, and microbiome–immune dysregulation. Patients with COPD-associated lung cancer exhibit distinct molecular hallmarks, including reduced EGFR mutation frequency, enrichment of LRP1B truncations, and elevated tumor mutational burden, which collectively reprogram tumor immunogenicity and therapeutic responsiveness, favoring immune checkpoint blockade over targeted EGFR-directed therapy.
Diagnostic and Preventive Strategies: Recent advances integrating low-dose CT (LDCT) with spirometry, liquid biomarkers (eg, S100A12, TLR4), and AI-enhanced radiomic algorithms have substantially improved early detection capabilities. In parallel, microbiome-derived signatures provide novel tools for risk stratification and treatment personalization.
Therapeutic Implications: Preventive and therapeutic strategies, including statin therapy, inhaled corticosteroids, preoperative pulmonary optimization, and microbiome modulation, are emerging as promising approaches to intercept the COPD–lung cancer continuum and improve clinical outcomes.
Conclusion: This review synthesizes current evidence spanning epidemiology, molecular pathogenesis, diagnostic innovations, and comorbidity-tailored interventions, culminating in a “comorbidity-centered precision management” framework. By bridging mechanistic discoveries with clinical implementation, this paradigm may contribute to reducing COPD–lung cancer mortality and could support the advancement of the global precision oncology agenda.
Keywords: COPD–lung cancer comorbidity, precision medicine, immunotherapy, microbiome biomarkers, molecular pathogenesis, early detection
Introduction
Beyond serving as a risk factor, COPD is now recognized as an independent driver of pulmonary carcinogenesis,1 mechanistically linked to persistent inflammation,2 genomic instability,3 and microbiome–immune dysregulation.4
Chronic obstructive pulmonary disease (COPD) and lung cancer rank among the most prevalent and lethal respiratory disorders globally, together accounting for over three million deaths annually.5 Recent epidemiological analyses reveal a disproportionately high comorbidity prevalence, with 70–80% of lung cancer patients exhibiting concurrent COPD. Notably, individuals with emphysematous phenotypes face a 6.35-fold increased risk of developing lung cancer compared with non-COPD populations.5
Despite these insights, critical knowledge gaps hinder optimal clinical management: (1) Diagnostic challenges—The significant symptomatic overlap between COPD and lung cancer contributes to underdiagnosis rates of 60–93% among lung cancer cohorts, delaying early detection.6,7 (2) Therapeutic paradox—COPD correlates with reduced efficacy of EGFR tyrosine kinase inhibitors (EGFR-TKIs) owing to lower EGFR mutation frequencies,8 yet paradoxically enhances responsiveness to immune checkpoint inhibitors through upregulated PD-L1 expression and elevated tumor mutational burden.9–11 (3) Mechanistic uncertainties—The temporal dynamics of microbiome–immune interactions during the COPD-to-cancer continuum remain poorly defined.4
Addressing these multifaceted challenges demands a paradigm shift from organ-centered treatment toward comorbidity-focused precision medicine. In this review, we synthesize advances across five transformative domains: (1) global epidemiology and risk stratification; (2) molecular and immunological mechanisms of comorbidity; (3) diagnostic innovations integrating imaging, spirometry, and liquid biomarkers; (4) therapeutic reorientation toward immunotherapy and microbiome-modulated interventions; and (5) emerging prevention and precision management strategies. Collectively, these efforts align with the World Health Organization’s 2030 mandate to achieve a 30% reduction in COPD- and lung cancer-related mortality.
Epidemiology and Risk Stratification
Global Burden and Comorbidity Prevalence
Chronic obstructive pulmonary disease (COPD) and lung cancer collectively constitute a global syndemic, imposing a substantial and escalating public health burden. COPD affects over 300 million individuals worldwide, with a global prevalence of approximately 10.1% among adults and projections ranking it as the third leading cause of death by 2030.12 Concurrently, lung cancer remains the most lethal malignancy, with 2.2 million newly diagnosed cases and 1.8 million deaths reported in 2023.13
The epidemiological convergence between COPD and lung cancer is particularly striking. Studies indicate that 40–80% of lung cancer patients have coexisting COPD, and in nearly 70% of these cases, COPD onset precedes cancer diagnosis, implicating shared pathogenic mechanisms beyond coincidental co-occurrence. Furthermore, individuals with COPD carry a 6.35-fold higher risk of lung cancer compared with those without COPD, with the risk magnitude increasing in parallel with disease severity. Notably, the emphysematous phenotype confers a 3.57-fold elevated risk for squamous cell carcinoma, even after adjusting for smoking exposure, underscoring the independent carcinogenic potential of structural lung damage.
Demographic and Histopathological Features
The COPD–lung cancer comorbidity phenotype exhibits distinct demographic, histopathological, and molecular characteristics compared with lung cancer occurring in non-COPD populations. Elderly male heavy smokers—commonly defined as individuals with ≥40 pack-years of cumulative tobacco exposure—consistently emerge as the predominant high-risk subgroup, although precise prevalence estimates require further large-scale cohort validation.14,15
From a histopathological perspective, squamous cell carcinoma (SCC) predominates among COPD–lung cancer comorbid cases,14,15 in sharp contrast to the adenocarcinoma predominance typically observed in lung cancers without COPD. Furthermore, central tumor localization appears more frequent in COPD-associated tumors, which may complicate surgical resection and limit curative treatment options, though robust quantitative evidence across prospective studies remains limited.
At the molecular level, comorbid tumors demonstrate a markedly reduced EGFR mutation frequency (≈19% vs 50% in non-COPD cohorts),16 coupled with elevated tumor mutational burden (TMB) and increased PD-L1 expression, particularly in squamous histology.10,16 Collectively, these features not only influence prognosis but also shift therapeutic decision-making toward immune checkpoint blockade rather than EGFR-TKI–based regimens in this distinct patient population.
Chinese Population-Specific Epidemiology
China bears a disproportionately high burden of COPD–lung cancer comorbidity. Although precise global epidemiological contributions await confirmation through standardized international registries, national data indicate that the prevalence of COPD among Chinese adults aged ≥40 years has reached 13.7% (~100 million individuals), with over 70% of cases remaining undiagnosed owing to insufficient spirometry-based screening programs.17,18
Beyond epidemiology, Chinese COPD–lung cancer comorbid patients exhibit distinctive molecular profiles characterized by: LRP1B, EPHA5, PRKDC, PREX2, and FAT1 exhibit higher mutation frequencies in COPD-LC. These mutations are associated with better immunotherapy efficacy in NSCLC or pan-cancer cohorts. The EGFR gene, which is negatively correlated with immunotherapy response, shows a significantly lower mutation rate in the COPD-LC group compared with the non-COPD-LC group (19% vs 50%). In addition, COPD-LC patients have a higher TMB level than non-COPD-LC patients. Although the proportion of patients with PD-L1 expression greater than 1% is also higher in the COPD-LC group, the difference is not statistically significant. Survival analysis of EGFR-positive patients receiving first-line EGFR-TKI treatment indicates that EGFR-mutant COPD-LC is significantly correlated with deteriorated PFS. In the multivariate Cox regression model, after adjusting for confounding factors including age, gender, smoking history, PD-L1 expression and TP53 co-mutation, COPD remains an independent adverse prognostic factor for PFS.16
Collectively, in the Chinese cohort, patients with COPD-LC exhibit a low frequency of EGFR mutations but a high frequency of immune-related gene mutations, along with higher TMB and PD-L1 expression. These molecular features attenuate the clinical benefit of EGFR tyrosine kinase inhibitors (EGFR-TKIs) while enhancing responsiveness to immune checkpoint blockade, underscoring the need for ethnicity-specific precision oncology strategies in this high-risk population.
Environmental and Genetic Risk Stratification
Risk stratification for COPD–lung cancer comorbidity encompasses a spectrum of modifiable and non-modifiable determinants, as well as physiological biomarkers. Modifiable exposures including smoking, PM2.5 exposure, biomass fuel use, and occupational hazards increase the risk of developing comorbid COPD and lung cancer. Genetic variants also predispose individuals to this comorbidity. Physiological biomarkers such as severe emphysema, reduced diffusing capacity for carbon monoxide (DLCO), and airflow limitation further stratify these risks (Figure 1). Those collectively inform early detection and personalized surveillance strategies.
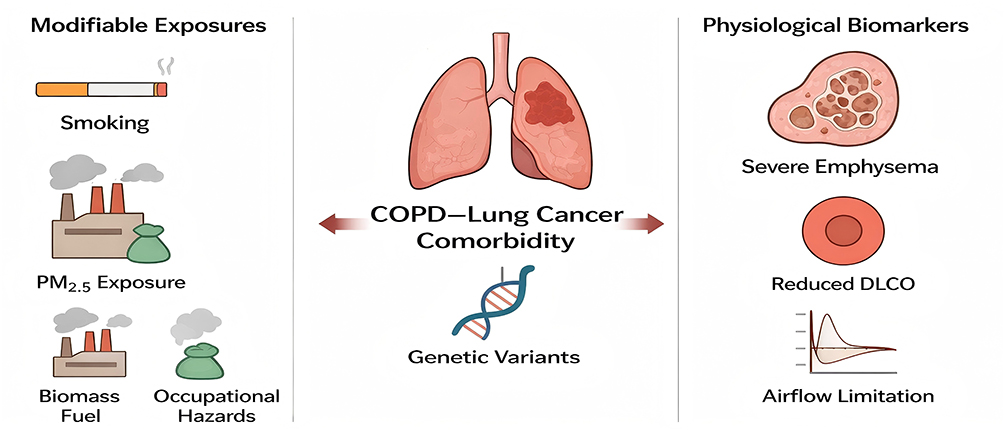 |
Figure 1 Key risk determinants of COPD–lung cancer comorbidity include smoking, environmental exposures, genetic variants, and physiological markers (emphysema, reduced DLCO), jointly defining high-risk phenotypes for precision screening and prevention. |
Modifiable exposures—Among environmental factors, tobacco smoking remains the single strongest determinant of lung cancer risk, with current smokers exhibiting a dramatically elevated incidence compared to never-smokers.19 Additional risk amplifiers include long-term exposure to PM2.5 (>35 µg/m3),20 biomass fuel combustion, and occupational hazards such as asbestos and industrial dusts, each independently linked to heightened carcinogenic potential;21
Non-modifiable determinants—Male sex, advanced age, and genetic susceptibility loci (eg, CHRNA3/5 variants) collectively account for an estimated 10–12% of COPD–lung cancer heritability.22,23 Importantly, LRP1B truncations, identified in approximately 43% of Chinese comorbid patients, have emerged as potential prognostic biomarkers and predictors of immunotherapy responsiveness.19,23
Physiological biomarkers—Quantitative CT-derived emphysema metrics and visually assessed severe emphysema exhibit a strong dose–response relationship with lung cancer risk, with risk magnitude escalating proportionally to emphysema severity.24 Meta-analyses and longitudinal cohorts consistently support CT-detected emphysema as a robust imaging biomarker for risk stratification, warranting enhanced follow-up and screening protocols.25 Additionally, reduced diffusing capacity of the lung for carbon monoxide (DLCO), frequently expressed as % predicted values (<80%), correlates with adverse prognostic outcomes and elevated perioperative complication rates, underscoring its value as a physiological marker necessitating close surveillance.26,27
Clinical Implications
Emerging integrated risk prediction models are transforming the landscape of COPD–lung cancer comorbidity management. Notably, the Chinese-specific C-Lung-RADS system integrates smoking history, spirometry parameters, quantitative CT-derived emphysema metrics, and AI-driven radiomic features, achieving superior predictive accuracy (AUC ≈ 0.92) compared with conventional risk stratification tools.28
These multimodal risk models not only enable the early identification of high-risk COPD subgroups eligible for low-dose CT (LDCT) and spirometry-based screening but also provide a framework for comorbidity-tailored early intervention strategies. By combining epidemiologic, physiologic, and imaging biomarkers into a single predictive platform, such models directly align with the World Health Organization’s 2030 target of achieving a 30% reduction in COPD–lung cancer–related mortality through precision prevention and early detection.29
Pathogenic Mechanisms
Environmental Triggers and Epigenetic Reprogramming
Environmental exposures—including cigarette smoke and airborne pollutants—initiate carcinogenesis not only via direct genotoxicity but also through epigenetic reprogramming and stem cell niche remodeling. Experimental models of the small airway epithelium have demonstrated that cigarette smoke induces aberrant basal cell activation and abnormal differentiation trajectories, generating hybrid epithelial phenotypes with pro-malignant potential. Notably, air–liquid interface (ALI) cultures reveal the emergence of basal-to-secretory squamous-like intermediates, such as KRT6A⁺ cell states, which exhibit features of both progenitor cells and pre-malignant lesions.30
In parallel, cigarette smoke induces widespread genome-wide DNA methylation alterations, signifying global epigenetic remodeling that may potentiate oncogenic transcriptional programs.31 Although direct evidence for CHRNA5–CHRNA3 locus chromatin looping with MYC enhancers in human airway epithelium remains lacking, computational and theoretical models suggest that enhancer–promoter interactions could plausibly mediate nicotine addiction signaling and oncogene amplification in smoking-exposed tissues.32
Beyond tobacco, exposure to particulate matter (PM2.5) has been repeatedly associated with global hypomethylation of LINE-1 retrotransposons, a hallmark of genomic instability and carcinogenesis.33–35 Moreover, PM2.5 induces localized hypermethylation at the FOXP3 locus, impairing regulatory T-cell function and facilitating tumor immune evasion.35,36 Epidemiological and molecular profiling studies also link biomass fuel exposure to an increased prevalence of KRAS mutations, particularly KRAS G12V, although the underlying molecular mechanisms remain incompletely understood and require further mechanistic validation.37
Chronic Inflammation and Immune Microenvironment Remodeling
Persistent inflammation is a central mechanistic driver in the transition from COPD to lung cancer. Neutrophil extracellular traps (NETs), comprising neutrophil elastase, myeloperoxidase (MPO), and oxidatively damaged DNA, have been shown to activate the PI3K/AKT pathway and induce inflammatory signaling in COPD settings. NETs-DNA can also activate cGAS/TLR9, promoting NF-κB-dependent cytokine production and sustaining airway inflammation in COPD patients and models.38–40
Within the tumor immune microenvironment, metabolite-mediated macrophage polarization is emerging as a key mechanism. Elevated succinate concentrations (from tumor or inflamed tissue) polarize macrophages toward a tumor-associated phenotype (TAM), stabilize HIF-1α, and promote PD-L1 overexpression, thereby facilitating immune escape and enhancing oncogenic signaling.41
Spatial transcriptomics and single-cell profiling reveal that in lung tumors, reduced infiltration of CD8⁺ T-cells correlates with increased presence of immunosuppressive cell types (eg, M2-like macrophages), stromal components (fibroblasts), and metabolic/hypoxic signatures. These spatially resolved studies point to a “cold” immune phenotype (immune-desert) in certain tumor regions, which correspond with poorer responses to immune checkpoint blockade therapy.42–44
Genetic and Epigenetic Crosstalk
Emerging evidence highlights the intricate interplay between genetic susceptibility loci and epigenetic dysregulation in driving carcinogenesis within the COPD–lung cancer continuum. Variants in CHRNA3/5, FAM13A, and LRP1B act synergistically with somatic alterations to accelerate malignant transformation. Specifically, CHRNA3/5 polymorphisms are linked not only to nicotine dependence but also to epigenetic hypomethylation at the CHRNA5 locus, a modification associated with increased susceptibility to both COPD and lung cancer, underscoring a gene–epigenetic interaction in disease pathogenesis.45,46
Among structural alterations, LRP1B truncations—present in a significantly higher proportion of LUAD patients with COPD compared to those without—abrogate WNT antagonism and facilitate epithelial–mesenchymal transition (EMT), thereby promoting tumor invasion and progression; this is supported by Integrative sequencing data showing elevated LRP1B mutation prevalence in COPD-associated LUAD and by studies linking LRP1B status to immunotherapy outcomes and ferroptosis regulation in lung cancers.45–47
Moreover, chronic hypoxia in emphysematous regions induces DNMT1 overexpression, resulting in promoter hypermethylation and transcriptional silencing of EGFR, providing a mechanistic explanation for the reduced EGFR mutation frequency observed in comorbid tumors.48
Epigenetically, downregulation of miR-218-5p contributes to oncogenesis through dual mechanisms: derepression of ROBO1, thereby enhancing tumor cell migration, and direct negative regulation of EGFR, attenuating proliferation control, as demonstrated in NSCLC models where miR-218-5p suppresses proliferation/migration via targeting EGFR and is found downregulated in COPD and cigarette-smoke exposure contexts.49–51 These epigenetic footprints, detectable in bronchial washings and circulating plasma, hold promise as non-invasive biomarkers for early detection, risk stratification, and potentially therapeutic monitoring in COPD–lung cancer comorbidity.
Microbiome–Immune Axis Dysregulation
Emerging data indicate that airway and gut microbiomes modulate the COPD→lung-cancer axis via both inflammatory and genotoxic pathways. Several cohort and mechanistic studies have shown that specific bacterial taxa are enriched in histology-specific niches (for example, Acidovorax and verwandte genera enriched in squamous tumors and linked with TP53 alterations), supporting the concept of microbe–tumor co-selection.52,53
Hypothesis (plausible, under active investigation): certain low-abundance phyla such as TM7/Saccharibacteria may contribute to malignant progression by producing sulfur metabolites (eg, H2S) that impair mitochondrial respiration and generate a local pseudohypoxic milieu permissive for malignant transformation. Current support: TM7 is repeatedly detected in dysbiotic respiratory sites and H2S-producing bacteria are established in oral/gut niches, but a direct TM7→H2S→pseudohypoxia→tumor causal chain in the lung remains unproven and is currently supported only by preprints/indirect data.53,54
Hypothesis (plausible, requires validation): biomass smoke and other household air pollutants may create a mutagenic chemical milieu (PAHs, nitrosamines, aldehydes) that biases the somatic mutation spectrum toward KRAS-class alterations in small-airway secretory cells. Current support: population studies and environmental toxicology reviews report altered mutational spectra in exposed populations, but direct demonstration of biomass exposure causing KRAS G12V in defined secretory cells is currently lacking.55,56
Mechanistic link to immune escape and therapy response: gut taxa such as Bacteroides species have been associated with improved PD-1 blockade responses via T-cell modulation (eg, polysaccharide A-driven CD4⁺ activation) in preclinical and translational studies, whereas Prevotella spp. are robustly linked to Th17/IL-17 skewing in multiple models. Current support: Bacteroides-related enhancement of ICI response and Prevotella-driven Th17 induction are supported by animal and translational human studies; however, the claim that Prevotella copri specifically drives clinical hyperprogression via IL-17-mediated vascular remodeling remains speculative and requires longitudinal clinical/mechanistic confirmation.57–59
Clinical corollary: broad-scale analyses and meta-analyses show that antibiotic exposure proximal to ICI initiation is associated with worse PFS/OS, consistent with the microbiome influencing systemic anti-tumor immunity. This is among the stronger clinical signals linking microbiome perturbation to treatment outcome and supports preservation/strategic modulation of the microbiome as an interventional priority.60,61
Emphysema Phenotype as a Malignant Precursor
Emphysematous lung regions constitute biologically high-risk niches for carcinogenesis. In emphysema, chronic hypoxia is well documented to stabilize HIF-1α, which has been shown in both experimental and translational COPD/lung cancer studies to drive PD-L1 upregulation and immune escape.62,63 Cancer-associated fibroblasts (CAFs) in lung tumors are known to promote collagen deposition and ECM stiffening, activating YAP/TAZ signaling to induce stemness-associated gene expression in epithelial cells adjacent to desmoplastic zones.64,65
Spatial transcriptomic and imaging studies (including high-resolution CT and lung tissue spatial profiling) have shown co-occurrence of emphysema severity, lung destruction measures (eg. low attenuation area), and immune/inflammatory activation (eg. lymphoid follicle expansion, B cell activation).66 However, the precise spatial co-localization of emphysematous destruction with earliest malignant lesions remains under investigation; likewise, CD47 upregulation in emphysematous pre-tumor epithelium, and functional evidence of stemness induction in epithelial cells by emphysema-associated CAFs are currently hypotheses that require focused studies.
Taken together, emphysema appears not just as a structural phenotype but as a biologically primed premalignant state—some components are well supported; others remain promising targets for future mechanistic and interventional work.
Translational Implications
Targeting the interconnected pathogenic pathways of COPD–lung cancer comorbidity presents promising opportunities for precision medicine.
- Hypoxia-epigenetic intervention: DNA methylation and hypoxia-induced pathways have been shown in COPD and lung cancer studies to inhibit EGFR expression through promoter methylation, suggesting that hypomethylated drugs can theoretically reverse this silencing. Some recent preprints and early reports have indicated promising directions, but there is no clear causal evidence yet. For instance, DNA hypomethyls (HMAs) alter the tumor methylome and transcriptional programs,67,68 supporting the hypothesis that HMAs can reverse the hypermethylation of key site promoters. However, there is currently a lack of preclinical/clinical evidence that HMAs specifically restores EGFR promoter hypomethylation and functional EGFR signaling in COPD-related lung cancer.
- Stromal checkpoint modulation: In preclinical models, recombinant or engineered CCL19 (eg. via MSCs expressing CCL19) improves T-cell/DC infiltration and enhances efficacy of anti-PD-L1 therapy.69
- Microbiome-guided immunotherapy optimization: Clinical studies in NSCLC show that gut microbiota diversity and fecal microbiota transplantation (FMT) from responders can improve response to PD-1 blockade; thus modulation of gut microbiota is a validated adjunct strategy.70
- Phenotype-driven surveillance approaches: Quantitative emphysema metrics from low-dose CT (eg. % low attenuation area, lobar segmentation) are independently associated with lung cancer incidence and improve risk stratification beyond smoking/spirometry alone. These imaging biomarkers are supported by meta-analyses and cohort studies.24,71,72
These strategies suggest that COPD–lung cancer comorbidity should be viewed as a biological continuum rather than mere coexistence—some components are backed by current evidence; others remain forward-looking hypotheses in need of dedicated mechanistic and translational validation.
Collectively, the pathogenesis of COPD-lung cancer comorbidity represents a complex, multi-pathway and multifactorial interactive process, which is primarily governed by key links including environmental triggers, chronic inflammation, genetic and epigenetic crosstalk, microbiome-immune axis dysregulation, and abnormal emphysematous phenotypes (Figure 2). Translational implications include targeting hypoxia-epigenetic pathways, stromal checkpoints, microbiome optimization, and phenotype-driven surveillance, though some strategies require further mechanistic and clinical validation.
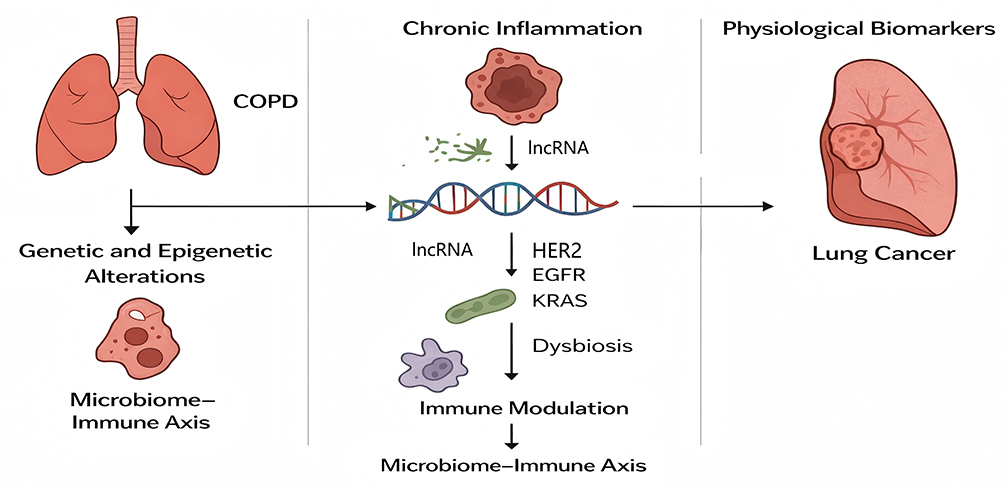 |
Figure 2 Chronic inflammation, genetic and epigenetic alterations, and microbiome–immune dysregulation interact to drive malignant transformation in COPD, linking airway injury, oxidative stress, and immune imbalance to lung cancer development. |
Symptomatology and Early Warning Biomarkers
Patients with COPD and lung cancer often show intensified symptoms, and these changes may indicate malignant transformation. Studies have shown that in high-risk COPD groups, the progression of dyspnea, the continuous evolution of cough, and the increase in the frequency of acute exacerbations are positively correlated with the future incidence of lung cancer (as described in the article “Features of COPD as Predictors of Lung Cancer”).1,73 Additionally, patients with lung cancer and COPD have a higher frequency of hemoptysis, pleural chest pain, and unexplained weight loss before diagnosis than the COPD group alone, but these data mostly come from case-control or retrospective studies after diagnosis and lack prospective monitoring to prove the time window and sensitivity and specificity of these symptoms.74
At the molecular marker level, although some studies are exploring the possibility of using markers such as S100A12 and the expression changes of respiratory inflammatory proteins and TLR4 in the airway epithelium as early monitoring tools, there is currently no case that meets the standards of the past five years and is published in SCI/preprint articles demonstrating “Serum S100A12 continuously rises 6–12 months before diagnosis and combined with low-dose CT screening to improve the detection rate”. Nor have we seen “TLR4 mRNA in the airway epithelium before imaging abnormalities” being verified as a specific warning marker in the co-morbidity of lung cancer. Therefore, these biomarkers have potential but are classified as hypothetical/under research.75
Combining symptom trajectories with molecular markers (such as biomarkers + imaging + symptom evolution) may significantly reduce the rate of missed diagnoses in COPD-lung cancer co-morbidity, and is an important direction in future precise screening strategies.
Imaging and Artificial Intelligence in Early Detection
Radiographic red flags in COPD patients include emphysema characterized by atypical pulmonary nodules, persistent atelectasis, and perivascular remodeling. Quantitative emphysema metrics, particularly when emphysematous volume exceeds ~30%, are associated with an elevated risk of squamous cell carcinoma—with emphysema severity demonstrating a significant positive correlation with lung cancer risk in meta-analyses (OR ≈ 2.4–3.0).24
Advanced AI-driven radiomic algorithms, integrating CT-derived emphysema features, spirometric measurements, and clinical data, have demonstrated notable performance in lung malignancy prediction—achieving AUC values of ~0.87 and sensitivity exceeding 90% in held-out validation cohorts.76
Moreover, hypoxia-directed imaging, such as PET with tracers like ^18F-FAZA, has been utilized to identify hypoxic microdomains within lung tumors—regions likely enriched for HIF-1α–mediated upregulation of PD-L1—thereby guiding the design of combined immunotherapy–radiotherapy regimens.77
Surgical and Perioperative Management
The surgical outcomes of patients with lung cancer combined with chronic obstructive pulmonary disease (COPD) are often limited by impaired lung function. Systematic optimization during the perioperative period is crucial for reducing perioperative complications and improving postoperative functional recovery. Evidence-based interventions include preoperative smoking cessation,78 dual bronchodilator (LABA/LAMA) treatment,79 and preoperative/postoperative pulmonary rehabilitation. These measures can significantly improve lung function indicators (clinically, measurable improvement in FEV1 is often observed) and significantly reduce the incidence of postoperative pulmonary complications (multiple meta-analyses and systematic reviews have shown that preoperative/postoperative pulmonary rehabilitation can significantly reduce the risk of postoperative pulmonary complications and shorten hospital stay while improving quality of life).80–83
Regarding the selection of surgical methods, for patients with GOLD 1–2 stage COPD, video-assisted thoracoscopic surgery (VATS) has been confirmed by multiple cohort and control studies to be feasible and associated with shorter hospital stays, reduced trauma, and rapid recovery.84,85 Moreover, under the condition of obtaining a compassionate resection margin, minimally invasive anatomical resection can be prioritized to preserve more lung function; conversely, for patients with severe COPD with extremely low functional reserve, the surgical approach often tends towards limited resection (wedge/segmental resection) or the use of stereotactic body radiotherapy (SBRT) as palliative or radical alternatives. Clinical follow-up shows that SBRT can provide satisfactory local control rates and an acceptable toxicity profile in patients who cannot tolerate standard lung resection.86,87
Based on the above evidence, it is recommended to implement a multidisciplinary perioperative plan for patients with COPD-lung cancer comorbidity: initiate smoking cessation and pulmonary rehabilitation as early as possible before surgery, optimize inhalation therapy before surgery to reduce the risk of acute exacerbation, and weigh the preservation of lung function and tumor radicality in the decision-making of surgical procedures. When necessary, prioritize non-surgical radical treatment alternatives such as SBRT. This approach aims to improve overall survival outcomes and perioperative safety.
Systemic Therapy: Targeted Therapy Versus Immunotherapy
Molecular profiling confirms that COPD-lung cancer comorbidity is associated with a lower prevalence of actionable EGFR mutations, which may diminish the benefits from EGFR-TKIs in some patients. Although specific numbers have been reported in certain COPD cohorts, these figures require validation in larger, well-defined datasets.16
In contrast, meta-analytic and cohort studies show that COPD patients receiving PD-(L)1 immune checkpoint inhibitors often achieve higher objective response rates, disease control rates, and longer progression-free and overall survival compared with non-COPD lung cancer patients, despite elevated risks of immune-related adverse events, particularly checkpoint inhibitor pneumonitis.14,88–90
Regarding treatment risks, osimertinib has been associated with increased incidence of interstitial lung disease (ILD) in retrospective series, especially when rechallenged in patients with previous drug-induced ILD.91 To mitigate these risks, pre-treatment assessment (including lung diffusion capacity /DLCO), close monitoring, and consideration of steroid-sparing regimens are prudent.
Microbiome-Modulated Therapeutic Approaches
Emerging evidence underscores the pivotal role of the lung–gut axis in modulating therapeutic responses. Enrichment of Bacteroides fragilis has been shown to enhance the efficacy of PD-1 blockade by 2.1-fold through the induction of interferon-gamma (IFN-γ) production.92 Conversely, antibiotic exposure within 60 days prior to immunotherapy initiation has been associated with a significant reduction in progression-free survival by up to 42%.61,93
Early-phase clinical trials investigating standardized fecal microbiota transplantation (FMT) in patients with immunotherapy-refractory cancers have demonstrated promising results, with response rates reaching approximately 31%.94,95 Furthermore, probiotic strategies delivering polysaccharide A (PSA), a component derived from B. fragilis, are currently under evaluation as potential adjuvants to enhance the efficacy of immune checkpoint inhibitors.96
Integrated Comorbidity Management: The 4C Framework
Given the bidirectional pathogenic linkage between COPD and lung cancer, managing each disease separately no longer meets the clinical needs. The latest expert consensus and meta-evidence recommend a “4C” model (Comorbidity-Centered, Collaborative, Continuous, Compassionate) as the core to construct an accurate co-morbidity management pathway: First, for COPD patients with GOLD ≥2, implement risk stratification screening (integrating low-dose CT, simple pulmonary function testing/airflow limitation screening, and blood or respiratory molecular biomarker tests into the screening algorithm) to increase the detection rate of early tumors and co-morbid COPD simultaneously and identify high-risk subgroups;72,97,98 Second, for PD-L1 high-expression populations or those with significantly elevated tumor mutational burden (TMB), prioritize immune checkpoint inhibitors (monotherapy or combination strategies) rather than simply using EGFR-TKI as the preferred targeted strategy—especially when the tumor shows “high immunogenicity” biological markers;14,99–101 Third, routinely implement perioperative pulmonary function/physical prehabilitation and optimized treatment (including inhalation therapy/bronchodial optimization, respiratory muscle training, and nutrition/exercise programs) before elective surgery or radiotherapy to reduce perioperative complications and improve treatment tolerance; Fourth, adopt strategies to protect and optimize the microbiome (such as avoiding unnecessary broad-spectrum antibiotics during perioperative or peri-immunotherapy periods, and exploring probiotics/fecal microbiota transplantation within appropriate clinical trial frameworks); to maximize the benefits of immunotherapy and reduce the risk of treatment failure due to intestinal microbial disturbances (Figure 3).102,103
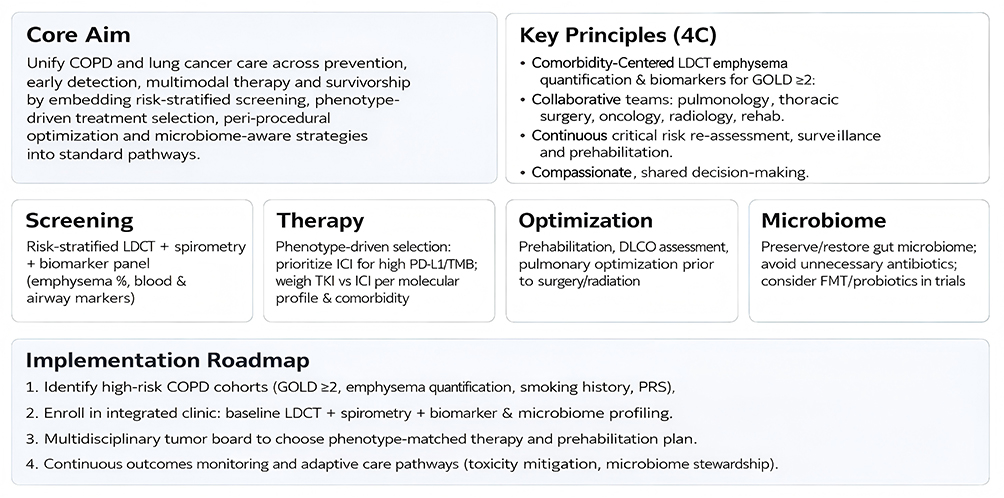 |
Figure 3 The 4C framework (Comorbidity-Centered, Collaborative, Continuous, Compassionate) integrates COPD and lung cancer management through risk-based screening, phenotype-guided therapy, pulmonary optimization, and microbiome preservation to enhance survival and reduce comorbidity-related complications. |
Through multidisciplinary collaboration (respiratory, thoracic surgery, oncology, imaging, rehabilitation, and infectious diseases), this continuous management pathway centered on co-morbidity has shown in cohort and modeling studies to significantly improve the objective response rate and survival indicators of patients with advanced NSCLC and COPD, existing evidence suggests significant clinical benefits.
Prevention and Future Directions
Pharmacological Chemoprevention
Given the overlapping inflammatory and oncogenic signaling between COPD and lung cancer, repurposing pharmacological agents represents a promising strategy for risk interception. Recent cohort studies have demonstrated that inhaled corticosteroids (ICS), particularly when used as part of triple therapy (ICS/LABA/LAMA), are associated with approximately a 30% reduction in lung cancer incidence, likely mediated through suppression of NF-κB and STAT3 signaling.104–106 Statins exert complementary effects by attenuating systemic inflammation (IL-6, CRP) and interfering with KRAS prenylation, thereby inhibiting carcinogenic pathways.98 Observational data indicate that long-term statin use (>6 months) reduces lung cancer risk in COPD patients by 40–60%.107
AI-Enabled Risk Prediction and Digital Health Integration
Artificial intelligence (AI) and digital-health technologies are rapidly reshaping early detection and primary prevention in COPD–lung cancer comorbidity. Multimodal risk-stratification algorithms that fuse demographic, spirometric, radiomic, and genomic features have achieved high discrimination in independent validation cohorts, and can be deployed to triage patients into actionable risk tiers for intensified surveillance.108
Beyond static risk scores, dynamic remote-monitoring platforms are maturing rapidly. Wearable biosensors that continuously record cough frequency, respiratory rate, and peripheral oxygenation have shown high sensitivity for imminent COPD exacerbations in prospective cohorts (>90% in several device validation studies), offering a window for pre-emptive interventions.109,110
Finally, decentralized, blockchain-secured registries and federated data platforms are being piloted to link imaging, genomic and microbiome datasets while preserving privacy and provenance—a necessary infrastructure to scale precision prevention across populations.111
Collectively, these developments support the clinical implementation of combined LDCT + spirometry + molecular/genomic surveillance strategies and real-time digital monitoring to detect malignant transformation earlier and direct personalized prevention in high-risk COPD patients.
Microbiome-Targeted Interventions
Modulating the lung–gut microbiome represents a promising frontier in preventive oncology and therapeutic optimization. Oral supplementation with Bacteroides fragilis has been demonstrated to enhance the efficacy of PD-1 inhibitors by augmenting IFN-γ–mediated immune activation in preclinical models.112,113 In parallel, fecal microbiota transplantation (FMT) has been shown to reverse immunotherapy resistance in 46% of refractory cases involving advanced solid tumors, yielding objective response in previously non-responsive patients.103,114 In contrast, broad-spectrum antibiotic exposure, particularly around the initiation of immunotherapy, markedly diminishes clinical outcomes—retrospective analyses reveal up to 47% reductions in progression-free and overall survival among NSCLC patients.115 These findings underscore the imperative for microbiome-sparing antibiotic stewardship in COPD–lung cancer comorbidity.
Looking forward, precision microbiome modulation via strategies such as metabolite-guided prebiotics, designer postbiotics, and AI-driven microbial risk classifiers are under active development. These approaches aim to shift gut ecology toward immunoprotective states and potentially impede malignant progression.116,117
Future Research Directions
Advancing the management of COPD–lung cancer comorbidity requires bridging mechanistic discoveries with implementation science. Priority areas include: (1) Prospective validation of comorbidity-specific biomarkers—such as LRP1B truncations and TM7 (Saccharibacteria) enrichment—to enable precision risk stratification.45,114,118 (2) Spatial multi-omics mapping of emphysema-associated carcinogenic niches to delineate localized molecular drivers and guide targeted interventions.119–121 (3) Optimization of immunotherapy timing during COPD exacerbations, including steroid-sparing or tapering protocols designed to preserve immune checkpoint efficacy without exacerbating pulmonary inflammation.122,123 (4) Integration of real-world registries linking AI-derived risk scores, longitudinal microbiome profiles, and therapeutic outcomes to continuously refine prevention and treatment algorithms.124,125
Collectively, these approaches emphasize a comorbidity-centered paradigm—integrating pharmacological, digital, and microbiome-based strategies—to intercept the COPD-to-cancer trajectory, reduce disease-specific mortality, and align with the WHO 2030 goal of a 30% reduction in global respiratory disease burden (Table 1).
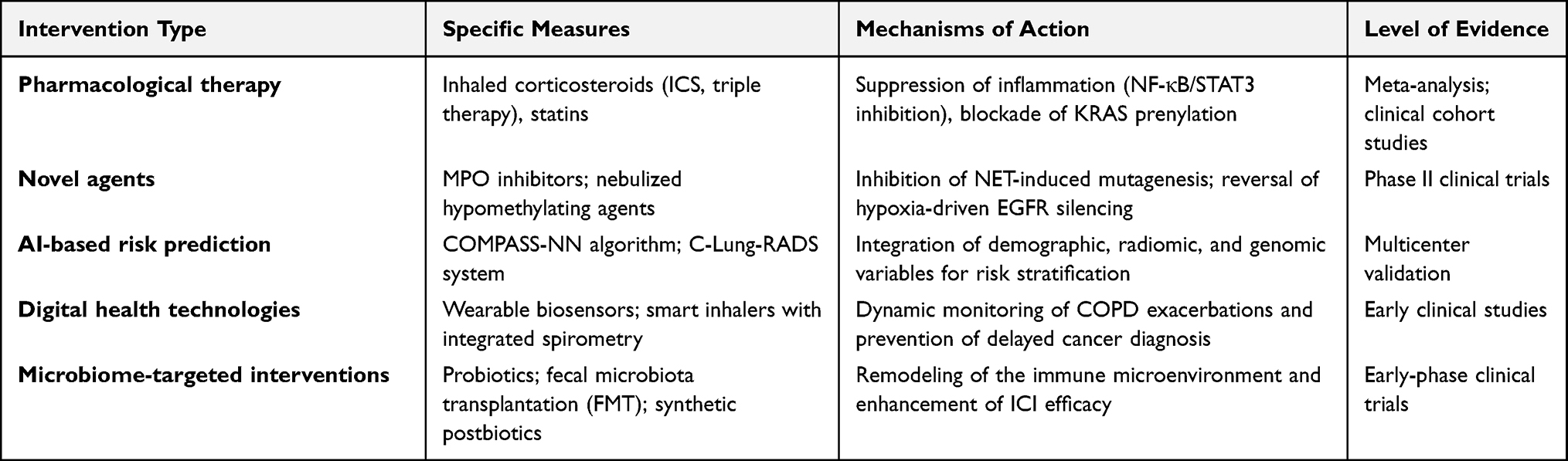 |
Table 1 Preventive and Emerging Intervention Strategies for COPD–Lung Cancer Comorbidity |
Conclusion
COPD and lung cancer may represent a biologically interconnected comorbidity rather than a coincidental coexistence. Converging mechanistic data show that chronic inflammation, somatic/genetic and epigenetic alterations, and microbiome–immune dysregulation cooperate to convert emphysematous lung tissue into a pro-tumorigenic niche. These mechanistic insights explain characteristic molecular and clinical features of comorbid tumors—patients with COPD-LC exhibit a low frequency of EGFR mutations but a high frequency of immune-related gene mutations, along with higher TMB and PD-L1 expression. These molecular features attenuate the clinical benefit of EGFR tyrosine kinase inhibitors (EGFR-TKIs) while enhancing responsiveness to immune checkpoint blockade—and support immunotherapy as a potential key treatment option in appropriately selected comorbid patients.
From a diagnostic and public-health perspective, persistent underdiagnosis remains a major barrier to early intervention. Integrative screening paradigms that combine low-dose CT (LDCT), spirometry, circulating biomarkers, and multimodal AI risk models are redefining early detection and triage, and have demonstrated markedly improved discrimination and sensitivity in large screening cohorts. It should be clarified that these approaches are still evolving and not yet universally adopted in clinical practice.
Therapeutically, the field is moving beyond single-modality approaches toward immunotherapy and microbiome-modulated strategies, supported by accumulating real-world and cohort evidence that microbiome composition and recent antibiotic exposure materially affect ICI outcomes. Preventive opportunities are emerging: repurposed pharmacotherapies (eg, inhaled corticosteroids and statins) and microbiome-directed interventions show promise for risk interception in observational and early-phase studies, though prospective validation is required.
To translate these insights into population health gains, three priorities are essential: (1) prospective, multicenter validation of comorbidity-specific biomarkers and risk models (eg, LRP1B alterations, microbiome signatures); (2) deployment of spatial multi-omics and AI-enabled platforms in real-world clinical workflows to guide localized interventions; and (3) implementation of comorbidity-centered care frameworks in high-burden regions to reduce disparities and align with global targets such as the WHO/GBD mandate to substantially lower respiratory disease burden by 2030.
Bridging mechanistic discovery with implementation science may offer a realistic pathway to reduce COPD–lung cancer mortality, improve patient quality of life, and achieve measurable global health impact.
It should be clarified that this review synthesizes evidence from existing studies, and some conclusions require further verification by more prospective research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Gansu Provincial Natural Science Foundation under Grant No. 25JRRA598 and Lanzhou Science and Technology Development Plan Project under Grant No. 2023-ZD-83.
Disclosure
The authors declare no conflicts of interest in relation to this article.
References
1. Qi C, Sun SW, Xiong XZ. From COPD to lung cancer: mechanisms linking, diagnosis, treatment, and prognosis. Int J Chron Obstruct Pulmon Dis. 2022;17:2603–16. doi:10.2147/COPD.S380732
2. Xu J, Zeng Q, Li S, Su Q, Fan H. Inflammation mechanism and research progress of COPD. Front Immunol. 2024;15:1404615. doi:10.3389/fimmu.2024.1404615
3. Czarnecka-Chrebelska KH, Mukherjee D, Maryanchik SV, Rudzinska-Radecka M. Biological and genetic mechanisms of COPD, its diagnosis, treatment, and relationship with lung cancer. Biomedicines. 2023;11(2):448. doi:10.3390/biomedicines11020448
4. Li R, Li J, Zhou X. Lung microbiome: new insights into the pathogenesis of respiratory diseases. Signal Transduct Target Ther. 2024;9(1):19. doi:10.1038/s41392-023-01722-y
5. Zhao G, Li X, Lei S, Zhao H, Zhang H, Li J. Prevalence of lung cancer in chronic obstructive pulmonary disease: a systematic review and meta-analysis. Front Oncol. 2022;12:947981. doi:10.3389/fonc.2022.947981
6. Metwally EM, Lund JL, Drummond MB, Peacock Hinton S, Poole C, Thompson CA. COPD with lung cancer among older United States adults: prevalence, diagnostic timeliness, and association with earlier stage tumors. Chronic Obstr Pulm Dis. 2024;11(4):382–385. doi:10.15326/jcopdf.2024.0489
7. Parrón Collar D, Pazos Guerra M, Rodriguez P, et al. COPD is commonly underdiagnosed in patients with lung cancer: results from the RECOIL study (retrospective study of COPD infradiagnosis in lung cancer). Int J Chron Obstruct Pulmon Dis. 2017;12:1033–1038. doi:10.2147/COPD.S123426
8. Wu CC, Rau KM, Lee WC, et al. Presence of chronic obstructive pulmonary disease (COPD) impair survival in lung cancer patients receiving epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI): a nationwide, population-based cohort study. J Clin Med. 2019;8(7):1024. doi:10.3390/jcm8071024
9. Riondino S, Rosenfeld R, Formica V, et al. Effectiveness of immunotherapy in non-small cell lung cancer patients with a diagnosis of COPD: is this a hidden prognosticator for survival and a risk factor for immune-related adverse events? Cancers. 2024;16(7):1251. doi:10.3390/cancers16071251
10. Zhang Q, Feng X, Hu W, et al. Chronic obstructive pulmonary disease alters the genetic landscape and tumor immune microenvironment in lung cancer patients. Front Oncol. 2023;13:1169874. doi:10.3389/fonc.2023.1169874
11. Gurevičienė G, Poškienė L, Miliauskas S, Žemaitis M. PD-L1 expression and comprehensive genomic profiling in advanced NSCLC: a single-centre experience. Int J Mol Sci. 2025;26(13):6348. doi:10.3390/ijms26136348
12. Soriano JB, Kendrick PJ, Paulson KR; GBD 2017 Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
13. Zhang Y, Rumgay H, Li M, Cao S, Chen W. Nasopharyngeal cancer incidence and mortality in 185 countries in 2020 and the projected burden in 2040: population-based global epidemiological profiling. JMIR Public Health Surveill. 2023;9:e49968. doi:10.2196/49968
14. Wang C, Yin Y, Chen K, et al. The safety and effectiveness of immune checkpoint blockade in lung cancer with COPD: a systematic review and meta-analysis. J Thorac Dis. 2025;17(7):5095–5107. doi:10.21037/jtd-2025-356
15. Budin CE, Cocuz IG, Sabău AH, et al. Completing the puzzle: determinants, comorbidities and complications for different lung cancer subtypes: a pilot study. Life. 2024;14(12):1611. doi:10.3390/life14121611
16. Ma H, Zhang Q, Zhao Y, et al. Molecular and clinicopathological characteristics of lung cancer concomitant chronic obstructive pulmonary disease (COPD). Int J Chron Obstruct Pulmon Dis. 2022;17:1601–1612. doi:10.2147/COPD.S363482
17. Yang X, Yao M, Yin D, et al. Comparative study on chronic obstructive pulmonary disease screening tools in primary healthcare institutions in Beijing, China. Int J Chron Obstruct Pulmon Dis. 2023;18:1773–1781. doi:10.2147/COPD.S419550
18. Huang X, Yu H, Huang E, et al. Feasibility and performance of the chronic obstructive pulmonary disease population screener and chronic obstructive pulmonary disease screening questionnaire in a Chinese physical examination center. J Thorac Dis. 2024;16(2):1378–1387. doi:10.21037/jtd-23-1967
19. Chen H, Hu XB, Zhou J, He CY, Wang K, Yi Q. Association of chronic obstructive pulmonary disease with risk of lung cancer in individuals aged 40 years and older: a cross-sectional study based on NHANES 2013–2018. PLoS One. 2024;19(10):e0311537. doi:10.1371/journal.pone.0311537
20. Holme JA, Vondráček J, Machala M, et al. Lung cancer associated with combustion particles and fine particulate matter (PM(2.5)) - the roles of polycyclic aromatic hydrocarbons (PAHs) and the aryl hydrocarbon receptor (AhR). Biochem Pharmacol. 2023;216:115801. doi:10.1016/j.bcp.2023.115801
21. Klebe S, Leigh J, Henderson DW, Nurminen M. Asbestos, smoking and lung cancer: an update. Int J Environ Res Public Health. 2019;17(1):258. doi:10.3390/ijerph17010258
22. Yang L, Yang Z, Zuo C, et al. Epidemiological evidence for associations between variants in CHRNA genes and risk of lung cancer and chronic obstructive pulmonary disease. Front Oncol. 2022;12:1001864. doi:10.3389/fonc.2022.1001864
23. Silverman EK. Genetics of COPD. Annu Rev Physiol. 2020;82(1):413–431. doi:10.1146/annurev-physiol-021317-121224
24. Shen J, Gao C, Lou X, et al. The association between emphysema detected on computed tomography and increased risk of lung cancer: a systematic review and meta-analysis. Quant Imaging Med Surg. 2025;15(3):2193–2208. doi:10.21037/qims-24-1879
25. Hunsaker AR. Emphysema as a predictor of lung cancer: implications for lung cancer screening. Radiology. 2022;304(2):331–332. doi:10.1148/radiol.220697
26. Kim JS, Kim EJ, Jang JG, Hong KS, Ahn JH. Low diffusion capacity predicts poor prognosis in extensive stage small cell lung cancer: a single-center analysis of 10 years. J Cancer Res Clin Oncol. 2023;149(10):7275–7283. doi:10.1007/s00432-023-04686-2
27. Shin S, Choi YS, Jung JJ, et al. Impact of diffusing lung capacity before and after neoadjuvant concurrent chemoradiation on postoperative pulmonary complications among patients with stage IIIA/N2 non-small-cell lung cancer. Respir Res. 2020;21(1):13. doi:10.1186/s12931-019-1254-0
28. Wang C, Shao J, He Y, et al. Data-driven risk stratification and precision management of pulmonary nodules detected on chest computed tomography. Nat Med. 2024;30(11):3184–3195. doi:10.1038/s41591-024-03211-3
29. Mascalchi M, Marzi C, Diciotti S. Artificial intelligence propels lung cancer screening: innovations and the challenges of explainability and reproducibility. Signal Transduct Target Ther. 2025;10(1):18. doi:10.1038/s41392-024-02111-9
30. Wohnhaas CT, Gindele JA, Kiechle T, et al. Cigarette smoke specifically affects small airway epithelial cell populations and triggers the expansion of inflammatory and squamous differentiation associated basal cells. Int J Mol Sci. 2021;22(14):7646. doi:10.3390/ijms22147646
31. Su D, Wang X, Campbell MR, et al. Distinct epigenetic effects of tobacco smoking in whole blood and among leukocyte subtypes. PLoS One. 2016;11(12):e0166486. doi:10.1371/journal.pone.0166486
32. Doyle B, Fudenberg G, Imakaev M, Mirny LA, Marti-Renom MA. Chromatin loops as allosteric modulators of enhancer-promoter interactions. PLoS Comput Biol. 2014;10(10):e1003867. doi:10.1371/journal.pcbi.1003867
33. Gavito-Covarrubias D, Ramírez-Díaz I, Guzmán-Linares J, et al. Epigenetic mechanisms of particulate matter exposure: air pollution and hazards on human health. Front Genet. 2023;14:1306600. doi:10.3389/fgene.2023.1306600
34. Sun Q, Ren X, Sun Z, Duan J. The critical role of epigenetic mechanism in PM(2.5)-induced cardiovascular diseases. Genes Environ. 2021;43(1):47. doi:10.1186/s41021-021-00219-w
35. Ji HW, Kang J, Kim HC, et al. The association between cumulative exposure to PM(2.5) and DNA methylation measured using methyl-capture sequencing among COPD patients. Respir Res. 2024;25(1):335. doi:10.1186/s12931-024-02955-3
36. Afthab M, Hambo S, Kim H, Alhamad A, Harb H. Particulate matter-induced epigenetic modifications and lung complications. Eur Respir Rev. 2024;33(174):240129. doi:10.1183/16000617.0129-2024
37. Letellier N, Wing SE, Yang JA, et al. The role of neighborhood air pollution exposure on somatic non-small cell lung cancer mutations in the Los Angeles Basin (2013–2018). Int J Environ Res Public Health. 2022;19(17):11027. doi:10.3390/ijerph191711027
38. Chen J, Wang T, Li X, et al. DNA of neutrophil extracellular traps promote NF-κB-dependent autoimmunity via cGAS/TLR9 in chronic obstructive pulmonary disease. Signal Transduct Target Ther. 2024;9(1):163. doi:10.1038/s41392-024-01881-6
39. Zhang H, Qiu SL, Tang QY, et al. Erythromycin suppresses neutrophil extracellular traps in smoking-related chronic pulmonary inflammation. Cell Death Dis. 2019;10(9):678. doi:10.1038/s41419-019-1909-2
40. Ma N, Liang XN, Chen QF, et al. Proteogenomic verifies targets underlying erythromycin alleviate neutrophil extracellular traps-induced inflammation. Respir Res. 2025;26(1):155. doi:10.1186/s12931-025-03226-5
41. Li M, Yang Y, Xiong L, Jiang P, Wang J, Li C. Metabolism, metabolites, and macrophages in cancer. J Hematol Oncol. 2023;16(1):80. doi:10.1186/s13045-023-01478-6
42. Sorin M, Rezanejad M, Karimi E, et al. Single-cell spatial landscapes of the lung tumour immune microenvironment. Nature. 2023;614(7948):548–554. doi:10.1038/s41586-022-05672-3
43. Xu L, Kong Y, Li K, et al. Neutrophil extracellular traps promote growth of lung adenocarcinoma by mediating the stability of m6A-mediated SLC2A3 mRNA-induced ferroptosis resistance and CD8(+) T cell inhibition. Clin Transl Med. 2025;15(2):e70192. doi:10.1002/ctm2.70192
44. Xiao M, Deng Y, Guo H, et al. Single-cell and spatial transcriptomics profile the interaction of SPP1(+) macrophages and FAP(+) fibroblasts in non-small cell lung cancer. Transl Lung Cancer Res. 2025;14(7):2646–2669. doi:10.21037/tlcr-2025-244
45. Ke ZH, Chen Y, Yu T, Zhang Q, Xiang Y, Lu KH. LRP1B suppresses immunotherapy efficacy in lung adenocarcinoma by preventing ferroptosis. Cancer Med. 2024;13(23):e70486. doi:10.1002/cam4.70486
46. Yao C, Joehanes R, Wilson R, et al. Epigenome-wide association study of whole blood gene expression in Framingham Heart Study participants provides molecular insight into the potential role of CHRNA5 in cigarette smoking-related lung diseases. Clin Clin Epigenet. 2021;13(1):60. doi:10.1186/s13148-021-01041-5
47. Xiao D, Li F, Pan H, Liang H, Wu K, He J. Integrative analysis of genomic sequencing data reveals higher prevalence of LRP1B mutations in lung adenocarcinoma patients with COPD. Sci Rep. 2017;7(1):2121. doi:10.1038/s41598-017-02405-9
48. He LX, Tang ZH, Huang QS, Li WH. DNA methylation: a potential biomarker of chronic obstructive pulmonary disease. Front Cell Dev Biol. 2020;8:585. doi:10.3389/fcell.2020.00585
49. Chen G, Wang Q, Wang K. MicroRNA-218-5p affects lung adenocarcinoma progression through targeting endoplasmic reticulum oxidoreductase 1 alpha. Bioengineered. 2022;13(4):10061–10070. doi:10.1080/21655979.2022.2063537
50. Zhu K, Ding H, Wang W, et al. Tumor-suppressive miR-218-5p inhibits cancer cell proliferation and migration via EGFR in non-small cell lung cancer. Oncotarget. 2016;7(19):28075–28085. doi:10.18632/oncotarget.8576
51. Song J, Wang QH, Zou SC. Role of microRNA-218-5p in the pathogenesis of chronic obstructive pulmonary disease. Eur Rev Med Pharmacol Sci. 2018;22(13):4319–4324. doi:10.26355/eurrev_201807_15428
52. Masson C, Thouvenin J, Boudier P, et al. Biological biomarkers of response and resistance to immune checkpoint inhibitors in renal cell carcinoma. Cancers. 2023;15(12):3159. doi:10.3390/cancers15123159
53. Joo YB, Lee J, Park YJ, Bang SY, Kim K, Lee HS. Associations of upper respiratory mucosa microbiota with rheumatoid arthritis, autoantibodies, and disease activity. PLoS One. 2024;19(8):e0308010. doi:10.1371/journal.pone.0308010
54. Wang Z, Kaplan RC, Burk RD, Qi Q. The oral microbiota, microbial metabolites, and immuno-inflammatory mechanisms in cardiovascular disease. Int J Mol Sci. 2024;25(22):2337.
55. O’Sullivan É, Keogh A, Henderson B, Finn SP, Gray SG, Gately K. Treatment strategies for KRAS-mutated non-small-cell lung cancer. Cancers. 2023;15(6):1635. doi:10.3390/cancers15061635
56. Pereira F, Ferreira A, Reis CA, Sousa MJ, Oliveira MJ, Preto A. KRAS as a modulator of the inflammatory tumor microenvironment: therapeutic implications. Cells. 2022;11(3):398. doi:10.3390/cells11030398
57. Li B, Gong T, Hao Y, Zhou X, Cheng L. Mining the gut microbiota for microbial-based therapeutic strategies in cancer immunotherapy. Front Oncol. 2021;11:721249. doi:10.3389/fonc.2021.721249
58. Abdelsalam NA, Hegazy SM, Aziz RK. The curious case of Prevotella copri. Gut Microbes. 2023;15(2):2249152. doi:10.1080/19490976.2023.2249152
59. Calcinotto A, Brevi A, Chesi M, et al. Microbiota-driven interleukin-17-producing cells and eosinophils synergize to accelerate multiple myeloma progression. Nat Commun. 2018;9(1):4832. doi:10.1038/s41467-018-07305-8
60. Crespin A, Le Bescop C, de Gunzburg J, et al. A systematic review and meta-analysis evaluating the impact of antibiotic use on the clinical outcomes of cancer patients treated with immune checkpoint inhibitors. Front Oncol. 2023;13:1075593. doi:10.3389/fonc.2023.1075593
61. Elkrief A, Méndez-Salazar EO, Maillou J, et al. Antibiotics are associated with worse outcomes in lung cancer patients treated with chemotherapy and immunotherapy. NPJ Precis Oncol. 2024;8(1):143. doi:10.1038/s41698-024-00630-w
62. Xu YR, Wang AL, Li YQ. Hypoxia-inducible factor 1-alpha is a driving mechanism linking chronic obstructive pulmonary disease to lung cancer. Front Oncol. 2022;12:984525. doi:10.3389/fonc.2022.984525
63. Cui Z, Ruan Z, Li M, et al. Intermittent hypoxia inhibits anti-tumor immune response via regulating PD-L1 expression in lung cancer cells and tumor-associated macrophages. Int Immunopharmacol. 2023;122:110652. doi:10.1016/j.intimp.2023.110652
64. Chen C, Guo Q, Liu Y, et al. Single-cell and spatial transcriptomics reveal POSTN(+) cancer-associated fibroblasts correlated with immune suppression and tumour progression in non-small cell lung cancer. Clin Transl Med. 2023;13(12):e1515. doi:10.1002/ctm2.1515
65. Chen C, Feng Y, FCF K, Lam SK, Yan S, JCM H. Lung cancer-associated fibroblasts-mediated collagen deposition drives mediastinal lymph node metastasis in non-small cell lung cancer. Front Oncol. 2025;15:1597585. doi:10.3389/fonc.2025.1597585
66. Rojas-Quintero J, Ochsner SA, New F, et al. Spatial transcriptomics resolve an emphysema-specific lymphoid follicle B cell signature in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2024;209(1):48–58. doi:10.1164/rccm.202303-0507LE
67. Bond DR, Burnard SM, Uddipto K, et al. Hypomethylating agents induce epigenetic and transcriptional heterogeneity with implications for acute myeloid leukemia cell self-renewal. Leukemia. 2025;39(9):2275–2280. doi:10.1038/s41375-025-02693-5
68. Ebelt ND, Loganathan S, Avsharian LC, Manuel ER. Effects of hypomethylating agents on gene modulation in the leukemic microenvironment and disease trajectory in a mouse model of AML. bioRxiv. 2024. doi:10.1101/2024.12.01.626276
69. Iida Y, Yoshikawa R, Murata A, et al. Local injection of CCL19-expressing mesenchymal stem cells augments the therapeutic efficacy of anti-PD-L1 antibody by promoting infiltration of immune cells. J Immunother Cancer. 2020;8(2):e000582. doi:10.1136/jitc-2020-000582
70. Ren S, Feng L, Liu H, Mao Y, Yu Z. Gut microbiome affects the response to immunotherapy in non-small cell lung cancer. Thorac Cancer. 2024;15(14):1149–1163. doi:10.1111/1759-7714.15303
71. Liu Y, Xu H, Lv L, et al. Risk-based lung cancer screening in heavy smokers: a benefit-harm and cost-effectiveness modeling study. BMC Med. 2024;22(1):73. doi:10.1186/s12916-024-03292-4
72. Labaki WW, Xia M, Murray S, et al. Quantitative emphysema on low-dose CT imaging of the chest and risk of lung cancer and airflow obstruction: an analysis of the National Lung Screening Trial. Chest. 2021;159(5):1812–1820. doi:10.1016/j.chest.2020.12.004
73. Carr LL, Jacobson S, Lynch DA, et al. Features of COPD as predictors of lung cancer. Chest. 2018;153(6):1326–1335. doi:10.1016/j.chest.2018.01.049
74. Butler SJ, Louie AV, Sutradhar R, Paszat L, Brooks D, Gershon AS. Impact of chronic obstructive pulmonary disease on lung cancer symptom burden: a population-based study in Ontario, Canada. Transl Lung Cancer Res. 2023;12(11):2260–2274. doi:10.21037/tlcr-23-560
75. Crapo JD, Gupta A, Lynch DA, et al. Baseline characteristics from a 3-year longitudinal study to phenotype subjects with COPD: the FOOTPRINTS study. Respir Res. 2023;24(1):290. doi:10.1186/s12931-023-02584-2
76. De Luca GR, Diciotti S, Mascalchi M. The pivotal role of baseline LDCT for lung cancer screening in the era of artificial intelligence. Arch Bronconeumol. 2025;61(6):359–367. doi:10.1016/j.arbres.2024.11.001
77. Kinoshita T, Fujii H, Hayashi Y, Kamiyama I, Ohtsuka T, Asamura H. Prognostic significance of hypoxic PET using (18)F-FAZA and (62)Cu-ATSM in non-small-cell lung cancer. Lung Cancer. 2016;91:56–66. doi:10.1016/j.lungcan.2015.11.020
78. Lugg ST, Tikka T, Agostini PJ, et al. Smoking and timing of cessation on postoperative pulmonary complications after curative-intent lung cancer surgery. J Cardiothorac Surg. 2017;12(1):52. doi:10.1186/s13019-017-0614-4
79. Lai YT, Tsai YH, Hsieh MJ, et al. Benefit of dual bronchodilator therapy on exacerbations in former and current smokers with chronic obstructive pulmonary disease in real-world clinical practice: a multicenter validation study (TOReTO). Respir Res. 2024;25(1):377. doi:10.1186/s12931-024-02971-3
80. Xu M, Yang X, Guo L. Effectiveness of preoperative and perioperative pulmonary rehabilitation nursing program for the management of patients undergoing thoracic surgery: a systematic review and meta-analysis. Pak J Med Sci. 2024;40(6):1280–1286. doi:10.12669/pjms.40.6.9259
81. Tenconi S, Mainini C, Rapicetta C, et al. Rehabilitation for lung cancer patients undergoing surgery: results of the PUREAIR randomized trial. Eur J Phys Rehabil Med. 2021;57(6):1002–1011. doi:10.23736/S1973-9087.21.06789-7
82. Liu Z, Qiu T, Pei L, et al. Two-week multimodal prehabilitation program improves perioperative functional capability in patients undergoing thoracoscopic lobectomy for lung cancer: a randomized controlled trial. Anesth Analg. 2020;131(3):840–849. doi:10.1213/ANE.0000000000004342
83. Tao W, Huang J, Jin Y, Peng K, Zhou J. Effect of pulmonary rehabilitation exercise on lung volume and respiratory muscle recovery in lung cancer patients undergoing lobectomy. Altern Ther Health Med. 2024;30(2):90–96.
84. Tahiri M, Goudie E, Jouquan A, Martin J, Ferraro P, Liberman M. Enhanced recovery after video-assisted thoracoscopic surgery lobectomy: a prospective, historically controlled, propensity-matched clinical study. Can J Surg. 2020;63(3):E233–E240. doi:10.1503/cjs.001919
85. Wang L, Cao J, Feng Y, Jia R, Ren Y. Application of uniportal video-assisted thoracoscopic surgery for segmentectomy in early-stage non-small cell lung cancer: a narrative review. Heliyon. 2024;10(9):e30735. doi:10.1016/j.heliyon.2024.e30735
86. Geng-Cahuayme AAA, Peregrín-Pastor B, Ramos-Albiac M, et al. Stereotactic ablative radiotherapy (SABR) for patients with lung tumor and severe pulmonary function impairment. Clin Transl Oncol. 2024;26(12):3246–3251. doi:10.1007/s12094-024-03557-7
87. McMillan MT, Shepherd AF, Kang M, et al. Safety and efficacy of stereotactic body proton therapy for high-risk lung tumors. J Radiosurg SBRT. 2023;9(1):63–74. doi:10.1093/jnci/djx208
88. Boudoussier A, Larrouture I, Henrot P, et al. COPD patients with non-small cell lung cancer respond better to anti-PD-(L)1 immune checkpoint inhibitors. Sci Rep. 2025;15(1):17145. doi:10.1038/s41598-025-02251-0
89. Li F, Zheng L, Xu X, Jin J, Li X, Zhou L. The impact of chronic obstructive pulmonary disease on the risk of immune-related pneumonitis in lung cancer patients undergoing immunotherapy: a systematic review and meta-analysis. BMC Pulm Med. 2024;24(1):393. doi:10.1186/s12890-024-03180-w
90. Dong W, Yin Y, Yang S, et al. Impact of chronic obstructive pulmonary disease on the efficacy and safety of neoadjuvant immune checkpoint inhibitors combined with chemotherapy for resectable non-small cell lung cancer: a retrospective cohort study. BMC Cancer. 2024;24(1):153. doi:10.1186/s12885-024-11902-w
91. Li MSC, Lee KWC, Mok KKS, et al. Brief report: risk of recurrent interstitial lung disease from osimertinib versus erlotinib rechallenge after symptomatic osimertinib-induced interstitial lung disease. JTO Clin Res Rep. 2024;5(4):100648. doi:10.1016/j.jtocrr.2024.100648
92. Peng K, Li Y, Yang Q, et al. The therapeutic promise of probiotic Bacteroides fragilis (BF839) in cancer immunotherapy. Front Microbiol. 2025;16:1523754. doi:10.3389/fmicb.2025.1523754
93. Chen H, Han KD, He ZJ, Huang YS. How to choose a survival period? The impact of antibiotic use on OS or PFS in NSCLC patients treated with immune checkpoint inhibitors: a systematic review and meta-analysis. Technol Cancer Res Treat. 2021;20:15330338211033498. doi:10.1177/15330338211033498
94. Borgers JSW, Burgers FH, Terveer EM, et al. Conversion of unresponsiveness to immune checkpoint inhibition by fecal microbiota transplantation in patients with metastatic melanoma: study protocol for a randomized phase Ib/IIa trial. BMC Cancer. 2022;22(1):1366. doi:10.1186/s12885-022-10457-y
95. Meng Y, Sun J, Zhang G. A viable remedy for overcoming resistance to anti-PD-1 immunotherapy: fecal microbiota transplantation. Crit Rev Oncol Hematol. 2024;200:104403. doi:10.1016/j.critrevonc.2024.104403
96. Eribo OA, du Plessis N, Chegou NN, Richardson AR. The intestinal commensal, Bacteroides fragilis, modulates host responses to viral infection and therapy: lessons for exploration during Mycobacterium tuberculosis infection. Infect Immun. 2022;90(1):e0032121. doi:10.1128/IAI.00321-21
97. Sharma M, Joshi S, Banjade P, Ghamande SA, Surani S. Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2023 guidelines reviewed. Open Respir Med J. 2024;18e18743064279064.
98. de-Torres JP, Alcaide AB, Campo A, et al. Lung cancer screening in people with COPD: the Pamplona-IELCAP experience. Arch Bronconeumol. 2024;60(2):95–100. doi:10.1016/j.arbres.2023.12.012
99. Shi S, Wang Y, Wu J, et al. Predictive value of PD-L1 and TMB for short-term efficacy prognosis in non-small cell lung cancer and construction of prediction models. Front Oncol. 2024;14:1342262. doi:10.3389/fonc.2024.1342262
100. Lin M, Huang Z, Chen Y, Xiao H, Wang T. Lung cancer patients with chronic obstructive pulmonary disease benefit from anti-PD-1/PD-L1 therapy. Front Immunol. 2022;13:1038715. doi:10.3389/fimmu.2022.1038715
101. Ba H, Liu L, Peng Q, Chen J, Zhu YD. The relationship between blood-based tumor mutation burden level and efficacy of PD-1/PD-L1 inhibitors in advanced non-small cell lung cancer: a systematic review and meta-analysis. BMC Cancer. 2021;21(1):1220. doi:10.1186/s12885-021-08924-z
102. Kim Y, Kim G, Kim S, et al. Fecal microbiota transplantation improves anti-PD-1 inhibitor efficacy in unresectable or metastatic solid cancers refractory to anti-PD-1 inhibitor. Cell Host Microbe. 2024;32(8):1380–1393.e9. doi:10.1016/j.chom.2024.06.010
103. Davar D, Dzutsev AK, McCulloch JA, et al. Fecal microbiota transplant overcomes resistance to anti-PD-1 therapy in melanoma patients. Science. 2021;371(6529):595–602. doi:10.1126/science.abf3363
104. Raymakers AJN, Sadatsafavi M, Sin DD, FitzGerald JM, Marra CA, Lynd LD. Inhaled corticosteroids and the risk of lung cancer in COPD: a population-based cohort study. Eur Respir J. 2019;53(6):1801257. doi:10.1183/13993003.01257-2018
105. Park JE, Lee E, Singh D, et al. The effect of inhaler prescription on the development of lung cancer in COPD: a nationwide population-based study. Respir Res. 2024;25(1):229. doi:10.1186/s12931-024-02838-7
106. Liu SF, Kuo HC, Lin MC, et al. Inhaled corticosteroids have a protective effect against lung cancer in female patients with chronic obstructive pulmonary disease: a nationwide population-based cohort study. Oncotarget. 2017;8(18):29711–29721. doi:10.18632/oncotarget.15386
107. Raymakers A, Sin DD, Sadatsafavi M, FitzGerald JM, Marra CA, Lynd LD. Statin use and lung cancer risk in chronic obstructive pulmonary disease patients: a population-based cohort study. Respir Res. 2020;21(1):118. doi:10.1186/s12931-020-01344-w
108. Niu C, Lyu Q, Carothers CD, et al. Medical multimodal multitask foundation model for lung cancer screening. Nat Commun. 2025;16(1):1523. doi:10.1038/s41467-025-56822-w
109. Shah AJ, Althobiani MA, Saigal A, Ogbonnaya CE, Hurst JR, Mandal S. Wearable technology interventions in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. NPJ Digit Med. 2023;6(1):222. doi:10.1038/s41746-023-00962-0
110. Coutu FA, Iorio OC, Ross BA. Remote patient monitoring strategies and wearable technology in chronic obstructive pulmonary disease. Front Med. 2023;10:1236598. doi:10.3389/fmed.2023.1236598
111. Eliwa EHI, Mohamed El Koshiry A, Abd El-Hafeez T, Omar A. Secure and transparent lung and colon cancer classification using blockchain and Microsoft Azure. Adv Respir Med. 2024;92(5):395–420. doi:10.3390/arm92050037
112. Zhao S, Lu Z, Zhao F, Tang S, Zhang L, Feng C. Assessing the impact of probiotics on immunotherapy effectiveness and antibiotic-mediated resistance in cancer: a systematic review and meta-analysis. Front Immunol. 2025;16:1538969. doi:10.3389/fimmu.2025.1538969
113. Xia L, Zhu X, Wang Y, Lu S. The gut microbiota improves the efficacy of immune-checkpoint inhibitor immunotherapy against tumors: from association to cause and effect. Cancer Lett. 2024;598:217123. doi:10.1016/j.canlet.2024.217123
114. Lin A, Huang L, Jiang A, et al. Microbiota boost immunotherapy? A meta-analysis dives into fecal microbiota transplantation and immune checkpoint inhibitors. BMC Med. 2025;23(1):341. doi:10.1186/s12916-025-04183-y
115. Deng F, Du X, Zhang P, Xu J, Li Y, Yang Z. Impact of antibiotic on efficacy and adverse reactions of chemoimmunotherapy in non-small cell lung cancer patients: a retrospective cohort study. Thorac Cancer. 2024;15(36):2560–2569. doi:10.1111/1759-7714.15490
116. Petrelli F, Ghidini A, Dottorini L, Ghidini M, Zaniboni A, Tomasello G. Clinical evidence for microbiome-based strategies in cancer immunotherapy: a state-of-the-art review. Medicina. 2025;61(9):1595. doi:10.3390/medicina61091595
117. Yousefi Y, Baines KJ, Maleki Vareki S. Microbiome bacterial influencers of host immunity and response to immunotherapy. Cell Rep Med. 2024;5(4):101487. doi:10.1016/j.xcrm.2024.101487
118. Eklund EA, Svensson J, Näslund LS, et al. Comprehensive genetic variant analysis reveals combination of KRAS and LRP1B as a predictive biomarker of response to immunotherapy in patients with non-small cell lung cancer. J Exp Clin Cancer Res. 2025;44(1):75. doi:10.1186/s13046-025-03342-6
119. Du Y, Ding X, Ye Y. The spatial multi-omics revolution in cancer therapy: precision redefined. Cell Rep Med. 2024;5(9):101740. doi:10.1016/j.xcrm.2024.101740
120. Liu X, Peng T, Xu M, et al. Spatial multi-omics: deciphering technological landscape of integration of multi-omics and its applications. J Hematol Oncol. 2024;17(1):72. doi:10.1186/s13045-024-01596-9
121. Zuo C, Xia J, Xu Y, et al. stClinic dissects clinically relevant niches by integrating spatial multi-slice multi-omics data in dynamic graphs. Nat Commun. 2025;16(1):5317. doi:10.1038/s41467-025-60575-x
122. Filho MM, Aguiar PN Jr, de Mello RA. Chronic obstructive pulmonary disease alters immune cell composition and immune checkpoint inhibitor efficacy in non-small cell lung cancer. Ann Transl Med. 2019;7(Suppl 1):S42. doi:10.21037/atm.2019.02.27
123. Lahousse L. Personalizing oral corticosteroid dose in severe COPD exacerbations. Chest. 2021;160(5):1581–1582. doi:10.1016/j.chest.2021.06.042
124. Blutt SE, Coarfa C, Neu J, Pammi M. Multiomic investigations into lung health and disease. Microorganisms. 2023;11(8):2116. doi:10.3390/microorganisms11082116
125. Gao J, Yi X, Wang Z. The application of multi-omics in the respiratory microbiome: progresses, challenges and promises. Comput Struct Biotechnol J. 2023;21:4933–4943. doi:10.1016/j.csbj.2023.10.016
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Targeted Treatment of Advanced Endometrial Cancer: Focus on Pembrolizumab
El-ghazzi N, Durando X, Giro A, Herrmann T
OncoTargets and Therapy 2023, 16:359-369
Published Date: 2 June 2023
Awareness and Predictors of the Use of Bioinformatics in Genome Research in Saudi Arabia
Alomair L, Abolfotouh MA
International Journal of General Medicine 2023, 16:3413-3425
Published Date: 11 August 2023
Lung Cancer Diagnosis and Prognostic Monitoring Through Cell-Free RNA via Liquid Biopsy
Pan Y, Jiang C, Ye M, Li D, Wang J
Therapeutics and Clinical Risk Management 2025, 21:1615-1636
Published Date: 2 December 2025
Nanomaterial-Enhanced Immunotherapy: Advancing T-Cell-Based Treatments for Bladder Cancer
Chen J, Fu Y, Zhang Z, Zhao J, Zuo J, Ye X, Xiong Q, Nie Z, Dong H, Shi H, Tan Z, Wang C, Chen B, Wang Z, Li X, Chen P, Wang H, Fu S
International Journal of Nanomedicine 2025, 20:15235-15275
Published Date: 18 December 2025
Hydrogel-Based Immunomodulation of Tumor Immune Microenvironment in Hepatocellular Carcinoma: Current Strategies and Future Directions
Zhang S, Ding L, Hou T, Lin D, Qu Y
International Journal of Nanomedicine 2026, 21:576091
Published Date: 4 March 2026