Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
COPD Patients with a High Exacerbation Risk: Baseline Data Analysis of a National Chinese Prospective Multi-Center Study of Quality Improvement Project
Authors Yang K ![]() , Chen D, Wang Y, Wang F, Wang L, Wang J, Yu T, Hou H, Liu W, Huang P, Yang H, Chen R
, Chen D, Wang Y, Wang F, Wang L, Wang J, Yu T, Hou H, Liu W, Huang P, Yang H, Chen R ![]()
Received 19 January 2026
Accepted for publication 28 May 2026
Published 3 June 2026 Volume 2026:21 597295
DOI https://doi.org/10.2147/COPD.S597295
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Zijing Zhou
Kai Yang,1,* Dandan Chen,1,* Yan Wang,1,* Fengyan Wang,2 Lingwei Wang,1 Jing Wang,3 Tingfeng Yu,4 Huina Hou,5 Wei Liu,6 Peirong Huang,7 Hongying Yang,8 Rongchang Chen1,2
1Department of Pulmonary and Critical Care Medicine, Shenzhen Key Laboratory of Respiratory Diseases, Shenzhen Institute of Respiratory Diseases, Shenzhen People’s Hospital (The First Affiliated Hospital, Southern University of Science and Technology, The Second Clinical Medical College, Jinan University), Shenzhen, People’s Republic of China; 2Guangzhou Institute of Respiratory Health, State Key Laboratory of Respiratory Disease, National Clinical Research Center for Respiratory Disease, National Center for Respiratory Medicine, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou, People’s Republic of China; 3Department of Respiratory Medicine, People’s Hospital of Luxi Yunnan Province, Honghe, People’s Republic of China; 4Department of Respiratory and Critical Care Medicine, Yiyang Central Hospital, Yiyang, People’s Republic of China; 5Department of Respiratory and Critical Care Medicine, Shangqiu Third People’s Hospital, Shangqiu, People’s Republic of China; 6Department of Respiratory and Critical Care Medicine, Luoyang Sixth People’s Hospital, Luoyang, People’s Republic of China; 7Department of Respiratory and Critical Care Medicine, Yuci District People’s Hospital, Jinzhong, People’s Republic of China; 8National Drug Clinical Trial Institution, Shenzhen People’s Hospital (the First Affiliated Hospital, Southern University of Science and Technology, The Second Clinical Medical College, Jinan University), Shenzhen, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Rongchang Chen, Department of Pulmonary and Critical Care Medicine, Shenzhen Key Laboratory of Respiratory Diseases, Shenzhen Institute of Respiratory Diseases, Shenzhen People’s Hospital (The First Affiliated Hospital, Southern University of Science and Technology, The Second Clinical Medical College, Jinan University), Shenzhen, People’s Republic of China, Email [email protected] Hongying Yang, National Drug Clinical Trial Institution, Shenzhen People’s Hospital (the First Affiliated Hospital, Southern University of Science and Technology, The Second Clinical Medical College, Jinan University), Shenzhen, People’s Republic of China, Email [email protected]
Purpose: Patients with chronic obstructive pulmonary disease (COPD) with a history of frequent exacerbations have a high disease burden and poor progression, demanding optimized management. This study aimed to evaluate the real-world clinical situation, adherence to Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommendations, and the associated factors.
Patients and Methods: We conducted a cross-sectional analysis of baseline data from the national multi-center Quality Improvement Program, which enrolled 1055 COPD patients with a high exacerbation risk from 40 hospitals across five geographic regions in China (NCT05638646). Patient characteristics, disease burden, management patterns and the associated factors were analyzed.
Results: The study population had a mean age of 66.2 years, and 85.6% were male. Most patients had substantial disease burden, with 43.3% classified as GOLD stages 3– 4 and 93.6% categorized into GOLD group E. In previous 12 months, 39.0% and 67.2% of these patients experienced at least one moderate or severe exacerbation, respectively. Overall, 75.1% received maintenance therapy using long-acting bronchodilators, but only 17.7% were receiving maintenance therapy consistent with the GOLD recommendations for initial treatment. Among patients receiving inhaled therapy, 70.9% initiated maintenance therapy within one month after diagnosis, whereas the self-reported good compliance was only 47.3%. Despite most patients received inhalation technique checks and education, only 61.9% can use the inhalation device appropriately, as evaluated by research team. Hospital level, hospital region, availability of blood eosinophil counts, and disease severity were significantly associated with the management patterns.
Conclusion: COPD patients with a high exacerbation risk in China had a substantial disease burden and important gaps between real-world management patterns and GOLD recommendations. These findings suggest opportunities to improve guideline implementation, particularly in secondary and county-based hospitals. Future studies should evaluate whether targeted quality improvement interventions can improve patient outcomes.
Trial Registration Number: NCT05638646.
Keywords: chronic obstructive pulmonary disease, disease burden, pharmacological treatment, non-pharmacological treatment, inhaled therapy management
Introduction
Chronic obstructive pulmonary disease (COPD) has become the most common chronic respiratory disease in China, affecting 13.7% of adults aged 40 years or older.1 Patients with a history of acute exacerbations (AECOPD) have poorer clinical outcomes, including a higher risk of future exacerbations, accelerated lung function decline, a higher incidence of cardiovascular events, and elevated mortality.2–5 Previous studies indicated that up to 50% of COPD patients had a characteristic of frequent AECOPD.6–9 Since the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2023 report, these patients are classified as group E, and the recommended initial inhaled therapy is either dual long-acting bronchodilators [long-acting β2-agonist (LABA) plus long-acting muscarinic antagonist (LAMA), LABA+LAMA] or triple therapy [LABA + LAMA combined with inhaled corticosteroid (ICS)], with a de-emphasis on the use of LABA+ICS as initial treatment option.10
In China’s tiered healthcare system, specialized clinical expertise and advanced facilities are disproportionately concentrated in the tertiary hospitals.11 Consequently, patients managed at secondary hospitals differ from those at tertiary centers in resource availability, healthcare access, and disease awareness. These disparities may contribute to the poor guideline adherence that hinders effective COPD management in China.12 A nationwide community-based survey in China indicated that less than 10% of COPD patients received any maintenance pharmacological treatment at stable stage.13 Inadequate medication treatments were also observed among COPD patients in outpatient clinics compared with GOLD recommendation.14–17 Beyond pharmacological gaps, the implementation of non-pharmaceutical treatment is an essential yet frequently overlooked component of COPD care.18 A recent study showed that comprehensive self-management interventions, such as patient education and pulmonary rehab, can improve quality of life and reduce exacerbations.19
However, previous COPD studies in China (eg., the REAL study) were derived from the stable COPD population, and studies specifically focusing on patients with high AECOPD are scarce.9 There remains a significant research gap in establishing how current clinical practice aligns with GOLD recommendations for high-risk patients across China’s healthcare system. Filling this gap is essential to characterize real-world management and to inform targeted quality improvement strategies aimed at improving patient outcomes.
In this study, we aimed to characterize the real-world management of patients at high risk of AECOPD and to identify specific deficiencies in care using baseline data from a national multi-center Quality Improvement Program (QIP).
Material and Methods
Study Design
The QIP study is a multi-center, prospective, cluster-randomized controlled study aimed at evaluating the effectiveness of implementing GOLD recommendations in the management of patients with COPD and AECOPD (Supplementary Figure 1).20 The present analysis is a cross-sectional study utilizing the baseline data of this ongoing longitudinal cohort to characterize current management patterns before intervention.
The study protocol was registered on the Clinical Trial website (NCT05638646). This study was conducted in compliance with the International Conference on Harmonization Good Clinical Practice guidelines, Declaration of Helsinki, and all relevant local regulations. Ethical approval was obtained from the Ethics Committee of Shenzhen People’s Hospital (SYL-202165-02) and all participating centers. Written informed consent was obtained from all participants prior to screening.
Study Participants
The patients in this study were recruited from 40 hospitals (20 secondary and 20 tertiary) across five geographic regions in China (Supplementary Figure 2 and Supplementary Table 1). The cases were selected in a time order of up to 27 at each site based on the sample size estimation for the interventional phase of this study. Therefore, the baseline data of the patients in this study might represent the current status of the management of COPD patients with a high AECOPD risk in China. Key inclusion criteria were: (1) 40–80 years old; (2) diagnosis of COPD (post-bronchodilator FEV1/FVC < 0.7); (3) FEV1% predicted ≥ 25%; (4) CAT ≥ 10; (5) with exacerbation history: at least two moderate or 1 severe exacerbation in the previous year, or one moderate exacerbation in the previous year with FEV1 < 50% predicted value at baseline; (6) ability to sign the informed consent form. Key exclusion criteria during the screening period/enrollment were as follows: (1) the main diagnosis of asthma, lung cancer, or other major respiratory diseases; (2) a history of lung surgery; (3) serious and uncontrollable diseases that may interfere with the study or affect the safety of the subjects; (4) any cancer diagnosis within the past 5 years; (5) requiring long-term home oxygen therapy or ventilatory support; (6) already receiving inhaled triple therapy regularly for more than half of the time in the last 3 months; (7) AECOPD requiring hospitalization and/or antibiotic administration and glucocorticoid administration within 4 weeks; and (8) currently involved in any other interventional studies or clinical trials.
Data Collection and Indicator Definition
All baseline data were prospectively recorded in a case report form according to the protocol. A history of AECOPD over the past 12 months was recorded. Moderate exacerbation was defined as the use of systemic corticosteroids and/or antibiotics for at least three days, and severe exacerbation was defined as COPD-related hospitalization or emergency treatment. Patient’s severity of flow limitation was classified into grade 1–4 by post-bronchodilator FEV1% predicted, consistent with GOLD guidelines. Classification into groups B and E was based on exacerbation history.21
Taking the GOLD report recommendation as the reference standard, the initial maintenance medication therapy with LABA + LAMA was considered appropriate for patients in groups B and E with eosinophil counts <300 cells/μL, and triple therapy for patients in group E with eosinophil counts ≥300 cells/μL. The consistency between the prescribed inhaled and guideline-recommended regimens was also calculated. The term “initial maintenance therapy within one month after diagnosis” was defined as the interval between the date of first inhaled maintenance therapy and the date of first spirometry-defined COPD diagnosis being less than one month. Self-reported good compliance was defined as ≥70% of treatment dosage used in patients receiving maintenance therapy containing long-acting bronchodilators. Appropriate use of inhalation device was assessed by trained research staff using a standardized 7-step checklist based on guideline-recommended steps (Supplementary Table 2).
Statistical Analysis
Descriptive statistics were used to summarize the study data, including the mean ± standard deviation (SD) for continuous variables with normality, median (interquartile range) for continuous variables without normality, and frequency (percentage) for categorical variables. Between-group comparisons were conducted using t-tests, chi-square tests, or Fisher’s exact tests as appropriate. Multivariable logistic regression model was performed to assess the associations of hospital level, hospital region, education level, occurrence of exacerbation, GOLD grade, CAT score, and availability of blood eosinophil counts with management patterns. Models were adjusted for age, sex, BMI, smoking status, occupation, time since spirometry-confirmed COPD diagnosis, and comorbidities, with all main variables mutually adjusted. In the multivariable analyses, missing data were imputed using multiple imputation by chained equations with 5 imputed datasets. Since multivariable logistic regression models were conducted for nine indicators of management patterns, a Bonferroni-corrected significance threshold of P<0.0056 (0.05/9) was used to control for Type I error. Statistical analysis was performed using SAS 9.4 (SAS Institute Inc., Cary, USA), and other statistical significance was defined as a two-sided P<0.05.
Results
Patient Characteristics
Between April 2023 and June 2024, 1055 COPD patients with COPD with a history of frequent exacerbations were included (Figure 1). The mean age was 66.2 (SD: 7.5) years, 903 (85.6%) were male, and the mean BMI was 23.0 (SD: 3.6) kg/m2 (Table 1). A history of smoking was reported in 847 (80.3%) patients, with a median exposure of 44.0 (IQR: 30.0, 54.0) pack-years. Exposure to solid fuel was reported by 9.3% for cooking and 13.7% for heating, while 24.6% had occupational exposures.
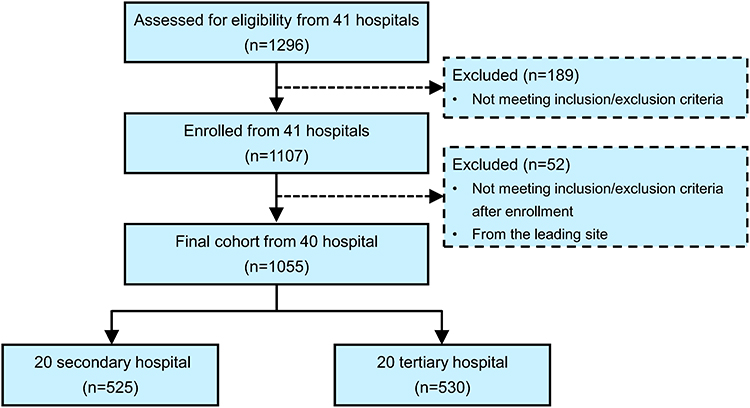 |
Figure 1 Flowchart of patient selection in this study. |
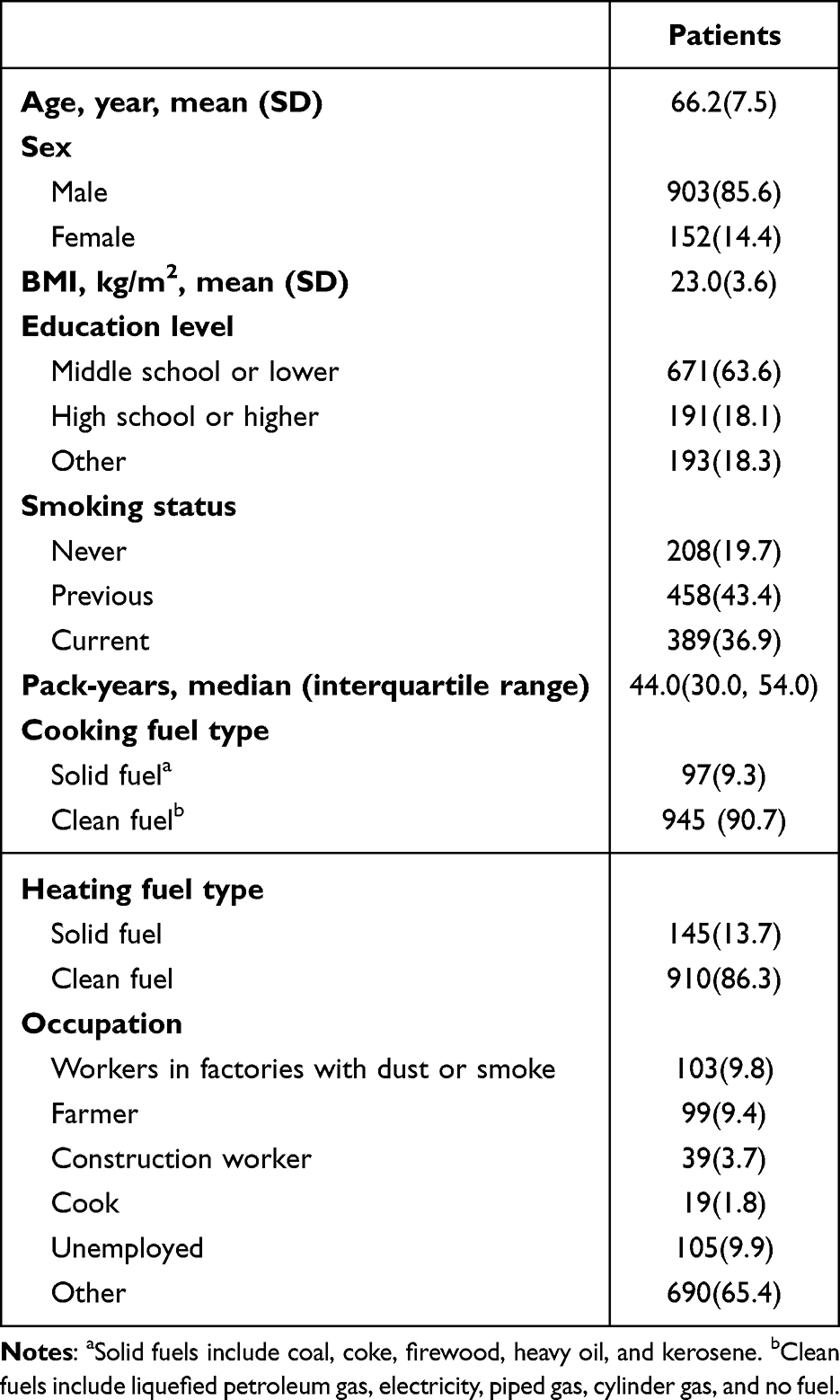 |
Table 1 Patient Characteristics in This Study |
Disease Burden
The median time since the first diagnosis of spirometry-defined COPD was 10.6 (IQR: 1.5, 48.3) months (Table 2). 446 (43.3%) patients were categorized into GOLD stages 3–4, 988 (93.6%) were categorized into GOLD group E, and the mean CAT score was 18.0 (SD: 5.7). In the past year, 411 (39.0%) and 709 (67.2%) reported at least one moderate and severe exacerbation, with an average of 1.5 (SD: 0.8) times per patient per year. Blood eosinophil counts were available for 694 patients, among whom 21.9% had ≥300 cells/μL. Lung function measurements showed that the mean post-bronchodilator FEV1% predicted was 54.8% (SD: 18.6%) and the mean post-bronchodilator FEV1/FVC was 53.1% (SD: 10.5%). The most prevalent comorbidities included hypertension, metabolic syndrome, history of respiratory infection, and other cardiovascular diseases, while other comorbidities were relatively infrequent (<6%).
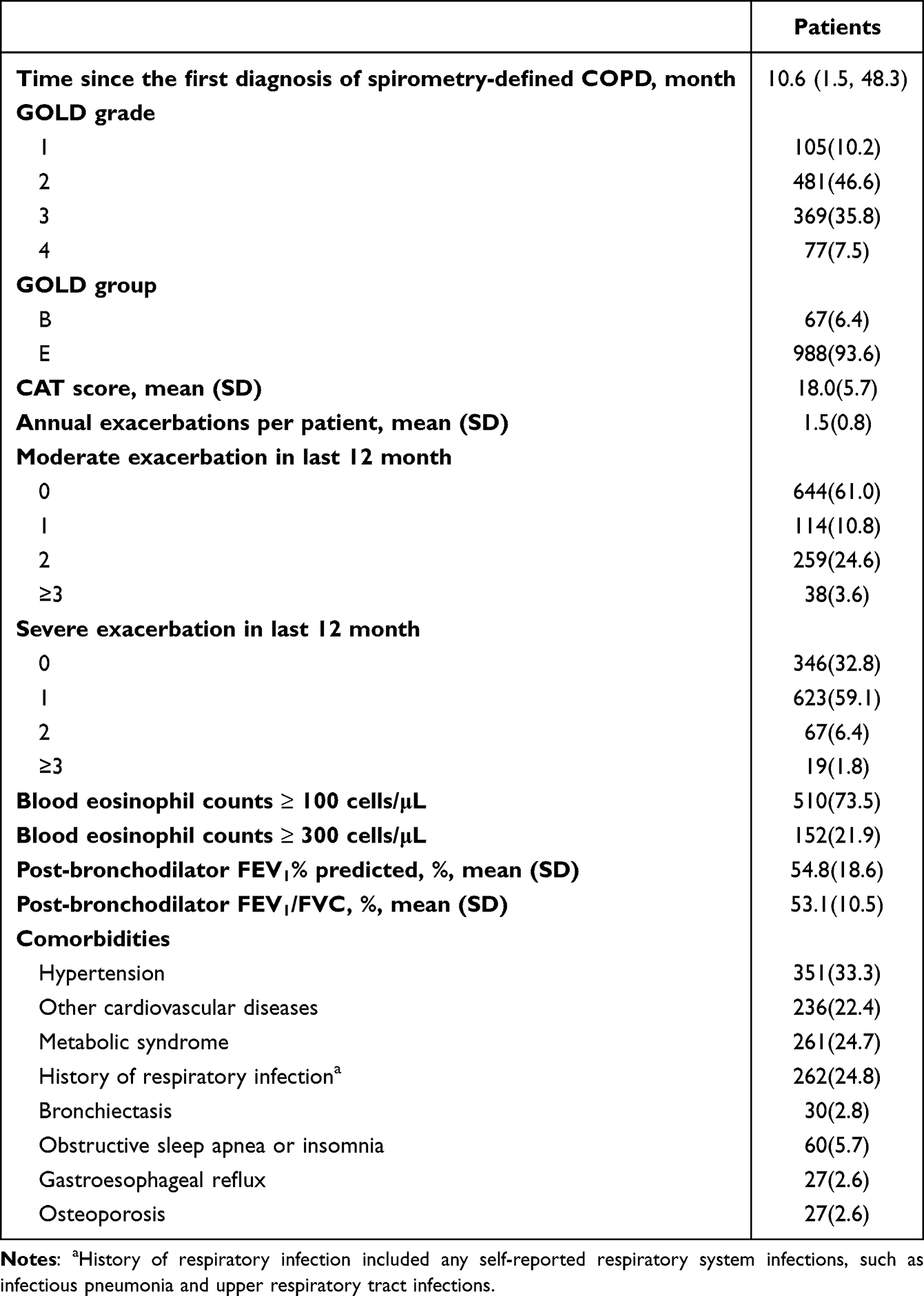 |
Table 2 Key Indicators Characterizing the Burden of COPD at High Exacerbation Risk |
Treatment and Inhaled Therapy Management
As shown in Table 3, the most common inhalation maintenance regimen was LABA + ICS (30.5%), followed by triple therapy (19.7%), LABA + LAMA (17.0%), and LAMA (10.4%). Overall, 792 (75.1%) patients received long-acting bronchodilators and 514 (48.7%) received ICS-containing regimens. However, only 126 (17.7%) patients were receiving maintenance therapy consistent with the GOLD recommendations for initial treatment.
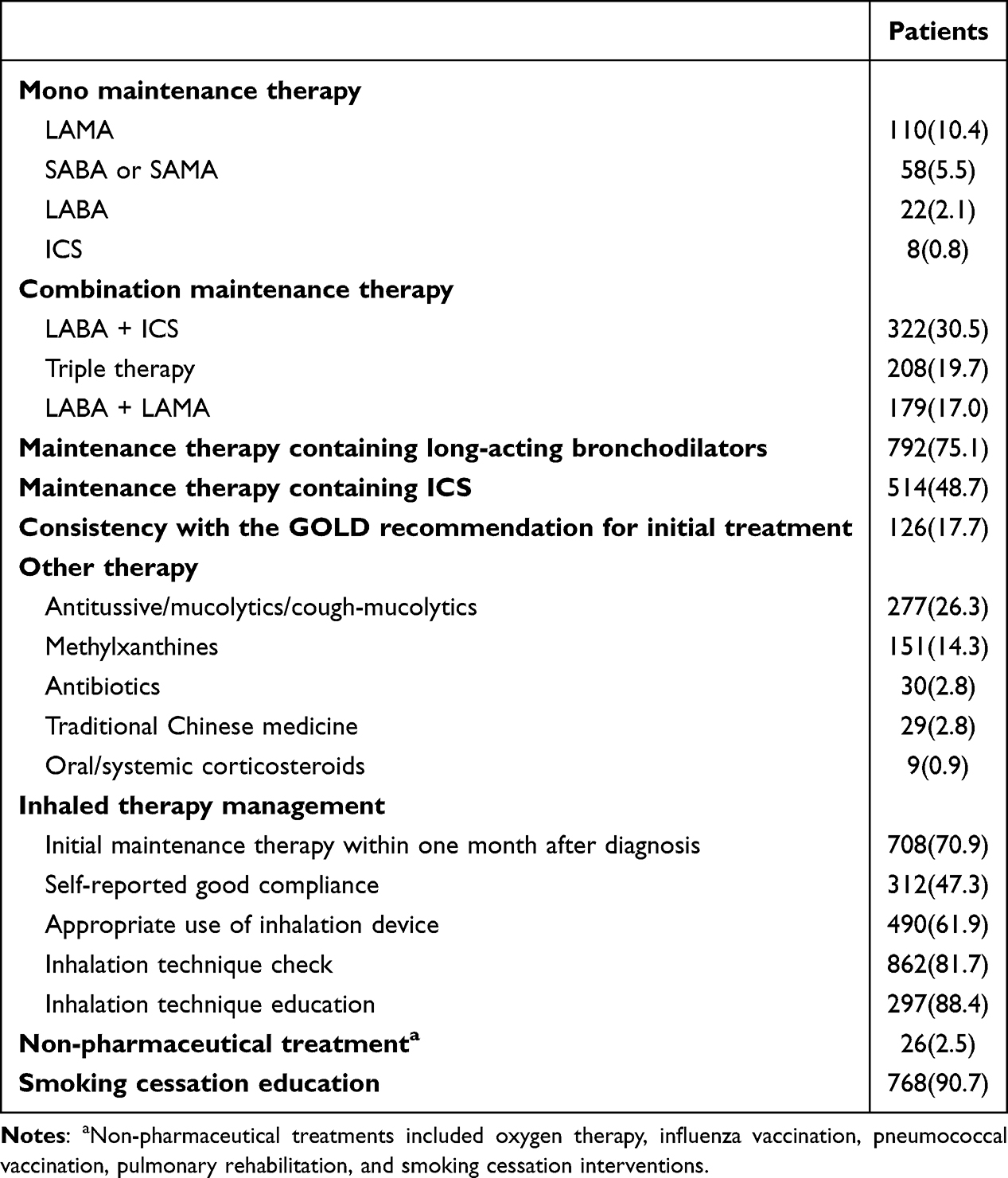 |
Table 3 The Treatment for Patients with COPD in This Study |
Among patients receiving inhaled therapy, 708 (70.9%) started the maintenance therapy within one month of diagnosis. However, only 47.3% reported good compliance. Although inhalation technique education and check were widely implemented, only 61.9% of patients appropriately used the inhalation device. Smoking cessation education was provided to 768 (90.7%) ever-smokers, whereas non-pharmaceutical treatment was rare (2.5%).
Treatment patterns for patients in GOLD group E were similar to the overall population (Supplementary Table 3). Notably, triple therapy was more frequently prescribed in patients with available blood eosinophil counts. However, no differences in the treatment patterns were observed across eosinophil levels.
Distribution of Disease Burden and Management Patterns Across Different Patient Groups
As shown in Supplementary Figure 3A and Supplementary Table 4, patients in tertiary hospitals had lower CAT scores, more moderate exacerbations, and fewer severe exacerbations than those in secondary hospitals. In terms of pharmacological treatment, patients in tertiary hospitals were more likely to receive LABA + LAMA and methylxanthines, but less likely to receive LABA + ICS and antibiotics (Figure 2A and Supplementary Table 5). However, smoking cessation education was more frequently provided in secondary hospitals.
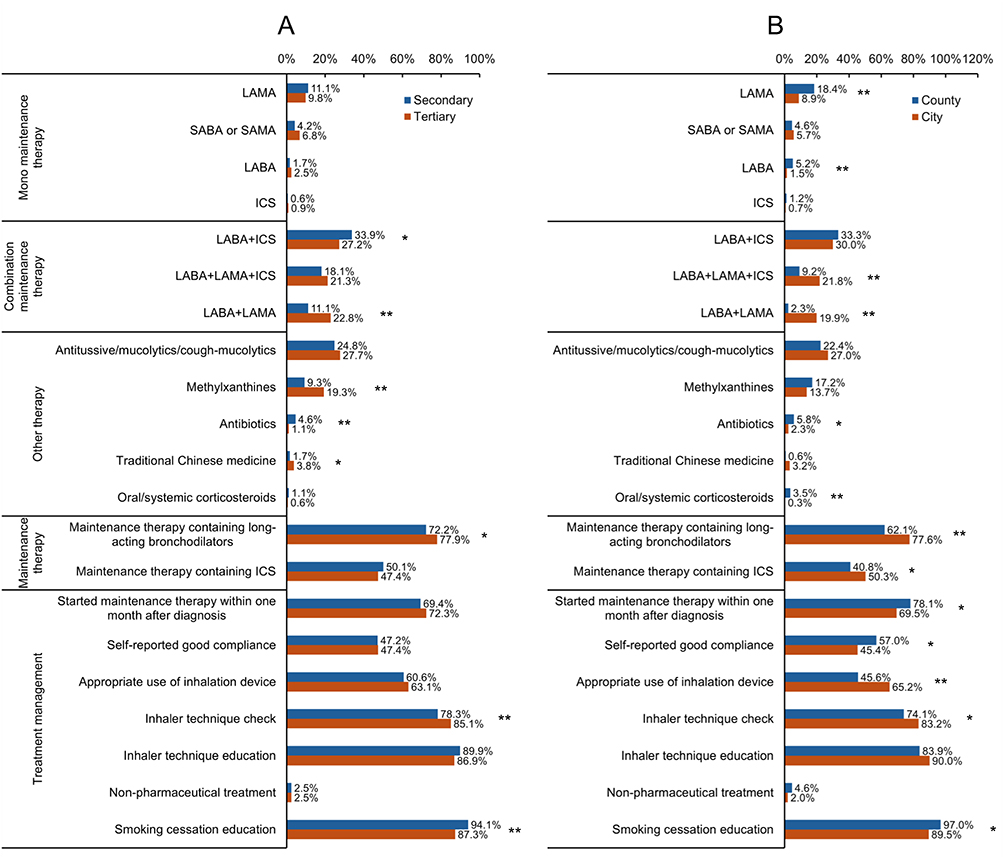 |
Figure 2 Management patterns of COPD patients at high exacerbation risk, stratified by hospital level (A) and hospital region (B). *P<0.05. **P<0.005. Abbreviations: LAMA, long-acting muscarinic antagonist; LABA, long-acting β2-agonist; ICS, inhaled corticosteroid; SABA, short-acting β2-agonist; SAMA, short-acting muscarinic antagonist. |
Compared with county-based hospitals, patients in city-based hospitals had higher BMI and education levels (Supplementary Figure 3B). They also showed lower symptom burden, more moderate exacerbations, fewer severe exacerbations, and greater comorbidity burden. Patients in city-based hospitals were more likely to receive combination maintenance therapy and demonstrated better inhalation technique (Figure 2B). Differences in clinical characteristics, disease burden, and treatment were also observed between city- and county-based hospitals within the same hospital level (Supplementary Tables 4 and 5).
Among other factors, higher education level was associated with better compliance (Supplementary Table 6); patients with more frequent exacerbations received more antitussive/mucolytics/cough-mucolytics (Supplementary Table 7); increased disease severity was associated with more triple therapy (Supplementary Table 8); and patients with lower symptom burden started maintenance therapy within one month after diagnosis (Supplementary Table 9).
Factors Associated with Management Patterns
Hospital region and the availability of blood eosinophil counts were dominant factors associated with management patterns (Table 4). Compared with county-based hospitals, city-based hospitals were significantly more likely to prescribe LABA + LAMA and maintenance therapies containing long-acting bronchodilators. In contrast, these patients were less likely to receive methylxanthines. Furthermore, city-based hospitals were independently associated with a lower likelihood of initial maintenance therapy within one month, while showing a higher likelihood of appropriate inhalation device use. The availability of blood eosinophil counts was strongly associated with pharmacological choices. Specifically, it was associated with a higher likelihood of prescribing triple therapy and maintenance therapy containing ICS, while showing an inverse association with LABA + LAMA, antitussive/mucolytics/cough-mucolytics, and methylxanthines.
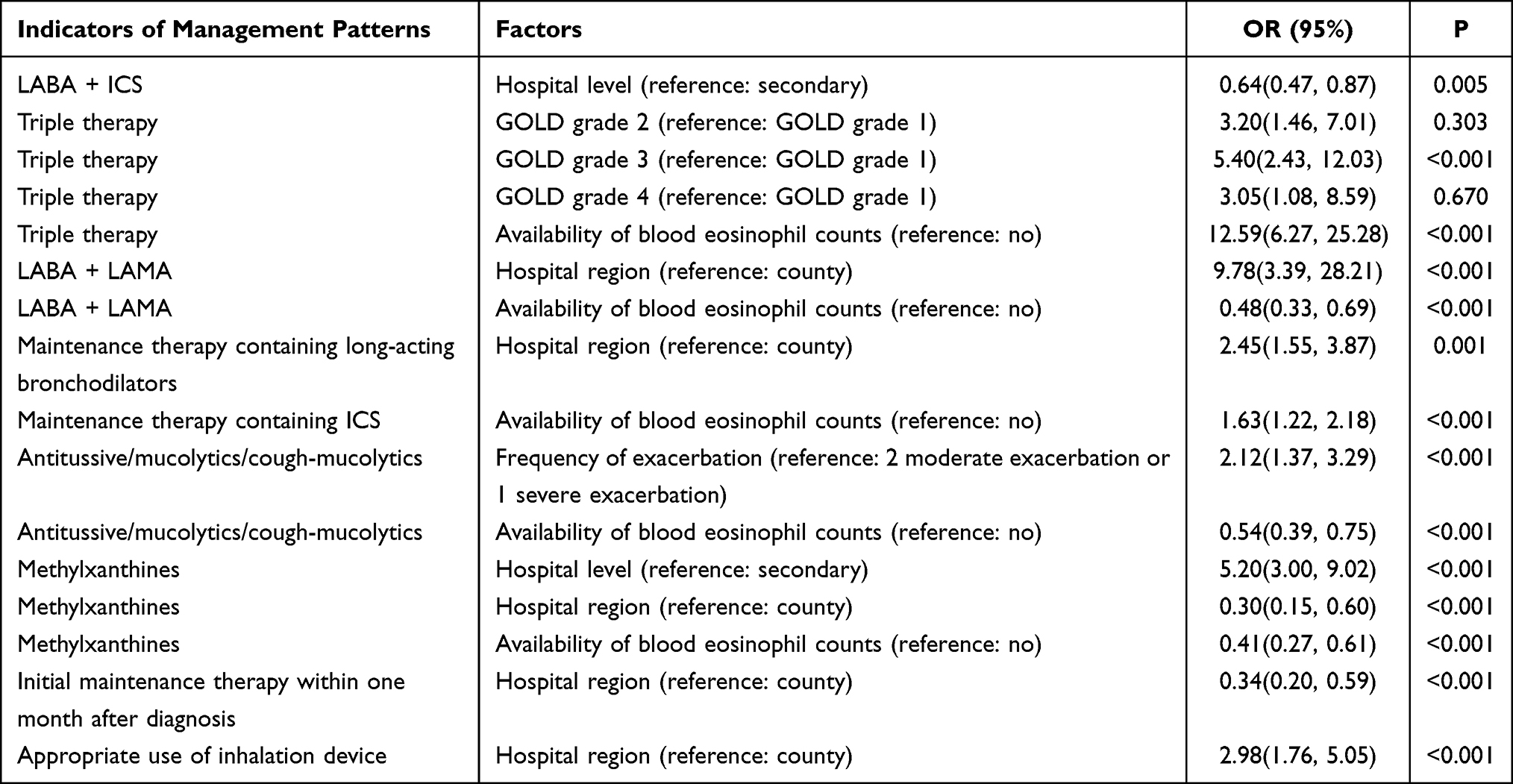 |
Table 4 Factors Significantly Associated with Management Patterns in Patients with COPD |
Regarding hospital levels, tertiary hospitals showed a strong positive association with methylxanthine use, but a lower likelihood of prescribing LABA + ICS compared to secondary hospitals. Patients with higher GOLD grade were significantly more likely to receive triple therapy, and a history of frequent exacerbations was independently associated with the use of antitussive/mucolytics/cough-mucolytics.
Discussion
This multicenter study provided a cross-sectional overview of real-world COPD management across diverse geographic regions and hospital levels in China. Focusing on patients with a high risk of exacerbation, our analysis revealed that nearly 30% of patients experienced delayed treatment initiation after diagnosis. Although three-quarters of patients received inhalation maintenance therapy, adherence to GOLD recommendations and guidelines in China remained limited, even among those in GOLD group E. In addition, hospital level, hospital region, availability of blood eosinophil counts, and disease severity were associated with management patterns.
The study population was characterized by a history of AECOPD and high CAT scores.14,22 Other demographic and clinical characteristics were similar to those reported in other outpatient-based studies, including age, BMI, education level, smoking history, blood eosinophil count, GOLD grade, and comorbidities, which epitomized the real-world situation of COPD patients in outpatient clinics in China.14,22,23 Consistent with expectations, these outpatients exhibited more severe disease profiles than those in the community-based cohorts, including older age, lower BMI, higher CAT scores, and more advanced GOLD grades.13,24 These findings highlight the substantial disease burden among COPD patients at high exacerbation risk and suggest important opportunities for improving disease management in routine practice.
In the GOLD 2023 report, dual bronchodilator was recommended as the initial maintenance therapy for patients in groups B and E with blood eosinophil counts <300 cells/μL. Triple therapy for patients in group E and blood eosinophile >300 cells/μL or step-up choice for patients with AECOPD even after dual bronchodilator treatment and blood eosinophile >100 cells/μL.10 However, LABA + ICS is still a frequently prescribed maintenance regimen, as in previous studies, although it is no longer recommended since the GOLD 2023 report.10,15 The frequent use of LABA+ICS may be partly explained by its inclusion in China’s medical insurance system nearly a decade earlier than dual bronchodilator and triple therapy, as well as its greater accessibility in primary and secondary healthcare settings, which may have contributed to deeply established prescribing habits among physicians.
The increasing use of dual bronchodilator compared to earlier real-world data is likely attributable to the improving drug availability and its coverage by China’s medical insurance in recent years.15,22 However, the prescription rate for triple therapy remained consistently low, which is similar to that reported in previous studies.15,23 Although triple therapy was prescribed more frequently in patients with available eosinophil measurements, treatment patterns did not substantially differ across eosinophil level, suggesting that blood eosinophil counts may still be underutilized in treatment decision-making in real-world practice. These data underscore the urgent need for guideline-based therapy in COPD patients with a high exacerbation risk to improve clinical outcomes.
Methylxanthines are commonly used in patients with COPD in China; however, their efficacy remains controversial.25–27 In contrast to previous reports, our study found that methylxanthines were used more frequently in tertiary hospitals.22 One possible explanation is that physicians in tertiary hospitals may prescribe methylxanthines as an adjunctive add-on therapy for symptom control in this high-risk population. Antitussive/mucolytics/cough-mucolytics are also frequently prescribed, which is recommended in patients with high airway mucus hypersecretion.28,29 More high-quality evidence is needed to evaluate the effects of these drugs in COPD patients with a high risk of exacerbation.
Non-pharmacological treatment is an important component of the comprehensive management of COPD.21 Recent systematic reviews in Asian low- and middle-income countries have shown that structured self-management interventions can reduce exacerbation rates and improve health-related quality of life.19 However, despite extensive smoking cessation education, other non-pharmacological treatments are severely underutilized. The low implementation rate suggests an important gap in current COPD management and highlights the need for greater integration of non-pharmacological support into quality improvement strategies.
Another novelty of our study was the real-world data on inhaled therapy management, as correct inhalation technique was associated with patient’s outcomes.30 However, inappropriate use of inhalation devices has been a problem for decades.31,32 Although the proportion of patients appropriately using inhalation devices in this study was relatively higher than that reported in some international studies, a substantial number of patients still failed to use the devices correctly despite widespread inhalation education and technique checks.31,33 These findings suggest that conventional educational approaches alone may be insufficient. New and better approaches, such as teach-back methods, repeated video instructions, and digital monitoring, may help improve inhaler technique and long-term treatment effectiveness.34–36 An interesting finding of this study was that patients in county-based hospitals were more likely to initiate maintenance therapy within one month, potentially reflecting closer follow-up and more streamlined physician-patient interactions. These findings suggest that quality improvement strategies may need to be tailored according to hospital level and regional resource availability.
Several limitations should be considered when interpreting these findings. First, several exclusion criteria may have introduced selection bias. In particular, patients already receiving regular triple therapy and those with particularly severe disease were excluded to facilitate evaluation of the subsequent intervention phase, which may have resulted in underrepresentation of a broader COPD population. Of note, the proportion of these excluded patients was relatively low. Second, since the recommendation of the treatment pattern in the GOLD report is used to guide the initial pharmacological treatment, the adherence rate in this study should be interpreted with caution in patients with prior treatment histories. Third, the COPD diagnosis date was defined as the date of the first spirometry-confirmed diagnosis, which may have led to an underestimation of treatment delays, as a clinical diagnosis might have been established earlier. Fourth, blood eosinophil data were unavailable for approximately one-third of patients, which may have influenced the assessment of guideline-concordant therapy. However, this missingness is inherently reflective of real-world clinical practice, where the integration of biomarker testing into routine COPD management remains suboptimal. Fifth, some subgroup analyses with relatively small sample sizes may lack sufficient statistical power to detect clinically meaningful differences and should be interpreted as exploratory. Sixth, data on disease burden and treatment were collected retrospectively, which may have been subject to recall bias. Finally, the cross-sectional design of this study precludes the establishment of causal relationships between the identified factors and management patterns, and limits a comprehensive assessment of treatment appropriateness.
Conclusion
In conclusion, this study highlights a substantial disease burden of COPD patients with a high exacerbation risk in China and reveals important gaps between real-world management patterns and GOLD recommendations. These findings suggest opportunities for improved guideline implementation, particularly in secondary and county-based hospitals. Beyond pharmacological optimization, greater emphasis should be placed on structured self-management and non-pharmacological support. Future research should evaluate whether targeted quality improvement initiatives can close this gap and improve patient outcomes.
Abbreviations
AECOPD, acute exacerbation of COPD; BMI, body mass index; CAT, COPD assessment test; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in the 1 second; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroid; IQR, interquartile range; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; QIP, Quality Improvement Program; SD, standard deviation.
Data Sharing Statement
The data supporting the findings of this study are available upon request from Rongchang Chen (e-mail: [email protected]).
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Shenzhen People’s Hospital (SYL-202165-02) and the independent ethics committees of all the study sites. Written informed consent was obtained from all participants prior to screening.
Acknowledgments
We would like to thank all the participants of the QIP study for their contribution to the site work and all study participants for their cooperation. Further members of the QIP Study Group are as follows: Huibin Lin (Department of Respiratory and Critical Care Medicine, Zhanjiang Central People’s Hospital, Zhanjiang, China), Weiquan Liang (Department of Respiratory and Critical Care Medicine, The Second People’s Hospital of Foshan, Foshan, China), Kun Xiao (Department of Pulmonary and Critical Care Medicine, The Baiyun Hospital of Guangzhou First People’s Hospital [The Second People’s Hospital of Baiyun District], Guangzhou, China), Xianyong Zheng (Department of Respiratory and Critical Care Medicine, Jieyang City People’s Hospital, Jieyang, China), Liying Pan (Department of Respiratory and Critical Care Medicine, Dongguan Huangjiang Hospital, Dongguan, China), Yingyu Wu (Department of Respiratory and Critical Care Medicine, Chencun Hospital Affiliated to Shunde Hospital of Southern Medical University, Foshan, China), Yonghua Chen (Department of Pulmonary and Critical Care Medicine, Nanhai District Seventh People’s Hospital of Foshan, Foshan, China), Na Li (Department of Respiratory Medicine, Shen Zhen Long Gang District Sixth People’s Hospital, Longgang Central Hospital of Shenzhen, Shenzhen, China), Qian Zhang (Department of Respiratory Medicine, Changzhou Second People’s Hospital, Changzhou, China), Zhijun Jie (Department of Respiratory Medicine, Shanghai Fifth People’s Hospital, Shanghai, China), Xiangqi Chen (Department of Pulmonary and Critical Care Medicine, Fujian Medical University Union Hospital, Fuzhou, China), Yimin Lu (Department of Respiratory and Critical Care Medicine, The First People’s Hospital of Kunshan, Suzhou, China), Junhui Ye (Department of Respiratory Medicine, Sanmen People’s Hospital, Taizhou, China), Jinbao Wu (Department of Respiratory Medicine, Jinxian County People’s Hospital, Nanchang, China), Qian Wang (Department of Respiratory Medicine, Shanghai Jing’an District Zhabei Central Hospital, Shanghai, China), Xiaopeng He (Department of Respiratory Medicine, Xian Yang Central Hospital, Xianyang, China), Rong Qiu (Department of Pulmonary and Critical Care Medicine, Suining Central Hospital, Suining, China), Xiaowei Cheng (Department of Respiratory Medicine, Sichun Province Panzhihua Central Hospital, Panzhihua, China), Hao Xiong (Department of Pulmonary and Critical Care Medicine, Yibin Second People’s Hospital, Yibin, China), Wenzhong Zhu (Department of Respiratory Medicine, The Jintai Hospital of Baoji City, Baoji, China), Limei Tang (Department of Respiratory Medicine, Yao An County People’s Hospital, Chuxiong, China), Yajun Yuan (Department of Pulmonary and Critical Care Medicine, Tangshan People’s Hospital, Tangshan, China), Hong Chen (Department of Respiratory Medicine, The 2nd Affiliated Hospital of Harbin Medical University, Harbin, China), Ke Wang (Department of Respiratory and Critical Care Medicine, Jilin University Second Hospital, Changchun, China), Li Yu (Department of Respiratory and Critical Care Medicine, Hebei Gucheng County Hospital, Hengshui, China), Minxuan Li (Department of Respiratory Medicine, Qian’an People’s Hospital, Tangshan, China), Yi Hu (Department of Respiratory Medicine, The Central Hospital of Wuhan, Wuhan, China), Fang Sun (Department of Respiratory and Critical Care Medicine, Henan Provincial Chest Hospital, Zhengzhou, China), Li Zhang (Department of Respiratory Medicine, Wuhan Red Cross Hospital, Wuhan, China), Weimin Song (Department of Respiratory and Critical Care Medicine, XinCai People’s Hospital, Zhumadian, China), Suli Pei (Department of Respiratory Medicine, Nanjing Red Cross Hospital, Nanjing, China), Yanfen Yao (Department of Respiratory and Critical Care Medicine, Xinle City Hospital, Shijiazhuang, China), Ruling Dai (Department of Respiratory and Critical Care Medicine, Central Hospital of Zhuanghe City, Dalian, China), Xiaomei Yuan (Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Xinxiang Medical University, Xinxiang, China), Yong Deng (Department of Pulmonary and Critical Care Medicine, Wuxi County People’s Hospital, Chongqing, China).
Funding
This work was supported by AstraZeneca China, Shenzhen Clinical Research Center for Respiratory Disease (20220819095941004), and Shenzhen Key Laboratory of Respiratory Diseases (SYSPG20241211173920041).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fang L, Gao P, Bao H, et al. Chronic obstructive pulmonary disease in China: a nationwide prevalence study. Lancet Respir Med. 2018;6(6):421–12. doi:10.1016/S2213-2600(18)30103-6
2. Kunisaki KM, Dransfield MT, Anderson JA, et al. Exacerbations of Chronic Obstructive Pulmonary Disease and Cardiac Events. A Post Hoc Cohort Analysis from the SUMMIT Randomized Clinical Trial. Am J Respir Crit Care Med. 2018;198(1):51–57. doi:10.1164/rccm.201711-2239OC
3. Wallström O, Stridsman C, Lindberg A, Nyberg F, Vanfleteren L. Exacerbation History and Risk of Myocardial Infarction and Pulmonary Embolism in COPD. Chest. 2024;166(6):1347–1359. doi:10.1016/j.chest.2024.07.150
4. Halpin DMG, Healey H, Skinner D, Carter V, Pullen R, Price D. Exacerbation history and blood eosinophil count prior to diagnosis of COPD and risk of subsequent exacerbations. Europ Resp J. 2024;64(4):2302240. doi:10.1183/13993003.02240-2023
5. Dransfield MT, Kunisaki KM, Strand MJ, et al. Acute Exacerbations and Lung Function Loss in Smokers with and without Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2017;195(3):324–330. doi:10.1164/rccm.201605-1014OC
6. Gedebjerg A, Szépligeti SK, Wackerhausen LH, et al. Prediction of mortality in patients with chronic obstructive pulmonary disease with the new Global Initiative for Chronic Obstructive Lung Disease 2017 classification: a cohort study. Lancet Respir Med. 2018;6(3):204–212. doi:10.1016/S2213-2600(18)30002-X
7. Song Q, Cheng W, Liu C, et al. The future exacerbation and mortality of different inhalation therapies among patients with chronic obstructive pulmonary disease in various GOLD groups: a focus on the GOLD 2017 and GOLD 2023 reports. Therapeut Adva Respiratory Dis. 2023;17:17534666231213715. doi:10.1177/17534666231213715
8. Song Q, Liu C, Cheng W, et al. Clinical characteristics and risk of all-cause mortality in low education patients with chronic obstructive pulmonary disease in the Chinese population. J Glob Health. 2023;13:04163. doi:10.7189/jogh.13.04163
9. Yang T, Cai B, Cao B, et al. Exacerbation in patients with stable COPD in China: analysis of a prospective, 52-week, nationwide, observational cohort study (REAL). Therapeut Adva Respiratory Dis. 2023;17:17534666231167353. doi:10.1177/17534666231167353
10. (GOLD) GIfCOLD. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease (2023 REPORT). 2023. Available from: https://goldcopdorg/2023-gold-report-2/.
11. Jiao Y, Cheng Z, Gao Y, et al. Development and status quo of digestive endoscopy in China: an analysis based on the national census in 2013 and 2020. J Transl Intern Med. 2024;12(2):177–187. doi:10.2478/jtim-2023-0115
12. Wang F, Wang M, Chen X, et al. Quality of Care and Outcomes of Inpatients with COPD: a Multi-Center Study in China. Int J Chronic Obstr. 2025;20:1787–1795. doi:10.2147/COPD.S510613
13. Kurmi OP, Davis KJ, Hubert Lam KB, et al. Patterns and management of chronic obstructive pulmonary disease in urban and rural China: a community-based survey of 25 000 adults across 10 regions. BMJ Open Respiratory Res. 2018;5(1):e000267. doi:10.1136/bmjresp-2017-000267
14. Yang T, Cai B, Cao B, et al. Severity distribution and treatment of chronic obstructive pulmonary disease in China: baseline results of an observational study. Respir Res. 2022;23(1):106. doi:10.1186/s12931-022-02021-w
15. Yang T, Cai B, Cao B, et al. Treatment patterns in patients with stable COPD in China: analysis of a prospective, 52-week, nationwide, observational cohort study (REAL). Therapeut Adva Respiratory Dis. 2023;17:17534666231158283. doi:10.1177/17534666231158283
16. He R, Ren X, Huang K, et al. Influenza and pneumococcal vaccination coverage and associated factors in patients hospitalized with acute exacerbations of COPD in China: findings from real-world data. Chinese Med J. 2024;137(10):1179–1189. doi:10.1097/CM9.0000000000002790
17. Pang H, Pan Z, Adams R, et al. Community lung health service design for COPD patients in China by the Breathe Well group. Npj Primary Care Respiratory Med. 2022;32(1):27. doi:10.1038/s41533-022-00286-8
18. Houben-Wilke S, Vaes AW, Cuijpers M, et al. An overview of the importance of allied healthcare for patients with COPD. Expert Rev Respiratory Med. 2026;2026:1–13. doi:10.1080/17476348.2026.2629007
19. Adhikari S, Thapa S, Rattanapan C, Laosee O, Sriram S, Bhatta J. Evaluating the impact of self-management interventions on COPD outcomes in low- and middle-income countries in Asia: a systematic review. Health Qual Life Outcomes. 2025;23(1):81. doi:10.1186/s12955-025-02382-y
20. Pullen R, Miravitlles M, Sharma A, et al. CONQUEST Quality Standards: for the Collaboration on Quality Improvement Initiative for Achieving Excellence in Standards of COPD Care. Int J Chronic Obstr. 2021;16:2301–2322. doi:10.2147/COPD.S313498
21. (GOLD) GIfCOLD. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease (2025 REPORT). 2025. Available from: https://goldcopdorg/2025-gold-report/.
22. Mao R, Liu Z, Zhao Y, et al. Stable Chronic Obstructive Pulmonary Disease (COPD) Management Under a Tiered Medical System in China. Int J Chronic Obstr. 2022;17:181–194. doi:10.2147/COPD.S333274
23. Zeng Y, Cai S, Chen Y, et al. Current Status of the Treatment of COPD in China: a Multicenter Prospective Observational Study. Int J Chronic Obstr. 2020;15:3227–3237. doi:10.2147/COPD.S274024
24. Bao H, Jia G, Cong S, et al. Phenotype and management of chronic obstructive pulmonary disease patients in general population in China: a nationally cross-sectional study. Npj Primary Care Respiratory Med. 2021;31(1):32. doi:10.1038/s41533-021-00243-x
25. Zacarias EC, Castro AA, Cendon S. Effect of theophylline associated with short-acting or long-acting inhaled beta2-agonists in patients with stable chronic obstructive pulmonary disease: a systematic review. J Pneumologia. 2007;33(2):152–160. doi:10.1590/S1806-37132007000200009
26. Jenkins CR, Wen FQ, Martin A, et al. The effect of low-dose corticosteroids and theophylline on the risk of acute exacerbations of COPD: the TASCS randomised controlled trial. Europ Resp J. 2021;57(6):2003338. doi:10.1183/13993003.03338-2020
27. Devereux G, Cotton S, Fielding S, et al. Effect of Theophylline as Adjunct to Inhaled Corticosteroids on Exacerbations in Patients With COPD: a Randomized Clinical Trial. JAMA. 2018;320(15):1548–1559. doi:10.1001/jama.2018.14432
28. Cazzola M, Calzetta L, Page C, et al. Influence of N-acetylcysteine on chronic bronchitis or COPD exacerbations: a meta-analysis. Eur Respiratory Rev. 2015;24(137):451–461. doi:10.1183/16000617.00002215
29. Poole P, Sathananthan K, Fortescue R. Mucolytic agents versus placebo for chronic bronchitis or chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2019;5(5):Cd001287. doi:10.1002/14651858.CD001287.pub6
30. Gregoriano C, Dieterle T, Breitenstein AL, et al. Use and inhalation technique of inhaled medication in patients with asthma and COPD: data from a randomized controlled trial. Respir Res. 2018;19(1):237. doi:10.1186/s12931-018-0936-3
31. Sanchis J, Gich I, Pedersen S. Systematic Review of Errors in Inhaler Use: has Patient Technique Improved Over Time? Chest. 2016;150(2):394–406. doi:10.1016/j.chest.2016.03.041
32. Bao LK, Khoa ND, Chi LTK, Anh NT. Prevalence and Factors Affecting Appropriate Inhaler Use in Elderly Patients with Chronic Obstructive Pulmonary Disease: a Prospective Study. J Clin Med. 2023;12(13):4420. doi:10.3390/jcm12134420
33. Cho-Reyes S, Celli BR, Dembek C, Yeh K, Navaie M. Inhalation Technique Errors with Metered-Dose Inhalers Among Patients with Obstructive Lung Diseases: a Systematic Review and Meta-Analysis of U.S. Studies. Chronic Obstruct Pulmonary Dis. 2019;6(3):267–280. doi:10.15326/jcopdf.6.3.2018.0168
34. Press VG, Arora VM, Shah LM, et al. Teaching the use of respiratory inhalers to hospitalized patients with asthma or COPD: a randomized trial. J Gen Intern Med. 2012;27(10):1317–1325. doi:10.1007/s11606-012-2090-9
35. Aung H, Tan R, Flynn C, et al. Digital remote maintenance inhaler adherence interventions in COPD: a systematic review and meta-analysis. Eur Respiratory Rev. 2024;33(174):240136. doi:10.1183/16000617.0136-2024
36. Maimaitiming M, Ma J, Dong X, et al. Factors associated with the delay in informed consent procedures of patients with ST-segment elevation myocardial infarction and its influence on door-to-balloon time: a nationwide retrospective cohort study. J Transl Intern Med. 2024;12(1):86–95. doi:10.2478/jtim-2023-0127
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Health Inequality in the Global Burden of Chronic Obstructive Pulmonary Disease: Findings from the Global Burden of Disease Study 2019
Li H, Liang H, Wei L, Shi D, Su X, Li F, Zhang J, Wang Z
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1695-1702
Published Date: 28 July 2022
Patients with Chronic Obstructive Pulmonary Disease and Evidence of Eosinophilic Inflammation Experience Exacerbations Despite Receiving Maximal Inhaled Maintenance Therapy
Chen S, Miravitlles M, Rhee CK, Pavord ID, Jones R, Carter V, Emmanuel B, Alacqua M, Price DB
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2187-2200
Published Date: 9 September 2022
The Multidimensional Burden of COPD in China: A Propensity Score-Matched Comparison with Other Prevalent Non-Communicable Diseases
Sun Q, Lu B, Chen Q, Zheng Z
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:576684
Published Date: 3 March 2026
Epidemiological Trends and Projections of PM2.5-Attributable COPD Burden in China Over 1990–2035
Li M, Wang L, Amhare AF, Song Y, Wan P, Shi S, Qiao L, Guo Y
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:565060
Published Date: 16 March 2026