Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Contouring Plus: A Comprehensive Approach of the Lower Third of the Face with Calcium Hydroxylapatite and Hyaluronic Acid
Authors Viscomi B, Faria G ![]() , Hernandez CA, Perez L, Spada J, De la Fuente V, Muniz M
, Hernandez CA, Perez L, Spada J, De la Fuente V, Muniz M
Received 25 January 2023
Accepted for publication 20 March 2023
Published 5 April 2023 Volume 2023:16 Pages 911—924
DOI https://doi.org/10.2147/CCID.S400605
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Video abstract presented by Bianca Viscomi.
Views: 837
Bianca Viscomi,1 Gladstone Faria,2 Claudia A Hernandez,3 Luiz Perez,4 Julieta Spada,5 Victoria De la Fuente,6 Mariana Muniz7
1Dermatologist, Bianca Viscomi Dermatologia Private Practice, São Paulo, Brazil; 2Plastic Surgeon, Gladstone Institute Private Practice, São Paulo, Brazil; 3Dermatologist, MD Dermatology Private Practice, Medellin, Colombia; 4Dermatologist, Espaço Mira Private Practice, São Paulo, Brazil; 5Dermatologist, Dermatología y Estética Private Practice, Buenos Aires, Argentina; 6Dermatologist, Senshi Derma Clinic Studio Private Practice, Mexico City, Mexico; 7Dermatologist, Mariana Muniz Dermatologia Private Practice, São Paulo, Brazil
Correspondence: Bianca Viscomi, R Correia Dias, 530 suite 131, São Paulo, SP, 04104-001, Brazil, Tel +5511 97222-0525 ; +55113051-2304, Email [email protected]
Abstract: A well-defined jawline is aesthetically pleasing, so that rejuvenation of the jawline is becoming part of routine aesthetic practice. Restoring balance to the lower face without surgical intervention requires a multiple treatment approach, among which the minimally invasive injectables play a central role. Nevertheless, amidst the plethora of different injectable products available, choosing the option that best suits the patient’s need can be a challenge. A panel of experts sought to describe herein 4 clinical cases, illustrating the Contouring Plus technique, which provides a practical guidance for lower third assessment, choice of products, and treatment execution, especially among hyaluronic acid and calcium hydroxylapatite, aiming for immediate, as well as mid-to-long-term results.
Keywords: rejuvenation, biostimulation, neocollagenesis, collagen, calcium hydroxylapatite, hyaluronic acid, jawline treatment
Introduction
Facial aging encompasses a series of physiologic and morphologic changes over time, at every anatomic level (bone, muscles, ligaments, fasciae, subcutaneous fat, and skin).1,2 It has been suggested that most of the changes observed occur in the middle3 and the lower face4 due to the effects of gravity.5 A well-contoured jawline is an aesthetically agreeable feature in both women and men.6 Among the hallmarks of a youthful lower face include a well-defined jawline coursing smoothly from the mandibular angle to the chin, uninterrupted by the jowl or post-jowl and pre-jowl sulcus,7 whilst sagging along the jawline is said to be an indicator of facial aging and can have a significant impact on the overall appearance. Hence, rejuvenation of the jawline is becoming part of routine aesthetic practice, and number of procedures targeting this area have increased in the past years.8,9 Restoring balance to the lower face without surgical intervention requires a multiple treatment approach in a single session or spaced sequentially over a few weeks,2 among which the minimally invasive injectables play a central role. Optimal results can rarely be achieved with monotherapy.10 Dermal fillers used in monotherapy or in combination with other therapeutic options, such as calcium hydroxylapatite that has biostimulatory properties, allow enhancement of the jawline whist postponing, in part of the cases, the need for surgical procedures.11 Nonetheless, there is paucity of literature that establishes a straightforward approach covering lower third assessment with the adequate choice of products, especially among hyaluronic acid and calcium hydroxylapatite. In this setting, we sought to describe herein four clinical cases, illustrating the Contouring Plus technique, which provides a practical guidance for assessment of patient’s needs and adequate product choice, aiming for immediate, as well as mid-to-long term results.
Methods
All procedures performed in this report involving human patients were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Ethics Approval
The study was approved by a centralized institutional review board (Faculdade Santa Marcelina; protocol number 62558222.2.0000.8125). Written informed consent has been provided by all the patients to have the case details and any accompanying images published.
A panel of six experts in minimally invasive injectable procedures was assembled, in order to reach a recommendation on lower face improvement and rejuvenation.
We report four cases of facial lower third rejuvenation treated with the combination of undiluted calcium hydroxylapatite with 0.3% lidocaine hydrochloride (CaHA (+); Radiesse® (+); Merz North America, Inc., Raleigh, NC, USA) and a cohesive hyaluronic acid filler in different concentrations (ie, Belotero® Volume; 26.0 mg/mL and Belotero® Intense 25.0 mg/mL; Cohesive poly-densified matrix hyaluronic acid; Merz Pharmaceuticals GmbH, Frankfurt, Germany). Eligible patients were men or women, older than 18 years, who sought lower third rejuvenation and agreed to participate in the study.
Photographs were taken at baseline, immediately after injection and after a follow-up interval of 30 and 90 days after the procedure. Two-dimensional photographs (2D) were taken with a digital camera (Vectra Software, Canfield, NJ, USA). Standardized indirect light, distance of the camera, as well as aperture and speed were controlled. Digital photographs were reconstructed in three dimensions (3D) with Vectra Software (Canfield NJ, USA).
Case Series Description
Demography
Patients enrolled were between 29 and 54 years of age (median age, 39 years) and no relevant medical history (eg, use of medications that cause bleeding, diabetes, conditions that cause Koebner response, hypertrophic scars or keloid, previous facial surgery, myasthenia gravis, connective tissue diseases, multiple sclerosis, allergies, urticaria, angioedema; recent history of acute respiratory infections, presence of active infections, dental treatment, use of permanent fillers and other inflammatory processes in the area to be treated, any injectable procedure or facial surgery within the last 12 months).
General Considerations
Anatomy and Aging
The mandible is considered the framework of the lower face, on top of which the muscles and soft tissues rest,12 and consists of an inferior portion with a horseshoe-like appearance, denominated body of the mandible, and two perpendicular parts known as mandibular ramus. The area between the mentum and the angle of the mandible is frequently named mandibular line.4 During aging, the mandible undergoes a series of changes resulting in decrease in bone support: decrease in mandible volume, resorption of the inferior border of the angle (next to body–ramus junction), increase in mandible angle from around 95° to 135°, while the chin becomes shorter, more anterior and oblique.13,14 Furthermore, the aging process of the mandible contour also comprises the atrophy of the mandibular fat compartments, weakening of the retaining ligaments and skin laxity,2,4,15 which lead to soft tissue descent, which combined with bone resorption, are clinically translated into two main aesthetic concerns: disruption of a smooth jawline and the development of jowls.14
The jowls are believed to be a product of the sum of alterations of jowl fat compartments, the mandibular septum and submandibular fat compartments and overlying skin.15 Among the mechanisms described for jowl formation are hypertrophy and displacement of jowl fat pads (both superior and inferior), as well as dehiscence of the mandibular septum, responsible for the downward movement of the superior and inferior compartments to the neck.4,15 Attenuation of the retaining ligaments (eg, masseteric ligaments) that should tether the soft tissues into the anatomic position of youth could contribute to jowl formation.16
The combination of anterior and posterior mandibular volume loss, in conjunction with jowl descent, become more pronounced at the mid-mandibular border, converting the youthful shape jawline to an irregular “W” shape.7 A genetically underdeveloped chin is also associated with an early loss of definition of the jawline.11
Caution Points
Although serious complications are rare, crucial structures in the jawline area, such as arteries, nerves (terminal branches of facial and trigeminal nerves), and the parotid gland, need to be avoided.11 The major vessel responsible for supplying blood to the face is the facial artery, which may be palpable as it crosses the lateral border of the mandible anterior to the insertion of the masseter.11,17 Extra care should be taken with the parotid, since the facial nerve crosses the gland and intraglandular injection may lead to parotiditis. Therefore, injecting in the correct plane is paramount to avoid complications (ie, subdermal subcutaneous plane while injecting the mandible body and supraperiosteal plane in the mandible angle). Moreover, injections into the masseter itself should be avoided as may lead to nodule formation.11
Patient Assessment
A careful patient assessment is paramount before any injection, to evaluate a patient’s needs, as well as align the patient’s expectations. Since the mid-face has also impact on neighboring esthetic units,18 it is crucial to assess the middle third and assure that it is not impacting the lower third. The overall objectives for lower third rejuvenation are to adjust the position and prominence of the mandibular angle, improve skin and subcutaneous tissue, improve cervical–mental angle, and adjust width height and projection of the chin. Furthermore, gender differences should always be considered, since the jaw figures among the facial features, that when seen in isolation, convey more information about perceived gender.19,20 Males have a square-shaped face, with a broader mandible, larger masseter, and wider and more prominent chin, while female faces are more triangular, with a more delicate chin and jawline.14 Moreover, males and females seem to differ regarding the injection site preference, so that males outnumber their female counterparts in a 6:1 ratio for filler injections along the jawline.21
For jawline rejuvenation, the most suitable dermal fillers include CaHA, an injectable HA with the most adequate rheological characteristic and mechanism of action for the aesthetic concern, or an association of CaHA and HA, depending on the patient’s needs and the desired aesthetic outcome.11 CaHA and HA injections can be performed in the same session or in different sessions.
First and foremost, the assessment of skin laxity should drive the evaluation, since it implies the use or not of a collagen biostimulator (Figure 1). If the patient presents laxity, the use of CaHA should always be indicated, as it can improve the extracellular matrix by inducing new tissue formation through neocollagenesis, dermal cell proliferation, angiogenesis and elastin production, and hence, contour improvement and laxity treatment.22–24 Nevertheless, even If no laxity is present, CaHA should also be considered as beneficial for aging prevention for both men and women.25
 |
Figure 1 Clinical algorithm for facial contour approach. CaHA(+) (Radiesse ®(+); Merz North America, Inc., Raleigh, NC, USA) should be the base for the lower face treatment for all patients, aiming for aging prevention (prejuvenation) in younger patients and to address laxity, sagging and loss of contour in older patients. If needed, combination treatment with hyaluronic acid can be performed (HAV; Belotero® Volume and HAI; Belotero® Intense; Cohesive poly-densified matrix hyaluronic acid; Merz Pharmaceuticals GmbH, Frankfurt, Germany). |
CaHA has one of the highest viscoelasticities when compared with other dermal fillers, allowing it to remain in the place where it is injected not migrating into the surrounding tissue.26 In the Contouring Plus technique, the undiluted CaHA with 0.3% lidocaine hydrochloride (CaHA (+); Radiesse® (+); Merz North America, Inc. Raleigh, NC, USA) is the CaHA presentation of choice, since it presents high ability to resist deformation and not to migrate (high viscoelasticity),17,26 ideal for use in specific areas that need focal support (eg, mandible body and ramus), as well as bio stimulation properties,22 ideal for laxity treatment. CaHA (+) presents 30% synthetic calcium hydroxylapatite suspended in a gel carrier of sterile water for injection, glycerin, and sodium carboxymethylcellulose, with 0.3% powdered lidocaine hydrochloride. Each pre-filled, steam-sterilized syringe (1.5 cc) has microspheres of calcium hydroxylapatite with smooth surface27 and particle-size range of 25‒45 µm.28 The choice of CaHA brand also considered the type of microspheres, since there is statistically significant difference if a microparticle has rough or smooth surface, as well as it is the interaction with the tissues.29 In the long-term biological response, microparticles with regular shape and smooth surface lead to the best tissue augmentation in the form of fibroblast and collagen fibers surrounding the microspheres, whilst foreign body granuloma is the main response to microparticles with rough surface and irregular shape.29
Besides laxity, it is important to evaluate the need of projection and/or volumization. If the patient has the need of projectionand/or volumization, the use of hyaluronic acid is indicated. HA can be injected sequentially in the same session as CaHA or in different sessions.
Concerning the choice of HA, it is crucial to consider the rheology (viscosity and elasticity) of the product. Viscosity of a gel (η* or Gʺ) relates to the ability of the fluid phase to resist shearing forces (eg, when filler is injected between two anatomical layers or is placed in a single layer but is influenced by the movements of another layer), so that a high-viscosity gel is more difficult to spread.26 Elasticity of a gel (elastic modulus; Gʹ), is the gel’s ability to resist deformation when shearing pressure is applied.26 The higher the Gʹ the more lift it can provide, since the less it deforms under pressure. Other parameters include 1) measurement of the compression force in static mode (mimicking the permanent pression of the skin on the filler) which correlates with the filler capacity to lift the tissues. The higher the Force normal (Fn) of a hyaluronic acid filler, the higher the lifting capacities; 2) elastic module measured under dynamic compression forces (Eʹ; mimicking the mobile compression forces applied on the filler during facial expressiveness), which reflects the space-filling capacity of a filler. The higher the Eʹ, the higher the volumizing capacity.30
Thus, when projection or structure is desired, a HA with high Gʹ, Eʹ and Fn30 (HAI; Belotero® Intense; Cohesive poly-densified matrix hyaluronic acid; Merz Pharmaceuticals GmbH, Frankfurt, Germany) provides better support for soft tissues.31 If volumization, shaping or enhancement of an area is needed, a moldable hyaluronic acid, with balanced Gʹ (HAV; Belotero® Volume; Cohesive poly-densified matrix hyaluronic acid; Merz Pharmaceuticals GmbH, Frankfurt, Germany) should be the choice.31,32
Treatment Plan
Mandible
An entry point located in the apex of the Jowl grants access to the mandible body in both directions (mandible angle and chin). Usually, a volume of 1.5mL/side of CaHA (+) is recommended. Linear retro-injection or injection of micro boluses of CaHA (+) (up to 0.05mL/bolus) should be performed with a 22G cannula, in the subdermal plane, slightly below the mandible body, along the vector lines in Figure 2, to elongate the lower third and enhance the facial frame. Using an entry point in the mandible angle, linear retro-injection or injection of micro boluses in a fanning pattern should be performed along the mandible ramus.
 |
Figure 2 Possible treatment areas in the contouring plus technique (Frontal view): (Radiesse® (+); Merz North America, Inc., Raleigh, NC, USA). In purple, areas to be approached with a moldable hyaluronic acid, with balanced Gʹ hyaluronic acid (HAV; Belotero® Volume; Cohesive poly-densified matrix hyaluronic acid; Merz Pharmaceuticals GmbH, Frankfurt, Germany), whilst in red, areas in which a HA with high resistance to deformity (high Gʹ, Eʹ and Fn; HAI; Belotero® Intense; Cohesive poly-densified matrix hyaluronic acid; Merz Pharmaceuticals GmbH, Frankfurt, Germany) should be the choice. Round areas correspond to supraperiosteal plane of injection. The triangle and rectangle areas correspond to injections performed in the subcutaneous plane. |
If further definition of the mandible line is sought, retro-injection of hyaluronic acid in the superficial subcutaneous plane can be performed along the mandible body (Figures 2–7). The choice of a moldable hyaluronic acid, with balanced Gʹ (HAV) should be preferable for women, since it allows shaping and conveys a subtle contour (Figure 4 and Figure 7), whilst in men the injection of a HA with high Gʹ, Eʹ and Fn27 (HAI; Belotero® Intense; Cohesive poly-densified matrix hyaluronic acid; Merz Pharmaceuticals GmbH, Frankfurt, Germany) in the deep subcutaneous plane maybe needed, since a more pronounced projection of the soft tissues is desired, to have a more defined mandible (Figures 5 and 6).
 |
Figure 3 Possible treatment areas in the contouring plus technique (oblique view): (Radiesse® (+); Merz North America, Inc., Raleigh, NC, USA) should be performed slightly below the mandible body (blue rectangle), whereas if further definition of the mandible line is sought, a moldable HA (purple rectangle; HAV; balanced Gʹ; Belotero® Volume; Cohesive poly-densified matrix hyaluronic acid; Merz Pharmaceuticals GmbH, Frankfurt, Germany) can be injected along the mandible body in the superficial subcutaneous plane, superior to CaHA. In red, areas to be approached with a high Gʹ, Eʹ and Fn hyaluronic acid (red; HAI; Belotero® Intense; Cohesive poly-densified matrix hyaluronic acid; Merz Pharmaceuticals GmbH, Frankfurt, Germany). Round areas correspond to supraperiosteal plane of injection, whilst triangle and rectangle areas correspond to injections performed in the subcutaneous planeI. |
 |
Figure 4 Clinical case 1: 34-year-old woman. In the chin: HAV 1mL was injected with cannula in the subcutaneous layer, while a 0.6 supraperiosteal bolus of HAI was injected with a 27-G needle, close to the inferior border of the chin. A total volume of 1.5mL of CaHA(+) per side was injected in the subcutaneous layer, slightly below the mandible ramus, along its length, while 0.5mL of HAV was injected in the superficial subcutaneous layer along the mandible ramus for further definition. Images taken with Vectra Software at baseline (A, D, G, J, M), after 30 days (B, E, H, K, N) and 90 days (C, F, I, L, O) after the treatment session. |
 |
Figure 5 Clinical case 4: 44-year-old man. In the chin: 1mL of HAV was injected with cannula in subcutaneous layer in the crease, while supraperiosteal boluses of HAI were injected (0.3 lateral bolus/0.6 central bolus/0.3 lateral bolus) close to the inferior border of the chin. A total volume of 1.0mL of CaHA(+) per side was injected in the subcutaneous layer, slightly below the mandible ramus, along its length, while 0.5mL of HAI was injected in the supraperiosteal plane in the mandible angle. Images taken with Vectra Software. at baseline (A, D, G, J, M), after 30 days (B, E, H, K, N) and 90 days (C, F, I, L, O) after the treatment session. |
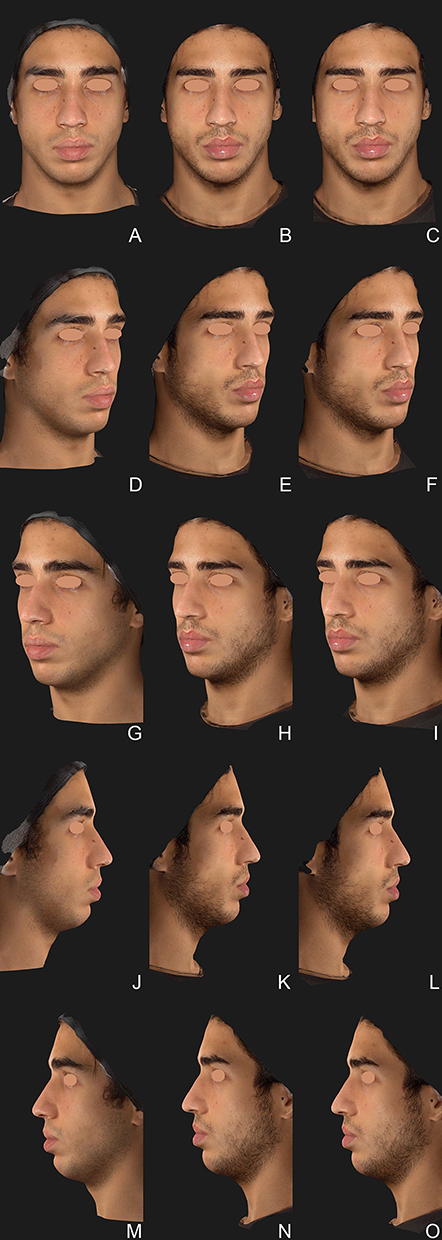 |
Figure 6 Clinical case 3: 29-year-old man. In the chin: 1mL of HAV was injected with cannula in subcutaneous layer in the crease, while supraperiosteal boluses of HAI were injected (0.3 lateral bolus/0.6 central bolus/0.3 lateral bolus) close to the inferior border of the chin. A total volume of 1.5mL of CaHA(+) per side was injected in the subcutaneous layer, slightly below the mandible ramus, along its length, while 0.5mL of HAI was injected in the supraperiosteal plane in the mandible angle. Images taken with Vectra Software. at baseline (A, D, G, J, M), after 30 days (B, E, H, K, N) and 90 days (C, F, I, L, O) after the treatment session. |
 |
Figure 7 Clinical case 2: 54-year-old woman. A 0.6mL supraperiosteal bolus of HAI was injected in in the pogonium (most anterior point of the chin) and 0.7mL of HAI was injected in each side of the pre-jowl sulcus. A total volume of 1.0mL of CaHA(+) per side was injected in the subcutaneous layer, slightly below the mandible ramus, along its length, while 0.5mL of HAV was injected in the superficial subcutaneous layer along the mandible ramus for further definition. Images taken with Vectra Software. at baseline (A, D, G, J, M), after 30 days (B, E, H, K, N) and 90 days (C, F, I, L, O) after the treatment session. |
In males, a supraperiosteal bolus of 0.5mL of HAI in the mandible angle allows further definition of the mandible angle and broadening of the face (Figure 6).
The volume needs to be tailored to each patient’s needs, but as a suggestion we used 0.5mL of HAV per side, with a 22G cannula and an entry point in the apex of the jowl. Avoid injecting near the apex of the jowl, as this could worsen its appearance. The injections can be performed in the same session or in different sessions. Although when crossing the mandible, the facial artery is in a subplatysmal location, it is important to point out that it superficializes becoming subdermal when approaching the modiolus. No major vessels are observed in the subdermal plane.1 Nevertheless, a careful approach should be taken when injecting in the supraperiosteal plane.
Pre-Jowl Sulcus
If deemed necessary, the treatment target of the pre-jowl sulcus should be a triangle area with its apex in the corner of the mouth (Figures 2,3 and 7). The entry point in the apex of the jowl allows retro-injection in a fanning pattern with a 22G cannula in the subdermal plane of 0.5mL of HA per side (Figures 2,3 and 7). For the corner of the mouth, injection of subdermal 0.2-mL bolus should be performed. The choice of a moldable hyaluronic acid (HAV) is preferable to provide a more natural look.
Labio-Mental Sulcus
Labio-mental sulcus should be assessed with HAV, subdermal with a 22G cannula, with an entry point located in one of the edges of the sulcus (Figures 2, 3 and 6).
Chin
Pogonium (or the most anterior point of the chin) should be evaluated beforehand, since treatment of this point is relevant for both improvement of the mandibular line, as well as the patient’s profile. For an anterior projection, a 0.5–1.0-mL bolus of HAI with a 27-G needle in the supraperiosteal plane. For further shaping of the chin, a moldable hyaluronic acid (HAV) should be injected in the deep subcutaneous plane with a 22–25G cannula, through the same entry point in the apex of the jowl (Figures 2–7).
Aiming for vertical projection of the chin, a supraperiosteal bolus of HAI with a 27-G needle, should be injected close to the inferior border of the chin. In females, a single bolus of 0.5mL should be injected to avoid widening of the chin, while in males, 3 boluses may be necessary to enlarge the chin (0.5mL central bolus and 0.25–0.3mL for each lateral bolus).
A total volume of 3mL of hyaluronic acid should be considered for the treatment of the chin. Approximately 1.5 cm superior to the mandibular border in line with the first and second premolar lies the mental neurovascular bundle, which should be avoided, since injury to the mental nerve results in anesthesia or dysesthesias of the lower lip and embolism can occur in the artery.11
Discussion
Sagging of the lower third is indicative of facial aging5 and can have a significant impact on appearance.11 Restoration of facial contour encompasses the repositioning of the descended facial tissues to the anatomic position of the youthful face.16 Treatment of the jawline improves both the anterior and lateral profiles of the face, which in association with repositioning of soft tissues of the cheek, may result in a lifting effect of the cheek and neck.33 Therefore, rejuvenation of the lower third is becoming an increasingly routine treatment and is essential for a good overall result. In a review from 2008 of the most frequent patient-preferred injection sites for facial volume augmentation with hyaluronic acid, jawline figured only in eighth place,9 whereas in 2018, the most popular treatment areas were the midface (37.6%) and jawline (prejowl sulcus, mandibular angle, and chin; 26.3%).8 Combination of multiple aesthetic therapies focusing on different aspects of the facial aging process, besides improving overall efficacy, also provides a higher level of patient satisfaction.34
When choosing an injectable product for the lower face, it is paramount to take into consideration the presence of laxity, the need of projection and/or volumization, as well as the rheological properties of the products. The presence of laxity implies the use of CaHA, aiming to induce neocollagenesis, elastin production, and angiogenesis, improving the extracellular matrix and dermal cell proliferation.22 The unique characteristics of CaHA (high elasticity and viscosity,26 as well as its ability to induce long-term collagen formation) render it with great versatility, appropriate for treating patients at any stage of the aging process17 from aging prevention to facial aging treatment per se. It is a recommendation of the panel of experts to use CaHA as the base for the lower face treatment for all patients, aiming for aging prevention (prejuvenation) in younger patients and to address laxity, sagging and loss of contour in older patients. Calcium hydroxylapatite provides immediate and long-lasting correction. It provides an initial immediate volume replacement. Over time, the carrier gel is gradually absorbed, leaving the CaHA microspheres to induce neocollagenesis at the injection site, resulting in longer term correction of laxity.23,24,35 Immunohistochemical analysis after neck laxity treatment with diluted CaHA (1:2 dilution (normal skin), 1:4 dilution (thin skin), and 1:6 dilution (atrophic skin)) demonstrated significant increases in collagen I and III expression compared with baseline, aligned with observation of improvement in skin elasticity and pliability and with increases in dermal thickness as assessed by ultrasound.36 A statistically significant improvement in jawline scores was observed at each post-treatment visit after a mean total volume of CaHA without lidocaine injected ranging from 3.90 mL in patients with mild sagging (score 1) at baseline to 6.68 mL in patients with mild to moderate sagging (score 1.5), in line with patient satisfaction (81% of the patients deemed contour restoration as “improved” to “very much improved” at one-year post injection).37 When CaHA(+) is used undiluted with lidocaine, given its lifting (high viscoelasticity), as well as bio stimulation properties,23,24 is ideal for focal collagen stimulation along the mandible contour. CaHA(+) injection for the treatment of the jawline presented significant results with a maximal 1.9-point decrease from baseline at 6 weeks using the jawline assessment scale, with long-lasting results up to 12 months.33 Similar results were observed in a randomized evaluator blinded trial, with an average of a 1.3-point improvement in a 5-point scale at Day 30 after injection of CaHA(+).38
While the biostimulatory effects of CaHA lead to global improvement and repositioning of the skin, if further projection or volumization is needed, the associated use of a hyaluronic acid is the best option. Cohesive polydensified matrix (CPM®) technology fillers contain a unique balance between viscosity and elasticity that allows for a more homogeneous intradermal distribution of the material, so that when compared to other fillers provide a “smoother” esthetic effect.39–41 For projection, the most appropriate choice would be a HA with high resistance to deformity (high Gʹ; elastic module)26 and high capacity to lift tissues (high Fn) such as HAI.30 In a double-blind, half-side comparison study, HAI was associate with a higher response rate (proportion of patients with at least 1-grade improvement in wrinkle severity (WSRS) for NLF) and higher patient’s satisfaction when compared to NASHA filler, possibly due to the slightly better esthetic results and lower pain.42
For volumization, a high volumization capacity (high Eʹ) hyaluronic acid should be the obvious choice. The higher the Eʹ, the higher the volumizing capacity since Eʹ reflects the space-filling capacity of a filler. HAV presented the highest Eʹ among nine marketed cross-linked hyaluronic acids.30 Furthermore, HAV has a combination of rheological properties that provides the product with several advantages including high plasticity (ability of gel to be shaped and molded after injection), balanced Gʹ with viscosity that maintains ease of injection, reduced risk of product migration, long duration of aesthetic effect and good tolerability.32 In a randomized, controlled, evaluator-blind, split-face clinical study, Global Aesthetic Improvement Scale (GAIS) rating showed that significantly more patients had better improvement with HAV than with the comparator (Juvéderm® Voluma®; Allergan Inc., Pringy, France) at month 1, 3, 12 and 18 (p=0.0032, p=0.0074, p=0.0384 and p=0.0110, respectively).43 This can be explained by the fact that HAV has a similar G prime to VYC-20 but has a higher resistance to dynamic compression (E prime).43 In an open-label study to evaluate the efficacy of HAV for the treatment of intermediate-to-severe volume loss in the mid-third of the face, at least 94% of the patients were rated as “very much improved” or “much improved” as per Investigators’ Global Aesthetic Improvement Scale (GAIS) assessment up to month 6. At Month 9, all patients still showed a benefit of treatment with 81% rated as “very much” or “much improved”.44
Conclusion
The association of products with distinct characteristics enables tailoring of the treatment for the patient’s needs, from the choice of the most adequate product to each anatomic area and aesthetic concern, to the injection technique and skin layer to be assessed. For instance, the improvement of laxity in the lower third is superior with the use of CaHA (+), due to its bio stimulatory properties,22 and hence should be the product of choice for lower third’s flaccidity, while HA with different rheological properties is indicated to project or volumize specific areas, according to the patient’s needs.
Acknowledgment
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Medical writing and editorial assistance were provided by Dr Danielle Shitara, (Private Practice) and was supported by Medical Affairs of Merz Aesthetics LATAM, through its affiliate Merz Farmaceutica Comercial Ltda, in accordance with Good Publication Practice guidelines.
Funding
Merz Aesthetics LATAM funded medical writing assistance and provided products to this study through its affiliate in Brazil - Merz Farmacêutica Comercial Ltda. Despite this support, this study was conducted with autonomy and independence by the medical authors, and Merz Farmacêutica Comercial, Ltda. had any participation or influence to design, conduct, collect, assess and evaluate the presented data.
Disclosure
Drs Viscomi, Faria, Hernández, Perez, Spada, De la Fuente, and, Muniz have been speakers for Merz Pharmaceuticals. Dr Luiz Perez, Dr Bianca VIscomi and Dr Claudia Hernández areGlobal Key Opinion Leaders for Merz Aesthetics. The authors report no other conflicts of interest in this work.
References
1. Suwanchinda A, Rudolph C, Hladik C, et al. The layered anatomy of the jawline. J Cosmet Dermatol. 2018;17(4):625–631. doi:10.1111/jocd.12728
2. Carruthers J, Carruthers A, Multimodal A. Approach to rejuvenation of the lower face. Dermatol Surg. 2016;42:S89–S93. doi:10.1097/DSS.0000000000000749
3. Cotofana S, Schenck TL, Trevidic P, et al. Midface: clinical anatomy and regional approaches with injectable fillers. Plast Reconstr Surg. 2015;136(5 Suppl):219S–234S. doi:10.1097/PRS.0000000000001837
4. Braz A, Humphrey S, Weinkle S, et al. Lower face. Plast Reconstr Surg. 2015;136:235S–257S. doi:10.1097/PRS.0000000000001836
5. Agarwal A, DeJoseph L, Silver W. Anatomy of the jawline, neck, and perioral area with clinical correlations. Facial Plast Surg. 2005;21(1):3–10. doi:10.1055/s-2005-871757
6. Mommaerts MY. The ideal male jaw angle – an internet survey. J Craniomaxillofac Surg. 2016;44(4):381–391. doi:10.1016/j.jcms.2015.12.012
7. Buckingham E, Glasgold R, Kontis T, et al. Volume rejuvenation of the lower third, perioral, and jawline. Facial Plast Surg. 2015;31:70–79.
8. Vandeputte J. Real-world experience with volume augmentation using cohesive polydensified matrix hyaluronic acid gel: a retrospective single-center analysis of 110 consecutive patients with medium- to long-term follow-up. J Clin Aesthet Dermatol. 2018;11(12):30–39.
9. Morris CL, Stinnett SS, Woodward JA. Patient-preferred sites of restylane injection in periocular and facial soft-tissue augmentation. Ophthalmic Plast Reconstr Surg. 2008;24(2):117–121. doi:10.1097/IOP.0b013e318166dd2a
10. Carruthers J, Burgess C, Day D, et al. Consensus recommendations for combined aesthetic interventions in the face using botulinum toxin, fillers, and energy-based devices. Dermatol Surg. 2016;42(5):586–597. doi:10.1097/DSS.0000000000000754
11. Moradi A, Shirazi A, David R. Nonsurgical Chin and jawline augmentation using calcium hydroxylapatite and hyaluronic acid fillers. Facial Plast Surg. 2019;35(2):140–148. doi:10.1055/s-0039-1683854
12. Romo T, Yalamanchili H, Sclafani AP. Chin and prejowl augmentation in the management of the aging jawline. Facial Plast Surg. 2005;21(1):38–46. doi:10.1055/s-2005-871762
13. Avelar LE, Cazerta CE, Avè MN, Shitara DI. Dynamic changes of facial supporting cornerstones (pillars): considerations in aesthetic approach. J Drugs Dermatol. 2018;17:466–470.
14. Toledo Avelar LE, Cardoso MA, Santos Bordoni L, et al. Aging and sexual differences of the human skull. Plast Reconstr Surg Glob Open. 2017;5(4):e1297. doi:10.1097/GOX.0000000000001297
15. Reece E, Rohrich R. The aesthetic jaw line: management of the aging jowl. Aesthet Surg J. 2008;28:668–674. doi:10.1016/j.asj.2008.09.007
16. Cohen S, Artzi O, Mehrabi JN, et al. Vectorial facial sculpting: a novel sub‐SMAS filler injection technique to reverse the impact of the attenuated retaining ligaments. J Cosmet Dermatol. 2020;19(8):1948–1954. doi:10.1111/jocd.13546
17. Van Loghem J, Yutskovskaya YA, Werschler WP. Calcium hydroxylapatite: over a decade of clinical experience. J Clin Aesthet Dermatol. 2015;8:38–49.
18. Wollina U. Facial rejuvenation starts in the midface: three-dimensional volumetric facial rejuvenation has beneficial effects on nontreated neighboring esthetic units. J Cosmet Dermatol. 2016;15(1):82–88. doi:10.1111/jocd.12175
19. Brown E, Perrett DI. What gives a face its gender? Perception. 1993;22(7):829–840. doi:10.1068/p220829
20. Faria GEDL, Bento AM, Dos Santos DB, et al. Facial beautification with fillers and main differences between genders. Rev Bras Cir Plást. 2021;36:100.
21. Wang JV, Valiga A, Albornoz CA, et al. Comparison of injectable filler locations in men and women: an age‐matched case analysis. J Cosmet Dermatol. 2021;20:2469–2471. doi:10.1111/jocd.14293
22. de Almeida AT, Figueredo V, da Cunha ALG, et al. Consensus recommendations for the use of hyperdiluted calcium hydroxyapatite (radiesse) as a face and body biostimulatory agent. Plast Reconstr Surg Glob Open. 2019;7:e2160. doi:10.1097/GOX.0000000000002160
23. González N, Goldberg DJ. Evaluating the effects of injected calcium hydroxylapatite on changes in human skin elastin and proteoglycan formation. Dermatol Surg. 2019;45(4):547–551. doi:10.1097/DSS.0000000000001809
24. Yutskovskaya Y, Sergeeva A, Kogan E. Combination of calcium hydroxylapatite diluted with normal saline and microfocused ultrasound with visualization for skin tightening. J Drugs Dermatol. 2020;19(4):405–411. doi:10.36849/JDD.2020.4625
25. Hogan SR, Zachary CB, Arndt KA. Prejuvenation: definition of the term and evolution of the concept. Dermatol Surg. 2021;47(6):871–872. doi:10.1097/DSS.0000000000002929
26. Sundaram H, Voigts B, Beer K, et al. Comparison of the rheological properties of viscosity and elasticity in two categories of soft tissue fillers: calcium hydroxylapatite and hyaluronic acid. Dermatol Surg. 2010;36 Suppl 3:1859–1865. doi:10.1111/j.1524-4725.2010.01743.x
27. Marmur ES, Phelps R, Goldberg DJ. Clinical, histologic and electron microscopic findings after injection of a calcium hydroxylapatite filler. J Cosmet Laser Ther. 2004;6(4):223–226. doi:10.1080/147641704100003048
28. Merz North America Inc. Radiesse (+) lidocaine instructions for use; 2022. Available from: www.Radiesse.com.
29. Laeschke K. Biocompatibility of microparticles into soft tissue fillers. Semin Cutan Med Surg. 2004;23(4):214–217. doi:10.1016/j.sder.2004.09.005
30. Gavard Molliard S, Albert S, Mondon K. Key importance of compression properties in the biophysical characteristics of hyaluronic acid soft-tissue fillers. J Mech Behav Biomed Mater. 2016;61:290–298. doi:10.1016/j.jmbbm.2016.04.001
31. van Loghem J, Sattler S, Casabona G, et al. Consensus on the use of hyaluronic acid fillers from the cohesive polydensified matrix range: best practice in specific facial indications. Clin Cosmet Investig Dermatol. 2021;14:1175–1199. doi:10.2147/CCID.S311017
32. Micheels P, Ascher B, Beilin G, et al. Évaluation clinique de l’efficacité et l’innocuité d’un acide hyaluronique volumateur de technologie CPM® pour le traitement de multiples zones du visage [Treatment of Age-related Mid-face Atrophy by Injection of Cohesive Polydensified Matrix Hyaluronic Acid Volumizer]. Réalités thérapeutiques en Dermato-Vénérologie. 2014;235:2–8.
33. Juhász MLW, Marmur ES. Examining the efficacy of calcium hydroxylapatite filler with integral lidocaine in correcting volume loss of the jawline—a pilot study. Dermatol Surg. 2018;44(8):1084–1093. doi:10.1097/DSS.0000000000001528
34. Humphrey S, Beleznay K, Fitzgerald R. Combination therapy in midfacial rejuvenation. Dermatol Surg. 2016;42 Suppl 2:S83–S88. doi:10.1097/DSS.0000000000000747
35. Dallara J-M, Baspeyras M, Bui P, et al. Calcium hydroxylapatite for jawline rejuvenation: consensus recommendations. J Cosmet Dermatol. 2014;13(1):3–14. doi:10.1111/jocd.12074
36. Yutskovskaya YA, Kogan EA. Improved neocollagenesis and skin mechanical properties after injection of diluted calcium hydroxylapatite in the neck and décolletage: a pilot study. J Drugs Dermatol. 2017;16:68–74.
37. Baspeyras M, Dallara J-M, Cartier H, et al. Restoring jawline contour with calcium hydroxylapatite: a prospective, observational study. J Cosmet Dermatol. 2017;16(3):342–347. doi:10.1111/jocd.12335
38. Boen M, Alhaddad M, Goldman MP, et al. A randomized, evaluator-blind, split-face study evaluating the safety and efficacy of calcium hydroxylapatite for jawline augmentation. Dermatol Surg. 2022;48(1):76–81. doi:10.1097/DSS.0000000000002582
39. Sundaram H, Cassuto D. Biophysical characteristics of hyaluronic acid soft-tissue fillers and their relevance to aesthetic applications. Plast Reconstr Surg. 2013;132:5S–21S. doi:10.1097/PRS.0b013e31829d1d40
40. Ducher G, Prasetyo AD, Rubin MG, et al. Hyaluronic acid fillers with cohesive polydensified matrix for soft-tissue augmentation and rejuvenation: a literature review. Clin Cosmet Investig Dermatol. 2016;9:257–280. doi:10.2147/CCID.S106551
41. Santoro S, Russo L, Argenzio V, et al. Rheological properties of cross-linked hyaluronic acid dermal fillers. J Appl Biomech Biomech. 2011;9(2):127–136. doi:10.5301/JABB.2011.8566
42. Buntrock H, Reuther T, Prager W, et al. Efficacy, safety, and patient satisfaction of a monophasic cohesive polydensified matrix versus a biphasic nonanimal stabilized hyaluronic acid filler after single injection in nasolabial folds. Dermatol Surg. 2013;39(7):1097–1105. doi:10.1111/dsu.12177
43. Kerscher M, Agsten K, Kravtsov M, et al. Effectiveness evaluation of two volumizing hyaluronic acid dermal fillers in a controlled, randomized, double-blind, split-face clinical study. Clin Cosmet Investig Dermatol. 2017;10:239–247. doi:10.2147/CCID.S135441
44. Micheels P, Vandeputte J, Kravtsov M. Treatment of age-related mid-face atrophy by injection of cohesive polydensified matrix hyaluronic acid volumizer. J Clin Aesthet Dermatol. 2015;8:28–34.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Tolerability of Hyperdiluted Calcium Hydroxylapatite (Radiesse) for Neck Rejuvenation: Clinical and Ultrasonographic Assessment
Trindade de Almeida AR, Marques ERMC, Contin LA, Trindade de Almeida C, Muniz M
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1341-1349
Published Date: 25 May 2023
Buttocks Beautification 3D with Calcium Hydroxylapatite (RadiesseTM): An Individualized Approach to Diagnosing and Treating Contour, Sagging, and Cellulite of the Buttocks in Seven Cases
Teodoro MDS, Di Sessa D, Barros JHDFA, Vasconcelos RCFD, Miot HA
Clinical, Cosmetic and Investigational Dermatology 2023, 16:3039-3051
Published Date: 24 October 2023
Applying the MD Codes™ to Treat Emotional and Social Attributes with HA Fillers: A Retrospective Serial Case Study
de Maio M, Brenninkmeijer EEA, Nurlin I, Colucci L, Sanchez T
Clinical, Cosmetic and Investigational Dermatology 2023, 16:3441-3453
Published Date: 29 November 2023
Starting Point for Protocols on the Use of Hyperdiluted Calcium Hydroxylapatite (Radiesse®) for Optimizing Age-Related Biostimulation and Rejuvenation of Face, Neck, Décolletage and Hands: A Case Series Report
Massidda E
Clinical, Cosmetic and Investigational Dermatology 2023, 16:3427-3439
Published Date: 29 November 2023