Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Buttocks Beautification 3D with Calcium Hydroxylapatite (RadiesseTM): An Individualized Approach to Diagnosing and Treating Contour, Sagging, and Cellulite of the Buttocks in Seven Cases
Authors Teodoro MDS, Di Sessa D ![]() , Barros JHDFA, Vasconcelos RCFD
, Barros JHDFA, Vasconcelos RCFD ![]() , Miot HA
, Miot HA ![]()
Received 19 July 2023
Accepted for publication 28 September 2023
Published 24 October 2023 Volume 2023:16 Pages 3039—3051
DOI https://doi.org/10.2147/CCID.S431391
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Matheus dos Santos Teodoro,1 David Di Sessa,2 João Henrique da Fonseca Armada Barros,1 Rossana Cantanhede Farias de Vasconcelos,3 Hélio Amante Miot4
1Instituto Corpo e Pele, Belo Horizonte, MG, Brazil; 2Clinica David Di Sessa, São Paulo, SP, Brazil; 3Clinica Nomina, São Paulo, SP, Brazil; 4Departamento de Dermatologia da FMB-Unesp, Botucatu, SP, Brazil
Correspondence: Hélio Amante Miot, Departamento de Dermatologia da FMB-Unesp Rua Magnólia, 400, Jd. Bom Pastor, Botucatu, SP, 18.607-670, Brazil, Tel +55 14 38134727, Email [email protected]
Background: The demand for body procedures is increasing, and buttocks beautification is one of the most sought-after procedures in dermatological and plastic surgery clinics. Several aspects affect the beauty of this area, including sagging, cellulite, contour irregularity, and volume reduction. This makes treatment of the area more challenging. Calcium hydroxylapatite (CaHA), which may be injected into the buttocks, stimulates local neocollagenesis, provides volume replacement, increases the strength and elasticity of the dermis, and thickens the underlying superficial fascia. However, no protocol for buttocks beautification tailors the dilution and deep application of CaHA filler simultaneously according to clinical assessments and personal priorities regarding contour, sagging, and cellulite.
Purpose: To report the results of a minimally invasive protocol using different dilutions of CaHA (Buttocks Beautification 3D) in the buttocks with application in different planes. The treatment was performed according to a previous individualized evaluation to improve the area aesthetically.
Patients and methods: Six women and one man were submitted to the protocol. An assessment was performed to determine the shape, sagging, cellulite (in women), and patients’ preferences for buttocks beautification. The dilution, volume, depth, and injection technique for CaHA were based on these assessments. The results of the treatment were then assessed using standardized photographs and patient satisfaction.
Results: We reported favorable results in six women and one man with different grades of sagging, female cellulite, and shapes of the gluteal region who were treated with CaHA injections according to a tailored protocol. All participants reported high satisfaction with the procedure.
Conclusion: Highly satisfactory results were achieved in seven adult patients who were assessed and treated for the buttocks with CaHA using an individualized protocol. Prospective studies should be performed to corroborate our findings and optimize the use of Buttocks Beautification 3D as a reliable modality of treatment for this body area.
Keywords: Rejuvenation, biostimulatory treatment, neocollagenesis, calcium hydroxylapatite
Introduction
The demand for aesthetic body procedures is increasing, especially in emerging markets such as Brazil, India, China, and Mexico. In 2020, even during the COVID-pandemic, more than a million procedures were performed, generating more than US$3 billion. Several factors are responsible for this phenomenon, including the availability of noninvasive and minimally invasive aesthetic procedures, the rising prevalence of obesity worldwide, and increasing public awareness of cosmetic procedures.1–3
The archetype of gluteal beauty is complex, has varied throughout history, and may differ depending on ethnicity and gender.4,5 Many factors influence gluteal attractiveness, including the level of curvaceousness, which may be influenced by the buttocks’ size, shape, and roundness.4,6 The paleolithic sculpture Venus of Willendorf (25,000–30,000 BC) reinforces the early representation of fertility as a curved silhouette in which the breasts and hips mainly contribute to the shape.7 Furthermore, the buttocks are included in society’s idealization of the perfect body. Therefore, there is an increasing interest in body contour improvement,8 and the treatment of the gluteal area is one of the most sought-after procedures in dermatological and plastic surgery clinics in Brazil.
Currently, people interested in improving the aesthetic aspects of the buttocks are seeking less-invasive, painless procedures with quick recovery and lower risks of procedure-related complications.9,10
Evaluation of the buttocks can reveal several combined aspects that cause integral management of buttocks beautification to be challenging.11 These include sagging, female cellulite, contour irregularity, and volume reduction, among others. Additionally, the complex pathogenesis of the female cellulite is characterized by alterations of the hypodermis associated with lymphatic stasis, the early fibrous changes make the treatment of the gluteal area even more complicated.12
RadiesseTM (Merz North America, Raleigh, N.C.) is a biocompatible, biodegradable, and resorbable biostimulatory calcium hydroxylapatite (CaHA) filler. Microspheres within the compound stimulate the local production of collagen, providing volume replacement.13,14 The filler can be diluted for injection on the face or in other body areas, such as the arms, abdomen, or buttocks, to increase the strength and elasticity of the dermis.10,15,16
In 2019, Kim J. described the multilayered injection technique (dermis, subdermis using dermal scraping technique, and fat layer) of CaHA filler on ischial soft tissue to rejuvenate the previous phase of chronic sitting pressure sore. Subdermal filler injection improved by volumization the depressed soft tissue, while intradermal micro-droplet injections of CaHA filler leaded to a better skin quality (which may be influenced by neocollagenesis by numerous fibroblasts and increased neovascularization).17 To date, no protocol for buttocks beautification has been established that tailors the dilution and the deep of application of CaHA filler, simultaneously, according to clinical assessment of and personal preferences regarding contour, sagging, and cellulite.
Therefore, this manuscript aims to report a therapeutic, minimally invasive protocol using different dilutions of CaHA in the buttocks (Buttocks Beautification 3D) with application in different planes according to previous individualized evaluations. The goal of the procedure was to improve the area aesthetically.
Patients and Methods
Seven adult patients (six women and one man) who desired to improve the appearance of their buttocks were submitted to the protocol (Buttocks Beautification 3D). They were photographed before the treatment (D0) and after 90, 150 or 180 days (D90, D150 and D180) to subside the assessment method and the effectiveness of the procedure. All participants gave written consent for image and data publication prior to study commencement.
Patient satisfaction was determined by asking each participant to rate the results using a ten-point scale ranging from completely unsatisfied to completely satisfied. The protocol was divided into three different phases, as described below.
PHASE 1: Assessment
In phase 1, a global evaluation of the buttocks was performed. The following criteria were evaluated: shape, sagging, and cellulite (in women). The shape of the buttocks was classified as an A-shape (characterized by greater amounts of fat in the lateral upper thigh and less fat in the lateral upper hip), a V-shape (in which most of the fat was located in the upper lateral hip area, with very little fat located at the lateral upper thigh), a short square shape (height and width in a 1:1 ratio), or a round shape (characterized by an excess of fat in the middle of the buttocks).18
Sagging was classified into five types: no skin laxity, mild skin laxity, moderate skin laxity, severe skin laxity, and very severe skin laxity. The evaluation was completed using photographs taken at a standardized angle of light and standardized distance between the light and the camera.19
Finally, cellulitis was divided into four grades: no cellulite; cellulite visible upon movement or compression; visible cellulite at rest; or cellulitis with more nodules, elevations, and discomfort.20–22
PHASE 2: Bespoke Evaluation
In phrase 2, the patients’ complaints were prioritized according to the clinical diagnoses and classification (eg, roundness, cellulite, sagging). This combined evaluation helped identify the aspect of priority for the treatment and subsequently determined how much of the filler was used for each treatment.
PHASE 3: Customized Demarcation and Dilution
Each buttock was divided into four quadrants, and each quadrant was demarcated individually as determined by the assessment (phases 1 and 2). The standardized dilutions and planes of injections are presented in Table 1.23–25
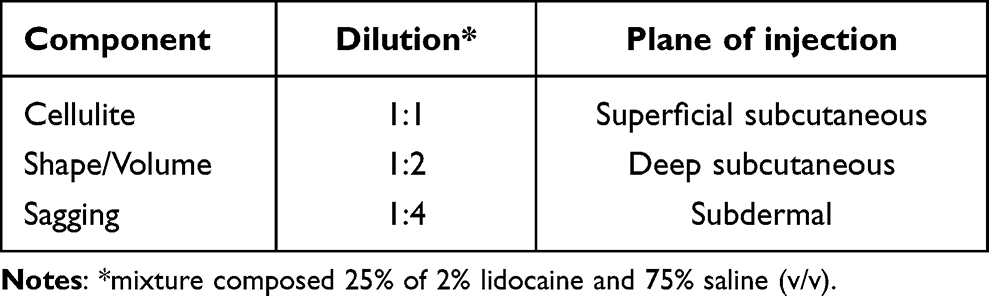 |
Table 1 Standardized Dilutions of CaHA (RadiesseTM) for Each Evaluated Criterion |
The different dilutions aim to act on different layers, enhancing results in the context of multilayered injection and the neocollagenesis stimuli.
For a 1:4 dilution, the dispersion of CaHA particles is diffuse and homogeneous in the subdermal layer, aiming to improve skin quality. We introduce the cannula at a 10 to 15-degree angle.
In a 1:2 dilution, a higher concentration of particles in the connective tissue and fascia is proposed. Therefore, the cannula is introduced at a 30 to 45-degree angle to target deeper tissues, leading to more effective focal neocollagenesis, structuring septa in the area, and potentially interacting with adipocytes, resulting in a lifting effect (septa) and volumetric increase (adipocytes).
The 1:1 dilution aims to treat the hypodermis and its septa. The CaHA particles are diluted but more concentrated than in other dilutions, with the additional goal of addressing cellulite. For this dilution, we introduce the cannula at a 15 to 30-degree angle.
For the injections, calcium hydroxylapatite (RadiesseTM, Merz North America, Raleigh, NC, USA) was diluted 1:1 with 1.5 mL of a mixture composed 25% of 2% lidocaine (XylestesinTM, Cristália, Itapira, SP, Brazil) and 75% saline (v/v); 1:2 with 3 mL of this mixture; or 1:4 with 6 mL of this mixture. The procedures were performed under sterile conditions. In the areas with cellulite, the solution was injected with a 22G cannula in a fan-like movement, complemented by direct injection of the solution with a 27G needle in each depression. To define the shape or treat sagging, the solution was injected with a cannula at different depths and dilutions (Table 1).
All patients were instructed to avoid physical exercise and perform active circular massage twice a day for the seven days following the procedure.
Results
The application strategies, demographic data, assessment details, and before and after images of the participants are presented in Figures 1–14. All participants expressed high satisfaction with the results and declared a desire to undergo the procedure again.
 |
Figure 1 Case 1, Buttocks Beautification 3D. Schematic representation of the injections (above). Standardized posterior images pre and 90 days post injection (below). Each syringe = 1.5 mL of CaHA. |
 |
Figure 2 Case 1, Buttocks Beautification 3D. Standardized oblique images pre and 90 days post injection. |
 |
Figure 3 Case 2, Buttocks Beautification 3D. Schematic representation of the injections (above). Standardized posterior images pre and 150 days post injection (below). Each syringe = 1.5 mL of CaHA. |
 |
Figure 4 Case 2, Buttocks Beautification 3D. Standardized oblique images pre and 150 days post injection. |
 |
Figure 5 Case 3, Buttocks Beautification 3D. Schematic representation of the injections (above). Standardized posterior images pre and 90 days post injection (below). Each syringe = 1.5 mL of CaHA. |
 |
Figure 6 Case 3, Buttocks Beautification 3D. Standardized oblique images pre and 90 days post injection. |
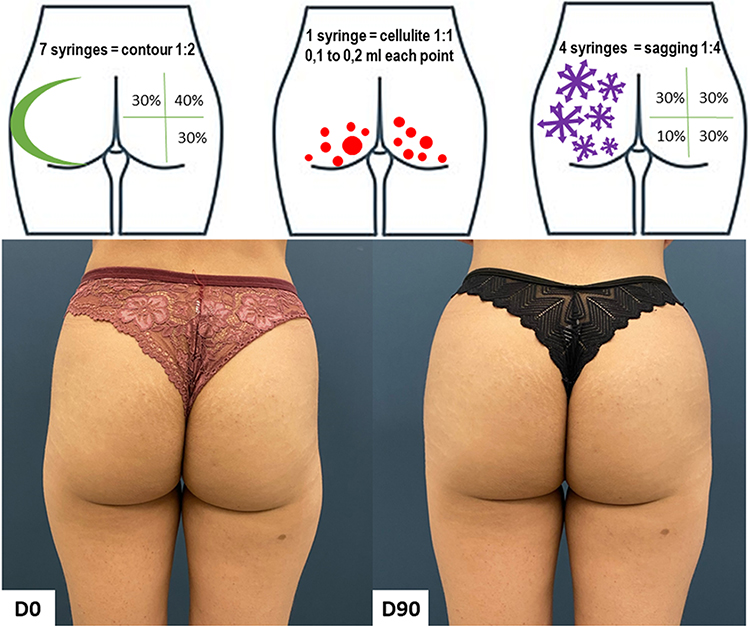 |
Figure 7 Case 4, Buttocks Beautification 3D. Schematic representation of the injections (above). Standardized posterior images pre and 90 days post injection (below). Each syringe = 1.5 mL of CaHA. |
 |
Figure 8 Case 4, Buttocks Beautification 3D. Standardized oblique images pre and 90 days post injection. |
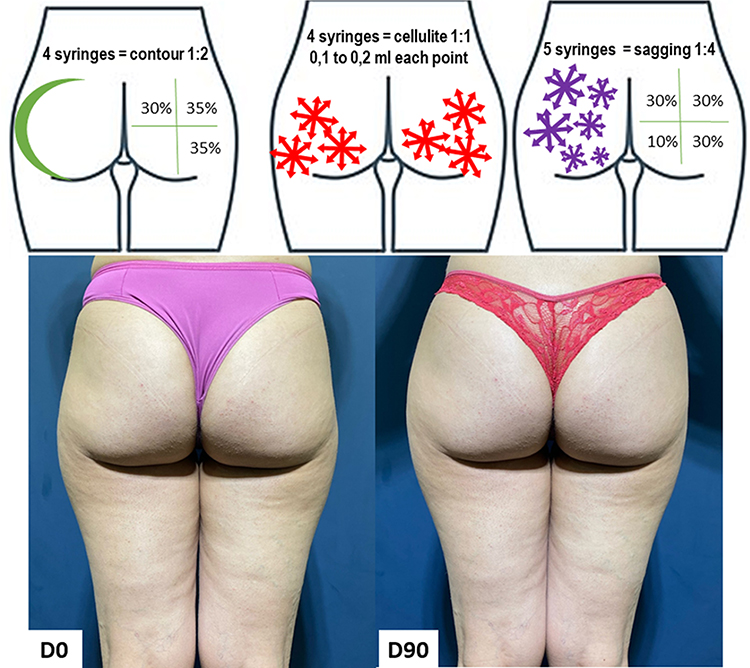 |
Figure 9 Case 5, Buttocks Beautification 3D. Schematic representation of the injections (above). Standardized posterior images pre and 90 days post injection (below). Each syringe = 1.5 mL of CaHA. |
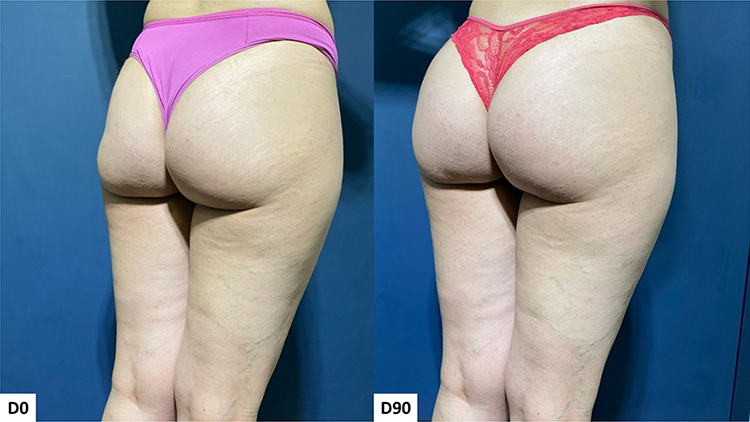 |
Figure 10 Case 5, Buttocks Beautification 3D. Standardized oblique images pre and 90 days post injection. |
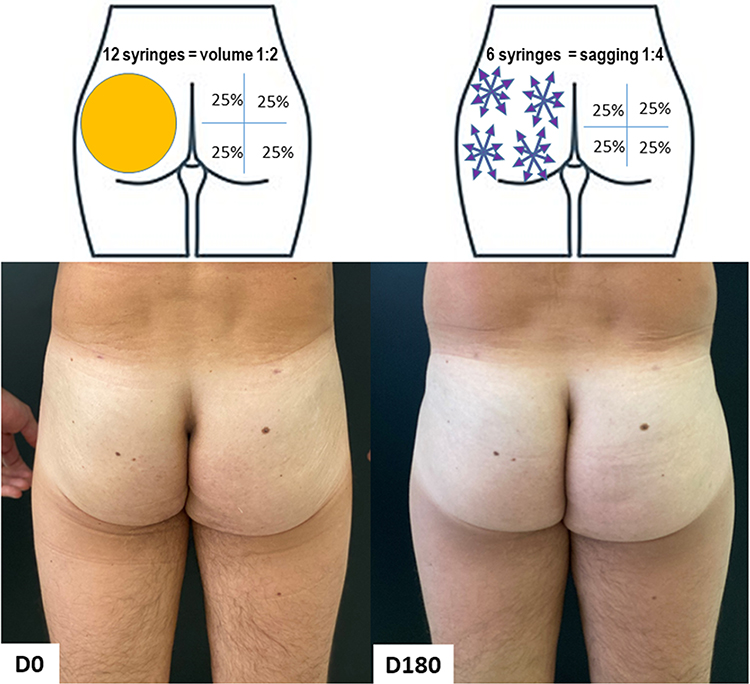 |
Figure 11 Case 6, Buttocks Beautification 3D. Schematic representation of the injections (above). Standardized posterior images pre and 180 days post injection (below). Each syringe = 1.5 mL of CaHA. |
 |
Figure 12 Case 6, Buttocks Beautification 3D. Standardized oblique images pre and 180 days post injection. |
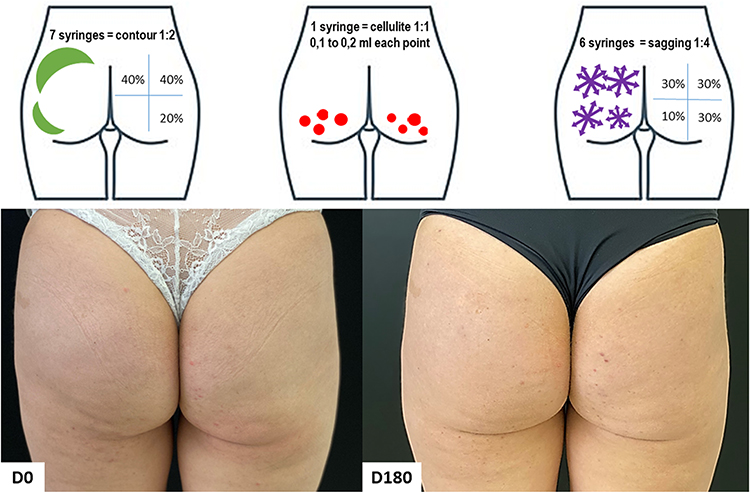 |
Figure 13 Case 7, Buttocks Beautification 3D. Schematic representation of the injections (above). Standardized posterior images pre and 180 days post injection (below). Each syringe = 1.5 mL of CaHA. |
 |
Figure 14 Case 7, Buttocks Beautification 3D. Standardized oblique images pre and 180 days post injection. |
No adverse events were reported after the procedure in any follow-up visit. The pain from the procedure was considered minimal, and the discomfort experienced during the first 72 h was manageable with rest and oral analgesics.
Case 1 was a 41-year-old eutrophic healthy woman who presented a square-shape buttocks. She was assessed as having grade 2 cellulite, moderate skin laxity, and a bespoke demand for improvement in laxity. Her treatment included 12 mL of CaHA (eight syringes). The results after 90 days and the scheme of application are presented in Figures 1 and 2. The patient expression satisfaction with the final results of the procedure as 7 out of 10.
Case 2 was a 38-year-old eutrophic healthy woman who presented with A-shaped buttocks. She was assessed as having grade 2 cellulite, moderate skin laxity, and a bespoke demand for improvement in laxity. Her treatment required 20 syringes of CaHA (30 mL). The results after 90 days and the application strategy are presented in Figures 3 and 4. The patient expression satisfaction with the final results of the procedure as 10 out of 10.
Case 3 was a 26-year-old eutrophic healthy woman who presented with round-shaped buttocks. She was assessed as having grade 1 cellulite, mild skin laxity, and a bespoke demand for improvement in contour. Her treatment required 10 syringes of CaHA (15 mL). The results after 90 days and the application strategy are presented in Figures 5 and 6. The patient expression satisfaction with the final results of the procedure as 8 out of 10.
Case 4 was a 23-year-old eutrophic healthy woman who presented with A-shaped buttocks. She was assessed as having grade 2 cellulite, mild skin laxity, and a bespoke demand for improvement in contour. Her treatment required 12 syringes of CaHA (18 mL). The results after 90 days and the application strategy are presented in Figures 7 and 8. The patient expressed satisfaction with the final results of the procedure as 8 out of 10.
Case 5 was a 44-year-old eutrophic healthy woman who presented with A-shaped buttocks. She was assessed as having grade 2 cellulite, moderate skin laxity, and a bespoke demand for improvement in laxity. Her treatment required 13 syringes of CaHA (19.5 mL). The results after 90 days and the application strategy are presented in Figures 9 and 10. The patient expressed satisfaction with the final results of the procedure as 10 out of 10.
Case 6 was a 42-year-old eutrophic healthy man who presented with square-shaped buttocks. He was assessed as having moderate skin laxity and a bespoke demand for improvement in laxity and contour. His treatment required 18 syringes of CaHA (27 mL), divided into three monthly sessions. The results after 180 days and the application strategy are presented in Figures 11 and 12. The patient expressed satisfaction with the final results of the procedure as 10 out of 10.
Case 7 was a 42-year-old eutrophic healthy woman who presented round-shaped buttocks. She was assessed as having grade 2 cellulite, moderate skin laxity, and a bespoke demand for improvement in asymmetry, cellulite, and contour. Her treatment required 14 syringes of CaHA (21 mL). The results after 90 days and the application strategy are presented in Figures 13 and 14. The patient expressed satisfaction with the final results of the procedure as 10 out of 10.
Discussion
The buttocks area has received increasing attention from the media, especially in Latin America. Consequently, patients’ demand for buttock reshaping and contouring, mostly through non-surgical procedures, has proportionally increased.10 Here, we presented a rational method for assessing and treating the area with CaHA.
Despite the lower risks and improved recovery compared to surgical procedures, the use of CaHA filler is complex considering the sites of injection, especially when the focus is the results.13 A protocol based on strategies that can be individualized for each patient facilitates the practical procedure and may help obtain better results and, consequently, improved patient satisfaction.
The fat tissue is organized into multiple layers, which begin from the surface and include the skin (epidermis and dermis), the superficial adipose or areolar tissue (SAT)/hypodermis, a fibrous horizontal layer of connective tissue (membranous layer or fascia superficialis), deep adipose or lamellar tissue (DAT), deep fascia, and the muscles.26–28 Understanding the organization is important because there is often confusion between the terms hypodermis and subcutaneous adipose tissue, which are mistakenly used interchangeably. However, these are two distinct and independent structures with separate metabolic responses, and knowing their behavior is crucial for selecting appropriate treatments.29
The SAT is essential for contour regularity, while the DAT plays an important role in volumizing the gluteal area. Histologically, the SAT is characterized by fibrous septa that connect the dermis with the fascia superficialis. These septa are composed of elastic and collagen fibers, defining oval-polygonal lobules of fat cells that form what Sbarbati called a peri-adipocyte collagen network. The compartments are well-vascularized by capillaries.28,29 The appearance of DAT (deep adipose tissue) differs from SAT. Its fat lobules are larger, flatter, and less defined, with less evident fibrous septa. In general, they are obliquely oriented and connected to the membranous layer of the deep fascia of the muscles.28 According to Sbarbati et al, the peri-adipocyte collagen network in this layer is described as incomplete, extremely fragile, and finely adherent. It has few vascular components, which apparently characterize it as an area of high lipid deposition.30
Cellulite is a complex issue to address, and it is a pathology specific to women due to the anatomical characteristics of the superficial adipose or areolar tissue (SAT)/hypodermis. In women, the fat lobules are larger and have parallel septa, while in men, the lobules are smaller and arranged in oblique planes.29 The pathogenesis of cellulite in women is characterized by alterations of the hypodermis associated with lymphatic stasis, as well as early edematofibrosclerotic panniculopathy and dermopaniculopathy. These factors make the treatment of the gluteal area even more complicated.10
Identifying the shape of the buttocks is a well-known, widely used strategy that facilitates surgical planning and designing the possible final results.18,20,21 However, the shape alone does not account for other important aspects necessary to a good final result, such as sagging and the presence of cellulite. Our method, based in the multilayered injection technique (dermis, subdermis using dermal scraping technique, and fat layer) of CaHA filler takes into consideration the main preoccupations of the patients, attempts to link all these aspects with the patient’s preferences.17 Consequently, improved clinical results and higher satisfaction are possible when the Buttocks Beautification 3D technique is used.
The authors treated more than one hundred patients using this technique for over five years, without severe adverse effects, which reinforces its safety. Nevertheless, this is a preliminary case series, and larger prospective studies using objective methods and reliable outcomes are needed to produce additional evidence supporting the procedure prior to global implementation of CaHA filling.31 However, the quality of the results was remarkable, and the straightforward evaluation and standardized procedure are strengths for the procedure’s use in aesthetic medicine clinics.
Complications associated with CaHA injections are infrequent, with the majority being temporary, such as localized pain, swelling, redness, and bruising. Vascular complications are unlikely in this region due to the plane of injection. Migration is not typically observed, as the diluted product is evenly distributed in the correct planes. While rare, erythematous nodules and granulomas have been reported with superficial CaHA injections, particularly in dynamic areas like the face and neck.13,32–34
This report has limitations, including a small sample size that limits the statistical validity of the results. Furthermore, objective measurements such as magnetic resonance or ultrasonography were not employed and are warranted in further studies. Lastly, the use of a high number of CaHA vials in this technique leads to a substantial procedural cost and an elevated risk of injection-related complications.35
Conclusion
High satisfactory results were achieved on seven adult patients who were assessed and submitted to an individualized protocol for treating the buttocks with CaHA. Further prospective studies should corroborate our findings and optimize the use of Buttocks Beautification 3D as a reliable modality of treatment for this body area.
Ethical Statement
This manuscript was approved by the institution’s (Unesp Medical School) review board (CAAE: 64331022.1.0000.5411).
Informed-Consent Statement
Written informed consent was obtained from patients to publish their data in this paper.
Acknowledgments
To the patients who are allowed to publish their anonymized photos.
Disclosure
Dr. Matheus Teodoro, Dr. David Di Sessa, and Dr. Rossana Vasconcelos are medical speakers for Merz. Dr. Helio Miot is a medical consultant for Merz, AbbVie, Galderma, and L’Oréal. The authors report no other conflicts of interest in this work.
References
1. Hotta TA. Consumer demand for medical aesthetics creating business opportunities. Plast Surg Nurs. 2018;38(3):83. In eng. doi:10.1097/PSN.0000000000000235
2. Phillips TL. Diverse perspectives in medical aesthetics matter more than ever. Dermatol Times. 2022;43(4):10.
3. Wang JV, Akintilo L, Geronemus RG. Growth of cosmetic procedures in millennials: a 4.5-year clinical review. J Cosmet Dermatol. 2020;19(12):3210–3212. doi:10.1111/jocd.13768
4. Lee EI, Roberts TL, Bruner TW. Ethnic considerations in buttock aesthetics. Semin Plast Surg. 2009;23(3):232–243. doi:10.1055/s-0029-1224803
5. Roberts TL, Weinfeld AB, Bruner TW, Nguyen K. ”Universal” and ethnic ideals of beautiful buttocks are best obtained by autologous micro fat grafting and liposuction. Clin Plast Surg. 2006;33(3):371–394. doi:10.1016/j.cps.2006.05.001
6. Fisher ML, Voracek M. The shape of beauty: determinants of female physical attractiveness. J Cosmet Dermatol. 2006;5(2):190–194. In eng. doi:10.1111/j.1473-2165.2006.00249.x
7. Weber GW, Lukeneder A, Harzhauser M, et al. The microstructure and the origin of the Venus from Willendorf. Sci Rep. 2022;12(1):2926. In eng. doi:10.1038/s41598-022-06799-z
8. Tijerina JD, Morrison SD, Nolan IT, Vail DG, Lee GK, Nazerali R. Analysis and interpretation of google trends data on public interest in cosmetic body procedures. Aesthet Surg J. 2020;40(1):NP34–NP43. doi:10.1093/asj/sjz051
9. Nteli Chatzioglou G, Govsa F, Bicer A, Ozer MA, Pinar Y. Physical attractiveness: analysis of buttocks patterns for planning body contouring treatment. Surg Radiol Anat. 2019;41(1):133–140. In eng. doi:10.1007/s00276-018-2083-4
10. Silveira I, Martinez B. Bilateral gluteal augmentation with hyperdilute calcium hydroxylapatite microspheres performed using the Bella Vida Instant Brazilian Butt Lift (BBL). Cureus. 2022;14(6):e26261. doi:10.7759/cureus.26261
11. Cuenca-Guerra R, Quezada J. What makes buttocks beautiful? A review and classification of the determinants of gluteal beauty and the surgical techniques to achieve them. Aesthetic Plast Surg. 2004;28(5):340–347. In eng. doi:10.1007/s00266-004-3114-6
12. Cunha M, Cunha A, Machado CA. Physiophatology of gynoid lipodystrophy. Surg Cosmet Dermatology. 2015;7:98–103.
13. Kadouch JA. Calcium hydroxylapatite: a review on safety and complications. J Cosmet Dermatol. 2017;16(2):152–161. In eng. doi:10.1111/jocd.12326
14. Nowag B, Casabona G, Kippenberger S, Zoller N, Hengl T. Calcium hydroxylapatite microspheres activate fibroblasts through direct contact to stimulate neocollagenesis. J Cosmet Dermatol. 2023;22(2):426–432. doi:10.1111/jocd.15521
15. Casabona G, Pereira G. Microfocused ultrasound with visualization and calcium hydroxylapatite for improving skin laxity and cellulite appearance. Plast Reconstr Surg Glob Open. 2017;5(7):e1388. In eng. doi:10.1097/GOX.0000000000001388
16. Figueredo VO, Miot HA, Soares Dias J, Nunes GJB, Barros de Souza M, Bagatin E. Efficacy and safety of 2 injection techniques for hand biostimulatory treatment with diluted calcium hydroxylapatite. Dermatol Surg. 2020;46(Suppl 1):S54–S61. doi:10.1097/DSS.0000000000002334
17. Kim J. Multilayered injection of calcium hydroxylapatite filler on ischial soft tissue to rejuvenate the previous phase of chronic sitting pressure sore. Clin Cosmet Investig Dermatol. 2019;12:771–784. doi:10.2147/CCID.S212599
18. Mendieta CG, Sood A. Classification system for gluteal evaluation: revisited. Clin Plast Surg. 2018;45(2):159–177. In eng. doi:10.1016/j.cps.2017.12.013
19. Kaminer MS, Casabona G, Peeters W, et al. Validated assessment scales for skin laxity on the posterior thighs, buttocks, anterior thighs, and knees in female patients. Dermatol Surg. 2019;45(Suppl 1):S12–S21. In eng. doi:10.1097/DSS.0000000000001994
20. Davis DS, Boen M, Fabi SG. Cellulite: patient selection and combination treatments for optimal results a review and our experience. Dermatol Surg. 2019;45(9):1171–1184. In eng. doi:10.1097/DSS.0000000000001776
21. Rossi AB, Vergnanini AL. Cellulite: a review. J Eur Acad Dermatol Venereol. 2000;14(4):251–262. In eng. doi:10.1046/j.1468-3083.2000.00016.x
22. Hexsel DM, Dal’forno T, Hexsel CL. A validated photonumeric cellulite severity scale. J Eur Acad Dermatol Venereol. 2009;23(5):523–528. doi:10.1111/j.1468-3083.2009.03101.x
23. Goldie K, Peeters W, Alghoul M, et al. Global consensus guidelines for the injection of diluted and hyperdiluted calcium hydroxylapatite for skin tightening. Dermatol Surg. 2018;44(Suppl 1):S32–S41. In eng. doi:10.1097/DSS.0000000000001685
24. de Almeida AT, Figueredo V, da Cunha ALG, et al. Consensus recommendations for the use of hyperdiluted calcium hydroxyapatite (Radiesse) as a face and body biostimulatory agent. Plast Reconstr Surg Glob Open. 2019;7(3):e2160. In eng. doi:10.1097/GOX.0000000000002160
25. Whipple LA, Fournier CT, Heiman AJ, et al. The anatomical basis of cellulite dimple formation: an ultrasound-based examination. Plast Reconstr Surg. 2021;148(3):375e–381e. In eng. doi:10.1097/PRS.0000000000008218
26. Gasperoni C, Salgarello M. Rationale of subdermal superficial liposuction related to the anatomy of subcutaneous fat and the superficial fascial system. Aesthetic Plast Surg. 1995;19(1):13–20. doi:10.1007/BF00209305
27. Lockwood TE. Superficial fascial system (SFS) of the trunk and extremities: a new concept. Plast Reconstr Surg. 1991;87(6):1009–1018. doi:10.1097/00006534-199106000-00001
28. Lancerotto L, Stecco C, Macchi V, Porzionato A, Stecco A, De Caro R. Layers of the abdominal wall: anatomical investigation of subcutaneous tissue and superficial fascia. Surg Radiol Anat. 2011;33(10):835–842. doi:10.1007/s00276-010-0772-8
29. da Cunha MG, da Cunha ALG, Machado CA. Hypodermis and subcutaneous adipose tissue-two different structures. Surg Cosmet Dermatol. 2014;6(4):355–359.
30. Sbarbati A, Accorsi D, Benati D, et al. Subcutaneous adipose tissue classification. Eur J Histochem. 2010;54(4):e48. doi:10.4081/ejh.2010.e48
31. Bagatin E, Miot HA. How to design and write a clinical research protocol in Cosmetic Dermatology. An Bras Dermatol. 2013;88(1):69–75. doi:10.1590/s0365-05962013000100008
32. Zhu V, Cole EL. Ossification and migration of a nodule following calcium hydroxylapatite injection. Cutis. 2022;110(4):E2–E3. doi:10.12788/cutis.0635
33. Trinh LN, McGuigan KC, Gupta A. Delayed complications following dermal filler for tear trough augmentation: a systematic review. Facial Plast Surg. 2022;38(3):250–259. doi:10.1055/s-0041-1736390
34. Nipshagen MD, Velthuis PJ, Cook E, Mosmuller DGM. Non-inflammatory nodule formation after hyperdiluted calcium hydroxyapatite treatment in the neck area. Dermatol Ther. 2020;33(6):e14272. doi:10.1111/dth.14272
35. Ianhez M, Souza MB, Miot HA. Frequency of complications of aesthetic facial fillers in Brazil. Plast Reconstr Surg. 2022;149(3):599e–601e. doi:10.1097/PRS.0000000000008839
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Contouring Plus: A Comprehensive Approach of the Lower Third of the Face with Calcium Hydroxylapatite and Hyaluronic Acid

Viscomi B, Faria G, Hernandez CA, Perez L, Spada J, De la Fuente V, Muniz M
Clinical, Cosmetic and Investigational Dermatology 2023, 16:911-924
Published Date: 5 April 2023
Efficacy and Tolerability of Hyperdiluted Calcium Hydroxylapatite (Radiesse) for Neck Rejuvenation: Clinical and Ultrasonographic Assessment
Trindade de Almeida AR, Marques ERMC, Contin LA, Trindade de Almeida C, Muniz M
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1341-1349
Published Date: 25 May 2023