Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Applying the MD Codes™ to Treat Emotional and Social Attributes with HA Fillers: A Retrospective Serial Case Study
Authors de Maio M, Brenninkmeijer EEA, Nurlin I, Colucci L, Sanchez T
Received 18 August 2023
Accepted for publication 1 November 2023
Published 29 November 2023 Volume 2023:16 Pages 3441—3453
DOI https://doi.org/10.2147/CCID.S430747
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Mauricio de Maio,1 Elian Elisabeth Anne Brenninkmeijer,2 Iman Nurlin,3 Ligia Colucci,4 Tania Sanchez5
1MD Codes Institute, Sao Paulo, SP, Brazil; 2Brenninkmeijer Aesthetic Dermatology, Amsterdam, the Netherlands; 3Ribelle Clinic, Örebro, Sweden; 4Clinica Colucci, Belo Horizonte, MG, Brazil; 5Instituto Dermatológico de Jalisco, Zapopan, Jalisco, Mexico
Correspondence: Mauricio de Maio, MD Codes Institute, Avenida Brigadeiro Faria Lima, 4509 - cjs 121, Vila Olímpia, Sao Paulo, SP, Brazil, Tel +55 11 5535-9286, Fax +55 11 5531-4720, Email [email protected]
Background: Aesthetic treatment directed at improving facial emotional messages and social attributes may maximize patient satisfaction with treatment results. The MD Codes™ is an approach to facial aesthetic treatment that accounts for emotional messages and social attributes while minimizing variability in patient assessment, injection technique, injection sites, and treatment outcomes.
Objective: To assess the impact of the MD Codes systematic treatment approach on emotional and social attributes and natural appearance after facial aesthetic treatment with hyaluronic acid (HA) fillers.
Methods: A retrospective analysis was performed in patients treated with 12 mL of HA fillers (Juvéderm® Vycross™ products) per patient using the MD Codes. Study injectors, experienced clinician observers, clinical staff, laypeople, and patients evaluated impact of treatment on emotional and social attributes and natural appearance based on pre- and post-treatment photographs of patients.
Results: Twelve patients and 49 external observers, from 12 countries, evaluated the images. More than 90% of patients named “eye bags” as the facial area most in need of aesthetic treatment; > 55% of external observers identified “cheeks.” The top 3 facial emotional attributes noted by all evaluators after treatment were, in order, “less tired”, “less saggy”, and “younger.” All patients reported a visible and positive change in emotional attributes except for “less sad.” After 9 months, most patients reported looking “less tired” (n=11/12), “less saggy” (n=8/12), and “less sad” (n=6/12). At months 6 and 9, all patients rated their appearance as natural looking. At least 90% of external observers considered the frontal view results natural for all but 1 patient. Patients reported improved positive social attributes (eg, “looking friendlier”) and improvements in well-being after treatment. No serious side effects were reported.
Conclusion: Implementing the MD Codes for facial aesthetic treatment may improve facial emotional attributes as well as enhance social attributes and well-being, with natural-looking results.
Keywords: aesthetics, dermal fillers, hyaluronic acid, rejuvenation, skin aging, skin wrinkling
Introduction
An individual’s emotional state may be misinterpreted when wrinkles, age-related structural changes, and other deficiencies, such as congenital volume deficits, impact facial expressions in an unfavorable way.1–3 People may be perceived as older, less attractive, and less healthy, or encounter a variety of other negative impressions, simply by having a nonneutral facial expression.4–6 For example, lines ingrained between the brows may be mistaken for anger, and sagging at the corners of the mouth may imply sadness.7–9 Individuals may be perceived as younger when their face looks happy instead of fearful, angry, or sad.10 Judgments based on facial appearance occur very rapidly, within milliseconds,11 and individuals may suffer social prejudices, impaired self-esteem, and psychological distress as a result of facial emotional miscues.2,6 The synergy between physical and mental wellness creates a strong sense of self-assurance, which, in turn, affects how individuals perceive themselves in social situations. A healthy appearance not only boosts their self-esteem but also enhances their social interactions.12
Patients seeking aesthetic treatment often present with vague cosmetic complaints such as “I look tired” or “I would like to look younger” and may request facial volume restoration.1,13 Correcting unwanted facial emotional messages, such as looking tired, angry, or sad, is a frequent objective of treatment,7,8 and requires restoration of the integrity and balance of facial bone, muscle, fat, and skin, which undergo displacement and deterioration with aging.3,14 Volume, definition, and contour in the face are associated with looking younger and more attractive.3,15 Patient satisfaction has been shown to increase when aesthetic treatment is directed at improving facial emotional messages rather than targeting specific, isolated facial regions.1,6–8,16
The MD Codes™ is an approach to facial aesthetic treatment that takes facial emotional attributes into account and was developed to minimize variability in patient assessment, injection technique, injection sites, and treatment outcomes.8 This approach considers 4 unfavorable attributes that faces might express (looking tired, looking sad, having a saggy appearance, and having an angry look) as well as 4 positive attributes (looking attractive, looking younger, looking more contoured, and having either a more feminine or a more masculine appearance).8 It provides a systematic approach to nonsurgical facial rejuvenation with injections of hyaluronic acid (HA) filler deep into areas for structural support, more superficially into fat tissue for contouring, and superficially or intradermally for refinement.8,16 The MD Codes uses anatomical unit codes (abbreviations for regions of the face with numbers representing subunits of these regions) and active numbers (recommended injection volumes, representing minimum volumes needed for visible, reproducible results).8
Although best practices for aesthetic treatments are clear that initial consultation should include full medical history, physical examination, patient expectation intake, systematic patient photography, and complication prevention measures,17,18 reports accounting for emotional attributes, as well as social attributes, are limited. This paper describes the implementation of MD Codes in clinical practice in the context of considering the emotional and social attributes of the face at the initial consultation and assessing the natural look of treatment results. The objective was not only to perform facial rejuvenation, but to improve patients’ self-perception and reception by others. As the fascination with cosmetic procedures continues to grow, it prompts us to explore their multifaceted effects, particularly in domains beyond the obvious physical transformations. HA fillers may influence the psychological and social dimensions of an individual’s well-being.19
Materials and Methods
Study Design
This retrospective analysis examined data from a group of 12 adult female patients from the Netherlands from their medical records who received aesthetic treatment from 12 expert clinicians (1 clinician per patient) as part of an MD Codes training and mentoring event in Amsterdam on February 10, 2019. The clinicians were dermatologists, plastic surgeons, and aesthetic physicians from Brazil, France, Greece, India, Malaysia, Mexico, Netherlands, New Zealand, Sweden, Taiwan, United Arab Emirates, and United Kingdom (1 clinician per country/territory).20 The first author and the clinician assessed each patient, and all parties agreed on a treatment plan.20 This study did not require ethics committee approval because it is a retrospective analysis of an educational activity that was performed for training purposes only.
Patients and Initial Consultation
The first author led the training event and selected patients based on their appropriateness for the training.20 To be included in the event, patients needed to have the following facial signs: temple volume loss, eyebags or tear trough defects, volume loss/saggy cheeks, dynamic nasolabial folds, deflated/thin lips, and recessed chin, jowls, submental excess skin, and/or chin wrinkling. Facial signs (none, mild, moderate, or severe) were graded based on clinical experience, and patients selected for the study had facial signs that ranged from mild to severe.20 Each patient’s medical history was obtained. Patients with HA filler or botulinum toxin type A (BoNT/A) injections during the previous 6 months and/or prior permanent filler treatment were excluded.
Patients’ faces were photographed using 2-dimensional photography from the frontal, left and right oblique, and left and right profile views, and at rest, smiling, kissing, and pouting. The lead author consulted with patients to confirm they were eligible for the training session. During this initial consultation, the patients referred to their photographs and their own mirror reflections and selected the top 3 anatomical regions of the face that they wanted to improve or correct, as well as the top 3 of 8 emotional attributes to improve with treatment (Table 1), as defined by the Multi-Dimensional Aesthetic Scan Assessment (MD ASA™), a tool developed by the lead author to help clinicians with patient assessment and treatment planning.20 Patients were given information about the procedure, risks, and potential side effects. All patients provided written informed consent for treatment and use of their photographs.20
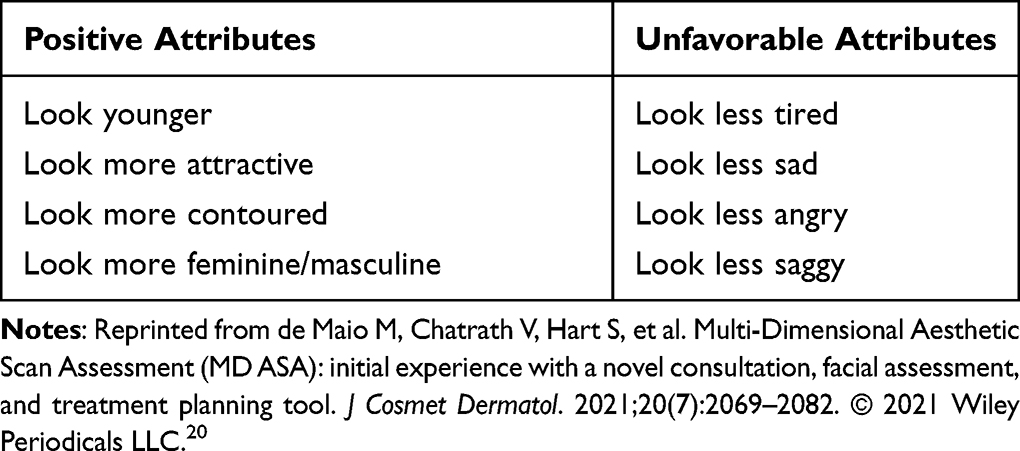 |
Table 1 Facial Emotional Attributes to Be Improved with treatment |
Treatment
Treatment was performed in a single session during the training event. However, in clinical practice, treatments may be divided into multiple sessions, and the use of 4 mL of injectable product per session is usually suggested. All clinicians followed the same MD Codes treatment plan using the respective codes, active numbers, and injection devices shown in Table 2.8,20 All treatments used the Vycross™ range of HA fillers: Juvéderm Voluma® (VYC-20L; 20 mg/mL); Volift® (VYC-17.5L; 17.5 mg/mL), and Volbella® (VYC-15L; 15 mg/mL; Allergan Aesthetics, an AbbVie Company, Irvine, CA).20–22 BoNT/A was not used. All patients received 12 mL of HA filler for both sides of the face, except for 1 patient who received 13 mL. Depending on nasolabial fold (NLF) severity, the number of syringes for NLFs varied from 1 mL distributed in NL1 (upper nasolabial fold) and NL2 (central nasolabial fold) for mild/moderate NLFs when smiling to 2 mL (1 mL per side) in NL1, NL2, and NL3 for severe NLFs.
 |
Table 2 Treatment Plan |
Assessments
Assessments occurred immediately after treatment and at 6 and 9 months after treatment. Immediately after injection, patients were photographed from the same facial views captured before treatment. Patients referred to their photographs and identified which emotional attributes had been improved.20 The 12 clinicians also referred to the photographs and rated the top 3 facial areas of each patient needing improvement (pretreatment), the top 3 emotional attributes to improve (pretreatment), and the impact of treatment on all 8 emotional attributes. The clinicians also ranked the 3 most impactful changes from the pretreatment images for all views. The 12 clinicians then independently recruited 3 groups of external observers (experienced clinicians, clinic staff, and laypeople) to make the same assessments as the clinicians based on the photographs. The external observers were selected as follows: (1) 12 clinicians who had at least 5 years of experience in facial aesthetics and injectable treatments, demonstrated skill in assessing results after injectable treatments, and did not inject any patients from the study; (2) 12 non-injector aesthetic clinic staff members, including skin therapists, beauticians, and assisting nurses, with professional experience within facial aesthetics and skin care; and (3) 12 laypeople without any professional experience in facial aesthetics or skin care.20 Like the injecting clinicians, the observers were a diverse international group from Brazil, France, Greece, India, Malaysia, Mexico, Netherlands, New Zealand, Sweden, Taiwan, United Arab Emirates, and United Kingdom. None of the external observers were affiliated with a pharmaceutical company or filler manufacturer.
Patients and observers also evaluated whether the treatment results appeared natural in frontal and oblique views. Results were classified as exceptionally natural, very natural, natural, unaltered, unnatural, or worsened. Patients also completed a questionnaire at 6 and 9 months after treatment to evaluate the results and impact of the treatment. Specifically, patients were asked what changes in the 8 emotional attributes and in 8 social attributes (ie, looking more trustworthy, confident, resilient, friendly, caring, energetic, knowledgeable, or optimistic; Table 3) they observed immediately after treatment and at 6 and 9 months; whether the results were natural immediately after treatment and at 6 and 9 months; and whether they noticed an improvement in overall results at 6 and 9 months.
 |
Table 3 Social Attributes to Be Improved with Treatment |
Safety
Side effects were recorded immediately after treatment and at 6 and 9 months. Follow-up lasted for up to 2 years for spontaneous reporting of any adverse event. Before injection, patients received 1 mL of 4 mg/mL dexamethasone intramuscularly to help reduce the rate of post-procedural injection site reactions, such as swelling.8,23 To minimize discomfort, lidocaine cream was applied to the facial areas to be injected 30 minutes before treatment. Proper antisepsis was carried out before and during the procedure.
Statistical Analysis
The results were analyzed to compare the impact of treatment on emotional and social attributes and natural results for each patient and between patients using descriptive statistics, including medians and percentages.
Results
Study Population
The 12 female patients, all Caucasian, had a mean age of 48.7 ± 6.3 years (range, 42–55 years).20 The 12 clinicians who treated the patients had a mean 13.2 ± 3.9 years of clinical aesthetic experience.20
Patient and Observer Assessments
All 12 patients completed the pre- and post-treatment self-assessments, and all 12 clinicians and all additional observers made assessments of all patients. All 12 patients selected the same attributes (saggy, tired, and sad) as the 3 unfavorable emotional attributes they wanted to improve with treatment from among the 8 MD ASA emotional attributes. Figure 1 shows the facial areas that the patients and observers identified as needing to be improved or corrected. Most (92%) of the patients named “eye bags”, whereas 56% of the observers identified “cheeks.” Across observers and patients, “less tired” was the top facial message to achieve for the frontal view of the face (Figure 2). This was also true for the oblique view; however, “less saggy” was the top facial message identified by observers and patients for the full-profile view.
 |
Figure 1 Facial areas patients need to improve or correct based on observer and patient evaluation of pretreatment patient photographs. For observers, the main area needing improvement was “cheek” (56%). Most patients (92%) named “eye bags” as the main area to improve. |
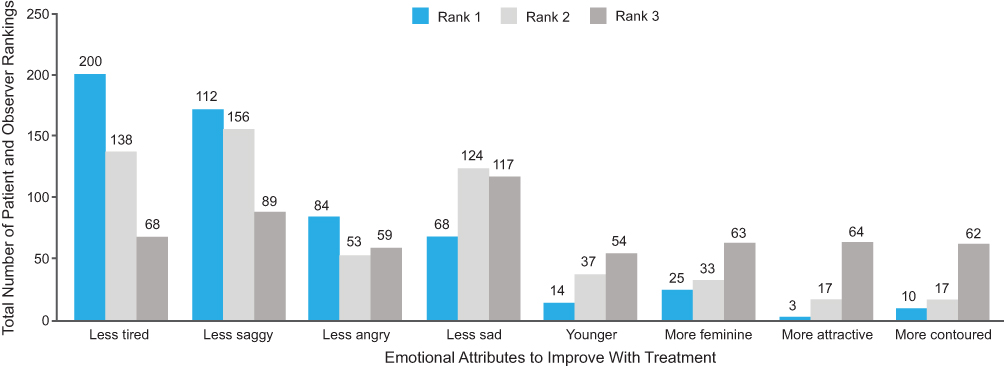 |
Figure 2 Emotional attributes to be achieved by treatment according to patients and observers. |
For all views, the top 3 emotional attributes achieved after treatment, according to both observer and patient assessments, were “less tired”, “less saggy”, and “younger.” Immediately after treatment, all patients reported a visible and positive change in emotional attributes (Figure 3), except for 5 of 12 patients, who disagreed with looking “less sad.” At 6 months after treatment, the patients also uniformly noticed an improvement in emotional attributes. After 9 months, the majority of patients still reported looking “less tired” (n=11/12), “less saggy” (n=8/12), and “less sad” (n=6/12). “Less tired” was the most changed attribute from the assessment of frontal views, followed by “more contoured” and “less sad”, and was also the most changed attribute in the oblique view, followed by “less sad” and “younger.” However, in the full-profile view, “less saggy” and “more contoured” were the top-rated changed attributes. In the full-profile view, 26% and 20% of the study injectors identified “more contoured” and “less sad”, respectively, as the second-most important facial attribute change in the patients’ appearance. “More contoured” was identified by 33% of patients as the third most significant emotional attribute changed, with “less saggy” being second.
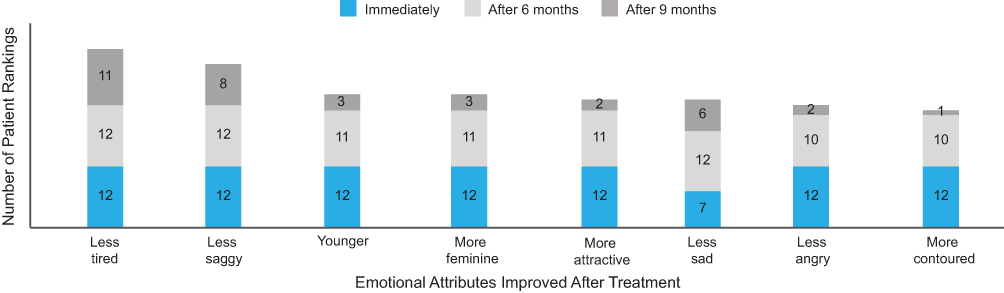 |
Figure 3 Changes in emotional attributes noticed by patients after treatment. |
All patients reported visual improvements in positive social attributes immediately after treatment (Figure 4). Except for the social attributes “more trustworthy”, “more caring”, and “more knowledgeable”, for which 1 patient per attribute did not report a change, most patients (n=8/12) reported a positive impact on their social attributes after 6 months. At 9 months, the majority of patients reported looking “friendlier” (n=10/12), “more energetic” (n=9/12), and “more optimistic” (n=7/12). The most highly ranked improvements in social attributes after 9 months were “more energetic”, “more optimistic”, and “friendlier.”
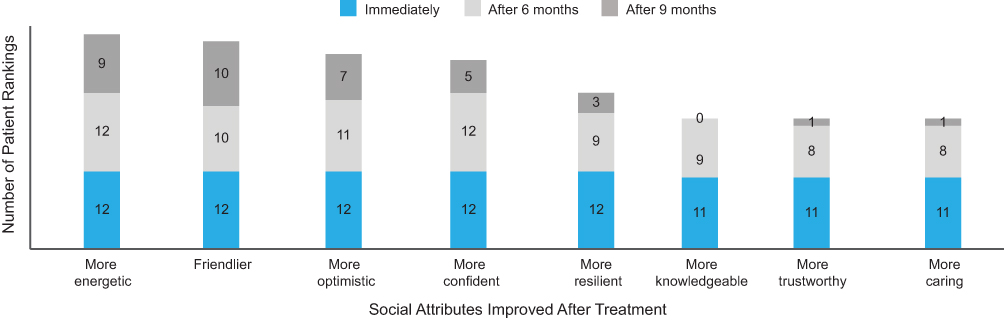 |
Figure 4 Changes in social attributes noticed by patients after treatment. |
Patients also had improved well-being, with most of them reporting feeling “better” (n= 5/12) or “much better” (n=6/12) at 6 months, whereas only 1 reported feeling “the same” after 6 months. At 9 months, the majority were still positive; 7 patients reported feeling “better” and 2 patients reported feeling “much better”, compared with 3/12 patients who reported feeling the same as before. No patients reported feeling worse about their appearance.
After months 6 and 9, all patients reported their individual results as natural looking. Among observers, >90% considered the outcome of treatment for the frontal view of 11 patients to be natural (ie, rated from “natural” to “exceptionally natural”). No “unaltered” and “unnatural” ratings were reported by study injectors and patients, but in the group of experienced clinician observers, there was 1 vote for “worsened”, as well as 2 “unaltered” and 2 “unnatural” votes. Results for naturalness of treatment were not substantially different among post-treatment patient photograph views; however, frontal and oblique views were more often evaluated as “exceptionally natural” and “very natural” when compared with the full-profile view, which was assessed more often as “unaltered.” Figures 5 and 6 show example before-and-after images.
 |
Figure 5 Full-face rejuvenation based on the MD Codes: a 49-year-old woman before (A–D) and immediately after (E–H) treatment. The woman presented with volume loss and sagging of the midface, bags and tiredness around the eyes, and a sagging and undefined jawline. Her primary concerns were jowls, bags around the eyes, and downturned oral commissures. The treatment plan for this patient was full-face rejuvenation with Juvéderm Voluma, Juvéderm Volift, and Juvéderm Volbella as described in Table 2. As she presented with deep NLFs, she received 1 mL in each NLF, resulting in a total injected volume of 13 mL HA filler. After treatment, she was assessed as having restored volume in the midface and around the eyes, with better structural support, an “exceptionally natural” outcome, and a friendlier, more confident, and energetic face. HA, hyaluronic acid; NLF, nasolabial fold. |
 |
Figure 6 Full-face rejuvenation based on the MD Codes: a 42-year-old woman before (A–D) and immediately after (E–H) treatment. The woman presented with loss of definition in the cheekbone area, hollowing and dark circles under the eyes, and fullness and sagging in the lower face, with a double chin. Her primary concerns were bags around the eyes, double chin, and NLFs. The treatment plan for this patient was full-face rejuvenation with Juvéderm Voluma, Juvéderm Volift, and Juvéderm Volbella as described in Table 2 with no deviations and a total injected volume of 12 mL HA filler. After treatment, she was assessed as having a refreshed, less tired appearance and a more contoured and slimmer-looking face with more caring and optimistic social attributes. HA, hyaluronic acid; NLFs, nasolabial folds. |
Safety
No serious side effects were reported. The most commonly reported side effects were injection site responses, such as swelling, bruising, redness, and bleeding, which were mild in severity and resolved without treatment. One month after injection, 1 patient developed persistent intermittent delayed swelling, which was considered to be triggered by genital herpes and was treated with prednisolone (20 mg once daily) and valaciclovir (500 mg thrice daily) for 5 days, in which time the patient recovered with no recurrence. All patients were vaccinated against COVID-19 after the treatment, and no adverse event occurred in the treated areas related to the vaccines.
Discussion
Injectable treatment with HA fillers is a continuously growing field, with more than 4 million procedures performed worldwide in 2020.24 The conventional method for performing injectable aesthetic treatments has mainly consisted of filling the lines and wrinkles upon request, sometimes leading to unsatisfactory and inconsistent results.8 The versatile capabilities of HA fillers extend far beyond their traditional role of addressing facial folds. Today, these injectables are harnessed either individually or in strategic combinations to enhance a wide spectrum of facial aesthetic units, ultimately leading to the enhancement of one’s overall facial appearance and delivering exceptional outcomes.25 The current study is unique in its focus on emotional and social attributes and natural-looking results in individuals treated with HA fillers using a systematic and reproducible full facial treatment protocol based on the MD Codes. Throughout time, we have realized the core essence of aesthetic procedures lies not merely in assessing the static appearance of the face, but in comprehending how it presents itself in motion. Moreover, it involves decoding the language of emotions conveyed through these facial expressions. As of today, the outcomes of these endeavors have been satisfying.26
The findings of the current study are important because messages of the face play a role in everyday social interaction, affecting both an individual’s self-confidence and others’ perceptions.6,27 Most patients reported improvements in all 8 emotional attributes addressed by the MD Codes (ie, looking less tired, saggy, angry, or sad; younger; more feminine, attractive, or contoured) through 6 months. The top 3 emotional attribute improvements were looking “less tired”, “less saggy”, and “less sad.” Patients recognized their overall improvements in emotional attributes beyond the initial benefit noticed immediately after treatment. All but 1 patient continued to report looking less tired even 9 months after initial treatment, suggesting a durable effect on “looking tired” with the MD Codes. As “tiredness” was better observed in frontal and oblique views, and “sagginess” was better observed in full-profile view, evaluation of treatment outcomes by viewing patients from different angles is recommended. Similar improvements in social attributes were reported by patients immediately after treatment and persisting through 9 months.
The current study supports previously published data on improved facial attributes, social perceptions, patient satisfaction, and psychological impacts with the use of full facial aesthetic treatment approaches.6,16,27 In a study of 250 patients who underwent full facial treatment using the MD Codes systematic approach to address facial aesthetic concerns such as sagginess, downturned corners of the mouth, an older-looking appearance, and facial hollowness, there was high patient satisfaction and significant improvements in patient-reported outcomes (PROs).16 An analysis of the perceptions of 2000 blinded study respondents based on pre- and post-treatment images of 84 patients (168 images) from the US HARMONY Study found that patients treated with HA fillers, onabotulinumtoxinA, and an eyelash growth product were consistently perceived as being more attractive, more approachable, more socially adept, and friendlier, and having a variety of other socially advantageous attributes, after treatment.6 A study of PRO measures in patients treated with the HA injectable gel VYC-12 (Juvéderm Volite®; Allergan Aesthetics, an AbbVie Company, Irvine, CA) in the cheeks, the forehead, and, optionally, the neck found significant improvements in patients’ Satisfaction with Skin scores at months 1, 4, 6, and 9 after initial/touch-up treatment and month 1 after repeat treatment.28 Similarly, studies of onabotulinumtoxinA (Botox® Cosmetic; Allergan Aesthetics, an AbbVie Company, Irvine, CA) treatment for forehead lines, glabellar lines, and crow’s feet lines showed significant improvements for up to 12 months (including after repeat treatment) in appearance-related psychological and emotional impacts, such as being bothered by facial lines, looking older than actual age, looking less attractive, and having appearance-related age, anger, tiredness, emotional unhappiness, and negative self-esteem.29,30 Recent clinical trials have even suggested that treatment with botulinum toxin in upper facial lines can be therapeutic for depression.31 These data, combined with the findings of the current study, support the strategy of decreasing or eliminating negative facial attributes to lay the foundation of achieving the patient’s desired aesthetic outcomes.
The overall aesthetic outcomes reported herein were perceived as natural by all patients, which satisfies the desire of individuals seeking aesthetic treatment to achieve a natural look,32 supports existing data on natural-looking results with the use of HA fillers,33 and provides an association between natural-looking results and full facial aesthetic treatment using the MD Codes. The majority of patients were assessed “natural” to “exceptionally natural” by all observers and patients, considering possible bias of the study injector group. The frontal and oblique views were more often evaluated as “exceptionally natural” and “very natural” compared with the full profile view, which was assessed more frequently as “unaltered”, confirming the importance of treatment evaluation using different views of the patient.
Similar to other studies relying on both patient and objective evaluations of the effects of treatment on facial appearance,34,35 there were discrepancies between patient self-assessment and observer assessments after treatment. Observers differed from patients in their assessments of the facial areas most in need of treatment and in the weight given to the emotional attribute “less tired.” This reflects the importance of the patient’s perspective in deciding whether an optimal aesthetic outcome has been achieved.
Remarkably, all patients received identical treatments using the MD Codes anatomical subunits (12 mL); only 1 patient required a volume adjustment with 1 added syringe of HA filler (13 mL), due to the severity of deep lines in the nasolabial fold. Treatment was well tolerated and the safety profile was consistent with HA fillers. No reaction to COVID-19 vaccination was reported in the follow-up period of almost 2 years. Based on the outcomes of the study, the chosen volume of HA dermal fillers with different rheological and physicochemical properties (ie, up to 13 distributed over the face following the MD Codes) may be appropriate for most patients to improve emotional and social attributes and attain a visible rejuvenation. However, it is vital that the injector perform a sufficient medical and aesthetic assessment to make the correct diagnosis and determine patient eligibility for global aesthetic treatment of the face. It is also important for the injector and the patient to set expectations for aesthetic goals. Patient education is, of course, key to a successful consultation. The processes of aging and the concepts of a global, rather than focal, assessment need to be explained. Determining the appropriate amount of filler is necessary; in the authors’ clinical experience, under-correction often results in less satisfying outcomes or reduced patient motivation along the treatment journey. Distributing full-face treatments across multiple sessions as suggested in this study may allow the patient to appreciate the gradual improvement as well as adequately plan for the cost of treatment.
Although a systematic treatment approach may be critiqued as a “cookie cutter” solution that makes aesthetic treatment less artistic or too “rigid” or technical, the current study demonstrates that a systematic protocol can be successful across many different individuals with unique facial features and different ages, without distorting the natural anatomy, but improving the global appearance. It also represents a more scientific approach in contrast to an intuitive approach. Applying a protocol may guide injectors to follow a path for achieving more natural and safer results because the design of the MD Codes comes with anatomical and volume application guidance. However, to ensure measurable, consistent outcomes, it is critical to implement standardized photography to properly evaluate the results with patients’ pre- and post-treatment images, as done in this study.
This study, as a retrospective pilot study, included a small number of patients. This sample size may not have been large enough to make definitive conclusions regarding the use of MD Codes for the improvement of emotional and social messages. On the other hand, the controlled, technical protocol using the consistent and reproducible MD Codes system may mitigate the number of technical variables that would negatively impact results and conclusions of clinical trials with injectables. The study objective was achieved by reducing, as much as possible, the number of technical variables that could negatively affect the desired outcome.
In clinical practice, training and education gaps may exist that render these results unreproducible for some injectors who are not yet familiar with the MD Codes system. The study depended on the injectors’ ability to apply the MD Codes protocol correctly, including all the controlled details of the technique, such as the manner of distribution (fanning, linear, or bolus deposition of filler); recommended amount of product; appropriate device (needle or cannula) for distributing the product in the safest way; appropriate anatomical layer for injection (skin, fat layer, muscle, or supraperiosteal layer); and adaptation of injection angles and positioning in relation to anatomical structures (retaining ligament and muscle insertions and origins to enable desired myomodulation effects).8 However, a treatment protocol with clear injection guidance for clinicians to follow seems to be more reproducible and safer than any intuitive or artistic approach.
The current analysis was not a blinded, controlled study and therefore may have involved potential bias in patient and observer assessments of treatment effects. The study did not use validated patient-reported outcomes such as the FACE-Q; rather, it relied on subjective self-report measures and expert ratings to evaluate emotional attributes and message regulation. Larger, more comprehensive studies that include objective psychosocial measures will be needed to provide further value to these findings.
Additionally, the patients who were selected for treatment may have been more aesthetically aware and eager to receive complimentary treatment, which could have influenced their treatment assessments and satisfaction levels. Formal, controlled studies could provide further validation and refine the information available to clinicians considering adopting the approach in their own facial aesthetics practice.
Despite these limitations, we strongly believe that the lack of consistency in technique in medical aesthetics may be a critical factor in patients’ dissatisfaction with treatments and unnatural results. We would like to reiterate that this study was a pilot investigation, and we acknowledge the need for larger, more comprehensive studies to confirm our findings. Our intention with this retrospective study was to serve as a pilot and a source of inspiration for researchers to incorporate these findings of a structured approach to medical aesthetics over an intuitive approach into more extensive investigations on this topic in the future. Nonetheless, we are encouraged by the potential impact our study may have on the field of emotional and social messages as an additional objective for patients who are looking for aesthetics procedures.
Conclusions
The results of this study suggest that the MD Codes protocol designed for the training session discussed herein can influence facial appearance in a multifaceted way, improving the transmission of emotionally and socially related messages, as well as patients’ feelings about themselves, while achieving instant and long-term natural results. This research may assist injectors with evaluating the success of treatment, not based on wrinkle reduction, but on the impact of global appearance. The ultimate measure of a successful treatment is the patient’s perceived outcome and self-estimated degree of satisfaction. In the authors’ experience, the same protocol could be applied to any patient presenting with similar signs of facial aging and similar unfavorable emotional and social messages, regardless of ethnicity and gender. The protocol may also be beneficial for training sessions for clinicians willing to learn how to deliver treatment beyond the correction of lines or folds, reduce adverse events, and increase patient satisfaction with aesthetic procedures.
On a final note, despite the large body of scientific literature on aesthetic procedures, the practice of aesthetic medicine still needs to be taken more seriously by nonaesthetic practitioners and not viewed simply as “pure vanity.” The MD Codes system may be considered a reproducible alternative to solidify a scientific approach with injectables.
Abbreviations
BoNT/A, botulinum toxin type A; HA, hyaluronic acid; NLF, nasolabial fold; PRO, patient-reported outcome.
Data Sharing Statement
AbbVie is committed to responsible data sharing regarding the clinical trials we sponsor. This includes access to anonymized, individual, and trial-level data (analysis data sets), as well as other information (eg, protocols, clinical study reports, or analysis plans), as long as the trials are not part of an ongoing or planned regulatory submission. This includes requests for clinical trial data for unlicensed products and indications.
These clinical trial data can be requested by any qualified researchers who engage in rigorous, independent, scientific research, and will be provided following review and approval of a research proposal, Statistical Analysis Plan (SAP), and execution of a Data Sharing Agreement (DSA). Data requests can be submitted at any time after approval in the US and Europe and after acceptance of this manuscript for publication. The data will be accessible for 12 months, with possible extensions considered. For more information on the process or to submit a request, visit the following link: https://www.abbvieclinicaltrials.com/hcp/data-sharing.
Ethical Statements
The study was conducted in accordance with the Declaration of Helsinki. This study did not require ethics committee approval because it is a retrospective analysis of an educational activity that was performed for training purposes only. Patients were given information about the procedure, risks, and potential side effects.
Consent for Publication
All patients provided written informed consent for treatment and use of their photographs.
Acknowledgments
Medical writing and editorial assistance were provided by Regina Kelly, MA (Peloton Advantage, LLC, an OPEN Health company) and funded by an unrestricted educational grant provided by Allergan Aesthetics, an AbbVie Company. The authors thank the other injectors at the clinical education event, Drs. Sherina Balaratnam, Vandana Chatrath, Pegah Ceric-Dehdari, Sarah Hart, Anna Jen Shi Hoo, Izzy Lung I. Lee, Alexandre Marchac, and Dimitrios Sykianakis, and Michael Silberberg, MD of Allergan Aesthetics, an AbbVie Company, Marlow, UK, for his support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
AbbVie funded medical writing and editorial support for this publication through an unrestricted educational grant and participated in the review and approval of the publication. All authors had access to relevant data and participated in the drafting, review, and approval of this publication. No honoraria or payments were made for authorship.
Disclosure
All authors are consultants for Allergan Aesthetics, an AbbVie Company. No honoraria or payments were made for authorship. Dr Elian Brenninkmeijer also reports participation within the internal mentorship team of Mauricio de Maio, Allergan Medical Institute. The authors report no other conflicts of interest in this work.
References
1. Michaud T, Gassia V, Belhaouari L. Facial dynamics and emotional expressions in facial aging treatments. J Cosmet Dermatol. 2015;14(1):9–21. doi:10.1111/jocd.12128
2. Palumbo R, Adams RB Jr, Hess U, Kleck RE, Zebrowitz L. Age and gender differences in facial attractiveness, but not emotion resemblance, contribute to age and gender stereotypes. Front Psychol. 2017;8:1704. doi:10.3389/fpsyg.2017.01704
3. de Maio M. Myomodulation with injectable fillers: an innovative approach to addressing facial muscle movement. Aesthetic Plast Surg. 2018;42(3):798–814. doi:10.1007/s00266-018-1116-z
4. Ganel T. Smiling makes you look older. Psychon Bull Rev. 2015;22(6):1671–1677. doi:10.3758/s13423-015-0822-7
5. Zebrowitz LA, Montepare JM. Social psychological face perception: why appearance matters. Soc Personal Psychol Compass. 2008;2(3):1497. doi:10.1111/j.1751-9004.2008.00109.x
6. Dayan S, Rivkin A, Sykes JM, et al. Aesthetic treatment positively impacts social perception: analysis of subjects from the HARMONY study. Aesthet Surg J. 2019;39(12):1380–1389. doi:10.1093/asj/sjy239
7. Khan JA. Aesthetic surgery: diagnosing and healing the miscues of human facial expression. Ophthal Plast Reconstr Surg. 2001;17(1):4–6. doi:10.1097/00002341-200101000-00002
8. de Maio M. MD codes: a methodological approach to facial aesthetic treatment with injectable hyaluronic acid fillers. Aesthetic Plast Surg. 2021;45(2):690–709. doi:10.1007/s00266-020-01762-7
9. Folster M, Hess U, Werheid K. Facial age affects emotional expression decoding. Front Psychol. 2014;5:30. doi:10.3389/fpsyg.2014.00030
10. Voelkle MC, Ebner NC, Lindenberger U, Riediger M. Let me guess how old you are: effects of age, gender, and facial expression on perceptions of age. Psychol Aging. 2012;27(2):265–277. doi:10.1037/a0025065
11. Martinez L, Falvello VB, Aviezer H, Todorov A. Contributions of facial expressions and body language to the rapid perception of dynamic emotions. Cogn Emot. 2016;30(5):939–952. doi:10.1080/02699931.2015.1035229
12. Gupta MA, Gilchrest BA. Psychosocial aspects of aging skin. Dermatol Clin. 2005;23(4):643–648. doi:10.1016/j.det.2005.05.012
13. Raspaldo H, Aziza R, Belhaouari L, et al. How to achieve synergy between volume replacement and filling products for global facial rejuvenation. J Cosmet Laser Ther. 2011;13(2):77–86. doi:10.3109/14764172.2011.564629
14. Swift A, Liew S, Weinkle S, Garcia JK, Silberberg MB. The facial aging process from the “inside out”. Aesthet Surg J. 2021;41(10):1107–1119. doi:10.1093/asj/sjaa339
15. Braz AV, Sakuma TH. Midface rejuvenation: an innovative technique to restore cheek volume. Dermatol Surg. 2012;38(1):118–120. doi:10.1111/j.1524-4725.2011.02161.x
16. Bertossi D, Nocini PF, Rahman E, Heydenrych I, Kapoor KM, de Maio M. Non surgical facial reshaping using MD Codes. J Cosmet Dermatol. 2020;19(9):2219–2228. doi:10.1111/jocd.13596
17. Urdiales-Galvez F, Delgado NE, Figueiredo V, et al. Preventing the complications associated with the use of dermal fillers in facial aesthetic procedures: an Expert Group Consensus Report. Aesthetic Plast Surg. 2017;41(3):667–677. doi:10.1007/s00266-017-0798-y
18. Philipp-Dormston WG, Goodman GJ, De Boulle K, et al. Global approaches to the prevention and management of delayed-onset adverse reactions with hyaluronic acid-based fillers. Plast Reconstr Surg Glob Open. 2020;8:e2730.
19. Cohen JL, Rivkin A, Dayan S, et al. Multimodal facial aesthetic treatment on the appearance of aging, social confidence, and psychological wellbeing: HARMONY study. Aesthet Surg J. 2022;42(2):NP115–NP124. doi:10.1093/asj/sjab114
20. de Maio M, Chatrath V, Hart S, et al. Multi-Dimensional Aesthetic Scan Assessment (MD ASA): initial experience with a novel consultation, facial assessment, and treatment planning tool. J Cosmet Dermatol. 2021;20(7):2069–2082. doi:10.1111/jocd.14216
21. Jiang B, Ramirez M, Ranjit-Reeves R, Baumann L, Woodward J. Noncollagen dermal fillers: a summary of the clinical trials used for their FDA approval. Dermatol Surg. 2019;45(12):1585–1596. doi:10.1097/DSS.0000000000002141
22. Bertossi D, Giampaoli G, Lucchese A, et al. The skin rejuvenation associated treatment-Fraxel laser, Microbotox, and low G prime hyaluronic acid: preliminary results. Lasers Med Sci. 2019;34(7):1449–1455. doi:10.1007/s10103-019-02738-z
23. Siperstein R, Montes JR, Speranza A. A retrospective review of the safety and efficacy of low-dose triamcinolone mixed with hyaluronic acid fillers to reduce post-injection infraorbital swelling. J Clin Aesthet Dermatol. 2022;15(4):13–19.
24. International Society of Aesthetic Plastic Surgery. ISAPS international survey on aesthetic/cosmetic procedures performed in 2020; 2021. Available from: https://www.isaps.org/discover/about-isaps/global-statistics/reports-and-press-releases/global-survey-2020-full-report-and-press-releases-english/.
25. Michon A, Hassan H. Is more better? Benefits of hyaluronic acid soft tissue filler on the psychological- and social-related quality of life dimensions. Aesthet Surg J Open Forum. 2022;4.
26. Lipko-Godlewska S, Bolanča Ž, Kalinová L, et al. Whole-face approach with hyaluronic acid fillers. Clin Cosmet Investig Dermatol. 2021;14:169–178. doi:10.2147/CCID.S292501
27. de Maio M. Myomodulation with injectable fillers: an update. Aesthetic Plast Surg. 2020;44(4):1317–1319. doi:10.1007/s00266-020-01768-1
28. Ogilvie P, Safa M, Chantrey J, et al. Improvements in satisfaction with skin after treatment of facial fine lines with VYC-12 injectable gel: patient-reported outcomes from a prospective study. J Cosmet Dermatol. 2020;19(5):1065–1070. doi:10.1111/jocd.13129
29. Rivkin AZ, Ogilvie P, Dayan S, Yoelin SG, Weichman BM, Garcia JK. OnabotulinumtoxinA for simultaneous treatment of upper facial lines: subject-reported satisfaction and impact from a Phase 3 study. Dermatol Surg. 2020;46(1):50–60. doi:10.1097/DSS.0000000000001883
30. De Boulle KL, Werschler WP, Gold MH, et al. Phase 3 study of onabotulinumtoxinA distributed between frontalis, glabellar complex, and lateral canthal areas for treatment of upper facial lines. Dermatol Surg. 2018;44(11):1437–1448. doi:10.1097/DSS.0000000000001612
31. Wollmer MA, Magid M, Kruger THC, Finzi E. The use of botulinum toxin for treatment of depression. Handb Exp Pharmacol. 2021;263:265–278.
32. Carruthers A, Cohen JL, Cox SE, et al. Facial aesthetics: achieving the natural, relaxed look. J Cosmet Laser Ther. 2007;9(suppl 1):6–10. doi:10.1080/17429590701523927
33. Monheit G, Beer K, Hardas B, et al. Safety and effectiveness of the hyaluronic acid dermal filler VYC-17.5L for nasolabial folds: results of a randomized, controlled study. Dermatol Surg. 2018;44(5):670–678. doi:10.1097/DSS.0000000000001529
34. Ogilvie P, Fink B, Leys C, et al. Improvement of radial cheek lines with hyaluronic acid-based dermal filler VYC-17.5L: results of the BEAM study. Dermatol Surg. 2020;46(3):376–385. doi:10.1097/DSS.0000000000002057
35. Weinkle SH, Werschler WP, Teller CF, et al. Impact of comprehensive, minimally invasive, multimodal aesthetic treatment on satisfaction with facial appearance: the HARMONY study. Aesthet Surg J. 2018;38(5):540–556. doi:10.1093/asj/sjx179
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Safe and Effective Lip Enhancement with VYC-15L in Chinese Adults
Li D, Gao Z, Sun J, Li Q, Jiang P, Zhang L, Chawla S
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2427-2436
Published Date: 10 November 2022
Contouring Plus: A Comprehensive Approach of the Lower Third of the Face with Calcium Hydroxylapatite and Hyaluronic Acid

Viscomi B, Faria G, Hernandez CA, Perez L, Spada J, De la Fuente V, Muniz M
Clinical, Cosmetic and Investigational Dermatology 2023, 16:911-924
Published Date: 5 April 2023
Efficacy and Tolerability of Cosmetic Serums Enriched with Five Forms of Hyaluronic Acid as Part of Biweekly Diamond Tip Microdermabrasion Treatments for Facial Skin Dryness and Age-Associated Features
Makino ET, Huang PC, Emmerich T, Jiang LI, Mehta RC
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1123-1134
Published Date: 27 April 2023
Long-Term Efficacy and Tolerability of a Medium G’ HA Filler with Tri-Hyal Technology on the Rejuvenation of the Mobile Facial Zone
David M, Braccini F, Garcia P, Loreto F, Benadiba L, Gorj M, Grand-Vincent A, Rumyantseva Mathey E, Deutsch JJ, Ehlinger A, Cartier H, Nadra K, Fanian F
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1795-1805
Published Date: 13 July 2023
Mitigating Glycation and Oxidative Stress in Aesthetic Medicine: Hyaluronic Acid and Trehalose Synergy for Anti-AGEs Action in Skin Aging Treatment
Chmielewski R, Lesiak A
Clinical, Cosmetic and Investigational Dermatology 2024, 17:2701-2712
Published Date: 28 November 2024