Back to Journals » Infection and Drug Resistance » Volume 19
Construction of a Diagnostic Model for Pneumocystis Jirovecii Pneumonia in HIV-Negative Patients Based on Single-Center Patient Data
Authors Liang J ![]() , Xiong G
, Xiong G ![]() , Han F, Zhuge S
, Han F, Zhuge S
Received 2 November 2025
Accepted for publication 26 February 2026
Published 16 March 2026 Volume 2026:19 573344
DOI https://doi.org/10.2147/IDR.S573344
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Jianghong Liang,1 Guirun Xiong,1 Fang Han,1 Siliang Zhuge2
1Department of Emergency Medicine, Tongde Hospital of Zhejiang Province, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Emergency Medicine, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital, Hangzhou Medical College), Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Fang Han, Department of Emergency Medicine, Tongde Hospital of Zhejiang Province, Hangzhou, Zhejiang, 310012, People’s Republic of China, Tel/Fax +86-13588700698, Email [email protected] Siliang Zhuge, Department of Emergency Medicine, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital, Hangzhou Medical College), Hangzhou, Zhejiang, 310014, People’s Republic of China, Tel/Fax +86-18603294101, Email [email protected]
Background: Given the rising incidence, acute onset of Pneumocystis jirovecii pneumonia (PJP) in HIV-negative patients, and the limitations of existing diagnostic methods (poor sensitivity, low accessibility, and difficulty distinguishing infection from colonization), this study aims to develop and validate a diagnostic prediction model for PJP in this population.
Methods: A retrospective observational study was conducted on hospitalized patients with suspected PJP at Zhejiang Provincial People’s Hospital from 2017 to 2022. Based on the inclusion and exclusion criteria, 115 HIV-negative patients were enrolled, including 37 with confirmed PJP and 78 with PJP ruled out. Clinical data including age, gender, comorbidities, laboratory indicators, and treatment history were collected. The LASSO method was used to screen predictive variables for constructing a model, which was internally validated via Bootstrap resampling and visualized as a nomogram.
Results: A 7-variable PJP diagnostic prediction model was constructed following LASSO variable screening. The model exhibited good performance in distinguishing whether HIV-negative patients were afflicted with PJP, with an area under the ROC curve (AUC) of 0.895 (95% CI: 0.834– 0.956). The calibration curve revealed high consistency between predicted and actual probabilities, and decision curve analysis demonstrated its superior clinical net benefit over all-intervention and no-intervention strategies. Bootstrap internal validation yielded a stable AUC of 0.895 (95% CI: 0.831– 0.947) with consistent calibration.
Conclusion: This study established a predictive model for Pneumocystis jirovecii pneumonia (PJP) in HIV-negative patients, and this effort is clinically meaningful. However, due to several limitations of the present study, it should be emphasized that the final nomogram only serves as a supplement to, rather than a replacement for, existing diagnostic approaches. The findings of this study warrant further validation in future multicenter or prospective investigations.
Keywords: pneumocystis jirovecii pneumonia, HIV-negative patients, diagnosis, predictive model
Introduction
Pneumocystis was first discovered in the lungs of rats and guinea pigs by Carlos Chagas in 1909. In the same year, it was also identified in the lungs of deceased patients infected with trypanosomes.1 Subsequently, cases of human pneumonia caused by Pneumocystis were reported. However, such cases were rare initially, yet the incidence of Pneumocystis pneumonia rose drastically following the outbreak of acquired immunodeficiency syndrome (AIDS) in the 1980s.2 In 1988, Edman JC et al3 identified Pneumocystis as a fungus by analyzing ribosomal RNA (rRNA) sequences, refuting the earlier view that it was classified as a “protozoan” based on its morphological characteristics and other traits.4 Meanwhile, studies have also confirmed that Pneumocystis is a genus-specific pathogenic fungus; to distinguish the specificity of different Pneumocystis organisms, the pathogen that infects humans was named Pneumocystis jirovecii (PJ).5
Pneumocystis jirovecii pneumonia (PJP) is a life-threatening opportunistic fungal infection. Currently, there are no reports of it causing disease in hosts with fully normal immune function, and it is most commonly seen in patients with AIDS.2 However, with the increased awareness of PJP among clinicians and the advances in AIDS diagnosis and treatment, the incidence and mortality of this infection in HIV-positive patients have shown a downward trend.6,7 And, with the increase in stem cell and solid organ transplants, the prolonged survival of cancer patients, and the use of higher-dose and more effective immunosuppressive and cytotoxic drugs in autoimmune and inflammatory diseases (AIIDs), kidney diseases, and other conditions, immune dysfunction complicated with PJP is becoming increasingly common in HIV-negative patients.8,9 Globally, approximately 105,000 cases of PJP occur in HIV-negative patients each year (incidence: 6.5/100,000 population); in China, the annual number of cases reaches 9,241 (incidence: 0.64/100,000 population).10 A survey conducted in Germany11 revealed that 82.9% of PJP cases were diagnosed in HIV-negative patients, representing an approximately 21.8% increase over five years. Similar rising trends have also been observed in France6 and the US.12 Furthermore, HIV-negative patients with PJP tend to present with a more acute onset, alongside a higher risk of respiratory failure and mortality.13 This poorer outcome is largely attributed to the challenges in establishing a timely and accurate diagnosis.
Since PJ cannot grow on conventional culture media, the gold standard diagnostic methods for PJP involve special staining (eg., Gomori methenamine silver staining, immunofluorescence staining) of respiratory specimens followed by a direct microscopic examination. While these methods have high specificity, they suffer from low sensitivity and prolonged turnaround times,14 often failing to provide timely, effective support for HIV-negative PJP patients with rapidly progressive disease. Currently, clinically available molecular techniques for PJP include polymerase chain reaction (PCR), next-generation sequencing (NGS), loop-mediated isothermal amplification (LAMP), flow cytometry (FCM), and antibody/antigen detection.15,16 However, these techniques have inherent limitations. Taking PCR and NGS as examples: first, they are not widely accessible in public hospitals in China, and specimens usually need testing at specialized laboratories—imposing a heavier economic burden. Second, despite their extremely high sensitivity, they may fail to distinguish between Pneumocystis infection and colonization, particularly given the pathogen’s colonization rate in healthy individuals (positive detection rates: 20–80% across age groups, varying by method).17,18 Consequently, clinical practice is characterized by the frequent underdiagnosis, of PJP and a lack of proactive prophylaxis among HIV-negative patients.
Several studies have reported the development of diagnostic models for PJP; however, none have been identified that specifically focus on the HIV-negative patient population. By analyzing clinical data of PJP patients from a regional tertiary grade A hospital, our objective was to develop an exploratory diagnostic prediction model to distinguish the probability of PJP development in patients with suspected PJP; subsequently, the model was presented in the form of a nomogram and validated.
Materials and Methods
Patients
This is a single-center, retrospective observational study. This study retrospectively screened inpatients admitted to the Infectious Diseases Department, Respiratory Medicine Department, Hematology Department, ICU, EICU, and Critical Care Rehabilitation Department between 2017 and 2022. The data were retrieved from the clinical case system, Clinical Laboratory Center, and microbiology laboratory testing database of Zhejiang Provincial People’s Hospital.
Inclusion criteria were as follows: I. Age ≥ 18 years; II. Clinical symptoms suggestive of fungal pneumonia; III. Having undergone etiological tests (methenamine silver staining and/or quantitative real-time PCR [qPCR]).
Exclusion criteria were as follows: I. Missing clinical data items accounting for more than 20% of the total items; II. HIV-positive patients; III. Cases where neither PJP diagnosis could be confirmed nor ruled out in the patient’s disease assessment.
Sample Testing
Etiological testing samples included bronchoalveolar lavage fluid (BALF) and induced sputum, which were collected by clinicians. Methenamine silver staining and qPCR were performed by the hospital’s Clinical Laboratory Center and Microbiology Laboratory. Methenamine silver staining was conducted by the Clinical Laboratory in accordance with standard operating procedures for methenamine silver staining. For qPCR testing, the specimens were lysed with 4% sodium hydroxide (NaOH) and centrifuged. Subsequently, 200 μL of the supernatant was subjected to specific binding and elution to obtain the target DNA. The Hongshi SLAN-96P qPCR system and reagents from Shengxiang Biotechnology Co., Ltd. were used. Detection results were determined based on fluorescent signal readouts; a cycle threshold (Ct) values < 37 with a typical S-shaped amplification curve was defined as positive in accordance with the kit’s reference criteria. Samples with a Ct values of 37 to 40 were subjected to retesting for the PJ specific gene.
Definition of Pneumocystis Jirovecii Pneumonia
According to international guidelines19 and other studies,6,8,20 PJP was defined in this study as follows:
Confirmed PJP: (1) Typical clinical manifestations of pneumonia (fever, respiratory symptoms, dyspnea, hypoxemia), (2) Radiological findings (interstitial changes), and (3) Etiological evidence (NGS, PCR) in respiratory specimens, induced sputum, bronchial aspirate, or bronchoalveolar lavage fluid. When Pneumocystis jirovecii was detected by direct microscopic examination of respiratory specimens (using methenamine silver staining in this study), the diagnosis of PJP was confirmed.
Ruled out PJP: (1) Etiological evidence in respiratory specimens, induced sputum, bronchial aspirate, or bronchoalveolar lavage fluid (BALF), but with clinical symptoms and radiological findings inconsistent with PJP, suggesting Pneumocystis jirovecii colonization; or (2) Clinical symptoms and radiological findings consistent with PJP, but negative results from direct microscopic examination and qPCR.
Patients who could not be classified into either the “confirmed PJP” or “ruled out PJP” categories were not included in the statistical analysis of this study.
Collection and Organization of Patients’ Clinical Data
Referring to factors potentially associated with the development of PJP in other studies,2,9,20 this study retrospectively collected the following data from enrolled patients on the day of etiological sampling: age, gender, comorbidities (autoimmune diseases, chronic obstructive pulmonary disease, malignancy, organ transplantation), laboratory indicators (lactate dehydrogenase [LDH], lymphocyte count, neutrophil count, G-test), HIV infection status, surgical history, mechanical ventilation history, as well as hospitalization and treatment history within the past month (including glucocorticoids, immunosuppressants, chemotherapeutic agents, etc).
The use of glucocorticoids in patients within the past month was collected, and all formulations were converted to cortisone equivalents based on the following potency equivalence ratio: cortisone 25 mg = hydrocortisone 20 mg = prednisone 5 mg = prednisolone 5 mg = methylprednisolone 4 mg = triamcinolone 4 mg = betamethasone 0.8 mg = dexamethasone 0.75 mg = beclomethasone 0.5 mg.
Statistical Analysis
Statistical analyses in this study were performed using packages such as rms, survival, MASS, glmnet, pROC, and forestplot in R (version 4.2.2). Missing data were handled using multiple imputation assuming data were missing at random. Cases with excessive missing data (>20%) were excluded from the analysis.
First, the baseline data of the included patients were summarized. The chi-square test and t-test were used to compare intergroup differences. Categorical variables were presented as n (percentage), while continuous variables were expressed as mean ± standard deviation. Subsequently, the least absolute shrinkage and selection operator (LASSO) method was applied to baseline data to screen for predictive variables and identify the independent predictors for model inclusion. Finally, the Bootstrap resampling method was used for internal validation with 1000 iterations of sampling with replacement. The model was evaluated using the receiver operating characteristic (ROC) curve, calibration curve (Hosmer-Lemeshow test), and decision curve analysis (DCA).
Ethics and Informed Consent Statement
This study was reviewed and approved by the Ethics Committee of Zhejiang Provincial People’s Hospital on February 18, 2025, with the approval number ZJPPHEC 20250 (044). Since this is a retrospective observational study and uses de-identified and anonymized data, the requirement for obtaining informed consent was waived. The study was conducted in accordance with the Declaration of Helsinki. AI tools were not utilized for study design, data collection, statistical analysis, or the writing of this manuscript.
Results
Patient Inclusion and Baseline Characteristics
In this study, 159 patients with suspected PJP who completed comprehensive etiological examinations between 2017 and 2022 were screened. Among these patients, 30 patients were positive for methenamine silver staining, and 39 patients were positive for qPCR; the positive results are presented in supplementary Table 1. Additionally, 90 patients were negative for etiological examinations. According to the definition of PJP, for 4 patients positive for qPCR, it was not possible to determine whether PJ was in a state of colonization or infection during the review of medical record data. Ultimately, 37 patients were confirmed PJP and 78 patients were ruled out PJP; these patients were included in the statistical analysis. The screening and inclusion process is shown in Figure 1.
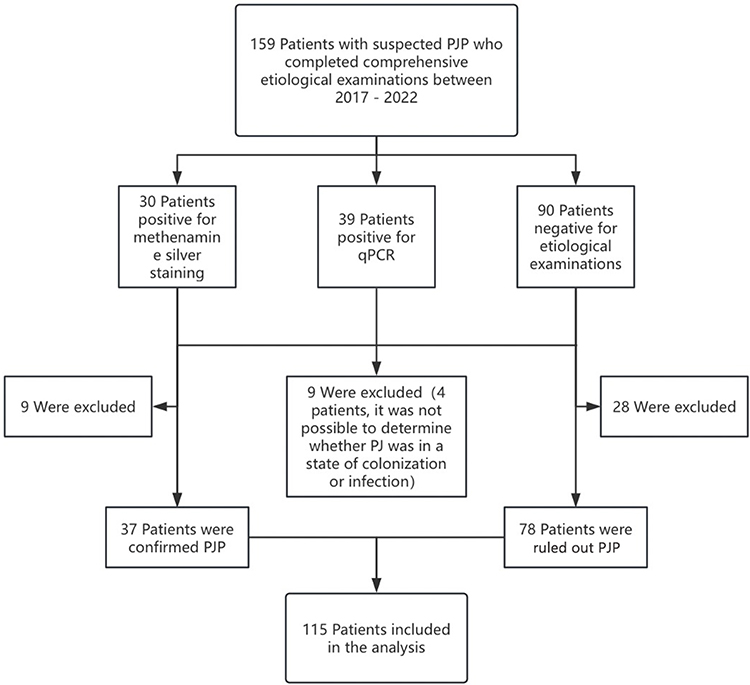 |
Figure 1 Flowchart of screening and inclusion of patients. Abbreviations: PJP, pneumocystis jirovecii pneumonia; PJ, pneumocystis jirovecii; qPCR, quantitative real-time polymerase chain reaction. |
Descriptive statistics were performed on the data of the 115 included patients, with the baseline distribution presented in Table 1. The two groups of patients showed statistically significant differences in age, neutrophil count, LDH, glucocorticoid dosage, immunosuppressant use, autoimmune disease status, and G-test results (p < 0.05).
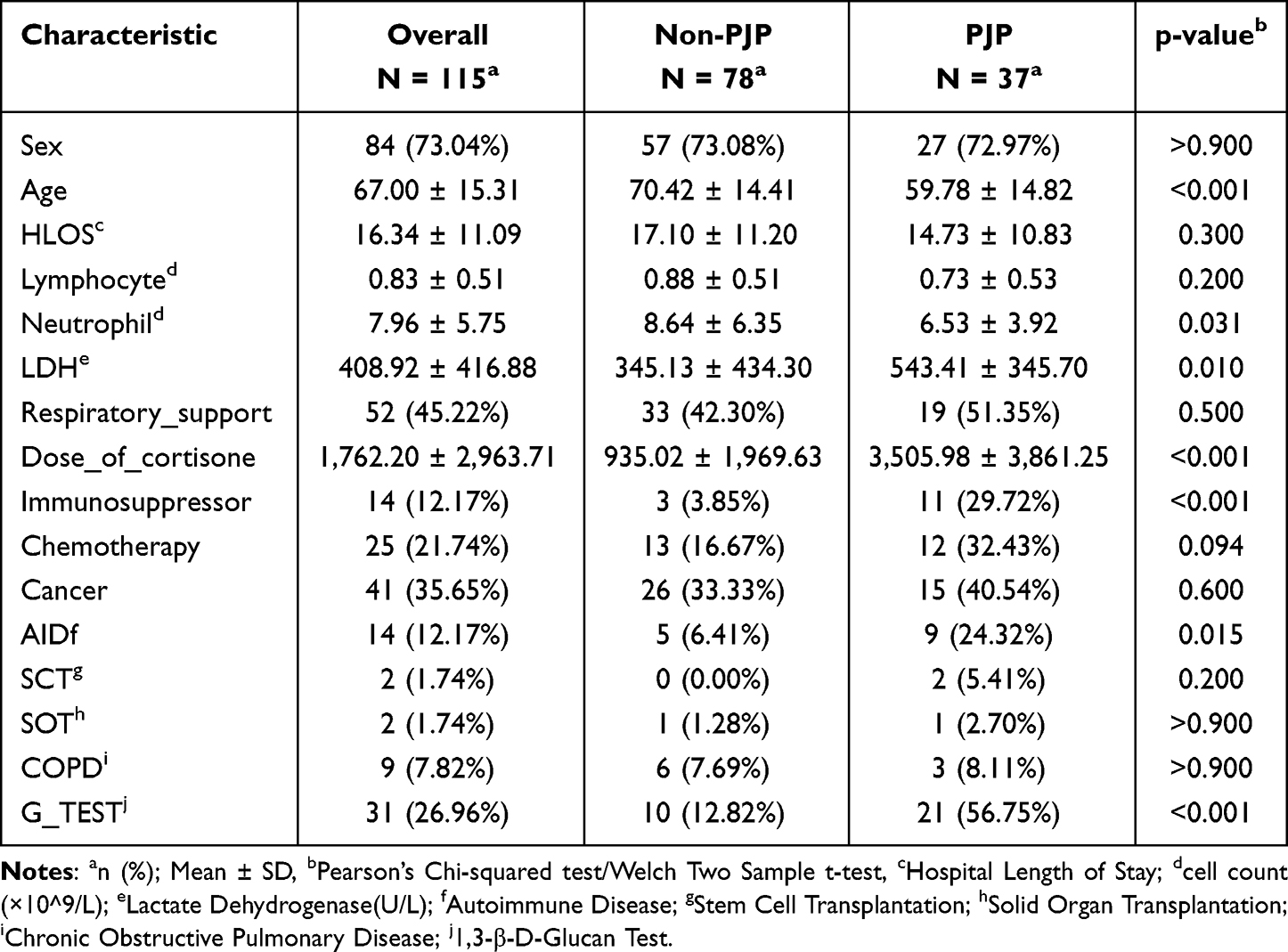 |
Table 1 Baseline Characteristics of 115 Patients |
Predictive Variable Screening
Predictive variables were screened using the LASSO method, and the process of gradually screening out variables that had no substantial impact on the outcome is shown in Figure 2A. At the optimal lambda point (the lowest point on the y-axis in Figure 2B), the model exhibited the best fit. At this point, 7 variables were screened out, namely: AGE, Neutrophil, LDH, Dose_of_cortisone, Immunosuppressor, AID, and G_TEST. Subsequently, univariate and multivariate risk factor analyses were conducted on the screened variables. The results showed that Neutrophil, Immunosuppressor, and G_TEST were independently associated with the occurrence of PJP, as shown in Figure 3.
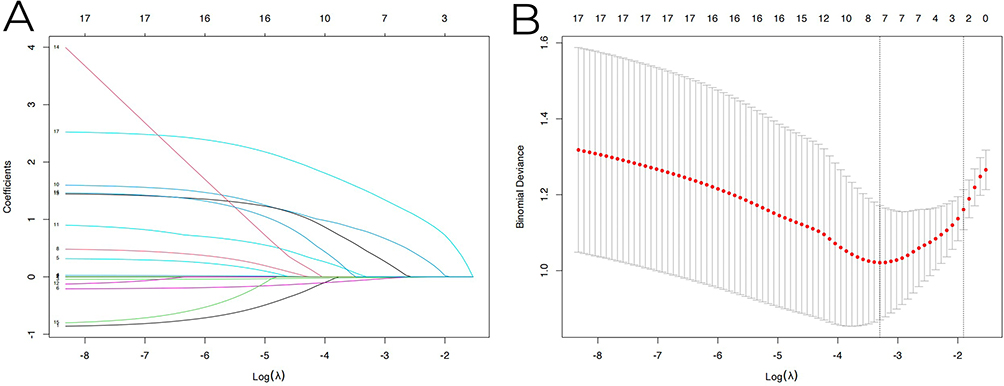 |
Figure 2 (A) LASSO regression coefficient profile plot:Log (lambda) is shown on the x-axis, and variable regression coefficients on the y-axis. Colored lines represent individual variables; coefficients shrink to zero with increasing lambda. (B) LASSO regression model fit plot: Log (lambda) is on the x-axis, and partial likelihood deviance on the y-axis. Vertical dashed lines mark the optimal lambda (minimum deviance) and λ.1se (one standard error from minimum), for determining the penalty parameter balancing model complexity and predictive performance. |
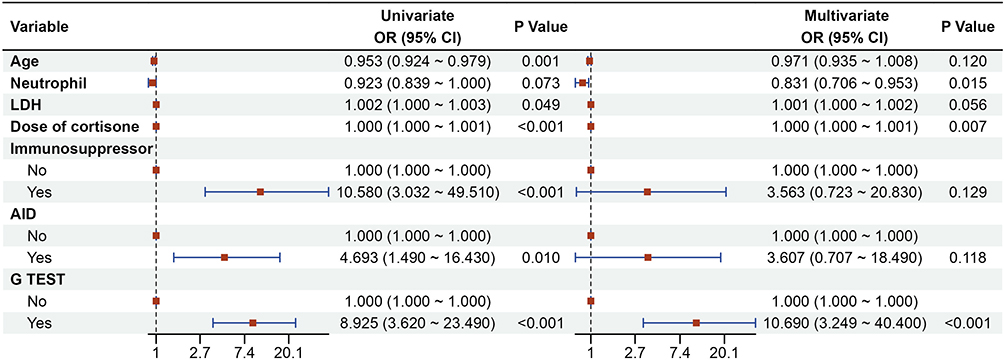 |
Figure 3 Forest Plot of Univariate and Multivariate Analyses for Screened Variables. Abbreviations: LDH, Lactate Dehydrogenase (U/L); AID, Autoimmune Disease; G TEST, 1;3-β-D-Glucan Test. |
Construction of the Predictive Model
A diagnostic prediction model was constructed using the 7 screened variables, the constructed logistic regression equation of the model is as follows:
logit(P) = 0.4097–0.0292 × AGE - 0.1851×Neutrophil + 0.0011 × LDH + 0.0003×Dose_of_cortisone + 1.2707 × Immunosuppressor + 1.2828 × AID + 2.3696 × G_TEST
(Neutrophil: neutrophil cell count (×109/L), LDH: Lactate Dehydrogenase (U/L), AID: Autoimmune Disease, G_TEST: 1,3-β-D-Glucan Test; Sensitivity: 0.892 (89.2%), Specificity: 0.756 (75.6%), Youden Index: 0.648).
And a nomogram was developed to present the results (Figure 4). This model exhibited good performance in distinguishing between PJP and non-PJP patients, with an area under the ROC curve (AUC) of 0.895 (95% CI: 0.834–0.956) (Figure 5A). Meanwhile, in the calibration curve, the x-axis represents predicted probability and the y-axis represents actual probability. The fitted line was close to the diagonal line (which represents the ideal model calibration curve, where actual occurrence probability equals predicted probability), indicating that the diagnostic model showed good calibration (Figure 5B). In the model’s decision curve analysis, across the entire probability range, the clinical net benefit of intervention based on the model’s predicted probability was higher than that of two extreme strategies: no intervention for all individuals and intervention for all individuals (Figure 5C).
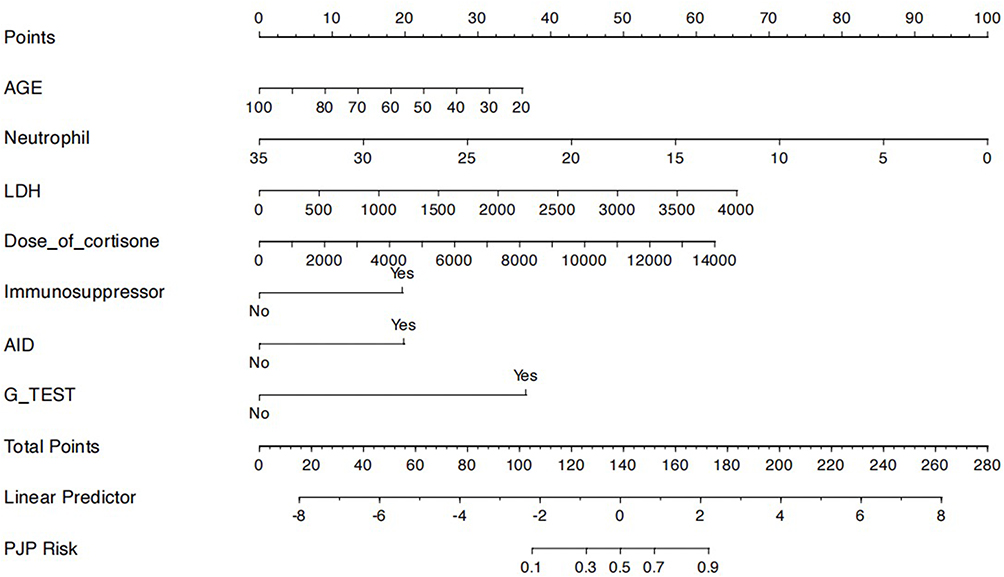 |
Figure 4 Nomogram for PJP Probability Prediction in HIV-Negative Patients: The value of each variable corresponds to a score on the dot scale axis. By summing up the scores of each variable, the total score can be easily calculated; then, by referencing the total score to the total score table below, the probability of PJP occurrence can be estimated. Abbreviations: LDH, Lactate Dehydrogenase (U/L); AID, Autoimmune Disease; G TEST, 1;3-β-D-Glucan Test; PJP, pneumocystis jirovecii pneumonia. |
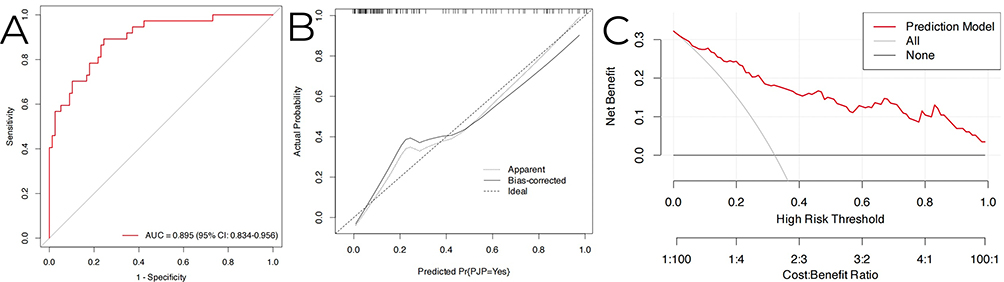 |
Figure 5 (A) ROC Curve of the Predictive Model, (B) Nomogram Calibration Curve, and (C) Nomogram Decision Curve Analysis (DCA). |
Internal Validation of the Model
Internal validation of the diagnostic model was performed using the Bootstrap resampling method, with resampling repeated 1000 times with replacement. During internal validation, the model exhibited good diagnostic performance for PJP: the AUC of the diagnostic model in the internal validation set was 0.895 (95% CI: 0.831–0.947) (Figure 6A). Similarly, the calibration curve of the internal validation also demonstrated good calibration of the diagnostic model (Figure 6B).
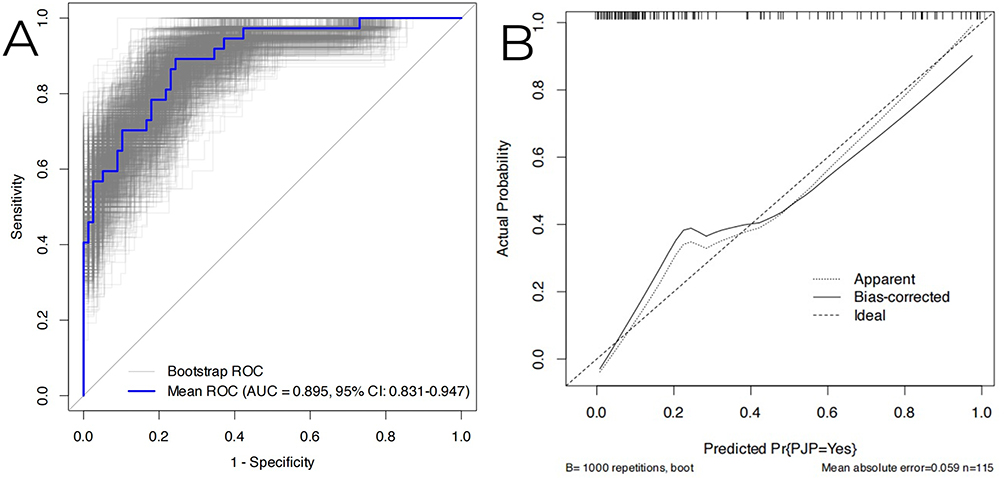 |
Figure 6 (A) Internal Validation ROC Curve, (B) Calibration Curve. |
Discussion
As mentioned earlier, PJP has shown an increasing trend in the incidence rate among HIV-negative patients, with its onset being more severe and acute. Thus, a growing number of studies have focused on this patient population.19–21 However, we still lack prevention guidelines for these patients as well as timely and effective diagnostic protocols.10–12 Therefore, it is of great significance to attempt to develop a more effective method to distinguish whether a patient has PJP or not.
With the development of analytical technologies and increased attention to this disease, there have been several attempts to develop diagnostic models for PJP, yielding promising findings. For instance, Zhou et al22 explored predictive markers for PJP in kidney transplant patients and found that CD8+ T cells < 241.11/μL and serum albumin (ALB) < 35.2 g/L provided reliable predictive value for the occurrence of PJP infection. Qin et al23 on the other hand, constructed and externally validated a model using data from 434 patients on oral glucocorticoids across 6 hospitals; this model demonstrated excellent discriminative ability, with an AUC of 0.82 in the development cohort and 0.87 in the validation cohort. Additionally, Peng et al24 developed a computed tomography (CT)-based radiomics prediction model to distinguish invasive pulmonary aspergillosis from PJP, which also showed good predictive performance, with an AUC of 0.808.
While many valuable studies have paved the way, a definitive investigation on this topic remains lacking, with most existing research featuring small sample sizes of PJP patients. Therefore, we hold that the present study carries significance as an incremental research that supplements regional data on HIV-negative PJP patients and an exploratory study that attempts to identify a more effective approach to determine the PJP status in this specific patient population. Furthermore, the PJP diagnostic criteria were more uniform and clear, and data on treatment medications and hospitalization history were obtained from the same medical record system—factors that may have enhanced the accuracy of data collection.
A diagnostic nomogram for PJP was developed and validated in this study, providing a convenient and efficient tool for distinguishing between PJP and non-PJP cases. This diagnostic tool exhibited good diagnostic performance both in the model itself and its internal validation. Additionally, DCA showed that our model achieved greater net benefit across almost all clinical thresholds. Clinicians can use this diagnostic nomogram to predict the probability of HIV-negative patients developing PJP, thereby informing decisions regarding further treatment and prevention.
Our study inevitably has limitations. First, this is a single-center, retrospective observational study. The enrollment of patient samples is entirely dependent on clinicians’ judgment of patients’ clinical conditions—ie., whether PJP is suspected in a patient and a pathogenic sample is submitted for testing. This gives rise to significant selection and information biases, which may render the study results difficult to generalize in clinical practice. Second, the overall sample size of this study is relatively small, which may cause overfitting of the diagnostic mo in this study, the LASSO method and bootstrap resampling were statistically employed to minimize the risk of model overfitting as much as possible, yet this issue still cannot be overlooked. Third, Although the predictive factors from other studies were referenced when collecting clinical data for this research, our work was still constrained by real-world clinical practice. For instance, T cell subtyping (CD8+ T cells in particular) has been identified to correlate with the development of PJP in numerous studies; however, very few patients included in our study had undergone T cell/lymphocyte subtyping tests. Consequently, the diagnostic model constructed in this study may be limited in its comprehensiveness. Finally, this study focused on the development of a diagnostic model, a type of research that requires external validation, which has not yet been conducted in the present study. Given the limitations of this study, it should be regarded merely as an exploratory study rather than a definitive one. We hold that the findings of this study need to be further validated with patient data of larger sample size and greater diversity, and the nomogram constructed in this study can only serve as an adjunct to existing diagnostic methods rather than a replacement for them.
Conclusion
In conclusion, we conducted an exploratory study based on single-center clinical data of patients with suspected PJP, and developed a diagnostic model consisting of 7 variables—namely AGE, Neutrophil, LDH, Dose_of_cortisone, Immunosuppressor, AID, and G_TEST, which is visualized in the form of a nomogram. This nomogram is designed to predict the probability of PJP in HIV-negative patients, demonstrating good sensitivity and specificity. Meanwhile, the decision curve analysis confirms that using this nomogram yields greater net benefit. However, given that this study is a retrospective investigation with a small sample size from a single center, coupled with its numerous limitations, it is important to emphasize that this nomogram can only serve as a minor supplement to, rather than a replacement for, existing diagnostic methods. The findings of this study also warrant validation by future multicenter or prospective research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hawksworth DL. Responsibility in naming pathogens: the case of Pneumocystis jirovecii, the causal agent of pneumocystis pneumonia. Lancet Infect Dis. 2007;7(1):3–10. doi:10.1016/S1473-3099(06)70663-6
2. Fishman JA. Pneumocystis jiroveci. Semin Respir Crit Care Med. 2020;41(1):141–157. doi:10.1055/s-0039-3399559
3. Edman JC, Kovacs JA, Masur H, et al. Ribosomal RNA sequence shows Pneumocystis carinii to be a member of the fungi. Nature. 1988;334(6182):519–522. doi:10.1038/334519a0
4. Francis G, Andrew HL, Terry W. Pneumocystis. Cold Spring Harb Perspect Med. 2014;4(12):a019828. doi:10.1101/cshperspect.a019828
5. James RS, Charles BB, Robert FM, et al. A new name for pneumocystis from humans and new perspectives on the host-pathogen relationship. Emerg Infect Dis. 2002;8(9):891–896. doi:10.3201/eid0809.020096
6. Anne-L B, Karim T, Irina P, et al. Pneumocystis pneumonia suspected cases in 604 non-HIV and HIV patients. Int J Infect Dis. 2016;46:11–17. doi:10.1016/j.ijid.2016.03.018
7. Sean W, Mark EE, Rulan G, et al. Burden of pneumocystis pneumonia in HIV-infected adults in Sub-Saharan Africa: a systematic review and meta-analysis. BMC Infect Dis. 2016;16(1):482. doi:10.1186/s12879-016-1809-3
8. Nicholas Q, d’A L, Philippe G, et al. Epidemiology, risk factors, and prophylaxis use for pneumocystis jirovecii pneumonia in the non-hiv population: a retrospective study in Québec, Canada. Open Forum Infect Dis. 2023;11(1):ofad639. doi:10.1093/ofid/ofad639
9. Weyant RB, Kabbani D, Doucette K, et al. Pneumocystis jirovecii: a review with a focus on prevention and treatment. Expert Opin Pharmacother. 2021;22(12):1579–1592. doi:10.1080/14656566.2021.1915989
10. D DW. Global incidence and mortality of severe fungal disease. Lancet Infect Dis. 2024;24(7):e428–e438. doi:10.1016/S1473-3099(23)00692-8
11. Benedikt K, Jubin -S-S, Christoph B, et al. Evolving epidemiology of pneumocystis pneumonia: findings from a longitudinal population-based study and a retrospective multi-center study in Germany. Lancet Reg Health Eur. 2022;15(18):100400.
12. Emily R, N KA. Prevalence and Healthcare Burden of Fungal Infections in the United States, 2018. Open Forum Infect Dis. 2022;9(1):ofab593. doi:10.1093/ofid/ofab593
13. Ting X, Xiaomei K, Liang M. Trends in the epidemiology of pneumocystis pneumonia in immunocompromised patients without HIV infection. J Fungi. 2023;9(8):812.
14. Yuan L, Guoya L, Chenyi Q, et al. PCR diagnosis of Pneumocystis pneumonia: a bivariate meta-analysis. J Clin Microbiol. 2011;49(12):4361–4363. doi:10.1128/JCM.06066-11
15. Maud G-M, White PL, Carlo M, et al. The fungal PCR initiative’s evaluation of in-house and commercial Pneumocystis jirovecii qPCR assays: toward a standard for a diagnostics assay. Med Mycol. 2020;58(6):779–788. doi:10.1093/mmy/myz115
16. Marjorie B, Rita O, Jay KK. Diagnosing Pneumocystis jirovecii pneumonia: a review of current methods and novel approaches. Med Mycol. 2020;58(8):1015–1028. doi:10.1093/mmy/myaa024
17. Lu B, Yantong L, Yantong L, et al. Advances in pathogen detection of Pneumocystis jirovecii pneumonia. Infect Med. 2025;4(4):100216. doi:10.1016/j.imj.2025.100216
18. Sarah R, James M, Aditya M, et al. Pneumocystis jirovecii Pneumonia in HIV-Negative, non-transplant patients: epidemiology, clinical manifestations, diagnosis, treatment, and prevention. Curr Fungal Infect Rep. 2024;18(2):125–135. doi:10.1007/s12281-024-00482-8
19. D JP, Sharon CC, Carol AK, et al. Revision and update of the consensus definitions of invasive fungal disease from the european organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin Infect Dis. 2020;71(6):1367–1376. doi:10.1093/cid/ciz1008
20. Romain L, Nahéma I, Fabrice C, et al. Characteristics and prognosis factors of pneumocystis jirovecii pneumonia according to underlying disease: a retrospective multicenter study. Chest. 2024;165(6):1319–1329. doi:10.1016/j.chest.2024.01.015
21. Peghin M, Fishman JA, Grossi PA. Pneumocystis jiroveci: still troublesome to diagnose and treat. Curr Opin Infect Dis. 2025;38(6):522–529.
22. Jingrun Z, Huaqin P, Jiarui Z, et al. Identification of predictive markers of Pneumocystis jirovecii pneumonia in kidney transplant recipients. Transpl Immunol. 2024;8(85):102074. doi:10.1016/j.trim.2024.102074
23. Qin L, Lijuan L, Yue Z, et al. Development and validation of a diagnostic nomogram for Pneumocystis jirovecii pneumonia in Non-HIV-Infected pneumonia patients undergoing oral glucocorticoid treatment. Infect Drug Resist. 2023;4(16):755–767. doi:10.2147/IDR.S398850.
24. Zhiguo P, Xingzhe G, Miao H, et al. Computed tomography-based radiomics prediction model for differentiating invasive pulmonary aspergillosis and Pneumocystis jirovecii pneumonia. Front Cell Infect Microbiol. 2025;10(15):1552556. doi:10.3389/fcimb.2025.1552556.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Lung Ultrasound-Based Nomogram for the Prediction of Refractory Mycoplasma pneumoniae Pneumonia in Hospitalized Children
Liu G, Wang G, Yang Z, Liu G, Ma H, Lv Y, Ma F, Zhu W
Infection and Drug Resistance 2022, 15:6343-6355
Published Date: 31 October 2022
The Incidence, Risk Factors, and Predictive Model of Obstructive Disease in Post-Tuberculosis Patients
Chang W, Li Z, Liang Q, Zhao W, Li F
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:2457-2466
Published Date: 19 November 2024