Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 15
Comprehensive Analysis of Tumor Microenvironment and PD-L1 Expression Associations with Clinicopathological Features and Prognosis in Diffuse Large B-Cell Lymphoma
Authors Xie YL ![]() , Ke LF, Zhang WW, Kang F, Lu SY, Wu CY, Zhu HH, Wang JC, Chen G
, Ke LF, Zhang WW, Kang F, Lu SY, Wu CY, Zhu HH, Wang JC, Chen G ![]() , Chen YP
, Chen YP
Received 9 June 2025
Accepted for publication 28 August 2025
Published 6 September 2025 Volume 2025:15 Pages 167—179
DOI https://doi.org/10.2147/BLCTT.S545717
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Wilson Gonsalves
Yun-Li Xie,1,2,* Long-Feng Ke,3,* Wen-Wen Zhang,1,* Fu Kang,1 Shu-Yi Lu,2 Chen-Yu Wu,2 Huan-Huan Zhu,2 Jian-Chao Wang,1,* Gang Chen,1 Yan-Ping Chen1,*
1Department of Pathology, Clinical Oncology School of Fujian Medical University, Fujian Cancer Hospital, Fuzhou, People’s Republic of China; 2The School of Basic Medical Sciences, Fujian Medical University, and Department of Pathology, Fujian Cancer Hospital, Fuzhou, People’s Republic of China; 3Department of Molecular Pathology, Clinical Oncology School of Fujian Medical University, Fujian Cancer Hospital, Fuzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan-Ping Chen, Jian-Chao Wang, Department of Pathology of Clinical Oncology School of Fujian Medical University, Fujian Cancer Hospital, Fuzhou, Fujian, People’s Republic of China, Tel +86 0591-83660063, Fax +860591-62752890, Email [email protected]; [email protected]
Introduction: The tumor microenvironment (TME) influences diffuse large B-cell lymphoma (DLBCL) progression, but the prognostic roles of tumor-infiltrating T-lymphocytes (TIL-T), tumor-associated macrophages (TAMs), and PD-L1 remain undefined. This study investigates the clinicopathological associations and prognostic impacts of TIL-T, TAMs, and PD-L1 expression in DLBCL.
Methods: This retrospective study evaluated 89 primary DLBCL cases, integrating clinicopathological data with automated immunohistochemical quantification of CD3, CD8, FOXP3, CD163, and PD-L1 expression in tumor hotspots and microenvironmental compartments. Prognostic associations of TIL-T, TAMs, and PD-L1 expression with PFS and OS were analyzed via Kaplan-Meier methods and Cox regression.
Results: High CD3+ infiltration correlated with lower Ki-67 expression, while elevated FOXP3+ levels linked to improved Eastern Cooperative Oncology Group Performance Status (ECOG). CD163+ TAMs varied by NCCN-IPI risk, ECOG, and cell of origin. Neoplastic PD-L1 (nPD-L1) positivity associated with higher NCCN-IPI scores, CD3+ T-cell infiltration, and CD163+ TAM enrichment. Microenvironmental PD-L1 (mPD-L1) correlated with age, ECOG, B symptoms, and infiltration of all T-cell subsets and TAMs. Survival analysis revealed prolonged overall survival (OS) with high CD3+, CD8+, FOXP3+ TIL-T, CD163+ TAMs, or mPD-L1 positivity, while progression-free survival (PFS) improved with CD3+ infiltration and mPD-L1. Univariate analysis identified B symptoms, extranodal involvement, and low TIL-T levels as OS risks, whereas ECOG 0 and mPD-L1+ were protective. Multivariate modeling confirmed B symptoms, extranodal disease, and CD3+ TIL-T as independent OS predictors; CD3+ TIL-T and B symptoms independently impacted PFS.
Discussion: The TME plays a crucial role in the biological behavior of DLBCL, particularly because TIL-T and TAMs are significantly associated with patient survival outcomes. These cell types may serve as critical biomarkers and provide novel immunotherapy targets in DLBCL.
Keywords: diffuse large B-cell lymphoma, tumor microenvironment, tumor-infiltrating lymphocytes, tumor-associated macrophages, programmed death-ligand 1
Introduction
Diffuse large B-cell lymphoma (DLBCL), the most prevalent adult-onset malignant lymphoma, exhibits pronounced biological heterogeneity. This disease presents distinct variations in clinical manifestations, histomorphological patterns, immunological features, and cytogenetic characteristics.1 The R-CHOP regimen—rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone—has improved the survival of most patients with DLBCL and remains the gold-standard first-line chemotherapy for patients with DLBCL. Although most patients achieve long-term remission or are cured, a substantial percentage ultimately succumb to complications arising from disease relapse or refractory disease.2,3
In recent years, the development of immune checkpoint inhibitors (ICIs), such as anti-PD-1/PD-L1 inhibitors, has considerably improved treatment precision and prolonged patient survival. However, their efficacy in DLBCL remains unpredictable due to limited biomarkers and incomplete understanding of the tumor microenvironment (TME).2,4,5 Emerging evidence indicates that the TME—particularly tumor-infiltrating T lymphocytes (TIL-T) and tumor-associated macrophages (TAMs)—modulates ICI response and influences anti-tumor immunity.4 While PD-L1 expression is established as a biomarker in Hodgkin’s and T-cell lymphomas, its prognostic and predictive role in DLBCL is poorly defined.6 Critically, prior studies lack standardized quantification methods and seldom integrate TME components with PD-L1 in DLBCL prognostication.
To address these gaps, this study employs immunohistochemistry (IHC) staining techniques combined with digital image analysis to characterize TME expression and quantify PD-L1 expression levels in DLBCL. We aimed to investigate TME characteristics and evaluate links among PD-L1 expression, clinicopathological factors, and prognosis in Chinese patients with DLBCL. This work advances DLBCL precision medicine by providing mechanistic insights into TME-immune interactions and delivering actionable biomarkers for risk stratification and therapy selection.
Methods
Case Collection and Histological Assessment
The study included 89 patients diagnosed with primary DLBCL at Fujian Cancer Hospital, China, between August 2012 and November 2022. Inclusion criteria were available histopathological specimens and comprehensive clinical documentation. Clinicopathological features were systematically analyzed through a retrospective review of electronic health records. Biopsy material was subjected to standard histological tissue processing; 10% formalin-fixed and paraffin-embedded (FFPE) tissues were sectioned at a thickness of 3 µm. Sections were stained with hematoxylin and eosin to facilitate microscopy and detailed histopathological analysis. Two hematopathologists independently reviewed all cases, using criteria outlined in the World Health Organization Classification of Tumors of Haematopoietic and Lymphoid Tissues (5th Edition) to confirm histological diagnoses. This study was conducted in strict accordance with the Declaration of Helsinki, and written informed consent was obtained from all participants or their legal guardians. The protocol was approved after a comprehensive review by the Institutional Review Board of Fujian Cancer Hospital (K2022-166-01).
IHC
IHC staining was performed using 3,3′-diaminobenzidine as the chromogen on a Ventana Benchmark XT automated staining system (Roche Diagnostics, Switzerland) at the Department of Pathology, Fujian Cancer Hospital. Sections of FFPE tissue (3 μm thick) were subjected to IHC staining in accordance with a standardized protocol involving specific antibodies against mouse anti-CD3 (MX036, MXB Biotechnologies), rabbit anti-CD8 (SP16, MXB Biotechnologies), mouse anti-FOXP3 (ab215206, Abcam), mouse anti-CD163 (MX081, MXB Biotechnologies), and PD-L1 (clone 28–8, Roche, RRID:SCR_019010). Antigen retrieval and staining protocols were systematically optimized and validated for each biomarker; experimental controls included both positive and negative specimens. Staining assessments were independently conducted by at least two certified pathologists to reach a consensus.
Semiquantitative Assessment of TIL-T and Analysis of PD-L1 Expression
Hematoxylin and eosin-stained and IHC-stained sections were digitally scanned using the IBL 500 automated slide scanning system. Hematopathologist marked the hotspot regions of positive cells in the IHC-stained sections, then the percentages of positive cells in hotspot regions for CD3, CD8, FOXP3, and CD163 markers were quantified using the “Positive Cell Detection” algorithm in QuPath software (version 0.5.1, RRID:SCR_018257). The optimal prognostic cutoff values for positive cells expressing each marker (CD3, CD8, FOXP3, and/or CD163) were determined via receiver operating characteristic (ROC) curve analysis; cases were categorized into low-expression (low) and high-expression (high) subgroups. PD-L1 expression was assessed using a compartment-specific definition: neoplastic PD-L1 (nPD-L1) positivity was defined as staining in >5% of tumor cells, whereas microenvironmental PD-L1 (mPD-L1) positivity was defined as staining in >5% of microenvironmental cells.7,8
Statistical Analysis and Data Availability
The primary endpoints were overall survival (OS) and progression-free survival (PFS). OS was defined as the interval between the date of diagnosis and the date of all-cause mortality. PFS was defined as the interval between the date of diagnosis and the date of recorded tumor progression or all-cause mortality. In terms of radiological assessments, PFS was characterized by evidence of local disease progression or distant metastasis. All statistical analyses were conducted using R software (version 4.3.0, RRID:SCR_001905). Comparisons of clinicopathological features in patients with DLBCL were performed using the t-test, χ2 test, analysis of variance, Fisher’s exact test, Kruskal–Wallis test, or Mann–Whitney U-test, as appropriate. Intergroup survival analysis was conducted using the Kaplan–Meier method. Univariate and multivariate analyses of prognostic factors were performed by Cox proportional hazards regression modeling. P values less than 0.05 were considered statistically significant. The data generated in this study are available within the article and its supplementary data files.
Results
Patient Clinical Characteristics
The clinicopathological features of the 89 patients with DLBCL included in this study are summarized in Table S1. The age distribution ranged from 25 to 78 years (median, 54 years). Among the 89 patients, 49 were men (55.06%) and 40 were women (44.94%), resulting in a male-to-female ratio of 1.2:1. According to the Ann Arbor staging system, six patients (6.74%) had stage I lymphoma, 32 (35.96%) had stage II lymphoma, 18 (20.22%) had stage III lymphoma, and 33 (37.08%) had stage IV lymphoma. Based on the cell of origin, 23 patients (25.84%) had the germinal center B-cell (GCB) subtype of DLBCL, whereas 66 (74.16%) had the non-germinal center B-cell (non-GCB) subtype. At the time of diagnosis, serum lactate dehydrogenase levels were elevated above the normal range in 37 patients (41.57%). Additionally, 11 patients (12.36%) exhibited B symptoms associated with lymphoma. According to Eastern Cooperative Oncology Group (ECOG) performance status score, nine patients (10.11%) had a score of 0, 74 patients (83.15%) had a score of 1, and six patients (6.74%) had a score of 2. Based on the National Comprehensive Cancer Network International Prognostic Index (NCCN-IPI), 25 patients (28.09%) were classified as low-risk, 52 (58.43%) as low-intermediate-risk, and 12 (13.48%) as intermediate-high-risk. The median follow-up duration was 32 months (range, 7–84 months).
Relationships of the TME with Clinicopathological Features
Optimal cutoff values were determined by receiver operating characteristic curve analysis, and patients were categorized into low-expression (low) and high-expression (high) groups based on the threshold. Among the 89 patients, 33 (37.08%) exhibited high CD3 expression, whereas 56 (62.92%) exhibited low CD3 expression. Patients in the high CD3 expression group had significantly lower Ki-67 expression levels (P=0.035). Notably, the inverse relationship between CD3 expression and Ki-67 proliferation index (P=0.035) reveals a previously underreported link between T-cell infiltration and tumor growth dynamics in DLBCL. In total, 36 patients (40.45%) showed high CD8 expression; 53 patients (59.55%) showed low CD8 expression. No statistically significant differences in clinicopathological features were observed between these groups. High FOXP3 expression was observed in 37 patients (41.57%), whereas 52 (58.43%) exhibited low expression. Patients in the high FOXP3 expression group had significantly lower ECOG scores (P=0.046), the association suggests immunomodulatory effects on patient functional status. Furthermore, 53 patients (59.55%) displayed high CD163 expression and 36 patients (40.45%) displayed low expression. Statistically significant differences between these groups were observed regarding NCCN-IPI score (P=0.003), NCCN-IPI risk stratification (P=0.004), cell of origin classification (P=0.020), and ECOG score (P=0.044) (Table 1 and Figures 1, S1).
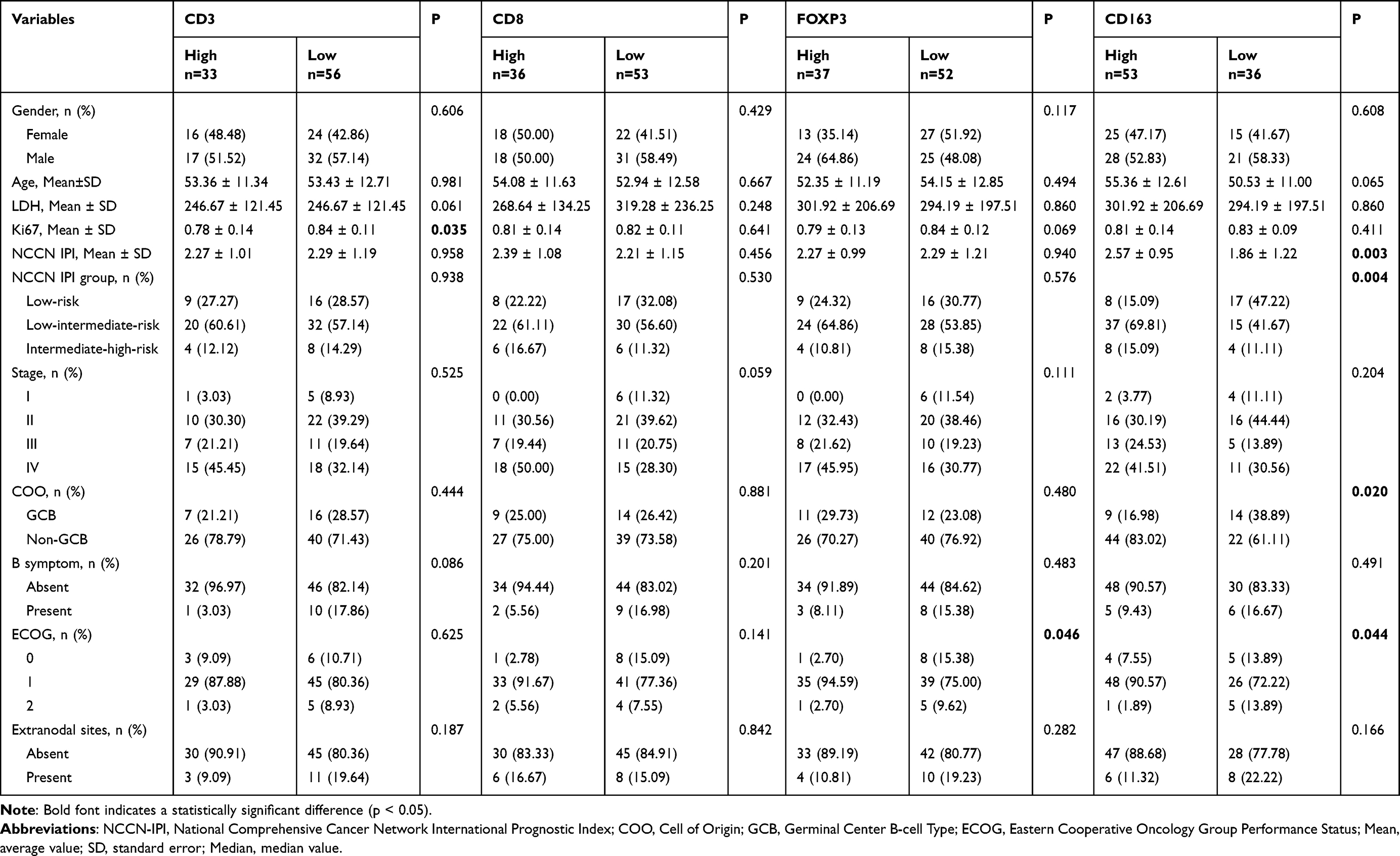 |
Table 1 Association Between Tumor Microenvironment (TME) Expression Profile and Clinical Pathological Factors in Diffuse Large B-Cell Lymphoma (DLBCL) |
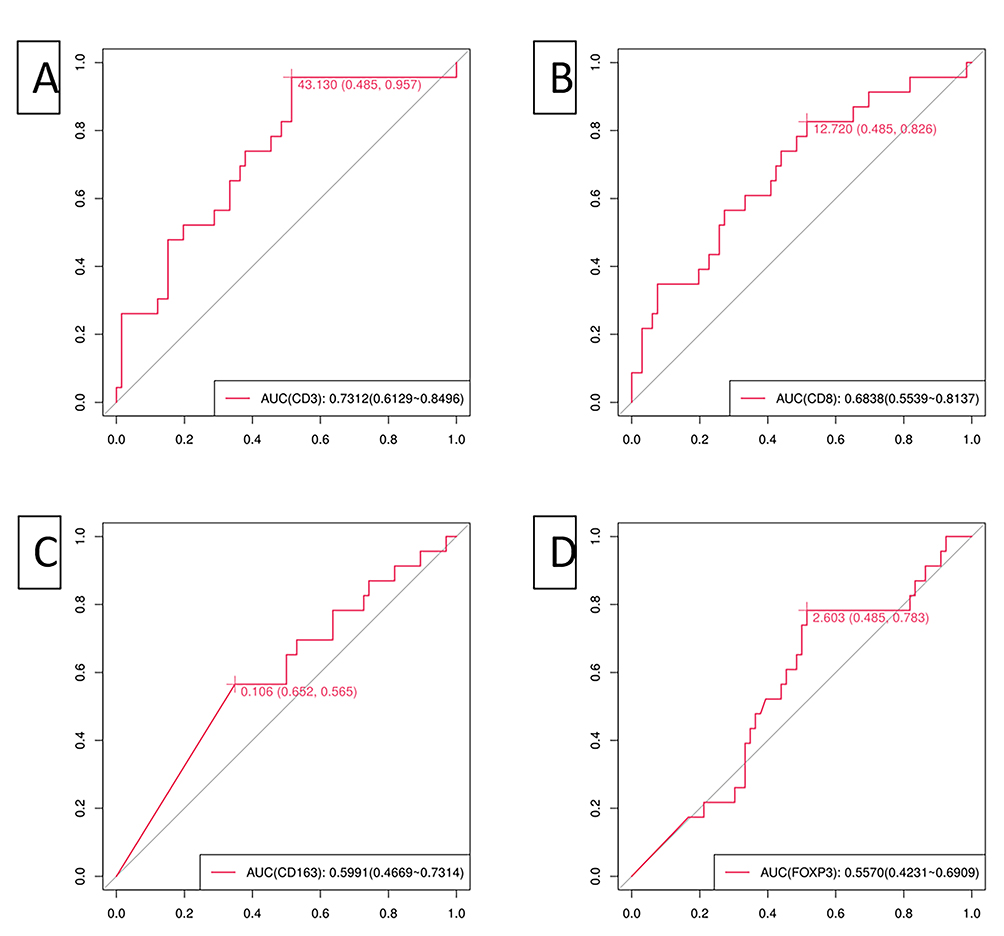 |
Figure 1 Receiver operating characteristic (ROC) curves of the ratio of tumor-infiltrating T-lymphocytes (TIL-T) and tumor-associated macrophages (TAMs): CD3 (A), CD8 (B), CD163 (C), and FOXP3 (D). |
Relationships of PD-L1 Expression with Clinicopathological Features in the TME Context
The expression levels of nPD-L1 and mPD-L1 were assessed; their associations with clinicopathological features and the TME were analyzed. Among the 89 patients, 37 (41.57%) displayed nPD-L1 positivity. nPD-L1 positivity was significantly associated with CD3+ T-cell infiltration (P=0.019), CD163+ macrophage infiltration (P<0.001), and NCCN-IPI risk stratification (P=0.021), especially patients with low-intermediate-risk. In total, 56 patients (62.92%) showed mPD-L1 positivity. Of particular novelty, mPD-L1 positivity was significantly associated with age (P=0.026), ECOG score (P=0.005), B symptoms (P=0.023), CD3+ T-cell infiltration (P=0.005), CD8+ T-cell infiltration (P=0.017), FOXP3+ T-cell infiltration (P=0.036), and CD163+ TAM infiltration (P<0.001). This comprehensive interplay positions mPD-L1 as a central regulator in DLBCL biology (Table 2 and Figure S2).
 |
Table 2 Association of PD-L1 Expression with Clinicopathological Factors and Tumor Microenvironment (TME) in Diffuse Large B-Cell Lymphoma (DLBCL) |
Differences in TME Composition and PD-L1 Expression Between GCB-Type and Non-GCB-Type DLBCL
Comparison of TME composition between GCB and non-GCB subtypes of DLBCL revealed that CD163+ TAMs were significantly more abundant in the non-GCB subtype than in the GCB subtype (P=0.020). No statistically significant differences were observed between the two subtypes regarding the ratio of TIL-T cells or the expression levels of nPD-L1 and mPD-L1 (Table 3). The results highlight subtype-specific macrophage biology as a key differentiator, potentially explaining the aggressive phenotype of non-GCB tumors.
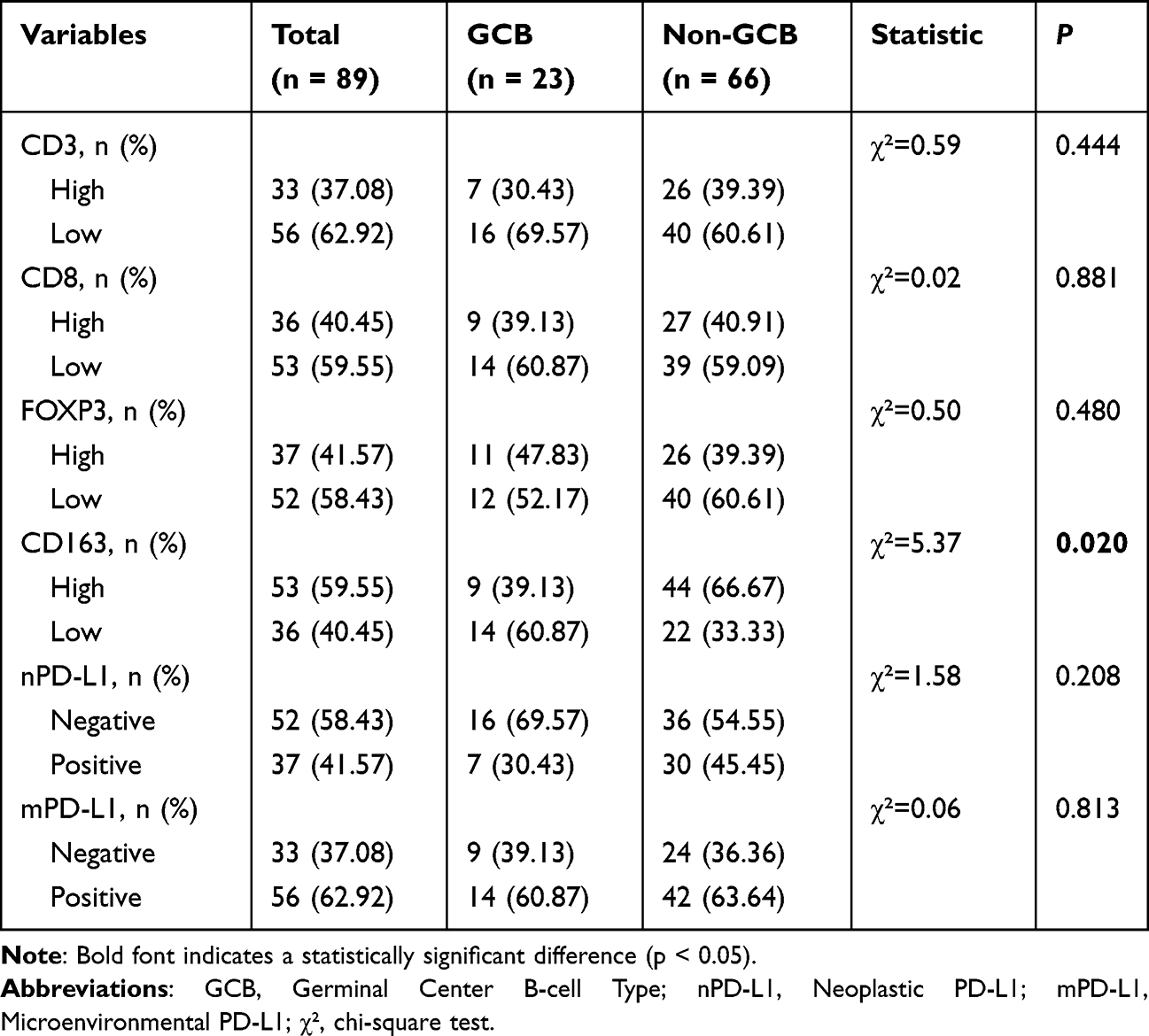 |
Table 3 Analysis of Tumor Microenvironment (TME) and PD-L1 Expression in Tumor-Cells versus Microenvironmental-Cells Between Germinal Center B-Cell Type (GCB) and Non-GCB Diffuse Large B-Cell Lymphoma (DLBCL) |
Relationships of the TME with PD-L1 Expression and Survival
Kaplan–Meier survival analysis showed that patients in the groups with low infiltration of CD3+ T cells (P<0.001), CD8+ T cells (P=0.016), FOXP3+ T cells (P=0.021), and CD163+ TAMs (P=0.047) had significantly shorter OS. Additionally, patients in the group with low CD3+ T-cell infiltration (P<0.001) exhibited worse PFS. Patients in the mPD-L1-negative group exhibited significantly worse PFS (P=0.008) and shorter OS (P=0.035) (Figures 2 and 3). According to univariate Cox regression analysis, shorter OS was significantly associated with the presence of B symptoms (P<0.001), extranodal involvement (P=0.039), low CD3 expression (P=0.006), low CD8 expression (P=0.024), and low FOXP3 expression (P=0.029). In contrast, longer OS was significantly associated with ECOG score 0 (P=0.041) and mPD-L1 positivity (P=0.042). Shorter PFS was significantly associated with the presence of B symptoms (P<0.001) and low CD3 expression (P=0.002), whereas longer PFS was significantly associated with nPD-L1 positivity (P=0.011). Subsequent multivariate Cox regression analysis revealed that B symptoms (P=0.005), extranodal involvement (P=0.022), and CD3+ T-cell infiltration (P=0.026) were independent prognostic factors for OS. Moreover, B symptoms (P=0.008) and CD3+ T-cell infiltration (P=0.022) were identified as independent prognostic factors for PFS (Table 4). Critically, multivariate analysis identified CD3+ T-cell infiltration as an independent prognostic factor for both OS (P=0.026) and PFS (P=0.022)–a finding reinforced by its consistent survival benefits across Kaplan-Meier curves (OS/PFS both P<0.001). This establishes stromal CD3+ T-cells as a novel, stand-alone biomarker eclipsing conventional PD-L1 metrics in prognostic power.
 |
Table 4 Prognostic Factor Analysis in Diffuse Large B-Cell Lymphoma (DLBCL) Using Univariate and Multivariate COX Proportional Risk Regression Modeling |
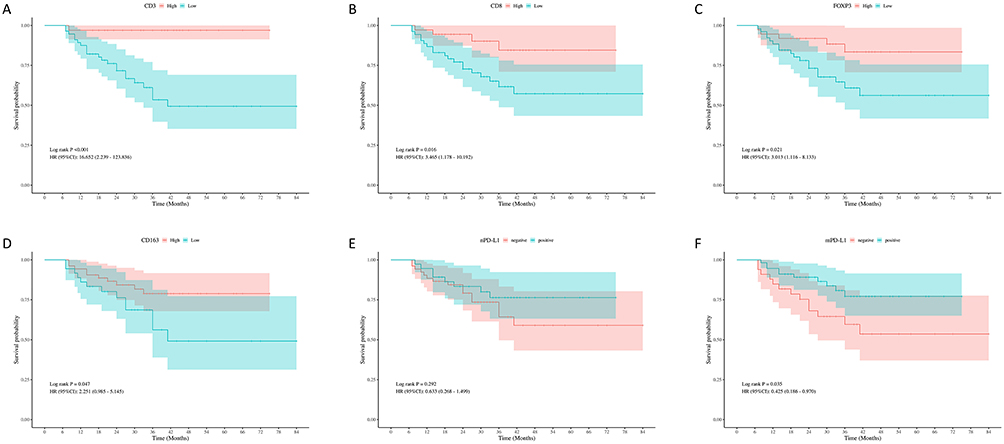 |
Figure 2 Kaplan-Meier survival analysis of tumor microenvironment (TME) characteristics, PD-L1 expression status, and overall survival (OS) outcomes: CD3 (A), CD8 (B), FOXP3 (C), CD163 (D), Neoplastic PD-L1 (nPD-L1) (E), Microenvironmental PD-L1 (mPD-L1) (F). |
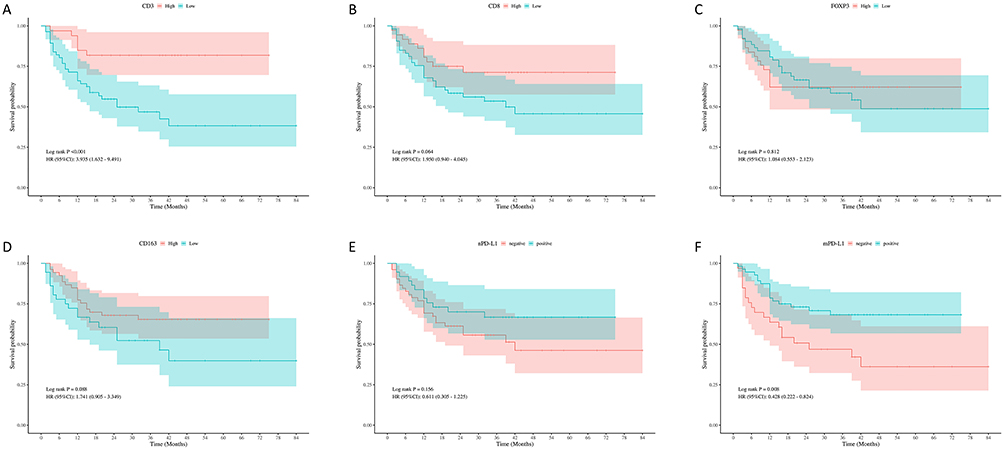 |
Figure 3 Kaplan-Meier survival analysis of tumor microenvironment (TME) characteristics, PD-L1 expression status, and progression-free survival (PFS) outcomes:CD3 (A), CD8 (B), FOXP3 (C), CD163 (D), Neoplastic PD-L1 (nPD-L1) (E), Microenvironmental PD-L1 (mPD-L1) (F). |
Discussion
In this study, we demonstrate that high infiltration of CD3+, CD8+, and FOXP3+ TIL-T and CD163+ TAMs within the TME independently predicts improved survival in DLBCL patients. Critically, PD-L1 expression—particularly in mPD-L1—correlates with favorable clinical features and prolonged PFS/OS, positioning it as a promising prognostic biomarker. These findings, validated through standardized digital pathology in a Chinese cohort, establish the TME’s clinical relevance for DLBCL risk stratification.
DLBCL, the most prevalent subtype of non-Hodgkin lymphoma, is characterized by pronounced clinical aggressiveness and substantial biological heterogeneity. In clinical practice, lymphoma prognosis is primarily evaluated based on clinical symptoms, disease classification, and cellular origin. However, the role of the TME is often overlooked in this assessment. Immune checkpoints and the TME have remained central to numerous oncological investigations. The TME plays a crucial role in the biological behavior of DLBCL; it consists of various immune cells, stromal cells, blood vessels, extracellular matrix components, cytokines, and chemokines. Consequently, the TME strongly influences tumor initiation and progression.3,5,9,10 In DLBCL, the TME is predominantly characterized by TIL-T and TAMs, which are significantly associated with patient survival. Additionally, the PD-1/PD-L1 immune checkpoint serves as a critical mechanism for evading immune surveillance.4 In this study, we conducted a retrospective analysis of DLBCL in Chinese patients to evaluate its impact on prognosis, in conjunction with PD-L1 expression levels and associated clinicopathological features.
TIL-T play a pivotal role in tumor immune mechanisms and function as key effector cells in tumor immunotherapy. They are regarded as important immunobiological markers in various solid tumors.5 Published studies have used markers such as CD3, CD8, and FOXP3 to investigate the effects of TIL-T in different solid tumors on patient survival,11–13 including melanoma, colorectal cancer, gastric cancer and hepatocellular cancer. The results showed that the percentage of TIL-T is significantly associated with patient prognosis. Lately, emerging evidence also underscores the prognostic relevance of TIL-T in lymphoma. Song et al demonstrated that a lower percentage of TIL-T in the TME of patients with DLBCL was associated with shorter survival.14
In our analysis of the relationship between CD3+ T-cell infiltration and clinicopathological factors, we noted that patients with low CD3+ T-cell infiltration exhibited a high Ki-67 proliferation index. This finding is consistent with results reported by Han et al.15 Additionally, our survival analysis revealed that high CD3+ T-cell infiltration was a favorable prognostic factor independently associated with patient outcomes, similar to findings from previous studies.2,15 Therefore, the assessment of CD3+ T-cell infiltration may serve as a prognostic indicator for patients with DLBCL.
As central effector cells in anti-tumor immune responses, CD8+ cytotoxic T lymphocytes play an important role in the prognostic assessment of various malignant tumors through their immune surveillance function. There is evidence that the extent of CD8+ T-cell infiltration within the TME is positively associated with improved prognosis in patients with DLBCL.1,16,17 This finding was confirmed in our study, where high CD8+ TIL-T infiltration was significantly associated with prolonged OS and PFS. These results provide a novel foundation for the identification and selection of immunotherapy targets in patients with DLBCL.
Regulatory T cells (Tregs), a key cell population involved in maintaining immune homeostasis, mediate self-tolerance by specifically suppressing the host’s anti-tumor immune responses and play a crucial regulatory role in the TME.18,19 Molecular biological studies have demonstrated that FOXP3 is a critical transcription factor and an important marker of Tregs; its expression level is closely associated with tumor immune escape mechanisms. Multiple studies have confirmed that high FOXP3+ Treg infiltration is significantly associated with prolonged survival in patients with DLBCL.20–23 This finding aligns with our results, suggesting that FOXP3+ Tregs within the TME of DLBCL influence tumor immune response intensity and clinical outcomes.
In recent years, immune scores have emerged as important prognostic indicators for cancer patients; they have been used to predict outcomes in various solid tumors, such as colorectal cancer and malignant melanoma.24–29 However, no standardized immune scoring system currently exists for lymphoma. In our study, some cases were diagnosed based on biopsy specimens, which precluded accurate determination of tumor cell infiltration at the tumor margin.
This study utilized digital image analysis software to evaluate TIL-T, considerably reducing inter-observer and intra-observer variability. This approach facilitates determination of the optimal cutoff value for TIL-T. However, this study was limited by its retrospective design; the cutoff value used to distinguish high and low TIL-T infiltration was not substantiated. Further validation of the cutoff value and results accuracy with an external cohort is required.
TAMs have been widely recognized for their critical contributions to tumor proliferation, invasion, and metastasis through diverse mechanisms.9 In this study, Kaplan–Meier survival curve analysis demonstrated that patients with high CD163+ TAM infiltration exhibited significantly prolonged OS. In patients with DLBCL receiving the R-CHOP regimen, greater CD163+ TAM infiltration may be positively associated with improved prognosis.30 However, some studies have not replicated this conclusion;31 the discrepancies might be attributed to factors such as heterogeneity in the study population and variability in IHC evaluation criteria. Prospective studies are needed to confirm the clinical utility of these findings.
Additionally, comparison of the TME between GCB and non-GCB subtypes of DLBCL revealed significantly greater CD163+ TAM infiltration in the TME of non-GCB subtype patients. This finding is consistent with the results of a multicenter cohort study by Autio et al, suggesting that this phenomenon contributes to the worse prognosis observed in patients with non-GCB subtype DLBCL relative to patients with the GCB subtype.32
The PD-1/PD-L1 pathway represents a critical mechanism for tumor immune evasion; PD-L1 expression is closely linked to the composition and function of the TME.6 PD-L1 expression in both tumor cells and cells within the TME was evaluated by IHC staining. Based on the morphology and staining results from representative cases, PD-L1-positive cells in the TME were primarily macrophages, consistent with findings reported by Mitteldorf et al.33 However, a methodological limitation of the present study was the absence of double IHC staining to identify specific cell types. Consequently, the possibility of PD-L1 expression in other TME cell populations could not be ruled out.
Our results showed a significant association between nPD-L1 positivity and CD163+ TAM infiltration, which might be attributed to the anti-inflammatory and tumor-promoting functions of CD163+ TAMs. Additionally, mPD-L1 positivity was significantly associated with patient age, presence of B symptoms, ECOG score, and the infiltration of various microenvironmental cells, including CD3+, CD8+, and FOXP3+ TIL-T, as well as CD163+ TAMs. Furthermore, Kaplan–Meier survival curve analysis and univariate Cox regression analysis revealed that mPD-L1 positivity was significantly associated with prolonged PFS and OS. Based on these findings, PD-L1 is expected to serve as a promising biomarker for assessing disease status and prognosis in patients with DLBCL. High PD-L1 expression has been associated with prolonged PFS in patients with DLBCL; it may also indicate a better response to chemotherapy.34,35 However, a study by Kwon et al, which examined PD-L1 immunostaining in 126 patients with DLBCL, revealed that high PD-L1 expression in both tumor cells and microenvironmental cells was significantly associated with the presence of B symptoms, although PD-L1 expression lacked prognostic significance.36 Another study demonstrated that patients with PD-L1 negativity exhibit significantly higher survival rates than those with PD-L1 positivity.17 Explanations for these diverse analytical results may include: 1) methodological differences in IHC staining, such as variations in automated staining platforms, antibody clone numbers, and standardized operating procedures, which can introduce data abnormalities; 2) inconsistent criteria for defining immune marker positivity, leading to heterogeneity in the results; and 3) the relatively limited sample size in this study, which may have contributed to variations in the final outcomes.
This study has limitations. Primarily, as a retrospective analysis, detailed standardized treatment information (eg, specific first-line and salvage regimens, dose intensity, transplant details, CAR-T therapy) was not systematically available for the entire cohort. While we adjusted for key clinical prognosticators, particularly the IPI score, variations in treatment could represent an unmeasured confounding factor influencing OS outcomes. Future prospective studies should prioritize the standardized collection of comprehensive treatment data. Validation of the prognostic and predictive value of the identified TME biomarkers within more uniformly treated patient cohorts (eg, R-CHOP only) and investigation of their interaction with specific therapies (eg, novel agents, immunotherapy, CAR-T) are important next steps to precisely define their clinical utility.
In conclusion, our data robustly demonstrate that high infiltration of CD3+, CD8+, and FOXP3+ TIL-T and CD163+ TAMs independently predicts improved survival outcomes in DLBCL patients, while validating these associations in a Chinese cohort through standardized digital pathology. Critically, PD-L1 expression in microenvironmental cells correlates with favorable clinical parameters and emerges as a potent prognostic biomarker. These results resolve key methodological inconsistencies in prior TME assessments and establish combinatorial TME signatures as clinically actionable tools for DLBCL risk stratification. Considering the sample size limitations in this study, additional investigations with larger cohorts are required to validate the clinical utility of these parameters in DLBCL and to identify practical new targets for immunotherapy.
Abbreviation
DLBCL, diffuse large B-cell lymphoma; TME, tumor microenvironment; TIL-T, tumor-infiltrating T-lymphocytes; TAMs, tumor-associated macrophages; ECOG, Eastern Cooperative Oncology Group Performance Status; NCCN-IPI, National Comprehensive Cancer Network International Prognostic Index; PD-1, programmed death receptor-1; PD-L1, programmed death-ligand 1; nPD-L1, Neoplastic PD-L1; mPD-L1, Microenvironmental PD-L1; GCB, Germinal Center B-cell type; IHC, immunohistochemistry; OS, overall survival; PFS, progression-free survival; Tregs, Regulatory T cells.
Data Sharing Statement
Data and material are available upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in strict accordance with the Declaration of Helsinki, and written informed consent was obtained from all participants or their legal guardians. The protocol was approved after a comprehensive review by the Institutional Review Board of Fujian Cancer Hospital (K2022-166-01).
Consent for Publication
Consent obtained directly from patients.
Acknowledgments
Yun-Li Xie, Long-Feng Ke and Wen-Wen Zhang are co-first authors for this study and Jian-Chao Wang and Yan-Ping Chen are co-correspondence authors for this study. We thank Ryan Chastain-Gross, Ph.D., from Liwen Bianji (Edanz) (www.liwenbianji.cn/) for editing the English text of a draft of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Joint Funds for the Innovation of Science and Technology, Fujian province (grant no. 2021Y9228 and grant no. 2021Y9215), the Natural Science Foundation of Fujian Province (grant no. 2023Y0058).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rajnai H, Heyning FH, Koens L, et al. The density of CD8+ T-cell infiltration and expression of BCL2 predicts outcome of primary diffuse large B-cell lymphoma of bone. Virchows Arch. 2014;464(2):229–239. doi:10.1007/s00428-013-1519-9
2. Cho Y, Lee J, Han B, et al. Tumor-infiltrating T lymphocytes evaluated using digital image analysis predict the prognosis of patients with diffuse large B-cell lymphoma. J Pathol Transl Med. 2024;58(1):12–21. doi:10.4132/jptm.2023.11.02
3. Autio M, Leivonen SK, Brück O, Karjalainen-Lindsberg ML, Pellinen T, Leppä S. Clinical impact of immune cells and their spatial interactions in diffuse large B-cell lymphoma microenvironment. Clin Cancer Res. 2022;28(4):781–792. doi:10.1158/1078-0432.CCR-21-3140
4. Alame M, Pirel M, Costes-Martineau V, et al. Characterisation of tumour microenvironment and immune checkpoints in primary central nervous system diffuse large B cell lymphomas. Virchows Arch. 2020;476(6):891–902. doi:10.1007/s00428-019-02695-6
5. Autio M, Leivonen SK, Brück O, et al. Immune cell constitution in the tumor microenvironment predicts the outcome in diffuse large B-cell lymphoma. Haematologica. 2021;106(3):718–729. doi:10.3324/haematol.2019.243626
6. Fang X, Xiu B, Yang Z, et al. The expression and clinical relevance of PD-1, PD-L1, and TP63 in patients with diffuse large B-cell lymphoma. Medicine. 2017;96(15):e6398. doi:10.1097/MD.0000000000006398
7. Xu T, Chai J, Wang K, et al. Tumor Immune Microenvironment Components and Checkpoint Molecules in Anaplastic Variant of Diffuse Large B-Cell Lymphoma. Front Oncol. 2021;11:638154. doi:10.3389/fonc.2021.638154
8. Yu J, Jin S, Yin X, Du H. Expression of the immune checkpoint molecules PD-L1 and PD-1 in EBV-associated lymphoproliferative disorders: a meta-analysis. Exp Ther Med. 2023;27(1):7. doi:10.3892/etm.2023.12294
9. Pollari M, Leivonen SK, Leppä S. Testicular Diffuse Large B-Cell Lymphoma-Clinical, Molecular, and Immunological Features. Cancers. 2021;13(16):4049. doi:10.3390/cancers13164049
10. Roussel M, Le KS, Granier C, et al. Functional characterization of PD1+TIM3+ tumor-infiltrating T cells in DLBCL and effects of PD1 or TIM3 blockade. Blood Adv. 2021;5(7):1816–1829. doi:10.1182/bloodadvances.2020003080
11. Brummel K, Eerkens AL, de Bruyn M, Nijman HW. Tumour-infiltrating lymphocytes: from prognosis to treatment selection. Br J Cancer. 2023;128(3):451–458. doi:10.1038/s41416-022-02119-4
12. Kimura S, Oshiro Y, Iwasaki H, et al. Programmed cell death-ligand 1 (PD-L1)+ tumour cells and low-reacting programmed cell death 1 (PD1)+ tumour-infiltrating lymphocytes predict poor prognosis in Epstein-Barr virus+ diffuse large B-cell lymphoma. Clin Exp Med. 2022;22(3):411–419. doi:10.1007/s10238-021-00754-4
13. Tay C, Tanaka A, Sakaguchi S. Tumor-infiltrating regulatory T cells as targets of cancer immunotherapy. Cancer Cell. 2023;41(3):450–465. doi:10.1016/j.ccell.2023.02.014
14. Song JY, Nwangwu M, He TF, et al. Low T-cell proportion in the tumor microenvironment is associated with immune escape and poor survival in diffuse large B-cell lymphoma. Haematologica. 2023;108(8):2167–2177. doi:10.3324/haematol.2022.282265
15. Han B, Yim J, Lim S, et al. Prognostic impact of the immunoscore based on whole-slide image analysis of CD3+ tumor-infiltrating lymphocytes in diffuse large B-cell lymphoma. Mod Pathol. 2023;36(9):100224. doi:10.1016/j.modpat.2023.100224
16. Kim S, Nam SJ, Park C, et al. High tumoral PD-L1 expression and low PD-1+ or CD8+ tumor-infiltrating lymphocytes are predictive of a poor prognosis in primary diffuse large B-cell lymphoma of the central nervous system. Oncoimmunology. 2019;8(9):e1626653. doi:10.1080/2162402X.2019.1626653
17. Xu-Monette ZY, Xiao M, Au Q, et al. Immune profiling and quantitative analysis decipher the clinical role of immune-checkpoint expression in the tumor immune microenvironment of DLBCL. Cancer Immunol Res. 2019;7(4):644–657. doi:10.1158/2326-6066.CIR-18-0439
18. Pollari M, Pellinen T, Karjalainen-Lindsberg ML, Kellokumpu-Lehtinen PL, Leivonen SK, Leppä S. Adverse prognostic impact of regulatory T-cells in testicular diffuse large B-cell lymphoma. Eur J Haematol. 2020;105(6):712–721. doi:10.1111/ejh.13484
19. Carreras J, Lopez-Guillermo A, Fox BC, et al. High numbers of tumor-infiltrating FOXP3-positive regulatory T cells are associated with improved overall survival in follicular lymphoma. Blood. 2006;108(9):2957–2964. doi:10.1182/blood-2006-04-018218
20. Coutinho R, Clear AJ, Mazzola E, et al. Revisiting the immune microenvironment of diffuse large B-cell lymphoma using a tissue microarray and immunohistochemistry: robust semi-automated analysis reveals CD3 and FoxP3 as potential predictors of response to R-CHOP. Haematologica. 2015;100(3):363–369. doi:10.3324/haematol.2014.110189
21. Tzankov A, Meier C, Hirschmann P, Went P, Pileri SA, Dirnhofer S. Correlation of high numbers of intratumoral FOXP3+ regulatory T cells with improved survival in germinal center-like diffuse large B-cell lymphoma, follicular lymphoma and classical Hodgkin’s lymphoma. Haematologica. 2008;93(2):193–200. doi:10.3324/haematol.11702
22. Menter T, Bodmer-Haecki A, Dirnhofer S, Tzankov A. Evaluation of the diagnostic and prognostic value of PDL1 expression in Hodgkin and B-cell lymphomas. Hum Pathol. 2016;54:17–24. doi:10.1016/j.humpath.2016.03.005
23. Lee NR, Song EK, Jang KY, et al. Prognostic impact of tumor infiltrating FOXP3 positive regulatory T cells in diffuse large B-cell lymphoma at diagnosis. Leuk Lymphoma. 2008;49(2):247–256. doi:10.1080/10428190701824536
24. Bruni D, Angell HK, Galon J. The immune contexture and Immunoscore in cancer prognosis and therapeutic efficacy. Nat Rev Cancer. 2020;20(11):662–680. doi:10.1038/s41568-020-0285-7
25. Galon J, Mlecnik B, Bindea G, et al. Towards the introduction of the ‘Immunoscore’ in the classification of malignant tumours. J Pathol. 2014;232(2):199–209. doi:10.1002/path.4287
26. Galon J, Lugli A, Bifulco C, et al. World-wide immunoscore task force: meeting report from the “Melanoma Bridge”, Napoli, November 30th-December 3rd, 2016. J Transl Med. 2017;15(1):212. doi:10.1186/s12967-017-1310-9
27. Kirilovsky A, Marliot F, El Sissy C, Haicheur N, Galon J, Pagès F. Rational bases for the use of the Immunoscore in routine clinical settings as a prognostic and predictive biomarker in cancer patients. Int Immunol. 2016;28(8):373–382. doi:10.1093/intimm/dxw021
28. Galon J, Fox BA, Bifulco CB, et al. Immunoscore and immunoprofiling in cancer: an update from the melanoma and immunotherapy bridge 2015. J Transl Med. 2016;14:273. doi:10.1186/s12967-016-1029-z
29. Galon J, Costes A, Sanchez-Cabo F, et al. Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science. 2006;313(5795):1960–1964. doi:10.1126/science.1129139
30. Riihijärvi S, Fiskvik I, Taskinen M, et al. Prognostic influence of macrophages in patients with diffuse large B-cell lymphoma: a correlative study from a Nordic Phase II trial. Haematologica. 2015;100(2):238–245. doi:10.3324/haematol.2014.113472
31. Cencini E, Fabbri A, Schiattone L, et al. Prognostic impact of tumor-associated macrophages, lymphocyte-to-monocyte and neutrophil-to-lymphocyte ratio in diffuse large B-cell lymphoma. Am J Blood Res. 2020;10(4):97–108.
32. Autio M, Brück O, Pollari M, et al. Characterization of tumor microenvironment and cell interaction patterns in testicular and diffuse large B-cell lymphomas. Haematologica. 2024;110(6):1339. doi:10.3324/haematol.2024.286267
33. Mitteldorf C, Berisha A, Pfaltz MC, et al. Tumor microenvironment and checkpoint molecules in primary cutaneous diffuse large B-cell lymphoma-new therapeutic targets. Am J Surg Pathol. 2017;41(7):998–1004. doi:10.1097/PAS.0000000000000851
34. Shi Y, Deng L, Song Y, et al. CD3+/CD8+ T-cell density and tumoral PD-L1 predict survival irrespective of rituximab treatment in Chinese diffuse large B-cell lymphoma patients. Int J Hematol. 2018;108(3):254–266. doi:10.1007/s12185-018-2466-7
35. Four M, Cacheux V, Tempier A, et al. PD1 and PDL1 expression in primary central nervous system diffuse large B-cell lymphoma are frequent and expression of PD1 predicts poor survival. Hematol Oncol. 2017;35(4):487–496. doi:10.1002/hon.2375
36. Kwon D, Kim S, Kim PJ, et al. Clinicopathological analysis of programmed cell death 1 and programmed cell death ligand 1 expression in the tumour microenvironments of diffuse large B cell lymphomas. Histopathology. 2016;68(7):1079–1089. doi:10.1111/his.12882
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prussian Blue Nanoparticle-Induced Alteration of the Polarization State of Tumor-Associated Macrophages as a Substantial Antitumor Mechanism Against Oral Squamous Cell Carcinoma (OSCC)

Zhang Z, Sun X, Gao Z, Lv X, Jia H, Huang B, Xia C, Yang X
International Journal of Nanomedicine 2025, 20:10667-10681
Published Date: 31 August 2025
DNA Methylation in Lung Cancer: Predictive Biomarkers for Effective Immunotherapy
Kumari K, Kumar V, Verma C, Hsu PC, Singh A
International Journal of General Medicine 2025, 18:7893-7910
Published Date: 31 December 2025
Integrative Single-Cell and Spatial Transcriptomic Analysis Reveals MAIT Cell Dysfunction in Relapsed HCC
Park GW, Jang H, Nguyen-Phuong T, Nam H, Park CG, Choi GH, Jeong S, Kim J, Yoon CJ, Lee JH, Kim HJ
Journal of Hepatocellular Carcinoma 2026, 13:575861
Published Date: 2 February 2026