Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
Complementary And Alternative Medicine Practitioner’s Management Of Acute Respiratory Tract Infections In Children – A Qualitative Descriptive Study
Authors Lucas S ![]() , Leach MJ
, Leach MJ ![]() , Kumar S
, Kumar S ![]() , Phillips AC
, Phillips AC ![]()
Received 12 September 2019
Accepted for publication 29 October 2019
Published 20 November 2019 Volume 2019:12 Pages 947—962
DOI https://doi.org/10.2147/JMDH.S230845
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sandra Lucas,1 Matthew J Leach,2 Saravana Kumar,1 Anna C Phillips1
1School of Health Sciences, Division of Health Sciences, University of South Australia, Adelaide, SA, Australia; 2Department of Rural Health, University of South Australia, Adelaide, SA, Australia
Correspondence: Sandra Lucas
School of Health Sciences, Division of Health Sciences, University of South Australia, North Tce, Adelaide, SA, Australia
Tel +61 4 8890 1240
Fax +61 8 8302 2853
Email [email protected]
Background: Acute respiratory tract infection (ARTI) is one of the most prevalent types of infection among children and a common reason for hospital admission. Although parents frequently consult complementary and alternative medicine (CAM) practitioners to assist with the management of childhood ARTI, little is known about the treatments that CAM practitioners recommend and why. The aim of this research was to understand what CAM practitioners typically prescribe for the management of childhood ARTI and how practitioners formulate decisions regarding the management of this condition.
Method: The research was guided by a qualitative descriptive framework. CAM practitioners across Greater Melbourne (Victoria, Australia) who had treated children aged 0–12 years with ARTI in the past 12 months were eligible to participate. Data were captured using semi-structured interviews, which were audio-recorded and transcribed verbatim. Multiple strategies to improve trustworthiness were implemented (e.g., triangulation of data). Data were analysed using inductive content analysis.
Results: Twenty-four CAM practitioners from ten different disciplines participated in the interviews. Most participants were female (75%), and more than half (54%) were practicing naturopaths. The treatments most commonly recommended were lifestyle modification (95%), nutrition/diet-based treatments (91%), and vitamin/mineral supplementation (87%). Practitioners’ decision-making process was underpinned by four key concepts namely: the approach to management, individualisation, do no harm, and collaborative practice. Individualisation and the safety of the child are cornerstones of treatment in the practitioner’s decision-making process.
Conclusion: This research sheds light on commonly used CAM interventions, many of which build on easily accessible and readily available treatments (such as soups) and are aligned with mainstream recommendations (such as rest). Practitioners’ decision-making process too aligns well with mainstream health care where the focus is on safety and informed by a biopsychosocial-cultural approach.
Keywords: traditional complementary integrated medicine, decision-making, paediatric, qualitative descriptive, respiratory infection, health personal
Background
Acute respiratory tract infections (ARTI) are the leading cause of mortality and morbidity worldwide.1 Nearly 2.38 million deaths globally resulted from lower respiratory tract infections in 2016, making lower respiratory tract infections the leading cause of death among children younger than 5 years.2 Respiratory tract infections are also the most common reason for childhood admission to hospital, with 20% of the admissions in the US related to ARTI.3 Additionally, ARTI is the most common reason for parents visiting a general health practitioner in the US, Australia and United Kingdom.4–7
The term ARTI refers to any short-term infectious illness involving the upper and/or lower respiratory system. Infections typically manifest with symptoms of cough, sore throat, fever, blocked nose, and/or infant feeding problems. Conditions captured under the umbrella term of ARTI include coughs and colds (also known as common cold, coryza, acute nasopharyngitis, acute pharyngorhinitis),8 laryngitis, pharyngitis/tonsillitis, acute rhinitis, acute rhinosinusitis, acute otitis media, pneumonia, bronchitis, and bronchiolitis.4,9 These conditions are not only unpleasant and disruptive, they can also impair future functional capacity.10
As well as the physical implications of acute respiratory tract infection, ARTI has significant socioeconomic consequences. According to the World Health Organization, respiratory tract infections are the most important global human health problem due to the high level of disease burden – this can be attributed to both the high incidence, and substantial economic, social, and treatment costs of the condition.8 For instance, childhood ARTI can impact both the family and workplace, resulting in parental stress, lost productivity, social disruption, work absenteeism, and increased use of healthcare services.11,12 When parental time off work is added to the costs of health care, acute respiratory tract infections pose a significant financial burden to the global community.13–16
The prompt and effective treatment of acute respiratory tract infection is critical to reducing a child’s suffering and avoiding potential complications, such as otitis media, sinusitis, or pneumonia.17 In most cases, the primary focus of ARTI treatment is symptomatic relief.18 While ARTI is typically managed using pharmaceutical interventions, such as antipyretic, analgesic,19,20 and antitussive agents,21 the evidence of effectiveness of these treatments remains inconclusive.22 Accordingly, there have been calls to avoid the use of these agents in ARTI, particularly in children.21 There are further concerns regarding the safety of pharmaceutical cough and cold medicines, with an estimated 1519 children under 2 years of age treated in US hospital emergency departments in 2004–2005 for adverse events associated with these treatments.23,24
In the majority of cases, childhood ARTI is managed by parents in the home.25 In some situations, this includes the use of complementary and alternative medicines and therapies (CAM). CAM refers to a group of systems and practices considered outside the domain of conventional medicine, which are used to prevent or treat illness and/or to promote health and well-being.26 While the evidence supporting the effectiveness of CAM for ARTI is limited, there is an emerging evidence base for some interventions. In one double-blind randomised active-controlled trial, garlic powder tablets were found to be significantly more effective than benzimidazole (an anti-infective agent) in preventing acute respiratory disease in children (i.e., aged 7–16 years).27 Similarly, positive findings have been reported in two systematic reviews examining the effectiveness of Ivy Leaf (Hedera Helix)28 and elderberry and elderflower (Sambucus nigra)29 for the treatment of ARTI.
As the popularity of and the evidence base underpinning CAM continues to grow, CAM may have a role to play in the management of childhood ARTI. However, current knowledge gaps persist in terms of what CAM practitioners are prescribing and/or recommending for the management of ARTI in children, and how they make these decisions – particularly in Australia.30 This research aimed to address this knowledge gap.
Methodology
Research Aims And Questions
This research set out to answer the following research questions:
- What CAM interventions are used by CAM practitioners for the treatment and prevention of ARTI in children aged between 0 and 12 years?
- How do CAM practitioners formulate decisions regarding the management of ARTI in children?
Research Design
A pragmatic theoretical framework31–33 underpins this research, which is described as a worldwide view that arises out of action, situation, and consequences.32 This framework
recognises that there are many different ways of interpreting the world and undertaking research, that no single point of view can ever give the entire picture and that there may be multiple realities.34
This research framework serves to further understanding of CAM practitioners’ treatment of ARTI.
The research was guided by a qualitative descriptive (QD) framework.35 The QD framework enables the production of well-grounded, rich descriptions and explanations of processes within an identifiable local context36 and unique as the main objective is to obtain an accurate portrayal of people’s characteristics, traits and behaviours in ordinary language.35,37,38 QD framework also focusses on the data with minimal interpretation. The COREQ (consolidated criteria for reporting qualitative research) checklist was used to guide the design and reporting of this research.39
Participant Selection/Sampling
Participants were recruited using maximum variation sampling (to capture the views of a diverse group of CAM practitioners)35 and snowball sampling (to facilitate the recruitment of participants).40 While there was no pre-determined sample size, it was anticipated that approximately 20 practitioners would be recruited based on the sample sizes reported in similar research.41,42 The final sample size was determined when data collection garnered no new information.35,38 Practitioners eligible for inclusion were acupuncturists, anthroposophic practitioners, ayurvedic practitioners, chiropractors, naturopaths, nutritionists, osteopaths, and traditional Chinese medicine practitioners. The rationale for the selection of these specific disciples was based on the findings from a previous research which identified these were the practitioner’s parents utilised for ARTI in their children.43 Participants were located in the Greater Melbourne area (Victoria, Australia), and had treated a child aged 0–12 years with ARTI within the last 12 months. Participants who were not able to speak or understand English or were unable to provide informed consent were excluded.
Recruitment
A Facebook page and recruitment flyer were generated to promote the research to potential participants. The Facebook page provided general information about the research and contact details of the lead researcher (SL). Links to this page were shared on other relevant Facebook groups and pages. Recruitment flyers were posted on the Facebook page and circulated electronically to CAM colleges and associations in Melbourne and Victoria, via electronic newsletters and/or membership email blasts. All recruitment material invited potential participants to contact the researcher either via email or private message (on the Facebook page) (Figure 1). Additionally, some research participants identified other potential practitioners that were also invited to participate via direct email or telephone.
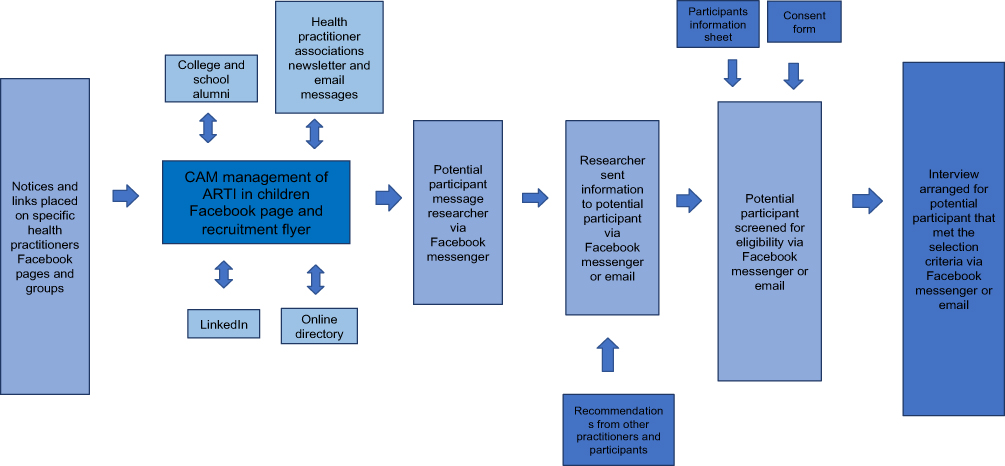 |
Figure 1 Schematic of process used to identify and recruit participants. |
Data Collection
Data were collected through face-to-face interviews. A 19-item in three sections, semi-structured interview agenda was developed informed by findings from a recent systematic review30 and previous qualitative research conducted.43 The interview agenda was pilot tested prior to undertaking the interviews, with four CAM practitioners. Feedback was sought regarding the timing, clarity, flow, conciseness, comprehensiveness, and relevance of questions. Minor changes were made to the interview agenda following the pilot testing, including the rewording of some questions, and the provision of a clear explanation of the terms ARTI and CAM at the beginning of the interview. The final interview agenda comprised six demographic questions, six closed-ended items on practitioner prescribing behaviour, and seven open-ended items on practitioner-prescribed treatments, prevention strategies, and parent decision-making (Appendix 1).
All interviews were conducted by the lead researcher (SL) between May and August 2018. The time and location (i.e., home, café, workplace) of the interviews were negotiated for each participant. Field notes were taken during and immediately after the interviews to assist in confirming the accuracy of the interview transcripts and to aid data interpretation; however, these notes were not included in the data analysis. All interviews were audiotaped using a digital voice recorder and transcribed verbatim by the lead researcher (SL) and RevTM transcription service. All transcriptions were checked for accuracy by the lead researcher. Due to time restraints and limited availability of participants, repeat interviews and cross-checking of transcripts were not able to be completed.
Data Analysis
Data were managed through NVivoTM software (version 10) and analysed using inductive content analysis.44 The inductive content analysis comprised three-stages: (1) preparation (immersing in the data and obtaining a sense of the whole; selecting the unit of analysis; deciding on the analysis of manifest content or latent content), (2) organisation (using open coding to create categories, grouping codes under higher order headings, and formulating a general description of the research topic through the generation of categories and subcategories), and (3) reporting (presenting the results utilising models, such as mind maps).44–46 Rigour was maintained by establishing credibility of the results (i.e., three researchers [SL, ML, AP] were involved in the coding of data), transferability (i.e., providing a thick description of the methods, data collection and analysis), dependability (i.e., triangulating the interview data with field notes), and confirmability (identifying and managing potential biases).
Role Of Researcher
Given the qualitative nature of this research, it is acknowledged that the lead researcher (SL) may exert some influence on the collection, analysis, and interpretation of data. Thus, it is important that the background of the lead researcher be disclosed. The lead researcher (SL) is a female PhD candidate, a parent, and a registered nurse with experience in the field of CAM and health care. To mitigate the extent to which these experiences influenced participant perspectives and responses before and during the interview, the lead researcher attended formal research training, adhered to the interview agenda, and engaged in regular discussions with other members of the research team (SK, ML, AP). Participants were also informed of the qualifications of the lead researcher and had an opportunity to speak informally with the interviewer prior to scheduling an interview. This ensured that the relationship between researcher and participants was non-personal, non-hierarchical, and non-manipulative.
Ethics And Privacy
Ethics approval was granted by the Human Research Ethics Committee of the University of South Australia (ID: 0000035018). Research participants provided informed written consent prior to participation. A unique identification number and pseudonym were allocated to each participant to maintain participant anonymity.
Terminology
The interviewees used a range of terms when referring to different areas of health care (e.g., allopathic medicine). For ease of interpretation, these terms were classified as either CAM or biomedicine. Captured under the term CAM were a broad and diverse range of therapies, including acupuncture, anthroposophic medicine, aromatherapy, ayurveda, chiropractic, nutritional medicine, energy healing, herbal medicine, homoeopathy, kinesiology, massage, naturopathy, osteopathy, and traditional Chinese medicine. Biomedicine encompassed the terms allopathic medicine, orthodox medicine, conventional medicine, mainstream medicine, general practitioner (GP) and medical specialist (e.g., paediatrician).
Results
Participant Characteristics
Figure 2 outlines the recruitment process, which resulted in a sample of 24 CAM practitioners.
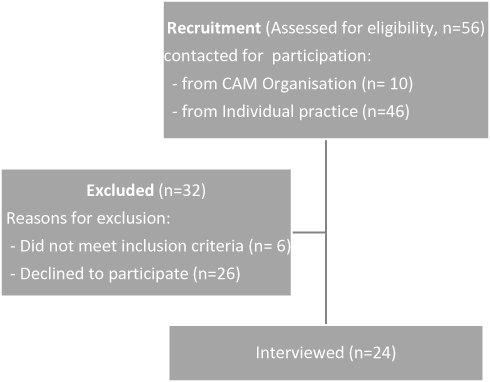 |
Figure 2 Flow chart of recruitment. |
The participants were predominantly female (n=18, 75%), aged 31–60 years (n=24,100%), with a mean age of 43 (SD 6.4) years. Participants spanned nine different CAM disciplines, with more than half (54%) being naturopaths, who worked across private practice, health food stores and pharmacies (Table 1).
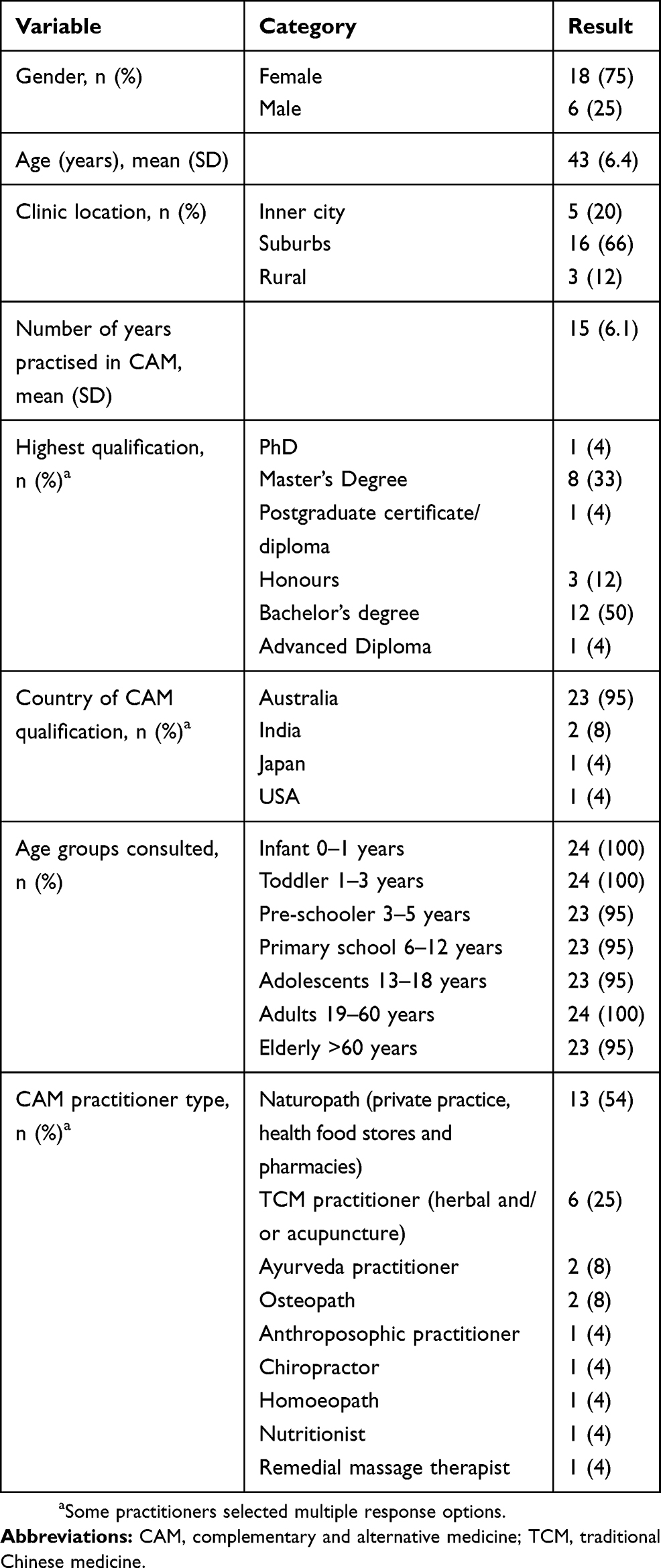 |
Table 1 Demographic Characteristics Of Participants (n=24) |
CAM Intervention That Practitioner Recommend
There were many CAM interventions recommended by practitioners. The interventions were grouped into broad categories. It was customary for practitioners to recommend lifestyle modifications, followed by nutrition and diet-based treatments for the management and prevention of ARTI in children aged between 0 and 12 years. An overview of the broad treatment categories is presented in Table 2.
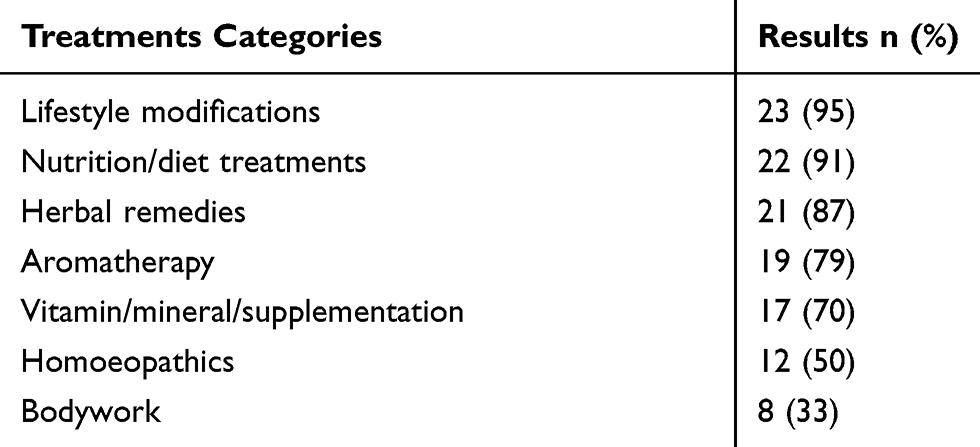 |
Table 2 Recommended By CAM Practitioners For Treatments For ARTI In Children |
There were 135 different CAM remedies recommended for ARTI. The full list of these is available in Appendix 2. The CAM treatments that were most commonly recommended by practitioners were foods as medicine followed by dairy reduction (Table 3).
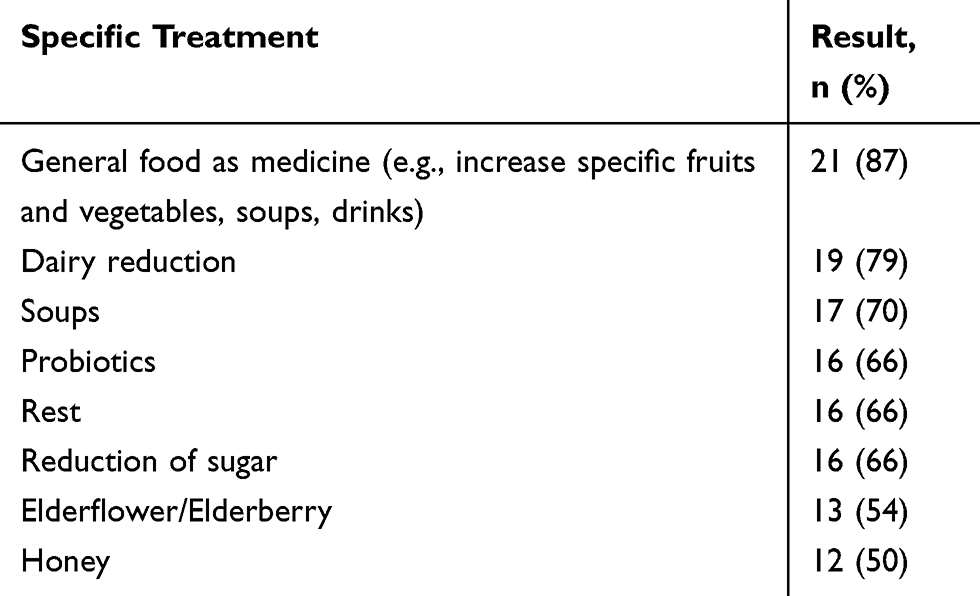 |
Table 3 Specific Treatment By CAM Practitioners For ARTI In Children |
Practitioner Decision-Making
Participants described in detail the many factors that influenced their decision-making regarding the management of ARTI in children. The initial coding of this data generated 71 nodes. These nodes were then grouped into three hierarchical levels: categories (n=4), subcategories (n=11), and elements (n=10). The 4 categories were (1) Approach to management, (2) Individualisation, (3) Do no harm, and (4) Collaborative practice. Figure 3 provides a diagrammatic overview of these.
 |
Figure 3 Diagrammatic overview of four key factors influencing practitioner decision-making regarding the management of ARTI in children. |
Approach To Management
Approach to management incorporates the practitioners’ fundamental principles, in conjunction with tangible treatments for children with ARTI. In this category, three subcategories emerged. This included treatment philosophy, modalities utilised and prevention strategies. The category approach to management is where the similarities and differences to practice came to light from all CAM streams.
Each participant had a core treatment philosophy underpinning their approach to the management of ARTI in children. All participants (n=24, 100%) indicated that their approach to management was guided by a treatment philosophy that formed the foundation for their practice.
For example:
Our underlying philosophy is … . each person is unique, … . But you do have particular periods of development in life that require more attention for certain children, particularly with the UTIs or the upper respiratory tract stuff. Faith
Three key elements emerged in relation to the treatment philosophy, these elements were: the immune system, wholism, and the underlying cause.
The child’s immune system was a central focus for many participants (n=20, 83%) in the management of ARTI. This included supporting, stimulating, or calming down the immune system, where appropriate;
[I use treatments] … to help support the immune system from its core. Grace (Osteopath/nutritionist)
I’m looking at symptomatic relief as well as supporting their immune system always. Odessa (Naturopath)
Some participants (n=11, 45%) articulated that wholism was a key part of their treatment philosophy. In the context of this study, wholism referred to a treatment approach that takes into consideration the impact and interactions between the biopsychosocial-cultural elements of a being, and not just the physical symptoms alone.
We need to always look at the whole of the organism(person/child). Faith (Homoeopath)
But the person comes to me with a sore foot, and we end up talking about their heart anyway, because it’s just holistic. Hailey (Naturopath)
One participant (4%) expressed concerns that biomedicine (general practice) is no longer wholistic,
It’s (biomedicine) probably not as wholistic as it used to be. I think GP’s used to be [wholistic] when I was a child. Grace (Osteopath/nutritionist)
Wholism also included environmental factors impacting on the child’s treatment, which was discussed by half of the participants (n=12, 50%). This was predominantly mentioned when addressing lifestyle factors such as inside and outside the home environment, mould, dust, dirt, and air temperature or quality;
… there will be an environmental component … from overly sterile school environment, home environment or …. where there’s excessive mould or there’s damp issues. Sacha (Naturopath)
There were several participants (n=8, 33%) that directed their approach toward treating the underlying cause of the ARTI. These participants referred to treating the specific symptoms of ARTI in addition to the reasons why the child had become unwell in the first place;
It depends what the underlying cause of the congestion is. Sacha (Naturopath)
If you do have the recurring acute things, it means that there’s something chronic underlying that needs to be sorted. Faith (Homoeopath)
All (n=24, 100%) participants adopted a multi-modal approach, where they discussed using a variety of different modalities in the treatment of children with ARTI. Treatments in this approach included lifestyle modification (n=23, 95%), nutrition and diet-based treatment (n=22, 91%), herbal medicine (n=21, 87%), aromatherapy (n=19, 79%), vitamin/mineral or supplementation (n=17, 70%), homoeopathic medicine (n=12, 50%), and bodywork (n=8, 33%). There was range of treatment modalities prescribed/recommended by participants, including 25 different modalities, 135 different remedies, and 9 different physical therapies. The top four remedies prescribed were soups, probiotics, elderflower/berry (Sambucas nigra), and honey.
Lifestyle changes were mentioned by the majority of participants (n=23, 95%), with one (4%) participant indicating they would discuss lifestyle changes only if the parents broached the topic first. Lifestyle changes referred to any change in activities (electronic screen time or physical), change in the environment, or change in clothing and bedding;
So, I might be doing long-time immune support using herbs like astragalus, identifying constitutional weaknesses, looking into diet and lifestyle. Velda (Naturopath)
As far as lifestyle things go in any baby that’s got persistent snotty bits, we talk about regular changing of bedding, dealing with mould in the house, putting pillows, doonas, mattresses out in the sun for the UV effect, looking at fireplaces. We talk about the impact of smoking. Albert (Chiropractor)
A specific lifestyle modification that most participants (n=16, 66%) recommended was rest. This referred to the child staying at home as much as possible, ideally in bed, and not going out to child care, preschool, or school;
Oh when they’re sick I keep them in bed as much as possible to rest … . Rochelle (Naturopath)
in bed, … on the couch with a blanket. Watching telly, or whatever. Tabitha (TCM)
Diet-based treatment was another modality utilised by most participants (n=22, 91%). Dietary advice focussed on adding and/or reducing specific foods in the child’s diet. Participants talked about diet mostly in general terms, such as increasing vegetables or reducing dairy;
High fruit, high veg, lots of water, no sugar, bit of protein. That’s my starting point. Albert (Chiropractor)
…,increasing their veggies. Green leafy veggies, their orange veggies, red veggies, yellow veggies. Soups. Broths. Kacey (Naturopath)
Food as medicine was a core focus of the treatment of childhood ARTI for most participants (n=23, 95%), with soups prevailing as the number one choice (n=17, 70%). Participants either provided parents with a soup recipe or advised on ingredients to be included in soup. Involving the parent and child in these discussions was important to participants;
a good old chicken soup with lots of ginger, garlic, galangal, bit of chilli, … If they’re prone to respiratory tract infections a lot, I would use astragalus in the broth. Whitney (Naturopath)
Many participants (n=19, 79%) discussed dairy products, specifically, the elimination of dairy from the diet during ARTI;
I’ll absolutely reduce dairy intake in the two, three, four, five, six-year old’s who’ve got respiratory stuff. Albert (Chiropractor)
Dairy will really worsen congestion. Usha (Naturopath)
All (n=24, 100%) participants recommended one or more preventive strategies as part of the management of ARTI in children. The strategies employed for the prevention of ARTI included dietary advice (n=19, 79%), lifestyle modification (n=14, 58%), herbal treatment (n=14, 58%), vitamin and mineral supplementation (n=12, 50%; with probiotics being the most common supplement, n=9, 37%), bodywork (n=4, 16%) and homoeopathic medicine (n=2, 8%);
prevention, it’s more about looking at where their vulnerabilities and their weaknesses are. Hailey (Naturopath)
Ayurveda is all about prevention. Daniel (Ayurvedic)
In summary, this category focused on the “approach to management” which encompassed an individual practitioner’s philosophy to management. Despite some differences in the modalities prescribed, there were substantial similarities in CAM practice.
Individualisation
Individualisation refers to the tailoring of a treatment approach to the specific needs of a child. A primary focus of the management of childhood ARTI, for all participants (n=24, 100%), was providing customised treatment. While there may be some similarities in the treatment provided for each age group or for specific illnesses, the final management plan was expected to be unique. For example, one participant gave herbal fluid extracts to primary school-aged children, but the actual herbs, dose and other modalities prescribed varied, depending on the child’s needs, as other participants also indicated;
[treatment] depends on the child. Albert (Chiropractor)
There might be some things that I look at, but it might be that the child will not do that, so it has to be individualised. Jacinta (Naturopath)
There were five subcategories that emerged within the category of individualisation: (1) child-centred considerations, (2) simplistic care, (3) compliance, (4) affordability, and (5) dose.
A number of child-centred considerations were factored into the management of childhood ARTI. Considerations such as age, developmental stage, and vulnerability of the child were amongst those mentioned the most. Treating children differently to adults emerged as an important point for many participants (n=22, 91%). For children with ARTI, there was a focus on using gentler physical treatments, reducing treatment time and using safer or simple herbs at lower doses;
[For] children, the dose needs to be very, very small. It’s very easy to overtreat them. Isaac (TCM)
I have to always look at severity and intensity when you’re with little ones in particular, and really alert around that because things can change very quickly. And babies are very delicate and vulnerable, and they need to be attended to acutely. Faith (Homoeopath)
The age of the child was another important consideration in the delivery of individualised care. The majority of participants (n=22, 91%) indicated that the child’s age was a key determinant of the treatments they prescribed, noting that different age groups (e.g., infant, toddler, pre-schooler, primary school-aged child) required a different treatment approach;
[For] toddlers, I use a laser machine. Lucas (TCM)
And so, radish is more for an older child, not for a younger child …. Maybe [those aged] eight. Tabitha (TCM)
Managing ARTI in a breastfeeding infant was considered by many participants, with a large percentage of participants (n=17, 70%) reporting that they treated infants with ARTI via the mother. The treatments varied from increasing the frequency of breastfeeds, increasing the amount of fluid the mother consumes, to prescribing remedies (herbal or vitamin and/or mineral) or dietary advice to the breastfeeding mother;
If the mum’s breastfeeding, I might recommend some things like herbs, nutritionals that are going to go through the breast milk. Kacey (Naturopath)
It depends on the presentation in the baby and also how it affects mum …, I try not to get Mum to avoid very much. The more variety, the better …. From an immune perspective … … I’m trying to make sure that mum is nutritionally replete, so that baby’s getting everything it needs from the breast milk. Odessa (Naturopath)
One participant (4%) stated that she would not treat the infant ARTI via the mother, arguing that:
… … there’s not a whole lot of good evidence that shows what actually passes into breast milk. Zelda (Naturopath)
Most participants (n=21, 87%) emphasised the need for a simplistic approach when treating children with ARTI, as opposed to adults with ARTI. In the context of this research, simplistic care referred to the use of treatments that have a long history of usage, and are gentler, conventional, and safer. It also referred to the use of non-complex treatment regimes, which were easy to understand and easily followed;
[For] the real little-ees, I keep them [the herbs] really simple. Usha (Naturopath)
I say rainbow colours [of food] to mum, to keep it [the diet] very simple. Rochelle (Naturopath)
I keep it really simple of just making sure they’re having some raw vegetables, as well as particularly vegetables really high in silica … . Just lots of whole foods. Grace (Osteopath/nutritionist)
Three-quarters (n=18, 75%) of participants expressed concerns about maintaining treatment compliance in children with ARTI. Common concerns included treatment plans not being followed, recommended foods not being eaten, and remedies not being consumed. Participants often prepared for this by ensuring that the treatment approach was as simple as it could be;
And I’ve had good feedback, but if the compliance isn’t there, I just keep it simple. Quinn (Naturopath)
And try and make it easy for parents. You don’t say, “I want you to get the bananas from the third palm on the right in Madagascar … [instead] you use the foods that are available. Barney (TCM)
The palatability of a remedy can impact treatment compliance, and many participants (n=18, 75%) took this into consideration when prescribing. The participants were conscious of the unpleasant taste of their remedies, and noted that if they wanted the child to be compliant with the remedy, then the treatment needed to be palatable;
Lemon, honey. Ginger as they get older, again palatability depending. Usha (Naturopath)
But I always try and have about at least thirty percent of the mix in a glycetract to make it palatable. Jacinta (Naturopath)
Some participants (n=8, 33%) used other strategies, like storytelling, to encourage children to swallow the remedies;
Depending on the age of the child, you can talk about how the flavour chases the bad away. It tastes bad because you need to make the bad energy leave you. Tabitha (TCM)
The cost of treatment (including the cost of the remedies and the consultation) impacted clinical decision-making in almost half of the participants (n=11, 45%). Participants expressed a desire to minimise the cost of treatment for parents, and to help the child. Different approaches used by participants to reduce the cost of treatment included: recommending food as medicine, conducting follow-up consultations over the phone, limiting the number of products prescribed, and suggesting more affordable products for parents to buy over-the-counter;
I have to be mindful of cost, I’m a real minimalist. So, I focus more on the treatment of the infant, and food as medicine and lifestyle with mum. Usha (Naturopath)
Dose was a subcategory of child-centredness. The dose – encompassing amount or volume, frequency and duration of treatment – was discussed by all participants (n=24, 100%) with regards to both bodywork treatments and oral/topical remedies. The dose was something that was individually calculated for each child in accordance with the child’s age, body type, and level of vitality/wellness;
But then my experience comes in, and I’m looking at the individual child, working out what they’re going to take doses for, etcetera. Kacey (Naturopath)
Individualisation was integral to delivering personalised management strategies in children with ARTI. Accordingly, many aspects of a child’s life were taken into consideration when managing ARTI.
Do No Harm
The concept of do no harm was important to almost all practitioners, with safety a key consideration in 83% (n=20). Participants expressed that the well-being of the child was first and foremost in their mind when planning treatment;
Hippocratic Oath do no harm. Know your limitations. Sacha (Naturopath)
Okay, the infants are tricky because technically naturopaths don’t treat infants. So, I would always work alongside a doctor with the infants. Nadeen (Anthroposophic)
There were two subcategories under the category of do no harm. These were child well-being/safety and clinical practice.
The child well-being/safety subcategory referred to the measures a practitioner put in place to ensure that the child receiving treatment for ARTI was safe. This includes the products that they recommend and the techniques that they use. In this subcategory, two elements were identified. These included: parent education (n=20, 83%), and empowering the child (n=5, 20%).
Parental education (n=20, 83%) was seen as imperative to protecting the safety and well-being of the child. Parental education included informing parents about the important signs and symptoms (or red flags) they should look for in their child, and the action they should take, including consulting a health practitioner, possibly biomedical;
I’ll actually spend a lot of time doing that [explaining signs and symptoms of red flags]. Nadeen (Anthroposophic)
If it was a red flag, I’d refer … Yeah, I do [educate parents on red flags]. Sacha (Naturopath)
For 20% (n=5) of participants, empowering the child was crucial to improving treatment compliance. Participants empowered the child by involving them in the consultation, discussions, and the dispensing of remedies;
Yeah, [I empower the child], and I think it infuses personal care of their body, appreciation of their body, and they’re less likely to choose harm - I think its harm minimisation for the future. Madaline (TCM)
I usually get them involved in dispensing … .when they’re involved, compliance is fantastic. Sacha (Naturopath)
A further subcategory under the category of do no harm was clinical practice precautions. This related to the clinical actions that a participant undertook to ensure that the child under their care was not at risk of harm. Within this subcategory were four elements: remedy safety (n=16, 66%), referral for ARTI (n=22, 91%), limitations of practice (n=13, 54%) and research-informed practice (n=14, 58%).
Participants (n=16, 66%) expressed an awareness of the need to avoid certain remedies (especially essential oils and herbal medicine) at certain phases of a child’s life. The practitioner’s choice of treatment was impacted by the safety and well-being of the child and the specific needs of the child. This was reflected in their clinical practice. For instance, products that were seen as unsafe in a child were often discussed. Two products that participants mentioned regarding possible contra-indications or non-therapeutic reaction were essential oils and honey in the context of child safety and overall well-being;
So with a baby, I don’t want the oils too close [to the baby], . even something as simple as lavender, it’s a very safe essential oil … .but don’t wanna over-do it because remember the infant is so young at that point. Rochelle (Naturopath)
No, I’d hold off [giving honey to an infant]. Whitney (Naturopath)
No camphor and then I guess it’s also in consultation if there’s a baby at home, … so no baby comes in contact with camphor. Madaline (TCM)
Participants (n=22, 91%) acknowledged that some presenting conditions were either outside their scope of practice or not within their area of expertise. Participants stated that when necessary, they would refer the child to another health practitioner/service, most commonly GPs (n=19, 79%), hospital emergency departments (n= 10, 41%), and other CAM practitioners from the same or different disciplines. Participants even perceived that referrals among all health practitioners were increasing;
Referral. It’s increasing. I think that people are working more collectively. Faith (Homoeopath)
Yes, absolutely [I refer]. If it’s a really nasty whatever, then to a GP, or to homoeopathy, or Chinese medicine. Albert (Chiropractor)
Two (8%) participants stated they would not refer a child to another practitioner, including biomedical practitioners. One (4%) participant stated they did not see a need for referral and the other participant (4%) stated that the parents and children had already consulted a biomedical practitioner for the current condition and had made a decision to see them to try a different approach;
[No I don’t refer] … normally they [the patient] come to me after they’ve seen the GP. Hailey (Naturopath)
Approximately one-half of participants (n=13, 54%) recognised the shortcomings in their skills. They acknowledged that they were not able to treat all children with ARTI all of the time. Furthermore, they indicated they were not comfortable working outside their scope of training, and this often triggered a referral to another health practitioner;
Yeah for example, if it is something out of our boundary, you know definitely if we need their [biomedical] help- Paige (Ayurvedic)
I think it’s about knowing the limitations of what you can do and knowing what else is out there and what’s appropriate, what works, what we have good research for, and that’s about knowing your limitations too. Odessa (Naturopath)
Many participants (n=14, 58%) expressed concern about the limited availability of research evidence to inform their decisions regarding the treatment of ARTI in children. Despite concerns about the limited quality and volume of research, many participants (n=14, 58%) were keen to stay up-to-date and to change their clinical practice as new evidence emerged;
I welcome the advances in research. Coby (Osteopath)
I follow the current research base. Zelda (Naturopath)
In summary, the category of “do not harm” explored the critical safety considerations practitioners built into their decision-making process when recommending CAM modalities to children with ARTI. The diverse and wide-ranging safety considerations explored by practitioners highlight the careful and considered approach used by this group.
Collaborative Practice
Over half (n=13, 54%) of the participants expressed a desire to collaborate with other health practitioners, including biomedical practitioners, on the care of a child with ARTI. They viewed their role as playing just one part in a complex healthcare system. Two-thirds (n=16, 66%) of the practitioners viewed biomedical practitioners positively, and desired to work with them;
I find the GP’s definitely pretty understanding. Grace (Osteopath/nutritionist)
Yeah, yeah, that’s where I first look into allopathy (biomedicine). Both systems have positives and negatives and need to be used wisely. Paige (Ayurvedic)
… I consider myself complementary, not alternative. Usha (Naturopath)
Within the category of collaborative practice was one subcategory: assessment.
Participants acknowledged the limitations of their knowledge and skills, and collaborated with biomedical practitioners for their assessment skills, either for a second opinion or a primary diagnosis. It was almost routine for some participants (n= 15, 62%) to utilise the assessment skills of biomedical practitioners. If participants were unsure of the child’s diagnosis, or if the child’s condition was not improving, they often sought biomedical assistance;
[If] their chest is compromised, or their tonsils are looking like they’re got an infection, I’ll send them off to have a GP to double check. Nadeen (Anthroposophic)
They (GP’s) are the diagnostic specialists, you know. Usha (Naturopath)
The category “collaborative practice” encompassed a CAM practitioner’s desire to work hand-in-hand with other health professionals. This desire served to address the practitioner’s clinical limitations, for the betterment of the child with ARTI.
Discussion
Despite the growing popularity of CAM, there continues to remain numerous knowledge gaps. One such gap pertains to the interventions used by CAM practitioners for the treatment and prevention of ARTI in children, and how CAM practitioners formulate their decisions regarding the management of ARTI. This research aimed to address these knowledge gaps. The findings indicate that CAM practitioners utilise lifestyle modification (95%) and dietary advice (91%) as initial strategies for the treatment and prevention of ARTI in children. The decision-making processes used by the practitioners were influenced by four key aspects – approach to management, individualisation, “do no harm”, and collaborative practice. Some of these findings are consistent with the results of previous research exploring parent utilisation of CAM for children with ARTI.43
A common recommendation of CAM practitioners for the management for ARTI in children was lifestyle modification, specifically rest. Rest, as a lifestyle modification, had two different components; first the reduction of the children’s activity outside the home (e.g., not doing sport or staying home from school), and second, the adjustments to the environment where the child physically rested at home (e.g., change to bedding or bedroom ventilation). The role of rest in the recovery of ARTI in children is supported by clinical practice guidelines.47,48 The role of specific lifestyle modifications in the management of acute respiratory infections in children is less clear, however.49
Another important finding from this research was the use of common foods as medicine. The use of foods as medicine dates back to the 19th century philosophy of CAM; as stated by Sebastian Kneipp (1821–1897), “The path to your health leads through the kitchen and not through pharmacies”.50,51 Food as medicine included removing some foods, such as dairy, and increasing the intake of other foods such as green, red, orange, and yellow vegetables. The use of soups was also common, and this is immersed in historical traditions, as well as being supported by some research. For example, the research by Rennard et al52 indicated soups may inhibit neutrophil chemotaxis and may exert a mild anti-inflammatory effect. Saketkhoo et al53 also reported increased nasal mucus velocity and decreased nasal airflow resistance following soup consumption. The use of soups as one of the frontline home remedies for ARTI corroborates previous research of Australian parents.43 Such strikingly similar approaches for managing ARTI in children suggest shared ideas, perhaps through past experiences, between practitioners and parents.
Many CAM practitioners recommended a change to or removal of dairy from the child’s diet during ARTI. Presently, there is conflicting evidence regarding the role of dairy in this condition. Yusoff et al54 demonstrated dairy may thicken mucus, and for asthmatic children who were on an egg-free milk-free diet, there was reduced atopic symptoms and improved lung function. In a randomized, double‐blinded controlled study design of adults that experienced subjective awareness of excessive production of nasal secretions with no cow’s milk intolerance, the elimination of dairy products was shown to decrease nasopharyngeal secretions.55 Other research highlighting the negative impacts of dairy in ARTI has been restricted to children with existing dairy allergies.56,57 By contrast, findings from other studies suggest that dairy has no impact on the symptoms of mucus production and ARTI.58,59 Given these conflicting findings, more research is required to investigate what, if any, impact dairy has on children with ARTI.
CAM practitioner decision-making regarding the management of ARTI in children was informed by four underlying principles – “do no harm”, individualisation, approach to management, and collaborative practice. These principles were operationalized in clinical practice through a nuanced and considered approach. For example, despite some prevailing perceptions that CAM practitioners may be unsafe and contribute to harm in their patients,60,61 this research identified CAM practitioners, irrespective of their discipline (TCM, naturopathy, ayurvedic), as driven by the ethos of doing no harm. The ethos to “do no harm” is shared across all mainstream health disciplines (medical, nursing, allied health, pharmacy, dentistry), and our finding indicates that this may be explicitly shared by CAM practitioners too.
Another important finding from this research relates to the individualisation of treatment strategies as part of the broader decision-making process. Individualisation of CAM treatment was informed by all aspects of a child’s life – biological, psychological, social, environmental, and cultural. This approach is congruent with the contemporary healthcare practices underpinned by the seminal works of Engel.62 The biopsychosocial-cultural model emphasises a complete and comprehensive assessment and intervention that gives consideration to biological, psychological, and socio-cultural factors.63,64 By considering the biological (i.e., age of the child and type of respiratory symptoms), psychological (i.e., compliance with remedies and child’s personal preferences for treatment options), social (i.e., cost of treatments, family home/environment), and cultural (i.e., family preferences for types of foods as medicine) aspects, CAM practitioners appear to provide nuanced, wholistic and patient-centred care to children with ARTI.65
Limitations
As with any research, there are limitations to this research as well. Given the qualitative nature of this study, generalisability of the findings is limited. As means of improving transferability, a range of CAM practitioners across diverse geographical locations were recruited to be part of this research. About 75% of the sample in this research were female and it is unknown what, if any, different perspectives may have been captured if there were more male participants. The over-representation of female participants, however, reflects the gender divide commonly seen in CAM practitioners.66 Although member checking did not occur, there remains debate regarding the usefulness of this process.37 As means of addressing this issue, field notes were taken during and immediately after the interviews to assist in confirming the accuracy of the interview (although these were not used as part of data analysis).
Clinical Implications
CAM practitioners appear to play a critical role for, and contribute to, the management of ARTI in children in the community. While these practitioners use a range of similar modalities, many treatments are easily accessible and readily available to parents (such as soups) and are aligned with mainstream recommendations (such as rest). The decision-making process adopted by these practitioners appears to be informed by a biopsychosocial-cultural approach, with safety being a key consideration, as well as an eagerness to collaborate with other health professionals. From a clinical perspective, these findings showcase the emergent role of CAM practitioners and their nuanced yet practical decision-making approach for ARTI, which readily align with mainstream and contemporary healthcare approaches.
Conclusion
This is the first known study to explore the types of interventions used by CAM practitioners for the treatment and prevention of ARTI in children. The results indicate that many of the treatments prescribed are easily accessible and readily available to parents (such as soups) and are well aligned with mainstream recommendations (such as rest). The study also sheds light on the decision-making process of CAM practitioners regarding the management of ARTI in children. These findings suggest that CAM practitioners’ decision-making process is informed by a biopsychosocial-cultural approach and focuses on safety – not dissimilar to that of mainstream healthcare providers. Collectively, these findings further our understanding of the role of CAM, and CAM services, in the treatment of ARTI and in health care more broadly.
Abbreviations
ARTI, acute respiratory tract infection; CAM, complementary and alternative medicine; GP, general medical practitioners; TCM, traditional Chinese medicine; QD, qualitative descriptive.
Availability Of Data And Material
The datasets generated during and/or analysed during the current research are available from the corresponding author on reasonable request.
Consent For Publication
Written informed consent obtained from all participants for data to be used in publications.
Ethics Approval And Consent To Participate
Ethics approval was granted by the Human Research Ethics Committees of the University of South Australia (ID: 0000035018). Written informed consent obtained from all participants to participate in this study.
Acknowledgments
The authors would like to thank the CAM practitioners for their participation in the research. SL acknowledges the Australian Government Research Training Program Scholarship that funds her PhD.
Author Contributions
SL participated in the research concept and design, data acquisition, data analysis, data interpretation, manuscript drafting, critical revision of the manuscript, and the final review of the manuscript. SK participated in the research concept and design, data analysis, data interpretation, manuscript drafting, critical revision of the manuscript, and the final review of the manuscript. MJL participated in the research concept and design, data analysis, data interpretation, manuscript drafting, critical revision of the manuscript, and the final review of the manuscript. AP reviewed research concept and design, and participated in the data analysis and interpretation, manuscript drafting, critical revision of the manuscript, and the final review of the manuscript. All authors made critical contributions and/or review to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Troeger C, Blacker B, Khalil IA, et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018;18(11):1191–1210. doi:10.1016/S1473-3099(18)30310-4
2. GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390::1151–1210.
3. Hall CB, Weinberg G, Iwane M, et al. The burden of respiratory syncytial virus infection in young children. N Engl J Med. 2009;360(6):588–598. doi:10.1056/NEJMoa0804877
4. Cabral C, Lucas PJ, Ingram J, Hay AD, Horwood J. “It’s safer to … ” parent consulting and clinician antibiotic prescribing decisions for children with respiratory tract infections: an analysis across four qualitative studies. Soc Sci Med. 2015;136–137:156–164. doi:10.1016/j.socscimed.2015.05.027
5. Leder K, Sinclair MI, Mitakaki TZ, Hellard ME, Forbes A, Fairley CK. A community-based study of respiratory episodes in Melbourne, Australia. Aust N Z J Public Health. 2003;27(4):399–404. doi:10.1111/j.1467-842X.2003.tb00416.x
6. Cabral C, Ingram J, Lucas PJ, et al. Influence of clinical communication on parents’ antibiotic expectations for children with respiratory tract infections. Ann Fam Med. 2016;14(2):141–147. doi:10.1370/afm.1892
7. Nyquist A-C, Gonzales R, Steiner JF, Sande MA. Antibiotic prescribing for children with colds, upper respiratory tract infections, and bronchitis. JAMA. 1998;279(11):875–877. doi:10.1001/jama.279.11.875
8. World Health Organization (WHO). Coughs and Cold Remedies for the Treatment of Acute Respiratory Infections in Young Children. Geneva, Switzerland: WHO; 2001. Available from: http://apps.who.int/iris/bitstream/10665/66856/1/WHO_FCH_CAH_01.02.pdf?ua=1&ua=1.
9. Zeng L, Zhang L, Hu Z, et al. Systematic review of evidence-based guidelines on medication therapy for upper respiratory tract infection in children with AGREE instrument. PLoS ONE. 2014;9:2.
10. Chan JYC, Stern DA, Guerra S, Wright AL, Morgan WJ, Martinez FD. Pneumonia in childhood and impaired lung function in adults: a longitudinal study. Pediatrics. 2015;135(4):607–616. doi:10.1542/peds.2014-3060
11. Chen Y, Kirk MD. Incidence of acute respiratory infections in Australia. Epidemiol Infect. 2014;142:1355–1361. doi:10.1017/S0950268813002471
12. Chow MYK, Morrow AM, Booy R, Leask J. Impact of children’s influenza-like illnesses on parental quality of life: a qualitative study. J Paediatr Child Health. 2013;49(8):664–670. doi:10.1111/jpc.2013.49.issue-8
13. Fendrick A, Monto AS, Nightengale B, Sarnes M. THe economic burden of non–influenza-related viral respiratory tract infection in the united states. Arch Intern Med. 2003;163(4):487–494. doi:10.1001/archinte.163.4.487
14. Hay AD, Heron J, Ness A; the ALSPAC study team. The prevalence of symptoms and consultations in pre-school children in the Avon Longitudinal Study of Parents and Children (ALSPAC): a prospective cohort study. Fam Pract. 2005;22(4):367–374. doi:10.1093/fampra/cmi035
15. Hollinghurst S, Gorst C, Fahey T, Hay A. Measuring the financial burden of acute cough in pre-school children: a cost of illness study. BMC Fam Pract. 2008;9(1):10. doi:10.1186/1471-2296-9-10
16. Thompson PL, Spyridis N, Sharland M, et al. Changes in clinical indications for community antibiotic prescribing for children in the UK from 1996 to 2006: will the new NICE prescribing guidance on upper respiratory tract infections just be ignored? Arch Dis Child. 2009;94(5):337–340. doi:10.1136/adc.2008.147579
17. Revai K, Dobbs LA, Nair S, Patel JA, Grady JJ, Chonmaitree T. Incidence of acute otitis media and sinusitis complicating upper respiratory tract infection: the effect of age. Pediatrics. 2007;119(6):e1408–e12. doi:10.1542/peds.2006-2881
18. World Health Organization (WHO). Coughs and Cold Remedies for the Treatment of Acute Respiratory Infections in Young Children. Geneva, Switzerland: WHO; 2001.
19. Little P, Moore M, Kelly J, et al. Ibuprofen, paracetamol, and steam for patients with respiratory tract infections in primary care: pragmatic randomised factorial trial. Br Med J. 2014;348(7949):13. doi:10.1136/bmj.g1606
20. (NICE) NIoHaCE. Fever in under 5s: assessment and initial management- Clinical Guidelines [CG160] 2013. updated August 2017. Available from: https://www.nice.org.uk/guidance/cg160/chapter/1-Recommendations#antipyretic-interventions–2.
21. Isbister GK, Prior F, Kilham HA. Restricting cough and cold medicines in children. J Paediatr Child Health. 2012;48(2):91–98. doi:10.1111/jpc.2012.48.issue-2
22. Weinberger M, Hendeles L. Nonprescription medications for respiratory symptoms: facts and marketing fictions. Allergy Asthma Proc. 2018;39(3):169–176. doi:10.2500/aap.2018.39.4117
23. Centers for Disease Control (CDC). Infant deaths associated with cough and cold medications–two states, 2005. MMWR Morb Mortal Weekly Rep. 2007;56(1):1–4.
24. Aono M, Bukirwa C, Luyinda E, et al. Medicine use practices in management of symptoms of acute upper respiratory tract infections in children (≤12 years) in Kampala city, Uganda. BMC Public Health. 2017;17(1):1–8. doi:10.1186/s12889-016-3954-4
25. Lim AG, Cranswick N, Skull S, South M. Survey of complementary and alternative medicine use at a tertiary children’s hospital. J Paediatr Child Health. 2005;41(8):424–427. doi:10.1111/jpc.2005.41.issue-8
26. Wieland LS, Manheimer E, Berman BM. Development and classification of an operational definition of complementary and alternative medicine for the Cochrane collaboration. Altern Ther Health Med. 2011;17(2):50–59.
27. Sobenin I, Andrianova I, Sereda E, Borodina L, Karagodin V, Orekhov A. The effects of time release garlic powder tablets on acute respiratory disease in children. Med Sci J. 2011;9(5):31–37.
28. Holzinger F, Chenot J-F. Systematic review of clinical trials assessing the effectiveness of ivy leaf (hedera helix) for acute upper respiratory tract infections. Evidence Based Complementary Altern Med. 2011;9.
29. Ulbricht C, Basch E, Cheung L, et al. An evidence-based systematic review of elderberry and elderflower (Sambucus nigra) by the Natural Standard Research Collaboration. J Diet Suppl. 2014;11(1):80–120. doi:10.3109/19390211.2013.859852
30. Lucas S, Leach M, Kumar S. Complementary and alternative medicine utilisation for the management of acute respiratory tract infection in children: a systematic review. Complementary Therapies Med. 2018;37:158–166. doi:10.1016/j.ctim.2018.03.001
31. Tashakkori A, Teddlie C. Handbook of Mixed Methods in Social and Behavioral Research. Thousands Oaks, CA: Sage; 2003.
32. Creswell J. Research Design:- Qualitative, quantitative, and Mixed Methods Approaches. USA: SAGE Publications, Inc; 2014.
33. Morgan DL. Paradigms lost and pragmatism regained. J Mix Methods Res. 2007;1(1):48–76. doi:10.1177/2345678906292462
34. Saunders M, Lewis P, Thornhill A. Research Methods for Business Students.
35. Sandelowski M. Focus on research methods. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334–340. doi:10.1002/(ISSN)1098-240X
36. Miles MB, Huberman AM. Qualitative Data Analysis: An Expanded Sourcebook.
37. Polit D, Beck C. Nursing Research:- Generating and Assessing Evidence for Nursing Practice. China: Wolters Kluwer| Lippincott Williams & Wilkins; 2012.
38. Polit DF, Beck CT. Essentials of Nursing Research: Appraising Evidence for Nursing Practice.
39. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
40. Liamputtong P. Research Methods in Health: Foundations for Evidence Based Practice. Oxford University Press; 2013. Available from: http://latrobe.eblib.com.au/patron/FullRecord.aspx?p=1986006
41. Ramadurai V, Sharf BF, Ramasubramanian S. Roads less traveled: finding a path to using complementary and alternative medicine. Qual Health Res. 2016;26(9):1216–1228. doi:10.1177/1049732315582009
42. Nichol J, Thompson EA, Shaw A. Beliefs, decision-making, and dialogue about Complementary and Alternative Medicine (CAM) within families using CAM: a qualitative study. J Altern Complementary Med. 2011;17(2):117–125. doi:10.1089/acm.2010.0171
43. Lucas S, Kumar S, Leach MJ, Phillips A. Parent use of complementary medicine remedies and services for the management of respiratory tract infection in children: a qualitative study. J Multidiscip Health Care. 2019;12:749–766. doi:10.2147/JMDH.S216687
44. Vaismoradi M, Turunen T, Bondas T. Content analysis and thematic analysis: implications for conducting a qualitative descriptive study. Nurs Health Sci. 2013;15(3):398–405. doi:10.1111/nhs.12048
45. Elo S, Kyngas H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
46. Crowe M, Inder M, Porter R. Conducting qualitative research in mental health: thematic and content analyses. Aust N Z J Psychiatry. 2015;49(7):616–623. doi:10.1177/0004867415582053
47. Biezen R, Pollack AJ, Harrison C, et al. Respiratory tract infections among children younger than 5 years: current management in Australian general practice. Med J Aust. 2015;202(5):262–265. doi:10.5694/mja14.00090
48. Group RE. Therapeutic Guidelines: Respiratory.
49. NPS Medicinewise. Respiratory tract infection action plan level 7/418A Elizabeth Street Surry Hills NSW 2010 nps.org.au; 2019 Available from: https://www.nps.org.au/medical-info/clinical-topics/reducing-antibiotic-resistance#resources.
50. World Naturopathic Federation. WNF white paper: naturopathic philosophies, principles and theories Canada2017. Available from: http://worldnaturopathicfederation.org/wp-content/uploads/2015/12/White-Paper_FINAL.pdf.
51. Hausser T, editor. Naturopathic history: origins of modern naturopathic practice.
52. Rennard BO, Ertl RF, Gossman GL, Robbins RA, Rennard SI. Chicken soup inhibits neutrophil chemotaxis in vitro. Chest. 2000;118(4):1150–1157. doi:10.1378/chest.118.4.1150
53. Saketkhoo K, Januszkiewicz A, Sackner MA. Effects of drinking hot water, cold water, and chicken soup on nasal mucus velocity and nasal airflow resistance. Chest. 1978;74(4):408–410. doi:10.1016/S0012-3692(15)37387-6
54. Yusoff N, Hampton S, Dickerson J, Morgan J. The effects of exclusion of dietary egg and milk in the management of asthmatic children: a pilot study. J R Soc Promot Health. 2004;124(2):74–80. doi:10.1177/146642400412400211
55. Frosh A, Cruz C, Wellsted D, Stephens J. Effect of a dairy diet on nasopharyngeal mucus secretion. Laryngoscope. 2019;129(1):13–17. doi:10.1002/lary.v129.1
56. Wuethrich B, Schmid A, Walther B, Sieber R. Milk consumption does not lead to mucus production or occurrence of asthma. J Am Coll Nutr. 2005;24:547S–55S. doi:10.1080/07315724.2005.10719503
57. Juntti H, Tikkanen S, Kokkonen J, Alho O-P, Niinimäki A. Cow’s milk allergy is associated with recurrent otitis media during childhood. Acta Otolaryngol. 1999;119(8):867–873. doi:10.1080/00016489950180199
58. Balfour-Lynn I. Milk, mucus and myths. Arch Dis Child. 2019;104(1):91–93. doi:10.1136/archdischild-2018-314896
59. Pinnock CB, Arney WK. The milk-mucus belief: sensory analysis comparing cow’s milk and a soy placebo. Appetite. 1993;20:61–70. doi:10.1006/appe.1993.1006
60. Wardle J, Adams J, Lui CW, Steel A. Current challenges and future directions for naturopathic medicine in Australia: a qualitative examination of perceptions and experiences from grassroots practice. BMC Complementary Altern Med. 2013;13:15. doi:10.1186/1472-6882-13-15
61. Hunt K, Ernst E. Evidence-based practice in British complementary and alternative medicine: double standards? J Health Serv Res Policy. 2009;14(4):219–223. doi:10.1258/jhsrp.2009.009009
62. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196:129–136. doi:10.1126/science.847460
63. Pham AV. Understanding ADHD from a biopsychosocial-cultural framework: a case study. Contemporary School Psychol. 2015;19(1):54–62. doi:10.1007/s40688-014-0038-2
64. Suls J, Krantz DS, Williams GC, et al. Three strategies for bridging different levels of analysis and embracing the biopsychosocial model. Health Psychol. 2013;32(5):597–601. doi:10.1037/a0031197
65. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
66. Leach M. Profile of the complementary and alternative medicine workforce across Australia, New Zealand, Canada, United States and United Kingdom. Complement Ther Med. 2013;21(4):364–378. doi:10.1016/j.ctim.2013.04.004
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.