Back to Journals » Clinical Ophthalmology » Volume 20
Comparison of Visual Performance and Patient Satisfaction Between Two Trifocal Intraocular Lenses: A Prospective, Paired-Eye Comparative Study
Authors Kang S ![]() , Arsenault SM, O'Brien RC, Chatzea MS, Zarei-Ghanavati S, Beniz LAF, Yoo SH
, Arsenault SM, O'Brien RC, Chatzea MS, Zarei-Ghanavati S, Beniz LAF, Yoo SH ![]()
Received 7 October 2025
Accepted for publication 9 December 2025
Published 17 January 2026 Volume 2026:20 572237
DOI https://doi.org/10.2147/OPTH.S572237
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Sujin Kang,1 Samantha M Arsenault,1,2 Robert C O’Brien,1 Marina S Chatzea,3 Siamak Zarei-Ghanavati,4 Luiz AF Beniz,5 Sonia H Yoo1
1Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, FL, USA; 2Department of Ophthalmology, Henry Ford Health System, Detroit, MI, USA; 3 1st Department of Ophthalmology, “G. Gennimatas” Hospital, National and Kapodistrian University of Athens, Athens, Greece; 4Eye Research Center, Mashhad University of Medical Sciences, Mashhad, Iran; 5Department of Ophthalmology and Visual Sciences, Paulista School of Medicine, Federal University of São Paulo, São Paulo, SP, Brazil
Correspondence: Sonia H Yoo, Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, 900 NW 17th Street, Miami, FL, 33136, USA, Email [email protected]
Purpose: This study compared the visual performance, patient-reported outcomes, and spectacle independence of two advanced trifocal intraocular lens (IOL) platforms, Clareon PanOptix and TECNIS Odyssey, in a paired-eye design. The primary hypothesis was that differences in optical design would yield distinct strengths in distance, intermediate, and near visual acuity (VA), contrast sensitivity (CS), and patient satisfaction.
Patients and Methods: In this prospective, single-center, single-surgeon trial at the Bascom Palmer Eye Institute, 19 patients (38 eyes; mean age 66.37 ± 10.61 years) undergoing bilateral cataract surgery were stratified by ocular dominance and randomized for dominant-eye IOL allocation. Each patient received a PanOptix (toric or non-toric) in one eye and an Odyssey (toric or non-toric) in the fellow eye, implanted one week apart. Postoperative assessments (≥ 1 month) included monocular distance-corrected VA at distance (CDVA, 4 m), intermediate (DCIVA, 60 cm), and near (DCNVA, 40 cm), uncorrected VAs, residual refraction, CS, and patient-reported visual quality and spectacle independence.
Results: Compared with PanOptix, Odyssey achieved significantly better CDVA (EMD=0.03 logMAR, 95% CI [0.01, 0.06], P=0.009) and UCDVA (EMD=0.06 logMAR, 95% CI [0.01, 0.12], P=0.03), while PanOptix demonstrated superior DCIVA (EMD=− 0.05 logMAR, 95% CI [− 0.09, − 0.01], P=0.03). DCNVA, UCIVA, and UCNVA did not differ significantly (P≥ 0.07). CS was higher in Odyssey eyes (EMD=− 5.47, 95% CI [− 10.50, − 0.42], P=0.03). Residual spherical equivalent was similar between groups (− 0.10 D vs − 0.09 D, P=0.91). Rates of starburst, halo, and glare were not significantly different (P≥ 0.34). Spectacle independence was achieved by 17 of 19 patients (89.47%) in both groups.
Conclusion: In a paired-eye comparison, PanOptix provided superior intermediate VA, while Odyssey delivered better distance VA and CS. Both lenses yielded high spectacle independence and comparable rates of photic phenomena, supporting their viability as presbyopia-correcting options in cataract surgery.
Keywords: cataract surgery, multifocal intraocular lenses, visual acuity, patient reported outcome measures, contrast sensitivity
Introduction
Advancements in intraocular lens (IOL) technology have significantly transformed presbyopia-correcting cataract surgery, enhancing visual outcomes for patients.1 Trifocal IOLs, in particular, have emerged to meet the near and intermediate range visual needs of an aging population increasingly dependent on digital devices such as computers, laptops, and smartphones.2,3 Compared to monofocal, bifocal, and extended depth of focus (EDoF) IOLs, trifocal IOLs provide a broader range of vision across near, intermediate, and distance ranges.4,5 This results in greater spectacle independence than traditional monofocal IOLs, with particularly high satisfaction rates among hyperopic presbyopic patients, who benefit most from the enhanced near vision correction.6–8 However, their diffractive, light-splitting optical design can increase the incidence of dysphotopsia, such as halos, glare, and starburst, potentially compromising contrast sensitivity (CS) and night vision, including driving performance.9–12
Among the leading trifocal IOLs, the Clareon PanOptix (Alcon, Fort Worth, TX, USA) and its toric variant are single-piece, diffractive, ultraviolet-filtering lenses. This optical design redistributes light and introduces an additional focal point at 120 cm to complement the standard intermediate focal point at 60 cm, creating three distinct functional foci without compromising near or distance visual acuity (VA).13 Manufactured from hydroxyethyl methacrylate (HEMA), the Clareon PanOptix is designed to minimize glistening and surface scattering, reducing visual disturbances compared to its predecessor, the AcrySof IQ PanOptix (Alcon, Fort Worth, TX, USA), which is made from acrylic phenylethyl methacrylate (PEMA).13 Despite these improvements, some studies have noted persistent photic disturbances with this lens design.14–16
More recently, the FDA-approved TECNIS Odyssey (Johnson & Johnson Vision, Santa Ana, CA, USA) and its toric version have also emerged as advanced single-piece, diffractive, ultraviolet-filtering lenses. Building on the TECNIS Synergy (Johnson & Johnson Vision, Santa Ana, CA, USA) platform, the Odyssey integrates multifocal and EDoF optical technologies. It features a proprietary freeform diffractive profile designed to reduce visual disturbances and incorporates chromatic aberration correction technology to enhance CS and potentially improve near VA compared to the PanOptix.17
Despite these technological advancements, clinical data on the Odyssey IOL remain limited.18 To address this gap, this pilot study conducts a prospective, stratified-randomized, paired-eye comparative analysis to evaluate VA outcomes, patient-reported visual quality, and spectacle independence between the two trifocal IOL platforms.
Materials and Methods
Study Design
This was a prospective, single-center, single-surgeon, paired-eye comparative study conducted at the Bascom Palmer Eye Institute, University of Miami, from March 2024 to March 2025. The study protocol adhered strictly to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board at the University of Miami (IRB reference ID 20210929). Written informed consent was obtained from all patients prior to enrollment. Importantly, this study was intended as an exploratory, pilot-type comparative investigation designed to provide early clinical data on the Odyssey IOL. Accordingly, no a priori sample size calculation was performed.
Study Population
Patients aged 45 years or older undergoing bilateral age-related cataract surgery were eligible if both eyes met predefined clinical criteria. Patients were excluded if they had ocular comorbidities (glaucoma, retinal, or corneal diseases), history of ocular surgery or trauma, irregular corneal astigmatism, abnormal corneal topography, systemic or congenital conditions potentially affecting visual outcomes, or were unable to understand or complete visual function questionnaires.
Study Procedure
Patients were stratified based on ocular dominance and randomized to determine the IOL assignment for the dominant eye, mitigating dominance-related bias. Participants underwent comprehensive preoperative evaluations, including medical history review, ocular dominance determination (Miles test), VA measurement, tonometry, slit-lamp and fundus examinations, manifest refraction assessment, and corneal topography with TMS-4N (Tomey USA, Phoenix, AZ, USA). Biometry parameters, including axial length, anterior chamber depth, pupil size, average total keratometry, and all IOL power calculations were obtained via the IOLMaster 700 (version 1.88, Carl Zeiss Meditec AG, Jena, Germany), utilizing the Barrett TK Universal II and Barrett TK Toric formulas. The cutoff for toric IOL implantation was total keratometric astigmatism ≥+1.00 D. Manufacturer-recommended lens constants were applied, without postoperative constant optimization, as this was an exploratory pilot study.
Each patient underwent uncomplicated bilateral cataract surgery, with the implantation of a PanOptix toric or non-toric IOL in one eye and an Odyssey toric or non-toric IOL in the fellow eye. Cataract surgery was performed sequentially one week apart by a single surgeon (SHY). Surgical procedures utilized the Opmi Lumera 700 microscope and the Callisto eye® System (Carl Zeiss Meditec AG, Jena, Germany).
Postoperative evaluations were conducted at ≥1 month, a time point at which refractive error and monocular VA are generally stable after cataract surgery.19,20 This interval was selected to obtain early comparative performance data on the newly introduced Odyssey IOL and is consistent with the 1-month outcomes reported in early clinical studies. Postoperative testing included distance-corrected and uncorrected at distance (4 m), intermediate (60 cm), and near (40 cm) using standardized Early Treatment Diabetic Retinopathy Study (ETDRS) charts under photopic conditions at 100% contrast, with results recorded in logMAR units. Additional postoperative assessments included manifest refraction, slit-lamp examination (with rotational alignment of toric IOLs confirmed by evaluating the IOL axis markings), CS measurement using the CSV-1000 test (VectorVision, Greenville, OH, USA) with distance-correction, and patient-reported outcome questionnaires assessing postoperative visual function and satisfaction.
Study Endpoints
Primary endpoints were monocular distance-corrected VAs measured at distance (4 m, CDVA), intermediate (60 cm, DCIVA), and near (40 cm, DCNVA). Distance-corrected VAs were prioritized over uncorrected VAs to objectively assess visual performance and minimize potential biases arising from individual patient preferences and personalized refractive targets or unintended residual refractive errors. Additionally, primary endpoints included patient-reported outcomes evaluating dysphotopsia (starburst, halo, and glare), visual quality perception via the Visual Function-7 (VF-7) questionnaire, and spectacle independence.
Secondary endpoints included monocular uncorrected visual acuities at distance (4 m, UDVA), intermediate (60 cm, UIVA), and near (40 cm, UNVA), refractive outcomes (sphere, cylinder, and spherical equivalent), and CS.
Statistical Analysis
All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA) and R statistical software (version 4.5.0). For paired-eye comparisons, statistical tests were selected to appropriately account for inter-eye correlation. Baseline ocular characteristics were compared using paired t-tests for continuous variables and the exact McNemar’s test for categorical variables. Postoperative continuous outcomes, including corrected and uncorrected VAs, residual spherical equivalent, and CS, were analyzed using generalized estimating equations (GEE) with an identity link and exchangeable correlation structure. Results are reported as estimated mean differences (EMD) with 95% confidence intervals (CIs). For binary outcomes, such as the presence of starburst, halo, and glare, GEE analyses with a logit link and exchangeable correlation structure were used to estimate odds ratios (OR) with 95% CIs. Spectacle independence was analyzed using the exact McNemar’s test. Statistical significance was defined as a two-sided P-value of less than 0.05.
Results
Patient Demographics and Ocular Characteristics
A total of 38 eyes from 19 patients were included in this paired-eye comparative study. The mean age of participants was 66.37 years (range: 48–85 years). Twelve of the 19 patients (63.16%) were female. PanOptix was implanted in the dominant eye in 12 patients, while Odyssey was implanted in the dominant eye in 7 patients (P=0.36). Preoperative ocular characteristics including IOL sphere power, cylinder power, axial length, anterior chamber depth, pupil size, average total keratometry, manifest refraction spherical equivalent, and proportion of toric IOL use showed no statistically significant differences between eyes assigned to PanOptix and Odyssey (all P≥0.31), confirming appropriate matching for comparative analysis (Table 1).
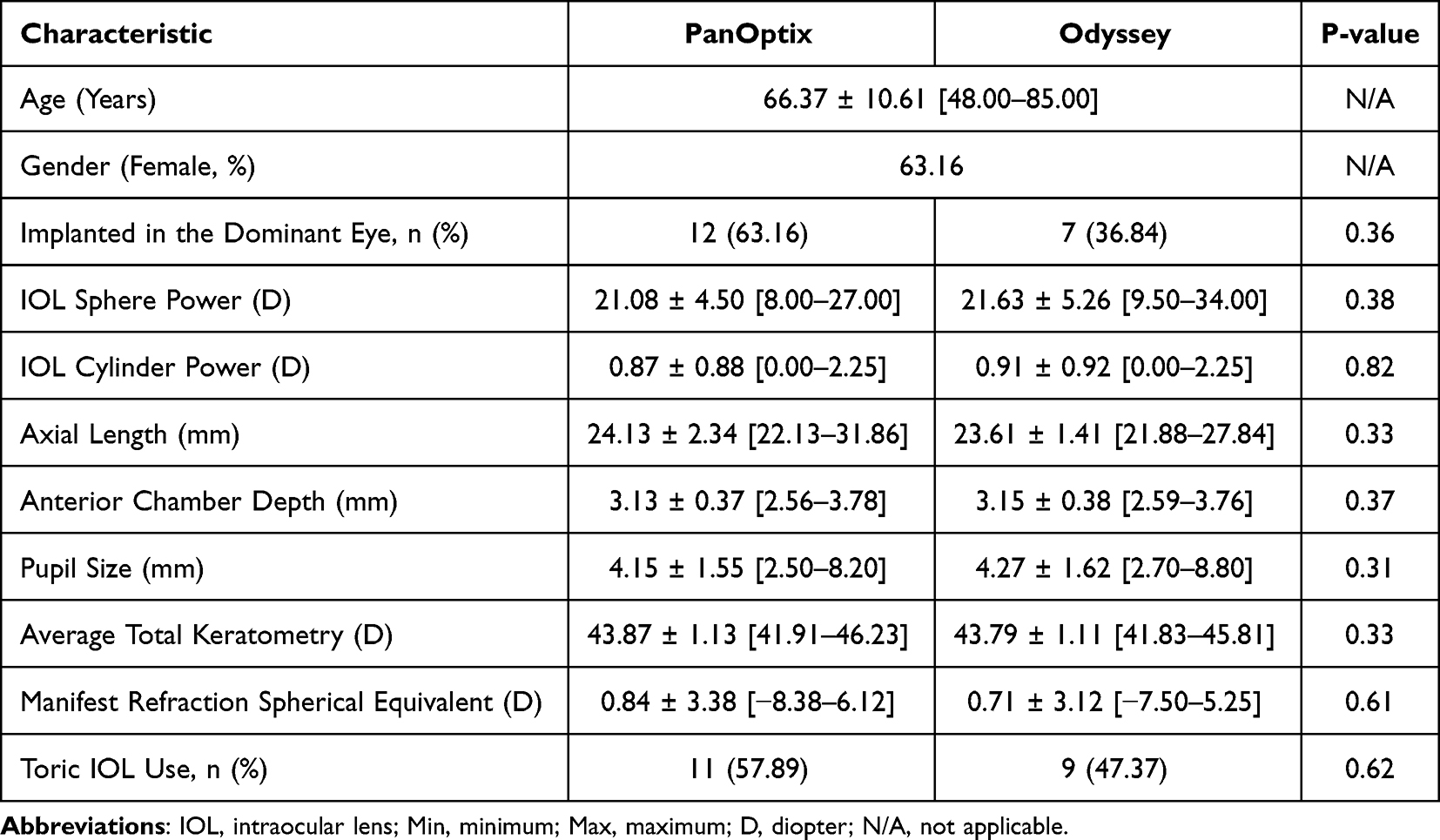 |
Table 1 Baseline Demographic and Biometric Characteristics of PanOptix and Odyssey IOLs in Fellow Eyes (Mean ± Standard Deviation [Min-Max]) |
Visual Acuity
Postoperative VA outcomes for both IOLs are summarized in Table 2. There were statistically significant mean differences (PanOptix – Odyssey) favoring the Odyssey eye in CDVA (EMD=0.03 logMAR, 95% CI [0.01, 0.06], P=0.009) and UCDVA (EMD=0.06 logMAR, 95% CI [0.01, 0.12], P=0.03). Conversely, the PanOptix eye demonstrated significantly better DCIVA (EMD=−0.05 logMAR, 95% CI [−0.09, −0.01], P=0.03). No significant differences were observed for DCNVA, UCIVA, and UCNVA between the two IOLs (all P≥0.07).
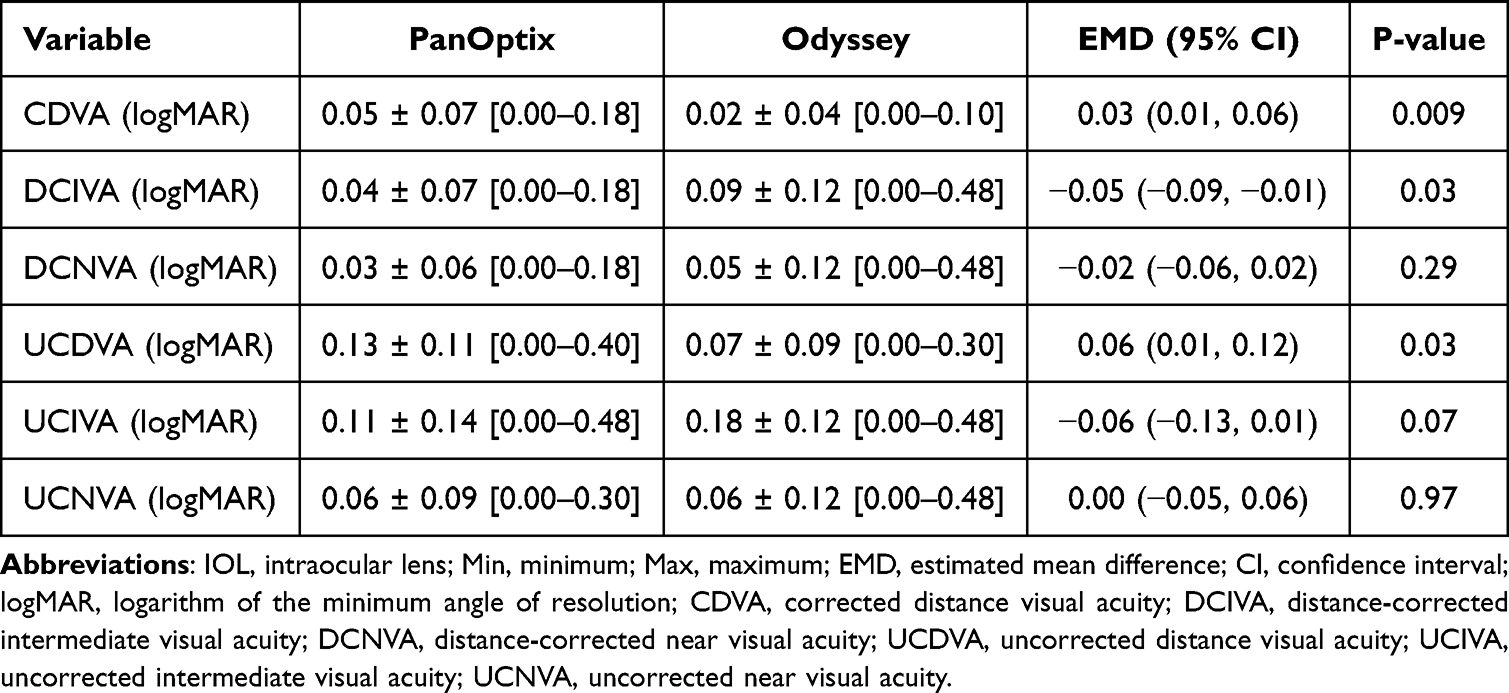 |
Table 2 Comparison of Visual Acuity Outcomes (LogMAR) Between PanOptix and Odyssey IOLs Across Multiple Distances (Mean ± Standard Deviation [Min-Max]) |
Figure 1 illustrates cumulative corrected VA distributions for both IOLs at various distances. For distance vision at 4 m (Figure 1A), 100% of patients implanted with Odyssey achieved a CDVA of 0.1 logMAR or better, compared to 0.2 logMAR or better with PanOptix. For intermediate vision at 60 cm (Figure 1B), 100% of patients with PanOptix reached 0.2 logMAR or better, whereas the Odyssey eye achieved 100% at 0.5 logMAR or better. Near vision at 40 cm (Figure 1C) showed comparable cumulative VA outcomes between both IOLs, with the PanOptix eye achieving 100% at 0.2 logMAR or better and the Odyssey eye at 0.5 logMAR or better.
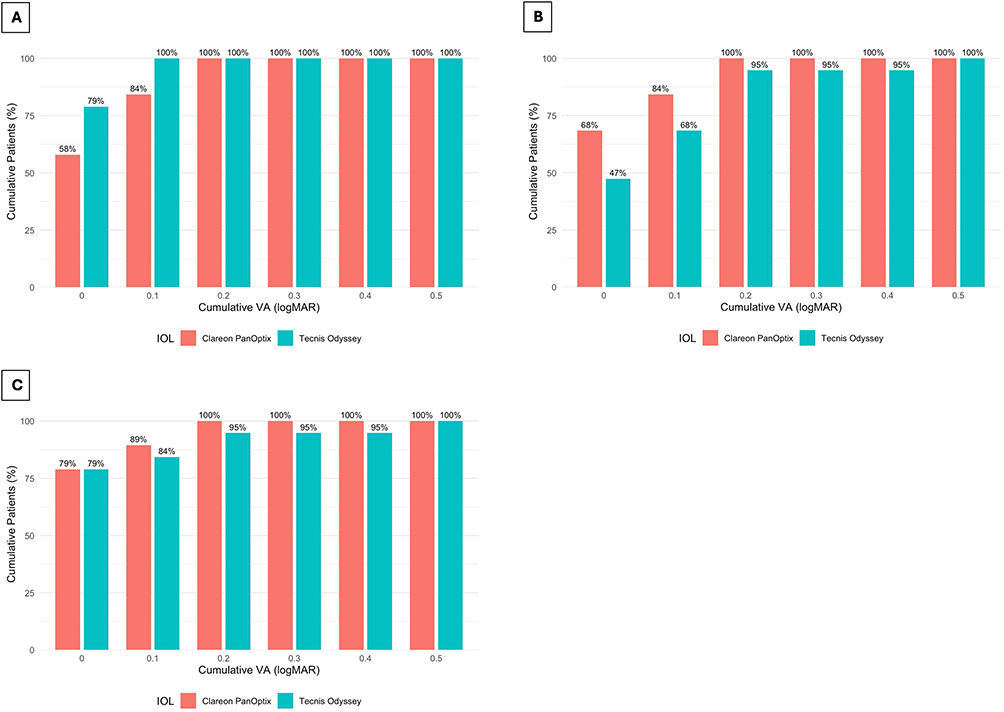 |
Figure 1 Cumulative percentage of patients achieving distance-corrected VA at (A) distance at 4 m, (B) intermediate at 60 cm, and (C) near at 40 cm. Abbreviations: VA, visual acuity. |
Residual Refractive Outcome and Contrast Sensitivity
Residual refractive spherical equivalents showed no significant differences between eyes implanted with PanOptix (−0.10 ± 0.52 D) and Odyssey (−0.09 ± 0.30 D; EMD=−0.01 D, 95% CI [−0.24, 0.22], P=0.91; Table 3). However, the Odyssey eye demonstrated significantly higher composite CS scores on the CSV-1000, which reflects summed performances across 3, 6, 12, and 18 cpd (EMD=−5.47, 95% CI [−10.50, −0.42], P=0.03; Table 3).
 |
Table 3 Postoperative Refractive Outcome and Contrast Sensitivity (Mean ± Standard Deviation [Min-Max]) |
Photic Phenomena and Spectacle Independence
In the PanOptix eye, starburst, halo, and glare were reported by 6 (31.58%), 7 (36.84%), and 6 (31.58%) of the 19 respondents, respectively. In the Odyssey eye, starburst, halo, and glare were reported by 5 (26.32%), 6 (31.58%), and 6 (31.58%) of the 19 respondents, respectively. Patient-reported visual disturbances did not differ significantly between the two IOLs, as demonstrated by the comparable frequencies and nonsignificant odds ratios (starburst: OR=1.28, 95% CI [0.77, 2.14], P=0.34; halo: OR=1.26, 95% CI [0.78, 2.03], P=0.34; glare: OR=1.00, 95% CI [0.49, 2.05], P=1.00; Table 4). Furthermore, spectacle independence was achieved by 17 of 19 patients (89.47%), while two patients required spectacles for both eyes irrespective of the IOL type (Table 4).
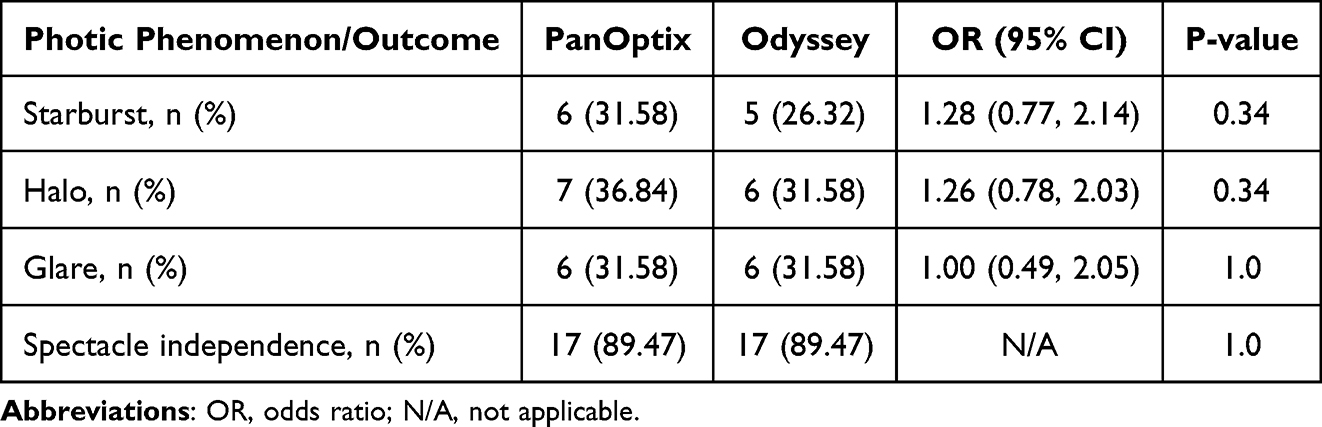 |
Table 4 Postoperative Photic Phenomena and Spectacle Independence |
Patient-Reported Visual Quality in Daily Life
Figure 2 summarizes patient-reported difficulties in daily visual tasks as assessed by the VF-7 questionnaire. The majority of patients reported minimal or no difficulty with tasks such as cooking, watching television, and navigating steps or curbs, with 17 out of 19 respondents indicating these tasks were “not applicable” and 2 reporting only “a little” difficulty for each. For fine handwork, 3 of 19 patients reported “a little” difficulty, while one reported “a great deal” of difficulty and another was “unable to perform” the task with both eyes. Night driving posed more challenge: 5 of 19 patients reported “a little” difficulty with both eyes equally, and another 5 reported “a moderate amount.” Among these, 3 patients attributed the difficulty more to the PanOptix eye and 1 to the Odyssey eye. In reading small print, 8 patients reported “a little” difficulty, with one each reporting “a moderate amount,” “a great deal,” or being “unable to perform” the task, all equally affecting both eyes. For reading traffic signs, street signs, or store signs, 3 patients reported “a moderate amount” of difficulty. One of these individuals attributed the difficulty specifically to the Odyssey eye; notably, this was the same patient who reported moderate night-driving difficulty associated with Odyssey.
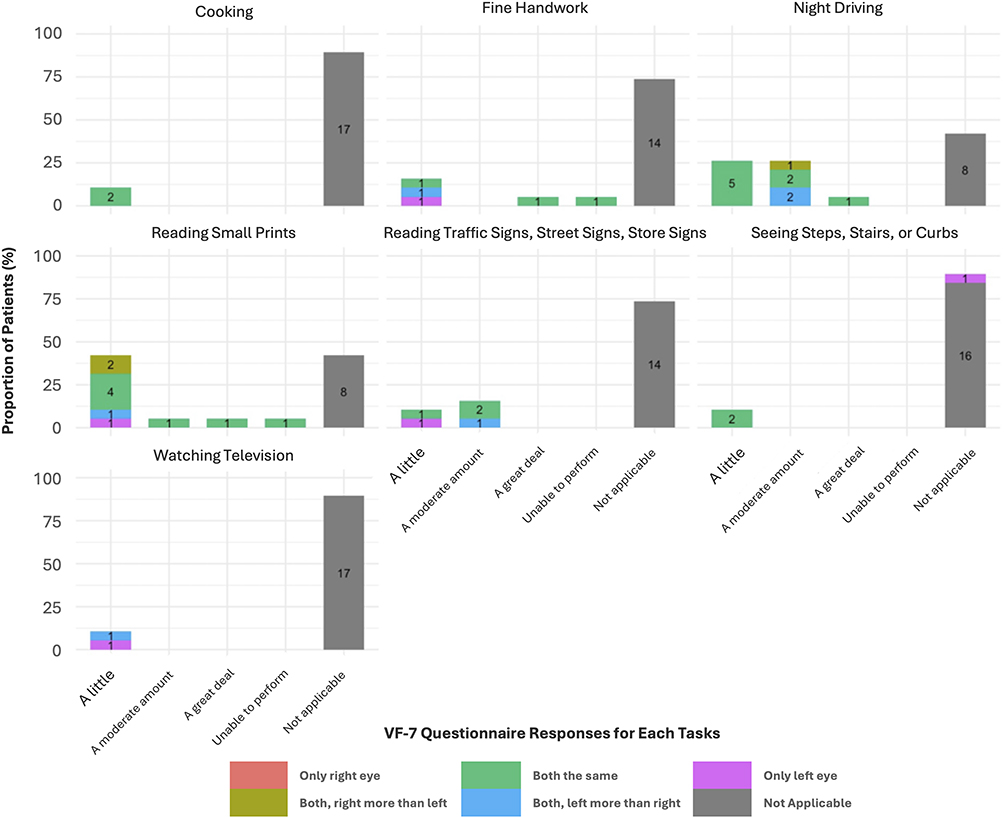 |
Figure 2 Patient responses to VF-7 Questionnaire. |
Discussion
While monofocal IOLs remain the most commonly implanted lenses for cataract surgery,21 the global demand for premium IOLs, including both multifocal and EDoF technologies, particularly among presbyopic patients seeking spectacle independence, is increasing.22 Recent meta-analyses have demonstrated that trifocal IOLs offer superior near vision compared to other premium lenses like EDoF, effectively addressing presbyopia-related accommodation loss.7,23,24 This study aimed to provide an initial comparative evaluation of the relatively newer Odyssey trifocal IOL against the widely used PanOptix trifocal IOL.
The PanOptix IOL, with its HEMA material and unique diffractive optical design, aims to enhance intermediate VA while maintaining visual quality. Our findings align with prior studies,19,25 confirming statistically significant superiority in DCIVA by 0.05 logMAR on average for PanOptix. Patient-reported photic phenomena in the PanOptix eye ranged from 31.58% to 36.84%, consistent with a recent multicenter study reporting a 37.5% incidence.26 Although direct comparisons of spectacle independence rates across studies are challenging due to variability in assessment methods, overall spectacle independence in this study reached 89.47%, comparable to previously reported rates.27,28
In contrast, the Odyssey eye showed significantly better CDVA by 0.03 logMAR on average. However, contrary to bench-testing data reporting superior near VA for Odyssey,17 this study found no significant difference in DCNVA between the two IOLs. This study recorded patient-reported photic phenomena as dichotomous (yes or no) responses, in contrast to the manufacturer’s data, which categorized visual symptoms based on severity levels (none/mild, moderate, or severe). Therefore, direct comparisons are challenging. However, the manufacturer’s one-month postoperative data indicate relatively low percentages of moderate-to-severe visual disturbances (halos: 7%, glare: 6%, starbursts: 0%),29 whereas this study found higher overall rates when severity was not considered (halos: 31.58%, glare: 31.58%, starbursts: 26.32%). However, the occurrence of these disturbances between the two IOLs were not significantly different. Both IOLs achieved identical spectacle independence rates of 89.47%, indicating comparable multifocality efficacy. Also, both IOLs demonstrated comparable postoperative residual spherical equivalent of −0.10 ± 0.52 D for the PanOptix eye and −0.09 ± 0.30 D for the Odyssey eye. The PanOptix results were similar compared to previous study results done at one month follow-up.20,30
The VF-7 questionnaire revealed minimal difficulty with daily tasks such as cooking, watching television, and navigating steps or curbs for both IOLs. However, tasks requiring high acuity at close range, such as fine handwork and reading small print, presented greater challenges, while night driving was notably problematic, with some patients attributing it to either their PanOptix or Odyssey eye. These findings align with prior research using modified Visual Function Quality of Life Questionnaire (VF-14 QOL), which also identified night driving and reading small print as the most challenging tasks for patients following trifocal IOL implantation.31 These challenges may be attributed to the diffractive optics of trifocal IOLs, which can disperse light across multiple focal points, potentially reducing CS.32
A key finding was the significantly better CS in the Odyssey eye compared to the PanOptix eye. A possible hypothesis explaining the relatively lower CS experienced by patients with PanOptix compared to Odyssey might relate to differences in diffracted light distribution across focal points. Specifically, PanOptix employs a trifocal diffractive design with three principal focal peaks at distance, 60 cm, and 40 cm, along with an additional intermediate enhancement around 120 cm. In contrast, the Odyssey lens uses a hybrid multifocal-EDoF diffractive profile that allocates more energy toward the distance focal point while providing a continuous extended intermediate range. This stronger emphasis on the distance focus may help preserve retinal illumination for distance tasks, potentially contributing to the superior CDVA and CS measured at 2.5 m with the CSV-1000. Conversely, the PanOptix design may distribute relatively more light toward intermediate and near focal points, potentially reducing retinal illumination available for distance vision, thereby compromising distance CS compared to Odyssey.
This study has several limitations that warrant consideration. The small sample size, consistent with an exploratory pilot study, reduces the statistical power to detect subtle yet clinically meaningful differences between the two IOLs. Therefore, these findings should be interpreted as preliminary and validated in larger, powered prospective trials. Moreover, the limited number of participants may exaggerate percentage-based differences, potentially overstating the clinical relevance of the observed variations. To reduce eye-dominance-related bias, patients were stratified by ocular dominance and randomized to determine IOL allocation for the dominant eye. However, the strength of dominance was not quantified, meaning its potential influence on distance vision could not be fully controlled. Additionally, we did not perform a defocus curve assessment, which could have provided valuable comparative information, as our primary focus was the visual outcome of the three focal lengths of the two trifocal IOLs. Regarding patient satisfaction, although we used the validated VF-7 questionnaire, participants in this paired-eye design may have struggled to attribute specific visual disturbances to a single eye, complicating interpretation of subjective outcomes. Future studies could address this limitation through simulated or technology-assisted monocular testing under controlled conditions. We also recommend considering bilateral implantation and paired-eye designs as separate study arms for a more comprehensive comparison. Finally, postoperative positive dysphotopsias have been reported to diminish significantly by the 12-month follow-up compared to the 3-month assessment.33 However, this study was not able to validate this trend as patient satisfaction was evaluated within a shorter postoperative window. It has been suggested that neuroadaptation over extended periods plays an essential role in reducing the subjective perception of visual disturbances.34 These findings suggest that the limitation of trifocal IOLs may decrease over time while preserving their visual benefits, consistent with prior studies reporting stable vision with trifocal IOLs.20,35 Therefore, future longitudinal studies evaluating Odyssey over extended postoperative periods may reveal improvements in subjective visual quality, as neuroadaptation may mitigate perceived disturbances. Also, as trifocal IOL technology continues to evolve, ongoing research comparing emerging designs with existing platforms remains essential.
In conclusion, PanOptix demonstrated superior DCIVA, while Odyssey provided superior CDVA and higher CS. Both IOLs resulted in high spectacle independence and overall patient satisfaction. Based on VF-7 responses, the most commonly reported residual visual difficulties for both lenses involved night driving and reading small print, which are recognized challenges with diffractive presbyopia-correcting IOLs. Overall, both the PanOptix and Odyssey platforms appear to be viable options for presbyopic patients seeking spectacle independence.
Acknowledgments
We would like to thank Alberta Pengo, OD and Julia Rose Campbell, OD at Bascom Palmer Eye Institute for their collaboration and support.
Author Contributions
All authors made significant contributions to the conception, study design, execution, data acquisition, analysis, and interpretation of the work reported. SK, SMA, and RCO performed the statistical analyses. SK drafted the manuscript, and all authors critically reviewed and revised subsequent versions. All authors gave final approval of the version to be published, agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work.
Disclosure
Dr Robert O’Brien reports personal fees for statistical consultation from University Hospitals Cleveland Medical Center, outside the submitted work. Prof. Dr. Sonia Yoo reports personal fees for consultancy from Carl Zeiss Meditec, Johnson and Johnson, and Alcon Labs, outside the submitted work. The authors have no other conflicts of interest or financial support to disclose for this work.
References
1. Stern B, Gatinel D. Presbyopia correction in lens replacement surgery: a review. Clin Exp Ophthalmol. 2025;53(6):668–10. doi:10.1111/ceo.14535
2. Sudhir RR, Dey A, Bhattacharrya S, Bahulayan A. AcrySof IQ panoptix intraocular lens versus extended depth of focus intraocular lens and trifocal intraocular lens: a clinical overview. Asia Pac J Ophthalmol. 2019;8(4):335–349. doi:10.1097/apo.0000000000000253
3. Ni W, Li X, Hou Z, Zhang H, Qiu W, Wang W. Impact of cataract surgery on vision-related life performances: the usefulness of real-life vision test for cataract surgery outcomes evaluation. Eye. 2015;29(12):1545–1554. doi:10.1038/eye.2015.147
4. Martínez de Carneros-Llorente A, Martínez de Carneros A, Martínez de Carneros-Llorente P, Jiménez-Alfaro I. Comparison of visual quality and subjective outcomes among 3 trifocal intraocular lenses and 1 bifocal intraocular lens. J Cataract Refract Surg. 2019;45(5):587–594. doi:10.1016/j.jcrs.2018.12.005
5. Li J, Sun B, Zhang Y, et al. Comparative efficacy and safety of all kinds of intraocular lenses in presbyopia-correcting cataract surgery: a systematic review and meta-analysis. BMC Ophthalmol. 2024;24(1):172. doi:10.1186/s12886-024-03446-1
6. Greenstein S, Pineda R. The quest for spectacle independence: a comparison of multifocal intraocular lens implants and pseudophakic monovision for patients with presbyopia. Semin Ophthalmol. 2017;32(1):111–115. doi:10.1080/08820538.2016.1228400
7. Karam M, Alkhowaiter N, Alkhabbaz A, et al. Extended depth of focus versus trifocal for intraocular lens implantation: an updated systematic review and meta-analysis. Am J Ophthalmol. 2023;251:52–70. doi:10.1016/j.ajo.2023.01.024
8. Zamora-de La Cruz D, Zúñiga-Posselt K, Bartlett J, Gutierrez M, Abariga SA. Trifocal intraocular lenses versus bifocal intraocular lenses after cataract extraction among participants with presbyopia. Cochrane Database Syst Rev. 2020;6(6):Cd012648. doi:10.1002/14651858.CD012648.pub2
9. Schallhorn JM. Multifocal and extended depth of focus intraocular lenses: a comparison of data from the United States food and drug administration premarket approval trials. J Refract Surg. 2021;37(2):98–104. doi:10.3928/1081597x-20201111-02
10. Cao K, Friedman DS, Jin S, et al. Multifocal versus monofocal intraocular lenses for age-related cataract patients: a system review and meta-analysis based on randomized controlled trials. Surv Ophthalmol. 2019;64(5):647–658. doi:10.1016/j.survophthal.2019.02.012
11. de Silva SR, Evans JR, Kirthi V, Ziaei M, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2016;12(12):Cd003169. doi:10.1002/14651858.CD003169.pub4
12. Mencucci R, Favuzza E, Caporossi O, Savastano A, Rizzo S. Comparative analysis of visual outcomes, reading skills, contrast sensitivity, and patient satisfaction with two models of trifocal diffractive intraocular lenses and an extended range of vision intraocular lens. Graefes Arch Clin Exp Ophthalmol. 2018;256(10):1913–1922. doi:10.1007/s00417-018-4052-3
13. Clareon PanOptix IOL Product Information. Alcon laboratories, Inc. Available from: https://www.myalcon.com/professional/cataract-surgery/iols/clareon-panoptix/.
14. Kohnen T, Herzog M, Hemkeppler E, et al. Visual performance of a quadrifocal (Trifocal) intraocular lens following removal of the crystalline lens. Am J Ophthalmol. 2017;184:52–62. doi:10.1016/j.ajo.2017.09.016
15. Carson D, Xu Z, Alexander E, Choi M, Zhao Z, Hong X. Optical bench performance of 3 trifocal intraocular lenses. J Cataract Refract Surg. 2016;42(9):1361–1367. doi:10.1016/j.jcrs.2016.06.036
16. Hovanesian JA, Jones M, Allen Q. The clareon vs acrysof panoptix trifocal IOL: a comparative study of patient satisfaction and visual performance. Clin Ophthalmol. 2024;18:2977–2984. doi:10.2147/opth.S476666
17. DOF2023CT4023: Bench and Clinical Evaluation of the TECNIS Odyssey™ IOL. Jacksonville, FL: Johnson & Johnson Vision; 2023.
18. Bissen-Miyajima H, Midorikawa M, Fujisaki R, Ota Y, Minami K, Honda R. Early clinical results of a newly developed continuous range of vision intraocular lens. Ophthalmol Ther. 2025;14(11):2937–2945. doi:10.1007/s40123-025-01235-7
19. Kohnen T, Lapid-Gortzak R, Ramamurthy D, et al. Clinical outcomes after bilateral implantation of a diffractive trifocal intraocular lens: a worldwide pooled analysis of prospective clinical investigations. Clin Ophthalmol. 2023;17:155–163. doi:10.2147/opth.S377234
20. Mendicute J, Lauzirika G, Illarramendi I, Martínez-Soroa I. Visual, refractive, functional, and patient satisfaction outcomes after implantation of a new trifocal diffractive intraocular lens. Clin Ophthalmol. 2024;18:2785–2795. doi:10.2147/opth.S480311
21. Hu JQ, Sarkar R, Sella R, Murphy JD, Afshari NA. Cost-effectiveness analysis of multifocal intraocular lenses compared to monofocal intraocular lenses in cataract surgery. Am J Ophthalmol. 2019;208:305–312. doi:10.1016/j.ajo.2019.03.019
22. Sieburth R, Chen M. Intraocular lens correction of presbyopia. Taiwan J Ophthalmol. 2019;9(1):4–17. doi:10.4103/tjo.tjo_136_18
23. Tavassoli S, Ziaei H, Yadegarfar ME, et al. Trifocal versus extended depth of focus (EDOF) intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2024;7(7):Cd014891. doi:10.1002/14651858.CD014891.pub2
24. Zhong Y, Wang K, Yu X, Liu X, Yao K. Comparison of trifocal or hybrid multifocal-extended depth of focus intraocular lenses: a systematic review and meta-analysis. Sci Rep. 2021;11(1):6699. doi:10.1038/s41598-021-86222-1
25. Kohnen T, Marchini G, Alfonso JF, et al. Innovative trifocal (quadrifocal) presbyopia-correcting IOLs: 1-year outcomes from an international multicenter study. J Cataract Refract Surg. 2020;46(8):1142–1148. doi:10.1097/j.jcrs.0000000000000232
26. Jo E, Kim B, Kim TI, Kim MK, Choi CY. Clinical outcomes of a new hydrophobic trifocal intraocular lens with hydroxyethyl methacrylate in cataract surgery: a prospective multicenter study. Korean J Ophthalmol. 2024;38(3):212–220. doi:10.3341/kjo.2023.0140
27. Newsom TH, Szabo B, Unsell K, Newsom C, Newsom BA, Hall B. Visual outcomes and quality of vision after bilateral implantation of a hydrophobic acrylic trifocal intraocular lens. Clin Ophthalmol. 2025;19:227–234. doi:10.2147/opth.S506516
28. Blehm C, Potvin R. Reported patient satisfaction and spectacle independence following bilateral implantation of the PanOptix(®) trifocal intraocular lens. Clin Ophthalmol. 2021;15:2907–2912. doi:10.2147/opth.S323337
29. DOF2023CT4050: based on 1-month postoperative data from a multicenter, retrospective, real-world clinical study conducted in the united states evaluating visual and patient-reported outcomes from subjects bilaterally implanted with TECNIS Odyssey™ IOL (n=96). Johnson & johnson vision. 2023.
30. Lee YW, Choi CY, Moon K, et al. Clinical outcomes of new multifocal intraocular lenses with hydroxyethyl methacrylate and comparative results of contrast sensitivity, objective scatter, and subjective photic phenomena. BMC Ophthalmol. 2022;22(1):379. doi:10.1186/s12886-022-02600-x
31. Brissette A, Cole B, Hall B. Visual function after implantation of trifocal and trifocal toric intraocular lenses using intraoperative aberrometry. Clin Ophthalmol. 2024;18:1547–1554. doi:10.2147/opth.S450979
32. Pieh S, Weghaupt H, Skorpik C. Contrast sensitivity and glare disability with diffractive and refractive multifocal intraocular lenses. J Cataract Refract Surg. 1998;24(5):659–662. doi:10.1016/s0886-3350(98)80261-7
33. Rementería-Capelo LA, Contreras I, Gros-Otero J, Mariñas L, Ruiz-Alcocer J. Visual quality, patient satisfaction, and photic phenomena with a diffractive intraocular lens and its new evolved materials version. J Refract Surg. 2024;40(11):e877–e883. doi:10.3928/1081597x-20240923-02
34. Oliveira RF, Vargas V, Plaza-Puche AB, Alió JL. Long-term results of a diffractive trifocal intraocular lens: visual, aberrometric and patient satisfaction results. Eur J Ophthalmol. 2020;30(1):201–208. doi:10.1177/1120672118818019
35. Bissen-Miyajima H, Ota Y, Hayashi K, Igarashi C, Sasaki N. Results of a clinical evaluation of a trifocal intraocular lens in Japan. Jpn J Ophthalmol. 2020;64(2):140–149. doi:10.1007/s10384-019-00712-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Optical Biometry and Lens Power Calculations in 500 Phakic Patients: Axial Length and Corneal Curvature in the Fellow Eye
Kristianslund O, Hassaf SE, Drolsum L
Clinical Ophthalmology 2022, 16:2775-2780
Published Date: 23 August 2022
Visual and Refractive Efficacy of Panoptix Toric Intraocular Lens in a Clinical Setting
Ackerman M, Lawless M, Levitz L, Bhatt U, Reich JA, Sutton G, Roberts TV, Tenen A, Kaur A, Hodge C
Clinical Ophthalmology 2022, 16:4227-4237
Published Date: 19 December 2022
Clinical Outcomes of a New Non-Diffractive Extended Depth-of-Focus Intraocular Lens Targeted for Mini-Monovision
Tomagova N, Elahi S, Vandekerckhove K
Clinical Ophthalmology 2023, 17:981-990
Published Date: 25 March 2023
Comparing the Accuracy of the Kane, Barrett Universal II, Hill-Radial Basis Function, Emmetropia Verifying Optical, and Ladas Super Formula Intraocular Lens Power Calculation Formulas
Moshirfar M, Sulit CA, Brown AH, Irwin C, Ronquillo YC, Hoopes PC
Clinical Ophthalmology 2023, 17:2643-2652
Published Date: 7 September 2023
Clinical Outcomes of a Monofocal, Optimized, Aspheric, Hydrophobic Acrylic Intraocular Lens Implant
García-Tomás B, Marín-Sánchez JM, García-Elskamp C, Alcon-Ruiz E, Montesinos-López L, García Martínez-Lozano B
Clinical Ophthalmology 2023, 17:3215-3224
Published Date: 27 October 2023