Back to Journals » Clinical Ophthalmology » Volume 17
Clinical Outcomes of a New Non-Diffractive Extended Depth-of-Focus Intraocular Lens Targeted for Mini-Monovision
Authors Tomagova N, Elahi S, Vandekerckhove K ![]()
Received 6 February 2023
Accepted for publication 13 March 2023
Published 25 March 2023 Volume 2023:17 Pages 981—990
DOI https://doi.org/10.2147/OPTH.S405267
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nikola Tomagova,* Sina Elahi, Kristof Vandekerckhove*
Clinical Study Department, Vista Alpina Eye Clinic, Visp, Switzerland
*These authors contributed equally to this work
Correspondence: Kristof Vandekerckhove, Clinical Study Department, Vista Alpina Eye Clinic, Bahnhofplatz 1a, Visp, 3930, Switzerland, Tel +41279467000, Email [email protected]
Purpose: To assess visual acuity, binocular defocus curve, spectacle independence, and photic phenomena after bilateral same-day cataract surgery with implantation of an extended depth-of-focus intraocular lens (IOL) with mini-monovision.
Methods: Single-center retrospective study including 124 eyes from 62 patients who underwent bilateral implantation of an isofocal EDOF lens [Isopure® (BVI)] with mini-monovision (− 0.50 D). Refraction, visual acuity at different distances, binocular defocus curves, spectacle independence, and subjective ratings of picture-referenced photic phenomena were assessed one to two months postoperatively.
Results: The mean postoperative refractive spherical equivalent was − 0.15± 0.41D in the dominant eyes and − 0.46± 0.35D in the mini-monovision eyes (p< 0.01). Overall, 98.4% and 87.7% of the eyes were within ± 1.00D and ± 0.50D of the target refraction, respectively. Postoperative monocular corrected distance visual acuity was − 0.04± 0.07 logMAR. Binocular uncorrected visual acuity was − 0.02± 0.07, 0.13± 0.11and 0.40± 0.20 logMAR for far, intermediate and near, respectively. At the visual acuity threshold of 0.20 logMAR (or better) the defocus curve ranged from − 1.6D to +0.9D. Reported spectacle-independence was 96% for far distance, 95% for intermediate, and 34% for near. Five percent of patients reported halos, 16% starburst, and 16% glare. Only 7% of all patients considered them bothersome.
Conclusion: In patients undergoing same-day bilateral cataract surgery, an isofocal EDOF lens provided an extended range of functional vision, up to 63 cm, resulting in useful uncorrected near vision, good uncorrected intermediate vision, and excellent uncorrected distance vision. Subjective patient satisfaction in terms of spectacle independence and photic phenomena was high.
Keywords: EDOF, extended-depth-of-focus, mini-monovision, same-day bilateral cataract surgery, Isopure
Introduction
With growing patient expectation of spectacle-independence after cataract surgery, more and more IOL designs are being introduced that aim to provide good uncorrected visual acuity at various distances while minimizing photic phenomena. Extended depth-of-focus (EDOF) IOLs create a single elongated focal point that extends the range of vision and are therefore associated with fewer photic phenomena1 than multifocal IOLs, which split the light into two or three foci creating overlapping images. Trifocal IOLs are more effective in improving unaided vision across the entire range of distances but are associated with a higher rate of photic phenomena, whereas EDOF IOLs and monofocal IOLs with monovision provide partial spectacle independence with fewer photic phenomena.2
A proposed option to increase the range of uncorrected vision is to leave one eye slightly myopic, ie, to induce monovision. Pseudophakic monovision has been used by several authors who achieved comparable visual outcomes and spectacle independence as with multifocal IOLs, but with less dysphotopsia.3 Mini-monovision aims to further minimize photic phenomena and loss of stereopsis by using a smaller dioptric power difference between the two eyes than traditional monovision. For two of the EDOF IOLs available on the market, the use of mini-monovision has been found to significantly improve uncorrected binocular visual acuity and spectacle independence.4–16
Isopure® is a hydrophobic aspheric non-diffractive IOL. Its EDOF properties are based on a polynomial surface design across the full optic providing a high amount of negative spherical aberrations, smoothly increasing from the center to the periphery of the optic. This modification of the spherical aberrations is known as isofocal technology. Only limited clinical data are currently available: Stodulka et Slovak17 reported promising results in terms of visual acuity and contrast in a small cohort of patients (n=18) as did Bova et Vita18 (n=21). Neither study used mini-monovision.
The aim of our study was therefore to evaluate visual acuity, defocus curves, patient-reported spectacle-independence and occurrence of photic phenomena after bilateral implantation of an isofocal EDOF lens with mini-monovision in a large cohort of cataract patients.
Patients and Methods
Patients
This was a single-center retrospective clinical study including 124 eyes from 62 patients undergoing routine bilateral same-day cataract surgery performed by a single surgeon (KV), with implantation of the isofocal EDOF lens. The study conforms to the Declaration of Helsinki and was approved by the local Ethics Committee (Commission Cantonale d’Ethique de la Recherche sur l’être humain, Lausanne, CER-VD 2021–02273). Informed consent was obtained from each patient for the procedures and for the use of de-identified clinical data.
Medical records of all consecutive patients aged 50 years or older, who underwent routine bilateral cataract surgery with the isofocal EDOF lens between March 2021 and November 2021 were reviewed, and patients without other vision-impairing comorbidities and with a regular corneal astigmatism of 1.5D or less were included in the study. Exclusion criteria were extraocular or intraocular vision-impairing comorbidities (maculopathies, retinopathies, advanced glaucoma or other retinal or optic nerve disorders, corneal pathologies, or amblyopia), an irregular cornea (including keratotomy), and non-age-related cataracts (congenital, uveitic, traumatic, or secondary). All reviewed patients, and reasons for exclusion were recorded in a monitoring log.
Study Design
All patients underwent immediate sequential bilateral phacoemulsification cataract surgery. Ocular biometry and corneal astigmatism (total corneal power) measurement was performed with an anterior optical coherence tomography biometer (Anterion, Heidelberg Engineering) and IOL power was calculated using the Barrett Universal II formula for most patients, modified by the Haigis-L, SRK/T and Hoffer Q formulas depending on the anatomy of each eye. All patients were targeted for mini-monovision of −0.50 D in the nondominant eye and emmetropia in the dominant eye. In eyes with corneal astigmatism of 0.6 D to 1.5 D, opposite clear corneal incisions were applied to reduce astigmatism. Patients were then examined one day, one week, and one to two months after surgery. At the last postoperative examination, uncorrected monocular and binocular distance (UDVA), intermediate (UIVA), and near (UNVA) visual acuity were assessed at 4 m, 80 cm and 33 cm, respectively. Monocular corrected distance visual acuity (CDVA) was also measured. Binocular distance-corrected defocus curves were then obtained in 0.5 D increments from +2.00 to −3.0 D defocus.
Patient-reported spectacle independence at various distances was assessed using an abbreviated PRSIQ19 questionnaire with a scale ranging from 0 (never comfortable without glasses) to 4 (always comfortable without glasses). Patients who were “almost always” or “always” comfortable without glasses were considered to be spectacle-independent at a given distance. Photic phenomena were assessed at the last postoperative visit (one to two months after surgery) using a modified and prompted NEI Quality of Vision questionnaire (RQL-42). Patients were shown pictures of halos, glare and starburst during the interview (see Appendix I).
Statistical Analysis
Statistical analysis included descriptive data for demographic characteristics, visual and refractive outcomes, and questionnaire results. All mean values are expressed as mean ± standard deviation. Student’s t-test, ANOVA, and logistic regression analyses were used to analyze data where appropriate. Statistical analysis was performed using Stata software (StataCorp 2019). Results with p values < 0.05 were considered statistically significant.
Results
Of the sixty-two patients (124 eyes) included in our study, 27 (44%) were female. The mean age at the time of the surgery was 70.6±7.4 years. Cataract surgery was uneventful in all cases.
Refractive Error Outcomes
One to two months after surgery, the mean manifest refractive spherical equivalent (MRSE) was −0.15±0.41D in the dominant eyes and −0.46±0.35D in the mini-monovision eyes (p<0.01). The pre-and postoperative refractive outcomes are summarized in Table 1. Figure 1 shows the postoperative distribution of the MRSE, showing the deviation from target refraction (0 D for the dominant eye and −0.50 D for the non-dominant eye). Overall, 98.4% and 87.7% of the eyes were within ±1.00D and ±0.50D of the target refraction, respectively.
 |
Table 1 Refractive and Visual Acuity Outcomes |
 |
Figure 1 Distribution of postoperative spherical equivalent in diopters for dominant and mini-monovision eyes. Note that the target refraction was emmetropia for the dominant eyes and −0.50 D for the mini-monovision eyes. The percentages of eyes within ±1.00 D and ±0.50 D of the target refraction are also shown. |
Visual Acuities and Defocus Curve
Table 1 also summarizes preoperative and postoperative visual acuities. Monocular CDVA improved by 3 lines from 0.26±0.17 logMAR (~Snellen 20/40) preoperatively to −0.04±0.07 logMAR (~20/20 Snellen) measured one to two months post-surgery. Postoperative binocular UDVA, UIVA and UNVA were −0.02±0.07 logMAR, 0.13±0.11 logMAR, and 0.40±0.20 logMAR. Figure 2 shows the cumulative binocular UDVA, UIVA, and UNVA values, monocular UDVA for the dominant and non-dominant eyes, as well as overall monocular CDVA. After surgery, 77% of patients had binocular UDVA of 20/20 or better (≤0.00 logMAR). At intermediate distance, 58% of patients had binocular UIVA of 20/25 or better (≤0.10 logMAR), and at near distance, 51% of patients achieved binocular UNVA of 20/40 or better (≤0.30 logMAR). On monocular testing, 84% and 98% of eyes had a CDVA of 20/20 or better (≤0.00 logMAR) and 20/25 or better (≤0.10 logMAR), respectively, demonstrating the safety of the isofocal EDOF lens. Figure 3 shows the mean monocular CDVA and the binocular UDVA, UIVA, and UNVA.
 |
Figure 2 (A) Cumulative binocular uncorrected visual acuity for distance (bin. UDVA), (B) intermediate (bin. UIVA), and (C) near (bin. UNVA). (D) Cumulative monocular uncorrected distance visual acuity (UDVA) for dominant and non-dominant eyes, and corrected distance visual acuity (CDVA) for all eyes. One to two months after surgery. |
 |
Figure 3 Mean ± standard deviation of monocular corrected distance visual acuity (CDVA),binocular uncorrected distance visual acuity (UDVA), binocular uncorrected intermediate visual acuity (UIVA), and binocular uncorrected near visual acuity (UNVA) one to two months after surgery. |
Figure 4 shows the postoperative photopic distance-corrected binocular visual acuities from +2.0 D to −3.0 D defocus. The binocular defocus curve exhibits a smooth slope over the tested range of diopters . Patients had 0.20 logMAR or better visual acuity between −1.6 D to + 0.9 D of defocus, corresponding to a theoretical range of vision of up to 63 cm.
 |
Figure 4 Distance-corrected binocular defocus curve. The left y-axis shows logMAR visual acuity and the right y-axis the Snellen equivalent. Error bars represent standard deviation. Abbreviation: D, diopters. |
Patient Satisfaction and Spectacle Independence
According to the PRSIQ questionnaire completed one to two months after surgery, 96% of patients felt comfortable seeing without glasses at far, 95% at intermediate, and 34% at near distances. The mean PRSIQ score for subjective reported spectacle-independence was 3.75±0.51, 3.75±0.74, and 1.91±1.30 for far, intermediate, and near, respectively. When shown images of photic phenomena, 5% (n=3/56) of patients reported halos, 16% (n=9/56) starburst, and 16% (n=9/56) glare. Only 7% (n=4/56) found these photic phenomena bothersome (Figure 5).
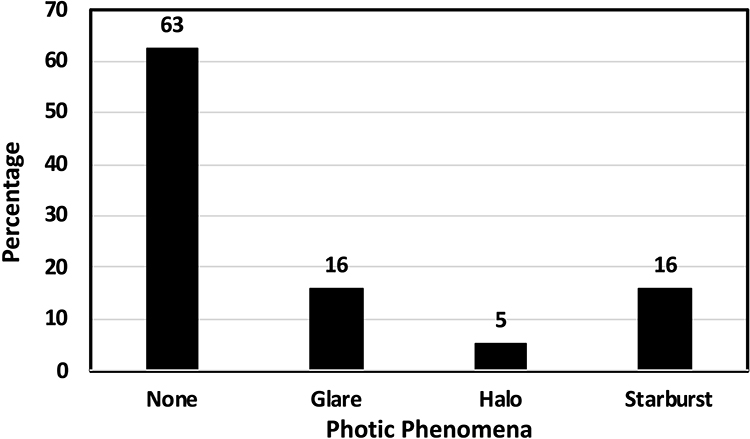 |
Figure 5 Percentage of patients reporting photic phenomena one to two months after surgery. Note: Patients were shown pictures of halos, glare and starburst during the interview. |
Discussion
This work is the first large cohort study of an isofocal EDOF lens to evaluate visual and refractive outcomes, spectacle independence, and the presence of photic phenomena. Aware of ongoing discussions about the correct definition of EDOF IOLs, in this paper we refer to “EDOF IOLs” in a broad clinical sense as IOLs that produce a single-elongated focal point that enhances depth-of-focus, as opposed to monofocal IOLs (one focal point) and multifocal IOLs (multiple discrete focal points).1
The isofocal EDOF lens was introduced in 2019, and there are few clinical data available to date. To our knowledge, there is one in-vitro study20 and two clinical studies with small samples.17,18 Łabuz et al20 performed an in-vitro comparison of four EDOF IOLs [Tecnis Eyhance ICB00 (Johnson and Johnson), AE2UV/ZOE (Eyebright Medical Technology), RayOne EMV (Rayner) and the isofocal EDOF lens (BVI)] and a standard monofocal lens [Tecnis ZCB00 (Johnson and Johnson)]. They found that the performance of the isofocal EDOF lens at −1.0 D was superior to that of the monofocal IOL. They also reported that its optical performance through a 3-mm pupil was minimally better than that of the other EDOF IOLs. These observations are clinically confirmed by the defocus curve in our study (see Figure 4). Stodulka et Slovak17 studied 18 patients implanted with the isofocal EDOF lens 4–6 months after surgery. In another small clinical study (n=21), Bova and Vita18 compared the isofocal EDOF lens with a monofocal IOL (Tecnis PCB00). Neither study used mini-monovision.
The mean postoperative MRSE in the dominant eyes (−0.15±0.41D) in our study was similar to the overall MRSE found by Stodulka17 (−0.15±0.51 D). We applied mini-monovision in all patients, with a target of −0.50 D in the non-dominant eye and achieved a postoperative MRSE of −0.46±0.35 D. Figure 1 shows that the postoperative MRSE of the dominant and mini-monovision eyes was close to their respective target refractions (0 and −0.50 D). A target refraction between −0.21 D and −0.63 D was reported by Jackson et al21 as the optimal range for nondominant eyes implanted with the Tecnis Symfony IOL (Johnson and Johnson) during bilateral cataract surgery. Using the same EDOF IOL with mini-monovision (target −0.50 D). Sevik et al14 obtained better binocular uncorrected visual performance at intermediate and near distances with Symfony and mini-monovision than with a low add multifocal IOL.
The defocus curve in our study revealed a smooth slope with gradually decreasing visual acuity over the defocus range (Figure 4). A visual acuity of 0.2 logMAR or better was achieved between −1.6 D and +0.9 D, similar to Stodulka et Slovak17 and better than Bova et Vita.18 The defocus curve of the Mini Well (SIFI S.p.A.) reported by Savini et al22 and that of the Tecnis Eyhance (Mencucci et al23 and Auffarth et al24) have similar characteristics. Bala et al25 and Chang et al,26 obtained visual acuity of 0.2 logMAR or better up to −2.0 D defocus with AcrySof IQ Vivity IOL (Alcon) and Symfony IOL.
Figure 2 provides the cumulative outcomes for visual acuity at different distances. Far vision (binocular UDVA) was 20/20 or better in 77% of patients and at intermediate distance, binocular UIVA was 20/25 or better in 58% of patients. Binocular UDVA and monocular CDVA reported in our study (−0.02 ± 0.07 and −0.04 ± 0.07 logMAR, respectively) are consistent with the results previously reported with the isofocal EDOF lens17 and slightly better than those obtained with other non-diffractive EDOF IOLs (AcrySof IQ Vivity13,25,27 and Tecnis Eyhance23,24) and diffractive EDOF IOLs [AT LARA 829MP (Carl Zeiss Meditec) and Tecnis Symfony].28
Figure 3 shows the mean values for different visual acuities. The binocular UIVA in our study (0.13 ± 0.11 logMAR) was similar to the findings of Stodulka et Slovak17 and better than the findings of Bova et Vita.18 Stodulka found a monocular CDVA of −0.06±0.04 logMAR and binocular intermediate visual acuities of 0.12±0.11 logMAR and 0.20±0.14 logMAR at 80 cm and 66 cm, respectively. Comparing the isofocal EDOF lens with a monofocal IOL (Tecnis PCB00), Bova and Vita18 found that the monocular and binocular CDVA and UDVA were similar, and that UIVA was significantly higher in the isofocal EDOF lens group (binocular UIVA 0.22±0.06 logMAR).
Stodulka17 and Bova18 did not report near vision outcomes, so our study is the first to report near vision outcomes with the isofocal EDOF lens. Binocular UNVA in our study was 0.40±0.20 logMAR. Of note, we measured near vision at a closer distance (33 cm) than in most clinical studies with EDOF IOLs (in which 40 cm is common). Despite the close testing distance, 51% of patients had a UNVA of 0.3 logMAR (20/40), which is often considered a threshold for reading. The binocular UIVA and UNVA results in our study with mini-monovision approach (0.13±0.11 and 0.40±0.20 logMAR, respectively) were comparable to those obtained with another non-diffractive EDOF IOL, Tecnis Eyhance, without mini-monovision (0.16±0.10 and 0.33±0.05 logMAR, respectively)23. Furthermore, binocular UIVA and UNVA in our study were similar to the 4-to-6-month results for the diffractive EDOF IOL Tecnis Symfony when no mini-monovision was used28 (0.11±0.14 and 0.30±0.17 logMAR, respectively). Tecnis Symfony with mini-monovision on the other hand achieved better UIVA and UNVA (−0.02±0.03 and 0.09±0.05 logMAR, respectively), and was as good as the diffractive trifocal IOL AT LISA Tri 839 MP.29 AcrySof IQ Vivity with mini-monovision approach provided better binocular UIVA at 66cm and UNVA at 40 cm (0.00 to 0.06 and 0.12 to 0.23)13,15,16 than the isofocal EDOF lens in our study. In another AcrySof IQ Vivity study without mini-monovision27 even the monocular UNVA was as high as 0.15±0.16 logMAR, but interestingly, all patients still needed an addition of at least +1.0 D for near. The better uncorrected intermediate and near visual acuities with AcrySof IQ Vivity IOL compared to other non-diffractive EDOF IOLs, including the isofocal EDOF lens, are likely due to its slightly greater depth of focus, as mentioned before.
To our knowledge, there are currently no published clinical data on photic phenomena after implantation of an isofocal EDOF lens. Approximately one-third of the patients in our study had experienced photic phenomena when interviewed in the early postoperative period (one to two months) (see Figure 5). Only one-fifth of these patients found them bothersome in daily life. The rates of halos (5%), glare (16%), and starburst (16%) were lower than the one-month data reported by Reinhard et al28 for the non-diffractive EDOF IOLs AT LARA 829MP (53% halos) and Tecnis Symfony (41% halos). Newsom et al13 used a recently developed QUVID questionnaire to assess photic phenomena in patients implanted with AcrySof IQ Vivity in combination with mini-monovision and noted high rates of halos (45%), glare (42%), and starburst (61%) three months after surgery. Slightly lower rates of photic phenomena were described by Arrigo et al30 using the McAlinden Quality of Vision Questionnaire three months after implantation of AcrySof IQ Vivity: 33% halos, 30% glare, and 18% starburst. The differences in the rates of photic phenomena between the studies could be due to different methods of questionnaire administration and their timing after surgery, as well as the use of mini-monovision. In our study, we showed images of photic phenomena (glare, halos and starburst) to the patients, which may have prompted more positive responses than a simple questionnaire. The duration of the postoperative neuroadaptation period also seems to play a role in the perception of photic phenomena, as suggested by Arrigo.30 In addition, ocular surface dryness due to postoperative topical treatment may contribute significantly to photic phenomena in the first weeks after surgery. Therefore, the rates of reported photic phenomena in our study can be deemed low compared to most other studies with EDOF or multifocal IOLs, considering the methodology (image-referenced) and timing (one to two months after surgery) of the questionnaire, as well as the use of mini-monovision.
Spectacle independence for far and intermediate (96% and 95%, respectively) was high. Spectacle-free near vision was achieved in 34% of patients. Twenty-nine percent of patients reported that they were comfortable without glasses at all three distances and can therefore be considered completely spectacle-free. Spectacle independence for intermediate and near distances was higher than reported for other non-diffractive EDOF IOLs: Tecnis Eyhance (80% and 5%, respectively),23 and similar to diffractive EDOF IOLs: Tecnis Symfony (94% and 26%, respectively).28 Tecnis Symfony with mini-monovision achieved higher spectacle independence including near distance (64%),29 but at the expense of a high rate of photic phenomena (halos 57% and glare 50%). In a large, multi-country study of AcrySof IQ Vivity, spectacle independence for intermediate distance was 75.5%. In the same study, spectacle independence for near (29%) was identical to that in our study, despite a significantly higher binocular UNVA (0.23±0.16 logMAR at 40 cm).25
We have used mini-monovision in all study patients. So far, Symfony and Vivity are the only EDOF IOLs for which clinical data from studies using mini-monovision have been reported. Our mini-monovision approach (with a target of −0.50 D, achieving a MRSE of −0.46D) likely contributed to the high level of spectacle-independence. Importantly, it was well tolerated, as previously demonstrated in studies with Tecnis Symfony IOL.7,8 Despite the mini-monovision, the rate of patient-reported halos was low (5%) and binocular UDVA was excellent (−0.02±0.07 logMAR). Mean monocular UDVA was 0.13±0.16 logMAR in the eyes with mini-monovision, compared to 0.06±0.11 logMAR in the dominant eyes, resulting in a statistically significant yet clinically minor loss of 0.07±0.15 logMAR (0.7 Snellen lines; p<0.01) in the eyes with mini-monovision. In our study, the excellent safety of mini-monovision was further corroborated by the binocular defocus curve, which showed the good tolerance of the isofocal EDOF lens for light postoperative myopia: at a bilateral offset of −0.50 D, binocular distance vision was still very good (0.05 logMAR).
Our study has some limitations, mainly due to its retrospective and non-comparative nature. In addition, intermediate visual acuity was measured at 80 cm, which, although a common distance used in our clinic, makes it difficult to compare with other studies since 66 cm is more commonly used in clinical studies and is also the standard for the ANSI EDOF criteria (ANSI Z80.35–2018). On the other hand, we have measured near visual acuity at 33 cm instead of the more common 40 cm. In addition, contrast sensitivity was not studied. Finally, a longer clinical follow-up would be useful to further support our results, even though a growing body of evidence suggests that refractive stabilization occurs within one week following cataract surgery,31 and although our immediate sequential bilateral surgery approach allowed for faster visual rehabilitation and neuroadaptation.32
In patients undergoing bilateral cataract surgery, an isofocal EDOF lens with mini-monovision provided an extended range of functional vision up to 63 cm, resulting in usable uncorrected near vision, good uncorrected intermediate vision, and excellent uncorrected distance vision. Subjective patient satisfaction in terms of spectacle independence and photic phenomena was high. The excellent corrected distance visual acuity underlines the safety of the isofocal EDOF lens.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kanclerz P, Toto F, Grzybowski A, Alio JL. Extended depth-of-field intraocular lenses: an update. Asia Pacific J Ophthalmol. 2020;9(3):194–202. doi:10.1097/apo.0000000000000296
2. Rodov L, Reitblat O, Levy A, Assia EI, Kleinmann G. Visual outcomes and patient satisfaction for trifocal, extended depth of focus and monofocal intraocular lenses. J Refract Surg Thorofare. 2019;35(7):434–440. doi:10.3928/1081597x-20190618-01
3. Labiris G, Toli A, Perente A, Ntonti P, Kozobolis VP. A systematic review of pseudophakic monovision for presbyopia correction. Int J Ophthalmol. 2017;10(6):992–1000. doi:10.18240/ijo.2017.06.24
4. Cochener B. Influence of the level of monovision on visual outcome with an extended range of vision intraocular lens. Clin Ophthalmol. 2018;12:2305–2312. doi:10.2147/opth.s184712
5. Ganesh S, Brar S, Pawar A, Relekar KJ. Visual and refractive outcomes following bilateral implantation of extended range of vision intraocular lens with micromonovision. J Ophthalmol. 2018;2018:7321794. doi:10.1155/2018/7321794
6. Sandoval HP, Lane S, Slade S, Potvin R, Donnenfeld ED, Solomon KD. Extended depth-of-focus toric intraocular lens targeted for binocular emmetropia or slight myopia in the nondominant eye: visual and refractive clinical outcomes. J Cataract Refract Surg. 2019;45(10):1398–1403. doi:10.1016/j.jcrs.2019.05.019
7. Tan J, Qin Y, Wang C, Yuan S, Ye J. Visual quality and performance following bilateral implantation of TECNIS Symfony intraocular lenses with or without micro-monovision. Clin Ophthalmol. 2019;13:1071–1077. doi:10.2147/opth.s202380
8. Sandoval HP, Lane S, Slade SG, Donnenfeld ED, Potvin R, Solomon KD. Defocus curve and patient satisfaction with a new extended depth of focus toric intraocular lens targeted for binocular emmetropia or slight myopia in the non-dominant eye. Clin Ophthalmol. 2020;14:1791–1798.
9. Ota Y, Bissen-Miyajima H, Nakamura K, Hirasawa M, Minami K. Binocular visual function after staged implantation of extended-depth-of-focus intraocular lens targeting emmetropia and −0.5 diopter: a prospective comparison. PLoS One. 2020;15(8):e0238135. doi:10.1371/journal.pone.0238135
10. Schojai M, Schultz T, Jerke C, Böcker J, Dick HB. Visual performance comparison of 2 extended depth-of-focus intraocular lenses. J Cataract Refr Surg. 2020;46(3):388–393. doi:10.1097/j.jcrs.0000000000000068
11. Georgiev S, Palkovits S, Hirnschall N, Döller B, Draschl P, Findl O. Visual performance after bilateral toric extended depth-of-focus IOL exchange targeted for micromonovision. J Cataract Refr Surg. 2020;46(10):1346–1352. doi:10.1097/j.jcrs.0000000000000290
12. Turhan SA, Sevik MO, Toker E. Comparison of reading performance with low add bifocal and extended depth of focus intraocular lenses implanted with mini-monovision. Int Ophthalmol. 2021;41(1):315–323. doi:10.1007/s10792-020-01584-1
13. Newsom TH, Potvin R. Evaluation of quality of vision and visual outcomes with bilateral implantation of a non-diffractive extended vision intraocular lens with a target of slight myopia in the non-dominant eye. Clin Ophthalmol. 2022;16:183–190. doi:10.2147/opth.s350850
14. Sevik MO, Turhan SA, Toker E. Clinical outcomes with a low add multifocal and an extended depth of focus intraocular lenses both implanted with mini-monovision. Eye. 2022;36(6):1168–1177. doi:10.1038/s41433-021-01600-3
15. Van AT, Webers VSC, Bauer NJC, Clement LHH, Biggelaar FJHM, van den Nuijts RMMA. Visual outcomes of a new nondiffractive extended depth-of-focus intraocular lens targeted for minimonovision: 3-month results of a prospective cohort study. J Cataract Refr Surg. 2022;48(2):151–156. doi:10.1097/j.jcrs.0000000000000825
16. Coassin M, Mori T, Zazzo AD, et al. Effect of minimonovision in bilateral implantation of a novel non-diffractive extended depth-of-focus intraocular lens: defocus curves, visual outcomes, and quality of life. Eur J Ophthalmol. 2022;32(5):2942–2948. doi:10.1177/11206721211064018
17. Stodulka P, Slovak M. Visual performance of a polynomial extended depth of focus intraocular lens. Open J Ophthalmol. 2021;11(3):214–228. doi:10.4236/ojoph.2021.113017
18. Bova A, Vita S, Teus M. Clinical and aberrometric evaluation of a new monofocal IOL with intermediate vision improvement. J Ophthalmol. 2022;2022:4119698. doi:10.1155/2022/4119698
19. Morlock R, Wirth RJ, Tally SR, Garufis C, Heichel CWD. Patient-Reported Spectacle Independence Questionnaire (PRSIQ): development and validation. Am J Ophthalmol. 2017;178:101–114. doi:10.1016/j.ajo.2017.03.018
20. Łabuz G, Son HS, Naujokaitis T, Yildirim TM, Khoramnia R, Auffarth GU. Laboratory investigation of preclinical visual-quality metrics and halo-size in enhanced monofocal intraocular lenses. Ophthalmol Ther. 2021;10(4):1093–1104. doi:10.1007/s40123-021-00411-9
21. Jackson MA, Edmiston AM, Bedi R. Optimum refractive target in patients with bilateral implantation of extended depth of focus intraocular lenses. Clin Ophthalmol. 2020;14:455–462. doi:10.2147/opth.s237457
22. Savini G, Balducci N, Carbonara C, et al. Functional assessment of a new extended depth-of-focus intraocular lens. Eye. 2019;33(3):404–410. doi:10.1038/s41433-018-0221-1
23. Mencucci R, Cennamo M, Venturi D, Vignapiano R, Favuzza E. Visual outcome, optical quality, and patient satisfaction with a new monofocal IOL, enhanced for intermediate vision: preliminary results. J Cataract Refr Surg. 2021;46(3):378–387. doi:10.1097/j.jcrs.0000000000000061
24. Auffarth GU, Gerl M, Tsai L, et al. Clinical evaluation of a new monofocal IOL with enhanced intermediate function in patients with cataract. J Cataract Refr Surg. 2021;47(2):184–191. doi:10.1097/j.jcrs.0000000000000399
25. Bala C, Poyales F, Guarro M, et al. Multicountry clinical outcomes of a new nondiffractive presbyopia-correcting IOL. J Cataract Refr Surg. 2022;48(2):136–143. doi:10.1097/j.jcrs.0000000000000712
26. Chang DH, Janakiraman DP, Smith PJ, et al. Visual outcomes and safety of an extended depth-of-focus intraocular lens: results of a pivotal clinical trial. J Cataract Refr Surg. 2022;48(3):288–297. doi:10.1097/j.jcrs.0000000000000747
27. McCabe C, Berdahl J, Reiser H, et al. Clinical outcomes in a United States registration study of a novel extended depth of focus intraocular lens with a nondiffractive design. J Cataract Refr Surg. 2022;2022:1. doi:10.1097/j.jcrs.0000000000000978
28. Reinhard T, Maier P, Böhringer D, et al. Comparison of two extended depth of focus intraocular lenses with a monofocal lens: a multi-centre randomised trial. Graefes Archiv Clin Exp Ophthalmol. 2021;259(2):431–442. doi:10.1007/s00417-020-04868-5
29. Webers VSC, Bauer NJC, Saelens IEY, et al. Comparison of the intermediate distance of a trifocal IOL with an extended depth-of-focus IOL: results of a prospective randomized trial. J Cataract Refr Surg. 2020;46(2):193–203. doi:10.1097/j.jcrs.0000000000000012
30. Arrigo A, Gambaro G, Fasce F, Aragona E, Figini I, Bandello F. Extended depth-of-focus (EDOF) AcrySof® IQ Vivity® intraocular lens implant: a real-life experience. Graefes Archiv Clin Exp Ophthalmol. 2021;259(9):2717–2722. doi:10.1007/s00417-021-05245-6
31. Charlesworth E, Alderson AJ, Juan V, Elliott DB. When is refraction stable following routine cataract surgery? A systematic review and meta‐analysis. Ophthal Physl Opt. 2020;40(5):531–539. doi:10.1111/opo.12719
32. Kwedar K, Arnold J, Hesemann N. Visual recovery after immediate sequential bilateral cataract surgery at a veterans’ hospital. J Cataract Refract Surg. 2022;48(11):1260–1263. doi:10.1097/j.jcrs.0000000000000966
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Optical Biometry and Lens Power Calculations in 500 Phakic Patients: Axial Length and Corneal Curvature in the Fellow Eye
Kristianslund O, Hassaf SE, Drolsum L
Clinical Ophthalmology 2022, 16:2775-2780
Published Date: 23 August 2022
Intraocular Lens Unfurling Time Exponentially Decays with Increased Solution Temperature

Rocher EE, Mukherjee R, Pitingolo J, Levenshus E, Alexander G, Park M, Acharya R, Khan S, Shuff J, Aguirre A, Matin S, Walter K, Eghrari AO
Clinical Ophthalmology 2023, 17:2471-2481
Published Date: 21 August 2023
Comparing the Accuracy of the Kane, Barrett Universal II, Hill-Radial Basis Function, Emmetropia Verifying Optical, and Ladas Super Formula Intraocular Lens Power Calculation Formulas
Moshirfar M, Sulit CA, Brown AH, Irwin C, Ronquillo YC, Hoopes PC
Clinical Ophthalmology 2023, 17:2643-2652
Published Date: 7 September 2023
Comparison of Visual Performance and Patient Satisfaction Between Two Trifocal Intraocular Lenses: A Prospective, Paired-Eye Comparative Study
Kang S, Arsenault SM, O’Brien RC, Chatzea MS, Zarei-Ghanavati S, Beniz LAF, Yoo SH
Clinical Ophthalmology 2026, 20:572237
Published Date: 17 January 2026
Clinical Performance After Implantation of a New Purely Refractive Extended Depth of Field Intraocular Lens in Cataract Patients
Auffarth GU, Negoescu AT, Kremser F, Chychko L, Vogormian L, Khoramnia R, Yildirim TM
Clinical Ophthalmology 2026, 20:583059
Published Date: 23 March 2026