Back to Journals » Journal of Pain Research » Volume 19
Comparison of Pecto-Intercostal Fascial Block Vs Transversus Thoracic Plane Block and Their Pharmacogenomics for Pain Management After Sternotomy in Cardiac Surgery: A Narrative Review
Authors Breaux AM, Von-Koeller-Jones BM, Dufour SI, Drinkard J, Moore P, Griffin P, Shekoohi S ![]() , Ahmadzadeh S
, Ahmadzadeh S
Received 29 January 2026
Accepted for publication 21 May 2026
Published 25 May 2026 Volume 2026:19 599378
DOI https://doi.org/10.2147/JPR.S599378
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jinlei Li
Austin M Breaux,1 Beatrix M Von-Koeller-Jones,2 Sarah I Dufour,1 Joseph Drinkard,3 Peyton Moore,3 Patricia Griffin,3 Sahar Shekoohi,3 Shahab Ahmadzadeh3
1School of Medicine, Louisiana State University Health Sciences Center at Shreveport, Shreveport, LA, 71103, USA; 2Facultad de Ciencias de la Salud, Universidad Peruana de Ciencias Aplicadas, Lima, 15067, Peru; 3Department of Anesthesiology, Louisiana State University Health Sciences Center at Shreveport, Shreveport, LA, 71103, USA
Correspondence: Sahar Shekoohi, Email [email protected]
Abstract: Median sternotomy remains a standard approach for cardiac surgery but is associated with significant postoperative pain and increased opioid requirements. Inadequate pain control may contribute to respiratory complications, prolonged mechanical ventilation, and delayed recovery. Ultrasound-guided fascial plane blocks, including the pecto-intercostal fascial block (PIFB) and the transversus thoracic plane block (TTPB), have emerged as effective components of multimodal analgesia strategies. This narrative review compares PIFB and TTPB for post-sternotomy analgesia, focusing on clinical outcomes, pharmacological properties, and interindividual variability. Available clinical studies suggest that both techniques provide comparable analgesic efficacy and opioid-sparing effects, although some evidence indicates that PIFB may be associated with reduced opioid consumption or prolonged time to first analgesic request. Anatomical differences between techniques may influence dermatomal coverage, technical complexity, and risk profile. In addition, pharmacokinetic, pharmacodynamic, and genetic factors may contribute to variability in analgesic response and should be considered when tailoring perioperative pain management strategies. Practical considerations, including operator expertise, procedural feasibility, and patient-specific factors, further influence block selection. Overall, both PIFB and TTPB are effective for post-sternotomy analgesia. Their optimal use should be guided by an individualized approach that integrates clinical evidence, anatomical considerations, and patient-specific characteristics.
Keywords: block, pecto-intercostal fascial block, transversus thoracic plane block, pain, post-op, opioid, sternotomy
Introduction
Median sternotomy has been the standard approach in many open-heart procedures, including CABG, valve repair and replacement, and congenital heart surgeries. This approach allows access to the mediastinum but is associated with significant postoperative pain due to disruption of the skin, sternum, and surrounding soft tissues, including the intercostal nerves and costosternal joints. Inadequately controlled pain leads to impaired breathing, which may lead to prolonged mechanical ventilation. This higher level of pain leads to increased opioid consumption, which correlates with respiratory depression, postoperative nausea and vomiting, and possible delirium. One nationwide cohort study of sternotomy patients found that 25–50% of sternotomy patients develop persistent pain after coronary artery bypass surgery.1 Optimizing pain management is therefore a critical component of these procedures.
Historically, thoracic epidural analgesia has been the gold standard, but its use is associated with the possibility of epidural hematoma. As a result, use has shifted toward ultrasound-guided fascial plane blocks, which offer a favorable safety profile. The pecto-intercostal fascial block (PIFB) and the transversus thoracic plane (TTPB) both aim to block the anterior cutaneous branches of intercostal nerves to reduce sternal and parasternal pain. A prospective randomized study found that PIFB resulted in lower 24-hour postoperative morphine usage when compared to TTPB.2 A second randomized controlled trial comparing PIFB and TTPB reported similar 24-hour morphine usage and pain scores between groups, but with a longer time to pain control requests in the PIFB group.3
These results highlight the need for a second look at these blocks and their use in sternotomy patients. There is limited data on long-term outcomes, chronic pain, and comparison of performance on the two blocks. So, this narrative review aims to compare PIFB and TTP for pain management after sternotomy in cardiac surgery, focusing on pharmacodynamic, kinetic, and possible individual genetic predispositions.
Methods
This study was conducted as a narrative review. A comprehensive, non-systematic literature search was performed to identify relevant studies. Electronic databases including PubMed (MEDLINE) and Google Scholar were searched. Additional relevant articles were identified through manual screening of reference lists.
The search strategy included combinations of keywords such as “pecto-intercostal fascial block”, “transversus thoracic plane block”, “sternotomy”, “cardiac surgery”, “postoperative pain”, “opioid consumption”, “pharmacokinetics”, “pharmacodynamics”, and “pharmacogenomics”. Boolean operators (AND, OR) were used to refine and combine search terms. Articles published up to 2025 were considered, with emphasis placed on literature from 2020 onward. Earlier foundational studies were included when necessary to support key pharmacologic concepts.
Inclusion criteria comprised peer-reviewed articles relevant to regional anesthesia in sternotomy, pharmacology of local anesthetics and pharmacogenomic aspects of pain management. Eligible study designs included randomized controlled trials, observational studies, systematic reviews and meta-analyses. Exclusion criteria included studies that did not meet inclusion criteria or lacked relevance.
Study selection was based on relevance to the topic and clinical applicability. Preference was given to studies with stronger levels of evidence when available. Articles were screened based on title and abstract for relevance, followed by full-text review. Given the narrative nature of this review, a formal systematic screening process, flow diagram and risk-of-bias assessment tools were not applied.
Individual Genetic Differences to Blocks
Emerging evidence suggests that interindividual variability in response to regional anesthesia may be explained by genetic factors influencing pain perception, local anesthetic pharmacodynamics and systemic drug handling.
Polymorphisms in the catechol-o-methyltransferase (COMT) gene, particularly the Val158Met variant, have been associated with altered catecholamine metabolism and increased pain sensitivity, contributing to variability in postoperative pain intensity and analgesic requirements.4,5 In the context of fascial plane blocks such as PIFB and TTPB, patients carrying low COMT activity variants may report higher pain scores despite technically correct nerve blockade, affecting overall efficacy.
Genetic variation may also influence the pharmacodynamic response to local anesthetics. Variants in genes encoding voltage-gated sodium channels like SCN9A have been associated with altered nociceptive signaling differences in sensitivity to sodium channel blockade.6 As local anesthetics exert their effect through inhibition of these channels, these polymorphisms may contribute to variability in block effectiveness.
Pharmacokinetic variability may further contribute to interindividual differences. Polymorphisms affecting cytochrome P450 enzymes, such as CYP1A2 and CYP3A4 may alter the metabolism of amide local anesthetics, influencing both systemic exposure and duration of action.7 Additionally, genetic variation in CYP2D6 enzyme may influence the metabolism of commonly used opioid analgesics. Although it does not directly affect the performance of regional blocks, it can contribute to variability in overall analgesic response when these techniques are used as part of a multimodal scheme.8,9
Direct evidence linking these genetic factors to the efficacy of fascial plane blocks like PIFB and TTPB remain limited, as most pharmacogenomic data has been derived from studies in systemic analgesics.
Block Pharmacodynamics
Pharmacodynamics describes the interaction of local anesthetics with neuronal targets and their effects on nerve conduction. In the context of regional anesthesia, local anesthetics produce analgesia by reversibly blocking sodium channels in peripheral nerves.10,11 Both the pecto-intercostal fascial block (PIFB) and the transversus thoracic plane block (TTPB) rely on this pharmacological principle. Their distinction arises not from the drug itself, but from the anatomical plane of injection and the distribution of neural blockade.
Mechanism of Action and Anatomic Targets
Local anesthetics act by reversibly blocking voltage-gated sodium channels, thereby stabilizing the neuronal membrane and preventing propagation of action potentials along nociceptive fibers.11,12 This type of blockade is “use-dependent”, which means local anesthetics bind with greater affinity to sodium channels in their open or inactivated state, making rapidly firing pain fibers more susceptible to conduction block.13 By reducing excitability, local anesthetics inhibit nociceptive signal propagation along peripheral nerve fibers.
In the pecto-intercostal fascial block, the injectate is deposited between the pectoralis major and internal or external intercostal muscles, producing a spread that anesthetizes the anterior cutaneous branches of intercostal nerves T2-T6. This produces reliable superficial anesthesia to the parasternal region but is generally limited in depth,14,15 sometimes requiring multiple injections to extend cephalocaudal coverage.
In contrast, the transversus thoracic plane block, local anesthetic is deposited between the internal intercostal and transversus thoracic muscles, targeting anterior intercostal nerves in a deeper retrosternal plane.16,17 This deeper distribution allows for broader neural coverage compared to PIFB.16,18
Variability in Response
The clinical efficacy of fascial plane blocks may vary depending on local tissue conditions. For instance, tissue acidosis reduces the proportion of non-ionized (lipid-soluble) forms of the anesthetic, delaying onset and reducing effectiveness, particularly relevant in inflamed or ischemic tissues.19,20 Additionally, inflammation may enhance neuronal excitability, potentially diminishing block effectiveness.11,13
Anatomical variation in the course of intercostal nerves and the extent of fascial spread further contributes to heterogeneity in block performance. These factors may influence the distribution of neural blockade and help explain differences in analgesic coverage between patients and techniques.
Clinical Implications
At the molecular level, the pharmacodynamics of local anesthetics are identical in both blocks. The difference lies in the anatomical distribution of the injectate, which determines the dermatomal coverage achieved. PIFB provides more superficial parasternal analgesia and is considered technically simpler. TTPB, while more technically demanding, offers deeper retrosternal coverage and may provide superior analgesia in selected patients.
Block Pharmacokinetics
Pharmacokinetics is the study of the absorption, distribution, metabolism, and elimination (ADME) of drugs, describing how the body processes an administered agent over time. It characterizes the relationship between drug dose and plasma concentration and is essential for understanding drug duration and systemic exposure.10
In fascial plane blocks, pharmacokinetics is influenced by both the physicochemical properties of local anesthetics and the vascular characteristics of the injection site. Because both PIFB and TTPB blocks employ similar amide anesthetics, differences in pharmacokinetics arise primarily from anatomical factors that influence systemic absorption.
Absorption
Systemic absorption of local anesthetics is directly correlated with the vascularity of the injection site.13 Intercostal and parasternal regions are among the most vascular in the body, predisposing these blocks to higher plasma uptake. In PIFB, local anesthetic is deposited in a relatively superficial fascial plane between the pectoralis major and intercostal muscles, producing moderate systemic absorption. In contrast, TTPB involves injection in a deeper plane adjacent to internal thoracic vessels (internal mammary artery and vein), where richer vascularity facilitates faster uptake. This anatomical relationship may result in higher systemic absorption and increased plasma concentrations compared to more superficial techniques.
Distribution
Once absorbed, the distribution of local anesthetics depends on lipid solubility and plasma protein binding. Bupivacaine, a highly lipophilic agent, exhibits extensive protein binding (up to 95%), which prolongs its duration of action and influences the fraction of free drug circulating.21,22 Lidocaine demonstrates moderate protein binding (60–80%), resulting in more rapid distribution and shorter duration of effect, while prilocaine distributes more rapidly due to lower protein binding.
In populations with altered protein levels, the unbound fraction of local anesthetic may increase, thereby increasing systemic exposure.
Metabolism and Elimination
Amide local anesthetics, including lidocaine, bupivacaine, and ropivacaine, undergo hepatic metabolism via CYP450 enzymes, primarily CYP1A2 and CYP3A4.3,19 Initial N-dealkylation generates metabolites that may retain pharmacologic activity. The metabolites are ultimately excreted, primarily via renal excretion. Hepatic dysfunction, renal impairment, or genetic variability in metabolic capacity may prolong drug clearance and increase systemic exposure.23
Clinical Implications
From a pharmacokinetic perspective, both blocks share similar metabolic pathways, but differ in the extent of systemic absorption due to their anatomical location. PIFB, being more superficial, entails lower systemic uptake. On the other hand, TTPB may result in higher plasma concentrations due to its proximity to major thoracic vessels. These pharmacokinetic characteristics may increase the risk of local anesthetic systemic toxicity (LAST), particularly relevant in high-risk populations, highlighting the importance of careful dose selection and monitoring.10,16,18
Role of Opioids in Multimodal Analgesia
Opioid analgesics remain an important component of postoperative pain management following cardiac surgery, particularly as part of multimodal analgesic strategies. However, their use is associated with well-known adverse effects, including respiratory depression, nausea, ileus, and the risk of prolonged opioid dependence. In this context, regional anesthesia techniques such as the pecto-intercostal fascial block (PIFB) and the transversus thoracic plane block (TTPB) have gained increasing relevance due to their opioid-sparing potential.24,25 Interindividual variability in opioid response is influenced by genetic factors affecting both pharmacodynamics and pharmacokinetics. Polymorphisms in the μ-opioid receptor gene (OPRM1) have been associated with differences in analgesic sensitivity, while variations in drug metabolizing enzymes, particularly cytochrome P450 CYP2D6, play a key role in the bioactivation and clearance of several commonly used opioids, such as codeine and oxycodone.9,24,26,27 These genetic differences may lead to variability in both analgesic efficacy and the risk of adverse effects among patients.In the setting of PIFB and TTPB, these pharmacogenomic factors are particularly relevant, as regional anesthesia aims to reduce reliance on systemic opioids. Patients with altered opioid metabolism or increased susceptibility to opioid-related side effects may obtain greater benefit from effective regional techniques. Conversely, variability in opioid response may still influence overall pain control when these blocks are incorporated into multimodal analgesic regimens.24,25 Therefore, understanding the interaction between regional anesthesia and opioid pharmacogenomics may help optimize individualized pain management strategies. This approach further supports the role of PIFB and TTPB in reducing opioid exposure while maintaining effective analgesia after sternotomy.9,25,26
Discussion
Effective regional anesthesia has clear clinical importance due to its role in reducing opioid consumption, adverse events, and prolonged persistent pain. Both PIFB and TTPB have been shown to significantly reduce post-sternotomy pain. PIFB is a more superficial block and is easily performed, whereas TTPB targets deeper structures and may provide broader intercostal coverage.28,29 Despite these differences, current literature suggests that both blocks achieve comparable analgesic effects, with subtle variations that may be tailored based on patient and procedural factors. These findings are supported by available clinical data. Randomized controlled trials have reported comparable postoperative pain scores and opioid consumption between PIFB and TTPB, with some studies demonstrating reduced 24-hour morphine requirements or prolonged time to rescue analgesia in PIFB groups.2,3 However, variability across studies remains, which may reflect differences in technique, patient populations, and perioperative analgesic protocols. A summary of key clinical studies is presented in Table 1.
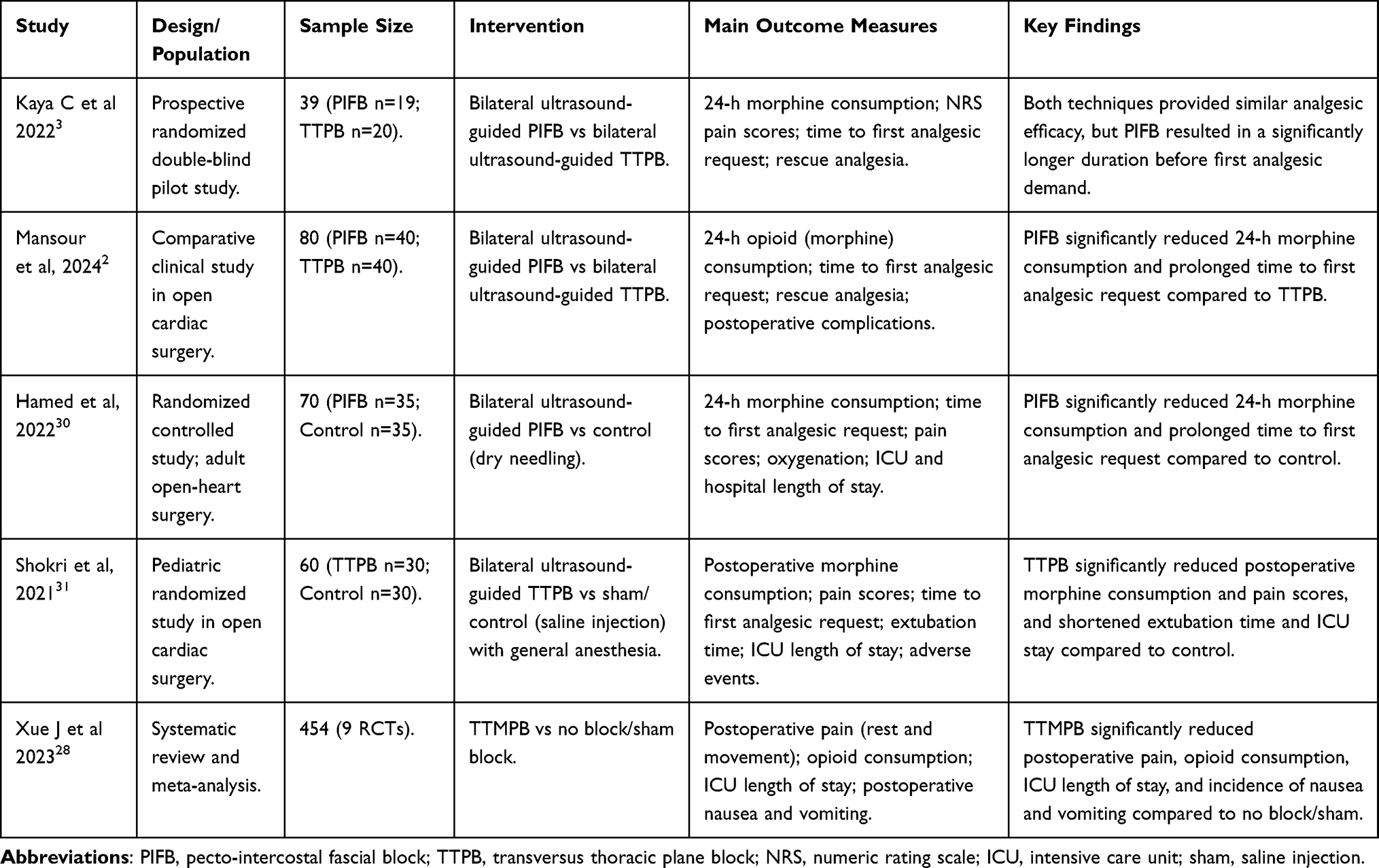 |
Table 1 Summary of Major Clinical Studies Relevant to PIFB and TTPB After Sternotomy |
In addition to anatomical considerations, the pharmacological properties of the local anesthetic used can influence the clinical performance of these blocks. Differences in lipid solubility, protein binding, and intrinsic potency among agents such as bupivacaine and ropivacaine may affect time onset, duration of analgesia and systemic absorption. Bupivacaine, with higher lipid solubility and protein binding, is associated with a prolonged duration of action but carries a higher risk of cardiotoxicity at elevated plasma concentrations.32–34 In contrast, ropivacaine demonstrates a safer profile due to its reduced cardiotoxic potential, even though it may provide slightly less potent sensory blockade. Clinical studies evaluating fascial plane blocks and truncal techniques have reported comparable analgesic efficacy across these agents. However, differences in duration of action and safety profiles have been reported, particularly in relation to bupivacaine and ropivacaine use in cardiac and thoracic surgery populations.35,36 Therefore, both the choice of local anesthetic and the anatomical plane of injection should be considered when tailoring regional anesthesia strategies.
Interindividual variability in genetic response may also be influenced by genetic factors. Polymorphisms such as those affecting COMT may alter pain perception, while genetic variation in sodium channel function may influence the pharmacodynamic response to local anesthetics. In addition, variability in drug metabolism, including CYP450 and CYP2D6 pathways, may affect both local anesthetic handling and the efficacy of adjunct opioid therapy. These mechanisms may help explain differences in postoperative pain control despite technically adequate regional blocks.
Both PIFB and TTPB contribute to opioid-sparing effects as well as fewer reports of nausea, vomiting, respiratory depression, and constipation.37 Clinically, these effects translate into earlier extubation, shorter ICU stays, and improved mobilization.2 However, the magnitude of opioid reduction varies across studies, which may reflect differences in technique, timing, patient populations and underlying biologic variability.
From a safety perspective, PIFB is generally considered easier to perform with a lower risk of complications such as pleural puncture due to its superficial approach.38 In contrast, TTPB involves a deeper fascial plane and therefore carries a higher risk of pneumothorax, vascular injury, or local anesthetic systemic toxicity, although these complications remain rare when performed under typical ultrasound guidance by experienced clinicians.39
Preliminary data suggest that both blocks can improve patient satisfaction, reduce perioperative anxiety, and facilitate earlier ambulation, supporting enhanced recovery after cardiac surgery.2,40 However, direct comparative trials remain limited, and long-term outcomes have been inconsistently reported.18
From a practical standpoint, selection between PIFB and TTPB may be guided by patient-specific and procedural factors. PIFB may be preferred in patients with higher procedural risk or when a safer and more superficial approach is desired. In contrast, TTPB may be considered in patients where broader retrosternal analgesia is required, such as those undergoing extensive sternotomy or with higher anticipated pain burden. Operator experience with ultrasound-guided techniques, equipment availability, and procedural time may also influence block selection, as more technically demanding approaches may be less feasible in resource-limited settings or in urgent clinical scenarios. Additional considerations, including patient comorbidities, bleeding risk, and need for rapid recovery may further influence block selection. Pharmacological factors, including the choice of local anesthetic and patient-related variables, including genetic variability in pain perception and drug metabolism, may influence both the perceived efficacy of regional blocks and the overall effectiveness of multimodal analgesic strategies. Although these considerations do not yet constitute a formal decision algorithm, they provide a clinically relevant framework to support a more individualized approach to regional anesthesia in cardiac surgery patients.41–44 A comparative overview of PIFB and TTPB is summarized in Table 2.
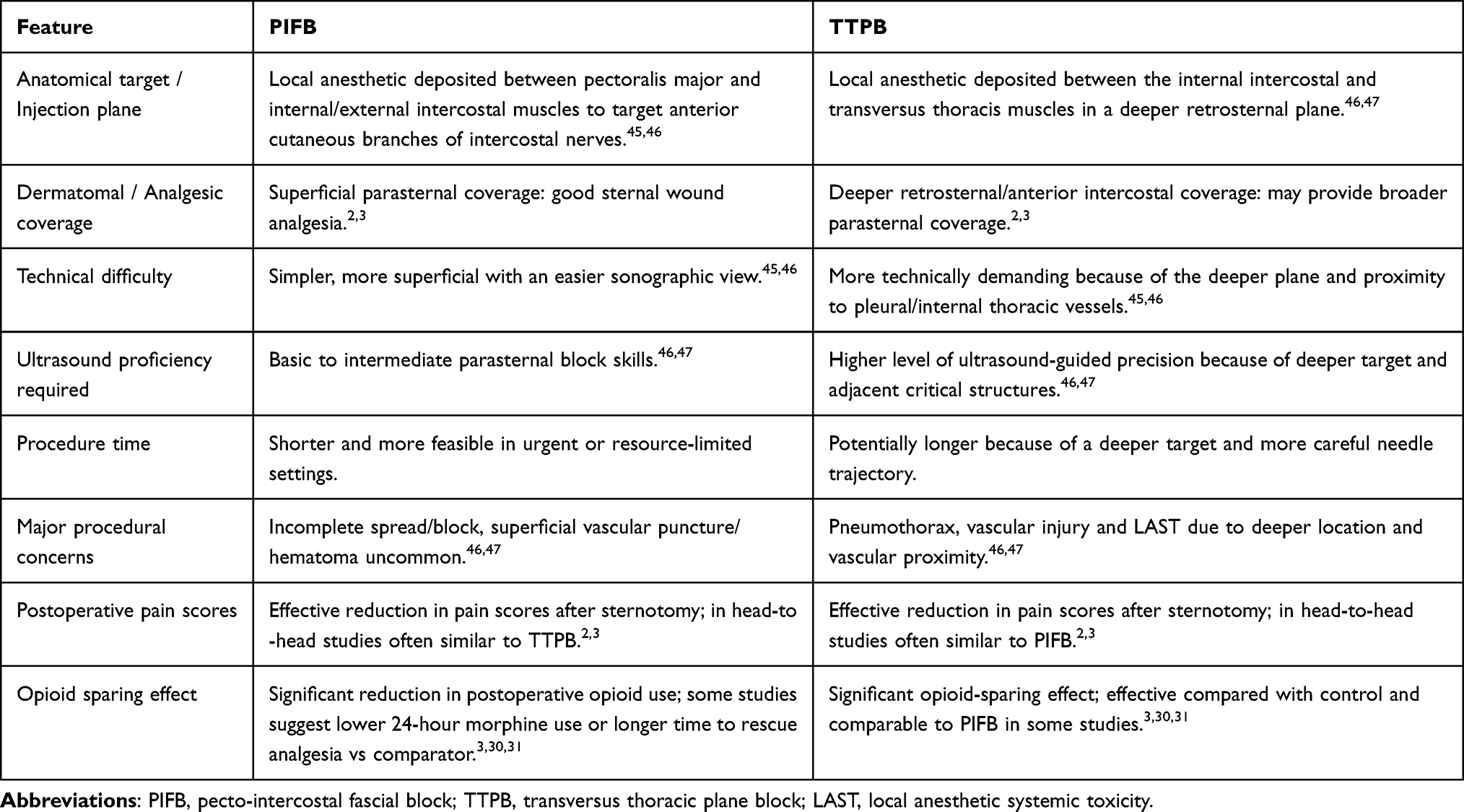 |
Table 2 Comparative Characteristics of PIFB and TTPB for Post-Sternotomy Analgesia |
Future studies should incorporate larger patient cohorts, standardized techniques, and long-term follow up to better define the comparative effectiveness of PIFB and TTPB. In addition, further research exploring the role of genetic variability may help refine patient selection and optimize individualized analgesic strategies.
Conclusion
Both the pecto-intercostal fascial block (PIFB) and the transversus thoracic plane block (TTPB) are effective regional anesthesia techniques for the management of post-sternotomy pain, demonstrating comparable analgesic efficacy and significant opioid-sparing effects in the current literature. While TTPB may offer broader retrosternal coverage, PIFB is generally considered technically simpler and associated with a more favorable safety profile.
The choice between these techniques should not rely solely on anatomical considerations but also incorporate clinical evidence, pharmacological factors, and patient-specific characteristics. Variability in analgesic response may be influenced by interindividual differences in pain perception, drug metabolism, and genetic factors, highlighting the importance of a more personalized approach to perioperative pain management.
Although current evidence supports the use of both blocks, further high-quality, large-scale studies are needed to better define their comparative effectiveness and long-term outcomes. Future research integrating pharmacogenomic insights may contribute to more precise and individualized analgesic strategies in cardiac surgery patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Elmistekawy E, Attia A. Chronic post sternotomy pain: the role of sternal wire removal—a review. AME Med J. 2020;5:31. doi:10.21037/amj.2020.03.06
2. Mansour MA, Mahmoud HE, Fakhry DM, Kassim DY. Comparison of the effects of transversus thoracic muscle plane block and pecto-intercostal fascial block on postoperative opioid consumption in patients undergoing open cardiac surgery: a prospective randomized study. BMC Anesthesiol. 2024;24(1):63. doi:10.1186/s12871-024-02432-w
3. Kaya C, Dost B, Dokmeci O, Yucel SM, Karakaya D. Comparison of ultrasound-guided pecto-intercostal fascial block and transversus thoracic muscle plane block for acute poststernotomy pain management after cardiac surgery: a prospective, randomized, double-blind pilot study. J Cardiothorac Vasc Anesth. 2022;36(8):2313–9. doi:10.1053/j.jvca.2021.09.041
4. Flood P, Clark D. Genetic variability in the activity of monoamines: a window into the complexity of pain. Anesth Analg. 2014;119(5):1032–1038. doi:10.1213/ANE.0000000000000447
5. Chadwick A, Frazier A, Khan TW, Young E. Understanding the psychological, physiological, and genetic factors affecting precision pain medicine: a narrative review. J Pain Res. 2021;14:3145–3161. doi:10.2147/JPR.S320863
6. Harsa MS, Herawati L, Hidayati HB. SCN9A and SCN10A polymorphism and therapeutic effectiveness of lidocaine local anesthetic injection in subjects with diabetic neuropathy pain. Pharmacogn J. 2025;16(6):1259–1263. doi:10.5530/pj.2024.16.204
7. DiMaria S, Mangano N, Bruzzese A, Bartula B, Parikh S, Costa A. Genetic variation and sex-based differences: current considerations for anesthetic management. Curr Issues Mol Biol. 2025;47(3):202. doi:10.3390/cimb47030202
8. Pratt VM, Scott SA, Pirmohamed M, Esquivel B, Kattman BL, Malheiro AJ. Medical Genetics Summaries [Internet]. Bethesda (MD): National Center for Biotechnology Information (US); 2012 Available from: http://www.ncbi.nlm.nih.gov/books/NBK61999/.
9. Crews KR, Monte AA, Huddart R, et al. Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6, OPRM1, and COMT Genotypes and Select Opioid Therapy. Clin Pharmacol Ther. 2021;110(4):888–896.PubMed PMID: 33387367; PubMed Central PMCID: PMC8249478. doi:10.1002/cpt.2149
10. Baggot JD. Pharmacokinetic-pharmacodynamic relationship. Ann Rech Veterinaires Ann Vet Res. 1990;21(Suppl 1):29S–40S. PubMed PMID: 2080844.
11. Tetzlaff JE. The pharmacology of local anesthetics. Anesthesiol Clin N Am. 2000;18(2):217–233. [PubMed PMID: 10935008]. doi:10.1016/s0889-8537(05)70161-9
12. Yagiela JA. Local anesthetics. Anesth Prog. 1991;38(4–5):128–141. PubMed PMID: 1819966; PubMed Central PMCID: PMC2190304.
13. Heavner JE. Local anesthetics. Curr Opin Anaesthesiol. 2007;20(4):336–342.PubMed PMID: 17620842. doi:10.1097/ACO.0b013e3281c10a08
14. Liu V, Mariano ER, Prabhakar C. Pecto-intercostal fascial block for acute poststernotomy pain: a case report. AA Pract. 2018;10(12):319–322.PubMed PMID: 29293481. doi:10.1213/XAA.0000000000000697
15. Kaye AD, Vuong CA, Hawkins AM, et al. Pecto-intercostal fascial plane block for pain management after cardiothoracic surgery. Curr Pain Headache Rep. 2025;29(1):84.PubMed PMID: 40375035. doi:10.1007/s11916-025-01398-9
16. Elbardan IM, Shehab AS, Mabrouk IM. Comparison of transversus thoracis muscle plane block and pecto-intercostal fascial plane block for enhanced recovery after pediatric open-heart surgery. Anaesth Crit Care Pain Med. 2023;42(4):101230.PubMed PMID: 37031816. doi:10.1016/j.accpm.2023.101230
17. Cui YY, Xu ZQ, Hou HJ, Zhang J, Xue JJ. Transversus thoracic muscle plane block for postoperative pain in pediatric cardiac surgery: a systematic review and meta-analysis of randomized and observational studies. J Cardiothorac Vasc Anesth. 2024;38(5):1228–1238.PubMed PMID: 38453555. doi:10.1053/j.jvca.2024.02.016
18. Vanjare H, Deshmukh CP, Barasker SK, Kassim AM, Arya B. Comparative analysis of ultrasound-guided pain management approaches for sternotomy in cardiac surgeries-transversus thoracic muscle plane block vs pecto-intercostal fascial block. Ochsner J. 2025;25(1):11–16.PubMed PMID: 40123926; PubMed Central PMCID: PMC11924972. doi:10.31486/toj.24.0052
19. Becker DE, Reed KL. Local anesthetics: review of pharmacological considerations. Anesth Prog. 2012;59(2):90–101.PubMed PMID: 22822998; PubMed Central PMCID: PMC3403589. doi:10.2344/0003-3006-59.2.90
20. Garmon EH, Hendrix JM, Huecker MR. Topical, Local, and Regional Anesthesia and Anesthetics. [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Available from: http://www.ncbi.nlm.nih.gov/books/NBK430894/.
21. Steverink JG, Piluso S, Malda J, Verlaan JJ. Comparison of in vitro and in vivo toxicity of bupivacaine in musculoskeletal applications. Front Pain Res Lausanne Switz. 2021;2:723883. PubMed PMID: 35295435; PubMed Central PMCID: PMC8915669.doi:10.3389/fpain.2021.723883
22. Routledge PA, Barchowsky A, Bjornsson TD, Kitchell BB, Shand DG. Lidocaine plasma protein binding. Clin Pharmacol Ther. 1980;27(3):347–351.PubMed PMID: 7357791. doi:10.1038/clpt.1980.46
23. Smith DA. Pharmacokinetics and pharmacodynamics in toxicology. Xenobiotica Fate Foreign Compd Biol Syst. 1997;27(5):513–525.PubMed PMID: 9179991. doi:10.1080/004982597240479
24. Kaye AD, Garcia AJ, Hall OM, et al. Update on the pharmacogenomics of pain management. Pharmacogenomics Pers Med. 2019;12:125–143. doi:10.2147/PGPM.S179152
25. Bugada D, Lorini LF, Fumagalli R, Allegri M. Genetics and opioids: towards more appropriate prescription in cancer pain. Cancers. 2020;12(7):1951. doi:10.3390/cancers12071951
26. Wong AK, Somogyi AA, Rubio J, Philip J. The role of pharmacogenomics in opioid prescribing. Curr Treat Options Oncol. 2022;23(10):1353–1369.PubMed PMID: 36001223; PubMed Central PMCID: PMC9526685. doi:10.1007/s11864-022-01010-x
27. Owusu Obeng A, Hamadeh I, Smith M. Review of opioid pharmacogenetics and considerations for pain management. Pharmacotherapy. 2017;37(9):1105–1121.PubMed PMID: 28699646. doi:10.1002/phar.1986
28. Xue JJ, Cui YY, Busse JW, et al. Transversus thoracic muscle plane block for pain during cardiac surgery: a systematic review and meta-analysis. Int J Surg Lond Engl. 2023;109(8):2500–2508.PubMed PMID: 37246971; PubMed Central PMCID: PMC10442103. doi:10.1097/JS9.0000000000000470
29. Zhang Y, Min J, Chen S. Perioperative pain management with bilateral pecto-intercostal fascial block in pediatric patients undergoing open cardiac surgery. Front Cardiovasc Med. 2022;9:825945. PubMed PMID: 35811718; PubMed Central PMCID: PMC9256953.doi:10.3389/fcvm.2022.825945
30. Hamed MA, Abdelhady MA, Hassan AASM, Boules ML. The analgesic effect of ultrasound-guided bilateral pectointercostal fascial plane block on sternal wound pain after open heart surgeries: a randomized controlled study. Clin J Pain. 2022;38(4):279–284.PubMed PMID: 35132025. doi:10.1097/AJP.0000000000001022
31. Shokri H, Ali I, Kasem AA. Evaluation of the analgesic efficacy of bilateral ultrasound-guided transversus thoracic muscle plane block on post-sternotomy pain: a randomized controlled trial. Local Reg Anesth. 2021;14:145–152. PubMed PMID: 34803399; PubMed Central PMCID: PMC8594901.doi:10.2147/LRA.S338685
32. El-Boghdadly K, Pawa A, Chin KJ. Local anesthetic systemic toxicity: current perspectives. Local Reg Anesth. 2018;11:35–44. PubMed PMID: 30122981; PubMed Central PMCID: PMC6087022.doi:10.2147/LRA.S154512
33. Neal JM, Bernards CM, Butterworth JF, et al. ASRA practice advisory on local anesthetic systemic toxicity. Reg Anesth Pain Med. 2010;35(2):152–161.PubMed PMID: 20216033. doi:10.1097/AAP.0b013e3181d22fcd
34. McClure JH. Ropivacaine. Br J Anaesth. 1996;76(2):300–307.PubMed PMID: 8777115. doi:10.1093/bja/76.2.300
35. Kim DH, Kim SJ, Liu J, Beathe J, Memtsoudis SG. Fascial plane blocks: a narrative review of the literature. Reg Anesth Pain Med. 2021;46(7):600–617.PubMed PMID: 34145072. doi:10.1136/rapm-2020-101909
36. Pawa A, King C, Thang C, White L. Erector spinae plane block: the ultimate ‘plan A’ block? Br J Anaesth. 2023;130(5):497–502. doi:10.1016/j.bja.2023.01.012
37. Wardhana A, Sudono H, Kurniawaty J. Effectiveness of pecto-intercostal fascia plane block in reducing total postoperative opioid consumption in cardiac surgery involving sternotomy: a meta-analysis. Ann Card Anaesth.;28(3):219–227. PubMed PMID: 40629776; PubMed Central PMCID: PMC12324778. doi:10.4103/aca.aca_248_24
38. Toscano A, Capuano P, Perrucci C, et al. Which ultrasound-guided parasternal intercostal nerve block for post-sternotomy pain? Results from a prospective observational study. J Anesth Analg Crit Care. 3(1):48. PubMed PMID: 37974241; PubMed Central PMCID: PMC10652511. doi:10.1186/s44158-023-00134-2
39. Toscano A, Capuano P, Rinaldi M, Brazzi L. Successful use of single-shot pectointercostal fascial block for awake sternal wound revision. Ann Card Anaesth. 2022;25(3):377–378.PubMed PMID: 35799576; PubMed Central PMCID: PMC9387629. doi:10.4103/aca.aca_120_21
40. Elhaddad AMM, Hassan PF. Efficacy of ultrasound-guided, single-level, pectointercostal facial block (PIFB) for postoperative analgesia after sternotomy in paediatric cardiac surgery: a randomised controlled trial. Indian J Anaesth. 2025;69(5):483–488.PubMed PMID: 40364943; PubMed Central PMCID: PMC12068439. doi:10.4103/ija.ija_1181_24
41. Neal JM, Barrington MJ, Fettiplace MR, et al. The Third American Society of Regional Anesthesia and Pain Medicine Practice Advisory on Local Anesthetic Systemic Toxicity: executive Summary 2017. Reg Anesth Pain Med. 2018;43(2):113–123.PubMed PMID: 29356773. doi:10.1097/AAP.0000000000000720
42. Caruso TJ, Lawrence K, Tsui BCH. Regional anesthesia for cardiac surgery. Curr Opin Anaesthesiol. 2019;32(5):674–682.PubMed PMID: 31356362. doi:10.1097/ACO.0000000000000769
43. Dost B. Fascial plane blocks in the era of modern regional anesthesia: shaping the future of pain management. J Anesth Analg Crit Care. 5(1):
44. Coleman SR, Chen M, Patel S, et al. Enhanced recovery pathways for cardiac surgery. Curr Pain Headache Rep. 2019;23(4):28.PubMed PMID: 30868281. doi:10.1007/s11916-019-0764-2
45. Zhu A, Malgieri C, Hayward G. Pecto-Intercostal Fascial Plane Block. [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Available from: http://www.ncbi.nlm.nih.gov/books/NBK603717/.
46. Capuano P, Sepolvere G, Toscano A, et al. Fascial plane blocks for cardiothoracic surgery: a narrative review. J Anesth Analg Crit Care. 2024;4(1):20.PubMed PMID: 38468350; PubMed Central PMCID: PMC10926596. doi:10.1186/s44158-024-00155-5
47. Desire SM, Hayward G. Transversus Thoracic Muscle Plane Block (TTMPB). [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Available from: http://www.ncbi.nlm.nih.gov/books/NBK587362/.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Impact of Opioid Receptor Gene Polymorphism on Fentanyl and Alfentanil’s Analgesic Effects in the Pediatric Perioperative Period
Lilic J, Marjanovic VG, Budic I, Stefanovic N, Stokanovic D, Marjanovic GT, Jevtovic-Stoimenov T, Golubovic M, Zecevic M, Velickovic-Radovanovic R
Pharmacogenomics and Personalized Medicine 2024, 17:41-49
Published Date: 30 January 2024
Research Trends and Knowledge Mapping of Opioid-Free Anesthesia: A Global Bibliometric Analysis
Guo Z, Shan Z, Wang F
Journal of Multidisciplinary Healthcare 2025, 18:4145-4157
Published Date: 21 July 2025
Machine Learning Approach to Predict Postoperative Pain and Opioid Usage in Elective Primary Spine Surgery: A Retrospective Study
Saksenberg DL, Lee RY, Vaidya S, Yuan A, Jeong SJ, Lockwood N, Li J, Russo GS
Journal of Pain Research 2026, 19:596384
Published Date: 27 March 2026
Trigeminal Terminal Branch Neuralgias in a Headache Unit: A 15-Year Series
Ros González I, Recio García A, Sierra Mencía Á, González Osorio Y, García-Azorín D, Guerrero Peral ÁL
Journal of Pain Research 2026, 19:588731
Published Date: 27 May 2026