Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Combining Transarterial Chemoembolization with Sorafenib Improves Survival in Selected Patients with Hepatocellular Carcinoma and Extrahepatic Spread: A Multicenter Real-World Study
Authors Yuan Y, Qiao Y, Zhu Y, Guo P, Gou J, Liu K, Wang L, Zhao S, Zhang Y, Liu Y, Wang E, Liu L
Received 30 October 2025
Accepted for publication 23 December 2025
Published 30 December 2025 Volume 2025:12 Pages 3049—3062
DOI https://doi.org/10.2147/JHC.S575739
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Gerber
Yue Yuan,1,* Yu Qiao,2,3,* Yejing Zhu,2,* Ping Guo,4 Jiakun Gou,1 Kai Liu,1 Linqian Wang,2,5 Shoujie Zhao,2 Yongchao Zhang,6 Yunjie Liu,1 Enxin Wang,1 Lei Liu2
1Department of Digestive Diseases, Air Force Hospital of Western Theater Command, PLA, Chengdu, People’s Republic of China; 2Department of Infectious Diseases, Xijing Hospital, State Key Laboratory of Holistic Integrative Management of Gastrointestinal Cancers and Xijing Hospital of Digestive Diseases, Fourth Military Medical University, Xi’an, People’s Republic of China; 3Department of Gastroenterology, Yanan University Affiliated Hospital, Yan’an, People’s Republic of China; 4Center for Disease Control and Prevention of Western Theater Command, PLA, Chengdu, People’s Republic of China; 5Northwest University Medical College, Xi’an, People’s Republic of China; 6Department of Medical Affairs, Air Force Hospital of Western Theater Command, PLA, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Enxin Wang, Department of Digestive Diseases, Air Force Hospital of Western Theater Command, PLA, Chengdu, 610083, People’s Republic of China, Email [email protected] Lei Liu, Department of Infectious Diseases, Xijing Hospital, State Key Laboratory of Holistic Integrative Management of Gastrointestinal Cancers and Xijing Hospital of Digestive Diseases, Fourth Military Medical University, Xi’an, 710032, People’s Republic of China, Email [email protected]
Aim: The prognosis of hepatocellular carcinoma with extrahepatic spread (HCC-EHS) remains poor. While systemic therapy is standard, intrahepatic progression often drives mortality. This study evaluated whether combining transarterial chemoembolization (TACE) with sorafenib (TACES) improves outcomes versus TACE alone in HCC-EHS.
Methods: In this multicenter, retrospective study, 423 HCC-EHS patients (Child-Pugh A) were categorized into TACE-alone (n = 294) or TACES (n = 129) groups. The primary endpoint was overall survival (OS). Inverse probability of treatment weighting (IPTW) was used to adjust for confounding. Radiological response was assessed per mRECIST.
Results: After IPTW adjustment, the TACES group demonstrated significantly superior tumor response, with higher objective response (33.3% vs 16.4%, p = 0.004) and disease control rates (63.2% vs 46.3%, p = 0.008) compared to the TACE-alone group. This translated into a significant survival benefit, with a median OS of 10.4 months for TACES versus 7.0 months for TACE alone (IPTW-adjusted hazard ratio: 0.68; 95% CI: 0.52– 0.88; p = 0.004). The survival advantage remained consistent in landmark analyses. Subgroup analyses indicated that the absolute benefit from combination therapy was most pronounced in patients with high intrahepatic tumor burden and preserved liver function.
Conclusion: This real-world study demonstrates that in carefully selected patients with HCC-EHS, a combination of TACE and sorafenib provides significantly better tumor control and survival outcomes than TACE monotherapy. These findings suggest that an integrated therapeutic strategy, which aggressively manages the intrahepatic disease in conjunction with systemic therapy, can improve outcomes in this challenging-to-treat population and warrants validation in prospective studies.
Keywords: hepatocellular carcinoma, transarterial chemoembolization, sorafenib, survival
Introduction
According to the Barcelona Clinic Liver Cancer (BCLC) staging system, hepatocellular carcinoma (HCC) with extrahepatic spread (EHS) is classified as advanced stage, for which systemic therapy is the standard first-line recommendation.1–4 Among these advanced features, EHS represents an independent predictor of poor prognosis, with natural history studies and meta-analyses consistently demonstrating a median overall survival of less than 7 months for this patient population.5,6 The presence of EHS not only signifies systemic dissemination but also presents unique therapeutic challenges that remain inadequately addressed by current treatment paradigms.
While systemic agents constitute the standard of care for advanced HCC according to established guidelines,3,4 their efficacy in the specific subgroup of HCC-EHS patients remains suboptimal. Recent sub-group analyses from pivotal clinical trials and real-world evidence have revealed particularly limited survival benefits in this population, with objective response rates rarely exceeding 10% and median overall survival generally remaining below 10 months.7–9 This therapeutic plateau underscores the urgent need for more effective treatment strategies that can meaningfully improve outcomes for this challenging patient population.
An important clinical observation that informs potential treatment approaches is that patients with HCC-EHS frequently succumb to intrahepatic tumor progression and subsequent liver failure rather than direct consequences of extrahepatic lesions.10,11 This pattern of disease progression highlights the critical importance of controlling intrahepatic disease burden, even in the context of established extrahepatic metastases. Transarterial chemoembolization (TACE), though not formally recommended for advanced HCC by current guidelines, has been widely utilized in real-world practice for patients with significant intrahepatic tumor burden.12 Substantial evidence indicates that selected patients achieving radiographic response to TACE can derive meaningful survival benefit, particularly when intrahepatic disease represents the dominant clinical challenge.12–18
The combination of TACE with sorafenib presents a compelling therapeutic strategy for HCC-EHS, potentially leveraging synergistic mechanisms to address both intrahepatic and extrahepatic disease components.19–21 This combined approach aims to capitalize on the rapid cytoreductive capability of TACE against intrahepatic tumors while maintaining continuous systemic control through sorafenib’s anti-angiogenic and antiproliferative effects. However, the comparative effectiveness of TACE plus sorafenib versus TACE alone in this specific population remains inadequately investigated. Therefore, this multicenter, real-world study aimed to comprehensively compare the efficacy of TACE combined with sorafenib versus TACE alone in HCC-EHS patients, utilizing rigorous statistical methods to address potential confounding factors.
Patients And Methods
Study Population
Clinical data were extracted from a nation-wide database of HCC patients treated with TACE at sixteen Chinese tertiary centers from January 2013 to December 2023. HCC was diagnosed according to the treatment guidelines of European Association for the Study of Liver disease and American Association for the Study of Liver Disease.3,4 Current study screened 674 HCC patients receiving TACE as their initial treatment and diagnosed with EHS which was confirmed by pathological or imaging methods, such as digital radiography, contrast-enhanced computed tomography (CT) /magnetic resonance imaging (MRI), or bone scan. Through excluding 227 patients with Child-Pugh grade > A and 24 patients with Eastern Cooperative Oncology Group (ECOG) score > 1, 423 HCC patients with EHS were finally included in the whole cohort; excluding 25 patients missing radiological evaluation within 3 months after TACE, the remaining 398 patients were included in imaging assessment cohort (Figure 1).
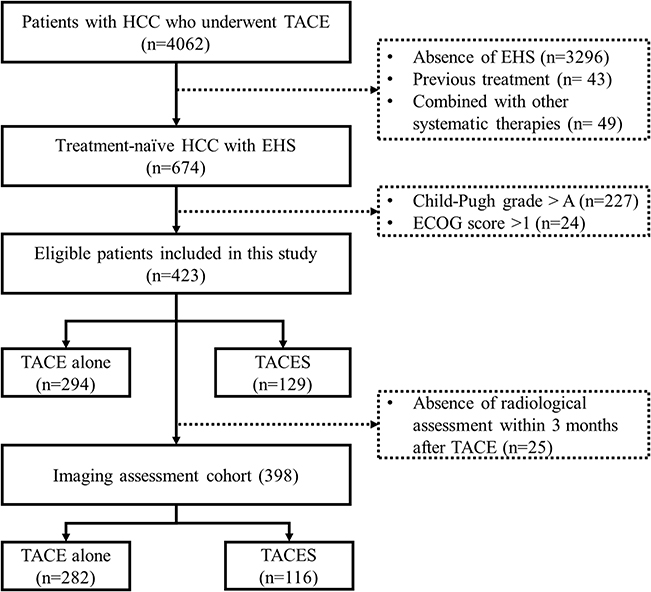 |
Figure 1 Flow-chart of the current study. |
Medical Treatment
Both conventional TACE (cTACE) and drug-eluting bead TACE (DEB-TACE) were permitted. No subgroup analysis was conducted due to the small sample size in each arm. cTACE regimens included doxorubicin (20–60 mg), epirubicin (30–70 mg), oxaliplatin (50–100 mg), or cisplatin (50–75 mg) emulsified with lipiodol (3–20 mL), followed by embolization using gelatin sponge or polyvinyl alcohol particles. DEB-TACE employed doxorubicin-loaded microspheres (70–300 μm). Superselective catheterization targeting segmental or subsegmental arteries was consistently pursued to achieve complete tumor embolization, performed at the most distal feasible level based on tumor vasculature, with the remainder performed at the lobar level. The choice of chemotherapeutic agents and doses, as well as the selection and volume of embolic materials, followed each center’s clinical practice, and all operators across centers had more than 8 years of TACE experience, ensuring procedural consistency despite inter-center variations. Currently, there are no definitive criteria for repeating TACE in patients with advanced HCC. In clinical practice, subsequent TACE sessions are typically considered when imaging confirms viable tumor (eg, new intrahepatic lesions or progression of treated lesions), provided that the patient’s liver function and performance status remain adequate. All retreatment decisions are made through multidisciplinary team discussion and require individual informed consent. Sorafenib was initially administered at a dosage of 400 mg twice daily, which was modified upon the development of adverse events and mainly according to an individual’s drug tolerance. Unless the toxicities were too serious to endure, the patients were typically encouraged to continue sorafenib therapy. Upon the occurrence of intolerable toxicity, the sorafenib dose was gradually reduced in a stepwise manner until the severity of the adverse events was considered acceptable by the patient. Temporary discontinuation was allowed in cases of persistent intolerability; in these patients, sorafenib treatment was reinitiated as soon as the toxicity became tolerable. Permanent discontinuation was also permitted if unmanageable or life-threatening adverse events occurred. For the whole cohort of 423 patients, there were 294 (69.5%) patients treated with mono TACE and 129 (30.5%) with TACE and concomitant systemic therapies (TACES) (Figure 1).
Follow-Up
According to the study protocol, laboratory examination was performed every four to six weeks; radiological evaluation was carried out during week fourth and eighth after TACE and every eight weeks thereafter using the contrast-enhanced CT or MRI, along with bone scan if applicable. Because of 25 patients missing the radiological evaluation within 3 months after TACE, the remaining 398 patients were included in imaging assessment cohort, with 282 (70.9%) patients in TACE group and 116 (29.1%) in TACES group. In our study, the radiological response was evaluated by two independent reviewers according to the modified Response Evaluation Criteria in Solid Tumors (mRECIST), which consisted of complete response (CR), partial response (PR), stable disease (SD) and progression disease (PD). Follow-up imaging data were unavailable for a subset of patients, which was attributed to mortality prior to the scheduled scan or clinical loss to follow-up. Overall survival (OS) was defined as the time from TACE initiation until the date of death or last follow-up; considering there were only 13 (3.1%) patients surviving more than 36 months, our study censoring them at the 36-month timepoint to ensure the robustness and precision of the data.
Statistics
Missing baseline data were handled using multiple imputation with chained equations (MICE). Five imputed datasets were created with 20 iterations per chain to ensure convergence, and estimates were pooled using Rubin’s rules. All analyses were performed on the pooled dataset. Categorical variables were described by frequencies and percentages, and continuous data as mean with standard deviation. Given the limited number of patients who underwent DEB-TACE, only 46 (15.7%) in the TACE alone group and 21 (16.33%) in the TACES group, these cases were pooled for analysis. To mitigate treatment selection bias and strengthen causal inference, we applied inverse probability of treatment weighting (IPTW). Propensity scores were derived from logistic regression incorporating the following covariates: diameter of the largest tumor, tumor number, age (> 60 years), gender, etiology, ECOG performance status, macrovascular invasion, extrahepatic metastasis (lung, bone, adrenal, and others), Child–Pugh score, alpha‑fetoprotein (≥ 400 ng/mL), albumin, total bilirubin, aspartate aminotransferase, creatinine, platelet count, and international normalized ratio. Weights were truncated at the 1st and 99th percentiles to limit the impact of extreme values and enhance stability. Covariate balance was evaluated using standardized mean differences (threshold < 0.1). Weighted Cox models employed robust sandwich estimators for variance, and the proportional hazards assumption was assessed via Schoenfeld residuals. Survival outcomes were analyzed through Kaplan-Meier curves with Log rank tests for unadjusted comparisons and IPTW-weighted survival curves with weighted Cox proportional hazards models for propensity-adjusted estimates, providing hazard ratios with 95% confidence intervals. Objective response rate (ORR, PR only) and disease control rate (DCR, PR + SD) analyzed using both unadjusted methods (chi-square tests, logistic regression) and IPTW-adjusted survey-weighted generalized linear models. To address immortal time bias, we conducted landmark analyses at both 3-month and 6-month timepoints, excluding patients who died before each landmark and analyzing subsequent survival trajectories from the landmark time forward. Extensive subgroup analyses explored treatment effect heterogeneity across pre-specified strata including age, macrovascular invasion (MVI), ECOG status, ALBI grade, and alpha-fetoprotein (AFP) levels through multivariable Cox regression, IPTW-adjusted models within strata, and formal interaction testing, visualized via forest plots displaying hazard ratios with confidence intervals and interaction p-values. Treatment benefit heterogeneity was further investigated using continuous interaction models with absolute risk reduction (ARR) and number needed to treat (NNT) calculations across predictor quantiles. Comprehensive sensitivity analyses validated findings through multiple statistical approaches, both unadjusted and fully adjusted models, rigorous balance diagnostics, and various subgroup definitions, all implemented in R version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria) with set random seed for reproducibility, following STROBE guidelines for observational research with statistical significance defined as two-tailed p < 0.05 and appropriate consideration for multiple testing in subgroup analyses.
Results
Patient Characteristics
Figures S1 and S2 present the missing data pattern and the post-imputation data distribution, respectively. Baseline characteristics of the entire study cohort (N=423) are summarized in Table 1. The study population had a mean age of 52.2 years, and most commonly had hepatitis B virus infection as the underlying etiology of liver disease (382 patients, 90.3%). Macrovascular invasion (MVI), involving the portal vein or inferior vena cava, was identified in 221 patients. Lymph nodes (247, 58.4%) were the most frequent site of EHS, followed by the lungs (133, 30.8%), bones (39, 9.2%), adrenal glands (27, 6.4%), and other sites (32, 7.6%). Most patients had only one (373, 88.2%) or two (45, 10.6%) types of EHS. After IPTW adjustment, balance improved substantially, with nearly all covariates falling below the 0.1 standardized mean difference threshold (Figure S3). Subsequent therapies were summarized in Table S1.
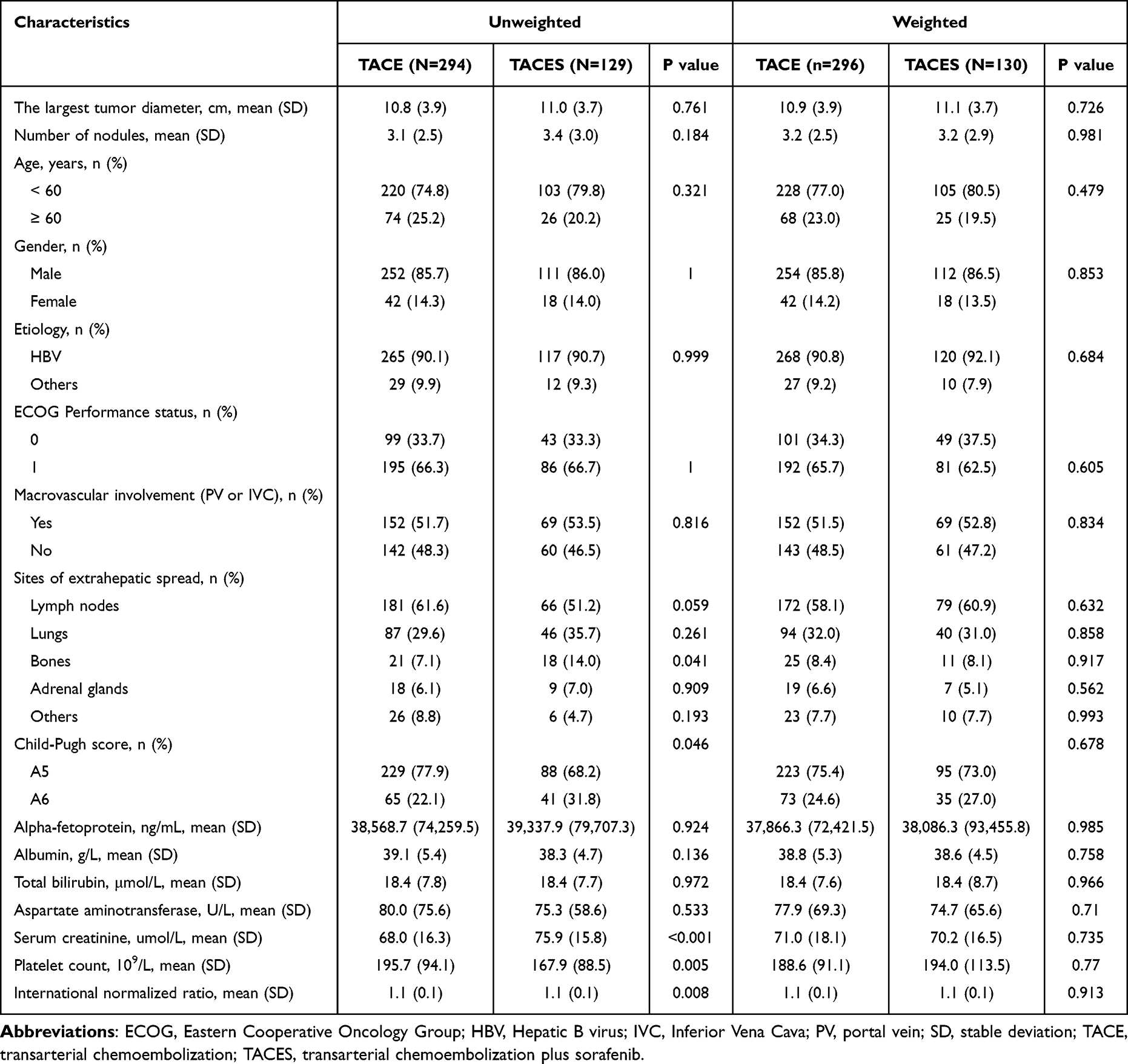 |
Table 1 Baseline Characteristics for Current Study Cohort |
Radiological Response Assessment
In total, there were 398 participants having available radiological evaluation according to mRECIST criteria within 3 months after TACE treatment and included in the imaging assessment cohort (Table 2). Before IPTW adjustment, no complete responses were observed in either group. The TACE group showed PR in 48 patients (17.0%), SD in 90 (31.9%), and PD in 144 (51.1%). Corresponding figures in the TACES group were 30 (25.9%), 37 (31.9%), and 49 (42.2%) patients, respectively. The ORR was significantly higher in the TACES group (25.9% vs 17.0%; Odds ratio [OR] = 1.70, 95% CI: 1.01–2.85; p = 0.045). Although the DCR was numerically higher with TACES (57.8% vs 48.9%), this difference did not reach statistical significance (OR = 1.43, 95% CI: 0.92–2.21; p = 0.136). Following IPTW adjustment, response distribution in the TACE group was 46 (16.4%) PR, 84 (29.9%) SD, and 151 (53.7%) PD, compared to 39 (33.3%) PR, 35 (29.9%) SD, and 43 (36.8%) PD in the TACES group. After propensity score weighting, TACES demonstrated significantly superior outcomes in both ORR (33.3% vs 16.4%; OR = 2.52, 95% CI: 1.34–4.72; p = 0.004) and DCR (63.2% vs 46.3%; OR = 1.98, 95% CI: 1.19–3.29; p = 0.008).
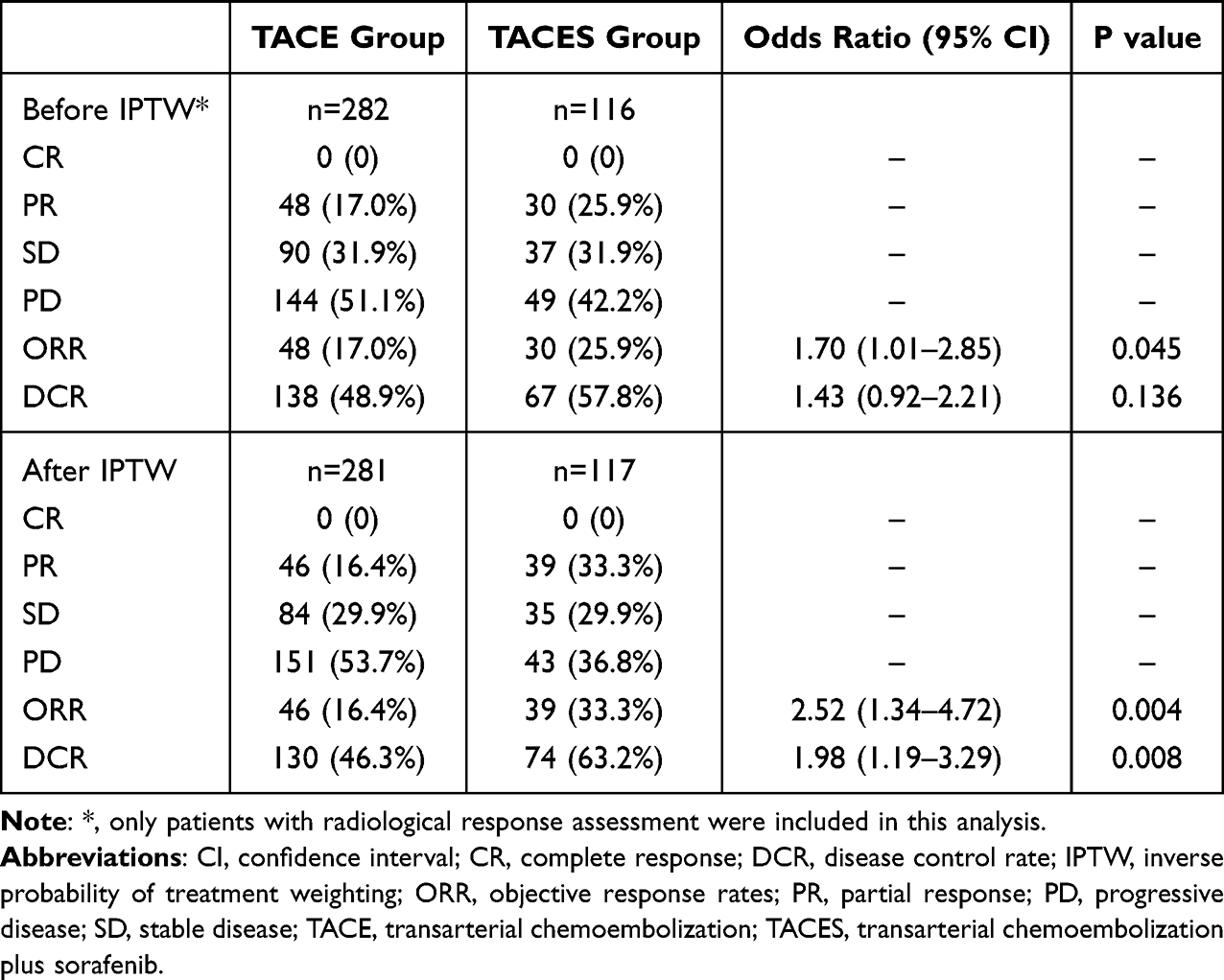 |
Table 2 Radiological Response Assessment Within 3 months After TACE |
Survival
During 4043.3 person-months of follow-up, 332 (78.5%) patients were died and only 13 (3.1%) patients remained alive. In unweighted samples, the TACES group showed a median overall survival of 8.7 months (95% CI: 7.5–10.5) compared to 7.3 months (95% CI: 6.4–8.3) in the TACE group, with no statistically significant difference observed (log-rank p = 0.15; Figure 2A). Consistent with this finding, landmark analyses conducted at 3 and 6 months also revealed no significant survival differences (p = 0.095, Figure 2C; p = 0.25, Figure 2E, respectively). Following IPTW adjustment, TACES was associated with significantly improved overall survival compared with TACE alone: median overall survival was 10.4 months (95% CI: 8.7–16.5) versus 7.0 months (95% CI: 5.3–8.2), respectively (log‑rank p = 0.004; Figure 2B). The IPTW‑adjusted hazard ratio was 0.68 (95% CI: 0.52–0.88, p = 0.004). The proportional hazards assumption was satisfied (global test p = 0.62; Figure S4), and robust variance estimation was employed. This survival benefit remained consistent in landmark analyses, demonstrating significant advantages at both 3 months (IPTW-adjusted HR: 0.64 [95% CI: 0.48–0.86], p = 0.003; Figure 2D) and 6 months (IPTW-adjusted HR: 0.66 [95% CI: 0.46–0.94], p = 0.02; Figure 2F).
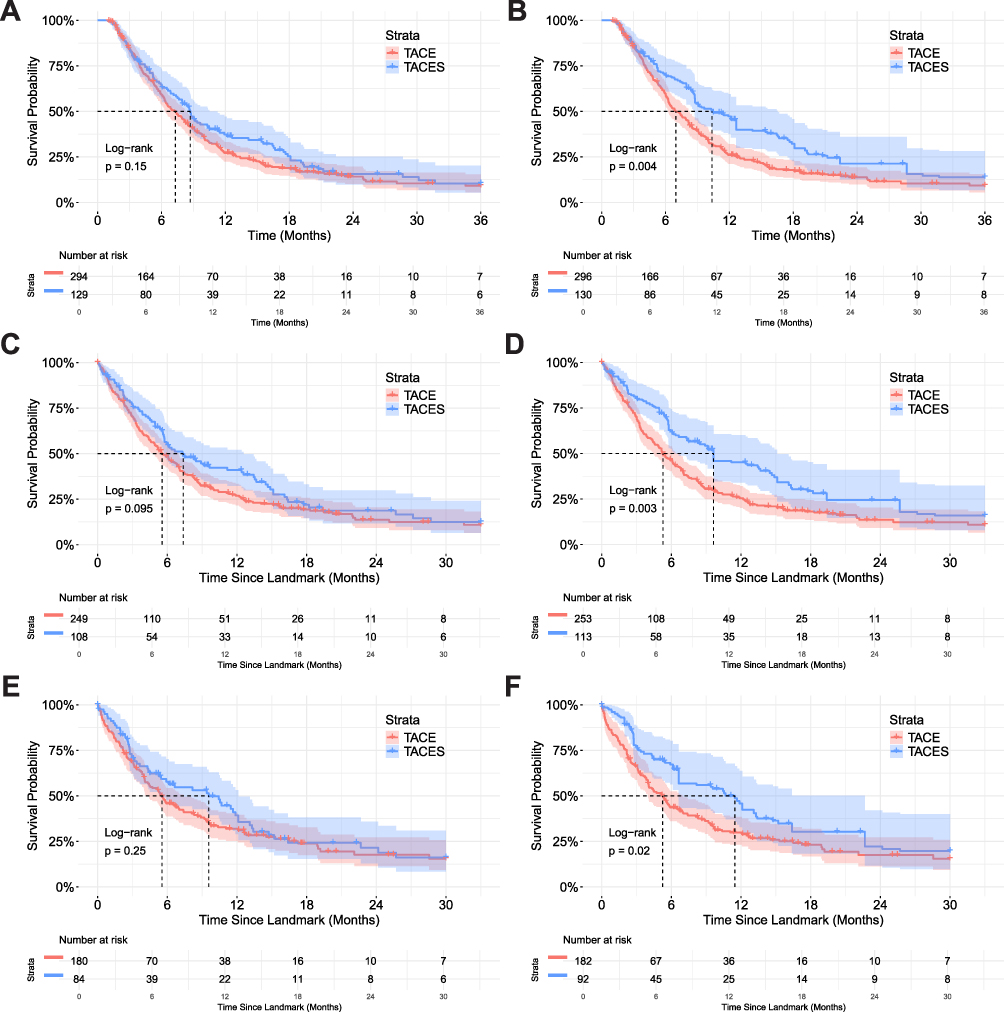 |
Figure 2 Kaplan-Meier survival curves comparing overall survival between patients receiving TACE and TACES treatments. (A) Overall survival (OS) analysis from initial treatment (unadjusted); (B) Inverse probability of treatment weighting (IPTW)-adjusted OS analysis from initial treatment; (C) Landmark analysis at 3 months (unadjusted); (D) IPTW-adjusted landmark analysis at 3 months; (E) Landmark analysis at 6 months (unadjusted); (F) IPTW-adjusted landmark analysis at 6 months. Log-rank p-values are shown for each comparison. The number of patients at risk at each time point is indicated below the survival curves. Abbreviations: TACE, transarterial chemoembolization; TACES, TACE combined with sorafenib. |
Prognostic Factors
In the multivariable analysis before IPTW, tumor number (HR: 1.08 [95% CI: 1.03–1.13], p < 0.001), AST (HR: 1.00 [95% CI: 1.00–100], p < 0.001) and INR (HR: 3.30 [95% CI: 1.20–9.11], p = 0.02) were consistent independent risk factors (Table 3). The abovementioned variables were consistently identified in the analysis after IPTW (Table 3). The IPTW-adjusted model further strengthened the findings, confirming TACES therapy (compared to TACE, HR: 0.66 [95% CI: 0.50–0.86], p = 0.002) as an additional independent predictor of improved outcomes, and identifying absence of other EHS as a significantly prognostic factor (Table 3).
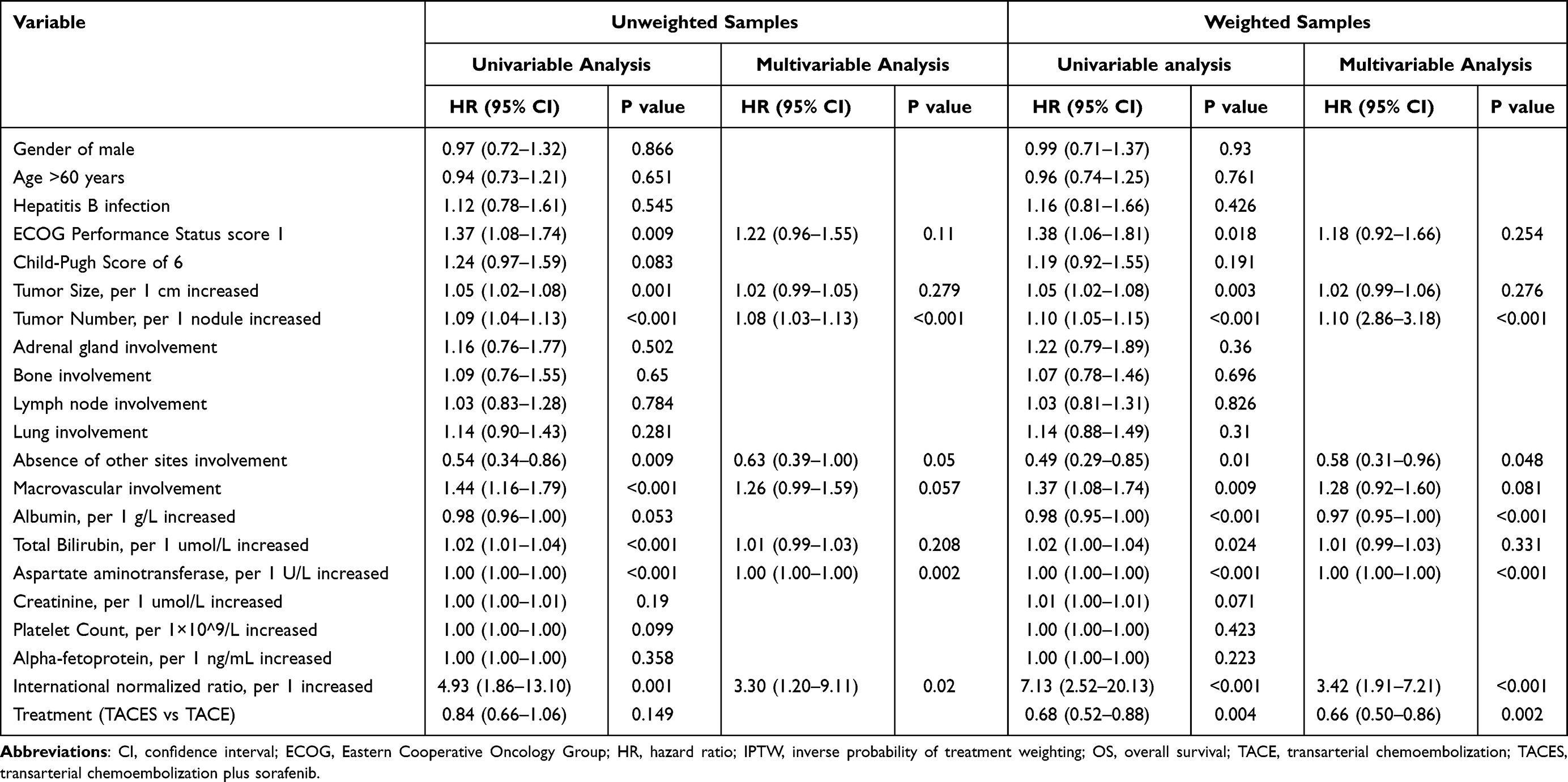 |
Table 3 Univariable and Multivariable Cox Analysis of OS Before and After IPTW |
Subgroup Analysis
After adjusting potential confounders, the prolonged OS were consistently observed in most subgroups before and after IPTW with absence of interaction between subgroups and treatment (Figure 3A and B). Multivariable Cox regression analyses incorporating IPTW were conducted to evaluate potential treatment effect modification by key baseline characteristics. However, trend analyses revealed notable patterns in ARR (Figure 4A–C). Specifically, patients with increased tumor size, and more preserved liver function (higher ALBI scores), and decreased tumor number, derived greater absolute benefit from TACES compared to TACE. This was supported by progressively increasing ARR values across quantiles (Figure 4D) and lower numbers needed to treat (NNT) in these high-risk subgroups (Figure 4E). No statistically significant interactions were detected between treatment type and tumor size (p = 0.396), tumor number (p = 0.667), or ALBI score (p = 0.518), suggesting that the treatment effects remained consistent across these patient subgroups (Figure 4F). Furthermore, the positive ARR in TACES group consistently identified in all categorical subgroups (Figure S5A and S5B).
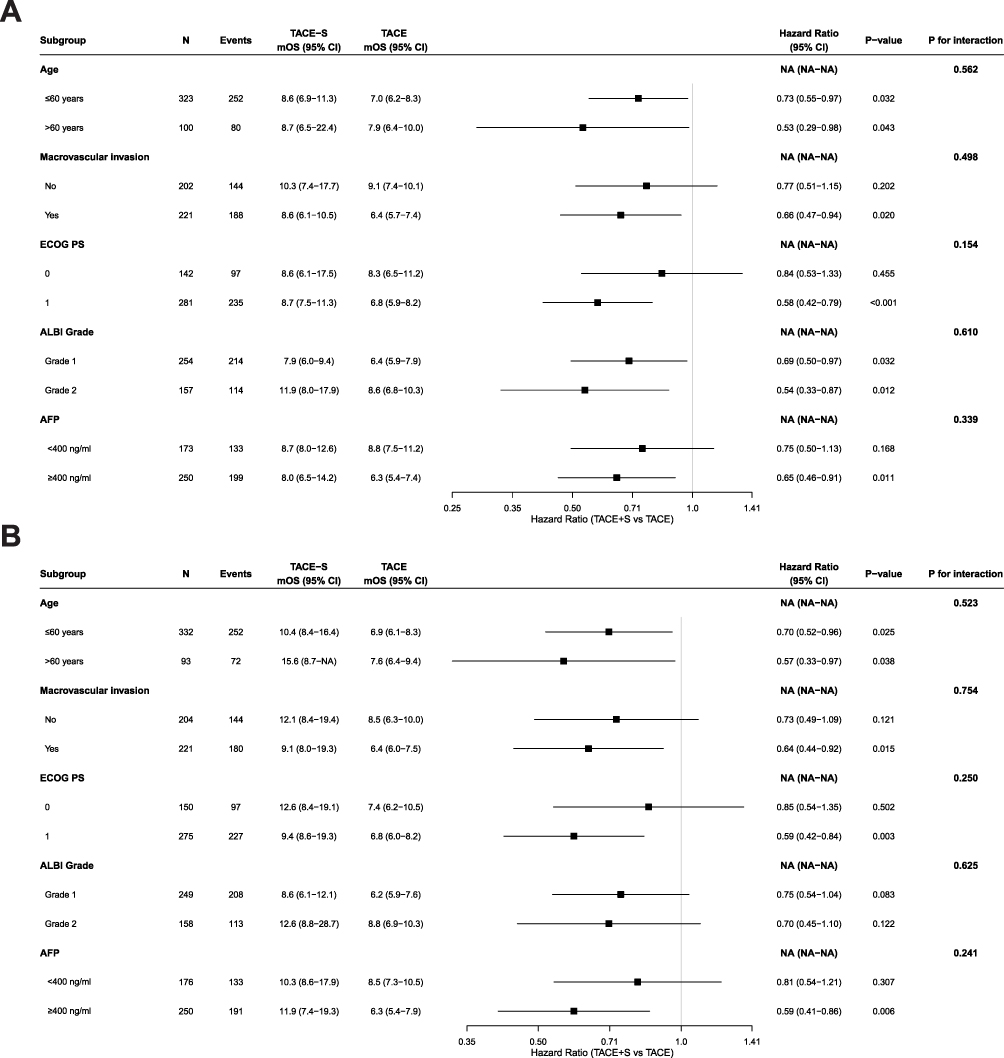 |
Figure 3 Events, survival rates, adjusted HRs and interaction test for overall survival by risk categories and treatment before (A) and after inverse probability of treatment weighting (B). |
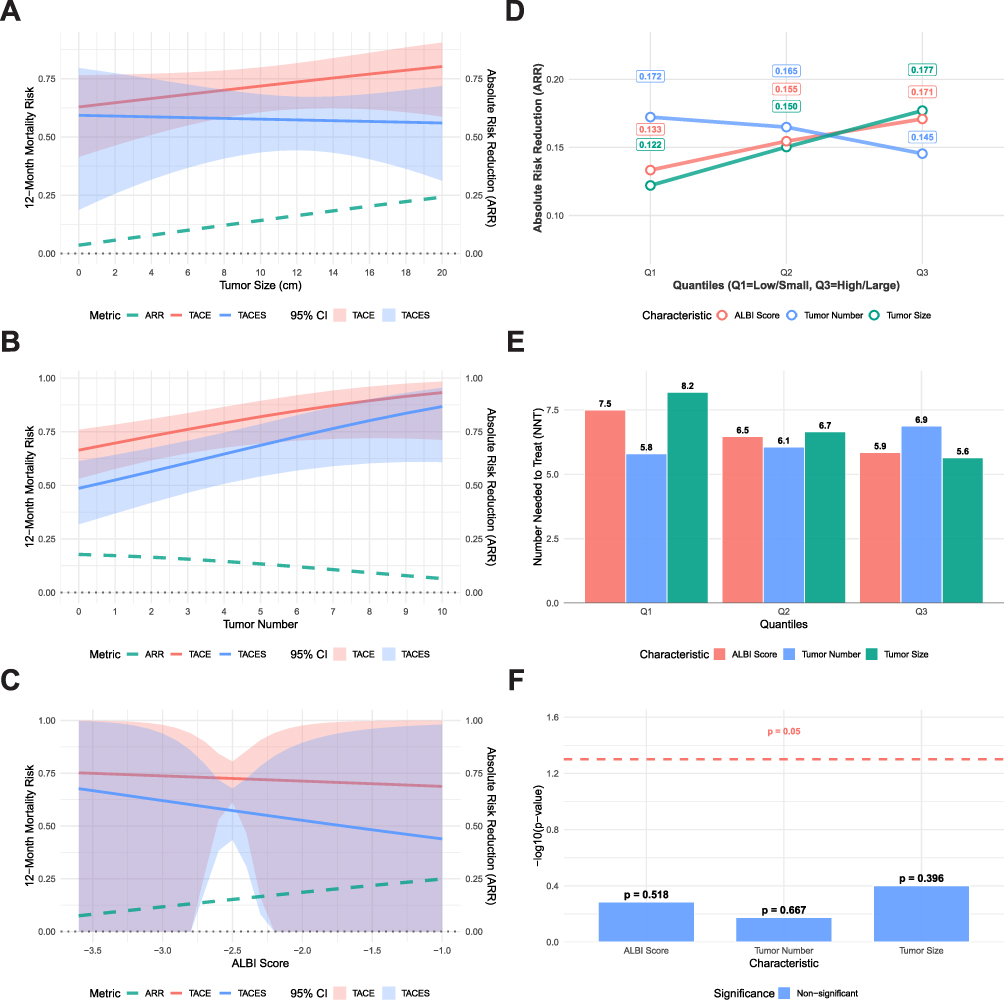 |
Figure 4 Treatment benefit assessment of TACES versus TACE alone after inverse probability of treatment weighting. (A–C) Absolute risk reduction (ARR) in 12-month mortality for TACES compared to TACE across different patient characteristics: (A) tumor size, (B) tumor number, and (C) ALBI score. The ARR and 95% confidence intervals are shown along with the estimated mortality risk for each treatment group. (D) Trends in absolute risk reduction (ARR) across quantiles (Q1 to Q3) of each characteristic. Q1 represents low ALBI score, few tumors, or small tumor size; Q3 represents high ALBI score, numerous tumors, or large tumor size. (E) Number needed to treat (NNT) across quantiles of each characteristic. Lower NNT indicates greater treatment efficiency. (F) Significance of treatment-characteristic interaction terms from multivariable Cox regression, expressed as –log10(p-value). A dashed line indicates the threshold for statistical significance (p = 0.05). All analyses are based on multivariable-adjusted models with IPTW. Abbreviations: TACE, transarterial chemoembolization; TACES, TACE combined with sorafenib; ALBI, albumin-bilirubin; ARR, absolute risk reduction; NNT, number needed to treat. |
Discussions
This multicenter real-world study offers valuable insights into the management of HCC with EHS, a population characterized by a particularly poor prognosis and for whom optimal treatment sequencing remains uncertain. The principal finding of this study is that combining TACE with sorafenib significantly enhances radiological response and, after rigorous inverse probability of treatment weighting (IPTW) adjustment for selection bias, confers a clinically meaningful survival advantage over TACE alone. The IPTW-adjusted hazard ratio of 0.68 (95% CI: 0.52–0.88) and the extension of median OS from 7.0 to 10.4 months underscore the potential of this combined modality approach, challenging the conventional paradigm that assigns locoregional therapy only a secondary role in systematically advanced disease.
One key aspect of our findings concerns the role of TACE in EHS patients with significant intrahepatic tumor burden. Although TACE is not recommended as first-line therapy for advanced HCC,3,4 our findings highlight its potential value in EHS patients with significant intrahepatic tumor burden. Effective management of intrahepatic lesions is particularly critical in this population, as liver tumor progression, rather than EHS, remains a leading cause of mortality.10,11,21 In this context, TACE provides rapid and definitive local control, contrasting with the generally slower onset and limited objective response rates of systemic therapies alone.15 The absence of an untreated control group precludes a definitive assessment of TACE’s therapeutic efficacy. While the observed ORR and DCR provide indirect evidence of biological activity, and the overall cohort survival of 7.8 months compares favorably with historical data of less than 7 months for untreated patients, a direct comparison with a contemporaneous untreated cohort would be necessary to objectively confirm whether TACE unequivocally prolongs survival in this population. The significantly higher objective response rate (ORR: 33.3% vs 16.4%) and disease control rate (DCR: 63.2% vs 46.3%) observed in the TACES group after IPTW adjustment provide compelling evidence that combining TACE’s rapid cytoreductive capacity with sorafenib’s systemic activity yields synergistic antitumor efficacy, addressing both intra‑ and extrahepatic disease. Mechanistically, the pronounced benefit seen in patients with high intrahepatic tumor burden may reflect not only the local‑systemic synergy of the two modalities, but also enhanced activation of programmed cell death pathways. Recent advances highlight the role of PANoptosis, an integrated pro‑inflammatory cell death pathway that converges pyroptosis, apoptosis, and necroptosis, in overcoming treatment resistance and immune evasion in HCC.22 We propose that TACE‑induced ischemia and inflammation, combined with sorafenib’s multi‑kinase inhibition, may cooperatively promote PANoptotic signaling, leading to more effective tumor clearance in high‑burden settings. This aligns with the evolving understanding that simultaneous engagement of multiple cell death pathways can improve outcomes in advanced HCC and underscores the biological rationale for multimodal therapy in this population. Our results thus support the concept that HCC with EHS, while systemically disseminated, often remains “liver-dominant” in its clinical impact, and that aggressive management of intrahepatic disease remains essential even in the presence of extrahepatic metastases.
Furthermore, while immune-based therapies represent the current standard for advanced HCC, patients with EHS continue to face limited therapeutic response and poor survival outcomes,23–25 underscoring the ongoing need to explore complementary treatment strategies. Our study demonstrates that in a carefully selected cohort of patients with preserved liver function (Child-Pugh A) and good performance status (ECOG 0–1), TACES can provide a meaningful survival benefit. This underscores that even in an era of systemic immunotherapies, the strategic integration of locoregional treatment may enhance outcomes, particularly in patients with liver-dominant disease. Importantly, TACES occupies a distinct clinical role today: it serves as an effective, accessible alternative for patients ineligible for or lacking access to newer ICI-based regimens, whether due to autoimmune conditions, economic or regional constraints, or high intrahepatic tumor burden requiring local control. This pragmatic approach ensures therapeutic continuity in settings where newer standards are not feasible, and reinforces that considerations of accessibility and equity must remain integral to both clinical decision-making and guideline development. Importantly, for patients who progress following TACES, particularly those who retain preserved liver function, transitioning to immunotherapy merits clinical consideration and further investigation. The emerging concept of ICI rechallenge in HCC provides a relevant framework: it demonstrates that reintroducing immune checkpoint inhibition, often with an altered mechanism or combination, can regain antitumor activity even after prior immunotherapy exposure or failure.26 Building on this principle, patients progressing after TACES may similarly benefit from subsequent ICI-based therapy, as their tumors have been preconditioned by the immunomodulatory effects of prior locoregional and antiangiogenic treatment. Future prospective studies should evaluate the efficacy and safety of established ICI combinations, such as atezolizumab plus bevacizumab or dual checkpoint blockade, in this sequential setting. Such an approach could extend the therapeutic continuum for EHS patients and represents a logical, biologically informed strategy to address progression after combined modality therapy.
A critical consideration in interpreting our findings is the potential influence of socioeconomic factors on treatment selection. Throughout most of the study period, sorafenib was not covered by national health insurance in China and posed a substantial financial barrier for many patients. This economic reality inevitably influenced clinical decision-making, resulting in a scenario in which patients receiving TACE alone were not only selected based on clinical criteria but were also frequently those for whom combination therapy was financially inaccessible. This introduces a potential socioeconomic confounder that, while partially mitigated by IPTW adjustment for measured clinical variables, may still residually affect the observed outcomes. Therefore, our results should be interpreted as reflecting the comparative effectiveness of TACES versus TACE monotherapy under real-world constraints, rather than a pure efficacy comparison unaffected by access-to-care issues.
Several limitations of this study should be acknowledged. First, the retrospective design, despite sophisticated statistical adjustment, cannot fully eliminate residual confounding. Second, the retrospective design precluded the prospective, standardized collection of safety data. The inability to provide a robust analysis of treatment-related adverse events therefore constitutes an important limitation of this study. While the established safety of TACES, as confirmed by prior prospective research, allows this retrospective analysis to focus primarily on evaluating its comparative effectiveness. Third, the specific timing and reasons for initiating or discontinuing systemic therapy in relation to TACE procedures were not consistently documented, limiting our understanding of the optimal sequencing strategy.
Conclusion
In conclusion, this study demonstrates that combining TACE with sorafenib significantly improves tumor response and survival outcomes in carefully selected patients with HCC and EHS compared to TACE alone. These findings challenge the conventional therapeutic paradigm and suggest that patients with HCC-EHS, particularly those with significant intrahepatic tumor burden and preserved liver function, may derive meaningful benefit from an integrated strategy that addresses both intrahepatic and extrahepatic disease components, even in the current era of advanced systemic therapies. Prospective randomized trials are warranted to validate these findings and refine patient selection criteria for combined-modality therapy in this challenging clinical population.
Abbreviation
AFP, alpha-fetoprotein; ARR, absolute risk reduction; BCLC, Barcelona Clinic Liver Cancer; CR, complete response; DCR, disease control rate; ECOG, Eastern Cooperative Oncology Group; EHS, extrahepatic spread; HR, hazard ratio; IPTW, inverse probability of treatment weighting; HCC, hepatocellular carcinoma; mRECIST, modified Response Evaluation Criteria in Solid Tumors; MVI, macrovascular invasion; NNT, number needed to treat; ORR, objective response rate; OS, overall survival; PD, progression disease; PR, partial response; SD, stable disease; TACE, transarterial chemoembolization; TACES, transarterial chemoembolization plus sorafenib.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to containing information that could compromise research participant privacy but are available from the corresponding author (Prof. Lei Liu) on reasonable request and with permission of the local Institutional Review Board.
Ethics Approval Statement
The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Medical Ethics Committee of the First Affiliated Hospital of Air Force Military Medical University (Review Number:KY20233099-1). Given that this is a retrospective study, no biological sample collection or invasive interventions were conducted at any stage of the research, meaning there was no expected harm to the study participants. Additionally, strict measures have been put in place to eliminate any risk of personal privacy being compromised. For these considerations, individual informed consent for the study was exempted by the Medical Ethics Committee of the First Affiliated Hospital of Air Force Military Medical University, in accordance with its ethical review guidelines.
Acknowledgments
The authors sincerely thank all the patients and their families for participating in this study, without whom this research would not have been possible. We are grateful to the clinical and research staff at all participating centers for their invaluable contributions to patient care and data collection. Special thanks are due to our statistician, Dongdong Xia, from Fourth Military Medical University, for his expert guidance and rigorous statistical analysis.
Author Contributions
Enxin Wang and Lei Liu shared co-corresponding authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (Grant Numbers 82173143 and 82373409). The authors also acknowledge the support from the Shaanxi Outstanding Youth Science Fund Project (Grant Number 2024JC-JCQN-78). The funders had no role in the study design, data collection, analysis, interpretation, or writing of the manuscript.
Disclosure
All authors have nothing to disclose.
References
1. Hwang SY, Danpanichkul P, Agopian V, et al. Hepatocellular carcinoma: updates on epidemiology, surveillance, diagnosis and treatment. Clin Mol Hepatol. 2025;31:S228–S254. doi:10.3350/cmh.2024.0824
2. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76:681–693. doi:10.1016/j.jhep.2021.11.018
3. Singal AG, Llovet JM, Yarchoan M, et al. AASLD practice guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78:1922–1965. doi:10.1097/HEP.0000000000000466
4. European association for the study of the l. EASL clinical practice guidelines on the management of hepatocellular carcinoma. J Hepatol. 2025;82:315–374. doi:10.1016/j.jhep.2024.08.028
5. Llovet JM, Bustamante J, Castells A, et al. Natural history of untreated nonsurgical hepatocellular carcinoma: rationale for the design and evaluation of therapeutic trials. Hepatology. 1999;29:62–67. doi:10.1002/hep.510290145
6. Cabibbo G, Maida M, Genco C, et al. Natural history of untreatable hepatocellular carcinoma: a retrospective cohort study. World J Hepatol. 2012;4:256–261. doi:10.4254/wjh.v4.i9.256
7. Uka K, Aikata H, Takaki S, et al. Clinical features and prognosis of patients with extrahepatic metastases from hepatocellular carcinoma. World J Gastroenterol. 2007;13:414–420. doi:10.3748/wjg.v13.i3.414
8. Bruix J, Raoul JL, Sherman M, et al. Efficacy and safety of sorafenib in patients with advanced hepatocellular carcinoma: subanalyses of a Phase III trial. J Hepatol. 2012;57:821–829. doi:10.1016/j.jhep.2012.06.014
9. Cheng AL, Guan Z, Chen Z, et al. Efficacy and safety of sorafenib in patients with advanced hepatocellular carcinoma according to baseline status: subset analyses of the phase III Sorafenib Asia-Pacific trial. Eur J Cancer. 2012;48:1452–1465. doi:10.1016/j.ejca.2011.12.006
10. Uchino K, Tateishi R, Shiina S, et al. Hepatocellular carcinoma with extrahepatic metastasis: clinical features and prognostic factors. Cancer. 2011;117:4475–4483. doi:10.1002/cncr.25960
11. Sohn W, Paik YH, Cho JY, et al. Sorafenib therapy for hepatocellular carcinoma with extrahepatic spread: treatment outcome and prognostic factors. J Hepatol. 2015;62:1112–1121. doi:10.1016/j.jhep.2014.12.009
12. Park JW, Chen M, Colombo M, et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: the BRIDGE Study. Liver Int. 2015;35:2155–2166. doi:10.1111/liv.12818
13. Wang E, Liu L, Xia D, et al. Chemoembolization for hepatocellular carcinoma in patients with extrahepatic spread: prognostic determinants and appropriate candidates. J Vasc Interv Radiol. 2017;28:956–962. doi:10.1016/j.jvir.2017.02.016
14. Kim J, Sinn DH, Choi MS, et al. Hepatocellular carcinoma with extrahepatic metastasis: are there still candidates for transarterial chemoembolization as an initial treatment? PLoS One. 2019;14:e0213547. doi:10.1371/journal.pone.0213547
15. Xia D, Wang Q, Bai W, et al. Optimal time point of response assessment for predicting survival is associated with tumor burden in hepatocellular carcinoma receiving repeated transarterial chemoembolization. Eur Radiol. 2022;32:5799–5810. doi:10.1007/s00330-022-08716-4
16. Yoo DJ, Kim KM, Jin YJ, et al. Clinical outcome of 251 patients with extrahepatic metastasis at initial diagnosis of hepatocellular carcinoma: does transarterial chemoembolization improve survival in these patients? J Gastroenterol Hepatol. 2011;26:145–154. doi:10.1111/j.1440-1746.2010.06341.x
17. Lee IC, Huo TI, Huang YH, et al. Transarterial chemoembolization can prolong survival for patients with metastatic hepatocellular carcinoma: a propensity score matching analysis. Hepatol Int. 2012;6:753–762. doi:10.1007/s12072-011-9322-7
18. Pinter M, Hucke F, Graziadei I, et al. Advanced-stage hepatocellular carcinoma: transarterial chemoembolization versus sorafenib. Radiology. 2012;263:590–599. doi:10.1148/radiol.12111550
19. Zhao Y, Bai W, Ding R, et al. Transarterial chemoembolization plus sorafenib versus sorafenib alone in advanced hepatocellular carcinoma (SELECT): a multicenter, phase 3, randomized, controlled trial. Liver Cancer;2025. 1–14. doi:10.1159/000546530
20. Choi GH, Shim JH, Kim MJ, et al. Sorafenib alone versus sorafenib combined with transarterial chemoembolization for advanced-stage hepatocellular carcinoma: results of propensity score analyses. Radiology. 2013;269:603–611. doi:10.1148/radiol.13130150
21. Peng Z, Chen S, Wei M, et al. Advanced recurrent hepatocellular carcinoma: treatment with sorafenib alone or in combination with transarterial chemoembolization and radiofrequency ablation. Radiology. 2018;287:705–714. doi:10.1148/radiol.2018171541
22. Xiang J, Li Y, Mei S, et al. Novel diagnostic and therapeutic strategies based on PANoptosis for hepatocellular carcinoma. Cancer Biol Med. 2025;22:928–939. doi:10.20892/j.issn.2095-3941.2025.0150
23. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med. 2020;382:1894–1905. doi:10.1056/NEJMoa1915745
24. Rimassa L, Chan SL, Sangro B, et al. Five-year overall survival update from the HIMALAYA study of tremelimumab plus durvalumab in unresectable HCC. J Hepatol. 2025;83:899–908. doi:10.1016/j.jhep.2025.03.033
25. Yau T, Galle PR, Decaens T, et al. Nivolumab plus ipilimumab versus lenvatinib or sorafenib as first-line treatment for unresectable hepatocellular carcinoma (CheckMate 9DW): an open-label, randomised, phase 3 trial. Lancet. 2025;405:1851–1864. doi:10.1016/S0140-6736(25)00403-9
26. Li J, Liang YB, Wang Q-B, et al. Rechallenge with immune checkpoint inhibitors in patients with hepatocellular carcinoma: a narrative review. Liver Cancer. 2025. doi:10.1159/000549355
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of TACE Combined with Regorafenib Plus PD-1 Inhibitor in the Treatment of Hepatocellular Carcinoma After Sorafenib Resistance
Zou X, Xu Q, You R, Yin G
Journal of Hepatocellular Carcinoma 2023, 10:267-279
Published Date: 16 February 2023
Transarterial Chemoembolization Plus Sorafenib versus Transarterial Chemoembolization Alone for Advanced Hepatocellular Carcinoma: An Umbrella Review of Meta-Analyses and Systematic Reviews
Yan J, Wen Y, Deng M, Ye B, Liu X, Zhang L
Journal of Hepatocellular Carcinoma 2023, 10:1723-1733
Published Date: 5 October 2023
Changes in Posttreatment Spleen Volume Associated with Immunotherapy Outcomes for Advanced Hepatocellular Carcinoma

Chen BB, Liang PC, Shih TTF, Liu TH, Shen YC, Lu LC, Lin ZZ, Hsu C, Hsu CH, Cheng AL, Shao YY
Journal of Hepatocellular Carcinoma 2024, 11:1015-1029
Published Date: 5 June 2024
Sorafenib Combined with Tislelizumab and Transarterial Chemoembolization for Advanced-Stage Hepatocellular Carcinoma: A Phase II Study
Liang L, Zhou J, Huang J, Guo Y, Zhou Z, Chen Y, Lin L, Hong X, Shi W, Lin Z, Liu J, Zhu K, Huang W, Cai M
ImmunoTargets and Therapy 2025, 14:1187-1200
Published Date: 25 October 2025
Extent of Embolization as an Independent Prognostic Factor in Superselective Conventional Transarterial Chemoembolization for Hepatocellular Carcinoma
Okumura K, Ogi T, Matsumoto J, Asato N, Kitao A, Kobayashi S, Kozaka K
Journal of Hepatocellular Carcinoma 2026, 13:573705
Published Date: 26 February 2026