Back to Journals » International Journal of Women's Health » Volume 17
Clinical Prognostic Factors for Overall Survival in Patients Undergoing Radical Radiotherapy for Cervical Cancer
Authors Hao F ![]() , Xiao N, Wang M, Sang H, Luo J, Song J
, Xiao N, Wang M, Sang H, Luo J, Song J
Received 31 May 2025
Accepted for publication 10 September 2025
Published 29 September 2025 Volume 2025:17 Pages 3347—3359
DOI https://doi.org/10.2147/IJWH.S543995
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Fangfang Hao,1,* Nanfeng Xiao,1,* Meng Wang,2,* Houyi Sang,3 Judong Luo,2,3 Jing Song4
1Department of Obstetrics and Gynecology, Jiangnan University, Wuxi, Jiangsu, People’s Republic of China; 2Department of Radiotherapy, Tongji Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 3Department of Radiotherapy, The Affiliated Changzhou Second People’s Hospital of Nanjing Medical University, Nanjing Medical University, Changzhou, People’s Republic of China; 4Department of Obstetrics and Gynecology, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Song, Email [email protected] Judong Luo, Email [email protected]
Objective: Cervical carcinoma (CC) represents the predominant malignancy affecting the female population, with patient outcomes being a critical focus of clinical investigation. This research conducts a comprehensive evaluation of the clinical determinants influencing short-term survival rates in CC patients receiving definitive radiotherapy treatment.
Methods: A total of 99 cervical cancer patients who received radical radiotherapy between April 2017 and March 2022 at two medical institutions were retrospectively examined. Clinical outcomes were evaluated using the Kaplan-Meier method and the Cox proportional hazards model.
Results: A total of ninety - nine patients with cervical cancer who received radical radiotherapy were included in the study. The overall survival (OS) rate at 2 - year follow - up was 77.8%.COX unifactorial and multifactorial showed that the analysis of prognostic-related factors suggested that the higher the history of miscarriage and FIGO stage, the lower 2-year OS, and that the history of miscarriage and FIGO stage were independent factors affecting the short-term overall survival, and the difference of all of them was statistically significant (P < 0.05).
Conclusion: A history of miscarriage and the FIGO classification stage serve as independent predictors of overall survival (OS) during the initial 24-month period for cervical carcinoma patients undergoing definitive radiotherapy. This study conducted a comprehensive analysis of short-term prognostic indicators for cervical squamous cell carcinoma patients undergoing radical chemoradiotherapy.
Keywords: cervical cancer, radical radiotherapy, overall survival, prognostic
Introduction
Globally, cervical carcinoma represents a predominant malignancy in female populations, exhibiting the second most elevated fatality rate following mammary gland cancer. In terms of prevalence, it consistently maintains a position within the leading trio of cancer occurrences. Specifically, in nations undergoing developmental transitions and those in transitional phases, this neoplasm occupies the second and third positions in incidence rankings, respectively, succeeding pulmonary and breast carcinomas in frequency.1 Statistical data indicates that over 58% of worldwide cervical carcinoma incidents are concentrated in the Asian continent, where more than 50% of total mortality cases are recorded. The epidemiological distribution reveals that China contributes to 18% of the global cervical cancer incidence rate, corresponding to 17% of total fatalities associated with this malignancy.2 The predominant histological type observed in cervical malignancies is squamous cell carcinoma, with therapeutic interventions primarily encompassing surgical procedures, radiation therapy, and chemotherapeutic agents. Surgery is typically indicated for patients with early-stage cervical cancer, specifically those in stage IA1-IB1 who have no contraindications to the procedure, and for locally advanced (stages IB3 and IIA2) and intermediate to advanced (stages IIB to IVA), as well as other early-stage (stages IA1-IB1) patients, radiotherapy and chemotherapy are just crucial.3 Radiotherapy serves as both a primary therapeutic option for locally advanced cervical cancer (LACC) and an adjunctive treatment for postoperative patients with early-stage cervical cancer.4 However, according to previous studies, there is still a small amount of recurrence and metastasis after radical radiotherapy, and the local recurrence rate of patients after radiotherapy is about 30% ~ 44%,5 the recurrence rate among patients diagnosed with stage IB -IIA and IIB cervical squamous cell carcinoma (SCC) following radical radiotherapy is approximately 30%. This rate escalates to 50% for those in stage III of the disease6 and the recurrence of radiotherapy leads to the cervical cancer patients with a decrease in the overall survival rate. To enhance the overall survival rate following radiotherapy for this specific condition, there has been increasing focus on prognostic prediction. SCC, as the main type of cervical cancer, has a significant impact on overall survival rates. To conduct a more precise evaluation of SCC, histological subtypes other than squamous cell carcinoma, such as adenocarcinomas, were systematically omitted from the study. This scientific inquiry is designed to identify and analyze the indicators of short-term prognosis in patients with SCC receiving radical radiation treatment.
Materials and Methods
Data Collection
We retrospectively reviewed the medical records of 99 cases of histologically confirmed SCC of the cervix from two participating treatment centers, Jiangnan University Hospital and Changzhou Second People’s Hospital.All patients received curative radiotherapy during the five-year period from April 2017 to March 2022. The research population consisted of patients who had received a confirmed histological diagnosis of SCC. Inclusion criteria required participants to meet the FIGO 2018 classification criteria for disease staging, undergo radical radiotherapy as primary treatment without surgical intervention, and complete pelvic CT imaging examinations both pre- and post-treatment. The participant selection process is illustrated in Figure 1. The study exclusion criteria encompassed participants presenting with any of the following circumstances: previous surgical intervention for cervical carcinoma, incomplete clinical documentation, concurrent malignancies, non-adherence to scheduled follow-up appointments, or suboptimal imaging quality. The variables we analyzed were obtained from patients’ electronic medical records. The baseline data for SCC-Ag, LMR (lymphocyte-to-monocyte ratio), NLR (neutrophil-to-lymphocyte ratio), and PLR (platelet-to-lymphocyte ratio) prior to radiotherapy were laboratory data from within one week before radiotherapy. The presence or absence of HPV infection was determined using a combined HPV and Pap smear test. Post-radiotherapy intestinal reactions, urinary tract reactions, white blood cell counts, platelet counts, and hemoglobin levels were categorized based on the lowest values recorded throughout the entire radiotherapy process from initiation to completion. Tumor dimensions were determined based on pre-radiotherapy CT imaging findings, with the largest measurable diameter serving as the primary parameter for classification. The cohort was stratified using a 40-mm threshold as the grouping criterion. Patients with comorbid other cancers and patients who died from non-squamous cervical cancers were excluded throughout the follow-up, and death was the primary outcome of the event during follow-up; therefore, recurrence or metastasis during follow-up were not included in the influencing factors studied.
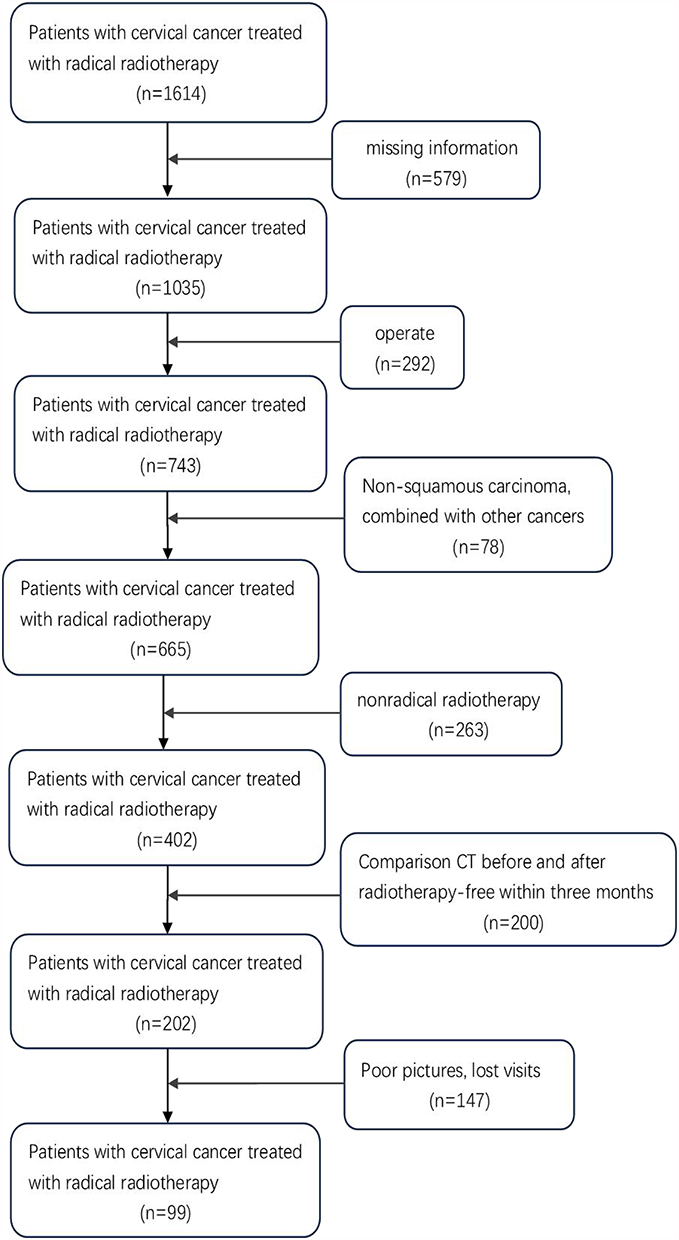 |
Figure 1 Patients flow chart. |
Treatments
The therapeutic protocol employed a bimodal strategy combining teletherapy (EBRT) and intracavitary radiation (BT). The pelvic region was subjected to external beam radiotherapy employing a three-dimensional conformal technique. Patients received radiation therapy at total doses varying between 45.0 and 50.4 Gy, with individual fraction sizes of 1.8 to 2.0 Gy administered in daily treatment sessions. The treatment protocol consisted of five consecutive sessions per week, with a two-day interval between treatment cycles. After external irradiation, CT image-guided intracavitary back-loaded radiotherapy was performed, 5. 0 Gy / times, 4 ~ 6 times in total, 1 ~ 2 times per week. Synchronous chemotherapy was platinum-based.
Follow-Up
The study cohort underwent systematic post-radiotherapy surveillance, extending from treatment completion until patient mortality or the study’s endpoint in March 2024. The observation protocol implemented a median observation period of 33 months, with monitoring intervals structured as follows: quarterly assessments during the initial two years, semi-annual evaluations between years three and five, and annual check-ups beyond the five-year mark. The primary outcome indicator for follow-up was overall survival. The duration of overall survival (OS) was calculated as the interval commencing from treatment initiation and extending to either mortality due to any factor or the last documented follow-up assessment.
Statistical Analysis
All statistical computations were executed through the application of SPSS (Statistical Package for the Social Sciences), version 27.0. Kaplan-Meier methodology was utilized to construct survival curves, while COX proportional hazards regression models were applied for univariate and multivariate analyses. The criterion for statistical significance was set at P < 0.05.
Result
This research investigation incorporated a final cohort comprising 99 participants who had received a confirmed diagnosis of SCC. In this retrospective analysis, the patient cohort demonstrated a median age of six decades, with the age distribution extending from 35 to 86 years. The inflammatory markers were computed using standard formulas: NLR (neutrophil-to-lymphocyte ratio) was derived from pre-radiotherapy hematological parameters by dividing neutrophil counts by lymphocyte counts; PLR (platelet-to-lymphocyte ratio) was calculated as platelet counts divided by lymphocyte counts; while LMR (lymphocyte-to-monocyte ratio) was established through lymphocyte counts divided by monocyte counts. For statistical analysis, stratification was performed using median values as cut-off points for age, LMR, NLR, and PLR. Table 1 provides a comprehensive overview of the patients’ fundamental clinical parameters, categorized by their survival status (alive or deceased).
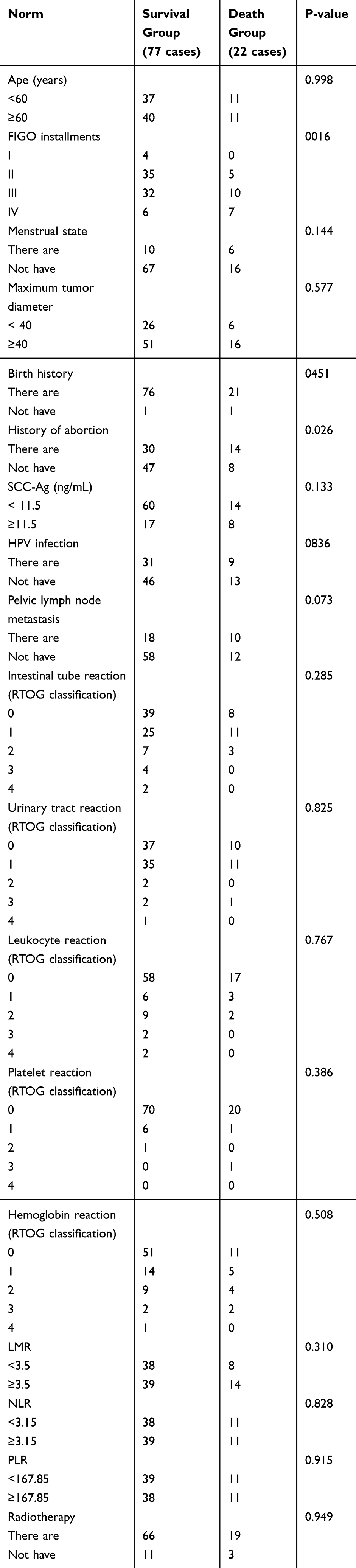 |
Table 1 Distribution of Patient Parameters |
The two-year overall survival (OS) rate across the study cohort was 77.8%, comprising both surviving patients (n=77) and deceased cases (n=22). When stratified by disease stage, patients diagnosed with stage II and III SCC, which represent the most prevalent stages, demonstrated distinct survival outcomes, with 87.5% and 76.2% 2-year OS rates, respectively. The later the stage, the progressively lower their 2-year survival rate (Figure 2). The following factors demonstrated no statistically significant associations: patient age, menopausal status, tumor size (maximum diameter), reproductive history, pretreatment SCC-Ag levels, HPV infection status, pelvic lymph node involvement, gastrointestinal and urinary tract responses to radiation therapy, hematologic parameters (including leukocyte, platelet, and hemoglobin classifications), systemic inflammatory markers (LMR, NLR, PLR), and chemotherapy administration status. Through univariate assessment, significant correlations were observed regarding FIGO classification and history of miscarriage (HR=2.426, 95% CI: 1.106–5.318, P=0.027; HR=4.073, 95% CI: 1.316–12.607; P=0.015). The comprehensive multifactorial evaluation encompassed all singular variables, demonstrating result consistency with the univariate examination. Notably, FIGO classification and history of miscarriage were identified as crucial prognostic indicators in cervical squamous cell carcinoma cases (See Table 2).
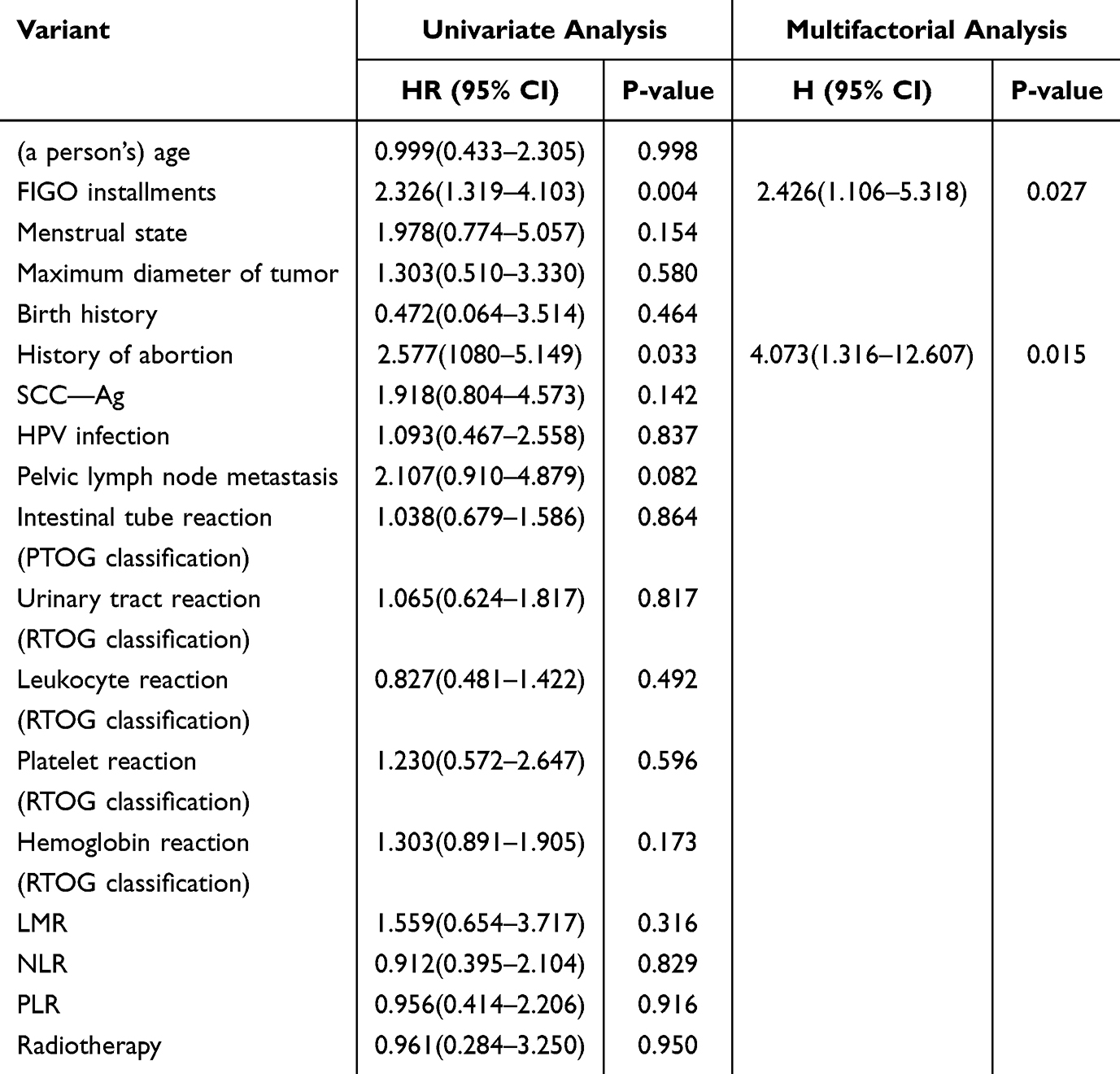 |
Table 2 Unifactorial and Multifactorial Analyses of COX |
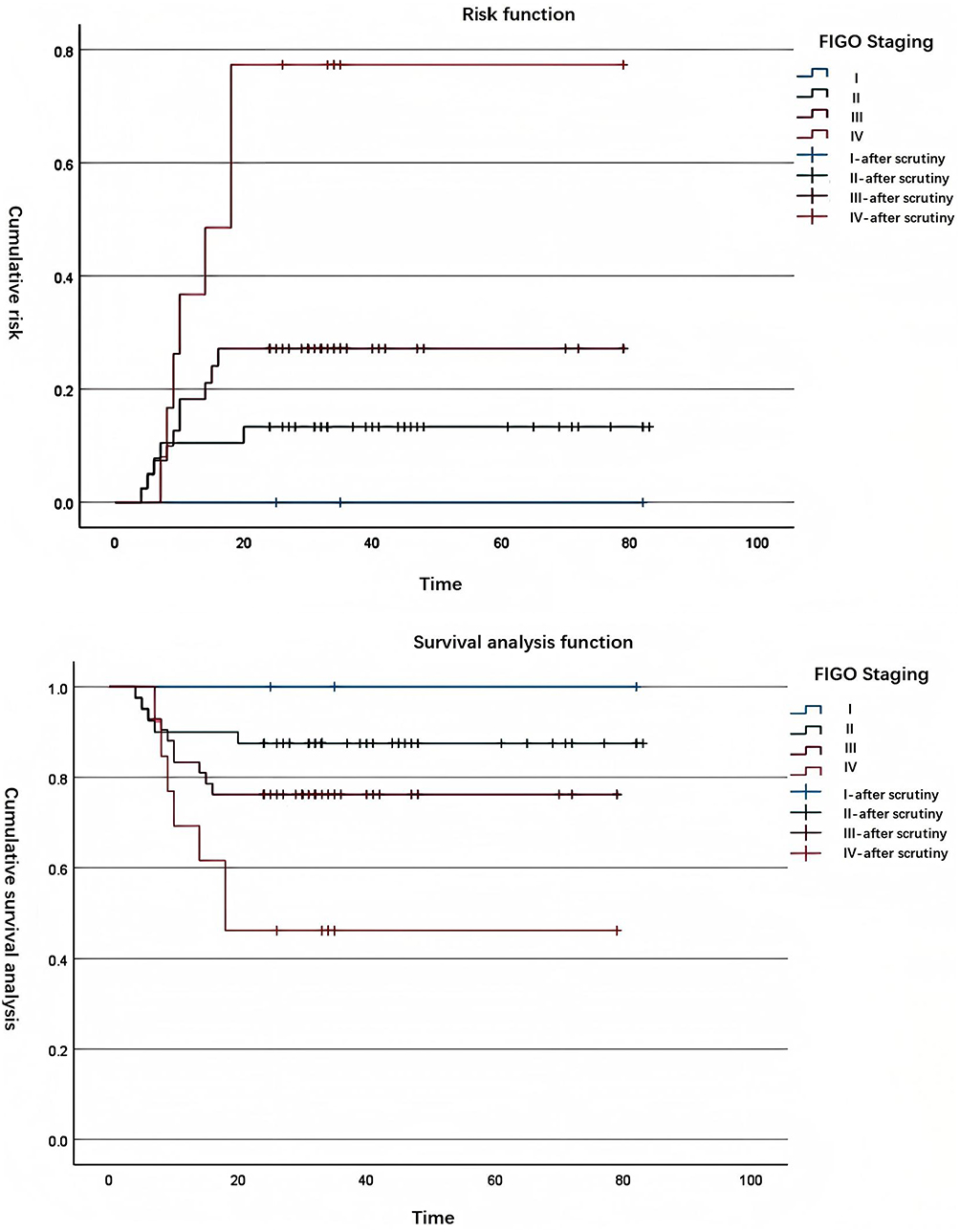 |
Figure 2 Kaplan-Meier analysis of stage-specific overall survival for all eligible cervical cancer patients. Later staging was associated with poorer 2-year overall survival (P<0.05). |
Discussion
In the past 20 years, the morbidity and mortality of gynaecological malignant tumours in China have continued to rise, and have become one of the major problems threatening women’s health. Especially cervical cancer, its standardised mortality rate not only rises year by year, but also the incidence of the disease shows a younger trend.7 This situation imposes a substantial escalation in fiscal pressures for households and the community at large. Therefore, effectively predicting prognosis and providing personalised interventions are important to improve patients’ prognosis and enhance their quality of life.2 In our study, we found that age, menstrual status, maximum tumour diameter, fertility history, SCC-Ag before radiotherapy, presence of HPV infection, pelvic lymph node metastasis, intestinal response after radiotherapy, urinary tract response, leukocyte grading, platelet grading, haemoglobin grading, LMR (lymphocyte to monocyte ratio), NLR (neutrophil to lymphocyte ratio), PLR (platelet to lymphocyte ratio), PLR (platelet-to-lymphocyte ratio) and the presence or absence of chemotherapy were not significantly different. The overall survival outcomes in cervical cancer patients have been found to be substantially affected by various clinicopathological variables.8
Drawing upon prior research, Zang et al developed a prognostic model involving 396 individuals diagnosed with SCC who received radical radiotherapy. Their findings demonstrated that pretreatment serum SCC-Ag levels served as a significant prognostic indicator, with patients exhibiting elevated SCC-Ag concentrations prior to treatment showing substantially poorer clinical outcomes compared to those with lower SCC-Ag levels.9 Several studies have shown that SCC patients with low serum concentrations of SCC Ag before treatment have better PFS (progression free survival) compared to patients with high concentrations of SCC Ag,10,11 Pre-treatment assessment of squamous cell carcinoma antigen concentrations has been established as a critical prognostic indicator, with higher baseline levels demonstrating a strong association with reduced survival rates in cervical cancer cases.12 SCC-Ag is a glycoprotein that is physiologically expressed in normal squamous epithelium. Although not tissue-specific, SCC-Ag has clinical utility beyond cervical cancer, serving as a biomarker for diagnosis and therapeutic response assessment in various malignancies, including lung cancer, esophageal cancer, and head and neck cancers.8 The current study failed to demonstrate a statistically meaningful association between pretreatment squamous cell carcinoma antigen (SCC-Ag) concentrations and patient survival outcomes, aligning with the definitive results obtained from independent investigations carried out by Chen et al and Cheng’s group. This absence of correlation between baseline SCC-Ag values and overall survival (OS) rates corroborates previous research findings in this field. While both research groups identified pre-treatment SCC Ag levels as a significant prognostic indicator for OS in their univariate analyses, this parameter failed to demonstrate independent prognostic value when subjected to multivariate analysis,10,11 Nevertheless, the threshold criteria employed across these investigations exhibited significant variability. A predominant threshold of 1.5 ng/mL emerged as a potential prognostic indicator, though its clinical validity requires more extensive verification. It should be noted that potential inaccuracies might exist in certain aspects of the data collection procedure. Furthermore, substantial discrepancies were observed in the follow-up periods across different studies, compounded by instances of participant attrition and false-positive cases. High concentrations of SCC Ag did not show a statistically significant prognosis with OS.
In a retrospective cohort analysis performed by Atahan’s research team, survival data were evaluated for patients with cervical malignancies treated exclusively with radiation therapy. The study findings indicated that younger individuals diagnosed with cervical carcinoma demonstrated significantly reduced survival rates compared to their older counterparts,13 and other studies have come to the same conclusion that younger age leads to poorer prognosis in cervical cancer.14,15 So age is a poor prognostic factor for cervical cancer.16 The patient cohort in our investigation exhibited a median age of 60 years. This demographic characteristic demonstrates a significant contrast with previous clinical trials reporting median ages ranging from 45 to 50 years, indicating that our study population was approximately a decade older. This age distribution pattern underscores the clinical reality that radiotherapy-treated cervical cancer patients in our national context predominantly belong to an advanced age group. Consequently, the potential influence of aging on both oncological outcomes and treatment-related adverse effects warrants particular consideration within this specific patient population.
Extensive research has identified several predictive indicators for cervical carcinoma outcomes, encompassing pretherapeutic neoplasm dimensions, staging according to the International Federation of Gynecology and Obstetrics (FIGO) system, and metastatic spread to pelvic lymph nodes. Clinical evidence demonstrates that increased neoplasm dimensions prior to therapeutic intervention, advanced FIGO classification stages, and the presence of metastatic spread to pelvic lymph nodes are all associated with decreased overall survival rates in affected patients.17,18 The results indicating that FIGO staging demonstrates limited prognostic value for overall survival (OS) in cervical cancer patients align with the conclusions drawn from prior research investigations.
Concerning the influence of chemotherapy on cervical cancer prognosis, a prior investigation involving 183 cervical cancer patients treated with radical radiotherapy revealed that concurrent chemotherapy significantly affected survival outcomes. Specifically, patients who did not receive concurrent radiotherapy exhibited poorer overall survival (OS) rates.13 Extensive research has consistently demonstrated comparable outcomes, indicating that cervical cancer patients undergoing concurrent radiation therapy exhibit superior overall survival rates and experience a mortality risk reduction ranging from 30% to 50% when compared to those receiving definitive radiotherapy alone.19,20 Zang et.al developed a predictive model to estimate overall survival (OS) in patients with SCC undergoing definitive radiotherapy. Their investigation revealed that chemotherapeutic intervention served as a significant prognostic indicator within this patient cohort. Indeed, chemotherapy is considered a radiosensitizer and is aimed at eradicating occult metastases.9 At present, the combination of platinum-based agents with concurrent radiochemotherapy has demonstrated superior efficacy in survival outcomes compared to radical radiotherapy as a standalone approach, establishing itself as a conventional therapeutic strategy for early-stage cervical carcinoma.21
The dimensions of neoplastic growth, status of lymphatic involvement, and FIGO staging parameters, despite being recognized as independent predictors of cervical cancer outcomes, are not consistently implemented in clinical practice owing to their inadequate diagnostic precision and patient-specific reliability. Lymphocytes serve as crucial components in the immunological defense mechanisms of the host organism. These immune cells exert suppressive effects on neoplastic cell growth and their metastatic potential through the initiation of cytotoxic cellular apoptosis and the secretion of immunoregulatory cytokines. Within the tumor microenvironment, lymphocyte populations that infiltrate malignant tissues participate in various phases of oncological development and progression. Clinical studies have demonstrated that tumor-infiltrating lymphocytes, particularly those expressing CD8 and CD4 surface markers, serve as negative prognostic biomarkers in various neoplastic diseases. Conversely, lower lymphocyte counts may result in inadequate immune response leading to poor survival in many cancers.
The neutrophil-to-lymphocyte ratio (NLR) serves as an indicator of the equilibrium between inflammatory responses and immunological regulation, while simultaneously representing the dynamic interplay between tumor-promoting and tumor-suppressing conditions. A comprehensive investigation was performed by Choi et.al regarding solid tumor characteristics following radiation treatment. Analysis of clinical data indicated that higher pre-treatment neutrophil-to-lymphocyte index values showed a substantial inverse relationship with long-term survival probabilities in individuals undergoing radiation therapy for cervical malignancies.22 Research evidence from multiple clinical investigations has established the prognostic significance of NLR in cervical cancer patients treated with synchronous radiotherapy. The scientific literature indicates that pretreatment NLR elevation independently correlates with adverse clinical outcomes, manifesting as reduced rates of both progression-free and overall survival,23,24 The study demonstrates that pretreatment elevation in the neutrophil-lymphocyte ratio (NLR) represents a crucial prognostic marker for poor clinical prognosis in cervical cancer patients, exhibiting substantial associations with diminished overall survival rates and decreased progression-free survival durations. This hematological parameter reflects a biological predisposition toward enhanced tumor-promoting inflammatory responses coupled with diminished anti-neoplastic immune activity. Elevated pre-treatment neutrophil-to-lymphocyte ratio (NLR) levels have been identified as a consistent prognostic indicator for poor clinical outcomes in cervical cancer patients, demonstrating significant correlation with reduced overall survival duration. This hematological parameter, measured before initiation of therapeutic protocols, shows substantial predictive capacity for unfavorable disease progression in this oncological population.25,26,27
The PLR metric serves as an indicator reflecting the equilibrium between pro-tumorigenic mechanisms and the host’s immunological defense against malignancies. Extensive research examining PLR parameters in cervical malignancy has revealed two significant findings: firstly, patients exhibiting elevated PLR levels before treatment initiation show markedly poorer OS rates compared to those with reduced PLR values; secondly, there exists a direct relationship between heightened PLR measurements and augmented cervical cancer risk.2829,30 However, there are also studies with the same results as ours, where PLR showed no significant difference in OS for cervical cancer.23 Several studies indicated that cervical cancer patients exhibiting reduced PLR levels prior to treatment demonstrated marginally improved overall survival rates compared to those with elevated pretreatment PLR values. However, this observed difference did not reach statistical significance. Empirical evidence indicated that the integrated assessment of NLR and PLR biomarkers provided more accurate prognostic predictions than the isolated evaluation of either parameter in cervical cancer patients. The combined analytical approach demonstrated a marked improvement in predictive capacity, highlighting the clinical significance of utilizing these inflammatory markers in conjunction for enhanced prognostic stratification.31 In investigations focusing on platelet-to-lymphocyte ratio (PLR) among cervical cancer patients, the optimal threshold values for high and low subgroups are typically determined through ROC curve analysis. However, our study adopted median-based subgroup classification, which could potentially introduce distinct variations in outcome interpretation. The investigation additionally demonstrated that the combined prognostic potential of neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) exhibited superior predictive performance compared to their individual prognostic capacities when assessed separately in cervical carcinoma patients. This synergistic effect between the two hematological parameters was found to be statistically significant in clinical evaluations.32 However, there was also a systematic evaluation with the same results as our study, which did not show a significant difference in the prognostic aspect of LMR in cervical cancer.29 Concerning the prognostic value of LMR in cervical carcinoma, while numerous investigations have demonstrated its potential as a prognostic indicator, substantial contradictory evidence exists in the scientific literature. The conclusive role of LMR as a dependable prognostic indicator for cervical carcinoma continues to be uncertain and remains a topic of persistent scientific discourse.
Research has demonstrated a significant correlation between history of miscarriage and both cervical precancerous conditions and the progression to cervical carcinoma. Notably, individuals with a history of recurrent pregnancy loss exhibit a substantially elevated probability of developing malignant cervical neoplasms,33,34,37 Initial investigations into the predictive factors for miscarriage and cervical cancer outcomes were initiated in 1999, focusing on the prognostic value of pre-treatment and during-treatment variables in individuals with advanced cervical carcinoma undergoing exclusive radical radiotherapy. These studies demonstrated that the frequency of history of miscarriage in patients exerted a substantial and autonomous influence on survival rates. Furthermore, a prior occurrence of miscarriage was identified as an autonomous prognostic marker for patient outcomes.38 The research conducted by Charach et.al demonstrated a significant correlation between repeated pregnancy loss and unfavorable clinical outcomes in patients diagnosed with cervical carcinoma. Their investigation indicated that women experiencing recurrent miscarriage exhibited poorer prognostic indicators when concurrently presenting with cervical malignancy.39 A research investigation conducted on cervical cancer patients receiving ambulatory care demonstrated consistent findings. The analysis revealed that individuals with a prior history of miscarriage exhibited a 67% elevated mortality risk when compared to their counterparts without such history of miscarriage. This comparative study specifically examined the survival outcomes among outpatient populations diagnosed with cervical malignancies.40 A retrospective cohort study performed by Li et al revealed that decreased parity and higher frequency of miscarriage correlated with worse survival rates among cervical cancer patients. These relationships remained statistically significant even after adjustment in the Cox proportional hazards model. Extensive research has repeatedly confirmed the existence of these well-documented prognostic parameters. Specifically, study participants with a history of three or more abortions had a 65% increased risk of recurrence compared to cervical cancer patients with no history of abortion.16 These results indicate that miscarriage history constitutes a distinct prognostic variable in cervical cancer progression.41,42 Consistent with our observations regarding miscarriage history, the recognition of prior miscarriage as a negative prognostic indicator for cervical carcinoma was correlated with diminished overall survival rates in affected cohort, which corroborates our initial observations. Multiple induced miscarriage can induce traumatic effects on the uterine cervix, resulting in squamous epithelial metaplasia within the cervical transformation zone. This pathological alteration creates favorable conditions for human papillomavirus (HPV) invasion. Concurrently, recurrent abortion procedures may compromise the patient’s immunological competence.41 HPV exhibits a remarkable capacity to escape immune surveillance. Following infection of host cells, the viral genome incorporates itself into the human DNA, facilitating the persistent production of HPV-encoded E6 and E7 oncoproteins. These proteins are known to disrupt the function of key tumor suppressors, namely p53 and pRb, thereby inhibiting programmed cell death and promoting uncontrolled cellular growth. Additionally, HPV integration can trigger multiple genomic abnormalities near the insertion site, including the amplification of oncogenes, structural chromosomal changes, and genomic instability. Over time, the accumulation of such DNA modifications contributes to the development of cervical cancer.43 While multiple investigations have identified patient age, lymph node involvement, and tumor dimensions as significant prognostic variables in cervical cancer cases, our research yielded different findings. Specifically, our analysis revealed no correlation between treatment outcomes and parameters such as lymph node status or tumor dimensions. This discrepancy might be explained by the limited cohort size in our investigation.
This investigation demonstrates multiple methodological advantages. Primarily, the research incorporates a comprehensive array of determinant variables in examining prognostic indicators for SCC patients undergoing radical radiotherapy, establishing a robust analytical framework. Furthermore, the study extensively builds upon existing literature through thorough citation practices while incorporating an expanded spectrum of clinical staging parameters.
Several methodological limitations should be acknowledged in this research. Primarily, the analytical framework lacked both sensitivity assessment and examination of potential publication bias. Secondly because it was a retrospective design, bias could not be completely eliminated even after controlling for covariates in the model. The exclusion of a higher number of patients included in the previous period due to inadequate or invalid medical records reduces the statistical validity of the study and limits the generalization of our results to a wider population. The small sample size and relatively small number of individual cases were relatively limited for the study factors, preventing a more in-depth study of the factors involved and a relatively large error. Third, all included studies were published in English, ignoring papers published in other languages, especially Chinese and German, which resulted in selection bias. Fourthly, the cut-off values of hematologic immunological indices of the included investigations, with alternative research employing receiver operating characteristic curve-derived cut-off points. The utilization of median values for NLR, PLR, and LMR thresholds could potentially influence diagnostic accuracy parameters, particularly in terms of sensitivity and specificity. In contrast, ROC curve-based threshold determination might yield enhanced diagnostic performance, potentially impacting the overall findings of this investigation. Fifth, the research did not incorporate datasets from emerging economies across different global regions. Future prospective studies are needed, and blood immunological markers need to be further explored as more accurate biomarkers of tumor subgroups so as to select appropriate treatment populations to maximize patient benefit, as well as to more effectively confirm the association between factors and OS.
Conclusion
To summarize the findings of our investigation, the analysis reveals that both FIGO classification and history of miscarriage could potentially function as predictive indicators for SCC outcomes, as demonstrated through both univariate and multivariate COX regression analyses.
Data Sharing Statement
Research data are not shared.
Ethics Approval and Consent to Participate
All procedures were carried out following the ethical standards declared by the World Medical Association. We confirmed that all methods were carried out in accordance with the Declaration of Helsinki and were approved by the Affiliated Hospital of Jiangnan University Ethical Review Committee. Given the retrospective nature of the study, the requirement for informed consent was waived, and patient data were kept confidential. This study was approved by the Affiliated Hospital of Jiangnan University Ethical Review Committee (Approval Number: LS2024539).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding for this research.
Disclosure
The authors declare no competing interests in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Singh D, Vignat J, Lorenzoni V, et al. Global estimates of incidence and mortality of cervical cancer in 2020: a baseline analysis of the WHO global cervical cancer elimination initiative. Lancet Glob Health 2023. 2023;11(2):e197–e206. doi:10.1016/S2214-109X(22)00501-0
3. Bhatla N, Aoki D, Sharma DN, et al. Cancer of the cervix uteri. Int J Gynecol Obstet. 2018;143(suppl 2):22–36. doi:10.1002/ijgo.12611
4. Xiu YT, Meng FX, Wang Z, et al. Prognostic factors for IB2-IIIB cervical cancer patients treated by radiation therapy with high-dose-rate brachytherapy in a single-institution study. J Contemp Brachyther 2022. 2022;14(4):332–340. doi:10.5114/jcb.2022.118933
5. Hong JH, Tsai CS, Lai CH, et al. Risk stratification of patients with advanced squamous cell carcinoma of cervix treated by radiotherapy alone. Int J Radiat Oncol Biol Phys. 2005;63(2):492–499. doi:10.1016/j.ijrobp.2005.02.050
6. Hong JH, Tsai CS, Chang JT, et al. The prognostic significance of pre- and posttreatment SCC levels in patients with squamous cell carcinoma of the cervix treated by radiotherapy. Int J Radiat Oncol Biol Phys. 1998;41(4):823–830. doi:10.1016/S0360-3016(98)00125-7
7. Jiang X, Tang H, Chen T. Epidemiology of gynecologic cancers in China. J Gynecol Oncol. 2018;29(1):e7. doi:10.3802/jgo.2018.29.e7
8. Liu Z, Shi H, Li J, Hou Q, Tang B. Prognostic role of squamous cell carcinoma antigen in cervical cancer: a meta-analysis. Med Sci Monit. 2022;28:e934588. doi:10.12659/MSM.934588
9. Zang L, Chen Q, Lin A, et al. A prognostic model using FIGO 2018 staging and MRI-derived tumor volume to predict long-term outcomes in patients with uterine cervical squamous cell carcinoma who received definitive radiotherapy. World. J Surg Oncol. 2023;21:210. doi:10.1186/s12957-023-03093-8
10. Chen W, Xiu S, Xie X, et al. Prognostic value of tumor measurement parameters and SCC-Ag changes in patients with locally-advanced cervical cancer. Radiat Oncol. 2022;17:6. doi:10.1186/s13014-021-01972-6
11. Cheng YK, Kuo S-H, Yen HH, et al. The prognostic significance of pretreatment squamous cell carcinoma antigen levels in cervical cancer patients treated by concurrent chemoradiation therapy and a comparison of dosimetric outcomes and clinical toxicities between tomotherapy and volumetric modulated arc therapy. Radiat Oncol. 2022;17:91. doi:10.1186/s13014-022-02063-w
12. Charakorn C, Thadanipon K, Chaijindaratana S, et al. The association between serum squamous cell carcinoma antigen and recurrence and survival of patients with cervical squamous cell carcinoma: a systematic review and meta-analysis. Gynecologic Oncol. 2018;150(1):190–200. doi:10.1016/j.ygyno.2018.03.056
13. Atahan IL, Onal C, Ozyar E, et al. Long-term outcome and prognostic factors in patients with cervical carcinoma: a retrospective study. Int J Gynecological Cancer. 2007;17(5):833–842. doi:10.1136/ijgc-00009577-200707000-00013
14. Wang J, Wang T, Yang -Y-Y, et al. Patient age, tumor appearance and tumor size are risk factors for early recurrence of cervical cancer. Mol Clin Oncol. 2015;3(2):363–366. doi:10.3892/mco.2014.465
15. Ferioli M, Benini A, Malizia C, et al. Classical prognostic factors predict prognosis better than inflammatory indices in locally advanced cervical cancer: results of a comprehensive observational study including tumor-, patient-, and treatment-related data (ESTHER Study). J. Pers. Med. 2023;13(9):1229. doi:10.3390/jpm13081229
16. Li J, Liu G, Luo J, et al. Cervical cancer prognosis and related risk factors for patients with cervical cancer: a long-term retrospective cohort study. Sci Rep. 2022;12:13994. doi:10.1038/s41598-022-17733-8
17. G RP, Java J, W WC, et al. Nomograms predicting progression-free survival, overall survival, and pelvic recurrence in locally advanced cervical cancer developed from an analysis of identifiable prognostic factors in patients from NRG oncology/gynecologic oncology group randomized trials of chemoradiotherapy. J Clin Oncol. 2015;33(19):2136–2142. doi:10.1200/JCO.2014.57.7122
18. Wang X, Xu J, Zhang H, et al. The effect of albumin and hemoglobin levels on the prognosis of early-stage cervical cancer: a prospective, single-center-based cohort study. BMC Women’s Health. 2023;23:553. doi:10.1186/s12905-023-02713-5
19. Luvero D, Plotti F, Aloisi A, et al. Patients treated with neoadjuvant chemotherapy + radical surgery + adjuvant chemotherapy in locally advanced cervical cancer: long-term outcomes, survival and prognostic factors in a single-center 10-year follow-Up. Med Oncol. 2016;33(1):110. doi:10.1007/s12032-016-0830-0
20. Wang W, Hou X, Yan J, et al. Outcome and toxicity of radical radiotherapy or concurrent Chemoradiotherapy for elderly cervical cancer women. BMC Cancer. 2017;17:510. doi:10.1186/s12885-017-3503-2
21. Yu J, Huang L, Dong T, et al. Prediction of outcomes after chemoradiotherapy for cervical cancer by neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio. J Obstetrics Gynaecol. 2024;44(1):236185. doi:10.1080/01443615.2024.2361858
22. Choi N, Kim JH, Chie EK, et al. A meta-analysis of the impact of neutrophil-to-lymphocyte ratio on treatment outcomes after radiotherapy for solid tumors. Medicine. 2019;98(18):e15599. doi:10.1097/MD.0000000000015599
23. Onal C, Guler OC, Yildirim BA. Prognostic use of pretreatment hematologic parameters in patients receiving definitive chemoradiotherapy for cervical cancer. Int J Gynecological Cancer. 2016;00(00):1–7.
24. Jin L, Cao F, Zhang Y, et al. Nomograms for predicting prognostic value of combined neutrophil-to-lymphocyte ratio and SCC-Ag in locally advanced cervical cancer. Transl Cancer Res. 2024;13(3):1323–1335. doi:10.21037/tcr-23-1501
25. Wu J, Chen M, Liang C, et al. Prognostic value of the pretreatment neutrophil-to-lymphocyte ratio in cervical cancer: a meta-analysis and systematic review. Oncotarget. 2017;8(8):13400–13412. doi:10.18632/oncotarget.14541
26. Huang QT, Man QQ, Hu J, et al. Prognostic significance of neutrophil-to-lymphocyte ratio in cervical cancer: a systematic review and meta-analysis of observational studies. Oncotarget. 2017;8(10):16755–16764. doi:10.18632/oncotarget.15157
27. Zou PJ, Yang E, Li ZY. Neutrophil-to-lymphocyte ratio is an independent predictor for survival outcomes in cervical cancer: a systematic review and meta-analysis. Sci Rep. 2020;10:21917. doi:10.1038/s41598-020-79071-x
28. Ma JY, Ke LC, Liu Q. The pretreatment platelet-to-lymphocyte ratio predicts clinical outcomes in patients with cervical cancer. Medicine. 2018;97(43):e12665. doi:10.1097/MD.0000000000012897
29. Han XP, Liu SY, Yang G, et al. Prognostic value of systemic hemato-immunological indices in uterine cervical cancer: a systemic review, meta-analysis, and meta-regression of observational studies. Gynecologic Oncol. 2021;160(1):351–360. doi:10.1016/j.ygyno.2020.10.011
30. Gao ZR, Zhao ML, Yang XJ, et al. Assessment of peripheral platelet to lymphocyte ratio and prognostic nutritional index in the efficacy and prognosis of radiotherapy for cervical cancer. Current Oncol. 2023;30:2834–2844. doi:10.3390/curroncol30030216
31. Lee JW, Seol KH. Pretreatment neutrophil-to-lymphocyte ratio combined with platelet-to-lymphocyte ratio as a predictor of survival outcomes after definitive concurrent chemoradiotherapy for cervical cancer. J Clin Med. 2021;10(7):2199. doi:10.3390/jcm10102199
32. Mao Y, Chen D, Duan SZ, et al. Prognostic impact of pretreatment lymphocyte-to-monocyte ratio in advanced epithelial cancers: a meta-analysis. Can Cell Inter. 2018;18:201. doi:10.1186/s12935-018-0698-5
33. Duan W, Li H, Hu H. Study on the relationship between the number of artificial abortion and the high risk human papillomavirus infection and cervical cancer. Practical J Cancer. 2018;33(8):1364–1367.
34. Salari S, Raesi R, Daneshi S, et al. Prevalence of cervical cancer and premalignant cases based on pap smear screening in Iran in 2022. Curr Cancer Ther Rev. 2024;20:1–11.
35. Mikkelsen AP, Egerup PE, Ebert JFM, et al. Pregnancy loss and cancer risk: a nationwide observational study. EClinicalMedicine. 2019;10:80–88.
36. Weldegebreal F, Worku T. Precancerous cervical lesion among HIV-positive women in sub-saharan africa: a systematic review and meta-analysis. Cancer Control. 2019;26(1):1–11.
37. Sharmaa P, Pattanshetty SM. A study on risk factors of cervical cancer among patients attending a tertiary care hospital: a case-control study. Clin Epidemiol Global Health. 2018;6(2):83–87.
38. Karolewski K, Korzeniowski S, Sokołowski A, et al. Prognostic significance of pretherapeutic and therapeutic factors in patients with advanced cancer of the uterine cervix treated with radical radiotherapy alone. Acta Oncologica. 1999;38(4):461–468.
39. Charach R, Sheiner E, Beharier O, et al. Recurrent pregnancy loss and future risk of female malignancies. Arch Gynecol Obstetrics. 2018;298(4):781–787.
40. Aguade AE, Gashu C, Jegnaw T. The trend of change in cervical tumor size and time to death of hospitalized patients in Northwestern Ethiopia during 2018–2022: retrospective Study Design. Health Sci Rep. 2023;6:e1121.
41. Li J, Luo JY, Liu GM, et al. Influencing factors and risk prediction model for cervical cancer recurrence. Zhong nan da xue xue bao yi xue ban. J Central South Univ Med Sci. 2022;47(12):1711–1720.
42. Gari SF, Biru TF, Gurmu SE. Application of the joint frailty copula model for analyzing time to relapse and time to death of women with cervical cancer. Int J Women’s Health. 2023;15:1295–1304.
43. Kusakabe M, Taguchi A, Sone K, Mori M, Osuga Y. Carcinogenesis and management of human papillomavirus-associated cervical cancer. Int. J. Clin. Oncol. 2023;28(8):965–974.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Hyperfibrinogenemia as a Poor Prognostic Indicator in Myelodysplastic Syndrome
Shi C, Gong S, Wu A, Niu T, Wu N, Zhang Y, Ouyang G, Mu Q
Cancer Management and Research 2022, 14:1857-1865
Published Date: 4 June 2022
Prognostic Value of a Serum Panel of Inflammatory Factors in Non-Metastatic Nasopharyngeal Carcinoma Patients Undergoing Radical Radiotherapy with Adjuvant Chemotherapy
Liang T, Xiao D, Lu S, Ye X, Xiao Z
Cancer Management and Research 2022, 14:2763-2772
Published Date: 16 September 2022
Prognostic Value of Body Composition and Systemic Inflammatory Markers in Patients with Locally Advanced Cervical Cancer Following Chemoradiotherapy
Guo H, Feng S, Li Z, Yin Y, Lin X, Yuan L, Sheng X, Li D
Journal of Inflammation Research 2023, 16:5145-5156
Published Date: 10 November 2023
Development and Internal-External Validation Models for Cervical Cancer Overall Survival Prognosis: A SEER-Based Study and Chinese Data
Shi Y, Xu JN, Wang QQ, Wang SY, Wang LY
International Journal of Women's Health 2025, 17:2051-2062
Published Date: 12 July 2025
Long-Term Survival Outcomes of HPV DNA–Negative Cervical Cancer Compared with HPV DNA–Positive Disease in a Thai Tertiary Cohort
Phisalmonhkhon T, Kantathavorn N, Wetcho T, Samrarn J, Kittikhun R, Sukjariangporn H, Thongaram M
International Journal of Women's Health 2026, 18:601452
Published Date: 24 April 2026