Back to Journals » Clinical Ophthalmology » Volume 17
Intraocular Lens Unfurling Time Exponentially Decays with Increased Solution Temperature
Authors Rocher EE ![]() , Mukherjee R, Pitingolo J, Levenshus E, Alexander G, Park M, Acharya R, Khan S, Shuff J, Aguirre A, Matin S, Walter K, Eghrari AO
, Mukherjee R, Pitingolo J, Levenshus E, Alexander G, Park M, Acharya R, Khan S, Shuff J, Aguirre A, Matin S, Walter K, Eghrari AO ![]()
Received 15 April 2023
Accepted for publication 17 July 2023
Published 21 August 2023 Volume 2023:17 Pages 2471—2481
DOI https://doi.org/10.2147/OPTH.S417357
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supplementary video of "Increased solution temperature decreases IOL unfurling time" [ID 417357].
Views: 111
Erick E Rocher,1 Rishima Mukherjee,1 James Pitingolo,1 Eli Levenshus,1 Gwyneth Alexander,1 Minyoung Park,1 Rupsa Acharya,1 Sarah Khan,1 Jordan Shuff,1 Andres Aguirre,1 Shababa Matin,2 Keith Walter,3 Allen O Eghrari4
1Center for Bioengineering Innovation and Design, Department of Biomedical Engineering, Johns Hopkins University, Baltimore, MD, USA; 2Rice 360 Institute for Global Health Technologies, Rice University, Houston, TX, USA; 3Department of Ophthalmology, Wake Forest Baptist Health, Winston-Salem, NC, USA; 4Department of Ophthalmology, Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, MD, USA
Correspondence: Allen O Eghrari, Department of Ophthalmology, Wilmer Eye Institute, Johns Hopkins University School of Medicine, 400 N Broadway, Smith 5013, Baltimore, MD, 21231, USA, Email [email protected]
Purpose: Intraocular lens (IOL) unfurling can be a rate-limiting step in cataract surgery, limiting operative efficiency. Furthermore, inefficient unfurling has important implications for clinical outcomes. We examine the effects of solution temperature on IOL unfurling time using three in vitro models of the ocular environment.
Methods: IOLs were injected into a 6-well plate filled with balanced salt solution (BSS), dispersive ophthalmic viscoelastic device (OVD), or cohesive OVD. Experiments were also performed in a plastic eye filled with dispersive or cohesive OVD. IOL unfurling time was recorded against the temperature of the respective solution.
Results: IOL unfurling time decayed exponentially as solution temperature increased in all experiments, including the BSS-filled 6-well plate, the OVD-filled 6-well plate, and the OVD-filled plastic eye. IOLs failed to unfurl within 10 min at 10°C, below the glass transition temperature of the tested IOLs. Increasing solution temperature from 20°C to 30°C decreases IOL unfurling by greater than 2 min. Further heating to 40°C did not significantly decrease IOL unfurling time.
Conclusion: Increased solution temperature rapidly decreases IOL unfurling time in vitro. IOLs do not unfurl within a clinically acceptable timeframe at or below their glass transition temperature. Increased BSS and/or OVD temperature may be a potential method to decrease IOL unfurling time in cataract surgery. However, future research is needed to elucidate potential consequences of warmed BSS and/or OVD on post-operative outcomes. This study demonstrates the potential for temperature regulation to decrease cataract surgery operative time and provides preliminary evidence to justify future clinical validation of this relationship.
Plain Language Summary: During cataract surgery, a prosthetic intraocular lens (IOL) is inserted into the eye once the clouded lens is removed. The IOL must then unfurl before the procedure can proceed. When IOLs fail to unfurl or unfurl slowly, this can delay the operation and may even cause post-operative complications. Thus, we studied the effect temperature may have on IOL unfurling time to optimize this segment of the operation.
We injected IOLs into solutions of saline (balanced salt solution) or ophthalmic viscoelastic device (OVD), two fluids injected into the eye during surgery. In both a well plate and a plastic eye, we found that increasing the temperature of the solution significantly affected IOL unfurling time. Specifically, heating the solution from refrigeration to room temperature decreased unfurling time from over 10 min to less than four. Heating to physiological temperature further decreased unfurling time to less than a minute.
Our results show promise for potentially utilizing heated BSS and/or OVD to accelerate IOL unfurling and decrease cataract surgery operative time.
Keywords: cataract surgery, balanced salt solution, ophthalmic viscoelastic device
Introduction
Globally, cataracts are the prevailing cause of blindness in adults over 50 years of age.1 Cataract surgery, where a patient’s native, clouded lens is replaced with a prosthetic one, remains the only effective treatment for this disease. Cataract surgery is a highly optimized procedure, with few uncontrolled parameters. Surgeons have precise control over flow rate of irrigation fluid and intraocular pressure via phacoemulsification devices. However, surgeons currently lack temperature control of the ocular surgical environment. As a consequence, ocular temperature transiently drops during several segments of the operation.2
During cataract surgery, balanced salt solution (BSS) is used to irrigate the eye. BSS is used throughout the surgery, with periods of irrigation occurring in several segments of the procedure. Ophthalmic viscoelastic device (OVD) is a fluid used in cataract surgery to maintain structural support of the capsular bag containing the lens and to minimize damage to the endothelial cells lining the back of the cornea during phacoemulsification. OVD is typically injected into the eye at the beginning of the surgery and throughout the procedure as needed.
Following phacoemulsification, a folded intraocular lens (IOL) is injected into the eye. Once injected, the IOL must unfurl in order to be properly positioned, leaving surgeons waiting for the IOL to be planar before proceeding. IOL unfurling can take minutes, representing a substantial portion of the total surgical time. Further, extended unfurling time prevents effective IOL fixation, leading to rotation of the IOL and even dislocation into the vitreous cavity.3 Predictable unfurling is vital during the implantation of toric IOLs, when precise alignment of the optic is needed to restore optimal vision.4,5 Thus, parameters surrounding IOL unfurling represent an important clinical interest to minimize surgical time and operative costs while improving clinical outcomes.
Given the acrylic composition of hydrophobic IOLs, it is known that temperature significantly affects their material properties. In fact, a surgical technique6 was described as far as 1996 recommending direct heating of IOLs prior to injection. However, a rigorous study has not been conducted to investigate whether this method will accelerate IOL unfurling in modern IOLs, which is conducted here.
Previous work elucidated methods to accelerate IOL unfurling using warmed BSS and/or OVD, as they are the primary fluids present within the anterior chamber during IOL injection. Minami et al7 decreased IOL unfurling time by loading the injection cartridge with warmed OVD. Eom et al8 demonstrated the ability to accelerate unfurling time of prehydrated hydrophobic acrylic MX60 IOLs via injection of warmed OVD prior to IOL insertion. Less significant effects were seen with hydrophobic acrylic SN60AT and ZNB00 IOLs, which was attributed to their lower glass transition temperatures. However, these studies did not assess IOL unfurling in multiple types of OVD, with high trial counts, across a large temperature range, nor in multiple in vitro conditions. The present study will assess IOL unfurling across a broad range of solution temperatures, with decreased IOL re-usage, in both solutions of BSS, cohesive, and dispersive OVD, and in both unconstrained (well plate) and constrained (plastic eye) environments. Further, we will demonstrate how hydrophobic acrylic IOLs unfurl below their glass transition temperature, which has been shown to be in the range of 12.5°C to 15.5°C for the tested IOLs.9–11 Finally, this study will investigate whether temperatures above 35°C may further minimize unfurling time. By exploring these additional factors, we aim to precisely quantify solution temperature on IOL unfurling kinetics, thereby providing a framework to accurately inform the minimal ocular temperature needed to minimize IOL unfurling in practice. This information may prove useful for informing future work to maintain ocular temperature during surgery, a point of discussion by Minami et al.2
Materials and Methods
This study is a benchtop study on the kinetics of IOL unfurling. Three in vitro models of the ocular environment were chosen with varied submersion fluid and spatial constraints. First, IOLs were injected into a 6-well plate filled with BSS (BSS Sterile Irrigating Solution, Alcon, Geneva, Switzerland) at various temperatures. BSS was used to assess the intrinsic temperature dependence of IOL unfurling kinetics independent of thermal changes to solution viscosity, as commonly observed with OVD. Second, IOLs were injected into a 6-well plate filled with OVD at various temperatures. This better simulates the fluid environment of cataract surgery, as the anterior chamber is typically filled with OVD upon IOL injection. These two experiments allowed IOLs to unfurl in a spatially unconstrained environment, permitting the most uncomplicated evaluation of solution temperature effects on IOL unfurling time. Third, IOLs were injected into a plastic eye filled with OVD at various temperatures to introduce the spatial constraints expected during surgery.
Two methods of temperature modulation were examined. First, the IOL was directly heated via submersion in a water bath of constant temperature prior to injection. In subsequent experiments, the temperature of the solution into which the IOL was injected was modulated. Thus, both the effects of IOL temperature upon injection and the solution temperature were investigated for their effects on IOL unfurling time.
Unless otherwise specified, IOLs were loaded into a size D IOL cartridge using dispersive OVD (Viscoat, Alcon, Geneva, Switzerland), which was then placed into a size D IOL injector (Monarch III, Alcon, Geneva, Switzerland). The cartridge was filled with 0.20 mL of room temperature (22.8°C) OVD for each trial (N=4). The first haptic of the IOL was folded on top of the optic, and then the second haptic was tucked into the cartridge on top of the optic. The metal rod of the injector was rotated until the IOL reached the tip of the cartridge, and the IOL was retained in the injector for 1 min prior to insertion. IOL unfurling was video recorded and shown to three independent blinded adjudicators, who determined start and stop time required for full IOL unfurling for each trial. The IOL was classified as fully unfurled when there was no curvature in the body of the IOL and the optic was planar (Figure S1). The true IOL unfurling time was taken as the average of the three reported times. See Supplementary Video for representative trials. If an IOL failed to unfurl in 10 min, the adjudicators capped the trial at this time (600s) and “IOL failed to unfurl” was noted. As the entire duration of a cataract surgery often lasts less than this time, unfurling times over 10 min are not clinically relevant. In such a scenario, clinicians would reasonably intervene with surgical manipulation under this circumstance. Each IOL was used twice. A paired-sample t-test was performed across all experiments, which demonstrated that IOLs could be reliably used twice, as there were no statistically significant differences in unfurling time between two consecutive uses of the same IOL. IOLs were kept within 3.5 diopters in each experiment (see Table S1 for descriptive statistics of IOL diopters used in each experiment). Of note, additional experimentation demonstrated that IOL diopter does not affect unfurling time in vitro (Figure S2).
IOL Unfurling Following Pre-Heating of Lens
In the initial study, toric IOLs (AcrySof SA6AT3, Alcon, Geneva, Switzerland) were submerged in a water bath at 10°C, 20°C, 30°C, or 40°C for 5 min prior to cartridge loading and injection into a 6-well plate filled with BSS at constant room temperature (22°C). IOLs were not retained in the injector for 1 min to minimize heat loss prior to injection. Mean time from exit of heat bath to injection was 59s (SD 10.6). In all subsequent experiments, IOL temperature was constant (22°C) prior to injection, while the temperature of the solution upon injection was modulated.
IOL Unfurling in Heated BSS
Toric, monofocal, and multifocal IOLs (AcrySof SA6AT3, AcrySof IQ SN60WF, AcrySof IQ ReSTOR +3.0 D SN6AD1, Alcon, Geneva, Switzerland) were injected into a 6-well plate filled with BSS at 10°C, 20°C, 30°C, or 40°C.
IOL Unfurling in Heated OVD
Toric and monofocal IOLs (AcrySof SA6AT3, AcrySof IQ SN60WF, Alcon, Geneva, Switzerland) were injected into a 6-well plate filled with either dispersive or cohesive OVD (Viscoat, ProVisc, Alcon, Geneva, Switzerland) at 10°C, 20°C, 30°C, or 40°C. At room temperature, injection cartridge was filled with the corresponding OVD of that experiment.
IOL Unfurling in OVD-Filled Plastic Eye
Toric IOLs (AcrySof SA6AT3, Alcon, Geneva, Switzerland) were injected into a Kitaro Easy Eye (Frontier Vision, Hyogo, Japan), a plastic eye model, for simulation of the spatial constraints of cataract surgery (Figure 1). The anterior chamber was filled with refrigerated, operating room temperature, or physiological temperature OVD immediately prior to IOL injection. This better simulates the environment of the eye in surgery, where OVD often occupies the majority of the volume of the capsular bag during IOL injection and unfurling. Both dispersive and cohesive OVDs (Viscoat, ProVisc, Alcon, Geneva, Switzerland) were used, and the injection cartridge was filled with the corresponding room temperature OVD (22°C) of that experiment.
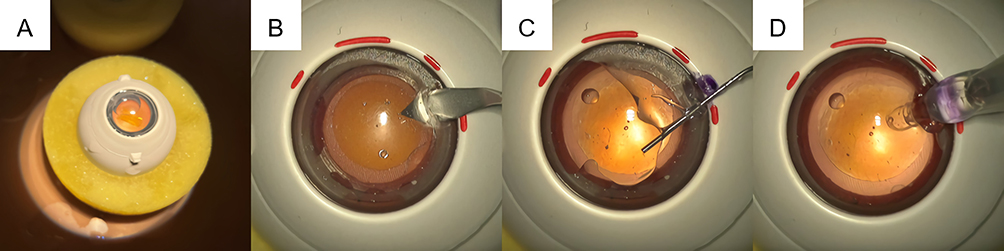 |
Figure 1 Plastic eye model set-up. (A) The plastic eye was placed under a surgical microscope for filming. (B) An incision was made at the base of the cornea. (C) The anterior chamber was filled with either dispersive or cohesive OVD at the desired temperature. (D) The IOL was injected and unfurling was recorded for review by three independent blinded adjudicators. Abbreviations: OVD, ophthalmic viscoelastic device; IOL, intraocular lens. |
Statistical Analysis
Unless otherwise noted, differences in IOL unfurling times between temperatures in an experiment were calculated using one-way ANOVAs with Tukey posttests to calculate pair-wise significance (assessed at the 0.05 level). Conditions where IOLs failed to unfurl were not included in these calculations. When shown, IOL unfurling time was plotted against solution temperature. For the resulting distributions, various linear, power, and exponential models were compared to determine an optimal fit (OriginPro 2022b, OriginLab, Northampton, MA). An exponential model was optimized for each distribution. Significance was assessed by comparing the fitted function against a function of constant IOL unfurling time at the 0.05 level.
Results
When IOLs were pre-heated in a water bath, loaded, and injected into BSS at room temperature, there were no significant differences in unfurling time at any of the tested temperatures (10°C, 20°C, 30°C, or 40°C), which spans the reasonable temperature range expected for supplies in an operating room (Figure S3).
When IOLs were injected into BSS at various temperatures, a strong negative and exponential relationship was observed between IOL unfurling time and temperature. At 10°C, IOLs failed to unfurl within 10 min in all trials across all tested IOL types (N=4). Heating from 20°C to 30°C significantly decreased mean unfurling times for toric (172s to 16s), monofocal (187s to 9s) and multifocal (155s to 11s) IOLs (P < 0.01). However, further heating to 40°C did not significantly decrease unfurling times, with a mean unfurling time of 7s, 5s, and 5s for toric, monofocal, and multifocal IOLs, respectively (Figure 2A–C). This distribution was best described by an exponential function (Figure 2D). These functions predict IOL unfurling times ranging from 156s to 187s at 20°C, 9s to 17s at 30°C, and 0.5s to 1.6s at 40°C. These functions were extrapolated to predict the true unfurling time at 10°C, falling between 30 min and 1 h. See Table S2 for detailed function descriptions. The results of this experiment are visually represented in Figure 3. One-way ANOVA with Tukey posttest demonstrated no difference in unfurling time between the three optic types at each temperature.
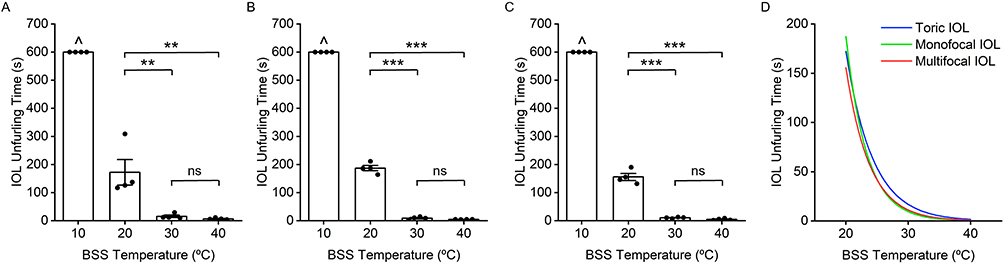 |
Figure 2 IOL unfurling time decreases exponentially with increased solution temperature independent of optic type. (A) Toric, (B) monofocal, and (C) multifocal IOLs were injected into a 6-well plate filled with a solution of BSS at various temperatures. (D) Exponential regressions (N = 12, P < 0.001) for toric (R2 = 0.731), monofocal (R2 = 0.986), and multifocal (R2 = 0.967) IOLs using points at 20°C, 30°C, and 40°C. ^IOLs failed to unfurl within ten-minute time cap at 10°C. **P < 0.01. ***P < 0.001. Abbreviations: ns, not significant; IOL, intraocular lens; BSS, balanced salt solution. |
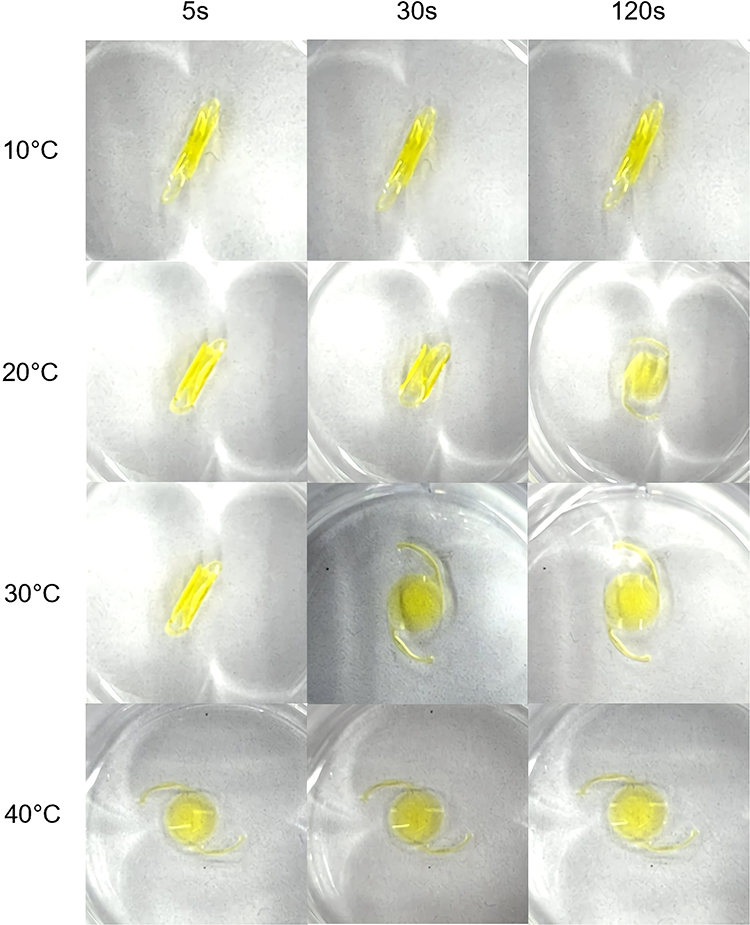 |
Figure 3 Representative IOL unfurling in BSS solution. In all trials, IOLs failed to unfurl at 10°C within 10 minutes. Average IOL unfurling time in BSS across toric, monofocal, and multifocal lenses was under 200s at 20°C, 20s at 30°C, and 7s at 40°C. Displayed: multifocal IOLs. Abbreviations: IOL, intraocular lens; BSS, balanced salt solution. |
A similar distribution resulted when IOLs were injected into a 6-well plate filled with OVD (Figure 4A–D). Again, IOLs failed to unfurl within 10 min at 10°C in all trials (N=4) under all conditions. Heating from 20°C to 30°C significantly decreased mean unfurling times for toric IOLs in dispersive (290s to 22s) and cohesive OVD (152s to 28s) and monofocal IOLs in dispersive (196s to 18s) and cohesive OVD (191s to 29s) (P < 0.01). Further heating to 40°C did not significantly decrease unfurling times for toric IOLs in dispersive (35s) and cohesive OVD (12s) nor monofocal IOLs in dispersive (22s) and cohesive OVD (12s). Fitted exponential functions predict IOL unfurling times ranging from 152s to 290s at 20°C, 23s to 31s at 30°C, and 2.6s to 6s at 40°C (Figure 4E). See Table S2 for detailed function descriptions.
 |
Figure 4 IOL unfurling time decreases exponentially with increased OVD temperature. IOLs were injected into a 6-well plate filled with OVD at various temperatures, including toric IOLs in (A) dispersive and (B) cohesive OVD, and monofocal IOLs in (C) dispersive and (D) cohesive OVD. (E) Exponential regressions (N = 12, P < 0.0001) for toric IOLs in dispersive OVD (R2 = 0.738), toric IOLs in cohesive OVD (R2 = 0.961), monofocal IOLs in dispersive OVD (R2 = 0.866), and monofocal IOLs in cohesive OVD (R2 = 0.962) using points at 20°C, 30°C, and 40°C. ^IOLs failed to unfurl within ten-minute time cap at 10°C. **P < 0.01. ***P < 0.001. Abbreviations: ns, not significant; IOL, intraocular lens; OVD, ophthalmic viscoelastic device. |
Finally, a plastic eye was filled with OVD at refrigeration temperature, operating at room temperature, or physiological temperature prior to the insertion of an IOL. IOLs injected into a plastic eye filled with refrigerated OVD failed to unfurl within 10 min in two of four trials in dispersive OVD and in all trials (N=4) in cohesive OVD. A two-sample t-test revealed significant decreases in IOL unfurling time when OVD at physiological temperature is used rather than OVD at operating room temperature (Figure 5A and B) (P < 0.01). This held true for both dispersive (133s to 42s) and cohesive (200s to 36s) OVD. Characteristic samples from this experiment are represented in Figure 6.
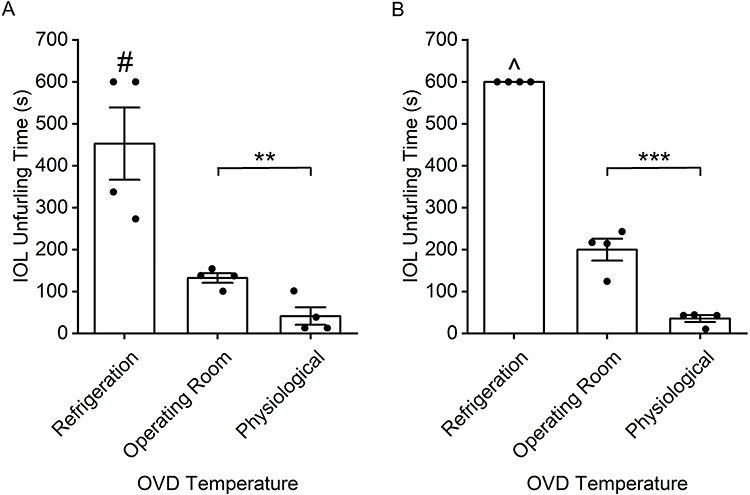 |
Figure 5 IOL unfurling time in a (A) dispersive and (B) cohesive OVD-filled plastic eye. Temperatures reflect OVD temperatures upon injection of OVD and subsequent insertion of IOL. #IOLs failed to unfurl in ten-minute time cap at 10°C for two trials. ^IOLs failed to unfurl in ten-minute time cap at 10°C for all trials. **P < 0.01. ***P < 0.001. Abbreviations: IOL, intraocular lens, OVD, ophthalmic viscoelastic device. |
 |
Figure 6 Representative IOL unfurling in OVD-filled plastic eye. IOLs often failed to unfurl within 10 minutes using refrigerated OVD. Average IOL unfurling time in across dispersive and cohesive OVD was under 200s using operating room temperature OVD and under 45s using physiological temperature OVD. Displayed: cohesive OVD. Abbreviations: IOL, intraocular lens; OVD, ophthalmic viscoelastic device. |
Discussion
This study aims to quantify the effect of temperature on IOL unfurling time. First, pre-heating of IOLs prior to injection was investigated as a method to modulate IOL unfurling time. However, this method proved ineffective at significantly modulating IOL unfurling time, even when time from heating to injection was minimized to a mean of less than 1 min. Several factors contributed to this distribution. First, during IOL loading and insertion, the IOL was able to exchange heat with the atmosphere, moderating its final temperature upon insertion. Finally, upon IOL insertion, the temperature of the solution rapidly warmed or cooled the lens to the surrounding temperature, mitigating the effects of pre-heating. This lack of significant changes in IOL unfurling time occurred despite this maximally optimized scenario. Translationally, it could not be reasonably expected for an IOL to be removed from a heating environment, loaded into an IOL, and injected into a patient’s eye in less than 1 min with reliability or safety. Thus, pre-heating the IOL presents an ineffective and impractical method to modulate IOL unfurling time.
However, it has been demonstrated in multiple models that the temperature of the solution upon IOL injection significantly affects IOL unfurling time in vitro. Specifically, IOL unfurling time can be significantly decreased by increasing the temperature of the fluid environment. This relationship held true across multiple IOL types, in solutions of BSS, dispersive OVD, or cohesive OVD, and in both spatially constrained and unconstrained environments. The first two models conducted in a 6-well plate allowed for precise quantification of this relationship, as temperature could be more precisely controlled and measured. Further, additional variables, such as contact with the edges of the anterior chamber and other variability introduced from injection technique, could be minimized. These experiments demonstrated similar distributions of exponential decay from a regression of IOL unfurling time versus solution temperature (P < 0.001). Due to the exponential nature of these results, significant decreases in IOL unfurling time occurred when warming from low temperatures. However, increments starting at higher temperatures, such as increases from 30°C to 40°C, led to minimal decreases in unfurling time. Thus, increases in solution temperature from cooler temperatures have the greatest impact on IOL unfurling time in vitro. The final model, utilizing a plastic eye, allowed for the most realistic re-creation of the surgical workflow. OVD was removed from refrigeration, at room temperature, or at physiological temperature, and the three most common temperature conditions for surgical materials in the OR were injected into a modeled anterior chamber prior to IOL injection. In this scenario, OVD temperature could not be precisely monitored following injection into the plastic eye, allowing only general trends to be observed. However, an analogous relationship was observed, with IOLs often failing to unfurl within 10 min when refrigerated OVD was used. Further, significant decreases in unfurling time were demonstrated when physiological temperature OVD, rather than operating room temperature OVD, was used. Unsurprisingly, this experiment saw greater variability in results due to the introduced spatial restriction. For example, IOLs injected near edges of the anterior chamber may be slower to unfurl, while IOLs may slide against the edge of the anterior chamber during injection, accelerating unfurling. This variability would be expected clinically, but also highlights the importance of the previous 6-well plate studies as the simplest model with the fewest confounding variables.
Of note, all IOLs were at room temperature (22°C) upon loading and injection (apart from the first experiment, which modulated IOL temperature prior to injection). Thus, changes to IOL unfurling kinetics were due to in situ heating or cooling of the IOL by the fluid in which the IOL was injected into. A second contributor to decaying IOL unfurling rates is changes in solution viscosity with temperature. This was not a large contributor in the BSS model but was certainly an important factor in the OVD-filled 6-well plate and plastic eye models, as OVD viscosity is known to vary greatly across the temperature range of our experiments.
We have consistently demonstrated that solutions at 10°C or below significantly hamper the ability for IOLs to unfurl in a clinically acceptable timeframe. This supported our hypothesis, as 10°C is below the glass transition temperature of the tested IOLs. Thus, the IOLs existed in a solid, glassy state, rather than the flexible, rubbery state observed above their glass transition temperature.
Further, increasing solution temperature from 20°C to 30°C decreases IOL unfurling time on the scale of minutes. Heating above 30°C may further accelerate IOL unfurling time, as our results showed trends in that direction, but this was not significant with the given sample size. Thus, we predict that utilizing BSS and/or OVD largely above 30°C will not accelerate IOL unfurling time with large clinical significance. This is demonstrated by our fitted functions, which predict IOL unfurling times ranging from 9s to 31s at 30°C and from 0.5s to 6s at 40°C.
Reductions in IOL unfurling time from increased solution temperature hold significant clinical relevance, as cataract surgeries are otherwise extremely efficient, often lasting only 10 min. When IOLs fail to efficiently unfurl, this is an idle part of surgery that remains one of few unoptimized segments of the entire procedure. Thus, decrease in IOL unfurling time by even 30s represents a 5% decrease in surgical time.
However, a key limitation of our study is its in vitro method. Although we successfully assessed the kinetics of IOL unfurling using a benchtop study with minimized confounding variables, cataract surgery introduces several additional considerations. While new BSS and OVD are introduced into the eye throughout the surgery, patients’ body temperature may contribute to the temperature of the solution the IOL is injected into. Well-plate and plastic eye models were selected to allow for precise assessment of IOL unfurling kinetics, but there may be additional IOL interactions with the anatomy of the eye, particularly the capsular bag, in clinical settings. Environmental factors could be accounted for if testing is repeated ex vivo in porcine or cadaver eyes. Given these in vitro limitations, our results cannot be precisely generalized to the surgical environment. However, consistent results between experiments show reasonable support for an exponential distribution between IOL unfurling time and solution temperature across IOL and solution types and lead us to expect a similar distribution exists in other potential models.
Other potential variables affecting IOL unfurling time remain to be investigated. Surgeons have additional methods at their disposal to accelerate IOL unfurling when desired, including direct BSS irrigation onto the surface of the IOL as well as bimanual pulling of the IOL haptics. Further, it remains to be investigated whether filling the IOL injector with warmed OVD7 or injecting warmed OVD directly into the eye8 will have greater consequences on IOL unfurling time. Finally, the consequences of how tightly the optic is wrapped within the injector prior to injection were not investigated for its effect on unfurling time.
This study is not representative of IOLs from multiple manufacturers. Further, although multiple IOL types (toric, monofocal, multifocal) were used, our results only describe the unfurling kinetics of acrylic hydrophobic IOLs. Specifically, only Alcon AcrySof IOLs were tested. Although the AcrySof material is currently being phased-out, the vast majority of IOLs in use in the United States are similarly hydrophobic acrylic.12,13 As of 2021, 79% of surgeons preferred the two leading acrylic hydrophobic monofocal IOLs for most cases. In the same year, 58% of surgeons preferred the AcrySof material for toric IOLs, with hydrophobic acrylic being the preferred material for virtually 100% of surgeons.14 In 2023, AcrySof IOLs remain the lens of choice for premium, non-premium, presbyopic, toric, and monofocal applications.15 Furthermore, Eom et al8 found no difference in the unfurling kinetics between their two tested dry-packaged hydrophobic acrylic IOLs, which can be attributed to their glass transition temperatures within 1°C. Another study11 found the glass transition temperatures of five leading dry-packaged hydrophobic acrylic IOLs to be within 4°C. More recent IOLs are largely made of the same materials, and we expect similar trends would emerge.
Despite these limitations, the results of this study warrant further investigation into the potential for increasing the temperature of surgical disposables as a method to decrease IOL unfurling time and thereby decrease operative time. A prospective clinical study is needed to answer this question, and potential consequences on surgical outcomes should be assessed. Notably, several studies have shown the potential benefit of cold BSS in protecting the corneal endothelium16 and macula17 during phacoemulsification. Thus, it may be optimal for warm OVD and/or BSS to be used only following phacoemulsification and during IOL injection, when a clinical benefit from accelerated IOL unfurling may be seen. Based on the results of this study, we hypothesize that the following trends would be replicated in surgery. Often, OVD and BSS are injected into the eye below operating room temperature. We expect to see the largest decreases in IOL unfurling time when these disposables are brought to operating room temperature. Accelerated IOL unfurling would occur with increased heating until approximately 30°C. Further heating, such as to physiological temperature, would lead to only small decreases in IOL unfurling time.
While rapid unfurling may introduce a risk of trapping OVD within the capsular bag, higher temperatures decrease OVD viscosity, making it easier to remove without the need for extensive manipulation.18 Warm OVD has already been demonstrated to have potential positive effects in reducing surgical time.8 Conducting additional investigations to better understand the effects of temperature on other surgical metrics, such as corneal edema and endothelial cell function, may help create insights into ways to improve surgical outcomes via temperature modulation.
Conclusion
Our results provide preliminary evidence into the potential for temperature regulation to benefit cataract surgery procedures, namely a potential decrease in surgical time. Bringing OVD and/or BSS to 30°C or higher during or surrounding IOL injection may result in minimized unfurling times. However, a scarce number of studies regarding the clinical relevance of temperature in the ocular environment during cataract surgery exist. Further research into varying this parameter for application in cataract surgery may prove insightful for optimizing the procedure and improving outcomes.
Acknowledgments
The authors thank Shameema Sikder, MD, of the Wilmer Eye Institute at Johns Hopkins University School of Medicine, for her assistance in accessing laboratory facilities and materials. The authors additionally thank Sai Rayasam and Daniel Wang for serving as independent blinded adjudicators.
Funding
Supported by a grant from Department of Biomedical Engineering at Johns Hopkins University. Supported through access to time and tools at Ophthalmic Practice Lab at Johns Hopkins Hospital, Baltimore, MD, USA. No sponsors were involved in the design, data collection, analysis, writing, or submission of the paper.
Disclosure
EER, RM, JP, EL are employees of ThermOptik, LLC. EER, RM, JP, EL, KW, AOE are owners of ThermOptik, LLC. GA, MP, RA serve as board members of ThermOptik, LLC. KW is a consultant for Johnson & Johnson Vision, Inc. and reports equity from ThermoOptik, LLC. EER, RM, JP, EL, GA, MP, RA report patent applications pending to ThermOptik related to this work. The authors report no other conflicts of interest in this work.
References
1. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e1234. doi:10.1016/S2214-109X(17)30393-5
2. Minami K, Yaguchi S, Bissen-Miyajima H. Temperature-controlled porcine eye holder for observing intraocular temperature during cataract surgery. Sci Rep. 2023;13(1):4331. doi:10.1038/s41598-023-31070-4
3. Iwase T, Tanaka N. Unfolding characteristics of a new hydrophobic acrylic intraocular lens, and possible association with complications in triple procedures. Clin Exp Ophthalmol. 2007;35(7):635–639. doi:10.1111/j.1442-9071.2007.01565.x
4. Miyake T, Kamiya K, Amano R, Iida Y, Tsunehiro S, Shimizu K. Long-term clinical outcomes of toric intraocular lens implantation in cataract cases with preexisting astigmatism. J Cataract Refract Surg. 2014;40(10):1654–1660. doi:10.1016/j.jcrs.2014.01.044
5. Shah GD, Praveen MR, Vasavada AR, Vasavada VA, Rampal G, Shastry LR. Rotational stability of a toric intraocular lens: influence of axial length and alignment in the capsular bag. J Cataract Refract Surg. 2012;38(1):54–59. doi:10.1016/j.jcrs.2011.08.028
6. Shugar JK. Implantation of AcrySof acrylic intraocular lenses. J Cataract Refract Surg. 1996;22(Suppl 2):1355–1359. doi:10.1016/S0886-3350(96)80097-6
7. Minami K, Miyata K, Nagai N, Sasaki H. Use of a warmed ophthalmic viscoelastic device to accelerate the unfolding of 1-piece intraocular lenses in the capsular bag. J Cataract Refract Surg. 2015;41(10):2332–2333. doi:10.1016/j.jcrs.2015.09.003
8. Eom Y, Lee JS, Rhim JW, Kang SY, Song JS, Kim HM. A simple method to shorten the unfolding time of prehydrated hydrophobic intraocular lens. Can J Ophthalmol. 2014;49(4):382–387. doi:10.1016/j.jcjo.2014.06.002
9. Jung GB, Jin KH, Park HK. Physicochemical and surface properties of acrylic intraocular lenses and their clinical significance. J Pharm Investig. 2017;47(5):453–460. doi:10.1007/s40005-017-0323-y
10. Tehrani M, Dick HB, Wolters B, Pakula T, Wolf E. Material properties of various intraocular lenses in an experimental study. Ophthalmologica. 2004;218(1):57–63. doi:10.1159/000074568
11. Bozukova D, Pagnoulle C, Jérôme C. Biomechanical and optical properties of 2 new hydrophobic platforms for intraocular lenses. J Cataract Refract Surg. 2013;39(9):1404–1414. doi:10.1016/j.jcrs.2013.01.050
12. Leaming DV. Practice styles and preferences of ASCRS members--2003 survey. J Cataract Refract Surg. 2004;30(4):892–900. doi:10.1016/j.jcrs.2004.02.064
13. Bethke W. Surgeons share their views on IOLs. Rev Ophthalmol. 2018;25(1):42–44.
14. Bethke W. IOL survey: new lenses turn surgeons’ heads. Rev Ophthalmol. 2021;28(1):40–42.
15. Bethke W. Cataract surgeons embrace new options. Rev Ophthalmol. 2023;30(1):35–37.
16. Meduri A, Aragona P, Testagrossa B, et al. An alternative approach to cataract surgery using BSS temperature of 2.7 °C. Appl Sci. 2020;10(8):2682. doi:10.3390/app10082682
17. Meduri A, Oliverio GW, Bergandi L, et al. Role of Cold Balanced Salt Solution (BSS) in the prophylaxis of cystoid macular edema after cataract surgery: a prospective randomized study. Clin Ophthalmol. 2021;15:2519–2526. doi:10.2147/OPTH.S304146
18. Rahman MQ, Chuah KS, Macdonald EC, Trusler JP, Ramaesh K. The effect of pH, dilution, and temperature on the viscosity of ocular lubricants--shift in rheological parameters and potential clinical significance. Eye. 2012;26(12):1579–1584. doi:10.1038/eye.2012.211
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Optical Biometry and Lens Power Calculations in 500 Phakic Patients: Axial Length and Corneal Curvature in the Fellow Eye
Kristianslund O, Hassaf SE, Drolsum L
Clinical Ophthalmology 2022, 16:2775-2780
Published Date: 23 August 2022
Visual and Refractive Efficacy of Panoptix Toric Intraocular Lens in a Clinical Setting
Ackerman M, Lawless M, Levitz L, Bhatt U, Reich JA, Sutton G, Roberts TV, Tenen A, Kaur A, Hodge C
Clinical Ophthalmology 2022, 16:4227-4237
Published Date: 19 December 2022
Clinical Outcomes of a New Non-Diffractive Extended Depth-of-Focus Intraocular Lens Targeted for Mini-Monovision
Tomagova N, Elahi S, Vandekerckhove K
Clinical Ophthalmology 2023, 17:981-990
Published Date: 25 March 2023
Comparing the Accuracy of the Kane, Barrett Universal II, Hill-Radial Basis Function, Emmetropia Verifying Optical, and Ladas Super Formula Intraocular Lens Power Calculation Formulas
Moshirfar M, Sulit CA, Brown AH, Irwin C, Ronquillo YC, Hoopes PC
Clinical Ophthalmology 2023, 17:2643-2652
Published Date: 7 September 2023
Comparison of Visual Performance and Patient Satisfaction Between Two Trifocal Intraocular Lenses: A Prospective, Paired-Eye Comparative Study
Kang S, Arsenault SM, O’Brien RC, Chatzea MS, Zarei-Ghanavati S, Beniz LAF, Yoo SH
Clinical Ophthalmology 2026, 20:572237
Published Date: 17 January 2026