Back to Journals » Journal of Pain Research » Volume 12
Clinical Manifestations Of Adenomyosis Patients With Or Without Pain Symptoms
Authors Chen Q, Li YW ![]() , Wang S
, Wang S ![]() , Fan QB, Shi HH, Leng JH, Sun DW, Lang JH, Zhu L
, Fan QB, Shi HH, Leng JH, Sun DW, Lang JH, Zhu L ![]()
Received 13 April 2019
Accepted for publication 1 October 2019
Published 14 November 2019 Volume 2019:12 Pages 3127—3133
DOI https://doi.org/10.2147/JPR.S212117
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Qian Chen,* Yun-Wei Li,* Shu Wang, Qing-Bo Fan, Hong-Hui Shi, Jin-Hua Leng, Da-Wei Sun, Jing-He Lang, Lan Zhu
Department of Gynecology and Obstetrics, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shu Wang; Qing-Bo Fan
Department of Obstetrics and Gynecology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, 1 ShuaiFuYuan, Wangfujing, DongCheng District, Beijing 100730, People’s Republic of China
Tel +86-10-69156204
Fax +86-10-69154875
Email [email protected]; [email protected]
Purpose: Our study aims to investigate the distribution of pain symptoms and the association between pain symptoms and clinical parameters in patients with adenomyosis.
Patients and methods: The clinical and pathological data of 291 patients diagnosed with adenomyosis in the Obstetrics and Gynecology Department of Peking Union Medical College Hospital from March 2012 to September 2015 were collected, and analyzed in regard to the pain symptoms.
Results: The median age at disease onset was 34 years. 71.8% of the patients had pain symptoms (pain group) and 28.2% had no pain symptoms (painless group). Patients with symptoms accompanied by dysmenorrhea accounted for 68%, among which 30.3% were mild, 36.9% were moderate, and 32.8% severe, while 56.1% presented with progressive pain. Through comparison, significant differences were identified between the pain and painless groups with regard to age at diagnosis (P=0.009), age at onset of disease (P=0.008), and level of pre-surgical CA125 (P<0.001), as well as proportion of patients with rectal irritation (P=0.008), elevated CA125 level (P<0.001), thickened myometrial layer (P<0.001) and concurrent endometriosis (P=0.001). In the multivariable analysis, an elevated level of pre-surgical CA125 (P<0.001) and thickened posterior myometrial layer (P=0.023) were both independent risk factors for the morbidity of pain symptoms. Similar results except for the difference in rectal irritation were noticed when we made further comparison between the dysmenorrhea and non-dysmenorrhea groups in adenomyosis patients.
Conclusion: Our research analyzes the clinical features related to pain symptoms in patients with adenomyosis, which may provide clues for the possible presurgical diagnosis of adenomyosis, as well as references for pain management of adenomyosis.
Keywords: adenomyosis, pain symptoms, clinical features, risk factors
Introduction
Uterine adenomyosis is a status of hyperplasia and hypertrophy of uterine myometrium due to the ectopic growth of the endometrial glands and stroma.1 Though clinically common, it confuses us due to a lack of standard diagnostic criteria.2 Adenomyosis can be diagnosed by surgical procedure, such as hysterectomy, which gives an access to a full myometrial assessment, or by myometrial biopsies.3 Two common noninvasive imaging methods, transvaginal ultrasound (TVUS) and magnetic resonance imaging (MRI), are widely adopted in clinical work with high accuracy.4
Heterogeneous as it is in clinical features, adenomyosis may lead to various performances in different individuals, such as abnormal uterine bleeding (AUB), different forms of pain, nausea, difficulties with urination and so on. Among them, AUB and dysmenorrhea are the top two reasons for patients to see a doctor, which may exert burdensome impacts on their daily life. Several published literatures have shed light on the treatment of the pain caused by adenomyosis, especially dysmenorrhea.5–7 Few studies have focused on the factors or clinical behaviors related to pain arising from adenomyosis. Our previous study identified that patients with adenomyosis received less accurate preoperative diagnosis, as the accuracy rate was only 36.4%.8 Most patients with pain symptoms were not correctly diagnosed before surgery, resulting in inappropriate or inadequate treatment. We carried out this retrospective study with an intention to help understand the clinical features of patients with adenomyosis-related pain and improve the preoperative diagnosis rate of such patients, thus providing timely and effective treatment for them.
Methods
From March 2012 to September 2015, 361 patients received surgery and were pathologically diagnosed with uterine adenomyosis in the Department of Obstetrics and Gynecology at Peking Union Medical College Hospital. We enrolled 291 of them who were in accordance with our inclusion and exclusion criteria described in our previously published article8 (Figure 1). Relative clinical and pathological data were extracted for analysis, such as demographic characteristics, clinical manifestations, and pathological results.
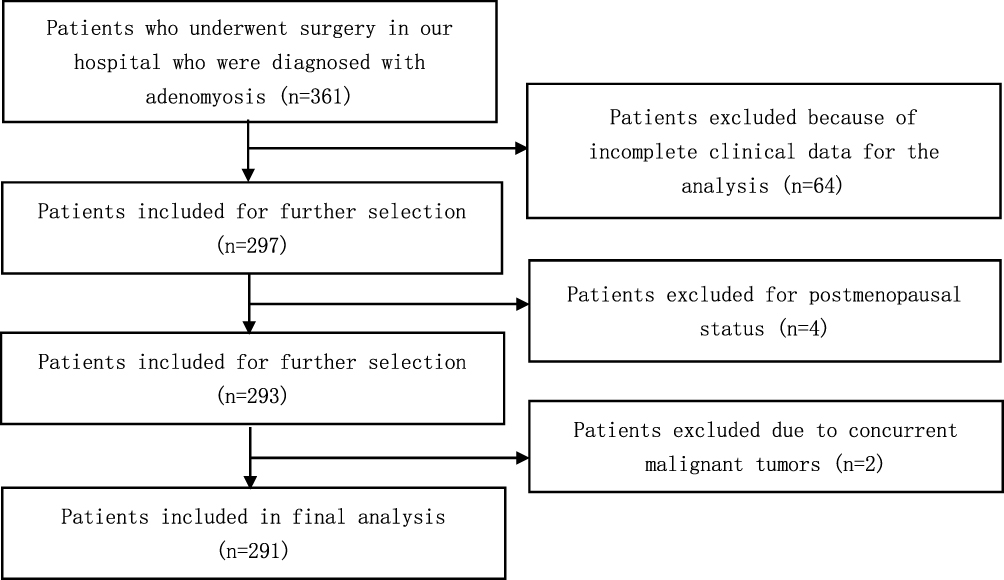 |
Figure 1 Flowchart for the patient selection progress. |
The severity of pain symptom was evaluated with the method of 10-cm Visual Analog Scale (VAS) before the use of any relative drugs or surgery based on the self-assessment of patients.9 The degree of pain was defined as mild if VAS was 1–3, moderate if 4–7, severe if 8–10, and none if 0. An elevated CA125 means the concentration of CA125 is above 35 U/mL.
We used IBM SPSS 23.0 software (IBM, USA) to statistically analyze the data. Continuous variables were analyzed with non-parametric U-test, and categorical variables with Chi-square test or Fisher’s exact test. Multivariate analysis was conducted with Cox proportional hazards regression model. A p-value of <0.05 was considered significant.
Results
Of the 291 included patients, 209 (71.8%) complained of pain symptom. A total of 198 (68.0%) patients presented dysmenorrhea, among which, 111 (56.1%) were progressively worsened. With regarding to the pain degree of the dysmenorrhea, mild cases accounted for 30.3%, moderate cases 36.9% and severe cases 32.8%. Totally, 70 (24.1%) patients’ symptoms were accompanied by chronic pelvic pain, 24 (8.2%) with dyspareunia, and 7 (2.4%) with anorectal pain (Table 1).
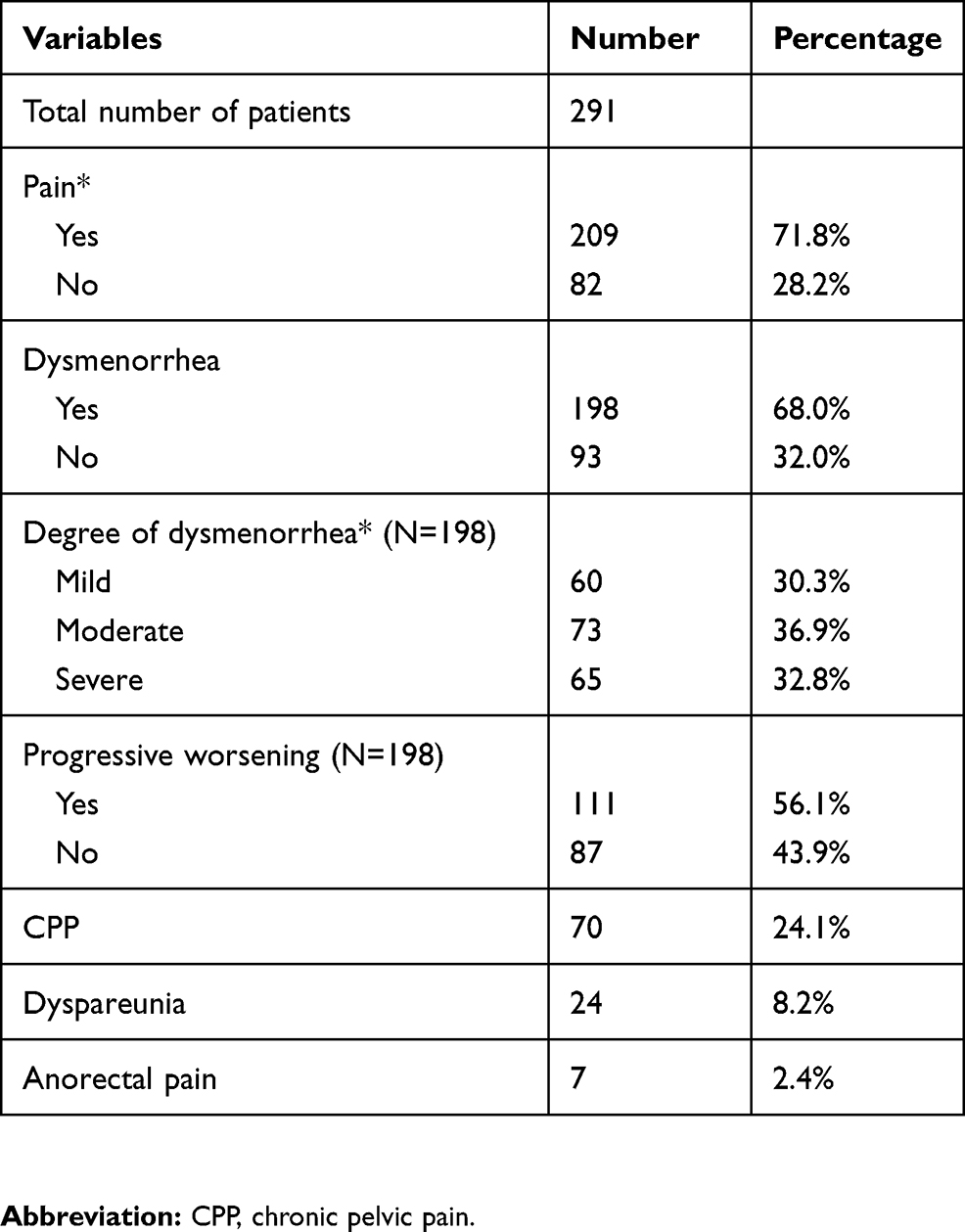 |
Table 1 Pain Characteristics In Patients With Adenomyosis |
The overlapping of pain symptoms were shown in Supplementary Table 1. The number of patients with pure dysmenorrhea, chronic pelvic pain, and dyspareunia were 131, 10, and 2, respectively. The remaining patients were with two or more kinds of pain symptoms.
Comparison Between Pain And Painless Group
We divided all the patients into two groups in terms of the pain manifestation: pain group and painless group (Table 2). Patients in pain group were much younger than those in painless group when focusing on the age at diagnosis and onset of disease (median [Q1, Q3], 40.0 [34.0, 44.0] vs 42.0 [36.0, 46.0] years, P = 0.009; 33.0 [28.0, 39.0] vs 36.0 [30.1, 42.0] years, P = 0.008, respectively). A higher level of pre-surgical CA125 was identified in patients of pain group (85.9 [43.0–176.7] vs 33.2 [16.3–58.5] U/mL, P<0.001). More patients in pain group presented rectal irritation (20.1% vs 7.3%, P = 0.008), elevated CA125 (65.1% vs 29.3%, P<0.001), thicken myometrial layer (18.7% vs 2.4%, P<0.001) and concurrent endometriosis (45.0% vs 23.2%, P = 0.001). Differences were not significant in the interval between onset and diagnosis, age of menarche, duration or interval of mense, gravidity, parity, menorrhagia, bladder irritation, HGB level, GnRHa injection, CA199 level, volume of uterus, coexisting uterine fibroids and benign endometrial diseases.
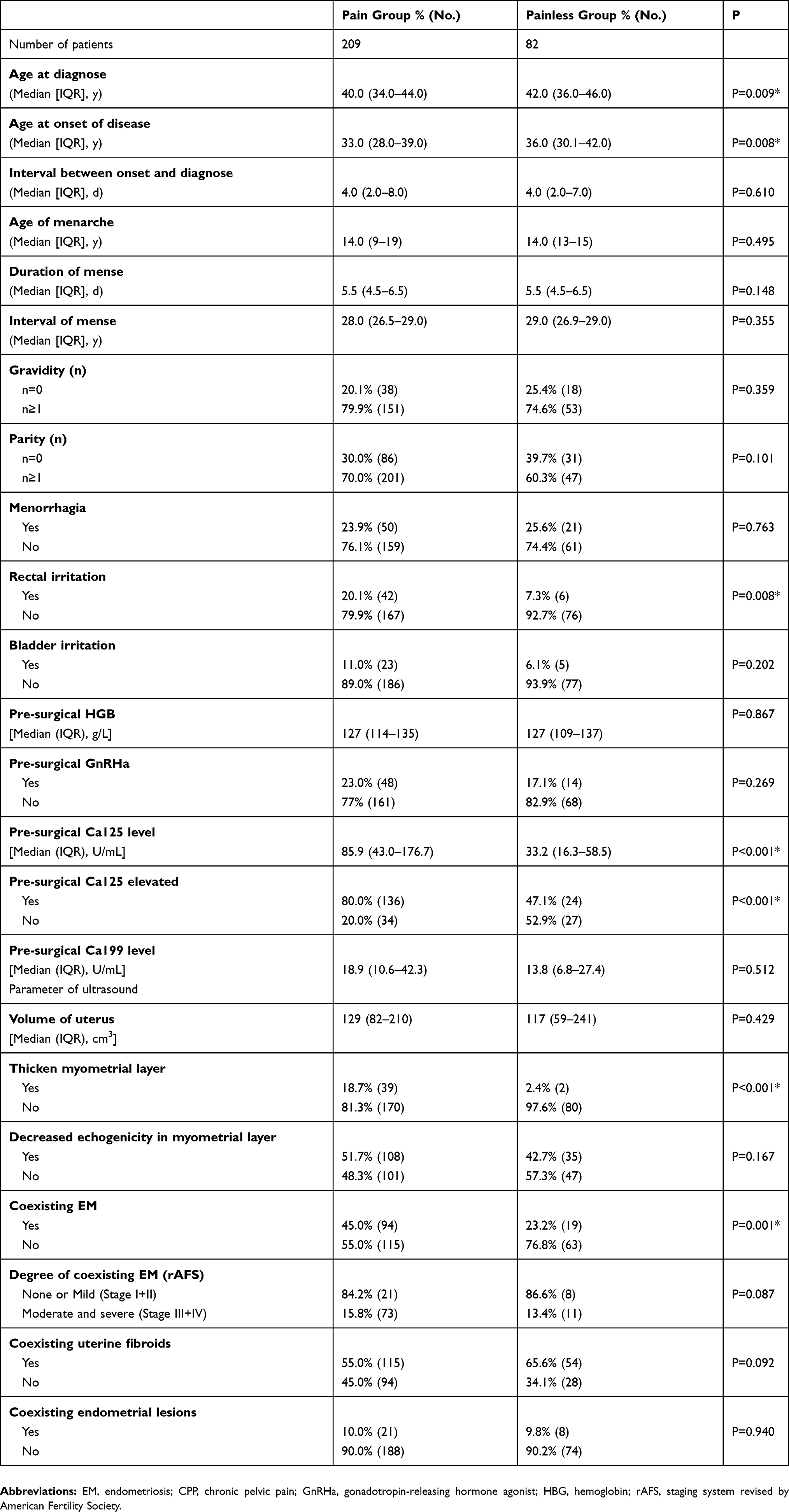 |
Table 2 The Comparison Between Adenomyosis Patients With Or Without Pain Symptoms |
In the multivariable analysis, an elevated level of pre-surgical CA125 (P<0.001) and thicken posterior myometrial layer (P = 0.023) were both independent risk factors for the appearance of pain symptoms (Table 3).
 |
Table 3 The Multivariate Analysis By Logistic Regression For Adenomyosis Patients With Pain Symptoms |
Comparison Between Dysmenorrhea And Non-Dysmenorrhea Group
Since 68% patients presented dysmenorrhea, we made a further analysis for adenomyosis patients with pure dysmenorrhea (131) (presented in Supplementary Table 1).
Patients in dysmenorrhea group were also much younger than those in non-dysmenorrhea group in terms of the age at diagnosis and onset of disease (P = 0.012 and P = 0.012, respectively). A higher level of pre-surgical CA125 was identified in patients of dysmenorrhea group compared with the other one (P<0.001). More patients in dysmenorrhea group presented elevated CA125 (P<0.001), thicken myometrial layer (P<0.001) and concurrent endometriosis (P = 0.023). (Supplementary Table 2). In the multivariable analysis, an elevated level of pre-surgical CA125 (P<0.001) and thicken posterior myometrial layer (P = 0.008) were both independent risk factors for the appearance of dysmenorrhea (Supplementary Table 3).
Discussion
In our study, we identified that most adenomyosis patients had symptoms accompanied by pain manifestation. Proportions of various forms of adenomyosis-related pain were also calculated, with dysmenorrhea ranking the first. Patients in pain group presented following characteristics compared to those without pain: younger onset age and younger diagnosed age, higher level of CA125, more likely to have concomitant rectal irritation, elevated CA125, thicken myometrial layer and endometriosis. We also identified that an elevated level of pre-surgical CA125 and thicken posterior myometrial layer were both independent risk factors for the morbidity of pain symptoms.
The pain manifestation was one of the main driving factors for adenomyosis patients to carry out relative physical examinations. In our research, adenomyosis-related pain included dysmenorrhea, chronic pelvic pain, dyspareunia, and anorectal pain, none of which were specific enough to be highly predictive for adenomyosis.10 An American study analyzed the symptoms of adenomyosis in the form of interviews, which provided us with more detailed and straight findings. Totally 11 different types of pain were documented together with several representative quotes, and dysmenorrhea was complained the most, which echoes our study. Pelvic pain and dyspareunia were also mentioned at lower frequencies.11
In our further analysis for dysmenorrhea, it was interesting to notice that the analysis results were consistent with the above pain analysis except for the symptom of rectal irritation. The elevated level of pre-surgical CA125 and thicken posterior myometrial layer were also independent risk factors for the appearance of dysmenorrhea. These results further indicated the close relationship between dysmenorrhea and adenomyosis.
Though poorly understood, a widespread theory is that the pathogenesis of adenomyosis is the presence of endometrial basalis layer in the myometrium through invagination, possibly because of the damage of the endometrial-myometrial border or the changes of the immune system.12,13 The occurrence of dysmenorrhea may attribute to increased prostaglandin production in adenomyotic tissues, inflammation, nerve fiber density as well as upregulated oxytocin receptors, all of which still needs to be further verified.14–16
Patients in pain group were at younger ages when diagnosed and suffered the onset of disease. Curiously, the median intervals between onset and diagnosis of the pain and painless group were the same, both 4 days. Maybe other symptoms such as AUB or subfertility were the driven factors for patients in painless group to obtain the diagnosis.
TVUS, either 2D or 3D, was widely used to make a diagnosis of adenomyosis with a group of studies carried out to evaluate its accuracy.17,18 It played important roles in evaluating the severity of adenomyosis and providing a reference for the treatment. J. Naftalin et al suggested a statistically significant association between the ultrasound features of adenomyosis and the severity of menstrual pain, in detail, the irregular endometrial–myometrial junction and asymmetrical myometrial thickening.19 A higher possibility of posterior thicken myometrial layer was also seen in pain group, with no significant differences between pain and painless group in concurrent uterine fibroids (P=0.092) or benign endometrial diseases (P=0.940).
The elevation of CA125 was quite common in adenomyosis, but it was far from satisfied to be a predictive marker because of the limited specificity. Actually, there are no biomarkers in use with certain values in differentiating adenomyosis from other gynecological disease, and more investigations are needed to bring through the standstill.10
Substantial similarities can be found between adenomyosis and endometriosis in terms of clinical features and pathogenetic pathways.20 38.8% of the 291 adenomyosis patients were identified with concurrent endometriosis, as previously reported in our group.8 We also noticed a significant difference between pain and painless group on rectal irritation. The theory that rectal irritation and EM are related with pain symptoms is mostly empirical, lacking of clinical research data to support. More patients were found with coexisting endometriosis in the pain group in this study, which made sense as dysmenorrhea was quite common among endometriosis patients. Our results were evidenced by real-world data, suggesting that we should pay attention to the presence of EM in patients with adenomyosis-related pain in clinical work.
For adenomyosis, no standard treatment guidelines are provided for clinical management and no drug is FDA approved. Nonsteroidal anti-inflammatory drugs (NSAIDs) are a common option for alleviating the pain symptoms, especially dysmenorrhea, but we should pay attention to its potential adverse effects.21 Other medical choices such as GnRHa, danazol, oral progestins, and aromatase inhibitors as well as surgical treatments are also applied in clinical work, but evidence from large randomized trials is needed to help select the best method.
Conclusion
We summarized some characteristics related to pain manifestation and, more specifically, dysmenorrhea in patients with adenomyosis. The symptoms of pain together with obvious elevation of CA125 and rectal irritation as well as thicken myometrial layer under the TVUS may be regarded as clues for clinicians when dealing with adenomyosis. A clinical model constituted by these characters may improve the preoperative diagnosis rate of adenomyosis, thus providing timely and effective treatment for the patients. Further investigations are required for better pain management in clinical work.
Ethical Approval And Consent
Our study has been approved by Ethics Committee of Peking Union Medical College Hospital, Beijing, China, and was performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from all individual participants included in the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Benagiano G, Habiba M, Brosens I. The pathophysiology of uterine adenomyosis: an update. Fertil Steril. 2012;98(3):572–579. doi:10.1016/j.fertnstert.2012.06.044
2. Seidman JD, Kjerulff KH. Pathologic findings from the Maryland Women’s Health Study: practice patterns in the diagnosis of adenomyosis. Int J Gynecol Pathol. 1996;15(3):217–221.
3. Struble J, Reid S, Bedaiwy MA. Adenomyosis: a clinical review of a challenging gynecologic condition. J Minim Invasive Gynecol. 2016;23(2):164–185. doi:10.1016/j.jmig.2015.09.018
4. Dueholm M, Lundorf E. Transvaginal ultrasound or MRI for diagnosis of adenomyosis. Curr Opin Obstet Gynecol. 2007;19(6):505–512. doi:10.1097/GCO.0b013e3282f1bf00
5. Radzinsky VE, Khamoshina MB, Nosenko EN, et al. Treatment strategies for pelvic pain associated with adenomyosis. Gynecol Endocrinol. 2016;32(sup2):19–22. doi:10.1080/09513590.2016.1232673
6. Osuga Y, Fujimoto-Okabe H, Hagino A. Evaluation of the efficacy and safety of dienogest in the treatment of painful symptoms in patients with adenomyosis: a randomized, double-blind, multicenter, placebo-controlled study. Fertil Steril. 2017;108(4):673–678. doi:10.1016/j.fertnstert.2017.07.021
7. Younes G, Tulandi T. Conservative surgery for adenomyosis and results: a systematic review. J Minim Invasive Gynecol. 2018;25(2):265–276. doi:10.1016/j.jmig.2017.07.014
8. Li YW, Liu YT, Wang S, et al. Clinical manifestations of adenomyosis patients with or without coexisting endometriosis. Chin Med J (Engl). 2018;131(20):2495–2498. doi:10.4103/0366-6999.243572
9. Bourdel N, Alves J, Pickering G, Ramilo I, Roman H, Canis M. Systematic review of endometriosis pain assessment: how to choose a scale? Hum Reprod Update. 2015;21(1):136–152. doi:10.1093/humupd/dmu046
10. Abbott JA. Adenomyosis and Abnormal Uterine Bleeding (AUB-A)-pathogenesis, diagnosis, and management. Best Pract Res Clin Obstet Gynaecol. 2017;40:68–81. doi:10.1016/j.bpobgyn.2016.09.006
11. Nelsen LM, Lenderking WR, Pokrzywinski R, et al. Experience of symptoms and disease impact in patients with adenomyosis. Patient. 2018;11(3):319–328. doi:10.1007/s40271-017-0284-2
12. Ferenczy A. Pathophysiology of adenomyosis. Hum Reprod Update. 1998;4(4):312–322. doi:10.1093/humupd/4.4.312
13. Ota H, Igarashi S, Hatazawa J, Tanaka T. Is adenomyosis an immune disease? Hum Reprod Update. 1998;4(4):360–367. doi:10.1093/humupd/4.4.360
14. Koike H, Egawa H, Ohtsuka T, Yamaguchi M, Ikenoue T, Mori N. Correlation between dysmenorrheic severity and prostaglandin production in women with endometriosis. Prostaglandins Leukot Essent Fatty Acids. 1992;46(2):133–137. doi:10.1016/0952-3278(92)90219-9
15. Zhang X, Lu B, Huang X, Xu H, Zhou C, Lin J. Innervation of endometrium and myometrium in women with painful adenomyosis and uterine fibroids. Fertil Steril. 2010;94(2):730–737. doi:10.1016/j.fertnstert.2009.03.026
16. Guo SW, Mao X, Ma Q, Liu X. Dysmenorrhea and its severity are associated with increased uterine contractility and overexpression of oxytocin receptor (OTR) in women with symptomatic adenomyosis. Fertil Steril. 2013;99(1):231–240. doi:10.1016/j.fertnstert.2012.08.038
17. Brosens JJ, de Souza NM, Barker FG, Paraschos T, Winston RM. Endovaginal ultrasonography in the diagnosis of adenomyosis uteri: identifying the predictive characteristics. Br J Obstet Gynaecol. 1995;102(6):471–474. doi:10.1111/j.1471-0528.1995.tb11320.x
18. Exacoustos C, Brienza L, Di Giovanni A, et al. Adenomyosis: three-dimensional sonographic findings of the junctional zone and correlation with histology. Ultrasound Obstet Gynecol. 2011;37(4):471–479. doi:10.1002/uog.8900
19. Naftalin J, Hoo W, Nunes N, Holland T, Mavrelos D, Jurkovic D. Association between ultrasound features of adenomyosis and severity of menstrual pain. Ultrasound Obstet Gynecol. 2016;47(6):779–783. doi:10.1002/uog.15798
20. Benagiano G, Brosens I, Habiba M. Structural and molecular features of the endomyometrium in endometriosis and adenomyosis. Hum Reprod Update. 2014;20(3):386–402. doi:10.1093/humupd/dmt052
21. Marjoribanks J, Ayeleke RO, Farquhar C, Proctor M. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Sys Rev. 2015;(7):CD001751.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.