Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Clinical Indicators for Asthma-COPD Overlap: A Systematic Review and Meta-Analysis
Authors Peng J, Wang M, Wu Y, Shen Y ![]() , Chen L
, Chen L ![]()
Received 10 May 2022
Accepted for publication 24 September 2022
Published 12 October 2022 Volume 2022:17 Pages 2567—2575
DOI https://doi.org/10.2147/COPD.S374079
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Min Zhang
Junjie Peng,* Min Wang,* Yanqiu Wu,* Yongchun Shen, Lei Chen
Department of Respiratory and Critical Care Medicine, West China Hospital, West China School of Medicine, Sichuan University, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lei Chen; Yongchun Shen, Department of Respiratory and Critical Care Medicine, West China Hospital, West China School of Medicine, Sichuan University, Chengdu, People’s Republic of China, Email [email protected]; [email protected]
Background: Some clinical indicators have been reported to be useful in differentiating asthma-chronic obstructive pulmonary disease (COPD) overlap (ACO) from pure asthma/COPD, but the results were inconsistent. This study aims to evaluate the diagnostic value of these indicators for ACO.
Methods: Databases of PubMed, EMBASE, Ovid and Web of Science were retrieved. Pooled standardized mean differences (SMDs) with 95% confidence intervals (CIs) were calculated in random-effects models.
Results: 48 eligible studies were included. The pooled results indicated, compared with pure asthma, ACO patients had lower levels of forced expiratory volume in the first second (FEV1)% predicted (pred) (SMD=− 1.09, 95% CI − 1.3 to − 0.87), diffusion lung capacity for carbon monoxide (DLCO)% pred (SMD=− 0.83, 95% CI − 1.24 to − 0.42), fractional exhaled nitric oxide (FeNO) (SMD=− 0.23, 95% CI − 0.36 to − 0.11), and higher levels of induced sputum neutrophil (SMD = 0.51, 95% CI 0.21 to 0.81), circulating YKL-40 (SMD = 0.96, 95% CI 0.27 to 1.64). However, relative to COPD alone, ACO patients had higher levels of FEV1% pred (SMD = 0.15, 95% CI 0.05 to 0.26), DLCO% pred (SMD = 0.38, 95% CI 0.16 to 0.6), FeNO (SMD = 0.59, 95% CI 0.40 to 0.78), serum total immunoglobulin (Ig)E (SMD = 0.42, 95% CI 0.1 to 0.75), blood eosinophil (SMD = 0.44, 95% CI 0.29 to 0.59), induced sputum eosinophil (SMD = 0.62, 95% CI 0.42 to 0.83), and lower levels of induced sputum neutrophil (SMD=− 0.48, 95% CI − 0.7 to − 0.27), circulating YKL-40 (SMD=− 1.09, 95% CI − 1.92 to − 0.26).
Conclusion: Compared with pure asthma/COPD, ACO patients have different levels of FEV1% pred, DLCO% pred, FeNO, serum total IgE, blood eosinophil, induced sputum eosinophil/neutrophil, and circulating YKL-40, which could be helpful to establish a clinical diagnosis of ACO.
Keywords: asthma, asthma-COPD overlap, COPD, indicators, meta-analysis
Introduction
Asthma-chronic obstructive pulmonary disease (COPD) overlap syndrome (ACOS) is a term to describe patients with both features of asthma and COPD, firstly proposed by a joint section of the Global Initiative for Asthma (GINA) and the Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) in 2014, and revised to “ACO” in GINA 2017.1 ACO is epidemiologically considered in 2% of the general population, 29.6% of asthmatic patients and 26.5% of COPD patients.2 Patients with ACO have a greater burden of symptoms, frequent exacerbations, poor quality of life, a more rapid decline in lung function and greater use of healthcare resources compared to patients with asthma or COPD alone, but global diagnostic criteria for ACO are inconclusive.3,4
To date, asthma and COPD are considered as two different types of chronic airway inflammation.5,6 T-helper (Th) 2 inflammatory pattern plays an important role in the development and progression of asthma, which is indicated by blood/sputum eosinophil, serum total immunoglobulin (Ig) E, circulating periostin and fractional exhaled nitric oxide (FeNO).1,5 However, COPD is often characterized by Th1 inflammation, dominated by macrophages and neutrophils.6 ACO shares some inflammatory characteristics between asthma and COPD, and in the past few years, some clinical indicators were reported to be useful in differentiating ACO from pure asthma or COPD, but the results were inconsistent.7–10
Therefore, we performed a systematic review and meta-analysis to evaluate the potential diagnostic value of these clinical indicators, including post-bronchodilator forced expiratory volume in the first second (FEV1)% predicted (pred), diffusing capacity of the lungs for carbon monoxide (DLCO)% pred, FeNO, serum total IgE, blood/induced sputum eosinophil, induced sputum neutrophil, and circulating YKL-40/periostin/neutrophil gelatinase-associated lipocalin (NGAL).
Methods
Searching Strategy
This meta-analysis was reported in accordance with the Meta-analysis of Observational Studies in Epidemiology (MOOSE) (Table S1).11 We systematically retrieved databases of PubMed, EMBASE, Ovid and Web of Science from inception to March 2022, with restrictions of human study and English language only. The search terms were as follows: ((asthma and chronic obstructive pulmonary disease overlap) OR (asthma and COPD overlap) OR (asthma-COPD overlap) OR (ACO and asthma) OR (ACO and COPD)) AND (biomarker OR DLCO OR FeNO OR IgE OR eosinophil OR sputum OR YKL OR periostin OR NGAL). Furthermore, we checked the references of relevant studies to seek out potentially eligible articles. No Ethics approval or patient-informed consent was needed as this meta-analysis was based on the published data.
Study Selection
To date, no global diagnostic standard for ACO was available. In the present study, referring to criteria of ACO from GOLD, GINA and Spanish consensus,3,4,12 the inclusion criteria were as follows: 1. Studies evaluated clinical indicators in differentiating ACO from pure asthma or COPD. 2. Studies were limited to cohort, case-control or cross-sectional. 3. In these studies, ACO patients suffered from persistent airflow limitation (post-bronchodilator FEV1/forced vital capacity (FVC) ratio <0.70) and meet at least one of the following principles: 1) a physician-diagnosed asthma with respiratory symptoms (episodic breathlessness, wheezing, cough, and chest tightness worsening at night or in the early morning), or long-term usage of asthma medications; 2) a self-reported asthma or respiratory symptoms, accompanied by variable expiratory airflow limitation that characterized by an increase of FEV1% pred ≥12% post-bronchodilator, or a diurnal variation in peak expiratory flow (PEF) ≥20%, or a decrease in FEV1% pred ≥15% post-bronchial provocation test; 3) an increase of FEV1 ≥400mL and/or an increase of FEV1% pred ≥15% post-bronchodilator. 4. Appropriate data were available for synthesis and calculation of pooled effect sizes. 5. As for duplicated data, only the most up-to-date were included.
Data Extraction
Two reviewers (JP and MW) independently extracted information from selected studies using a pre-designed excel form. For any inconsistencies, consensus was reached via discussion with a third reviewer (YW). The extracted information included first author, year of publication, sample size, age, sex, body mass index (BMI), smoking history, post-bronchodilator FEV1% pred, DLCO% pred, FeNO, serum total IgE, blood eosinophil counts, percentage of induced sputum eosinophils or neutrophils, circulating YKL-40/periostin/NGAL and study design. Data were combined for meta-analysis only if at least two studies reported the same indicators measured by a similar method. Moreover, if medians and interquartile ranges (IQRs) were offered only in a study, we converted the data into approximate means with standard deviations (SDs) according to the validated statistical method,13,14 and if there were two or more subgroups in a study, we calculated the combined means and SDs according to the Cochrane Handbook guidelines.15
Quality Evaluation
A scale with 11 items offered by the Agency for Healthcare Research and Quality (AHRQ) was applied to evaluate the quality of cross-sectional study.16 If an item of the scale met ‘Yes’, then it got a “1” score, or a “0” if it was “No” or “Unclear”. The total score was divided into three levels: low quality = 0-3, moderate quality = 4–7 and high quality = 8–11. The cohort and case–control studies were assessed by the Newcastle-Ottawa Scale (NOS),16 which contained the aspects of “selection, comparability and exposure” and three levels (low quality = 0–3, moderate quality = 4–6 and high quality = 7–9, respectively).
Statistical Analysis
The meta-analysis was performed by Review Manager (RevMan) Version 5.4 and Stata/MP version 16.0. Due to differences in testing methods of some indicators, the pooled standardized mean differences (SMDs) with 95% confidence intervals (CIs) were calculated, with a p-value <0.05 implying a statistically significant difference, and random-effects models were used to evaluate the pooled effects. Heterogeneity was assessed by the I-squared (I2) test, when I2 >50% indicating substantial heterogeneity, in which case multivariate meta-regression and subgroup analyses by year of publication, total sample size (n <200 or ≥200), study type, and quality score were conducted to explore sources of heterogeneity. The leave-one-out sensitivity analyses were performed to evaluate the stability of the pooled results. Funnel plots as well as begg’s and egger’s tests were adopted to assess publication bias when at least ten studies were included. Since the diagnostic criteria of ACO were not consistent in the included studies, linkage bias analyses based on the different populations in these studies, were conducted to explore the influence of such inconsistency on the pooled results.17
Results
Study Characteristics
A total of 1191 articles were identified, of which 141 articles were reviewed in full text, and 487–10,18–61 eligible studies (35 cross-sectional studies, 10 cohort studies and 3 case–control studies) were finally included (Figure 1). Of the 35 cross-sectional studies, 12 studies were of high quality, and the others were of moderate quality. In the 10 cohort studies, 4 studies were of high quality, and the other 6 studies were of moderate quality. The 3 case–control studies were of moderate quality. Characteristics of the included studies and detailed data of each indicator were listed in Table S2.
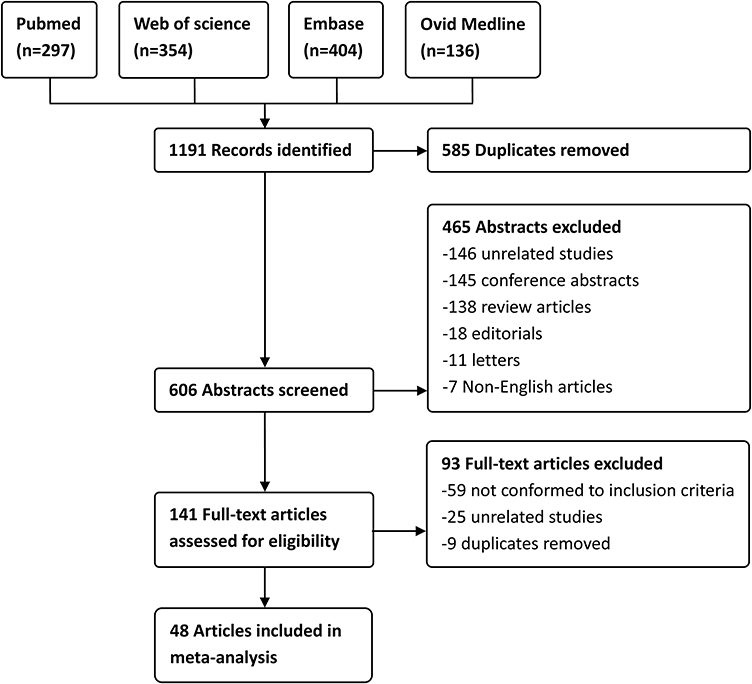 |
Figure 1 Flow chart of study selection and exclusion. |
Indicators
Compared to asthma alone, ACO patients had a higher percentage of induced sputum neutrophil and circulating YKL-40 level, but lower levels of FEV1% pred, DLCO% pred and FeNO. There were no statistical differences between patients with asthma and those with ACO in serum total IgE, blood eosinophil counts, percentage of induced sputum eosinophil or circulating periostin. However, compared to pure COPD, ACO patients had higher levels of FEV1% pred, DLCO% pred, FeNO, serum total IgE, blood eosinophil counts and percentage of induced sputum eosinophil, while lower percentage of induced sputum neutrophil and circulating YKL-40 level. There were no statistical differences between ACO and COPD with respect to circulating periostin or NGAL. Detailed results are summarized in Table 1.
 |
Table 1 Results of Comparisons on Each Indicator Between ACO and Pure Asthma or COPD |
Heterogeneity and Sensitivity
Meta-regression and subgroup analyses did not find out sources of heterogeneity in each indicator (data not shown). However, in the comparison of sputum eosinophils between ACO and pure asthma, the I2 dropped to 0 by excluding the study by Carpagnano et al,20 with no significant change in the pooled results, which could be attributed to the different inclusion criteria in this study. In addition, sensitivity analyses showed that the pooled results of serum total IgE between ACO and pure asthma/COPD were unstable,24,30,31,45,47 and the reasons could be the different allergic history of the subjects and various methods in detecting IgE (Figure S1).
Publication Bias
Visualized funnel plots (Figure S2) and begg’s tests (Table 1) indicated no significant publication bias. However, a publication bias was detected in the egger’s test (Table 1), when comparing the percentage of induced sputum neutrophil between ACO and pure asthma patients, which could be addressed via excluding the study by Carpagnano et al,20 without significant alteration in the pooled results.
Linkage Bias
Only linkage bias analyses with deterministic rules could be achieved due to limited data.17 By the Linkage Structure Classification Tree provided by Doidge et al,17 27 studies with a linkage structure of “nested” and the rest 21 studies with a linkage structure of “imperfect nest” were identified, and both of the linkages showed potential misclassification or measurement error associated with the pooled results (Table S3).
Discussion
In the present study, the percentage of induced sputum neutrophils and circulating YKL-40 level were higher and levels of FEV1% pred, DLCO% pred and FeNO were lower in ACO patients than in pure asthmatic patients, but the opposite was true when compared to patients with COPD alone. In addition, ACO patients had higher levels of serum total IgE, blood eosinophil counts and percentage of induced sputum eosinophils than those with pure COPD.
Airflow limitation in COPD is irreversible and progressive, while conversely, it is usually reversible in asthma. FEV1% pred, as a key indicator of small airway function, is applied in assessing the severity of airflow limitation in COPD and the extent of variation for airflow limitation in asthma.3,12 DLCO% pred is another indicator of lung function, reflecting gas exchange between alveoli and capillaries. Physiologically, carbon monoxide (CO) in lung units will diffuse across the alveolar cell, the basement membrane, the interstitial space, the capillary endothelium, the plasma, and the red blood cell membrane to combine with the hemoglobin.62 This physiological process can be disturbed by small airway remodeling and lung parenchyma destruction in COPD patients, while patients with asthma often preserve CO diffusing capacity, which may be explained by the improved ventilation–perfusion relationships in the apices of lungs.6,62 It was reported that adult smokers with normal DLCO% pred were more likely to be asthmatic, whereas those with low DLCO% pred were more likely to be COPD.63 Our study revealed that FEV1% pred and DLCO% pred in ACO patients were lower than those in patients with pure asthma but higher than in pure COPD.
FeNO, IgE and eosinophil are all biomarkers of Th2 inflammation. Exhaled nitric oxide is synthesized in the airway epithelial cells by inducible nitric oxide synthase (iNOS), which is mainly regulated by Th2 inflammatory molecules like interleukin (IL)-4 and IL-13, and FeNO testing is a noninvasive method that is widely used in the auxiliary diagnosis of asthma.5,23,64 Moreover, IgE is commonly associated with allergic inflammation, and specific IgE for inhaled allergens is a risk factor for asthma.64,65 A cytokine microenvironment consisted of IL-4 and IL-13 is necessary for the maturation of B-lymphocytes and their transformation to specific plasma cells, some of which can synthesize and secrete IgE.65 It was reported that patients with ACO had higher serum total IgE than those with pure COPD characterized by Th1 inflammation.6,66 In addition, eosinophils can be recruited to the lungs in response to stimulation of Th2 inflammatory factors such as IL-3 and IL-5, and promote persistent airway inflammation by releasing various inflammatory factors, among which eosinophil-derived neurotoxins are significantly higher in patients with ACO than those with pure COPD or asthma.64,67 Our study revealed that there were no statistical differences in serum total IgE, blood eosinophil counts and percentage of induced sputum eosinophil between ACO and pure asthma patients, however, patients with asthma alone had a higher FeNO level than those with ACO. When compared with pure COPD, ACO patients had higher levels of FeNO, serum total IgE, blood eosinophil counts and percentage of induced sputum eosinophil, indicating ACO might share more characteristics of Th2 inflammation than COPD.
As a Th1 inflammatory mediator, neutrophils can be identified in patients with COPD as well as in a group of asthmatic patients who express low-Th2 inflammatory cytokines.5,6,68 COPD is mainly associated with smoking, which can stimulate neutrophil production and recruitment to the lungs by some chemokines such as leukotriene-B4 (C-X-C motif) ligand 1 (CXCL1) and CXCL5 that are released by alveolar epithelial cells, macrophages or Th1 lymphocytes, to secrete inflammatory mediators and participate in a series of inflammatory reactions.6,68 Our study showed that patients with ACO had a higher percentage of induced sputum neutrophil than those with pure asthma but lower than those with pure COPD. Further, most of the included studies reported higher pack-years of smoking in patients with ACO than those with pure asthma, suggesting more features of cigarette smoke-associated Th1 inflammation in ACO patients than pure asthma. Moreover, Zhou et al reported more current smokers in patients with pure COPD than those with ACO,69 which implied smoking status could be a potential factor impacting neutrophil counts in patients with ACO and pure asthma/COPD. However, in the present study, due to limited data regarding smoking information, related subgroup analyses were unable to perform.
Moreover, it was reported that patients with both higher levels of circulating YKL-40 and periostin might be possibly diagnosed with ACO,10 and circulating NGAL level in ACO patients was higher than pure asthma and lower than pure COPD.41 Based on the limited data, this meta-analysis revealed circulating YKL-40 level in ACO patients was higher than in pure asthma but lower than COPD alone, and no statistical differences were observed in periostin and NGAL between ACO and pure asthma/COPD.
Although no global diagnostic standard for ACO was available, guidelines of ACO from Finnish, Czech and Spanish incorporated several items from the following indicators: age, tobacco exposure, history of atopy, spirometry, FeNO, serum total IgE, and sputum/blood eosinophilia, but the details varied from each other, leading to possible confusion in recognizing ACO.4 Our study uncovered that, in order to identify ACO, clinicians should pay attention to evaluation of Th2 inflammatory indicators in COPD patients who had some asthmatic features, while assessment of smoking status, FEV1% pred, DLCO% pred and Th1 inflammatory biomarkers in asthma patients with irreversible airflow limitation.
However, some limitations in this study should be considered. First, inconsistent inclusion criteria for ACO patients could lead to potential bias for the pooled results, which could not be well corrected. Second, significant heterogeneity existed in the comparisons, although it was resolved by meta-regression and subgroup analyses. Third, lack of data regarding age, sex, BMI, smoking status, allergic history and disease severity prevented further analyses.
Overall, compared with pure asthma/COPD, ACO patients have different levels of FEV1% pred, DLCO% pred, FeNO, serum total IgE, blood eosinophil, induced sputum eosinophil/neutrophil, and circulating YKL-40, which could be helpful to establish a clinical diagnosis of ACO. Large scale studies are warranted to validate the present findings.
Abbreviations
ACO, asthma-COPD overlap; AHRQ, Agency for Healthcare Research and Quality; BMI, body mass index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; DLCO, diffusion lung capacity for carbon monoxide; FeNO, fractional exhaled nitric oxide; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; I2, I-squared; IgE, Immunoglobulin E; IL, interleukin; IQR, interquartile range; NGAL, neutrophil gelatinase-associated lipocalin; NOS, Newcastle-Ottawa Scale; PEF, peak expiratory flow; SMD, standardized mean difference; SD, standard deviation; Th, T-helper.
Data Sharing Statement
The datasets used and/or analyzed in this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported in part by grant 2016YFC0901100 from the National Key Research and Development Program of China.
Disclosure
The authors declare that they have no competing interests.
References
1. Yanagisawa S, Ichinose M. Definition and diagnosis of asthma-COPD overlap (ACO). Allergol Int. 2018;67(2):172–178. doi:10.1016/j.alit.2018.01.002
2. Hosseini M, Almasi-Hashiani A, Sepidarkish M, Maroufizadeh S. Global prevalence of asthma-COPD overlap (ACO) in the general population: a systematic review and meta-analysis. Respir Res. 2019;20(1):229. doi:10.1186/s12931-019-1198-4
3. Global Initiative for Asthma. Global strategy for asthma management and prevention; 2021. Available from: https://ginasthma.org/wp-content/uploads/2021/05/GINA-Main-Report-2021-V2-WMS.pdf.
4. Nuñez A, Sarasate M, Loeb E, Esquinas C, Miravitlles M, Barrecheguren M. Practical guide to the identification and diagnosis of asthma-COPD overlap (ACO). COPD. 2019;16(1):1–7. doi:10.1080/15412555.2019.1575802
5. Fahy JV. Type 2 inflammation in asthma – present in most, absent in many. Nat Rev Immunol. 2015;15(1):57–65. doi:10.1038/nri3786
6. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011
7. Fu JJ, Gibson PG, Simpson JL, et al. Longitudinal changes in clinical outcomes in older patients with asthma, COPD and asthma-COPD overlap syndrome. Respiration. 2014;87(1):63–74. doi:10.1159/000352053
8. Inoue H, Nagase T, Morita S, et al. Prevalence and characteristics of asthma-COPD overlap syndrome identified by a stepwise approach. Int J Chron Obstruct Pulmon Dis. 2017;12:1803–1810. doi:10.2147/COPD.S133859
9. Kawamatawong T, Charoenniwassakul S, Rerkpattanapipat T. The asthma and chronic obstructive pulmonary disease overlap syndrome in tertiary care setting Thailand. Asia Pac Allergy. 2017;7(4):227–233. doi:10.5415/apallergy.2017.7.4.227
10. Shirai T, Hirai K, Gon Y, et al. Combined assessment of serum periostin and YKL-40 may identify asthma-COPD overlap. J Allergy Clin Immunol Pract. 2019;7(1):134–145.e1. doi:10.1016/j.jaip.2018.06.015
11. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–2012. doi:10.1001/jama.283.15.2008
12. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2021 report); 2020. Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20.
13. Luo D, Wan X, Liu J, et al. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
14. Wan X, Wang W, Liu J, et al. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14(1):135. doi:10.1186/1471-2288-14-135
15. Higgins JPT, Thomas J, Chandler J, et al. Cochrane handbook for systematic reviews of interventions version 6.2 (updated February 2021). Cochrane; 2021. Available from: www.training.cochrane.org/handbook.
16. Rostom A, Dube C, Cranney A, et al.; Celiac Disease. Agency for healthcare research and quality (US). Rockville (MD); 2004. Available from: https://www.ncbi.nlm.nih.gov/books/NBK35156/.
17. Doidge JC, Harron KL. Reflections on modern methods: linkage error bias. Int J Epidemiol. 2019;48(6):2050–2060. doi:10.1093/ije/dyz203
18. Fu JJ, McDonald VM, Gibson PG, et al. Systemic inflammation in older adults with asthma-COPD overlap syndrome. Allergy Asthma Immunol Res. 2014;6(4):316–324. doi:10.4168/aair.2014.6.4.316
19. Lee HY, Kang JY, Yoon HK, et al. Clinical characteristics of asthma combined with COPD feature. Yonsei Med J. 2014;55(4):980–986. doi:10.3349/ymj.2014.55.4.980
20. Carpagnano GE, Lacedonia D, Carone M, et al. Study of mitochondrial DNA alteration in the exhaled breath condensate of patients affected by obstructive lung diseases. J Breath Res. 2016;10(2):026005. doi:10.1088/1752-7155/10/2/026005
21. Cosio BG, Soriano JB, López-Campos JL, et al. Defining the asthma-COPD overlap syndrome in a COPD cohort. Chest. 2016;149(1):45–52. doi:10.1378/chest.15-1055
22. Gao J, Iwamoto H, Koskela J, et al. Characterization of sputum biomarkers for asthma-COPD overlap syndrome. Int J Chron Obstruct Pulmon Dis. 2016;11:2457–2465. doi:10.2147/COPD.S113484
23. Goto T, Camargo CA, Hasegawa K. Fractional exhaled nitric oxide levels in asthma-COPD overlap syndrome: analysis of the National Health and nutrition examination survey, 2007–2012. Int J Chron Obstruct Pulmon Dis. 2016;11:2149–2155. doi:10.2147/COPD.S110879
24. Kalinina EP, Denisenko YK, Vitkina TI, et al. The mechanisms of the regulation of immune response in patients with comorbidity of chronic obstructive pulmonary disease and asthma. Can Respir J. 2016;2016:4503267. doi:10.1155/2016/4503267
25. Bai JW, Mao B, Yang WL, et al. Asthma-COPD overlap syndrome showed more exacerbations however lower mortality than COPD. QJM. 2017;110(7):431–436. doi:10.1093/qjmed/hcx005
26. Gao J, Zhou W, Chen B, et al. Sputum cell count: biomarkers in the differentiation of asthma, COPD and asthma-COPD overlap. Int J Chron Obstruct Pulmon Dis. 2017;12:2703–2710. doi:10.2147/COPD.S142466
27. Kodama Y, Kishimoto Y, Muramatsu Y, et al. Antioxidant nutrients in plasma of Japanese patients with chronic obstructive pulmonary disease, asthma-COPD overlap syndrome and bronchial asthma. Clin Respir J. 2017;11(6):915–924. doi:10.1111/crj.12436
28. Kurashima K, Takaku Y, Ohta C, et al. Smoking history and emphysema in asthma-COPD overlap. Int J Chron Obstruct Pulmon Dis. 2017;12:3523–3532. doi:10.2147/COPD.S149382
29. Lacedonia D, Palladino GP, Foschino-Barbaro MP, et al. Expression profiling of miRNA-145 and miRNA-338 in serum and sputum of patients with COPD, asthma, and asthma-COPD overlap syndrome phenotype. Int J Chron Obstruct Pulmon Dis. 2017;12:1811–1817. doi:10.2147/COPD.S130616
30. Boulet LP, Boulay MÈ, Dérival JL, et al. Asthma-COPD Overlap Phenotypes and Smoking: comparative features of asthma in smoking or non-smoking patients with an incomplete reversibility of airway obstruction. COPD. 2018;15(2):130–138. doi:10.1080/15412555.2017.1395834
31. de Llano LP, Cosío BG, Iglesias A, et al. Mixed Th2 and non-Th2 inflammatory pattern in the asthma-COPD overlap: a network approach. Int J Chron Obstruct Pulmon Dis. 2018;13:591–601. doi:10.2147/COPD.S153694
32. Duong-Quy S, Tran Van H, Vo Thi Kim A, et al. Clinical and functional characteristics of subjects with asthma, COPD, and asthma-COPD overlap: a multicentre study in Vietnam. Can Respir J. 2018;2018:1732946. doi:10.1155/2018/1732946
33. Ekerljung L, Mincheva R, Hagstad S, et al. Prevalence, clinical characteristics and morbidity of the Asthma-COPD overlap in a general population sample. J Asthma. 2018;55(5):461–469. doi:10.1080/02770903.2017.1339799
34. Guo Y, Hong C, Liu Y, et al. Diagnostic value of fractional exhaled nitric oxide for asthma-chronic obstructive pulmonary disease overlap syndrome. Medicine. 2018;97(23):e10857. doi:10.1097/MD.0000000000010857
35. Jo YS, Kwon SO, Kim J, et al. Neutrophil gelatinase-associated lipocalin as a complementary biomarker for the asthma-chronic obstructive pulmonary disease overlap. J Thorac Dis. 2018;10(8):5047–5056. doi:10.21037/jtd.2018.07.86
36. Oh JY, Lee YS, Min KH, et al. Increased urinary l-histidine in patients with asthma-COPD overlap: a pilot study. Int J Chron Obstruct Pulmon Dis. 2018;13:1809–1818. doi:10.2147/COPD.S163189
37. Ojanguren I, Moullec G, Hobeika J, et al. Clinical and inflammatory characteristics of Asthma-COPD overlap in workers with occupational asthma. PLoS One. 2018;13(3):e0193144. doi:10.1371/journal.pone.0193144
38. Park HY, Lee SY, Kang D, et al. Favorable longitudinal change of lung function in patients with asthma-COPD overlap from a COPD cohort. Respir Res. 2018;19(1):36. doi:10.1186/s12931-018-0737-8
39. Shi F, Qiu C, Yu J, et al. Comparison of fractional exhaled nitric oxide in elderly patients with asthma-chronic obstructive pulmonary disease overlap and other airway inflammatory diseases. Iran J Allergy Asthma Immunol. 2018;17(3):232–239.
40. Takayama Y, Ohnishi H, Ogasawara F, et al. Clinical utility of fractional exhaled nitric oxide and blood eosinophils counts in the diagnosis of asthma-COPD overlap. Int J Chron Obstruct Pulmon Dis. 2018;13:2525–2532. doi:10.2147/COPD.S167600
41. Wang J, Lv H, Luo Z, et al. Plasma YKL-40 and NGAL are useful in distinguishing ACO from asthma and COPD. Respir Res. 2018;19(1):47. doi:10.1186/s12931-018-0755-6
42. Cai C, Bian X, Xue M, et al. Eicosanoids metabolized through LOX distinguish asthma-COPD overlap from COPD by metabolomics study. Int J Chron Obstruct Pulmon Dis. 2019;14:1769–1778. doi:10.2147/COPD.S207023
43. Chen FJ, Lin GP, Huang XY, et al. Evaluation of the characteristics of asthma in severe and extremely severe COPD. Int J Chron Obstruct Pulmon Dis. 2019;14:2663–2671. doi:10.2147/COPD.S225258
44. Kyogoku Y, Sugiura H, Ichikawa T, et al. Nitrosative stress in patients with asthma-chronic obstructive pulmonary disease overlap. J Allergy Clin Immunol. 2019;144(4):972–983.e14. doi:10.1016/j.jaci.2019.04.023
45. Park SY, Jung H, Kim JH, et al. Longitudinal analysis to better characterize Asthma-COPD overlap syndrome: findings from an adult asthma cohort in Korea (COREA). Clin Exp Allergy. 2019;49(5):603–614. doi:10.1111/cea.13339
46. Sevimli N, Yapar D, Türktaş H. The prevalence of asthma-COPD overlap (ACO) among patients with asthma. Turk Thorac J. 2019;20(2):97–102. doi:10.5152/TurkThoracJ.2018.18055
47. Backer V, Klein DK, Bodtger U, et al. Clinical characteristics of the BREATHE cohort – a real-life study on patients with asthma and COPD. Eur Clin Respir J. 2020;7(1):1736934. doi:10.1080/20018525.2020.1736934
48. Ding Q, Sun S, Zhang Y, et al. Serum IL-8 and VEGFA are two promising diagnostic biomarkers of asthma-COPD overlap syndrome. Int J Chron Obstruct Pulmon Dis. 2020;15:357–365. doi:10.2147/COPD.S233461
49. Gava G, Núñez A, Esquinas C, et al. Analysis of blood biomarkers in patients with chronic obstructive pulmonary disease (COPD) and with asthma-COPD overlap (ACO). COPD. 2020;17(3):306–310. doi:10.1080/15412555.2020.1761314
50. Ghosh N, Choudhury P, Kaushik SR, et al. Metabolomic fingerprinting and systemic inflammatory profiling of asthma COPD overlap (ACO). Respir Res. 2020;21(1):126. doi:10.1186/s12931-020-01390-4
51. Kang J, Zheng J, Cai B, et al. Current situation of asthma-COPD overlap in Chinese patients older than 40 years with airflow limitation: a multicenter, cross-sectional, non-interventional study. Ther Adv Respir Dis. 2020;14:1753466620961699. doi:10.1177/1753466620961699
52. Kobayashi S, Hanagama M, Ishida M, et al. Clinical characteristics and outcomes of patients with asthma-COPD overlap in Japanese patients with COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:2923–2929. doi:10.2147/COPD.S276314
53. Kubysheva N, Boldina M, Eliseeva T, et al. Relationship of serum levels of IL-17, IL-18, TNF-α, and lung function parameters in patients with COPD, asthma-COPD overlap, and bronchial asthma. Mediators Inflamm. 2020;2020:4652898. doi:10.1155/2020/4652898
54. Li M, Yang T, He R, et al. The value of inflammatory biomarkers in differentiating asthma-COPD overlap from COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:3025–3037. doi:10.2147/COPD.S273422
55. Lim JU, Kim DK, Lee MG, et al. Clinical characteristics and changes of clinical features in patients with asthma-COPD overlap in Korea according to different diagnostic criteria. Tuberc Respir Dis. 2020;83(Supple1):S34–S45. doi:10.4046/trd.2020.0031
56. Queiroz APA, Fonseca FR, Rê A, et al. Clinical, laboratory, and functional characteristics of asthma-COPD overlap in patients with a primary diagnosis of COPD. J Bras Pneumol. 2020;47(1):e20200033. doi:10.36416/1806-3756/e20200033
57. Chen YC, Tsai YH, Wang CC, et al. Epigenome-wide association study on asthma and chronic obstructive pulmonary disease overlap reveals aberrant DNA methylations related to clinical phenotypes. Sci Rep. 2021;11(1):5022. doi:10.1038/s41598-021-83185-1
58. Shi B, Li W, Hao Y, et al. Characteristics of inflammatory phenotypes among patients with asthma: relationships of blood count parameters with sputum cellular phenotypes. Allergy Asthma Clin Immunol. 2021;17(1):47. doi:10.1186/s13223-021-00548-z
59. Toyota H, Sugimoto N, Kobayashi K, et al. Comprehensive analysis of allergen-specific IgE in COPD: mite-specific IgE specifically related to the diagnosis of asthma-COPD overlap. Allergy Asthma Clin Immunol. 2021;17(1):13. doi:10.1186/s13223-021-00514-9
60. Lei J, Yang T, Liang C, et al. Comparison of clinical characteristics and short-term prognoses within hospitalized chronic obstructive pulmonary disease patients comorbid with asthma, bronchiectasis, and their overlaps: findings from the ACURE registry. Front Med. 2022;9:817048. doi:10.3389/fmed.2022.817048
61. Tamura K, Shirai T, Hirai K, et al. Mucus plugs and small airway dysfunction in asthma, COPD, and asthma-COPD overlap. Allergy Asthma Immunol Res. 2022;14(2):196–209. doi:10.4168/aair.2022.14.2.196
62. Hegewald MJ. Diffusing capacity. Clin Rev Allergy Immunol. 2009;37(3):159–166. doi:10.1007/s12016-009-8125-2
63. Enright MP. Office-based DLCO tests help pulmonologists to make important clinical decisions. Respir Investig. 2016;54(5):305–311. doi:10.1016/j.resinv.2016.03.006
64. Fujino N, Sugiura H. ACO (asthma-COPD overlap) is independent from COPD, a case in favor: a systematic review. Diagnostics. 2021;11(5):859. doi:10.3390/diagnostics11050859
65. Novosad J, Krčmová I. Evolution of our view on the IgE molecule role in bronchial asthma and the clinical effect of its modulation by omalizumab: where do we stand today? Int J Immunopathol Pharmacol. 2020;34:2058738420942386. doi:10.1177/2058738420942386
66. Hersh CP, Zacharia S, Chelvan R P, et al. Immunoglobulin E as a biomarker for the overlap of atopic asthma and chronic obstructive pulmonary disease. Chronic Obstr Pulm Dis. 2020;7(1):1–12. doi:10.15326/jcopdf.7.1.2019.0138
67. Tashkin DP, Wechsler ME. Role of eosinophils in airway inflammation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2018;13:335–349. doi:10.2147/COPD.S152291
68. Hammad H, Lambrecht BN. The basic immunology of asthma. Cell. 2021;184(6):1469–1485. doi:10.1016/j.cell.2021.02.016
69. Zhou XL, Zhao LY. Comparison of clinical features and outcomes for asthma-COPD overlap syndrome vs. COPD patients: a systematic review and meta-analysis. Eur Rev Med Pharmacol Sci. 2021;25(3):1495–1510. doi:10.26355/eurrev_202102_24857
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of Vitamin C Supplementation on Chronic Obstructive Pulmonary Disease (COPD): A Systematic Review and Meta-Analysis
Lei T, Lu T, Yu H, Su X, Zhang C, Zhu L, Yang K, Liu J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2201-2216
Published Date: 10 September 2022
Tezepelumab for Patients with Severe Uncontrolled Asthma: A Systematic Review and Meta-Analysis
Zoumot Z, Al Busaidi N, Tashkandi W, Aljohaney AA, Isse S, Vidyasagar K, Ukwaja KN
Journal of Asthma and Allergy 2022, 15:1665-1679
Published Date: 18 November 2022
Advancing Digital Solutions to Overcome Longstanding Barriers in Asthma and COPD Management
Bosnic-Anticevich S, Bakerly ND, Chrystyn H, Hew M, van der Palen J
Patient Preference and Adherence 2023, 17:259-272
Published Date: 28 January 2023
Obstructive Airway Disease is Associated with Increased Cardiovascular Disease Risk Independent of Phenotype: Evidence from Two Nationwide Population-Based Studies
Meng K, Zhang X, Dai H
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1435-1446
Published Date: 12 May 2025
Pharmacist-Driven Outcomes in Asthma and COPD: A Meta-Analysis of Clinical Outcomes and Medication Adherence
Xie W, Zhang X, Wei W, Li N, He X, Shi Z, Wang Y
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:547614
Published Date: 22 April 2026