Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 18
Clinical Characteristics and Malignancy Prevalence in Idiopathic Inflammatory Myopathies: A Single-Center Study from Southwestern Saudi Arabia
Authors AlMalki HH ![]() , Alomair MM
, Alomair MM ![]() , Alkhairi MA, Alahmari FS, Assiri HM
, Alkhairi MA, Alahmari FS, Assiri HM
Received 10 April 2026
Accepted for publication 2 July 2026
Published 15 July 2026 Volume 2026:18 615610
DOI https://doi.org/10.2147/OARRR.S615610
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Chuan-Ju Liu
Hanan H AlMalki,1,2,* Mohammed M Alomair,1,* Muhammed A Alkhairi,1 Fahad S Alahmari,1 Hassan M Assiri1
1Department of Medicine, Rheumatology Unit, Aseer Central Hospital, Abha, Saudi Arabia; 2Department of Medicine, Rheumatology Unit, King Khalid University Medical City, Abha, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Hanan H AlMalki, Department of Medicine, Rheumatology Unit, Aseer Central Hospital, Abha, 62523, Saudi Arabia, Email [email protected]
Purpose: To describe the clinical features of patients with idiopathic inflammatory myopathies (IIM) and report the prevalence of malignancy among them within a single-center cohort in southwestern Saudi Arabia.
Patients and Methods: We conducted a retrospective study at Aseer Central Hospital, reviewing records of patients diagnosed with IIM according to the ACR/EULAR 2017 classification criteria over a five-year period (January 2021–December 2025). Demographic, clinical, laboratory, and treatment data were collected and analyzed using appropriate statistical tests.
Results: Twenty-nine patients were included (75.9% female; mean age 41.9 years). Dermatomyositis (DM, 12/29, 41.4%) predominated, followed by polymyositis (PM, 10/29, 34.5%) and antisynthetase syndrome (ASA, 7/29, 24.1%). Skin manifestations were observed in all DM patients, with isolated involvement in one ASA patient (100% DM vs 0.0% PM vs 14.3% ASA; p < 0.001). Creatine phosphokinase (CPK) was significantly higher in PM and ASA versus DM (medians 4884 and 6334 vs 316 U/L; p = 0.005). Interstitial lung disease (ILD) was most prevalent in ASA (71.4% vs 20.0% PM vs 16.7% DM; p = 0.029). Two females with DM aged ≥ 40 years developed malignancy (ovarian and breast; 2/29, 6.9%). Anti-Jo1 antibodies were present in 7 of 27 tested patients (25.9%), and were significantly associated with ILD (71.4% vs 20.0%, p = 0.023). No malignancy occurred in patients with ILD or anti-Jo1 positivity. Full muscle strength recovery was achieved in 26 of 29 patients (89.7%), though 10 of 29 patients (34.5%) required escalation to intravenous immunoglobulin and/or rituximab for refractory disease.
Conclusion: Malignancy prevalence (2/29 patients, 6.9%) aligns with recent Saudi data but is lower than that reported in East Asian and many Western reports. In this study, cancer occurred exclusively in DM patients aged ≥ 40 years, lacking ILD or anti-Jo1 antibodies, consistent with established risk patterns. These findings support a clinically guided approach to cancer screening, particularly in patients with DM.
Keywords: dermatomyositis, polymyositis, antisynthetase syndrome, risk stratification, interstitial lung disease, anti-Jo1
Introduction
Idiopathic inflammatory myopathies (IIM) represent a heterogeneous group of autoimmune disorders characterized by skeletal muscle inflammation and proximal weakness. The major subtypes include dermatomyositis (DM), polymyositis (PM), inclusion body myositis (IBM), and immune-mediated necrotizing myopathy (IMNM), each with distinct clinical, histopathological, and immunological features.1,2 Their estimated incidence of 2–25 per 100,000 belies the significant morbidity they impose.3
The association between IIM and malignancy has long been recognized; early case series documented concurrent neoplasms in a substantial proportion of DM patients, and this observation has since been validated by large population-based studies and meta-analyses.4 Meta-analyses demonstrate that patients with DM face approximately a five-fold increased cancer risk, while PM confers roughly a 1.6-fold elevation compared to the general population.4 This elevated risk directly informs international cancer screening recommendations and shapes surveillance protocols in clinical practice.5 In this context, cancer-associated myositis is commonly defined as malignancy occurring within three years before or after IIM diagnosis.5
Geographical variation in IIM-associated malignancy is well-documented. Taiwanese cohorts report malignancy rates of approximately 9% in DM and 4% in PM.6 Korean studies document rates exceeding 25%,7 while Asian populations overall demonstrate approximately 10% prevalence.8 Middle Eastern data suggest lower rates, with Jordanian and Omani cohorts reporting 3% and 1.7%, respectively.9,10
Within Saudi Arabia, data remain limited. An early study reported 22.7% malignancy prevalence,11 while a recent Riyadh multicenter analysis documented 6.7%.12 No published data exist from Aseer region in southwestern Saudi Arabia. We aimed to describe the clinical characteristics of patients with IIM followed at our tertiary center and report the prevalence and characteristics of malignancy within this single-center cohort.
Materials and Methods
Study Design and Setting
This retrospective study was conducted at Aseer Central Hospital, a tertiary referral center serving the Aseer region of southwestern Saudi Arabia. The study was approved by the Institutional Review Board of Aseer Central Hospital (IRB-119-2025). The institutional review board waived the requirement for individual informed consent due to the retrospective design. All patient data were anonymized prior to analysis, handled confidentially, and reported in aggregate form without identifying information.
Participants
We identified all patients with a diagnosis of IIM who were diagnosed or followed in the rheumatology clinic from January 2021 to December 2025 through systematic medical record review. All included patients met the probability threshold for probable or definite IIM according to the 2017 American College of Rheumatology and the European Alliance of Associations for Rheumatology (ACR/EULAR) classification criteria.13 We excluded patients with drug-induced myositis, overlap syndromes with other connective tissue diseases, and those with incomplete records that prevented confirmation of IIM diagnosis, subtype classification, malignancy status, or follow-up outcomes.
Data Collection
Using a standardized instrument, we extracted: demographic data (age, sex); IIM subtype [DM, clinically amyopathic dermatomyositis (CADM), PM, ASA, IMNM, and IBM] (no IMNM or IBM cases were identified in our cohort), disease duration; comorbidities; clinical manifestations (myopathy pattern, skin features, dysphagia, ILD, arthritis/arthralgia, Raynaud phenomenon, mechanic hands); muscle strength at presentation and follow-up using Medical Research Council (MRC) scale; laboratory parameters (creatine phosphokinase [CPK], transaminases, lactate dehydrogenase, inflammatory markers); available serological data, including antinuclear antibody (ANA) and anti-Jo1 antibody; anti-Mi2 was recorded when available, while extended myositis-specific antibody testing was not routinely available during the study period; imaging findings; treatment modalities; and malignancy status including type and temporal relationship to IIM diagnosis. Baseline was defined as the time of IIM diagnosis or the earliest available IIM-related rheumatology evaluation. Follow-up data were obtained from the most recent documented rheumatology visit.
Definitions
The diagnosis of ASA was established based on the classification criteria by Connors et al and the preliminary criteria proposed by the CLASS Project; using available clinical, radiological, and serological data;14,15 CADM was defined according to Sontheimer standalone criteria as the presence of DM cutaneous manifestations in the absence of objective muscle weakness, with normal muscle enzymes and/or muscle studies for a minimum of six months;16 and juvenile-onset dermatomyositis (JDM) was defined according to the 2017 ACR/EULAR classification criteria as dermatomyositis with onset before 18 years.13
Cancer-associated myositis was defined as malignancy diagnosed within three years before or after IIM diagnosis, consistent with international consensus.5 Malignancy screening and follow-up investigations were performed as part of routine clinical care and were extracted from the medical records. ILD was identified by characteristic findings on high-resolution computed tomography, based on formal radiology reports interpreted by radiologists. The ILD pattern was recorded when specified in the radiology report, predominantly as a non-specific interstitial pneumonia pattern. Refractory disease was defined as persistent or worsening muscle weakness, persistently elevated muscle enzymes, active extramuscular disease, or inability to taper glucocorticoids despite conventional immunosuppressive therapy, necessitating escalation to intravenous immunoglobulin (IVIG) or rituximab.
Statistical Analysis
Analysis was performed using Python 3.x with SciPy and Pandas libraries. Normality was assessed using the Shapiro–Wilk test. Normally distributed continuous variables were expressed as mean ± standard deviation; non-normally distributed variables were expressed as median with interquartile range (IQR). Categorical variables were presented as frequencies and percentages. For two-group comparisons (eg, antibody subgroups), Fisher’s exact test was used for categorical variables and the Mann–Whitney U-test for continuous variables. For three-group IIM subtype comparisons, the Kruskal–Wallis test was used for continuous variables and Chi-square or Fisher’s exact test for categorical variables, with Bonferroni correction applied for post-hoc pairwise testing. Serological percentages were calculated using the number of patients tested as the denominator, excluding those without serological workup. Subgroup analyses compared IIM subtypes, age groups (< 40 versus ≥ 40 years), and antibody status. Malignancy prevalence was calculated as the number of patients with malignancy divided by the total number of included IIM patients. Given the small sample size, subgroup comparisons and correlation analyses were considered exploratory; correlations were performed using Spearman’s rank correlation coefficient (rs).
Results
Patient Characteristics
A total of 37 documented IIM records were screened through rheumatology clinic medical records. Eight records were excluded because of incomplete data or overlap syndromes with other connective tissue diseases. The final study population included 29 patients who met the inclusion criteria. Females predominated (n = 22, 75.9%), with a female-to-male ratio of 3.1:1. Mean age at diagnosis was 41.9 ± 11.8 years (range 21–66), and 17 patients (58.6%) were aged 40 years or older. Median disease duration was 3.0 years (IQR 2.0–9.0). DM spectrum disorders were most common (41.4%) followed by polymyositis (34.5%) and antisynthetase syndrome (24.1%). Demographic characteristics are summarized in Table 1.
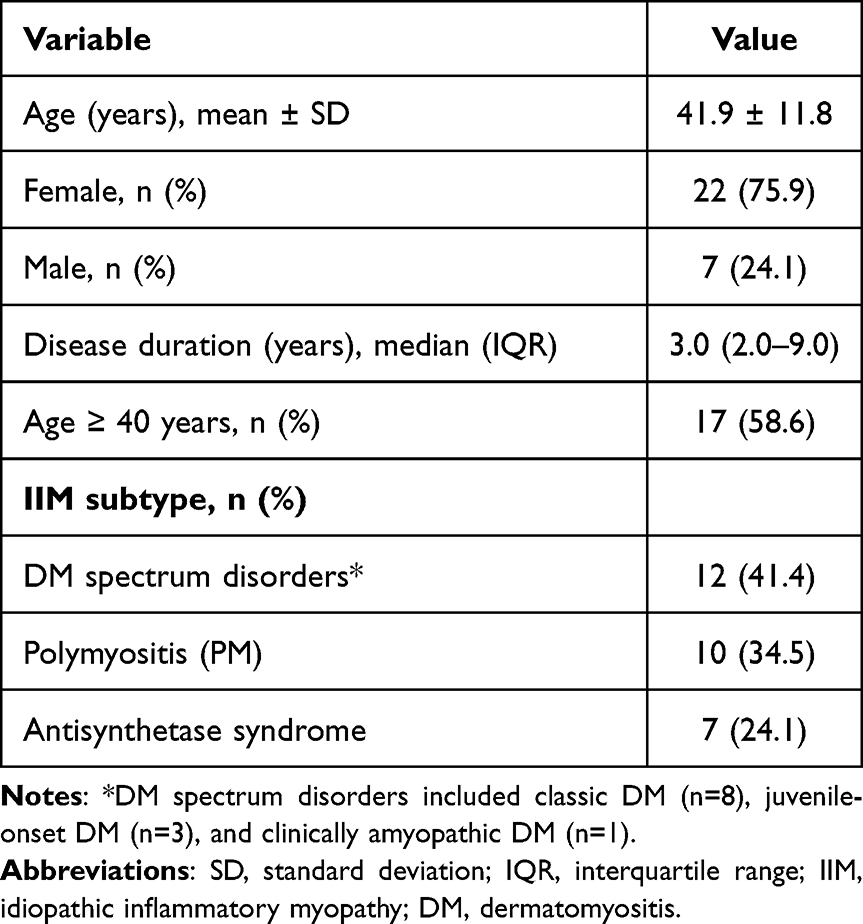 |
Table 1 Patient Demographics and Baseline Characteristics |
Clinical Manifestations
Proximal muscle weakness was present in 28 patients (96.6%). Dysphagia occurred in 8/29 patients, 27.6%. Skin manifestations were present in 13 of 29 patients (44.8%). Extramuscular features included arthritis/arthralgia (16/19, 55.2%), constitutional symptoms (11/29, 37.9%), ILD (9/29, 31.0%), and mechanic hands (5/29, 17.2%).
By subtype, skin manifestations were observed in all DM patients, with only isolated involvement in one ASA patient (p < 0.001). Dysphagia occurred more frequently in ASA (4/7, 57.1%) and DM (4/12, 33.3%) compared with PM (0/10, 0%; p = 0.029). Mechanic hands were most prevalent in ASA (3/7, 42.9% versus 2/12, 16.7% in DM and 0/10, 0% in PM). At the last follow-up, 26 patients (89.7%) had achieved full muscle strength recovery (MRC grade 5), with the DM group having the highest numerical rate of full recovery.
Clinical features by subtype are detailed in Table 2.
 |
Table 2 Clinical Features at Presentation |
Laboratory Findings
Median baseline CPK was markedly elevated at 2444 U/L (IQR 719–6334), decreasing to 80 U/L (IQR 42–221) at follow-up. AST decreased from 128 (IQR 82–322) to 26 (IQR 21–37) U/L, ALT from 111 (IQR 46–270) to 23 (IQR 16–40) U/L, and LDH from 589 (IQR 439–940) to 202 (IQR 169–261) U/L. Laboratory data are presented in Figure 1.
 |
Figure 1 Laboratory parameters at baseline and follow-up. (A) Creatine phosphokinase. (B) Aspartate aminotransferase. (C) Alanine aminotransferase. (D) Lactate dehydrogenase. Dashed horizontal lines indicate the upper limit of normal. |
Serological Profile
ANA was positive in 15 of 27 tested patients (55.6%), testing was not available for 2 patients. Anti-Jo1 antibody was detected in 7 of 27 tested patients (25.9%), while anti-Mi2 was positive in only one (3.7%). Anti-Jo1 positivity demonstrated a statistically significant association with ILD (5/7, 71.4% in anti-Jo1-positive versus 4/20, 20.0% in anti-Jo1-negative patients; p = 0.023). Mechanic hands were more frequently observed in anti-Jo1-positive patients (3/7, 42.9% versus 2/20, 10.0%), though this did not reach statistical significance (p = 0.091). No malignancy occurred in anti-Jo1-positive patients. Serological data are shown in Figure 2.
 |
Figure 2 Serological profile and HRCT chest findings. (A) Serological profile among patients with available serological testing (n=27). (B) HRCT chest findings (n=29). |
IIM Subtype Comparison
Comparison between DM spectrum, PM, and ASA revealed notable subtype differences (Table 3). Age and sex distribution were similar across groups. Baseline CPK levels differed significantly across the three groups (Kruskal–Wallis p = 0.005). Specifically, post-hoc pairwise comparisons revealed that DM patients had significantly lower median CPK levels compared to PM and ASA patients (p = 0.006 and p = 0.024, respectively). In contrast, CPK levels in PM and ASA patients were statistically comparable (p = 1.000). Regarding extra-muscular manifestations, ILD prevalence also varied significantly (p = 0.029), occurring most frequently in the ASA group (5/7, 71.4%) compared to the DM group (2/12, 16.7%; p = 0.045). Mean MRC grade improvement was numerically higher in PM patients. Malignancy occurred exclusively in DM patients.
 |
Table 3 Comparison of IIM Subtype |
Treatment and Outcomes
All patients received corticosteroids, with three patients (10.3%) receiving pulse therapy followed by tapering, while the remaining patients received 0.5–1 mg/kg/day with tapering. Currently, seven patients (24%) are on low-dose corticosteroids (2.5–5 mg/day). Steroid-sparing agents included azathioprine (16/29, 55.2%), methotrexate (15/29, 51.7%), and mycophenolate mofetil (9/29, 31.0%). Ten patients (34.5%) had refractory disease requiring escalation to intravenous immunoglobulin (IVIG) and/or rituximab. Functional outcomes were favorable: 28 patients (96.6%) showed clinical improvement, while 26 patients (89.7%) achieved full recovery, defined as MRC grade 5. Treatment data are shown in Figure 3.
 |
Figure 3 Treatment modalities and clinical outcomes. (A) Treatment modalities used during follow-up. (B) Muscle power distribution at baseline and follow-up using the Medical Research Council scale. (C) Functional outcome at last follow-up. (D) Treatment response. |
Correlation Analysis of Clinical and Laboratory Parameters
Correlations between clinical and laboratory parameters are illustrated in Figure 4. The strongest positive correlation among laboratory parameters was found between ESR and CRP (rs = 0.49), reflecting their shared role as inflammatory markers. There was a moderate negative correlation (rs = −0.46) between baseline CPK levels and muscle power, indicating that higher muscle damage markers were associated with reduced muscle strength. Age was positively correlated with disease duration (rs = 0.41), indicating that older patients in this cohort tended to have longer disease duration. Additionally, age was found to have a weak-to-moderate negative correlation (rs = −0.31) with follow-up muscle power, suggesting a trend toward less complete strength recovery in older individuals.
 |
Figure 4 Spearman correlation matrix of clinical and laboratory parameters. Correlation coefficients are shown within each cell; positive correlations are shown in red and negative correlations in blue. |
Malignancy
Malignancy was identified in 2 of 29 patients (6.9%). Both were females with dermatomyositis aged 42 and 50 years, presenting with ovarian and breast cancer, respectively. Both had Gottron papules but lacked ILD and anti-Jo1 positivity. No malignancy cases were observed in the PM or ASA subgroups. Case details are summarized in Table 4. International comparison data are presented in Table 5.
 |
Table 4 Characteristics of Patients with Malignancy-Associated Myositis |
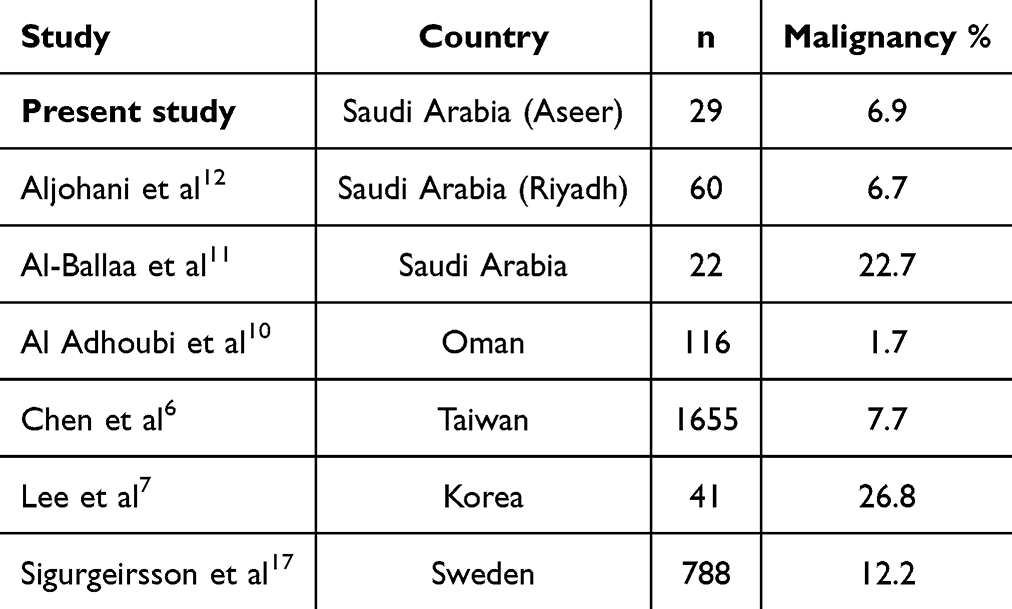 |
Table 5 International Comparison of Malignancy Rates in IIM |
Discussion
This study is, to our knowledge, the first report on IIM patients from Aseer region of Saudi Arabia, and one of the first in the Kingdom to systematically characterize three distinct IIM subgroups — DM, PM, and ASA — with subtype-specific clinical and laboratory profiles. The 6.9% malignancy prevalence is comparable to the recent Riyadh multicenter study (6.7%)12 but is substantially lower than the earlier Saudi report (22.7%)11 and East Asian studies (10–27%).6–8,18,19 This finding, along with recent Saudi data, contributes to a regional description of IIM-associated malignancy in Saudi Arabia. The observed differences from earlier Saudi and international reports may reflect evolving diagnostic criteria, different patient populations, screening practices, or genuine epidemiological variation.
Regional patterns are notable. Neighboring Middle Eastern countries also report low rates: Jordan 3.3%9 and Oman 1.7%.10 East Asian populations report higher figures, reaching 26.8% in Korean studies.7,19 Western countries report intermediate rates of 10–15%.17,20 The underlying drivers of this heterogeneity likely include genetic susceptibility, HLA allele frequency differences, environmental factors, and variation in cancer screening practices across health systems.
Cancer types also vary geographically. Nasopharyngeal carcinoma predominates in East Asia, particularly Taiwan,6,18 while our patients developed gynecological malignancies (ovarian and breast cancer) mirroring the common cancer types seen in Saudi women.21 This may suggest IIM-associated cancers partly reflect local cancer burden rather than universal specific tumor-myositis associations, at least in our cohort.
The distinctiveness of ASA as a separate entity from classic DM and PM in our regional cohort supports its recognition as a standalone IIM subtype, as reflected in contemporary classification criteria.14,15 DM, by contrast, was characterized by near-universal skin involvement (100%) with Gottron papules in 83.3% and heliotrope rash in 41.7% — findings highly significant across subtypes (p < 0.001) and clinically valuable for early subtype identification at bedside.
Our cancer patients matched established risk patterns:22,23 both had DM rather than PM or ASA, both were over 40, and neither had ILD or anti-Jo1 antibodies. Notably, the zero malignancy rate in our ASA group is consistent with published data showing anti-Jo1 positivity and ILD as protective factors against cancer-associated myositis.3,4 In our cohort, the significant association between anti-Jo1 positivity and ILD (p = 0.023) further supports the distinctness of the antisynthetase phenotype from cancer-associated myositis.13,15 Together, these observations are consistent with the clinical distinction between antisynthetase syndrome and cancer-associated dermatomyositis reported in previous studies.3,5,16 The unavailability of anti-TIF1γ testing, which carries the strongest malignancy association, represents an important limitation.
Published meta-analyses identify DM subtype, older age, male sex, dysphagia, cutaneous ulceration, and anti-TIF1γ positivity as independent malignancy risk factors, while ILD and anti-Jo1 positivity carry a protective effect.22,23 Our findings are broadly consistent with this risk profile. However, because only two malignancy cases were observed and anti-TIF1γ testing was not available, our study cannot determine independent predictors of malignancy. Further larger regional studies are needed to inform locally relevant cancer screening recommendations for patients with IIM.
Treatment responses in our cohort were encouraging, with 96.6% of patients showing improvement and 89.7% achieving full muscle strength recovery. However, 34.5% required escalation to IVIG and/or rituximab, reflecting the refractory nature of IIM in a substantial proportion of patients. Better functional recovery in PM and ASA patients despite substantially higher baseline CPK (median 4884 and 6334 U/L versus 316 U/L in DM) suggests possible different treatment responsiveness between subtypes, though this requires confirmation in larger cohorts.
Study limitations include the retrospective single-center design, small sample size limiting statistical power for subgroup analyses and detection of treatment–subtype differences, incomplete myositis-specific antibody panel and missing baseline laboratory data in some patients — particularly DM cases, as reflected by unexpectedly low CPK levels. In our center, ANA and anti-Jo1 testing were routinely available, while anti-Mi2 was recorded when available. Other myositis-specific antibodies (anti-TIF1γ, anti-MDA5, anti-NXP2, anti-SAE, anti-HMGCR, anti-SRP) could not be tested. Variable follow-up duration may have missed late-onset malignancies. Despite these limitations, this study provides the first IIM data from the Aseer region and adds to the growing body of Middle Eastern literature.
Conclusion
This study of 29 IIM patients from the Aseer region documents a malignancy prevalence of 2/29 patients (6.9%), consistent with recent Saudi data but lower than East Asian reports. Three clinically distinct subgroups were identified: DM was characterized by skin involvement and all malignancies occurred in DM; ASA was characterized by high ILD prevalence (5/7, 71.4%) and significantly elevated CPK with no observed malignancy; and PM exhibited intermediate features with numerically greatest functional recovery. Cancer-associated myositis occurred exclusively in DM patients over 40 years of age without ILD or anti-Jo1 positivity, consistent with previously reported risk patterns. These findings support consideration of disease subtype when planning cancer screening, especially in patients with dermatomyositis. However, the small ASA sample size and the lack of anti-TIF1γ testing limit conclusions regarding subtype-specific malignancy risk. Larger prospective cohorts with comprehensive myositis-specific antibody panels are needed to further characterize IIM in the Arabian Peninsula and to inform locally relevant cancer screening recommendations.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of Aseer Central Hospital (IRB-119-2025). The requirement for individual informed consent was waived due to the retrospective nature of the study. All methods were performed in accordance with the Declaration of Helsinki.
Consent for Publication
Not applicable. This manuscript does not contain any individual person’s data in any form.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Bohan A, Peter JB. Polymyositis and dermatomyositis (first of two parts). N Engl J Med. 1975;292(7):344–11. doi:10.1056/NEJM197502132920706
2. Bohan A, Peter JB. Polymyositis and dermatomyositis (second of two parts). N Engl J Med. 1975;292(8):403–407. doi:10.1056/NEJM197502202920807
3. Oldroyd A, Lilleker J, Chinoy H. Idiopathic inflammatory myopathies - a guide to subtypes, diagnostic approach and treatment. Clin Med Lond. 2017;17(4):322–328. doi:10.7861/clinmedicine.17-4-322
4. Yang Z, Lin F, Qin B, Liang Y, Zhong R. Polymyositis/dermatomyositis and malignancy risk: a metaanalysis study. J Rheumatol. 2015;42(2):282–291. doi:10.3899/jrheum.140566
5. Oldroyd AGS, Callen JP, Chinoy H, et al. International guideline for idiopathic inflammatory myopathy-associated cancer screening: an international myositis assessment and clinical studies group (IMACS) initiative. Nat Rev Rheumatol. 2023;19:805–817. doi:10.1038/s41584-023-01045-w
6. Chen YJ, Wu CY, Huang YL, Wang CB, Shen JL, Chang YT. Cancer risks of dermatomyositis and polymyositis: a nationwide cohort study in Taiwan. Arthritis Res Ther. 2010;12(1):R70. doi:10.1186/ar2987
7. Lee SW, Jung SY, Park MC, Park YB, Lee SK. Malignancies in Korean patients with inflammatory myopathy. Yonsei Med J. 2006;47(4):519–523. doi:10.3349/ymj.2006.47.4.519
8. Ungprasert P, Leeaphorn N, Hosiriluck N, Chaiwatcharayut W, Ammannagari N, Jirasiritham S. Clinical features of inflammatory myopathies and their association with malignancy: a systematic review in Asian population. ISRN Rheumatol. 2013;2013:509354. doi:10.1155/2013/509354
9. Mustafa KN, Dahbour SS, Ghanma IM. Clinical characteristics and outcomes of patients with idiopathic inflammatory myopathies from Jordan 1996-2009. Clin Rheumatol. 2010;29(12):1381–1385. doi:10.1007/s10067-010-1465-8
10. Al Adhoubi NK, Al Falahi Z, Al Rashdi S, Al Balushi F, Al-Riyami AM. Prevalence, epidemiological characteristics and survival rates of idiopathic inflammatory myopathies in Oman. Clin Exp Rheumatol. 2024;42(2):398–406. doi:10.55563/clinexprheumatol/o78ssl
11. Al-Ballaa ST, Al-Dalaan AN, El-Ramahi KM, Al-Janadi MA, Al-Shaikh A, Bahabri S. Pattern of adult onset of polymyositis and dermatomyositis and association with malignancy. Ann Saudi Med. 1993;13(5):525–529. doi:10.5144/0256-4947.1993.525
12. Aljohani G, Bin Awad EA, Alshahrani K, Alshalhoub R, Almoallim H. Prevalence, clinical features, predictive factors and investigations to screen for cancer in patients with inflammatory myositis. Saudi Med J. 2021;42(1):100–104. doi:10.15537/smj.2021.1.25590
13. Lundberg IE, Tjärnlund A, Bottai M, et al. 2017 European League Against Rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups. Ann Rheum Dis. 2017;76(12):1955–1964. doi:10.1136/annrheumdis-2017-211468
14. Connors GR, Christopher-Stine L, Oddis CV, Danoff SK. Interstitial lung disease associated with the idiopathic inflammatory myopathies: what progress has been made in the past 35 years? Chest. 2010;138(6):1464–1474. doi:10.1378/chest.10-0180
15. Zanframundo G, Connors GR, Christopher-Stine L, et al. The classification criteria for anti-synthetase syndrome (CLASS project). Arthritis Rheumatol. 2024;76(Suppl 9):1.
16. Sontheimer RD. Dermatomyositis: an overview of recent progress with emphasis on dermatologic aspects. Dermatol Clin. 2002;20(3):387–408. doi:10.1016/S0733-8635(02)00021-9
17. Sigurgeirsson B, Lindelöf B, Edhag O, Allander E. Risk of cancer in patients with dermatomyositis or polymyositis. N Engl J Med. 1992;326(6):363–367. doi:10.1056/NEJM199202063260602
18. Hsu JL, Liao MF, Chu CC, et al. Reappraisal of the incidence, various types and risk factors of malignancies in patients with dermatomyositis and polymyositis in Taiwan. Sci Rep. 2021;11(1):4545. doi:10.1038/s41598-021-83729-5
19. So MW, Koo BS, Kim YG, Lee CK, Yoo B. Idiopathic inflammatory myopathy associated with malignancy: a retrospective cohort of 151 Korean patients with dermatomyositis and polymyositis. J Rheumatol. 2011;38(11):2432–2435. doi:10.3899/jrheum.110320
20. Buchbinder R, Forbes A, Hall S, Dennett X, Giles G. Incidence of malignant disease in biopsy-proven inflammatory myopathy. Ann Intern Med. 2001;134(12):1087–1095. doi:10.7326/0003-4819-134-12-200106190-00008
21. Saudi Cancer Registry. Cancer Incidence Report 2022. Riyadh: National Cancer Center, Saudi Health Council; 2024. Available from: https://shc.gov.sa/Arabic/NewNCC/Activities/AnnualReports/Cancer%20Incidence%20Report%202022.pdf.
22. Oldroyd AGS, Lilleker JB, Amin T, et al. Systematic review and meta-analysis to inform cancer screening guidelines in idiopathic inflammatory myopathies. Rheumatology. 2021;60(6):2615–2628. doi:10.1093/rheumatology/keab166
23. Lu X, Yang H, Shu X, et al. Factors predicting malignancy in patients with polymyositis and dermatomyositis: a systematic review and meta-analysis. PLoS One. 2014;9(4):e94128. doi:10.1371/journal.pone.0094128
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors and Predictive Model for Dermatomyositis Associated with Rapidly Progressive Interstitial Lung Disease
Wang K, Tian Y, Liu S, Zhang Z, Shen L, Meng D, Li J
Pharmacogenomics and Personalized Medicine 2022, 15:775-783
Published Date: 1 September 2022
Clinical Characteristics and Associated Factors for Infection and in-Hospital Mortality in Inpatients with Polymyositis/Dermatomyositis in China: A Retrospective Study
Lao M, Ouyang H, Li N, Li H, Dai P, Zhan Z, Chen D
Infection and Drug Resistance 2023, 16:289-299
Published Date: 17 January 2023
Immune-Related Genes Associated with Interstitial Lung Disease in Dermatomyositis
Liu C, Ge Y
International Journal of General Medicine 2024, 17:5261-5271
Published Date: 14 November 2024
Clinical Significance of Abnormal Serum LGALS3BP Expression in Patients with Idiopathic Inflammatory Myopathies
Huang L, Huang X, Zhou W, Jiang Y, Zhu H, Lao Y, Deng Z, Tang Y, Wang J, Li X
Journal of Inflammation Research 2024, 17:9697-9710
Published Date: 25 November 2024
Clinical Features and Prognosis of Double-Positive Anti-MDA5 and Anti-CCP Antibodies in Dermatomyositis: A Retrospective Study
Xu X, Zhu L, Li S, Wang G, Ge Y
Journal of Inflammation Research 2025, 18:1929-1939
Published Date: 10 February 2025