Back to Journals » Risk Management and Healthcare Policy » Volume 19
Chronic Disease Prevalence and Modifiable Risk Factors Among Undergraduate Students at Ha’il University: A Population-Level Cross-Sectional Study
Authors Asweto CO, Hassan SUN ![]() , Alzain MA, Alsaif B
, Alzain MA, Alsaif B ![]() , Saeed ME, Kassar A, Mohammed Ali KE, Ghorbel M, Zrieq R
, Saeed ME, Kassar A, Mohammed Ali KE, Ghorbel M, Zrieq R ![]() , Hamed M
, Hamed M ![]() , Wang W
, Wang W ![]()
Received 18 February 2026
Accepted for publication 2 May 2026
Published 20 May 2026 Volume 2026:19 604127
DOI https://doi.org/10.2147/RMHP.S604127
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Gulsum Kaya
Collins Otieno Asweto,1,* Sehar-un-Nisa Hassan,2,* Mohamed Ali Alzain,2,3,* Bandar Alsaif,2 Mohammed Elshiekh Saeed,4,5 Ahmed Kassar,2 Kamal Elbssir Mohammed Ali,6 Mouna Ghorbel,7 Rafat Zrieq,8,9 Monzer Hamed,2 Wei Wang10,11
1Department of Community Health, School of Nursing, University of Embu, Embu, Kenya; 2Department of Public Health, College of Public Health and Health Informatics, University of Ha’il, Ha’il, Saudi Arabia; 3Department of Community Medicine, Faculty of Medicine and Health Sciences, University of Dongola, Dongola, Sudan; 4Department of Physiology, Faculty of Medicine, National University-Sudan, Khartoum, Sudan; 5Department of Physiology, Faculty of Medicine, University of Dongola, Dongola, Sudan; 6Department of Community Health, Occupation Health and Safety Program, Northern Border University, Arar, Saudi Arabia; 7Department of Biology, College of Sciences, University of Ha’il, Ha’il, Saudi Arabia; 8Medical-Surgical Nursing Department, College of Nursing, University of Ha’il, Ha’il, Saudi Arabia; 9Applied Science Research Centre, Applied Science Private University, Amman, Jordan; 10Clinical Research Centre, First Affiliated Hospital, Shantou University Medical College, Shantou, Guangdong, People’s Republic of China; 11Centre for Precision Health, Edith Cowan University, Joondalup, Western Australia, Australia
*These authors contributed equally to this work
Correspondence: Sehar-un-Nisa Hassan, Department of Public Health, College of Public Health and Health Informatics, University of Ha’il, Ha’il, Saudi Arabia, Email [email protected]
Background: Rising rates of chronic conditions among Saudi youth underscore the need for early prevention. Using a public‑health lens focused on demographic, academic, and lifestyle influences, this study investigates the risk and protective factors for chronic disease among students at the University of Ha’il to guide youth‑centered health policies and long‑term wellbeing initiatives.
Methods: A cross-sectional survey was conducted among 10,775 undergraduate students studying in bachelor’s degree programs at Ha’il University, Saudi Arabia. Descriptive analyses were used to assess demographic characteristics, academic status, health status, and health-related lifestyles. Multiple logistic regression models were applied to determine which demographic, academic, and health-related lifestyle factors significantly predicted chronic disease among university students.
Results: The overall prevalence of chronic diseases was 16.2% (n = 1748). Among chronic diseases, diabetes was the most prevalent 6.8% (n = 731), followed by migraines 5.4% (n = 583), heart disease 2.0% (n = 217), hypercholesterolemia 1.9% (n=201), and others 0.1% (n = 16). The results showed that younger, female, and married students had greater odds of developing chronic disease. Among the study-related variables, academic level, Grade Percentage Average (GPA), missed lectures, and intention to withdraw were significantly associated with chronic diseases. Among psychological variables, high stress levels significantly increased the odds of having chronic disease [AOR = 9.87 (95% CI: 8.01– 11.34), p < 0.001]. Students with unhealthy lifestyles were more likely to have chronic diseases than those with a healthy lifestyle [AOR = 2.60 (95% CI: 2.33– 2.90), p < 0.001].
Conclusion: The 16.2% prevalence of chronic health conditions among university students is a notable public health concern within this typically healthy population. Demographic and academic vulnerabilities were further intensified by modifiable lifestyle behaviors which showed strong associations with chronic disease prevalence thus findings imply prioritizing student health through culturally grounded interventions.
Keywords: health status, sleep, physical activity, academic stress, vulnerability
Introduction
Youth health is an important factor in determining a country’s progress in socioeconomic development indicators, and those suffering from chronic disease at this age may develop multiple physical and mental health impairments at a later age. Public health experts foresee that chronic diseases among young populations are among the emerging most serious public health challenges. Approximately 10–30% of youth globally are already living with chronic medical conditions and are at heightened risk for long-term negative health outcomes. They argue that current prevention approaches are insufficient.1,2 Chronic disease prevalence among university students in Saudi Arabia and other Arab countries a critical public health concern, given its potential to disrupt developmental trajectories and heighten disability risk in adulthood.3 While global public health frameworks, including the World Health Organization (WHO), define youth as individuals aged 10–24 years,4 this boundary is not universal. In Saudi Arabia, undergraduate students commonly fall within the 18–30‑year range due to later university entry, preparatory programs, and extended academic pathways. Developmentally, many individuals in this age group continue to experience transitional characteristics associated with youth, such as incomplete economic independence and evolving health behaviors. Therefore, for the purposes of this study, youth has been conceptually defined as university‑enrolled young people aged 18–30 years, reflecting both the local demographic reality and the extended period of psychosocial transition relevant to chronic disease risk.
Premature death caused by Non-Communicable Diseases (NCDs) in several Arab countries is as high as 20%.5 A research report based on the 2018 Saudi Arabian household survey demonstrated a high prevalence of chronic diseases at the national and regional levels in adult populations and has warned about the negative implications of chronic disease on well-being and quality of life in Saudi Arabia.6 Most of the previously published literature from Saudi Arabia reported the rates of prevalence and mortality associated with chronic diseases in older populations.6,7 Currently, there is limited empirical evidence available on adolescent population, that demonstrate an increase in the occurrence of various chronic diseases such as (hypertension, diabetes, asthma, and arthritis) among youth in Arab countries.8 One recent study from Saudi Arabia reported a 12% cumulative rate of obesity, asthma, anxiety, and conduct disorders among Saudi adolescents.9 A systematic review based on 21 observational studies from the Northern Borders Province (NBP) in Saudi Arabia reported that the total prevalence of chronic health problems among people in this region is up to 61%.10 Few studies that were included in this systematic review focused on the mental and behavioral health of male and female adolescents. The prevalence of obesity among male teenagers was 30% and approximately 56% screened positive for depression and anxiety symptoms. The rate of eating disorders among the female adolescents was 25.5%. This systematic review pointed towards the existing gap in the empirical literature that restricts the calculation of accurate estimates of the prevalence of various other chronic diseases among subpopulations in Saudi Arabia.
In the past decade, Saudi population as a whole and particularly, young adults rapidly adopted the unhealthy life habits of modern cultures such as increased consumption of fast food, intake of processed food items, more engagement in online activities.11 Teenagers avail restricted opportunities of mobility in daily life activities due to the non-preference for use of stairs and walkways and frequent use of various types of vehicles even for shorter distances.12 Moreover, traditional dietary practices in Saudi Arabia continue to include ceremonial foods and culturally acceptable food items are often high in sugars, refined carbohydrates, and salted baked items.13 The persistence of these energy‑dense, nutrient‑poor eating patterns that are combined with broader lifestyle risk factors actually contributes substantially to the rising burden of NCDs such as hypertension and risk for other cardiovascular diseases in youth.14 One of our own previous research found that unhealthy behaviors of young students significantly predicted sub-optimal health.15
Academic environments play a significant role in shaping youth health, with growing evidence linking academic pressures, performance demands, and school engagement to chronic disease risk. Theoretically, the biopsychosocial model suggests that academic stressors such as heavy workloads, competitive grading, and limited time for physical activity can trigger physiological stress responses that contribute to long‑term metabolic, cardiovascular, and mental health vulnerabilities.16 Empirically, research shows that students with chronic health conditions often face academic challenges, including frequent absences and reduced academic performance, which can reinforce stress and unhealthy coping behaviors. One study finding demonstrated that chronic illnesses like asthma are strongly associated with increased school absenteeism, which in turn affects academic success and may exacerbate stress‑related health risks.17
Further evidence indicates that multiple behavioral risk factors (MBRFs) such as physical inactivity, poor diet, smoking, and risky alcohol use are associated with poorer academic performance among university students. A large study of medical students found that clustering of these risk factors was inversely associated with academic achievement, with students exhibiting three or more risk behaviors earning significantly lower grades and distinctions.18 This suggests a bidirectional relationship as academic pressures may contribute to unhealthy behaviors, while these behaviors further impair academic performance and elevate chronic disease risk.
Additionally, young people with chronic conditions often engage in risky behaviors at rates similar to or higher than their healthy peers, compounding their vulnerability. This highlights the importance of analyzing the independent and cumulative impact of various factors such as demographic, academic variables and lifestyles in the development of chronic health conditions in youth.
The high prevalence of suboptimal health and NCDs among youth may threaten progress towards the 2030 Agenda for Sustainable Development in Saudi Arabia, which includes the target of reducing premature deaths from NCDs by one-third by 2030. This may also hinder the achievement of one of the goals of Saudi Vision 2030: to increase life expectancy from 75 to 80 by 2030. People with chronic health conditions experience poor financial health and squeeze valuable household and government budgets and resources spent on healthcare. The long-term negative impact of chronic diseases on youth is a repercussion of the formation of human capital. University-aged populations suffering from chronic diseases with a high frequency of sick leave absences may restrict them from accumulating the knowledge, skills, and optimal health status needed to achieve their full potential as productive members of the society.
The Saudi Public Health Authority, in collaboration with the World Bank, underscores the importance of evidence-based planning, prioritizing prevention, multisectoral engagement, and a life course perspective that supports health from early adulthood onward. Within this national vision, scaling up lifestyle-focused interventions to curb noncommunicable diseases (NCDs) is considered a central strategy. To ensure effectiveness, existing health promotion and preventive medicine frameworks require adaptation based on regional empirical evidence that identifies modifiable risk factors affecting young people’s current and future health. Consequently, there is a clear need for contemporary region-specific data on the prevalence of chronic diseases among youth and the determinants that shape these outcomes. Using regionally representative survey data conducted to assess health status of youth population in Ha’il region of Saudi Arabia, the objectives of the current study were to:
(1) To assess the prevalence of chronic diseases among university students living in the Ha’il region of Saudi Arabia.
(2) Examine demographic, academic, and lifestyle factors as predictors of chronic diseases among university students.
Our first objective addressed key questions such as: What percentage of university students suffer from chronic diseases living in the Ha’il region of Saudi Arabia? What are the epidemiological, academic, and lifestyle factors associated with chronic diseases among university students in the Ha’il region? These regional-level estimates of chronic diseases are important for determining the need for preventive actions tailored to address specific epidemiological factors at the population level and to control the negative impacts of adverse health at the individual and community levels. The second objective was to identify whether specific lifestyle factors are associated with chronic health conditions among young adults. Examining differences in health by key demographic characteristics, academic variables, and lifestyle factors is critical for designing tailored multilevel interventions and meeting the needs of those who are at the greatest risk for chronic diseases.
Material and Methods
Study Design, Population, and Study
The present study employed a descriptive and analytical population-level cross‑sectional analysis to assess the prevalence and predictors of chronic diseases among undergraduate students at Ha’il University. The investigation was conducted at the institutional level, targeting all enrolled undergraduate students during the May–June 2023 academic session. This broad sampling frame was selected to generate comprehensive evidence on disease patterns and associated demographic and lifestyle determinants within a large and diverse student population. Details regarding the overall sampling frame and participant recruitment procedures have been described in our previously published article on lifestyle and Suboptimal Health Status (SHS) among the same student cohort.15 However, in this analysis, we included all participants, including those with chronic diseases, who were excluded in the previous analysis.
Data was collected using a structured, close‑ended questionnaire designed to capture information on chronic disease history, lifestyle behaviors, and academic characteristics. The instrument was administered exclusively online to ensure wide reach across students studying in different regions and to minimize social desirability bias that may arise in face‑to‑face settings. Students received standardized invitations containing a secure survey link, information about the study purpose, confidentiality assurances, and instructions for voluntary participation. They completed the questionnaire independently using their personal devices, ensuring privacy and reducing interviewer influence.
A total of 11,875 undergraduate students were invited to participate, of whom 10,775 completed the survey, yielding a high response rate of 90.5%. The online mode of administration facilitated efficient data collection from a geographically dispersed student body and supported the reliability of self‑reported responses. While the present analysis focuses specifically on chronic disease prevalence and its predictors, it draws from the same dataset used in our earlier publication on lifestyle behaviors and SHS. The current study extends that work by examining additional health outcomes and applying a more targeted analytical approach to identify risk and protective factors relevant to chronic disease prevention among young adults in Saudi Arabia. The same recruitment infrastructure, sampling frame, and data collection period form the foundation of the current study, enabling methodological continuity and allowing this analysis to extend the earlier work by focusing specifically on chronic disease prevalence and its predictors within the same well‑defined cohort.
Inclusion and Exclusion Criteria
To ensure the validity of the collected data, the following criteria were followed for inclusion of the research participants:
- Respondents must be enrolled as undergraduate students at the University of Ha’il.
- The age of respondents must be at least 18 years.
- Respondents must agree to participate after reading the informed consent.
Participants who did not meet the inclusion criteria were excluded from this study.
Ethical Considerations
This study was approved by the Institutional Ethical Review Board of the University of Ha’il (approval no. H‑2021‑221). All the research procedures conformed to the ethical standards of the Declaration of Helsinki. Participants were presented with an electronic informed consent form outlining the study objectives, voluntary nature of participation, and the right to withdraw at any stage. Confidentiality and anonymity were strictly upheld throughout data collection and in the presentation of findings.
Data Collection
Survey Tool
The data collection tool was designed to collect data on chronic diseases, lifestyles, and academic status. The questionnaire was divided into four sections (1) demographic information (2) chronic diseases occurrence/prevalence (3) academic status-related variables (4) Body Mass Index (BMI) and (5) health-related lifestyle.
The first four parts of the survey form, namely demographic data, the presence of chronic diseases, academic variables and BMI, were designed on the basis of the review of literature on the subject and were adapted to the particularities of the university where the research would be conducted. Content validity was determined by seeking expert consultation in the field of public health and epidemiology. Each item was separately rated by experts on a four-point scale (1 = not relevant; 4 = highest relevance). Content Validity Index (CVI) was computed at the item level (I-CVI) and at the scale level (S-CVI), and those questions that obtained an I-CVI lower than 0.78 were eliminated or modified on the basis of further discussion among experts. The resulting questionnaire obtained an S-CVI of 0.91, thus confirming its high content validity. The demographic data part comprised four questions (age, gender, marital status and place of living); the chronic diseases part included one question with several possible answers (diabetes, migraine, heart disease, hypercholesterolemia, and open-ended option to report others); and the academic variable part comprised six questions (major/college, year of studies, GPA, number of registered credit hours, absence from lectures, and intent to drop out). One open‑ended question captured the data required to compute Body Mass Index (BMI).
Fourth section collected data on lifestyle data using a previously developed tool.19
Demographic Data
This section collected data on age, sex, marital status and residence.
Chronic Diseases
This section comprised a single item in which respondents were asked to indicate whether they had been diagnosed with any chronic health condition from a list provided (eg, diabetes, migraine, heart disease, hypercholesterolemia, and others with open-ended response option).
Academic Variables
This section focuses on academic-related factors, including college, academic level, grade point average (GPA), credit hours registered in the current semester, number of missed lectures, and intent to withdraw from the current semester.
Body Mass Index
An open-ended question asked the students to state their weight in (kg) and height in (cm). This data is used to calculate BMI.
Health-Related Lifestyle Assessment
We used the Simple Lifestyle Indicator Questionnaire (SLIQ).20 The instrument consists of 12 items distributed across five domains, capturing key lifestyle behaviors including physical activity, dietary practices, substance use (tobacco and alcohol), sleep patterns, and stress management. In the diet domain, assessing the quality and variety of participants dietary intake (fruits, vegetables, and whole grains), the raw score reflects the weekly frequency of consumption of healthy foods. A higher raw score (>10) corresponds to a healthier diet, (6–10) is considered moderate, while a lower score (<5) is considered a poor diet.15,16 The physical activity domain reflects the frequency, duration, and intensity of activities, and includes three items: engaging in vigorous, moderate, or light exercise.15,16 Life stress was assessed with a single question asking participants to rate their perceived stress level on a scale from 1 to 6. A Lower score (1–2) is considered very stressful, 3–4 intermediate stressful, and 5–6 considered not at all stressful. Sleep quality was classified based on reported sleep duration, with six hours considered healthy, seven to nine hours categorized as intermediate, and durations below six hours or above nine hours classified as unhealthy. Furthermore, raw scores were subsequently converted into categorical scores ranging from 0 to 2, where 0 denotes poor behavior, 1 indicates intermediate behavior, and 2 reflects healthy behavior. The sum of these category scores yields a total lifestyle score between 0 and 10, which is further classified into the overall lifestyle categories of unhealthy (1–5) and healthy (6–10) to determine the health-related lifestyle of undergraduate students in this study. The SLIQ has been validated in prior studies and reported adequate psychometric properties.19 Initial psychometric testing showed good internal consistency and stable factor structure, confirming that its five domains including (diet, physical activity, smoking, alcohol use, and stress) measure distinct lifestyle components.20 Additional studies in diverse settings, including rural youth populations, have further confirmed its applicability and consistent performance, reinforcing its suitability for assessing lifestyle patterns in epidemiological research.21
Data Analysis
Data was stored in an Excel spreadsheet and analyzed using IBM SPSS, version 25.0. Categorical variables were described using descriptive statistics, such as percentages. Binary logistic regression was performed to examine the relationship between the dependent variable (chronic disease) and the independent variables (academic status, lifestyle, and demographic characteristics), with significance set at p<0.05. Univariate logistic regression analyses were performed for each independent variable to calculate odds ratios (ORs). Subsequently, the adjusted odds ratio (AOR) was calculated to assess the strength of the association between independent and dependent variables after controlling for other confounding variables. Confidence intervals (CIs) were determined for both OR and AOR at a 95% confidence level.
Several diagnostic tests were used to assess the logistic regression model fit. Variance inflation factors (VIFs) were used to assess multicollinearity among the independent variables, and all values were below the standard threshold of 10. Model fit was assessed using the Hosmer-Lemeshow test; non-significant results indicated adequate calibration.
Results
Table 1 presents descriptive statistics for the demographic characteristics of the study participants and the prevalence of chronic diseases. Most of the participants fell into the age category of 20–24 years (n = 7558; % = 70.1) and single (n = 9785; % = 90.8). There was almost equal representation of male (n = 5538; % = 51.4) and female participants (n = 5237; %=48.6), and equal representation of students from four broad categories of academic fields (n = 3778; % = 35.1) in Engineering Sciences, followed by Social Sciences (n = 3721; % = 34.5) and Health Sciences (n = 3276; % = 30.4) as shown in Table 1.
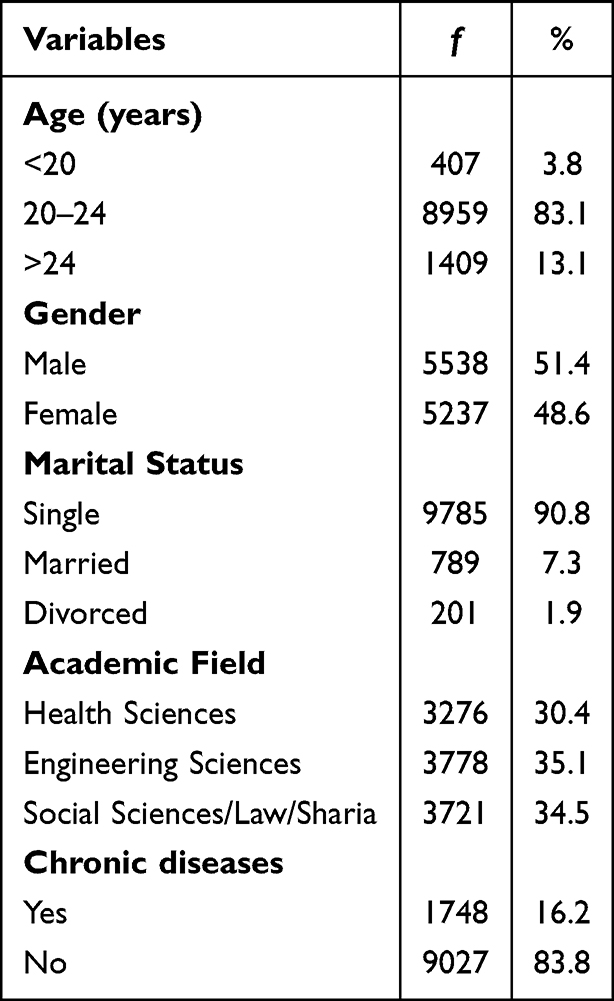 |
Table 1 Descriptive Statistics on Demographic Variables and Prevalence of Chronic Health Conditions Among Study Participants (n = 10,775) |
The prevalence of chronic diseases among undergraduate students in total sample of (N = 10,775) respondents was 16.2% (n = 1748). In this whole sample, diabetes was the most prevalent (6.8%, n = 731), followed by migraines (5.4%; n = 583), heart disease was prevalent among (2.0%; n = 217), hypercholesterolemia (1.9%; n = 201), and other chronic health conditions were below 1% (n = 16) as shown in Figure 1.
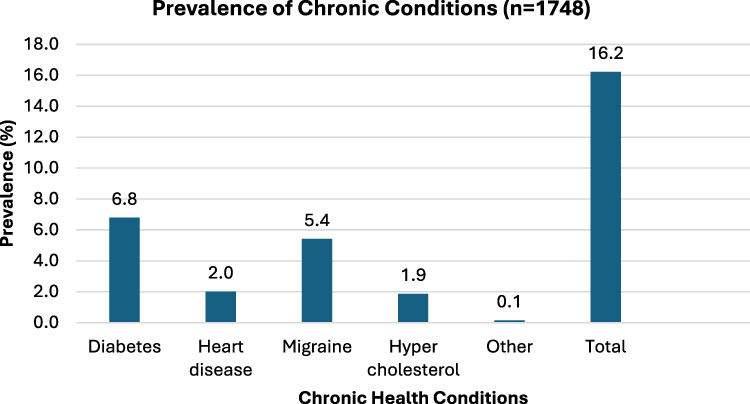 |
Figure 1 Prevalence of Chronic Conditions among University of Ha’il students (n=1748). |
Among all students who had any chronic disease (n = 1748), diabetes represented 41.8%, migraine represented 33.4%, heart diseases made up 12.4%, and high blood cholesterol levels comprised 11.5% of all diagnoses.
Table 2 presents findings from univariate and multivariate logistic regression analysis for demographic predictors of chronic diseases among university students. The results showed that age, gender and marital status have an influence on chronic diseases among university students. Younger students had almost 4 times greater odds of chronic diseases [AOR = 3.96 (95% CI:3.71–4.23), p value = <0.001], compared to older ones. Female students had greater odds of chronic diseases [AOR = 1.41 (95% CI: 1.09–1.64), p value = 0.03]; compared to male students. Likewise, married students had more than 5 times greater odds of chronic diseases [AOR = 5.06 (95% CI:1.41–10.39), p value = 0.001] compared to single students.
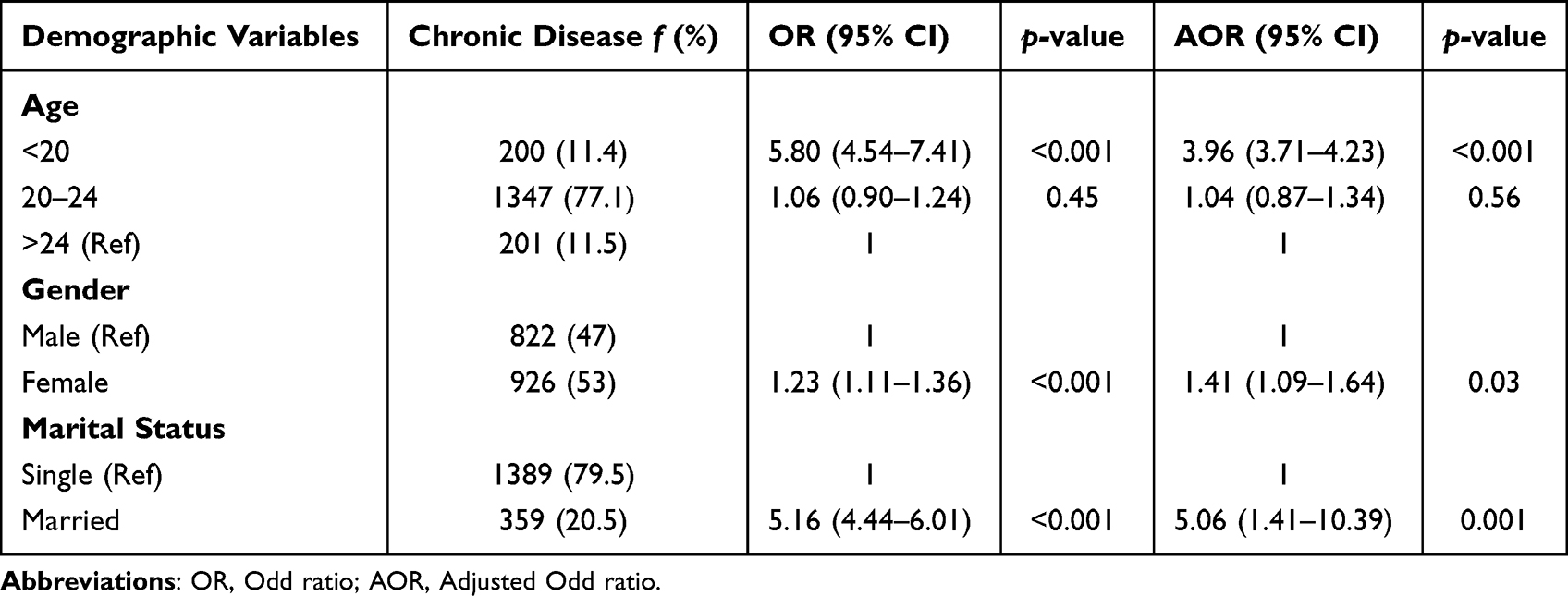 |
Table 2 Demographic Predictors of Chronic Diseases Among Undergraduate Students (n=1748) |
Table 3 illustrates the results of univariate and multivariate logistic regression analyses of the prevalence of chronic diseases and academic variables. The findings demonstrated that the field of study, academic level, GPA, missed lectures, and students’ intention to withdraw had an influence on chronic disease prevalence. Students in social sciences and health colleges had greater odds of chronic diseases (AOR = 5.90 (95% CI:1.05–11.67], p ≤ 0.001) and [AOR = 1.50 (95% CI:1.17–1.92), p = 0.001], respectively, when compared to students in engineering colleges. In terms of academic level, the odds were higher in the early years of academic experience than in later years. Overall, there was a U-shaped risk pattern, as the odds of having chronic diseases were higher in the early years of college and at the internship level, whereas they were somewhat lower in the middle years. For the GPAs, the first-class [AOR = 6.09 (95% CI:3.14–11.79), p ≤ 0.001] and second-class lower/pass [AOR = 57.0 (95% CI:5.16–9.07), p ≤ 0.001] had higher odds of chronic diseases compared to the second-class upper class. Moreover, students who intended to withdraw from their studies had greater odds of chronic diseases [AOR = 6.99 (95% CI:3.13–15.60), p < 0.001] than students who did not. Credit hours registered and missed lectures in the current semester did not influence chronic disease prevalence as shown in Table 3.
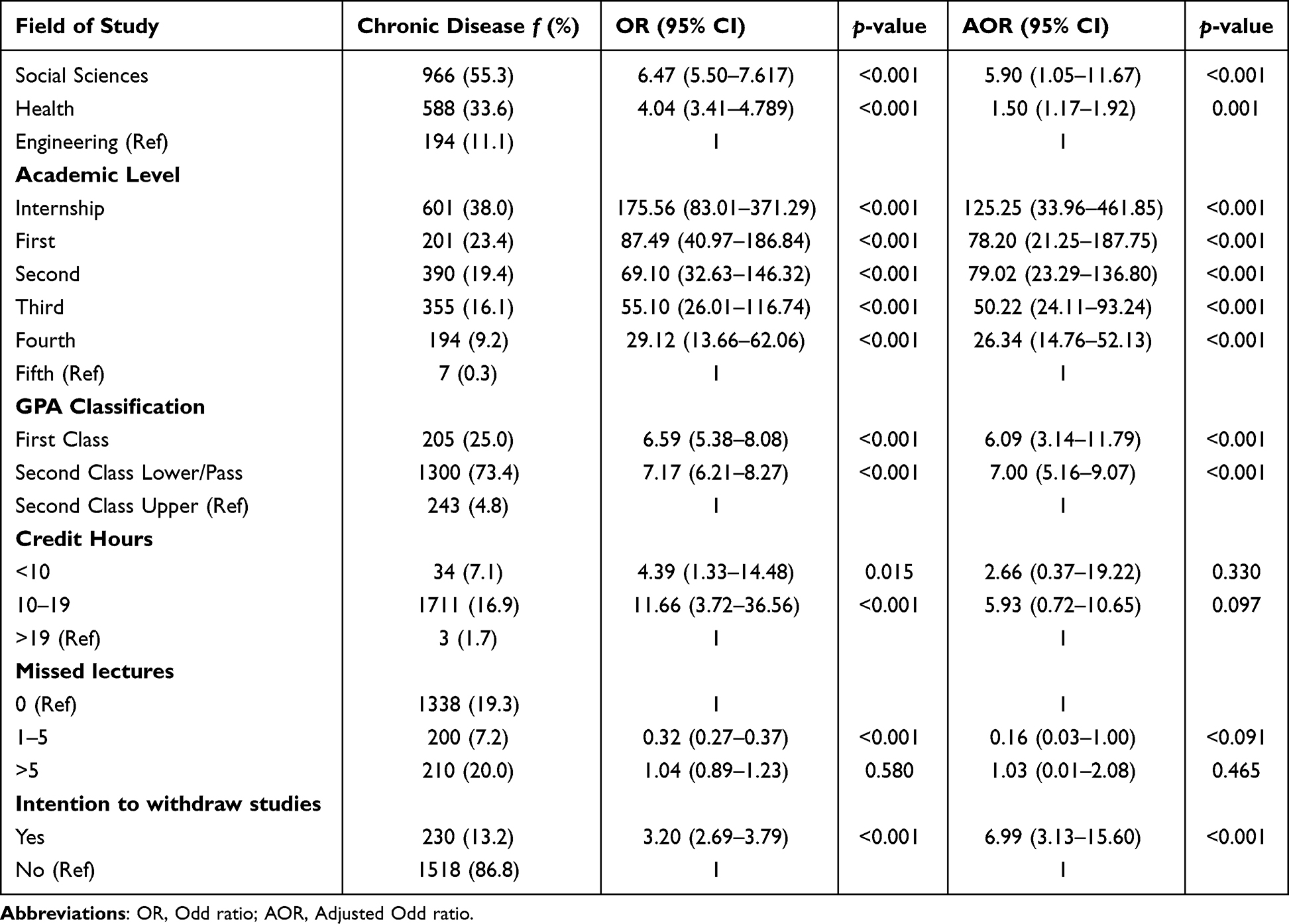 |
Table 3 Influence of Academic Variables on Risk for Chronic Diseases Among Undergraduate Students (n=1748) |
Table 4 demonstrates the findings from the univariate and multivariate logistic regression analysis for various lifestyle factors that may pose a risk of chronic diseases in undergraduate students. The lifestyle variables included diet, physical activity, stress, BMI, and sleep. Students with lower diet scores (0–5) had more than six times greater odds of having chronic disease [AOR = 6.40 (95% CI:3.67–10.28), p < 0.001] than those with higher diet scores (11–15). Those with light activity had greater odds of chronic disease [AOR = 14.25 (95% CI:9.34–24.90), p < 0.001] than those with vigorous activity Regarding stress level, the higher the stress, the higher the odds of having a chronic disease; life stress level 1 or 2 (very stressful) had almost 4 times [AOR = 3.69 (95% CI:2.12–6.41), p < 0.001], while life stress level 3 or 4 (intermediate stressful) had almost 10 times [AOR = 9.87 (95% CI:8.01–11.34), p < 0.001] compared to life stress level 5 or 6 (not at all stressful). Moreover, overweight and obese had greater odds of chronic disease than those with normal body weight with [AOR = 1.59 (95% CI:1.07–3.12), p < 0.001] and [AOR= 10.40 (95% CI:5.59–19.33), p < 0.001], respectively. Moreover, those sleeping for less than six hours [AOR = 1.21 (95% CI:1.09–1.53), p = 0.002] and more than nine hours [AOR = 6.11 (95% CI:2.84–13.14), p < 0.001] had greater odds of chronic disease than those sleeping for six hours. Overall, students with unhealthy lifestyles were more likely to have chronic diseases than those with a healthy lifestyle [AOR = 2.60 (95% CI:2.33–2.90), p < 0.001].
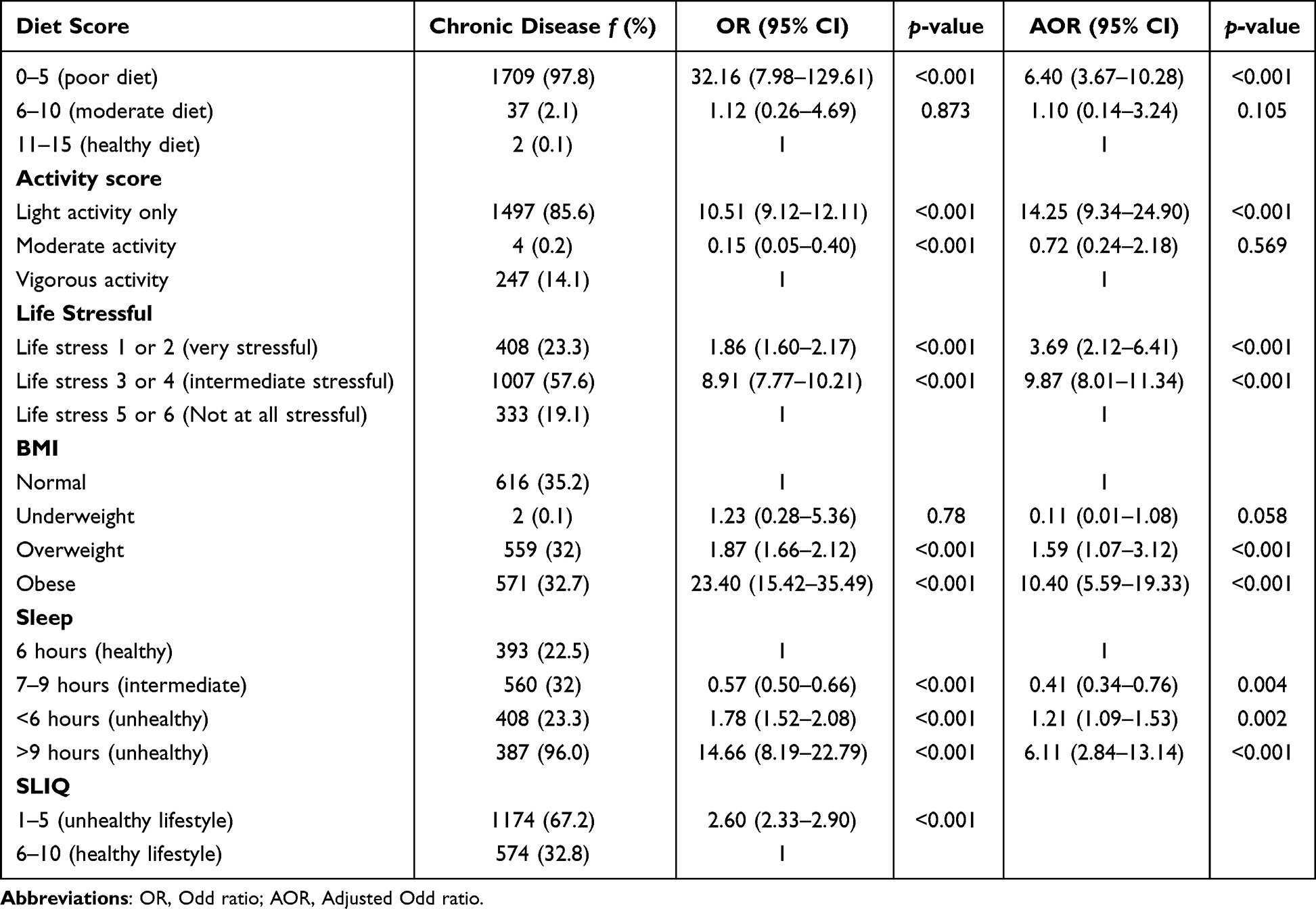 |
Table 4 Logistic Regression Analysis for Determining Lifestyle Predictors of Chronic Diseases Among Undergraduate Students (n=1748) |
Discussion
This study expands the existing literature by examining the role of several demographic, academic, and lifestyle factors associated with chronic diseases in youth living in the Ha’il region of Saudi Arabia. Youths comprise approximately 37% of the total population in Saudi Arabia and 35% of the population in the Ha’il region of Saudi Arabia. Thus, the findings of the current study have significant implications for addressing risk factors for chronic diseases in the target population.
Our study reported that the prevalence of chronic health conditions is up to 16% distributed among diabetes, migraines, heart disease and high cholesterol. Findings reveal that several demographic and lifestyle factors are associated with risk for chronic health problems among university students. Our findings are comparable with international studies that reported prevalence of chronic diseases including (obesity, asthma, migraine, depression, and metabolic disorders) among youth populations range from 16.5% to 30% and on average three or more behavioral risk factors associate with NCDs.22–24 Consistent with international literature, our findings underscore the role of demographic and lifestyle factors in shaping early chronic disease risk in young adult populations, reinforcing the need for university‑based screening and youth‑focused preventive interventions.
Analysis showed that among the demographic correlates, female, younger, and married students had higher odds of suffering from chronic health diseases. The implications of these findings, in light of recent studies and the broader social and cultural contexts of Arab countries, are discussed below. Global and regional evidence demonstrates that women face a disproportionately higher risk of poor physical and mental health25 due to the combined influence of biological vulnerabilities,26 gender-based social inequalities,27 psychological stressors, and economic disadvantages.28 In case of Saudi Arabia, social and cultural norms have significant influence on health behaviors of female population that pose as a significant risk factor for non-communicable diseases.29 The broader social and cultural context in Ha’il region of Saudi Arabia explains our study findings because females have more sedentary lifestyle due to personal preferences and environmental circumstances. Most of the female university students chose to participate in indoor activities. These sedentary lifestyles are supported by local social and cultural norms. There are also limited opportunities for physical sports, and very few female students participate in competitive sports events organized by universities. Several buildings on the university campus do not have specified areas for gyms or are equipped with accessories to support physical activity for female students. These gendered patterns mirror those reported in nationally representative community-based studies on young adults, suggesting that university environments are not effective in neutralizing these social and cultural influences.6
Our findings showed that younger students had higher odds of developing chronic diseases, which is somewhat contradictory to the usual epidemiology of chronic disorders. Possible explanations are the characteristics of the target population and study sample, which were restricted to university students in Ha’il. Previous research based on national Saudi data reported that low fruit and vegetable consumption was associated with young age and being a student.30 These unhealthy diet which were associated with chronic health disorders. Other researchers have also reported that unhealthy diet and physical inactivity prevalent among various segments of the population, including young adults, are not only a public health but a growing economic challenge in Saudi Arabia.30
Our study findings show that married students were at higher risk of developing chronic diseases and these findings are supported by previous study that has shown that being married is associated with greater odds of having at least one chronic condition, even after adjustment for other factors.30 Women in Saudi culture have different social and familial experiences after marriage such as dietary changes and low preference for physical activities to meet expectations of traditional roles of married women along with additional responsibilities of university studies. Together, these results suggest that gender, age, and marital status co-interact with each other, thus increasing the risk of chronic diseases among young married female students. These findings imply that university students are confronted with several transitions, such as adapting to adulthood roles, expectations to meet gender roles, and marital transitions, which may appear as measurable chronic disease risks. These findings imply the need for life-course-oriented prevention, rather than waiting until chronic disease is firmly established in later adulthood. Preventive interventions in universities should be stratified and tailored, such as gender‑sensitive physical activity programs and targeted health education and counseling programs for young and married students.
Academic variables are the most relevant and important factors for university students, and the investigation of these factors is a unique contribution of this study. Our study findings showed that students in social science and health colleges had greater odds of developing chronic diseases than those in engineering colleges. These findings are explained in light of a previous study from Saudi Arabia, which demonstrated the negative impact of chronic disease among medical students on their academic performance and were associated with stress and lifestyle disruption.31 Another recent study demonstrated that a high prevalence of sleep disorders among medical students increases the risk for poor health and chronic illnesses.32 It is important to note that among demographic factors, females were found to 1.2 times more at risk of experiencing chronic illnesses, and there was also a higher percentage of female students’ representation in medical and social science colleges than in engineering colleges. Thus, targeted programs to support female students in health colleges are crucial to prevent the development of chronic morbidities among students who are likely to be future healthcare providers.
Our study findings demonstrated that students in their early years of college had higher odds of experiencing chronic health problems. Besides, students in early years are exposed to multiple stressors such as adjusting in the new and demanding academic environment of university that may impact the health of students.33 The current study findings demonstrate increased vulnerability for students in internships as compared to middle years. Some studies from Saudi Arabia have reported elevated levels of stress and poor sleep quality among medical and health science interns; these factors are known to be associated with chronic disorders.34
Consistent with the findings of other regional studies, we found that the odds of developing chronic health problems were significantly higher among those with high and low academic performance. Moreover, study findings demonstrate that students intending to withdraw had nearly seven times higher odds of chronic disease. Intention to withdraw can be interpreted as a proxy for severe academic and psychosocial distress, aligning with the multidimensional well‑being framework during higher studies.35 University students are prone to facing pressures of academic achievement and failure and experience physiological and psychological stress responses, which increase the risk of chronic diseases. According to a systematic review of studies conducted in the past two decades in Saudi Arabia, the prevalence of depression, stress, and anxiety among students in higher education and internship is very high, which heightens their vulnerability to chronic illnesses.36 Thus, a plausible interpretation of these findings is that various demographic and academic factors independently as well as interact with each other to increase the risk of chronic illness. Young, female, married students who are also vulnerable to high mental pressures in a competitive academic environment during their early years and internships thus had higher odds of developing chronic illnesses. There is a need to provide adequate support to this vulnerable section of the youth population at multiple levels for better health and academic achievement.
The ever-rising higher rates of childhood obesity in Saudi Arabia also pose a risk for the development of chronic health problems in young adults.37 We also found that based on BMI measurements, students who were overweight and obese had higher risk of chronic diseases. Lack of awareness among university students about the risk factors for non-communicable diseases and the fact that many university students have unhealthy lifestyles38 that make them vulnerable to diabetes, heart diseases, and high cholesterol, as confirmed by our study. Our findings confirm that unhealthy behaviors of university students, including unhealthy diet, unhealthy sleep, low physical activity, and higher levels of stress, significantly increase the odds of having chronic health problems. The findings of this study align with emerging evidence on the growing burden of lifestyle-related health risks among Saudi youth.13 University students in the KSA increasingly exhibit unhealthy dietary patterns, insufficient sleep, low levels of physical activity, and heightened psychological stress, which collectively elevates their susceptibility to chronic health conditions. These patterns reflect broader national trends associated with rapid socioeconomic transitions, increased availability of energy-dense foods, sedentary lifestyles, and rising academic and social pressure.
Further understanding of the significance of the results is provided via cross-contextual comparison. There is evidence of a significant chronic disease burden among university students in the European region, with mental disorders, musculoskeletal issues, and respiratory illnesses being among the top three chronic diseases experienced by this demographic group.39 Despite certain similarities between the two sets of results, the main difference lies in the dominance of metabolic disorders, including diabetes mellitus and hypercholesterolemia, in the current sample population. The disparity can be explained by the ongoing epidemiological transition occurring in the GCC countries, during which rapid economic development goes hand in hand with the adoption of an unhealthy energy-dense diet and sedentary lifestyle.40
Another parallel case occurs in sub-Saharan Africa, where hypertension and sickle cell diseases have become prominent causes of chronic diseases among young adults.41,42 Although the disease profiles differ significantly from those in the current research, behavioral risk factors behind such morbidity outcomes are similar for the two populations. As for the North American context, mental health problems, especially depression, and respiratory illnesses, have become prevalent chronic diseases in the student population of North American universities.43 It is important to note that even though the incidence of diabetes in the Ha’il University student population is lower than that of other chronic diseases, the higher prevalence of the condition compared to other student populations is noteworthy, considering the genetic predisposition of Arabs to developing type 2 diabetes.44
In this context, the observed association between unhealthy behaviors and chronic health problems underscores the urgency of implementing comprehensive and pervasive preventive strategies targeting young adults. These interventions need to be implemented in a wide range of settings, including university campuses, internship sites, and community activities, to promote health and well-being, which are essential for achieving academic progress and professional development. Given that university students represent a critical segment of the Saudi population and are central to national development goals, promoting healthier lifestyles is essential not only for disease prevention but also for sustaining academic performance and future workforce productivity.
Risk Management and Public Health Policy Implications of Study Findings
The comparison of prevalence rates of chronic diseases among university student population in our study with general population in previous literature suggests that many young adults may remain undiagnosed. We found that diabetes was the most prevalent 6.8%, and around 2% of students suffered from heart disease and hypercholesterolemia. A recent study reported national prevalence of diabetes and hypertension among Saudi general population is as high as up to 16.1% and 13.0% respectively.45 Other studies from Saudi Arabia reported that 11.9–13.8% of people are diagnosed or undergoing treatment for high cholesterol levels.46 This underscores the need for routine diabetes and lipid screening in university settings to identify at‑risk individuals as early as possible to control the risk of development of chronic diseases in later age. Saudi guidelines on management of some chronic health conditions emphasize lifestyle modification and lipid‑lowering therapy as central prevention strategy; however, the implementation gaps persist. Thus, our findings reinforce the need for better adherence to screening protocols and treatment pathways, especially for younger populations who are often overlooked.
Current study findings urge for policy interventions that could integrate lifestyle counseling, nutrition programs, and physical activity promotion into campus health services. Universities represent a strategic point for primary prevention before risk accumulates. Thus, public health workers in collaboration with institutions must use the insights gained from the previous international and regional studies to design and implement culturally relevant initiatives that address diet, sleep, physical activity, and stress management, which could play a pivotal role in mitigating chronic disease risk and fostering long-term health and well-being among Saudi youth.
A scoping review of literature on health literacy among youth in African countries reports about young peoples’ lack of awareness about the risks of non-communicable diseases and identified a significant association between low health literacy and risk for chronic disease among this population.22 Thus, educating university students about these risks and supporting them in adapting to healthy lifestyles may help to decrease vulnerability. Risk management policies should prioritize risk‑communication campaigns tailored to youth, emphasizing the long‑term cardiovascular consequences of untreated chronic health conditions.
Our study findings showed that academic variables significantly associated with vulnerability for chronic diseases among university students. These findings validate the insights gained from a prior study emphasizing that academic life is a core dimension of student well‑being, influencing both mental and physical health.35 Academic stressors are not uniform across disciplines and programs with heavier cognitive, emotional, or clinical demands may elevate chronic disease risk through stress‑related pathways. Moreover, our study findings in congruence with Indrayathi et al found that students’ academic stage may influence their well‑being. Particularly, entry into university and transition to professional practice are critical stress points that may worsen health outcomes.35 Our study findings call for institutional-level risk management strategies to support student well‑being. Screening for chronic disease risk could be integrated into orientation programs, academic advising and internship preparation programs to reach out high‑risk groups such as (early-year students, interns, low GPA students and those intending to withdraw). Universities should adopt proactive, data‑driven health policies that address both academic and non‑academic determinants of student health.
Chronic disease prevalence is influenced by academic factors but likely mediated by psychosocial and environmental stressors. This supports a holistic model where chronic disease is not merely a medical issue but a reflection of the student’s overall well‑being ecosystem. Findings reinforce the need for integrated academic support systems that recognize the interconnectedness of academic stress, mental health, and physical health. At the systematic level, both the outdoor and indoor physical environment of university campuses should be redesigned and equipped in a way that creates more opportunities for university students to engage in physical activities. Moreover, food outlets on university campuses have replaced fast-food items and soft drinks with fruit and vegetable snacks and sugar-free drinks. Cultivating a sense of cohesion among students who adopt positive health behaviors may help reinforce healthy lifestyles among other students and increase their adherence to healthy nutrition and physical activity to mitigate the risk of chronic diseases. Youth club activities in universities should focus on health education programs designed and implemented in collaboration with the public health departments and Ministry of Health. Given that Ha’il City is expanding in terms of economic and social development, it is important to use this time to encourage investors to invest money in types of businesses (healthy food, sports, tourism) that promote health and well-being for youth and control the opening of fast-food outlets near university campuses. Given the gaps identified in current public health initiatives targeting youth in the Ha’il region, the Ministry of Health could strengthen chronic disease prevention by adopting a more coordinated, youth‑centered strategy that aligns with university settings. Priority actions include establishing routine health screening programs on campuses to detect early signs of obesity, hypertension, diabetes, and mental‑health concerns, and integrating these services with digital follow‑up systems to support continuity of care. The MoH could also collaborate with universities to improve campus food environments, regulate unhealthy food availability, and promote affordable, culturally acceptable healthy options.
Health counselors trained in lifestyle medicine should be hired by counseling and guidance centers in universities that conduct health-screening and monitoring programs. This initiative may help identify at-risk students, and one-to-one guidance should be provided by health counselors to students who are at risk for or currently suffering from chronic illnesses. This personalized care and psychoeducation provided by behavioral health professionals will have far-reaching benefits in developing a sense of commitment among students towards healthy lifestyles. Training university teaching staff to recognize and offer resources for chronic disorders to at-risk students, such as high and low academic achievers, will be beneficial not only to improve health concerns but can also significantly prevent their repercussions on their academic performance.31
In the collectivist culture of Saudi Arabia, families can play a pivotal role in tying together motivation and long-term behavioral changes among all members of the family. Prior literature suggests that promoting health behavior patterns in a social unit like the family may create longer-lasting and larger-scale behavioral changes for the adoption of healthy lifestyles.47 The community-based activities organized by public health and other youth clubs where students can participate along with their families can be beneficial in equipping family members with essential information to support each other to comply with health behaviors. This may have multiple benefits, as older adults who are already suffering from serious chronic illnesses are less likely to feel isolated due to dietary restrictions and receive support from young people to perform physical activities such as brisk walking in their daily routines.
These recommendations and implications of study findings are relevant and applicable to other regions of the world that are undergoing rapid lifestyle transitions, reinforcing the importance of early, context-specific interventions to protect the health of emerging adults.
Strengths and Limitations
This study had a large sample size and complete representation of the target population from the Ha’il region of Saudi Arabia, thus providing reliable estimates of the prevalence of chronic health conditions among university students. The current study findings indicate that in every 100 students, there are 16 who are suffering from chronic disease, which provides significant epidemiological information for public health organizations, university leaders, and social and community development sectors to design an action plan for disease prevention and health promotion programs targeting youth. Some suggestions for such interventions have been mentioned earlier while discussing the public health implications of this study.
Another key strength of this study is its comprehensive assessment of demographic, academic, and lifestyle-related behaviors, which enabled a multidimensional understanding of the determinants of chronic disease risk among university students. By capturing this broad spectrum of factors, this study provides a strong foundation for designing tailored multifactorial interventions that address the interconnected influences that shape students’ health outcomes. Our study findings also highlight the current gaps in ongoing public health initiatives targeting youth in the Ha’il region, which seem to be less effective in reducing lifestyle-related health risks. This study offers an evidence-based direction for strengthening targeted health education, enhancing healthcare infrastructure in underserved areas, and promoting greater family engagement in chronic disease prevention and management.
Furthermore, insights from the Ha’il region underscore the need for both institutional and family centered strategies to address academic pressures and lifestyle behaviors that contribute to chronic disease vulnerability. Given the gaps identified in current public health initiatives targeting youth in the Ha’il region, the Ministry of Health could strengthen chronic disease prevention by adopting a more coordinated, youth‑centered strategy that aligns with university settings. Priority actions include establishing routine health screening programs on campuses to detect early signs of obesity, hypertension, diabetes, and mental‑health concerns, and integrating these services with digital follow‑up systems to support continuity of care. The MoH could also collaborate with universities to improve campus food environments, regulate unhealthy food availability, and promote affordable, culturally acceptable healthy options.
Although this study offers important insights, several limitations must be acknowledged when interpreting its findings, including constraints related to the sampling methods and disadvantages of the cross-sectional design. Furthermore, the study utilized self-reported measures for data collection, which were affected by recall or social desirability bias; these could limit the accuracy of data, the causal interpretation of the results, and the generalizability of the findings. In addition, measuring chronic disease prevalence with a single self-report did not specify whether conditions were physician-diagnosed or self-perceived, so misclassification is possible. However, it was not possible to access the medical records of students due to ethical implications, thus self-report method was employed to inquire about chronic health conditions. Besides, the absence of sociocultural factors and nutrition literacy in our study limited our ability to understand the complex interactions of these factors.
To strengthen future research, we recommend verifying diagnoses and including comprehensive factors to provide a more nuanced understanding of the influence on health behaviors and outcomes. Moreover, community-based participatory approaches actively engage students, families, and local stakeholders throughout the research. Such methods would allow investigators to capture the cultural, social, and environmental nuances that shape lifestyle behaviors among Saudi youth. Moreover, participatory approaches create opportunities for simultaneous education and intervention, enabling researchers to persuade existing community assets and to develop culturally grounded strategies for chronic disease prevention and management. Embedding research within real community contexts may ultimately yield more sustainable and context-appropriate solutions to promote healthy lifestyles among young people in Saudi Arabia.
Conclusion
This study found that 16.2% of university students in Ha’il, Saudi Arabia, live with at least one chronic health condition, highlighting a pressing public health concern within a population traditionally considered healthy. The analysis revealed that female, younger, and married students were particularly vulnerable, and that academic pressures, especially during early college years, internships, and demanding fields of study, further intensified health risks. These demographic and academic vulnerabilities were compounded by modifiable lifestyle behaviors, including poor diet, inadequate sleep, physical inactivity, stress, and obesity, all of which were strongly associated with chronic disease prevalence.
Taken together, these findings challenge traditional prevention models that focus primarily on adults and emphasize the need for life‑course approaches that intervene during the university years, when health behaviors are still malleable. Addressing chronic disease risk among students requires multilevel strategies, such as improving campus environments, expanding access to healthy food, integrating gender‑responsive health programming, strengthening academic counseling, and engaging families in behavior‑change efforts. Prioritizing student health through culturally grounded interventions can help safeguard both individual wellbeing and the long‑term productivity of Saudi Arabia’s future workforce.
The rates of prevalence of chronic disease and risk factors identified in this study sample are comparable with regional and global studies discussed above; thus, apart from the local and regional implications, current study findings have significance in global public health context.22 Universities across the world have become more multicultural and multi-ethnic, the need to develop interventions that would be equally based on scientific research and respect for cultural specifics has become extremely important. This research supports this need as its outcome indicates that even in a homogenous student environment, factors such as gender, age, marital status, academic stress, and lifestyle behavior interact to form distinct and multiple health risks for students in higher education. The risks are diversified, thus a single strategy for health improvement cannot be developed even within the borders of one country. Therefore, global public health organizations, as well as university administration, especially in developing countries that experience rapid urbanization should consider introducing a similar multilevel intervention that includes structural, family-based, gender-specific, and cultural dimensions in chronic diseases prevention and treatment programs targeting college and university students. The chronic disease burden experienced by university students today affects not only individual students but has serious public health and development implications in an international context since it undermines sustainability of human capital and workforce productivity. Protecting student health is therefore not only a clinical or educational priority but a national development imperative.
Future research should investigate environmental and structural determinants, such as campus food environments, physical activity facilities, and academic workload policies, to understand how institutional contexts shape health risks. Qualitative studies can provide deeper insight into specific context factors that grounds experience of such academic pressure and cultural expectations, while comparative research across public and private universities may reveal institutional differences in risk profile.
Abbreviations
NCD, Non-communicable diseases; SLIQ, Simple Lifestyle Indicator Questionnaire; NBP, Northern Border Province; AOR, Adjusted Odd Ratio; CI, Confidence Interval.
Acknowledgments
We thank the Deanship of Scientific Research at the University of Hail-KSA for their support in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This research was funded by the Deanship of Scientific Research at the University of Ha’il (funding number RG-20215).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Russo K. Assessment and treatment of adolescents with chronic medical conditions. J Heal Serv Psychol. 2022;48(2):69–17. doi:10.1007/s42843-022-00059-4
2. Valanju R, Barani M, Mautner D, et al. Youth perspective on chronic disease prevention. Lancet Child Adolesc Heal. 2022;6(7):456–458. doi:10.1016/S2352-4642(22)00131-6
3. Alenazi AM, Alhwoaimel NA, Alqahtani BA, Alshehri MM, Alhowimel AS, Khunti K. Prevalence of multiple long-term chronic conditions and associated disabilities among community-dwelling adults in Riyadh. Front Public Health. 2024;12:1275124. doi:10.3389/fpubh.2024.1275124
4. World Health Organization. The Health of Young People: A Challenge and a Promise. World Health Organization; 1993.
5. Boutayeb W. The Growing trend of noncommunicable diseases in arab countries. In: Disease Prevention and Health Promotion in Developing Countries. Springer; 2020:61–72.
6. Alzahrani MS, Alharthi YS, Aljamal JK, Alarfaj AA, Vennu V, Noweir MD. National and regional rates of chronic diseases and all-cause mortality in Saudi Arabia—analysis of the 2018 household health survey data. Int J Environ Res Public Health. 2023;20(7):5254. doi:10.3390/ijerph20075254
7. Aljarid S, Alonazi W. Examining factors contributing to mortality in Saudi Arabia: proposing effective healthcare management approaches. BMC Public Health. 2025;25(1):1801. doi:10.1186/s12889-025-22421-z
8. Almahmoud OH, Arabiat DH, Saleh MY. Systematic review and meta-analysis: prevalence of hypertension among adolescents in the Arab countries. J Pediatr Nurs. 2022;65:e72–e79. doi:10.1016/j.pedn.2022.03.002
9. Almuqbil M, Rabbani SI, Gilkaramenthi R, et al. Non-communicable diseases in Saudi adolescents: prevalence, risk factors, and implications for public health. Front Public Health. 2025;13:1542339. doi:10.3389/fpubh.2025.1542339
10. Alenzi EO, Fatima W, Amara A, et al. A systematic review of chronic diseases and their prevalence among the population of northern borders province (NBP) in Saudi Arabia. J Multidiscip Healthc. 2023;Volume 16:1047–1056. doi:10.2147/JMDH.S401001
11. Alhusseini N, Alsinan N, Almutahhar S, et al. Dietary trends and obesity in Saudi Arabia. Front Public Health. 2024;11:1326418. doi:10.3389/fpubh.2023.1326418
12. Woodman A, Coffey M, Cooper-Ryan AM, Jaoua N. The relationship between lifestyle habits and obesity among students in the Eastern province of Saudi Arabia: using the Arab Teens Lifestyle (ATLS) questionnaire. BMC Public Health. 2024;24(1):2267. doi:10.1186/s12889-024-19353-5
13. AlQuaiz AM, Kazi A, Almigbal TH, AlHazmi AM, Qureshi R, AlHabeeb KM. Factors associated with an unhealthy lifestyle among adults in Riyadh City, Saudi Arabia. In: Healthcare. Vol. 9. MDPI; 2021:221.
14. Alibrahim MS, Said MA, Bursais AK, et al. Risk factors for cardiovascular disease among Saudi students: association with BMI, current smoking, level of physical activity, and dietary habits. PLoS One. 2025;20(5):e0321206. doi:10.1371/journal.pone.0321206
15. Alsaif B, Asweto CO, Hassan SUN, et al. Undergraduates’ lifestyle and Suboptimal Health Status (SHS): a cross-sectional study in the Ha’il region of Saudi Arabia. PLoS One. 2025;20(1):e0317127. doi:10.1371/journal.pone.0317127
16. Sperry L. Biopsychosocial model of chronic illness. In: Psychological Treatment of Chronic Illness: The Biopsychosocial Therapy Approach. American Psychological Association; 2006:25–39. doi:10.1037/11378-002
17. Wikel K, Markelz AM. Chronic health conditions, school attendance, and socioeconomic factors: a literature review. J Spec Educ Apprenticesh. 2023;12(2):9.
18. Linardakis M, Papadaki A, Smpokos E, Kafatos A, Lionis C. Prevalence of multiple behavioral risk factors for chronic diseases in medical students and associations with their academic performance. J Public Health. 2020;28(4):383–392. doi:10.1007/s10389-019-01030-2
19. Godwin M, Pike A, Bethune C, Kirby A, Pike A. Concurrent and convergent validity of the simple lifestyle indicator questionnaire. Int Sch Res Not. 2013;2013(1):529645.
20. Godwin M, Streight S, Dyachuk E, et al. Testing the simple lifestyle indicator questionnaire: initial psychometric study. Can Fam Physician. 2008;54(1):76–77.
21. Shekhar R, Aslami AN, Jha RR. Assessment of lifestyle in rural youth using simple lifestyle indicator questionnaire (SLIQ). Bangladesh J Med Sci. 2017;16(3):401–406. doi:10.3329/bjms.v16i3.32863
22. Menhas R, Dai J, Ashraf MA. et al. Physical inactivity, non-communicable diseases and national fitness plan of China for physical activity. Risk Manag Healthc Policy. 2021:2319–2331. doi:10.2147/RMHP.S258660
23. Oluwasanu AO, Akinyemi JO, Oluwasanu MM, et al. Temporal trends in overweight and obesity and chronic disease risks among adolescents and young adults: a ten-year review at a tertiary institution in Nigeria. PLoS One. 2023;18(4):e0283210. doi:10.1371/journal.pone.0283210
24. Nagheer D, Irvin R, Younger-Coleman N. Overview of the prevalence and Associated Risk, factors of Lifestyle Diseases in University students. Int J Clin Med. 2017;8(5):344–352. doi:10.4236/ijcm.2017.85032
25. Alnuwaysir N, Alturki H, Almalki B, Bin Amer L, Alotaibi R. Review of multimorbidity in Saudi Arabia: prevalence, gender differences, and common chronic diseases. J Multimorbidity Comorbidity. 2025;15:26335565251367588. doi:10.1177/26335565251367587
26. Bagby SP, Martin D, Chung ST, Rajapakse N. From the outside in: biological mechanisms linking social and environmental exposures to chronic disease and to health disparities. Am J Public Health. 2019;109(S1):S56–S63. doi:10.2105/AJPH.2018.304864
27. Short SE, Zacher M. Women’s health: population patterns and social determinants. Annu Rev Sociol. 2022;48(1):277–298. doi:10.1146/annurev-soc-030320-034200
28. Lam PH, Chen E, Chiang JJ, Miller GE, Nelson KE. Socioeconomic disadvantage, chronic stress, and proinflammatory phenotype: an integrative data analysis across the lifecourse. PNAS Nexus. 2022;1(4):pgac219. doi:10.1093/pnasnexus/pgac219
29. Al-Qahtani MF. Assessing healthy lifestyles in female university students: Eastern province, Saudi Arabia. Saudi J Heal Sci. 2017;6(3):169–175. doi:10.4103/sjhs.sjhs_102_17
30. Al-Hanawi MK, Keetile M. Socio-economic and demographic correlates of non-communicable disease risk factors among adults in Saudi Arabia. Front Med. 2021;8. doi:10.3389/fmed.2021.605912
31. Zaher A, Ali S, Alalwan M, Buzaid A, Aldandan H. Prevalence of chronic illnesses among medical students at King Faisal University (KFU) and their impact on academic performance. Int J Sci Res. 2016;5:2319–2324.
32. Alharbi SM, Alanazi AA, Alamri AS, et al. Obstructive sleep apnea: prevalence, risk factors, and impact on the academic performance of medical students at a Saudi Arabian University. Saudi J Med Med Sci. 2025;13(1):61–67. doi:10.4103/sjmms.sjmms_5_24
33. Bashir MM, Alshamsi M, Almahrooqi S, et al. Prevalence of chronic diseases among United Arab Emirates University students: cross-sectional study. Eur J Public Health. 2022;32(Supplement_3):ckac131–142. doi:10.1093/eurpub/ckac131.142
34. Alsuni Z, Alhubaishi A, Othman G, et al. Understanding the struggles of first-generation medical students and interns: a cross-sectional study in Saudi Arabia. J Med Life. 2024;17(10):934. doi:10.25122/jml-2024-0310
35. Indrayathi PA, Kovács E, Januraga PP, Pradnyani PE, Rahyuda I, Kolozsvári LR. Exploring determinants of well-being among international students: a basis for health policy and risk management in higher education. Risk Manag Healthc Policy. 2025;Volume 18:3359–3370. doi:10.2147/RMHP.S534448
36. Dabbagh R, Alwatban L, Alrubaiaan M, et al. Depression, stress, anxiety and burnout among undergraduate and postgraduate medical trainees in Saudi Arabia over two decades: a systematic review. Med Teach. 2023;45(5):499–509. doi:10.1080/0142159X.2022.2139669
37. Adam TR, Hamed AM, Mohammed HSM, et al. Prevalence of childhood obesity among children and adolescents in Saudi Arabia: a systematic review. Cureus. 2024;16(9). doi:10.7759/cureus.70135
38. Rahamathulla MP. Frequency and awareness of risk factors of non-communicable diseases among university students in Saudi Arabia. Pak J Med Sci. 2020;36(4):740.
39. Gazibara T, Pekmezović T, Popović A, Paunić M, Kisić-Tepavčević D. Chronic diseases among university students: prevalence, patterns and impact on health-related quality of life. Vojnosanit Pregl. 2018;75(12):1178–1184. doi:10.2298/VSP160920050G
40. Al-Hazzaa HM, Abahussain NA, Al-Sobayel HI, Qahwaji DM, Musaiger AO. Lifestyle factors associated with overweight and obesity among Saudi adolescents. BMC Public Health. 2012;12(1):354. doi:10.1186/1471-2458-12-354
41. Bigna JJ, Noubiap JJ. The rising burden of non-communicable diseases in sub-Saharan Africa. Lancet Glob Heal. 2019;7(10):e1295–e1296. doi:10.1016/S2214-109X(19)30370-5
42. Adigwe OP, Onoja SO, Onavbavba G. A critical review of sickle cell disease burden and challenges in sub-Saharan Africa. J Blood Med. 2023;Volume 14:367–376. doi:10.2147/JBM.S406196
43. Bruffaerts R, Mortier P, Kiekens G, et al. Mental health problems in college freshmen: prevalence and academic functioning. J Affect Disord. 2018;225:97–103. doi:10.1016/j.jad.2017.07.044
44. Abuhendi N, Qush A, Naji F, et al. Genetic polymorphisms associated with type 2 diabetes in the Arab world: a systematic review and meta-analysis. Diabet Res Clin Pract. 2019;151:198–208. doi:10.1016/j.diabres.2019.03.037
45. Alqunaibet A, AlMahmassani HA, Alghnam S, et al. Burden of chronic diseases and associated risk factors among adults in Saudi Arabia: results from a national telephone survey. BMC Public Health. 2026;26(1):1094. doi:10.1186/s12889-026-26234-6
46. Almubark SA, Almubark RA, Althumiri NA, et al. Exploring the sociodemographic and behavioral status of people living with hypercholesterolemia in Saudi Arabia: a nation-wide cross-sectional study. Risk Manag Healthc Policy. 2023;Volume 16:889–898. doi:10.2147/RMHP.S401989
47. Ho YCL, Mahirah D, Ho CZH, Thumboo J. The role of the family in health promotion: a scoping review of models and mechanisms. Health Promot Int. 2022;37(6):daac119. doi:10.1093/heapro/daac119
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Correlation of Circadian Rhythms of Heart Rate Variability Indices with Stress, Mood, and Sleep Status in Female Medical Workers with Night Shifts
Deng S, Wang Q, Fan J, Yang X, Mei J, Lu J, Chen G, Yang Y, Liu W, Wang R, Han Y, Sheng R, Wang W, Ba L, Ding F
Nature and Science of Sleep 2022, 14:1769-1781
Published Date: 6 October 2022
Examining Physical Wellness as the Fundamental Element for Achieving Holistic Well-Being in Older Persons: Review of Literature and Practical Application in Daily Life
Hung ST, Cheng YC, Wu CC, Su CH
Journal of Multidisciplinary Healthcare 2023, 16:1889-1904
Published Date: 5 July 2023
Declined Live Birth Rate from in vitro Fertilization Fresh Cycles Performed During Chinese New Year Holiday Season
Zhai J, Zhang J, He J, Li G, Hao G
Risk Management and Healthcare Policy 2023, 16:1703-1718
Published Date: 31 August 2023
Prevalence of Obesity and Lifestyle Risk Factors Following Two Years’ COVID-19 Related Service Closure at Wellness Center, Primary Health Care
Musa S, Al-Dahshan A, Singh R
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3851-3868
Published Date: 29 November 2023
Impact of Replacing Sedentary Behavior with Physical Activity and Sleep on Stroke Risk: A Prospective Cohort Study
Dong XF, Zhang Q, Wei JN, Zhou QY, Yang FJY, Liu YJ, Li YS, Sun CQ
Nature and Science of Sleep 2024, 16:1611-1622
Published Date: 13 October 2024