Back to Journals » ClinicoEconomics and Outcomes Research » Volume 18
Characteristics and Utilization Patterns of Medicare Beneficiaries Initiating Long-Acting Injectable Antipsychotic Medications
Authors Grabner M ![]() , Chiang YY, Teng CC, dosReis S
, Chiang YY, Teng CC, dosReis S ![]() , Harris KM
, Harris KM
Received 13 September 2025
Accepted for publication 8 January 2026
Published 17 February 2026 Volume 2026:18 567370
DOI https://doi.org/10.2147/CEOR.S567370
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Michael Grabner,1 Yueh-Yi Chiang,2 Chia-Chen Teng,1 Susan dosReis,2 Katherine M Harris1
1Carelon Research, Wilmington, DE, USA; 2Department of Practice, Sciences, and Health Outcomes Research, University of Maryland School of Pharmacy, Baltimore, MD, USA
Correspondence: Michael Grabner, Carelon Research, 123 Justison Street, Suite 200, Wilmington, DE 19801, USA, Email [email protected]
Purpose: US Medicare beneficiaries in fee-for-service (FFS) and Medicare Advantage (MA) plans may differ in sociodemographics, treatment patterns, and healthcare costs, but real-world evidence is limited. Our objective was to gain a holistic understanding of Medicare beneficiaries using long-acting injectable antipsychotic medications (LAI-AM) as a case study.
Patients and Methods: This observational study describes two distinct cohorts of new LAI-AM users enrolled in FFS or MA plans from July-2017 through December-2020. Data were extracted from the Centers for Medicare & Medicaid Services’ Chronic Conditions Data Warehouse (for FFS) and the Carelon Research Healthcare Integrated Research Database® (for MA). Setting the first LAI-AM claim as index date, we identified adult beneficiaries enrolled for ≥ 12-months before (baseline) and after (follow-up) the index date. We described LAI-AM users’ sociodemographic and clinical characteristics, medication adherence (proportion of days covered [PDC]), and healthcare costs.
Results: We identified 3180 FFS- and 525 MA-enrolled LAI-AM initiators. Compared to the MA cohort, the FFS cohort was younger (mean 49 vs 53 years), had more males (56% vs 45%), and had more living in the South and West. Many had a depressive mood disorder (70%) and/or substance use disorder (40%). The mean PDC was 0.52 (SD 0.34) for FFS and 0.46 (SD 0.34) for MA. Only 33% (FFS)/27% (MA) had a PDC≥ 0.8 (adherent). In both cohorts, total medical costs decreased and total pharmacy costs increased from baseline to follow-up.
Conclusion: Differences in sociodemographic characteristics between FFS and MA plan LAI-AM initiators did not correspond with different patterns or costs of treatment.
Keywords: long-acting injectable antipsychotics, Medicare, real-world evidence, schizophrenia
Introduction
Schizophrenia is a serious chronic, and often disabling, condition afflicting 1.2% (3.7 million) of US adults aged 18–65, according to data from 2020–2022.1 Symptoms typically emerge in late adolescence through early adulthood and include hallucinations, delusions, thought disorders, reduced expression of emotions, social instability, motor impairment, and cognitive impairment.2–4 Approximately half of individuals with schizophrenia have a co-occurring mental or behavioral disorder.5 The economic burden of schizophrenia was estimated at $343 billion in 2019 using a societal perspective.6
Antipsychotic medications are the first-line treatment for adults with schizophrenia.7 As of 2024, 25 antipsychotic agents have a US Food and Drug Administration (FDA)-approved indication for schizophrenia, of which 11 have a long-acting injectable (LAI) formulation. Administered by licensed healthcare providers every 2 to 8 weeks,8 LAI antipsychotic medications (LAI-AMs) are associated with higher adherence compared to oral-AMs.9,10
There are benefits and cost offsets for LAI-AMs. A meta-analysis published in 2024 found that LAI-AMs and oral-AMs were comparable in relapse prevention and treatment-emergent adverse events, but, in a subset of higher-quality studies of patients with extrapyramidal symptoms, LAI-AMs were superior to oral-AMs in preventing relapse and hospitalization.11 Another meta-analysis published in 2021 examining similar outcomes was less conclusive.12 Economic studies based on health care claims data, primarily in populations covered by Medicaid, show that reductions in hospitalizations, ED visits, and healthcare costs offset the higher acquisition costs of LAI-AMs.13 The benefits and cost offsets could have a significant impact on the Medicare population, as nearly half of adults with schizophrenia are covered under Medicare.14 However, the relatively few real-world studies on this topic used older (2005 to 2019) or narrower samples of Medicare beneficiaries enrolled in either traditional fee-for-service (FFS) Medicare or Medicare Advantage (MA).15–19
Our study extends the literature by comparing LAI-AM treatment patterns and health and economic outcomes among Medicare FFS and MA enrollees who initiated LAIs between 2016 and 2021. Inclusion of both FFS and MA samples allows a comprehensive assessment of the Medicare population and of the similarities and differences between FFS and MA.
Materials and Methods
Study Design and Data Sources
A retrospective study design utilized US administrative insurance claims data to derive two distinct cohorts of LAI-AM users with MA or FFS health plan coverage. The study leveraged two real-world data sources: the Healthcare Integrated Research Database (HIRD®) and the Centers for Medicare & Medicaid Services (CMS) Medicare Administrative database.
The HIRD integrates various data elements, including enrollment files, medical and pharmacy claims, outpatient laboratory data, and Electronic Health Records (EHR) for over 90 million members across the United States.20 These data are derived from routine clinical care and billing/reimbursement processes for members with employer-sponsored (the predominant portion), individually purchased, or public health insurance coverage. The demographic composition of the 2020 HIRD population is broadly representative of the 2020 US Census in terms of sex, age, and geographic region, although there is limited representation concerning race/ethnicity.21
The CMS database encompassed a 5% sample of the US Medicare population. The data comprise all paid claims for healthcare services, covering inpatient and outpatient settings, skilled nursing facilities, hospice, home health services, durable medical equipment, and prescription drugs for elderly and disabled US citizens.22–24 The CMS Medicare data, accessible through the Chronic Conditions Data Warehouse (CCW), permits dataset linkage via an encrypted beneficiary identifier.23 The CMS data was restricted to those enrolled in FFS plans.
The study incorporated individual-level race/ethnicity data as well as area-level social drivers of health (SDOH) from the American Community Survey (ACS) and the National Center for Health Statistics (NCHS) Urban-Rural Classification Scheme. Please refer to the Supplementary Methods 1 for further details.
Researchers accessed data in the format of a limited data set for which data use agreements were in place with the covered entities in compliance with the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. The study protocol for the FFS population was deemed exempt by the Institutional Review Board (IRB) of the University of Maryland Baltimore. An IRB did not review the study protocol for the MA population since only a limited data set was accessed by Carelon Research.
Study Population and Time Periods
The study period was 01-Jan-2016 through 31-Dec-2021. We identified new LAI-AM use during the cohort accrual period of 01-Jan-2017 through 31-Dec-2020, which allowed a twelve-month baseline for the earliest date and a twelve-month follow-up for the latest date of LAI-AM initiation. The date of the first observed medical or pharmacy claim for an LAI-AM within this period was designated as the index date. The baseline period included twelve months prior to the index date (exclusive) and outcomes were assessed over a twelve-month follow-up period from the index date (inclusive) (Supplementary Figure 1).
Patients were included if they were ≥18 years of age on the index date and had ≥12 months of continuous baseline and ≥12 months of continuous follow-up medical and pharmacy health plan enrollment. Patients were excluded if they had claims for >1 type of LAI-AM on the index date, or any claims for LAI-AMs during the baseline period.
Variable Definitions
Sociodemographic and Clinical Characteristics
Demographic characteristics, identified on the index date, included sex, age, geographical region of residence, race/ethnicity, the diversity index (a composite of the fractions of members belonging to each available race/ethnicity category),25 and enrollment features (MA: dual eligible special needs plans [D-SNPs]; FFS: dual eligibility status, original entitlement reason). Selected SDOH variables at the Census tract level (ACS) or county level (NCHS) included economic stability, education access and quality, neighborhood and built environment, an aggregated socioeconomic status (SES) index,26 and urbanicity. Baseline clinical characteristics included 30 CCW chronic conditions,27 mental health comorbidities, and schizophrenia type on or before LAI-AM initiation (see Supplementary Table 2 for a list of all assessed schizophrenia types).
Treatment Patterns
Type of LAI-AM, brand vs generic, specialty of the treating/prescribing provider, and administration site were collected on index date. Psychotropic medication use and non-pharmacologic interventions (such as psychotherapy) were assessed at baseline and follow-up. LAI-AM adherence during follow-up was measured using proportion of days covered (PDC), calculated as the sum of the number of days with available supply of the index LAI-AM divided by the number of days in the follow-up period (ie, 365). Days’ supply was imputed for all instances where LAI-AM administration was reimbursed under the medical benefit and therefore appeared as a medical claim (see Supplementary Methods 1). Patients with PDC ≥0.8 were considered adherent.28,29 LAI-AM persistence was measured by the number of continuous therapy days from the index date to the end of the follow-up period or discontinuation, whichever came first. A gap of 45 days or more after the previous fill’s exhaustion and the next LAI-AM fill defined discontinuation. Patients who discontinued their index LAI-AM and subsequently initiated a non-index LAI-AM at any time during the remainder of follow-up were considered to have switched.
Healthcare Resource Utilization (HCRU) and Costs
All-cause and mental health-related HCRU and costs were assessed during baseline and follow-up. HCRU included inpatient visits with length of stay (LOS), emergency department (ED) visits, outpatient visits (overall as well as in three selected subcategories of office visits, telehealth visits, and ambulance transports), and outpatient pharmacy fills. All-cause medical HCRU and costs included medical claims with any diagnosis codes, while all-cause pharmacy HCRU and costs included pharmacy fills for any drug. Healthcare costs, adjusted to 2022 US dollars (USD), included the total of health plan paid and patient paid amounts. Mental health-related HCRU and costs included all medical claims with diagnosis codes of schizophrenia or any other mental health-related conditions in any position on the claim, and any medical or pharmacy claims for psychotropic medications.
Statistical Analyses
All analyses were conducted separately for MA and FFS beneficiaries, ensuring that datasets remained independent, per data use agreement specifications. Therefore, no statistical comparisons were made between the two populations. All statistical analyses were exploratory and descriptive and performed using the Instant Health Data platform (Panalgo, Boston, MA) and Statistical Analysis System (SAS), Enterprise Guide version 8.3 (SAS Institute Inc., Cary, NC) for the MA cohort; SAS 9.4 (SAS Institute Inc., Cary, NC) was used for the FFS cohort.
Descriptive statistics were used for most analyses, including means and standard deviations (SD) for continuous variables, median and interquartile range (IQR) when appropriate, and frequencies for categorical values. Where missing data were present for variables, the percentage missing was reported as its own category, and no imputation was undertaken.
To examine factors associated with adherence to LAI-AMs, we performed multivariable logistic regression analyses with adherence (adherent [PDC ≥80%] = 1) as the dependent variable. A pre-specified list of covariates, identified based on literature and clinical relevance, was included in the model to assess associations between baseline characteristics and LAI-AM adherence.
A sensitivity analysis was conducted to understand the demographic characteristics and utilization patterns of LAI-AM users in a broader sample. Specifically, we analyzed selected demographic and treatment pattern characteristics after removing the requirements for continuous enrollment and no prior LAI-AM use. Please refer to Supplementary Table 7 for the results of this sensitivity analysis.
Results
Sociodemographic and Clinical Characteristics
We identified 525 MA-enrolled and 3,180 FFS-enrolled new LAI-AM users who met the study criteria. In both cohorts, the most attrition occurred after imposing 12 months of continuous health plan enrollment pre- and post-index date (Supplementary Figure 2).
The MA cohort was 45% male, compared with 56% male in the FFS cohort. Mean age in the MA cohort was approximately 5 years older than the FFS cohort (53.8 [SD 15.1] vs 48.6 [SD 15.3]). Individuals with dual eligibility for both Medicaid and Medicare constituted the majority of the FFS cohort (87%) and accounted for at least 47% of the MA cohort. More recent years accounted for a larger share of new LAI-AM users in the MA cohort, and a declining share in the FFS cohort. Most individuals in both cohorts were non-Hispanic/Latino White (MA 66% vs FFS 59%). The racial diversity index (MA 50% vs FFS 57%) and the proportion of patients with higher socioeconomic status were higher in the FFS cohort (Table 1 and Supplementary Table 1).
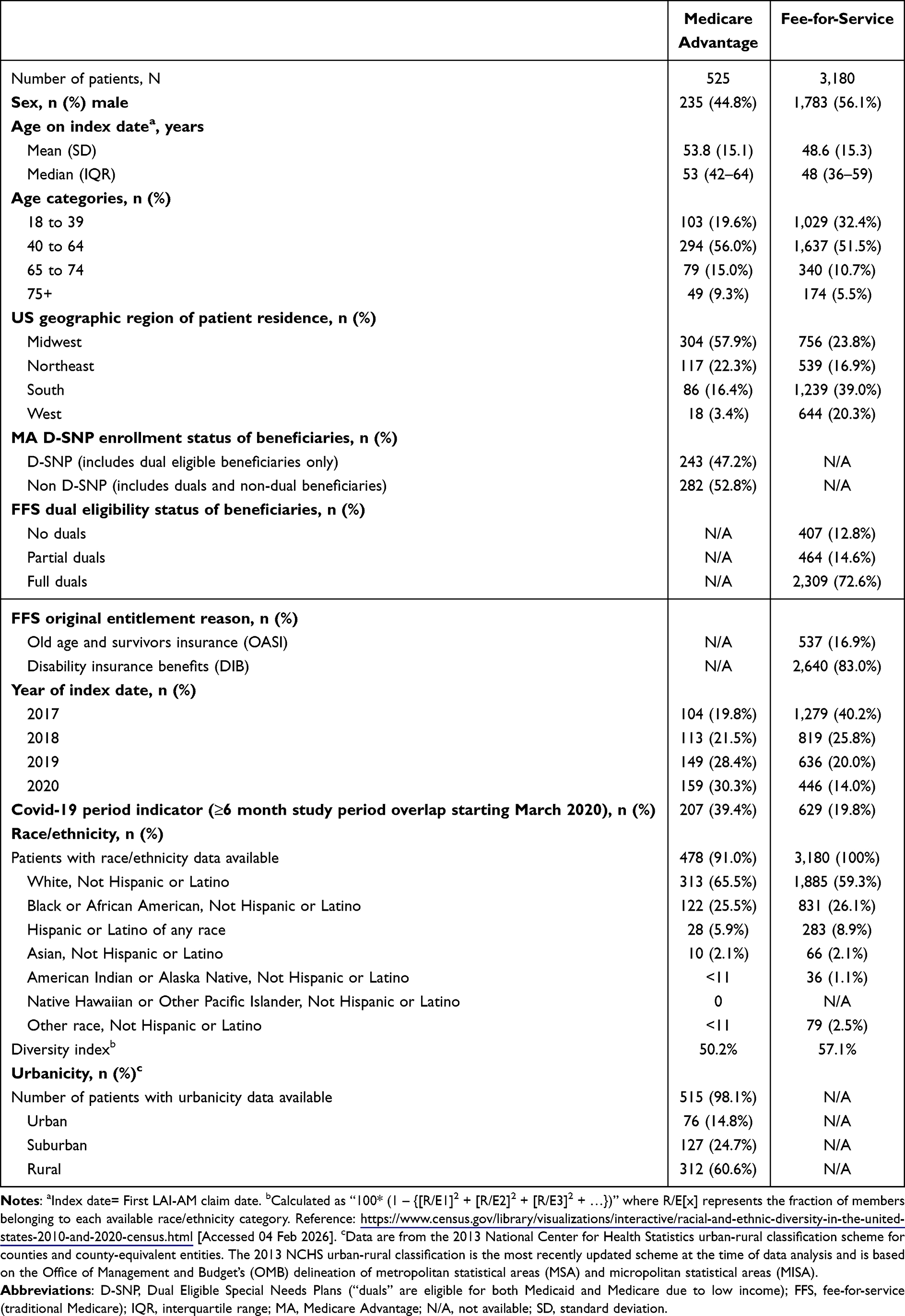 |
Table 1 Sociodemographic Characteristics |
Most individuals (MA 72% vs FFS 78%) had evidence of schizophrenia at baseline (Supplementary Table 2). Nearly half of individuals in both cohorts had other mental health comorbidities, including anxiety disorders, bipolar disorder, and depression. We observed substantial non-psychiatric comorbidity burden in both cohorts as well, with the most common being hypertension (MA 66% vs FFS 53%), hyperlipidemia (MA 52% vs FFS 44%), and overweight/obesity (MA 42% vs FFS 36%). Overall, a larger proportion of the MA cohort had mental health and medical comorbidities relative to the FFS cohort (Figure 1). The mean (SD) number of all comorbidities was 5.4 (3.3) in MA and 4.6 (3.5) in FFS.
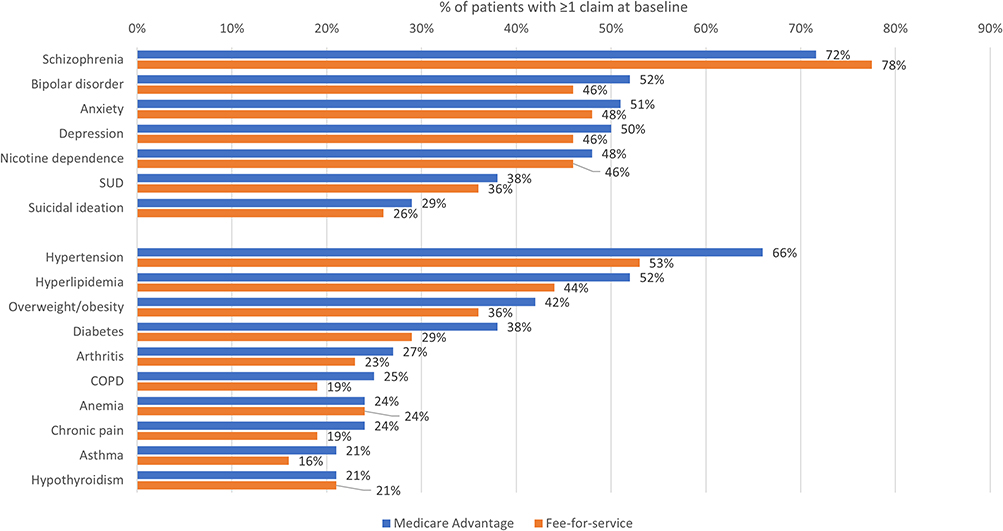 |
Figure 1 Mental health and other co-occurring conditions. Notes: COPD, Chronic Obstructive Pulmonary Disease; SUD, Substance Use Disorder. |
Treatment Patterns
Table 2 presents baseline psychotropic medication use as well as index LAI-AM utilization. Over 80% of individuals in both cohorts had evidence of non-LAI antipsychotic use at baseline, suggesting that LAI-AMs were not used as first-line treatments in this population. Additionally, over 60% of individuals in both cohorts received non-pharmacologic treatment such as psychotherapy (Supplementary Table 3). Approximately three-fourths of both cohorts initiated atypical LAI-AMs (MA 78% vs FFS 73%). In both cohorts, the most common atypical LAI-AM was paliperidone palmitate (MA 38% vs FFS 36%). Index LAI-AMs were predominantly prescribed by psychiatrists (MA 44% vs FFS 50%; also including a small number of psychologists), and nearly all (90%) of index LAI-AMs were identified through pharmacy claims. In FFS, 54% of prescriptions were filled in community pharmacies and 37% in long-term care pharmacies (the rest occurred in medical settings).
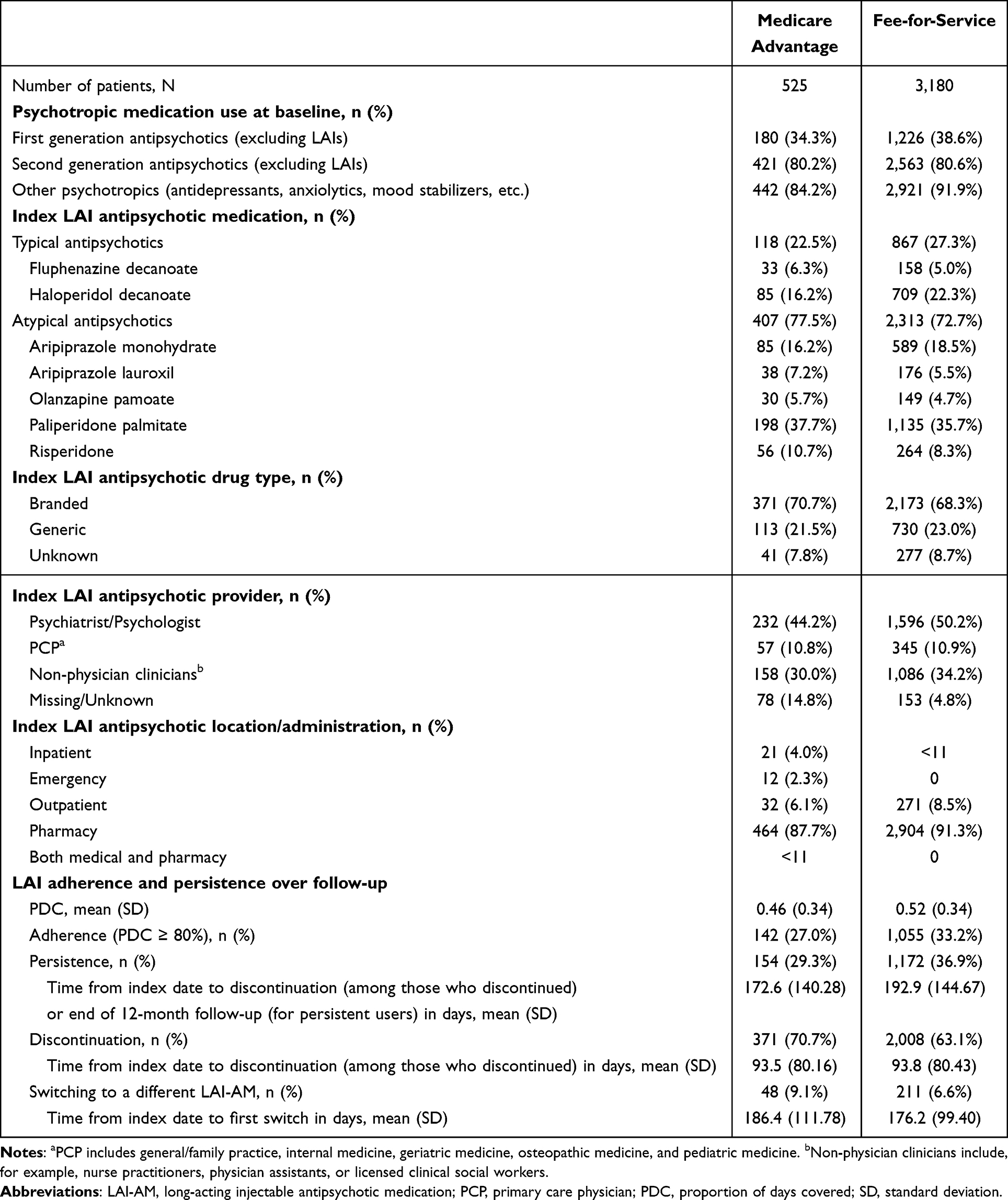 |
Table 2 Mental Health Pharmacotherapy Treatment Patterns |
In both MA and FFS cohorts, we observed low adherence and persistence to index LAI-AMs over the one-year follow-up period. For MA the mean PDC was 0.46 (SD 0.34) and for FFS it was 0.52 (SD 0.34). 27% of the MA cohort and 33% of the FFS cohort were classified as adherent (PDC ≥0.80); the fraction of patients considered persistent was similar (MA 29% vs FFS 37%).
Significant correlates of adherence in the MA cohort were male (odds ratio [OR]: 1.28; 95% confidence interval [CI]: 1.03–1.60), ages 18–39 years (OR: 1.52; 95% CI: 1.02–2.28), atypical index LAI-AM (OR: 1.47; 95% CI: 1.09–1.99), behavioral health comorbidities (OR: 0.84; 95% CI: 0.75–0.94), and anxiolytic, sedative, or hypnotic medication use (OR: 0.78; 95% CI: 0.62–0.99). Similar odds ratios for these factors were observed in the FFS cohort (Figure 2 and Supplementary Table 4).
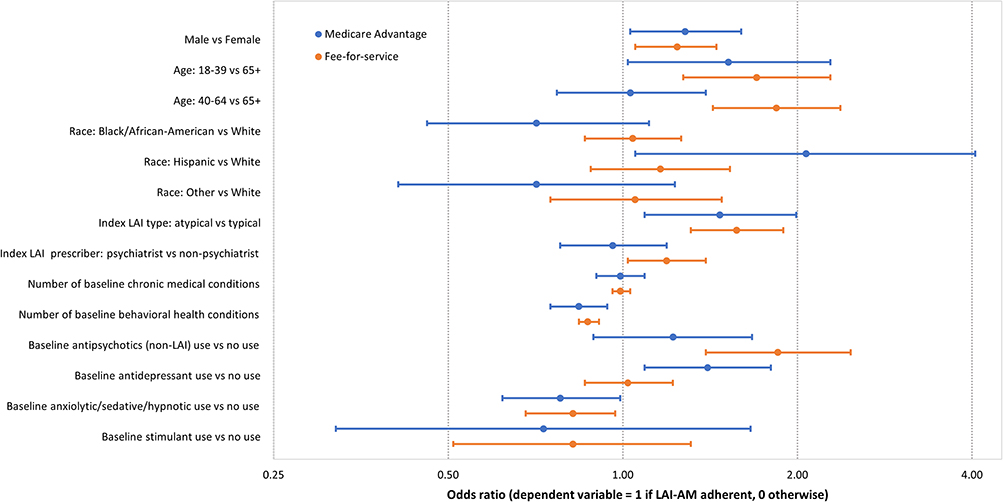 |
Figure 2 Association between characteristics and LAI-AM adherence. Notes: Results are based on two independent logistic regression models (one per cohort). Other characteristics adjusted for in the model included socioeconomic status category, US region of residence, LAI antipsychotic index year, baseline schizophrenia diagnosis, and baseline Rx counts (class level). We excluded individuals (MA: n=2 and FFS: n=21) with missing baseline characteristics (eg, SES index). |
HCRU and Costs
Supplementary Table 5a presents baseline and follow-up all-cause HCRU for the MA and FFS cohorts. At baseline, >60% of both cohorts had at least one inpatient or ED visit. The prevalence of inpatient and ED visits was lower in the follow-up period relative to baseline, with similar patterns in both cohorts. Relative to proportions in the FFS cohort, a smaller proportion of the MA cohort had psychiatrist office visits while a larger proportion of the MA cohort had a PCP office visit. Less than 20% of the MA and FFS cohort had at least one telehealth visit at baseline; however, the proportion using telehealth in both cohorts doubled during follow-up. Overall prescription drug use was high (>95%) in both cohorts at both baseline and follow-up. The patterns of all-cause and mental health-related HCRU pre- and post-index LAI-AM were similar (Supplementary Table 5b).
Figure 3 and Supplementary Table 6 present the baseline and follow-up mean one-year healthcare costs per beneficiary in the MA and FFS cohorts. At baseline, the all-cause mean (SD) one-year total costs (ie, medical and pharmacy costs) were $40,725 (SD $44,457) for the MA cohort and $37,663 (SD $40,374) for the FFS cohort. Inpatient hospitalization and pharmacy costs were the major cost components in both cohorts at baseline. Patient out-of-pocket payments accounted for 10–11% of medical costs and 2–3% of pharmacy costs. Total medical costs decreased from baseline to follow-up by 34% in the MA cohort and 26% in the FFS cohort, while total pharmacy costs increased by 124% for MA and 168% for FFS. Patient out-of-pocket payments decreased substantially for medical utilization and increased slightly for pharmacy fills. Mental health-related costs showed similar patterns as all-cause costs.
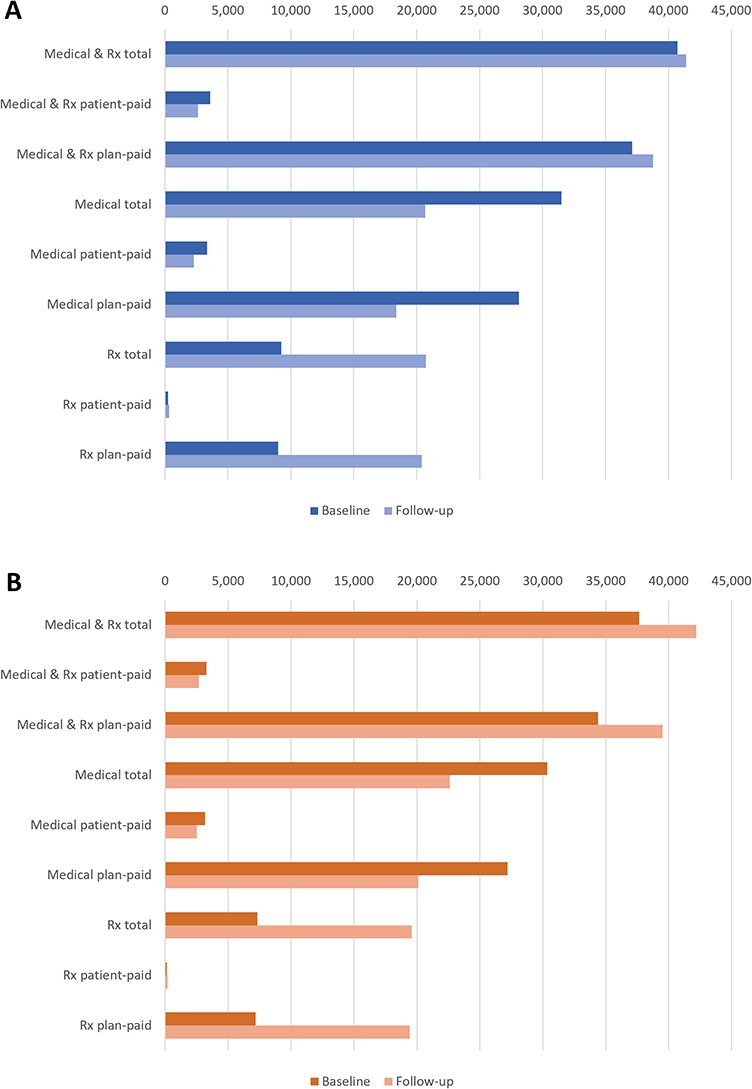 |
Figure 3 Baseline (1 year) and follow-up (1 year) healthcare costs (2022 USD) per beneficiary; Panel (A) Medicare Advantage; Panel (B) Fee-for-service. Notes: Rx, pharmacy; USD, US Dollar. Total costs are the sum of patient-paid and plan-paid amounts. |
Discussion
This study compared adult initiators of LAI-AMs enrolled in MA and FFS plan in terms of sociodemographic characteristics, medical conditions, LAI-AM adherence, healthcare utilization, and healthcare costs. Key findings are that LAI-AM adherence was low (ie, 27% of MA and 33% of FFS had a PDC ≥0.8), the prevalence of inpatient and ED visits was lower in the follow-up period after LAI-AM initiation for both MA and FFS beneficiaries, and health care costs were similar for MA and FFS. These findings offer important insights on the contributions of benefit design and care management in explaining LAI-AM utilization patterns and outcomes. MA plans that are contracted with CMS encourage care management to promote cost-efficient attainment of quality benchmarks,30 whereas CMS reimburses FFS providers based on a pre-established fee schedule. Our study period followed the implementation of the Medicare Access and CHIP Reauthorization Act (MACRA) of 2015, which encouraged individual providers to engage in quality improvement programs. We discuss the relevance of our findings within this policy context.
Observed differences in baseline characteristics across MA and FFS cohorts may reflect geographic variation in the availability of MA plans and the preferences of individual beneficiaries.31 While most patients in both groups were non-Hispanic White, FFS beneficiaries were more diverse and resided in higher SES areas. MA beneficiaries were roughly five years older than FFS beneficiaries, consistent with the overall trend toward MA enrollment of dual-eligibles and those with disabilities, reflecting high medical need.32 Even so, dual-eligibles comprised the majority of both MA and FFS. At the same time, the proportion with co-occurring medical and mental health conditions was similar across MA and FFS beneficiaries.
Index LAI-AM use in 2017 and 2020 comprised 40% and 14%, respectively, of the FFS cohort, while for the MA cohort the percentages were 20% and 30%. This may reflect a growing role of managed care in LAI-AM initiation. LAI-AM adherence for MA and FFS beneficiaries (PDC=0.46 and 0.52, with 27% and 33% having PDC≥0.80, respectively) was well below what is generally considered adherent. Three earlier studies of MA and/or FFS beneficiaries reported LAI-AM adherence estimates that were higher than our findings; these analyses used patient cohorts and adherence definitions different to ours in ways that may have increased adherence estimates (mean PDC for MA paliperidone palmitate users of 0.66, with 48% of patients having PDC≥0.8 using 2009–2014 data;16 PDC≥0.8 for 81% of FFS users, combining oral and LAI-AMs, during 2019;17 mean medication possession ratio [MPR] of 0.68 among patients with Medicare supplemental insurance from 2005–2010).19 One other study reported a mean PDC=0.69 among Medicaid enrollees in South Carolina initiating LAI-AMs between 2015–2018.33
Low adherence may reflect gaps in continuous access to settings where LAI-AMs are administered, rather than challenges with maintaining a medication routine. It is also known that family and caregiver support are essential to sustain a treatment plan.34 Most LAI-AMs were dispensed from outpatient pharmacies, but our data did not document where the LAI-AMs were administered or by whom, eg, physician, pharmacist, nurse, etc. Without this information it is not possible to draw conclusions about the relationship between the accessibility of LAI-AMs and the low adherence rates we observed.
Access to specialty providers differed between MA and FFS beneficiaries. The proportion visiting psychiatry specialty providers was lower among MA beneficiaries compared with their FFS counterparts. This difference may indicate greater use of alternative providers in MA plans to manage schizophrenia and related psychotic disorders. Consistent with prior research, inpatient and ED utilization was lower following LAI-AM initiation in both MA and FFS cohorts.11,12 It is possible that inpatient or ED episodes may motivate a switch from an oral antipsychotic to, or new initiation of, an LAI-AM.9,35
Although overall healthcare costs were similar for MA and FFS beneficiaries, the costs shifted in the period following LAI-AM initiation. Medical costs decreased during follow-up, while pharmacy costs increased. Of note, the payment structure differs between MA and FFS which limits direct comparability of costs.36
This study had unique strengths. The data sources captured a nationally representative sample of FFS Medicare beneficiaries and a cohort of MA enrollees from a large health insurer that reflects the age and sex distribution in US Census data. The use of RWD contributes valuable information about treatment patterns, healthcare resource utilization and costs for two populations that often are not examined jointly. Inclusion of both MA and FFS beneficiaries informed similarities and differences in the characteristics and treatment utilization for Medicare beneficiaries with these distinct health benefit plans.
It is also important to acknowledge study limitations. As with all claims-based studies, the potential for coding errors and the lack of clinical data (eg, on disease severity) introduces uncertainty that can distort the interpretation of our findings. Potentially important attributes, such as care management practices, reasons for initiating or discontinuing an LAI-AIM, health plan benefit design (including the structure of behavioral health coverage), individual-level health-related social needs, family history, and social services utilization were not available in the data. Such information would provide important context underpinning the observed trends. Also, the requirement of 12-month continuous enrollment after index date may have eliminated individuals newly enrolled in their health plans. Family and caregiver involvement or other supportive services were not available in the data, yet these factors could have influenced adherence. This pre-post study described real-world associations between LAI-AM treatment and selected health outcomes; further research is required to establish causal relationships in these observational data. The study period overlapped with the start of the COVID-19 pandemic when access to medical care was affected, which may have reduced LAI-AM use and adherence. While we included a comprehensive Medicare beneficiary population, our study results may not generalize to populations with commercial or no insurance. The MA sample had limited geographical representation stemming from plans’ decisions to engage in the MA market; the lack of continuous enrollment suggested a high amount of switching to other health plans in this population.
Conclusion
This study provides new evidence on LAI-AM treatment patterns in a large, generalizable cohort of US Medicare enrollees in FFS and MA plans, expending on the existing limited literature in this population. LAI-AM initiators in MA and FFS plans were similar in terms of demographic characteristics, prevalence of mental health conditions, and LAI-AM formulation; adherence to LAI-AMs was low. In both FFS and MA plans, the reduction in medical expenditures from lower inpatient and ED use was balanced by increased pharmacy spending. Future research should investigate access barriers to LAI-AMs that may underlie the observed low adherence (eg, does the lack of self-administration options negatively impact adherence), experiences of long-term LAI-AM users, and impacts on total costs of care of introductions of generic LAI formulations following the end of our study period. Another topic of interest is the selection of patients into MA and FFS and its impact on LAI-AM use.
Data Sharing Statement
The MA data that support the findings of this study are available from Carelon Research, but restrictions apply to the availability of these data to external sources, and therefore they are not publicly available. MA data may be made available through the corresponding author upon reasonable request and with permission of Carelon Research.
The FFS data generated in this study are not publicly available. The data used for this study were obtained under a data use agreement with the Centers for Medicare and Medicaid Services, and cannot be made publicly available.
Ethics Approval and Consent to Participate
Not required. Carelon Research’s federalwide assurance requires ethics review only for federally funded studies. Throughout this study, researchers’ access was limited to data removed of all identifiers to ensure confidentiality. No study subjects were contacted and informed consent was not obtained. Data use agreements were in place with the covered entities in compliance with the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. The study protocol for the FFS population was deemed exempt by the Institutional Review Board (IRB) of the University of Maryland Baltimore. An IRB did not review the study protocol for the MA population since only a limited data set was accessed by Carelon Research.
Acknowledgments
Elizabeth Marks, an employee of Carelon Research, provided editorial support for this manuscript. Partial findings from this study were previously presented at the annual meeting of the International Society for Pharmacoeconomics and Outcomes Research, held May 5-8, 2024, in Atlanta, GA, USA, and the annual meeting of the International Society for Pharmacoepidemiology, held August 24-28, 2024, in Berlin, Germany. The full study protocol is available on the RWE Registry at https://osf.io/ejrn7.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for the conduct of this study.
Disclosure
MG, CCT, KH are employees of Carelon Research (a wholly owned subsidiary of Elevance Health), which conducts health outcomes research with both internal and external funding, including a variety of private and public entities. MG, CCT, KH are shareholders of Elevance Health. SdR receives funding from GlaxoSmithKline for a project unrelated to the study described in this manuscript and conducts research that is funded by state and federal agencies. The authors report no other conflicts of interest in this work.
References
1. Ringeisen H, Edlund M, Guyer H, et al. Mental and substance use disorders prevalence study: ōFindings report RTI International;2023.
2. Hollis C, Rapoport J. Child and Adolescent Schizophrenia. In: Weinberger D, Harrison P, editors. Schizophrenia, 3rd Ed. London: Blackwell; 2008:24–13.
3. McGrath J, Saha S, Chant D, Welham J. Schizophrenia: a concise overview of incidence, prevalence, and mortality. Epidemiol Rev. 2008;30:67–76. doi:10.1093/epirev/mxn001
4. National Institute of Mental Health. Schizophrenia. U.S. department of health and human services. Available from: https://www.nimh.nih.gov/health/topics/schizophrenia.
5. Tsai J, Rosenheck RA. Psychiatric comorbidity among adults with schizophrenia: a latent class analysis. Psychiatry Res. 2013;210(1):16–20. doi:10.1016/j.psychres.2013.05.013
6. Kadakia A, Catillon M, Fan Q, et al. The economic burden of schizophrenia in the United States. J Clin Psychiatry. 2022;83(6). doi:10.4088/JCP.22m14458
7. Ameer M, Patel P, Saadabadi A. Neuroleptic Medications. In: In. StatPearls [Internet]. Treasure Island, FL:StatPearls Publishing; 2024
8. Riboldi I, Cavaleri D, Capogrosso CA, Crocamo C, Bartoli F, Carrà G. Practical guidance for the use of long-acting injectable antipsychotics in the treatment of schizophrenia. Psychol Res Behav Manag. 2022;15:3915–3929. doi:10.2147/prbm.S371991
9. Marcus SC, Zummo J, Pettit AR, Stoddard J, Doshi JA. Antipsychotic adherence and rehospitalization in schizophrenia patients receiving oral versus long-acting injectable antipsychotics following hospital discharge. J Manag Care Spec Pharm. 2015;21(9):754–768. doi:10.18553/jmcp.2015.21.9.754
10. Titus-Lay EN, Ansara ED, Isaacs AN, Ott CA. Evaluation of adherence and persistence with oral versus long-acting injectable antipsychotics in patients with early psychosis. Ment Health Clin. 2018;8(2):56–62. doi:10.9740/mhc.2018.03.056
11. Vita G, Tavella A, Ostuzzi G, et al. Efficacy and safety of long-acting injectable versus oral antipsychotics in the treatment of patients with early-phase schizophrenia-spectrum disorders: a systematic review and meta-analysis. Ther Adv Psychopharmacol. 2024;14:20451253241257062. doi:10.1177/20451253241257062
12. Kishimoto T, Hagi K, Kurokawa S, Kane JM, Correll CU. Long-acting injectable versus oral antipsychotics for the maintenance treatment of schizophrenia: a systematic review and comparative meta-analysis of randomised, cohort, and pre-post studies. Lancet Psychiatry. 2021;8(5):387–404. doi:10.1016/s2215-0366(21)00039-0
13. Lin D, Thompson-Leduc P, Ghelerter I, et al. Real-World evidence of the clinical and economic impact of long-acting injectable versus oral antipsychotics among patients with schizophrenia in the United States: a systematic review and meta-analysis. CNS Drugs. 2021;35(5):469–481. doi:10.1007/s40263-021-00815-y
14. Khaykin E, Eaton W, Ford D, Anthony C, Daumit G. Health insurance coverage among persons with schizophrenia in the United States. Psychiatric Serv. 2010;61(8):830–834. doi:10.1176/ps.2010.61.8.830
15. Doshi JA, Li P, Geng Z, Seo S, Patel C, Benson C. Out-of-pocket costs for long-acting injectable and oral antipsychotics among medicare patients with schizophrenia. Psychiatr Serv. 2024;75(4):333–341. doi:10.1176/appi.ps.20230142
16. Joshi K, Muser E, Xu Y, Schwab P, Datar M, Suehs B. Adherence and economic impact of paliperidone palmitate versus oral atypical antipsychotics in a medicare population. J Comp Eff Res. 2018;7(8):723–735. doi:10.2217/cer-2018-0003
17. Li P, Benson C, Geng Z, Seo S, Patel C, Doshi JA. Antipsychotic utilization, healthcare resource use and costs, and quality of care among fee-for-service medicare beneficiaries with schizophrenia in the United States. J Med Econ. 2023;26(1):525–536. doi:10.1080/13696998.2023.2189859
18. Li P, Benson C, Geng Z, Seo S, Patel C, Doshi JA. Racial and ethnic disparities in long-acting injectable antipsychotic use in a national sample of medicare beneficiaries with schizophrenia. JAMA Network Open. 2023;6(9):e2334016. doi:10.1001/jamanetworkopen.2023.34016
19. Offord S, Wong B, Mirski D, Baker RA, Lin J. Healthcare resource usage of schizophrenia patients initiating long-acting injectable antipsychotics vs oral. J Med Econ. 2013;16(2):231–239. doi:10.3111/13696998.2012.751025
20. Barron JJ, Willey VJ, Doherty BT, et al. The Healthcare Integrated Research Database (HIRD) as a real-world data source for pharmacoepidemiologic research. Pharmacoepidemiol Drug Saf. 2025;34(2):e70110. doi:10.1002/pds.70110
21. Stephenson JJ, Teng CC, Harris K. RWD100 assessing the representativeness of real-world claims databases. Value Health. 2024;27(6, Supplement):S376–S377. doi:10.1016/j.jval.2024.03.1754
22. Centers for Medicare & Medicaid Services. Limited Data Set (LDS) files. CMS.gov. Available from: https://www.cms.gov/data-research/files-for-order/limited-data-set-lds-files.
23. Centers for Medicare & Medicaid Services. Chronic conditions data warehouse. CMS.gov. Available from: https://www2.ccwdata.org/web/guest/home/.
24. Virnig B, Parsons H. Strengths and limitations of CMD administrative data in research. University of Minnesota. Available from: https://resdac.org/articles/strengths-and-limitations-cms-administrative-data-research.
25. United States Census Bureau. Racial and ethnic diversity in the United States: 2010 census and 2020 census. U.S. Census Bureau. Available from: https://www.census.gov/library/visualizations/interactive/racial-and-ethnic-diversity-in-the-united-states-2010-and-2020-census.html.
26. Bonito AJ, Bann C, Eicheldinger C, Carpenter L. Creation of new race-ethnicity codes and socioeconomic status (SES) indicators for medicare beneficiaries. final report, sub-task 2. (Prepared by RTI international for the centers for medicare and medicaid services through an interagency agreement with the agency for healthcare research and policy, under contract No. 500-00-0024, task No. 21). AHRQ Publication No. 08-0029-EF. Rockville, MD January 2008.
27. Centers for Medicare & Medicaid Services. Chronic conditions data warehouse. Chronic conditions. CMS.gov. Available from: https://www2.ccwdata.org/web/guest/condition-categories-chronic.
28. National Committee for Quality Assurance. Adherence to antipsychotic medications for individuals with schizophrenia. Available from: https://www.ncqa.org/report-cards/health-plans/state-of-health-care-quality-report/adherence-to-antipsychotic-medications-for-individuals-with-schizophrenia-saa/.
29. Peterson AM, Nau DP, Cramer JA, Benner J, Gwadry-Sridhar F, Nichol M. A checklist for medication compliance and persistence studies using retrospective databases. Value Health. 2007;10(1):3–12. doi:10.1111/j.1524-4733.2006.00139.x
30. Medicare Payment Advisory Commission (MedPAC). Medicare advantage program payment system. payment basics. MedPAC.gov. Available from: https://www.medpac.gov/wp-content/uploads/2024/10/MedPAC_Payment_Basics_24_MA_FINAL_SEC.pdf.
31. Freed M, Fuglesten Biniek J, Damico A, Neuman T. Medicare advantage in 2024: enrollment update and key trends. Kaiser Family Foundation (KFF). Available from: https://www.kff.org/medicare/issue-brief/medicare-advantage-in-2024-enrollment-update-and-key-trends/.
32. Ankuda CK, Ornstein KA, Covinsky KE, Bollens-Lund E, Meier DE, Kelley AS. Switching between medicare advantage and traditional medicare before and after the onset of functional disability. Health Affairs. 2020;39(5):809–818. doi:10.1377/hlthaff.2019.01070
33. Cai C, Kozma C, Patel C, et al. Adherence, health care utilization, and costs between long-acting injectable and oral antipsychotic medications in South Carolina medicaid beneficiaries with schizophrenia. J Manage Care Spec Pharm. 2024;30(6):549–559. doi:10.18553/jmcp.2024.30.6.549
34. Hu M, Li X, Zhu Y, et al. The role of family caregiving in the management of individuals with mental illnesses and the outcome of family-based interventions for mental illnesses in China: a scoping review. Lancet Reg Health West Pac. 2025;56:101184. doi:10.1016/j.lanwpc.2024.101184
35. Ross C, Adams KS, Crouse EL. Transitions of care: assessment of adherence to long-acting injectable antipsychotic treatment following discharge from inpatient psychiatry. Ment Health Clin. 2025;15(1):9–16. doi:10.9740/mhc.2025.02.009
36. Trish E, Ginsburg P, Gascue L, Joyce G. Physician reimbursement in medicare advantage compared with traditional medicare and commercial health insurance. JAMA Intern Med. 2017;177(9):1287–1295. doi:10.1001/jamainternmed.2017.2679
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Understanding the Health System Conditions Affecting the Use of Long-Acting Injectable Antipsychotics in the Treatment of Schizophrenia in Clinical Practice: A US Healthcare Provider Survey
Zhdanava M, Starr HL, Lefebvre P, Totev TI, Shah A, Sheng K, Pilon D
Neuropsychiatric Disease and Treatment 2022, 18:1479-1493
Published Date: 22 July 2022
Health-Care Utilisation and Costs of Transition from Paliperidone Palmitate 1-Monthly to 3-Monthly Treatment for Schizophrenia: A Real-World, Retrospective, 24-Month Mirror-Image Study
Chang BC, Kuo MH, Lee CH, Chu YL, Chen KP, Tung CL, Yang YH, Hung CS, Tsai JH, Chuang HY
Neuropsychiatric Disease and Treatment 2024, 20:1985-1993
Published Date: 19 October 2024
One-Year Evaluation of Paliperidone Palmitate 6-Monthly: Satisfaction and Perceived Effectiveness Among Patients, Relatives, and Clinicians
Manchado Perero S, Rodríguez Lorente A, García-Pérez A, Isidro García G, Forcen-Muñoz LA, Ovejero S, Sáez Povedano R, González-Galdámez AL, Iturralde LM, Bonilla MR, Fuentes-Pérez P, Ovejas-Catalán C, Suárez-Pinilla P, Fernandez Abascal Puente B, Omaña Colmenares M, Campos-Navarro MP, Baca-García E, Fernández AL, Benavente-López S, Platero AR, Navalón MB, Sánchez-Alonso S, Vázquez-Bourgon J, Pappa S, García-Carmona JA
Patient Preference and Adherence 2025, 19:1573-1582
Published Date: 28 May 2025
Long-Term Symptomatic and Functional Remission with Paliperidone Palmitate 6-Monthly Treatment in Schizophrenia: A 3-Year Post-Hoc Analysis
Hamilton JM, Johnston KL, Simples Jnr J, Turkoz I, Lim L, Antunes J, Obando C, Mattingly G
Neuropsychiatric Disease and Treatment 2025, 21:1203-1214
Published Date: 18 June 2025