Back to Journals » Journal of Inflammation Research » Volume 19
Central Nervous System Involvement in Inflammatory Bowel Disease: A Bibliometric Analysis of Collaboration, Hotspots, and Research Trends
Authors Li J, Ru W, Zhao Y, Liu C ![]()
Received 19 February 2026
Accepted for publication 15 May 2026
Published 17 June 2026 Volume 2026:19 604053
DOI https://doi.org/10.2147/JIR.S604053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alberto Caminero
Jingwen Li,1 Wen Ru,2 Yan Zhao,3 Chen Liu2
1 7T Magnetic Resonance Imaging Translational Medical Center, Department of Gastroenterology, Southwest Hospital, Third Military Medical University (Army Medical University), Chongqing, People’s Republic of China; 2 7T Magnetic Resonance Imaging Translational Medical Center, Department of Radiology, Southwest Hospital, Third Military Medical University (Army Medical University), Chongqing, People’s Republic of China; 3Army Medical University Library, Army Medical University (Third Military Medical University), Chongqing, People’s Republic of China
Correspondence: Chen Liu, 7T Magnetic Resonance Imaging Translational Medical Center, Department of Radiology, Southwest Hospital, Third Military Medical University (Army Medical University), Chongqing, People’s Republic of China, Email [email protected]
Purpose: Research on central nervous system (CNS) involvement in inflammatory bowel disease (IBD) has expanded rapidly, reflecting growing interest in the interaction between intestinal inflammation and brain-related disorders. This study aimed to systematically map the research landscape of IBD-related CNS involvement and to identify major research hotspots, intellectual structures, and emerging frontiers using bibliometric approaches.
Methods: Publications related to IBD and CNS disorders were retrieved from the Web of Science Core Collection, between January 1, 2005, and December 31, 2024. Bibliometric and visualization analyses were conducted utilizing CiteSpace, VOSviewer, and Bibliometrix to evaluate publication trends, collaboration patterns, thematic evolution and historical development.
Results: A total of 2,429 publications were included. The annual number of publications increased steadily from 2005 to 2024, with a marked acceleration after 2021, indicating increasing scholarly interest in this interdisciplinary field. Sixty-two countries/regions, 2,774 institutions, and 12,399 researchers have contributed to this field. The United States and China emerged as prominent contributors, with Mayo Clinic and Harvard Medical School recognized as central institutional centers. Thematic and keyword-based analyses revealed that research hotspots have evolved along three interrelated dimensions: a sustained focus on the gut-brain axis as the core mechanistic axis; an expansion of phenotypic profiling from general neurological involvement to a stratified central nervous system (CNS) phenotype spectrum; and a translational progression from descriptive correlations to precise predictions and targeted intervention.
Conclusion: By integrating multiple bibliometric indicators, this study provides the developmental trajectory and thematic structure of IBD-related CNS research. The findings highlight that gut microbiota and gut-brain axis mechanisms as prominent emerging hotspot, while neurodegenerative disorders represent an expanding clinical frontier. Future studies should strengthen interdisciplinary collaboration, longitudinal cohort design, multimodal phenotyping, and mechanism-informed translational research.
Keywords: inflammatory bowel disease, brain, visualization, bibliometric analysis
Introduction
Inflammatory bowel disease (IBD) is a chronic, immune-mediated disorder of the gastrointestinal tract, including ulcerative colitis (UC) and Crohn’s disease (CD).1,2 It poses a high disease burden worldwide, and more than 10 million new IBD cases are predicted by 2050 in newly industrialized countries such as Asia, the Middle East and South America with a varying and sometimes severe disease course.3,4 The primary clinical symptoms include bloody or purulent stool, recurrent diarrhea, rectal bleeding, weight loss and abdominal pain.5,6 Bowel perforation, septic shock, and various other serious complications can happen in severe situations. At present, there is no cure available.7,8 The rapid changes in lifestyle, diet and environment may be important contributors to the rising incidence of IBD.9,10 The etiology of IBD has not yet been fully elucidated, and its pathogenetic repercussions are thought to be a complex interplay of genetic, environmental, dietary, infectious, psychological, and other factors.11
Beyond these gastrointestinal manifestations, up to 50% of patients experience at least one extra-intestinal manifestation in the course of IBD.12 Psychiatric comorbidity, including depression, anxiety, and bipolar disorder (BD), is well known to be more prevalent in IBD.13,14 Many previous research on brain disorders among IBD patients has focused primarily on depression and anxiety.15,16 Of further note, increasing research shows that IBD has been associated with a higher risk of neurodegenerative diseases such as stroke or cerebrovascular accident, dementia, Parkinson’s disease (PD), multiple sclerosis (MS), and peripheral neuropathy.17,18 This evidence has indicated a complex relationship between intestinal inflammation and central nervous system disorders. Growing attention has therefore been directed toward the gut–brain axis, with gut microbiota, microbial metabolites, neuroinflammation, and barrier dysfunction being considered key mechanisms connecting intestinal and brain pathology.19–21 However, the directionality, causality, and overall knowledge structure of these associations remain insufficiently clarified.
Bibliometric analysis can effectively process large amounts of literature, assess the present research status, and predict future research hotspots.22,23 Although a few previous bibliometric studies on the IBD–brain axis have mainly focused on psychiatric comorbidities,24,25 and some reviews have separately addressed neurodegenerative diseases in IBD,17,26 a comprehensive bibliometric analysis covering the broader spectrum of central nervous system (CNS) disorders in IBD is still lacking. To address this gap, the present study provides a unified, macro-level mapping of the IBD–brain research landscape from 2005 to 2024, identifying not only the evolution of research output and collaboration patterns, but also emerging hotspots such as gut microbiota, gut–brain axis, and neurodegeneration. This broader perspective offers new insight into how the field is shifting from a predominantly psychiatric focus toward a more integrated neurological framework and may help guide future mechanistic and translational studies.
Methods
Data Source and Search Strategy
Relevant publications on inflammatory bowel disease and neurological aspects from January 1, 2005, to December 31, 2024, were retrieved from the Web of Science Core Collection (WoSCC) database on January 31, 2025. The search strategy was designed to achieve high sensitivity for studies concerning inflammatory bowel disease and its neurological or brain-related manifestations.
Based on the theme of the present study, the search terms were developed and refined with input from Yan Zhao an information specialist from the Army Medical University Library, to balance comprehensiveness and relevance. The topic search was performed using the following formula: TS = ((“inflammatory bowel disease” OR “ulcerative colitis” OR “Crohn disease”) AND (“brain” OR “gut-brain axis” OR “central nervous system” OR “cerebral” OR “neurolog”))**Two types of papers, articles and reviews in English language solely, were chosen. To ensure the relevance and quality of the included literature, two senior physicians (Dr. Jingwen Li and Dr. Ru Wen) specializing in gastroenterology independently reviewed the titles and abstracts of the retrieved articles. Duplicate records (if any) resulting from internal database indexing overlaps were systematically eliminated utilizing the automated deduplication algorithms inherent within the bibliometrix R package, followed by a secondary manual screening phase. Studies were excluded if they: (1) Focused on IBD but did not examine CNS disorders; (2) Investigated CNS disorders in contexts unrelated to IBD; (3) Discussed IBD without meaningful connection to CNS disorders. In cases of disagreement, a senior professor (Pro. Liu) served as an arbitrator to make the final inclusion decision.
A flow diagram illustrating the selection process is presented in Figure 1A. As a result, 2,429 relevant literatures were chosen and saved in plain .txt format, and complete records and cited references also included. The WoSCC database search results were used for further analysis, covering bibliographical profiles, citation trends, collaboration information, and other retrieved publications.
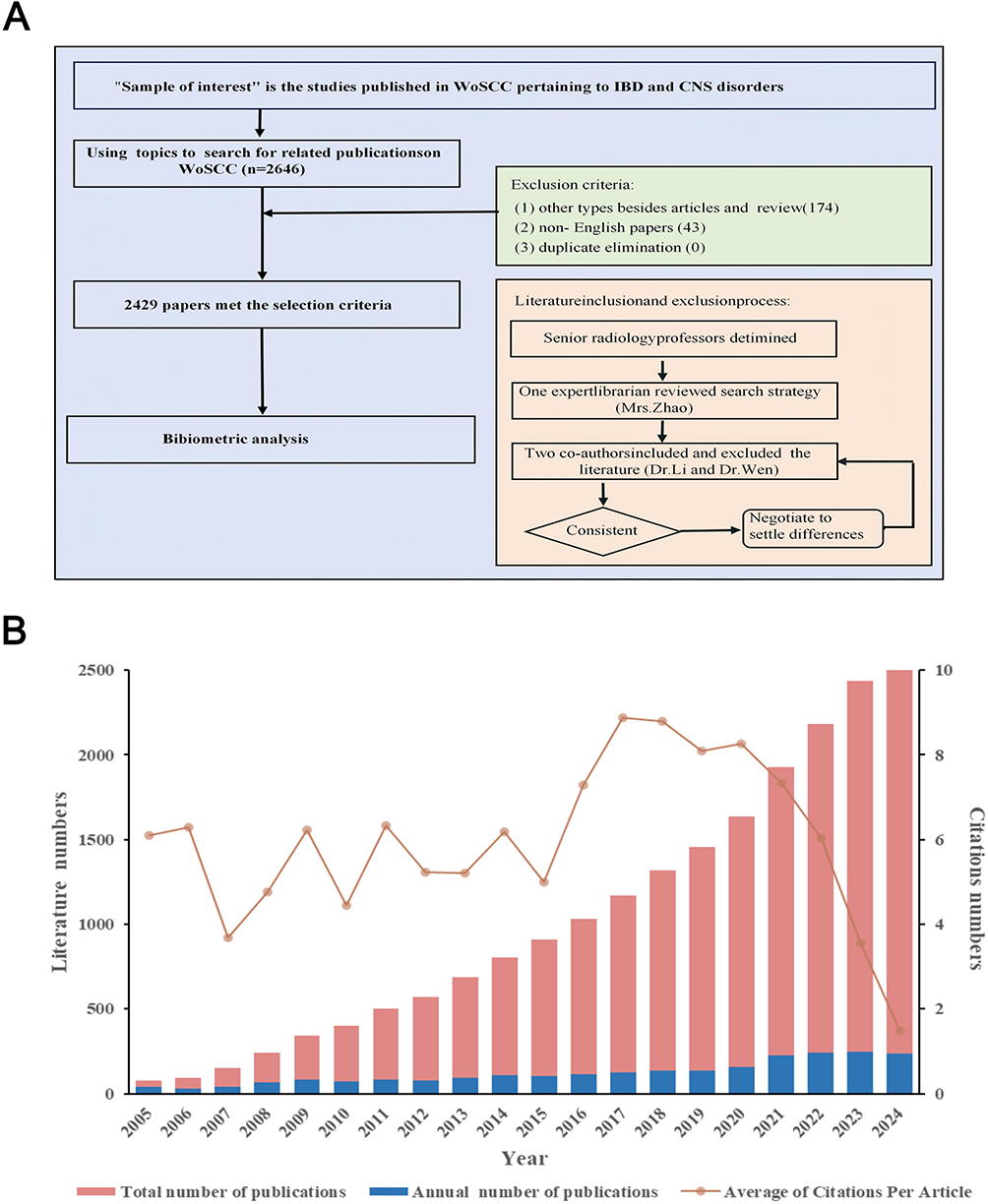 |
Figure 1 (A) Flow chart illustrating the process in this study. (B) Global trends in the number of published articles related to cerebral implications for IBD from 2005 to 2024. |
Analysis Methods
Data analysis utilized VOSviewer (v1.6.17), CiteSpace (v6.1.R6) and the Bibliometrix R package to comprehensively investigate the structural characteristics and developmental trends within the research domain.27 Firstly, VOSviewer was utilized to construct and visualize collaborative networks among countries, institutions, journals, authors, and keywords. In these visualizations, node sizes correspond to their respective weights, while the thickness of the connecting lines indicates the strength of collaboration, co-citation, or co-occurrence relationships. Secondly. CiteSpace was employed to perform analyses of citation bursts, reference co-citation, and keyword timelines, facilitating the identification of pivotal literature and the evolution of research topics. For cluster analysis, we assessed the capabilities of clustering using modularity (Q value) and silhouette (S value) metrics. A Q value greater than 0.3 suggests a significant clustering structure, while an S value exceeding 0.5 indicates that the clusters are reasonably homogeneous and well-separated.
Besides, CiteSpace demonstrated citation relationships across different disciplines and helped to identify research hotspots and emerging themes by making dual-map overlays. Finally, Bibliometrix was used to analyze publication counts, reference analysis, national distribution, collaboration patterns, thematic evolution analysis and historical analysis. This tool allows raw data from Web of Science databases, and supports descriptive statistical analysis, thereby elevating the systematic and reproducible nature of the study. The raw data utilized in this study are publicly accessible, eliminating the requirement for an ethical review. The flowchart for this research study was shown in Figure 1A.
Results
Annual Publications and General Characteristics
Totally, 2,429 publications on the relationship between inflammatory bowel disease and the brain (published 2005–2024) were identified for analysis (Figure 1A). Global trends in the field were shown in Figure 1B. The annual number of publications rose steadily over this period, from 38 in 2005 to nearly 250 in 2024, a seven-fold increase, with the sharpest surge occurring after 2021. The number of articles on IBD and CNS diseases had a significant raise. This suggested that worldwide research teams showed active interest in the past three years.
Analysis of Cooperation Condition
Countries/Regions
Relevant research spanned 62 countries; the USA (588; 24.2%) and China (379; 15.6%) jointly accounted for >40% of output (Figure 2A). The top 10 countries published 1777 articles, constituting nearly 73.2% of the total publications. Network analysis (Figure 2B) showed intensive bilateral links—particularly USA–China—plus an active “second ring” of UK, Germany and Canada. The collaboration network maps (Figure 2B) indicated active cooperation among countries. The extensive collaborations between 30 most productive countries were shown in Figure 2B. Countries with high productivity tended to have more collaboration, the United States and China were the two main contributors and their cooperation was far more common than that of other countries. The cooperation between the other countries such as the United Kingdom, Germany, and Canada was relatively frequent.
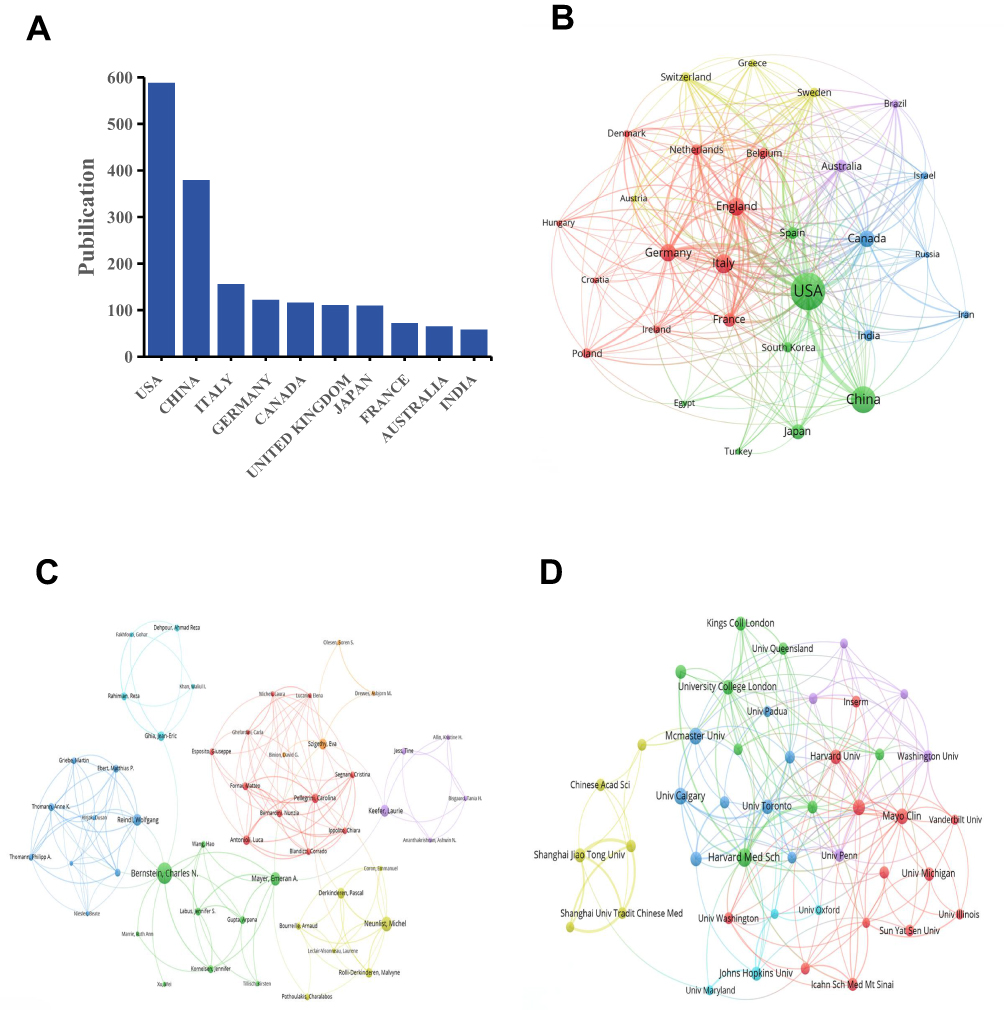 |
Figure 2 (A) The ten most productive countries. The network maps showing countries/regions (B), authors (C) and institutions (D) involved in the research on cerebral implications for IBD. |
Institutions
Research on IBD and CNS disorders was conducted at 2774 institutions globally, with Table 1 highlighting the top 10 institutions. Harvard University (138 papers) and the University of California system (>130) spearhead output (Table 1). The close collaborative relationships between different institutions in this field were illustrated in Figure 2C. The analysis of institutional co-occurrence revealed that institutions with high publication volumes tend to maintain close collaborative relationships, with domestic partnerships being more prevalent than international ones. The cooperation was more common among top institutions and countries.
Authors
Totally, over 12399 researchers participated in research about IBD and CNS diseases. Bruno Bonaz from France had the highest number of publications (n = 19), followed by Charles N Bernstein (n = 16) (Table 2). The author co-occurrence analysis revealed multiple research groups and collaborations among researchers in this field (Figure 2D). Nodes represented authors, with node size positively correlated to the authors’ publication numbers. Lines represented the cooperation between authors, and line thickness indicated the frequency of cooperation.
Analysis of Journals
Up to the end of 2024, 942 SCI journals published articles about IBD and brain. Table 3 listed the top 10 journals actively publishing articles. Among them, the INTERNATIONAL JOURNAL OF MOLECULAR SCIENCES had the highest number of publications (n=69) and citations (2713). FRONTIERS IN IMMUNOLOGY was the second published journal (n=49) with 1719 citations in total. The dual-map overlay of journals (Figure 3) illustrated the disciplinary spread of the IBD–brain literature. Research on this topic was published primarily in journals in the medical and life sciences (depicted on the left side of the dual-map), while the references cited by these articles were largely found in journals of neurology and immunology (right side). This suggested that the field draws on knowledge from neuroscience and immunology even as it remains rooted in the medical literatures.
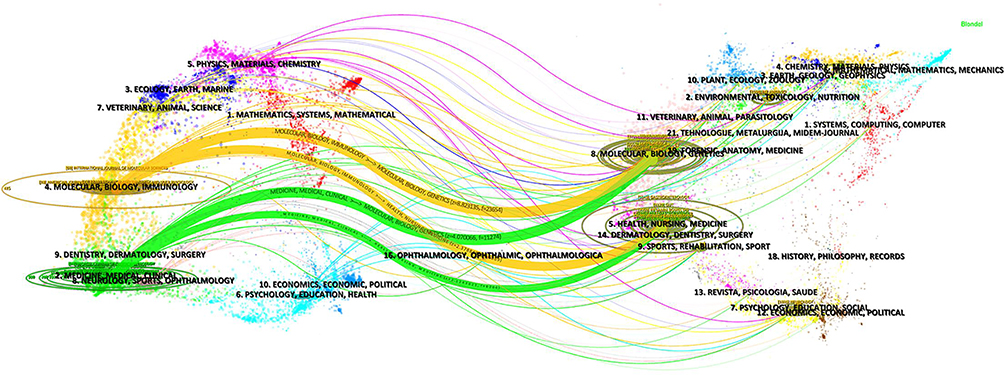 |
Figure 3 Dual-map overlay of journals, illustrating cross-disciplinary citation flows. Left: citing journals; Right: cited journals. Colored paths represent citation relationships. |
Analysis of Co-Cited References
Co-cited references are those references, which are cited together by other publications integrated into study. We constructed a co-citation network of references, aiming to explore the knowledge base of IBD and brain. Figure 4A illustrated the co-cited reference distribution network from 2005 to 2024, highlighting references cited more than 27 times. The lighter the color of the node indicated later citation.
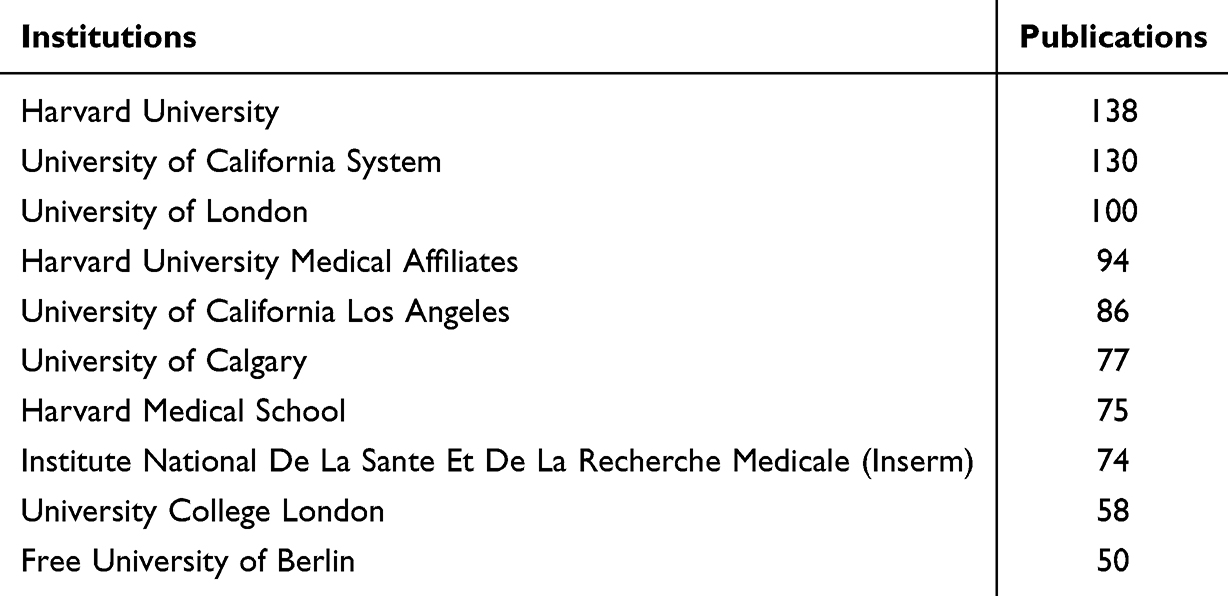 |
Table 1 The Top 10 Prolific Institutions |
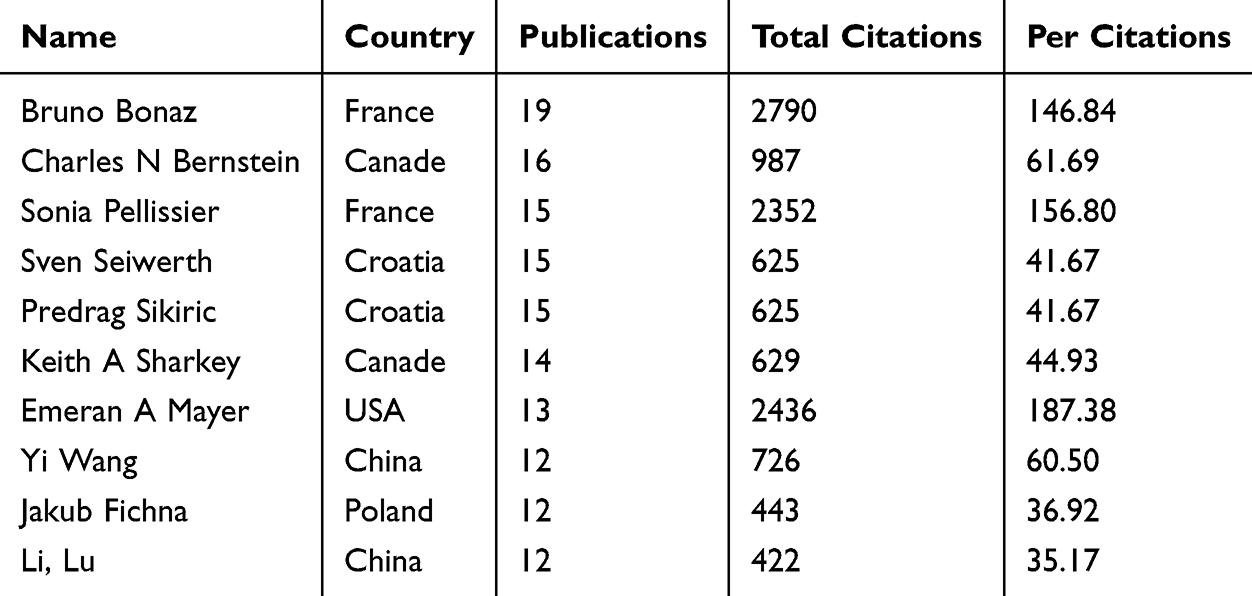 |
Table 2 The Top 10 Prolific Authors |
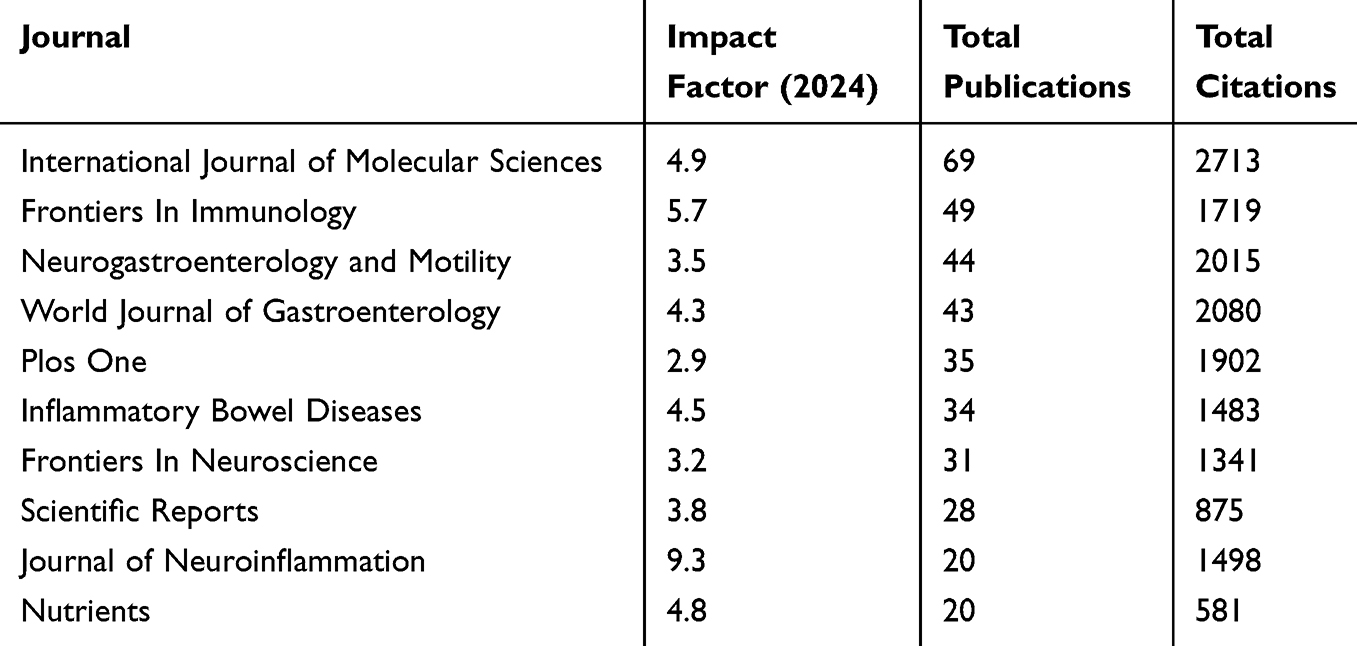 |
Table 3 The Top 10 Journals of Publications on Cerebral Implications for IBD (Sorted by Total Citations) |
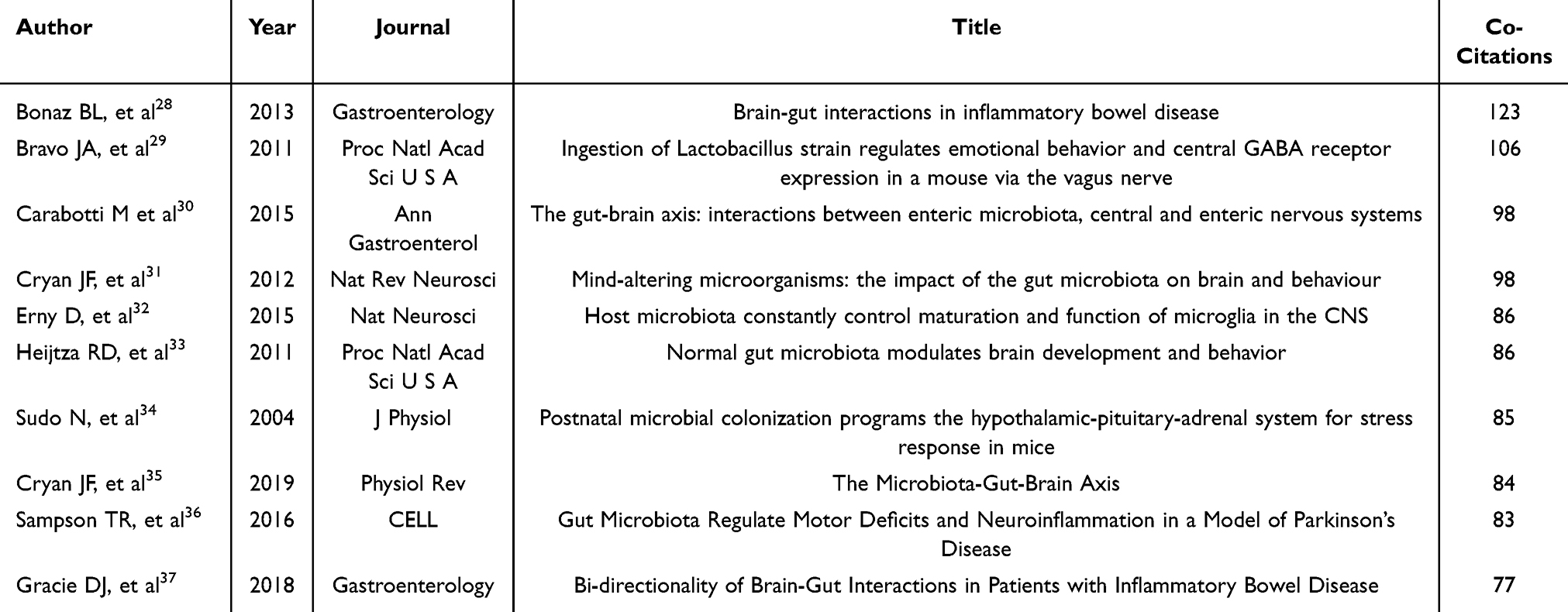 |
Table 4 The Top 10 High-Cited reference |
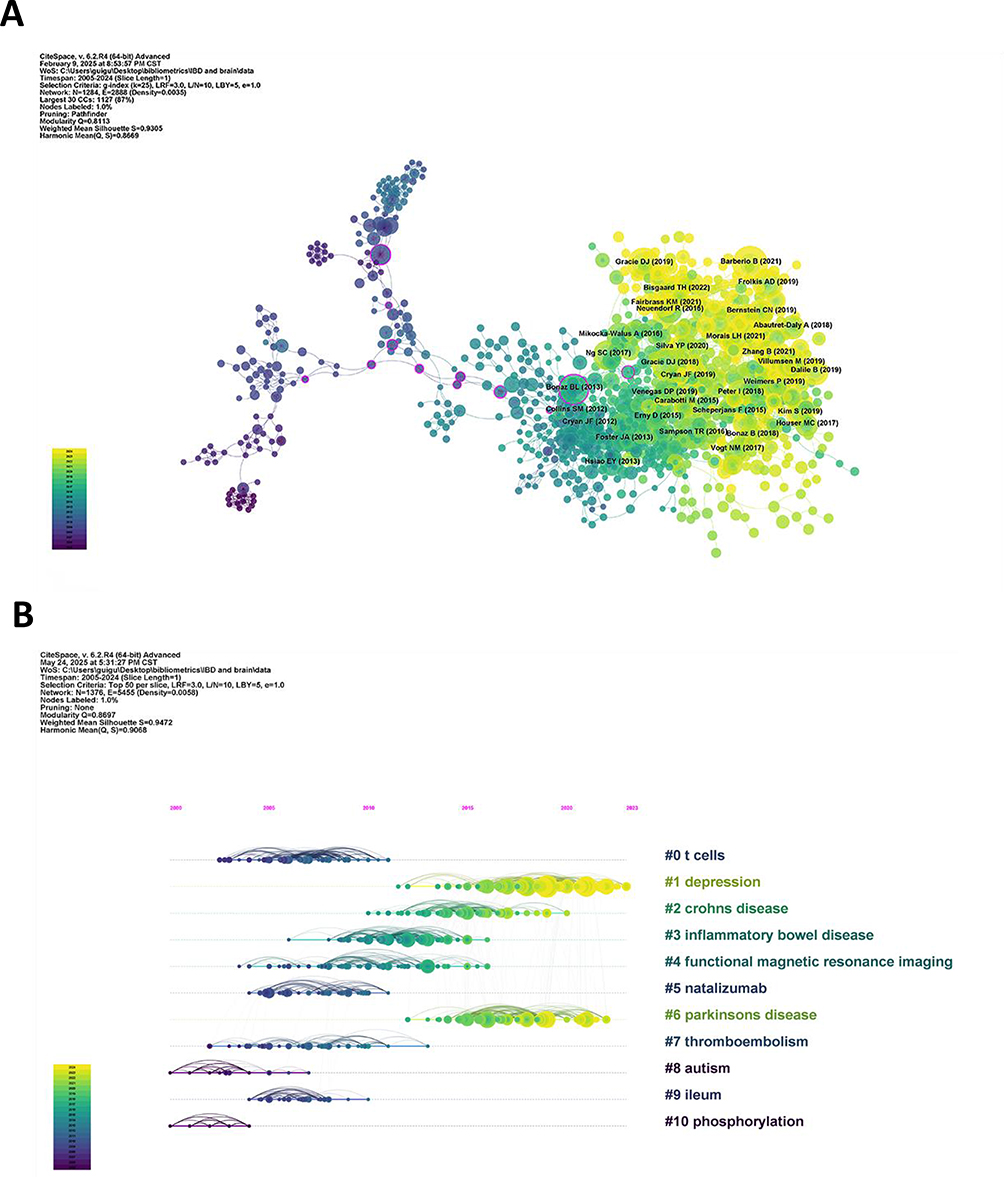 |
Figure 4 (A) The map of the co-cited references clusters. Node size represents publication output, with colors denoting distinct collaborative modules. (B) Timeline view of co-cited references clusters. |
The citation impact of publications is considered a crucial metric for evaluating scientific documents, despite being influenced by various factors. Table 4 presented the top 10 most frequently cited references. The article “Brain-gut interactions in inflammatory bowel disease,” published in GASTROENTEROLOGY, was the most frequently cited with 123 citations. The paper titled ‘Ingestion of Lactobacillus Strain Regulates Emotional Behavior and Central GABA Receptor Expression in Mice via the Vagus Nerve’ ranked second (n=106). The most cited articles in this field were published in leading journals. Among the top 10 co-cited references, all but one (Sudo N et al) were published after 2010, with approximately half published in the past ten years.
Based on CiteSpace’s clustering of the reference co-citation network, 20 clusters were recognized totally and the ten largest clusters were shown in Figure 4B. In the timeline map, nodes of different colors on the same line represented different years of references in a cluster, the older references were nearly closer to the left. Modularity Q (0.8697) was greater than 0.3, and Mean Silhouette (0.9472) values was greater than 0.7, indicating that the clustering structure was convincing. The ten largest clusters were as follows: “t cells” (cluster #0), “depression” (cluster #1), “crohns disease” (cluster #2), “inflammatory bowel disease” (cluster #3), “functional magnetic resonance imaging” (cluster #4), “natalizumab” (cluster #5), “parkinsons disease” (cluster #6), “thromboembolism” (cluster #7), “autism” (cluster #8), “ileum” (cluster #9), and “phosphorylation” (cluster #10). The timeline view of co-cited clusters showed the evolution of these research themes, with some clusters-notably those related to gut–brain axis mechanisms and microbiome interactions-emerging more prominently in recent years.
Citation bursts highlight references that receive notable citations during a specific timeframe. Figure 5 showed the top 20 articles with the strongest citation bursts, red bars indicated high citation frequency and green bars indicated low citation frequency. Many of these high-impact papers were published in the last decade (for instance, around 2015–2018) and correspond to breakthrough findings related to the gut–brain axis and IBD, such as the reference “Brain-Gut Interactions in Inflammatory Bowel Disease” by Bonaz BL with the highest burst strength (21.62). The presence of multiple recent citation bursts suggested rapidly growing interest in these novel topics.
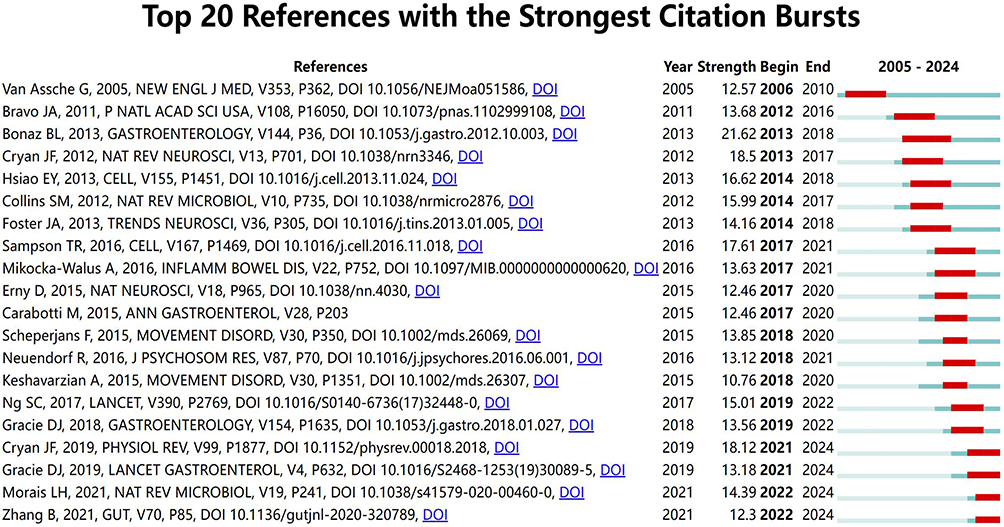 |
Figure 5 Visual analysis of references with the strongest citation bursts, highlighting the top 20 references with the strongest burst strengths. This figure is a CiteSpace-generated citation-burst visualization based on the analyzed WoSCC dataset; the displayed records represent bibliometric source records rather than all references directly cited in the manuscript text. |
Analysis of Keywords
Keyword co-occurrence analysis is used to explore the hot topics in the research field. We extracted and clustered the 100 most frequent keywords, with every keyword appearing at least 40 times. The different colored dots illustrated four clusters, containing 31, 30, 26, and 13 keywords, respectively. Cluster 1 (red) primarily related to possible cerebral implications in IBD, with keywords such as “inflammation”, “brain”, “pain”, and “Parkinson’s disease”. Cluster 2 (green) contained keywords related to emotional symptoms and survival of IBD, such as “stress”, “depression”, “pain” and “quality of life”. Cluster 3 (blue) and Cluster 4 (yellow) focused on potential mechanisms and gut microbiota, respectively (Figure 6A). The keyword burst detection (Figure 6B) further showed that terms like “gut–brain axis,” “gut microbiota,” and “metabolism” had strong citation bursts in recent years. These ongoing bursts indicated that these topics are current hotspots and are likely to remain focal points of future research. A marked growth in IBD–brain research indicated that the gut microbiota and gut–brain axis as prominent emerging themes in this field.
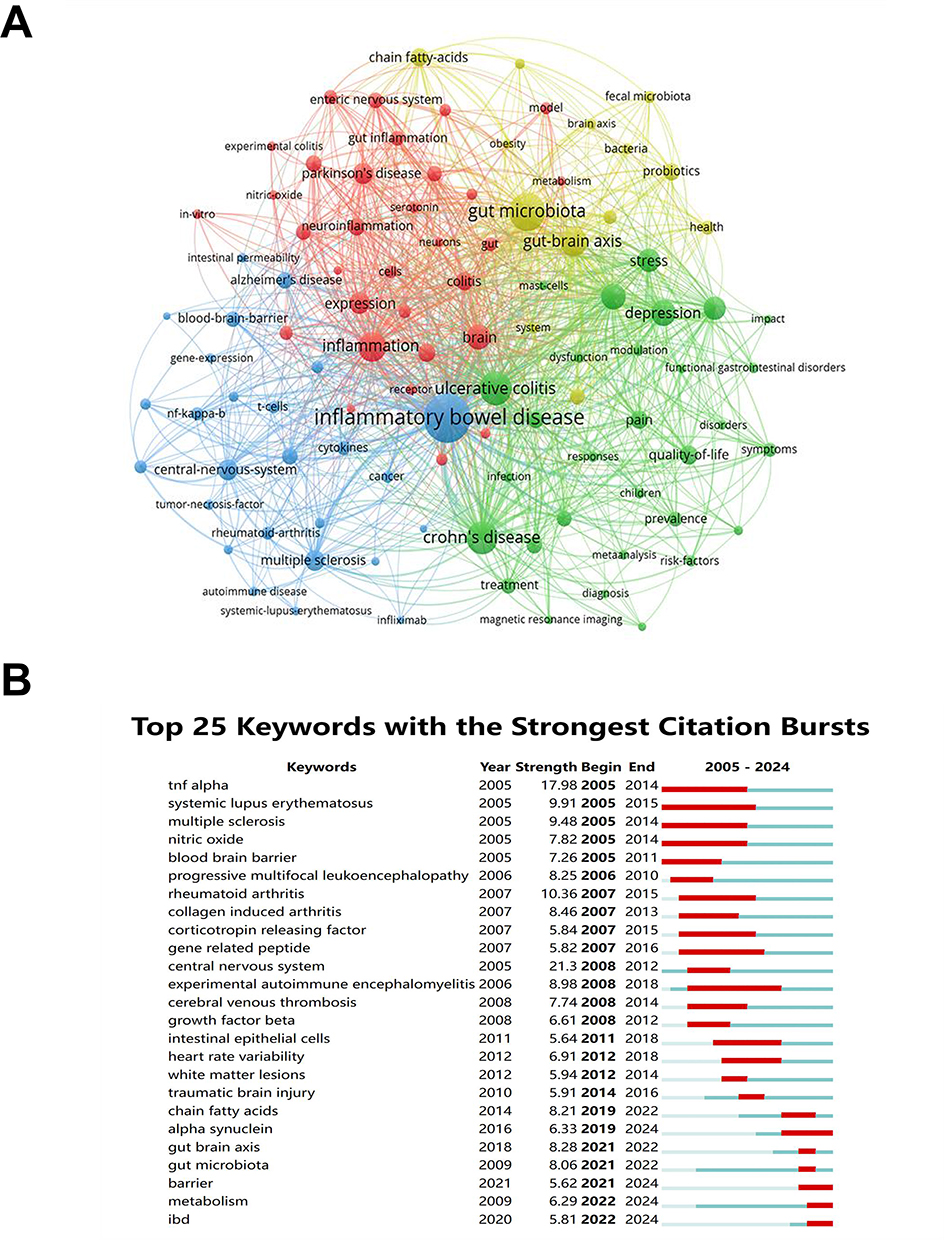 |
Figure 6 (A) Network map of the top 100 keywords organized into five distinct clusters. (B) Keywords with the strongest citation bursts on cerebral implications of IBD. |
Thematic Evolution Analysis
To comprehensively identify research priorities in this field, we performed thematic evolution analysis. In all the published literature, thematic evolution has gradually developed from inflammation, tight junction, microbiome, and vagus nerve in 2005–2019 to infliximab, chronic pain, gut microbiota, diagnosis, magnetic resonance imaging, and epidemiology in 2020–2024 (Figure 7A). In the thematic map of all articles, a four themes quadrant is provided based on the centrality and density along the x-axis and y-axis, the four quadrants of the map (counterclockwise) represent motor themes (first quadrant), highly specialised themes (second), emerging or disappearing themes (third), and core themes (fourth). The themes in first quadrant are “gut micribiota” “multiple scierosis” “blood brain barrier”, all of which are relevant and well-developed for the structuring of this research field, in second quadrant are “patient”, “complications” and “risk factor”, in third quadrant are “central nervous system”, “rheumatoid arthritis” and “experimental autoimmune encephalomyelitis”, themes between the third and fourth quadrants were “brain” “expression” and “activation”, in the fourth are “inflammatory bowel disease” ulcerative colitis, “crohn’s disease” (Figure 7B). Overall, the thematic map indicates that the knowledge structure of this field is centered on IBD-related topics, and gut microbiota-related research representing a prominent theme.
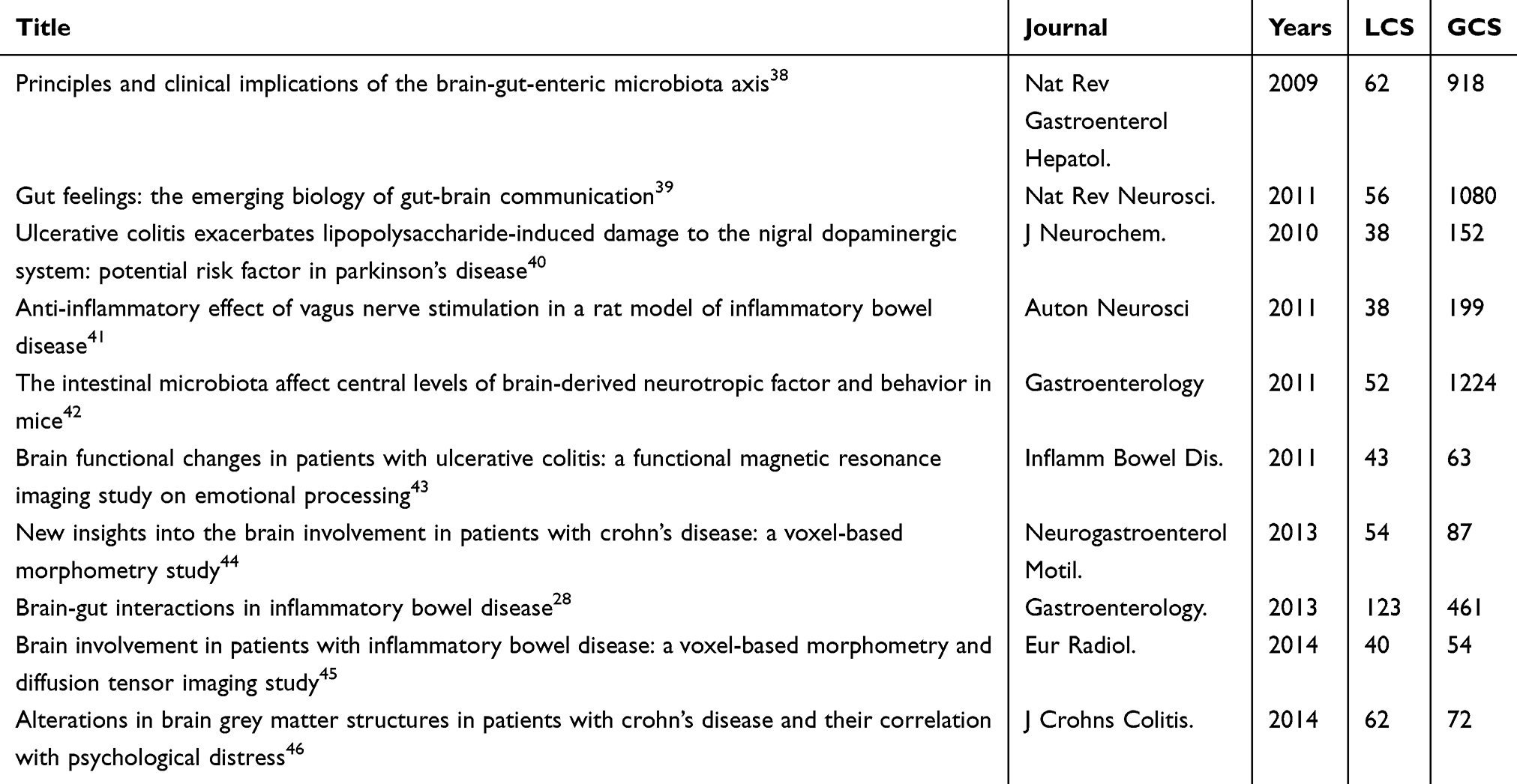 |
Table 5 Historiograph of IBD and CNS Orders |
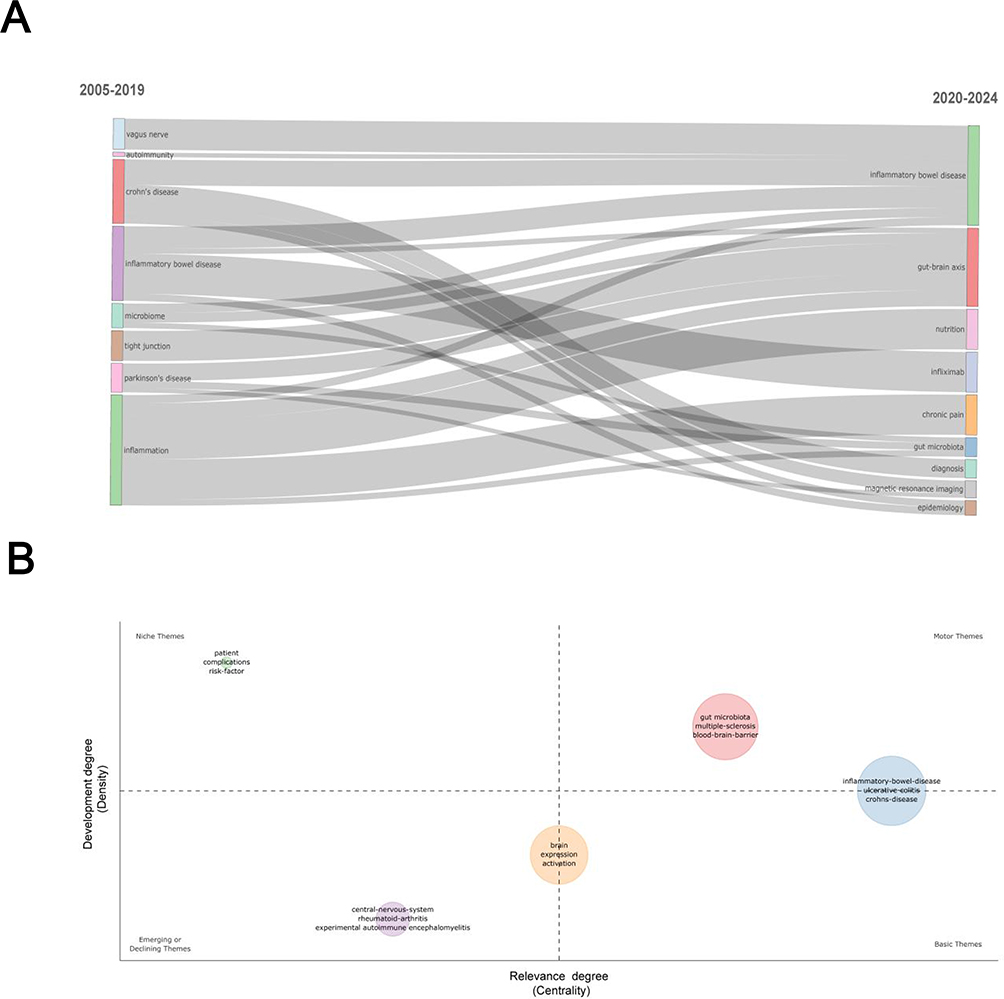 |
Figure 7 Theme changes and trend of published articles related to CNS disorders from 2005 to 2024. (A) thematic evolution of total published articles; (B) thematic map of total published articles. |
Historical Analysis of IBD and CNS Disorders Research
We further analyzed the historiograph of IBD and CNS disorders research in order to understand the publications that were important in the history of the discipline (Figure 8), which are also shown in Table 5. Early highly cited publications were mainly concentrated on the brain-gut-enteric microbiota axis, gut-brain communication, and experimental investigations concerning vagus nerve stimulation, microbiota, and CNS injury. Subsequent research expanded toward brain functional alterations,structural alterations, and the interactions between the brain and IBDin IBD patients. Numerous publications from the period 2013 to 2015 held pivotal roles within the citation network, serving as critical links between earlier studies and subsequent research. In Table 5, brain–gut interactions in inflammatory bowel disease (2013) had the highest LCS, while the intestinal microbiota affect central levels of brain-derived neurotrophic factor and behavior in mice (2011) had the highest GCS.
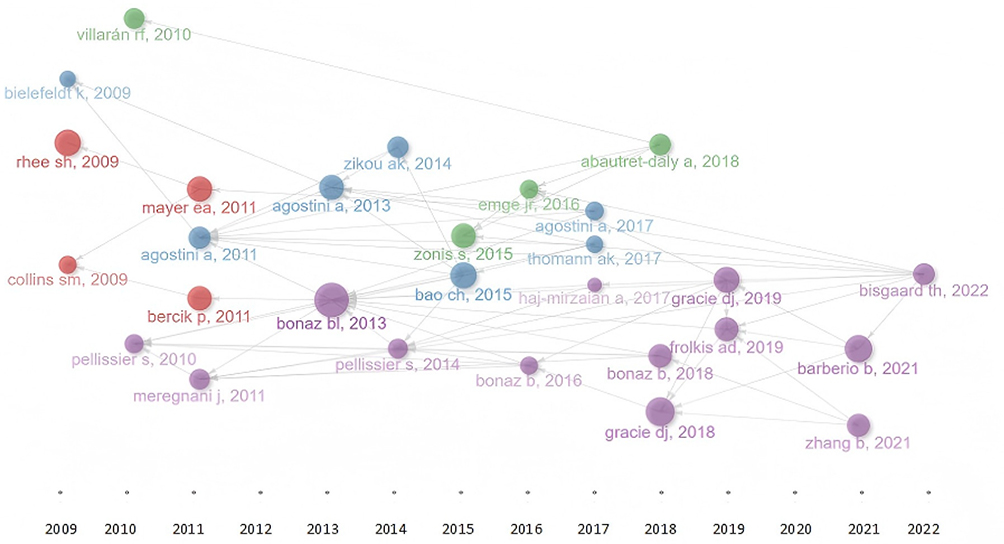 |
Figure 8 Historiograph of IBD and CNS disorders research. |
Discussion
IBD has become a globally health challenge impairing millions of patients, imposing a rising burden on healthcare systems significantly.2 In this context, research on neurological implications in IBD has expanded substantially over the past two decades. Our bibliometric analysis of 2,429 publications shows sustained growth in scientific attention, with especially rapid expansion between 2021 and 2024. The United States and China were the major contributors, and international collaboration networks were centered around institutions such as Mayo Clinic and Harvard Medical School. Although broad multidisciplinary journals published the largest number of papers, specialty journals such as Gastroenterology retained strong structural influence in the co-citation network. Compared with previous bibliometric studies that focused mainly on anxiety, depression, or emotional factors in IBD,24,25 the present analysis maps a broader spectrum of CNS disorders and suggests that the field is moving toward a more integrated neurological and microbiota-oriented framework.
Emerging Hotspots and Future Trend
Integrating co-citation analysis, citation burst detection, keyword co-occurrence, thematic mapping, and intellectual historiography, reveals a clear conceptual shift in the field. Earlier studies were largely framed within a conventional inflammation- and immune-centered model, emphasizing TNF-α, T-cell responses, blood-brain barrier dysfunction, and autoimmune mechanisms.5,47,48 In contrast, recent high-intensity bursts for terms such as gut-brain axis, metabolism, and neurodegeneration suggest a transition toward a more integrated framework centered on gut microbiota and microbially mediated signaling pathways. Overall, the main focus areas and emerging directions in IBD-related CNS disorders can be summarized from three aspects: molecular mechanisms, phenotypic change and disease relevance with translational applications. Importantly, these observations reflect patterns of scholarly attention rather than definitive biological hierarchies.
Mechanistically: From Traditional Inflammation to Intestinal-Brain Axis
Early high-frequency keywords and citation bursts were largely focused on inflammatory mediators, autoimmune overlap, and experimental evidence of CNS immune activation. It reflects an initial effort to explain the interrelationship of intestinal and neurological pathology through shared immunopathogenic mechanisms. In recent years, subsequent shifts in keyword importance indicate a growing expansion of research attention toward to brain–gut axis, especially that gut microbiota. The keyword network depicted in Figure 6A and the thematic map presented in Figure 7B further reveal that, the entities that have assumed a central role include gut microbiota, the gut-brain axis, neuroinflammation, the enteric nervous system, metabolism, chain fatty acids, and the barrier dysfunction. Research increasingly focuses on dysbiosis, loss of short-chain-fatty-acid-producing bacteria, altered bile acid and other microbial metabolite pathways, barrier dysfunction, and neuroimmune activation as candidate links between intestinal inflammation and CNS abnormalities.35,49–55 These observations support microbiota-centered gut-brain mechanisms as the most prominent emerging hotspot in the current IBD-CNS research landscape. Also, it indicates that the field moves the discussion beyond the simple proposition that IBD is associated with CNS involvement and instead directs attention to the biological routes through which this influence may occur.
Phenotypic Stratification: Beyond Monolithic CNS Involvement
Bibliometric evidence also suggests that the field has evolved toward a more stratified CNS phenotype framework. Rather than a variety of clinical symptoms, previous studies treated CNS manifestations as a monolithic complication of IBD.2 In contrast, the co-citation timeline (Figure 4B) in our analysis shows that depression, functional magnetic resonance imaging, and Parkinson’s disease are clustered together as a persistently active group. Figure 6A shows that topics such as depression, pain, stress, and diagnosis are situated within the region of high connectivity. This pattern indicates that the scope of IBD-related CNS manifestations has broadened to include anxiety, depression, pain-processing abnormalities, stress-related symptoms, white matter changes, and possible long-term neurodegenerative.56,57 More importantly, recent systematic reviews and meta-analyses have shown that IBD may be associated with increased risks of Parkinson’s disease, dementia, and related neurodegenerative outcomes, although effect sizes and causality remain uncertain.58–61 Therefore, neurodegeneration should be viewed as an important and growing clinical frontier rather than as a definitively established consequence of IBD. The current research focus is shifting from whether CNS involvement exists in IBD to what kinds of CNS phenotypes are present in different patient subgroups. The recent prominence of themes such as chronic pain and magnetic resonance imaging suggests that future studies should establish a stratified CNS phenotype spectrum according to disease subtype, disease activity, age, medication exposure, and symptom dimensions. Longitudinal neuroimaging and neuropsychological assessment will be particularly important for determining which patients progress from functional abnormalities to structural alterations.
Translational Shifts: From Descriptive Correlations to Targeted Interventions
The phenotypic expansion described above provides the basis for a further translational shift. Primary research topics have moved from earlier concepts such as autoimmunity and tight junctions toward more recent subjects including the gut-brain axis, nutrition, infliximab, and epidemiology (Figure 7). This pattern suggests that the literature is no longer concerned only with explaining the plausibility of gut–brain interactions but is increasingly focused on how these insights may be applied in clinical settings.29,33,34,37,62
At the same time, the prominence of the natalizumab-related cluster (Figure 4) and the early appearance of progressive multifocal leukoencephalopathy (Figure 6) indicate that early translational concerns were largely centered on neurological safety. More recently, the scope has broadened to include biologic-response stratification, nutritional and microbiota-targeted interventions, MRI-based monitoring, and population-level risk prediction.63,64 Combining the continuously emerging references in Figure 5 over the past few years, as well as the multi-disciplinary intersection shown in the double-layered graph in Figure 3,these trends suggest that future research should move from descriptive association toward clinically useful prediction, dynamic monitoring, and mechanism-informed intervention. However, whether dietary regulation, microbiota-directed therapy, or treatment optimization can modify CNS manifestations in IBD still requires stronger longitudinal and interventional evidence.
Limitations
There are some limitations inherent in this study. First, all data were sourced exclusively from the WoSCC, despite its extensive coverage and standardized citation metrics, which may not comprehensively encompass all academic disciplines or journals. This limitation could potentially result in the overrepresentation or underrepresentation of specific research areas. Second, non-English literature was not included in the database or analysis, possibly resulting in linguistic source bias. Furthermore, the IBD–CNS literature remains fragmented across partially connected areas, including psychiatric symptom research, neurological comorbidity research, and microbiota–gut–brain axis–oriented mechanistic studies. This fragmentation may hinder cross-field synthesis and cause bibliometric analyses to reflect parallel research streams rather than a fully integrated knowledge base. In addition, citation-based prominence should be interpreted cautiously, as citation counts may be influenced not only by scientific contribution but also by factors such as author reputation, journal impact, and self-citation. Accordingly, highly cited publications should be viewed primarily as indicators of visibility and influence within the field, rather than direct proxies for evidentiary strength. Finally, publication and citation patterns may be shaped by funding availability and publication bias.
Conclusions
This bibliometric analysis provides a macro-level overview of the IBD–CNS research landscape and reveals how the field has evolved over time. The findings indicate sustained growth in publication output, increasing interdisciplinary interaction, and a conceptual shift from inflammation-centered and symptom-oriented research toward microbiota-centered gut–brain mechanisms, phenotypic stratification, and translationally oriented investigation. Among the emerging hotspots identified in our analysis, gut microbiota and gut–brain axis-related mechanisms appear to be the most prominent, whereas neurodegenerative disorders represent an important and expanding clinical frontier within the broader IBD–CNS spectrum. Future progress in this field will require stronger international and interdisciplinary collaboration, especially through multicenter longitudinal cohorts, harmonized protocols, and integrated multimodal phenotyping, in order to bridge fragmented research streams and clarify which CNS manifestations in IBD are most clinically relevant, mechanistically informative, and potentially modifiable.
Data Sharing Statement
The data in this study is not of a confidential nature and is accessible in the public domain.
Ethical Approval
Ethical informed consent was not required because no clinical trials or patient consent were involved.
Acknowledgments
The authors would like to acknowledge the editors and the anonymous reviewers for their valuable comments and suggestions to improve the quality of the paper. Furthermore, we thank the Postdoctoral Research Start-up Fund of the First Affiliated Hospital of Army Medical University (grant number 4175zA3726) (No. 2021CFB449) for their support.
Author Contributions
Chen Liu, conceptualization, methodology, supervision, writing – review and editing. Jingwen Li, methodology, investigation, data curation, formal analysis, visualization, writing – original draft preparation. Ru Wen – Methodology, investigation, data curation, validation, writing – review and editing. Yan Zhao, methodology, validation, writing – review and editing. All authors read and approved the content of the manuscript, have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Postdoctoral Research Start-up Fund of the First Affiliated Hospital of Army Medical University (grant number 4175zA3726 & 5175za371N).
Disclosure
The authors declare no conflicts of interest associated with this publication.
References
1. Hodson R. Inflammatory bowel disease. Nature. 2016;540(7634):S97. doi:10.1038/540S97a
2. Kaplan GG. The global burden of IBD: from 2015 to 2025. Nat Rev Gastroenterol Hepatol. 2015;12(12):720–17. doi:10.1038/nrgastro.2015.150
3. Catalan-Serra I, Sebastian S. Global Inflammatory Bowel Disease: opportunities and Challenges for a New Era. United European Gastroenterol J. 2025;13(8):1410–1417. doi:10.1002/ueg2.70075
4. Sebastian S, Siegmund B, Teferra F, et al. Promoting equity in inflammatory bowel disease: a global approach to care. Lancet Gastroenterol Hepatol. 2024;9(3):192–194. doi:10.1016/S2468-1253(23)00368-0
5. Chang JT. Pathophysiology of Inflammatory Bowel Diseases. N Engl J Med. 2020;383(27):2652–2664. doi:10.1056/NEJMra2002697
6. Agrawal M, Spencer EA, Colombel JF, et al. Approach to the Management of Recently Diagnosed Inflammatory Bowel Disease Patients: a User’s Guide for Adult and Pediatric Gastroenterologists. Gastroenterology. 2021;161(1):47–65. doi:10.1053/j.gastro.2021.04.063
7. Torres J, Mehandru S, Colombel JF, et al. Crohn’s disease. Lancet. 2017;389(10080):1741–1755. doi:10.1016/S0140-6736(16)31711-1
8. Ungaro R, Mehandru S, Allen PB, et al. Ulcerative colitis. Lancet. 2017;389(10080):1756–1770. doi:10.1016/S0140-6736(16)32126-2
9. Ananthakrishnan AN, Kaplan GG, Ng SC. Changing Global Epidemiology of Inflammatory Bowel Diseases: sustaining Health Care Delivery Into the 21st Century. Clin Gastroenterol Hepatol. 2020;18(6):1252–1260. doi:10.1016/j.cgh.2020.01.028
10. Singh N, Bernstein CN. Environmental risk factors for inflammatory bowel disease. United European Gastroenterol J. 2022;10(10):1047–1053. doi:10.1002/ueg2.12319
11. Wu T, Cheng H, Zhuang J, et al. Risk factors for inflammatory bowel disease: an umbrella review. Front Cell Infect Microbiol. 2024;14:1410506. doi:10.3389/fcimb.2024.1410506
12. Rogler G, Singh A, Kavanaugh A, et al. Extraintestinal Manifestations of Inflammatory Bowel Disease: current Concepts, Treatment, and Implications for Disease Management. Gastroenterology. 2021;161(4):1118–1132. doi:10.1053/j.gastro.2021.07.042
13. Neuendorf R, Harding A, Stello N, et al. Depression and anxiety in patients with Inflammatory Bowel Disease: a systematic review. J Psychosom Res. 2016;87:70–80. doi:10.1016/j.jpsychores.2016.06.001
14. Barberio B, Zamani M, Black CJ, et al. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(5):359–370. doi:10.1016/S2468-1253(21)00014-5
15. Bisgaard TH, Allin KH, Keefer L, et al. Depression and anxiety in inflammatory bowel disease: epidemiology, mechanisms and treatment. Nat Rev Gastroenterol Hepatol. 2022;19(11):717–726. doi:10.1038/s41575-022-00634-6
16. Horst S, Chao A, Rosen M, et al. Treatment with immunosuppressive therapy may improve depressive symptoms in patients with inflammatory bowel disease. Dig Dis Sci. 2015;60(2):465–470. doi:10.1007/s10620-014-3375-0
17. Kim JS, Chen MH, Wang HE, et al. Inflammatory Bowel Disease and Neurodegenerative Diseases. Gut Liver. 2023;17(4):495–504. doi:10.5009/gnl220523
18. Zong J, Yang Y, Wang H, et al. The two-directional prospective association between inflammatory bowel disease and neurodegenerative disorders: a systematic review and meta-analysis based on longitudinal studies. Front Immunol. 2024;15:1325908. doi:10.3389/fimmu.2024.1325908
19. Tie Y, Huang Y, Chen R, et al. Current insights on the roles of gut microbiota in inflammatory bowel disease-associated extra-intestinal manifestations: pathophysiology and therapeutic targets. Gut Microbes. 2023;15(2):2265028. doi:10.1080/19490976.2023.2265028
20. Matsuoka K, Kanai T. The gut microbiota and inflammatory bowel disease. Semin Immunopathol. 2015;37(1):47–55. doi:10.1007/s00281-014-0454-4
21. Günther C, Rothhammer V, Karow M, et al. The Gut-Brain Axis in Inflammatory Bowel Disease-Current and Future Perspectives. Int J Mol Sci. 2021;22(16):8870. doi:10.3390/ijms22168870
22. Yu DHX, Hong X. A theme evolution and knowledge trajectory study in AHP using science mapping and main path analysis. Expert Syst Applications. 2022;205:117675. doi:10.1016/j.eswa.2022.117675
23. Wang F, Xie J, Xiong H, et al. A bibliometric analysis of inflammatory bowel disease and COVID-19 researches. Front Public Health. 2023;11:1039782. doi:10.3389/fpubh.2023.1039782
24. Wang R, Jiang J, Feng S, et al. Global bibliometric analysis of comorbid depression and anxiety in inflammatory bowel disease (2010–2024). Int J Colorectal Dis. 2026;41(1):41. doi:10.1007/s00384-026-05089-8
25. Asgharnezhad M, Rashidian P, Letafatkar N, et al. Bibliometric analysis of inflammatory bowel disease and emotional factors: trends, impact, and emerging research areas. Ann Med Surg (Lond). 2025;87(12):8405–8417. doi:10.1097/MS9.0000000000003982
26. Brudek T. Inflammatory Bowel Diseases and Parkinson’s Disease. J Parkinsons Dis. 2019;9(s2):S331–S344. doi:10.3233/JPD-191729
27. Chen C, Song IY, Yuan X, Zhang J. The thematic and citation landscape of Data and Knowledge Engineering (1985–2007). Data Knowl Eng. 2008;67(2):234–259. doi:10.1016/j.datak.2008.05.004
28. Bonaz BL, Bernstein CN. Brain-gut interactions in inflammatory bowel disease. Gastroenterology. 2013;144(1):36–49. doi:10.1053/j.gastro.2012.10.003
29. Bravo JA, Forsythe P, Chew MV, et al. Ingestion of Lactobacillus strain regulates emotional behavior and central GABA receptor expression in a mouse via the vagus nerve. Proc Natl Acad Sci U S A. 2011;108(38):16050–16055. doi:10.1073/pnas.1102999108
30. Carabotti M, Scirocco A, Maselli MA, et al. The gut-brain axis: interactions between enteric microbiota, central and enteric nervous systems. Ann Gastroenterol. 2015;28(2):203–209.
31. Cryan JF, Dinan TG. Mind-altering microorganisms: the impact of the gut microbiota on brain and behaviour. Nat Rev Neurosci. 2012;13(10):701–712. doi:10.1038/nrn3346
32. Erny D, Hrabě de Angelis AL, Jaitin D, et al. Host microbiota constantly control maturation and function of microglia in the CNS. Nat Neurosci. 2015;18(7):965–977. doi:10.1038/nn.4030
33. Diaz Heijtz R, Wang S, Anuar F, et al. Normal gut microbiota modulates brain development and behavior. Proc Natl Acad Sci U S A. 2011;108(7):3047–3052. doi:10.1073/pnas.1010529108
34. Sudo N, Chida Y, Aiba Y, et al. Postnatal microbial colonization programs the hypothalamic-pituitary-adrenal system for stress response in mice. J Physiol. 2004;558(Pt 1):263–275. doi:10.1113/jphysiol.2004.063388
35. Cryan JF, O’Riordan KJ, Cowan CSM, et al. The Microbiota-Gut-Brain Axis. Physiol Rev. 2019;99(4):1877–2013. doi:10.1152/physrev.00018.2018
36. Sampson TR, Debelius JW, Thron T, et al. Gut Microbiota Regulate Motor Deficits and Neuroinflammation in a Model of Parkinson’s Disease. Cell. 2016;167(6):1469–1480e1412. doi:10.1016/j.cell.2016.11.018
37. Gracie DJ, Guthrie EA, Hamlin PJ, et al. Bi-directionality of Brain-Gut Interactions in Patients With Inflammatory Bowel Disease. Gastroenterology. 2018;154(6):1635–1646e1633. doi:10.1053/j.gastro.2018.01.027
38. Rhee SH, Pothoulakis C, Mayer EA. Principles and clinical implications of the brain-gut-enteric microbiota axis. Nat Rev Gastroenterol Hepatol. 2009;6(5):306–314. doi:10.1038/nrgastro.2009.35
39. Mayer EA. Gut feelings: the emerging biology of gut-brain communication. Nat Rev Neurosci. 2011;12(8):453–466. doi:10.1038/nrn3071
40. Villarán RF, Espinosa-Oliva AM, Sarmiento M, et al. Ulcerative colitis exacerbates lipopolysaccharide-induced damage to the nigral dopaminergic system: potential risk factor in Parkinson`s disease. J Neurochem. 2010;114(6):1687–1700. doi:10.1111/j.1471-4159.2010.06879.x
41. Meregnani J, Clarençon D, Vivier M, et al. Anti-inflammatory effect of vagus nerve stimulation in a rat model of inflammatory bowel disease. Auton Neurosci. 2011;160(1–2):82–89. doi:10.1016/j.autneu.2010.10.007
42. Bercik P, Denou E, Collins J, et al. The intestinal microbiota affect central levels of brain-derived neurotropic factor and behavior in mice. Gastroenterology. 2011;141(2):599–609. doi:10.1053/j.gastro.2011.04.052
43. Agostini A, Filippini N, Cevolani D, et al. Brain functional changes in patients with ulcerative colitis: a functional magnetic resonance imaging study on emotional processing. Inflamm Bowel Dis. 2011;17(8):1769–1777. doi:10.1002/ibd.21549
44. Agostini A, Benuzzi F, Filippini N, et al. New insights into the brain involvement in patients with Crohn’s disease: a voxel-based morphometry study. Neurogastroenterol Motil. 2013;25(2):147–e182. doi:10.1111/nmo.12017
45. Zikou AK, Kosmidou M, Astrakas LG, et al. Brain involvement in patients with inflammatory bowel disease: a voxel-based morphometry and diffusion tensor imaging study. Eur Radiol. 2014;24(10):2499–2506. doi:10.1007/s00330-014-3242-6
46. Bao CH, Liu P, Liu HR, et al. Alterations in brain grey matter structures in patients with Crohn’s disease and their correlation with psychological distress. J Crohn’s Colitis. 2015;9(7):532–540. doi:10.1093/ecco-jcc/jjv057
47. Bonaz B. Inflammatory bowel diseases: a dysfunction of brain-gut interactions? Minerva Gastroenterol Dietol. 2013;59(3):241–259.
48. Chen Y, Cui W, Li X, et al. Interaction Between Commensal Bacteria, Immune Response and the Intestinal Barrier in Inflammatory Bowel Disease. Front Immunol. 2021;12:761981. doi:10.3389/fimmu.2021.761981
49. Hu J, Johnson TA, Zhang H, et al. The Microbiota-Gut-Brain Axis: gut Microbiota Modulates Conspecific Aggression in Diversely Selected Laying Hens. Microorganisms. 2022;10(6):1081. doi:10.3390/microorganisms10061081
50. Muller PA, Schneeberger M, Matheis F, et al. Microbiota modulate sympathetic neurons via a gut-brain circuit. Nature. 2020;583(7816):441–446. doi:10.1038/s41586-020-2474-7
51. Eslick S, Thompson C, Berthon B, et al. Short-chain fatty acids as anti-inflammatory agents in overweight and obesity: a systematic review and meta-analysis. Nutr Rev. 2022;80(4):838–856. doi:10.1093/nutrit/nuab059
52. Cai J, Sun L, Gonzalez FJ. Gut microbiota-derived bile acids in intestinal immunity, inflammation, and tumorigenesis. Cell Host Microbe. 2022;30(3):289–300. doi:10.1016/j.chom.2022.02.004
53. Mayer EA, Tillisch K, Gupta A. Gut/brain axis and the microbiota. J Clin Invest. 2015;125(3):926–938. doi:10.1172/JCI76304
54. Osadchiy V, Martin CR, Mayer EA. The Gut-Brain Axis and the Microbiome: mechanisms and Clinical Implications. Clin Gastroenterol Hepatol. 2019;17(2):322–332. doi:10.1016/j.cgh.2018.10.002
55. Dinan TG, Cryan JF. Gut-brain axis in 2016: brain-gut-microbiota axis - mood, metabolism and behaviour. Nat Rev Gastroenterol Hepatol. 2017;14(2):69–70. doi:10.1038/nrgastro.2016.200
56. Zeng R, Wang J, Jiang R, et al. Investigating Causality and Shared Genetic Architecture between Neurodegenerative Disorders and Inflammatory Bowel Disease. Aging Dis. 2023;14(4):1349–1359. doi:10.14336/AD.2022.12209
57. Garmendia JV, De Sanctis CV, Das V, et al. Inflammation, Autoimmunity and Neurodegenerative Diseases, Therapeutics and Beyond. Curr Neuropharmacol. 2024;22(6):1080–1109. doi:10.2174/1570159X22666231017141636
58. Kim GH, Lee YC, Kim TJ, et al. Risk of Neurodegenerative Diseases in Patients with Inflammatory Bowel Disease: a Nationwide Population-based Cohort Study. J Crohn’s Colitis. 2022;16(3):436–443. doi:10.1093/ecco-jcc/jjab162
59. Zhu F, Li C, Gong J, et al. The risk of Parkinson’s disease in inflammatory bowel disease: a systematic review and meta-analysis. Dig Liver Dis. 2019;51(1):38–42. doi:10.1016/j.dld.2018.09.017
60. Fu P, Gao M, Yung KKL. Association of Intestinal Disorders with Parkinson’s Disease and Alzheimer’s Disease: a Systematic Review and Meta-Analysis. ACS Chem Neurosci. 2020;11(3):395–405. doi:10.1021/acschemneuro.9b00607
61. Herrick MK, Tansey MG. Is LRRK2 the missing link between inflammatory bowel disease and Parkinson’s disease? NPJ Parkinsons Dis. 2021;7(1):26. doi:10.1038/s41531-021-00170-1
62. Lewis JD, Sandler RS, Brotherton C, et al. A Randomized Trial Comparing the Specific Carbohydrate Diet to a Mediterranean Diet in Adults With Crohn’s Disease. Gastroenterology. 2021;161(3):837–852e839. doi:10.1053/j.gastro.2021.05.047
63. Goyal A, Yeh A, Bush BR, et al. Safety, Clinical Response, and Microbiome Findings Following Fecal Microbiota Transplant in Children With Inflammatory Bowel Disease. Inflamm Bowel Dis. 2018;24(2):410–421. doi:10.1093/ibd/izx035
64. Perry S, Pillarisetti L, Gelfman T, et al. Gut-Brain Axis in Inflammatory Bowel Disease: pathogenesis and Therapeutics. Arch Intern Med Res. 2025;8(4):339–345. doi:10.26502/aimr.0227
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Bibliometric Analysis: Research Trends and Performances of Stroke on Acupuncture
Yang F, Cui Y, Zhao Y, Jiao H
Journal of Pain Research 2024, 17:1837-1851
Published Date: 22 May 2024
Theoretical Domains Framework: A Bibliometric and Visualization Analysis from 2005-2023
Zhou Y, Huang Y, Wang Y, Xu X, Yu Z, Gu Y
Journal of Multidisciplinary Healthcare 2024, 17:4055-4069
Published Date: 20 August 2024
The Traditional Chinese Medicine in Treating Diabetic Nephropathy: A Bibliometric Analysis
Sun J, Shen J, Liu L, Du J
Journal of Multidisciplinary Healthcare 2024, 17:4627-4636
Published Date: 4 October 2024
Exploring Research Trends and Mechanisms: Maternal Diabetes and Neural Tube Defects (1991–2023)
Cao L, Xi Y, Jing Z, Bao Z, Bai B, Lian X, Zhang X, Di J, Liu F
Journal of Multidisciplinary Healthcare 2025, 18:1107-1121
Published Date: 25 February 2025
Research Hotspots in Natural Products for Wound Healing: A Bibliometric Analysis and Literature Review
Yang F, Fang Z, Yang M, Cheng Z, Tian Y, Liang J, Li T
Clinical, Cosmetic and Investigational Dermatology 2025, 18:1985-1997
Published Date: 22 August 2025