Back to Journals » International Journal of Women's Health » Volume 17
Causal Link Between Thyroid Function and Female-Specific Cancers: A Bidirectional Two-Sample and Mediation Mendelian Randomization Study
Authors Gao B, Zhang C, Wang D, Luo D, Shan Z, Teng W, Tao T, Li J ![]()
Received 9 July 2025
Accepted for publication 10 October 2025
Published 27 October 2025 Volume 2025:17 Pages 3913—3927
DOI https://doi.org/10.2147/IJWH.S552719
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Bingrui Gao,1 Chenxi Zhang,1 Deping Wang,1,2 Dongdong Luo,1,3 Zhongyan Shan,1 Weiping Teng,1 Tao Tao,4 Jing Li1
1Department of Endocrinology and Metabolism, The Institute of Endocrinology, NHC Key Laboratory of Diagnosis and Treatment of Thyroid Diseases, The First Affiliated Hospital of China Medical University, Shenyang, Liaoning, 110000, People’s Republic of China; 2Department of Endocrinology and Metabolism, Hongqi Hospital Affiliated to Mudanjiang Medical College, Mudanjiang, Heilongjiang, 157011, People’s Republic of China; 3Department of Endocrinology and Metabolism, The Second Hospital of Dalian Medical University, Dalian, Liaoning, 116027, People’s Republic of China; 4Department of Endocrinology and Metabolism, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, 200127, People’s Republic of China
Correspondence: Jing Li, Department of Endocrinology and Metabolism, The Institute of Endocrinology, NHC Key Laboratory of Diagnosis and Treatment of Thyroid Diseases, The First Affiliated Hospital of China Medical University, Shenyang, Liaoning, 110000, People’s Republic of China, Email [email protected]; [email protected]
Background: Observational studies have reported associations between thyroid function, encompassing free thyroxine, thyroid-stimulating hormone, hyperthyroidism, and hypothyroidism, and female-specific cancers such as endometrial, breast, ovarian, and cervical cancers. However, the causal relationship remains unclear.
Objective: The researchers aimed to explore the causal relationship between thyroid function and female-specific cancers, while also investigating the role of sex hormones (total testosterone and estradiol) as potential mediators in this association.
Methods: Initially, the researchers preformed bidirectional two-sample (T-S) Mendelian randomization (MR) analysis using summary-level Genome-wide association studies to investigate the causal relationship between thyroid function and female-specific cancers. Subsequently, the researchers employed mediation MR analysis to assess the potential role of sex hormones as intermediaries in this relationship. The robustness of the findings of this study was further validated through a series of sensitivity analyses. Lastly, the researchers conducted bioinformatics analyses to explore underlying mechanisms, leveraging potentially relevant genes.
Results: Bidirectional T-S MR analyses indicated that hypothyroidism reduces the risk of endometrial cancer (OR: 0.33, P = 0.002) and breast cancer (OR: 0.48, P < 0.001). Mediation MR analyses further suggested that hypothyroidism may lower the risk of both endometrial and breast cancers by decreasing levels of total testosterone.
Conclusion: The researchers established the causal relationship between thyroid function and female-specific cancers, offering novel perspectives for the early prevention and intervention of endometrial and breast cancer. Furthermore, the researchers investigated the mediating role of sex hormones in the association between hypothyroidism and these cancers, providing valuable insights for future mechanistic research.
Keywords: thyroid function, cancer, female, testosterone, causality, mendelian randomization
Introduction
The thyroid, a vital endocrine organ and the largest gland of the endocrine system in the human body,1,2 serves a multifaceted regulatory function, encompassing bodily growth, development, and energy metabolism,3 while also participating in the feedback mechanisms of the hypothalamus and pituitary gland.4 Thyroid dysfunction could result in major harm to the body. Studies have shown that thyroid disorders are associated with various cancers and even impact the survival of patients with cancer. A prospective study indicates that patients with hypothyroidism exhibit a decreased risk of prostate cancer,5 while another controlled clinical study suggests that hypothyroidism is linked to a reduced risk of colorectal cancer.6
Epidemiological studies have revealed that the prevalence of thyroid dysfunction is significantly higher in females than in males7 and that the thyroid gland influences the female reproductive system both directly and indirectly through pleiotropic mechanisms.8,9 A prospective database study demonstrated that patients with endometrial cancer diagnosed with hypothyroidism experienced improved overall survival, cancer-specific survival, and recurrence-free survival.10 However, the relationship between thyroid function and female-specific cancers requires further investigation. Female-specific cancers primarily encompass endometrial cancer, breast cancer, ovarian cancer, and cervical cancer.11 Among these, endometrial cancer, breast cancer, and ovarian cancer are classified as hormone-sensitive tumors.12 These cancers are seriously affecting the health of females all over the world. According to the oncology database GLOBOCAN, the incidence of female breast, cervical, endometrial, and ovarian cancers ranks first, fourth, sixth, and eighth globally, respectively.13 Furthermore, breast, cervical, and ovarian cancers are the primary causes of cancer-related fatalities among women, ranking first, fourth, and eighth worldwide.14 Unfortunately, the early diagnosis of female-specific cancers remains a considerable challenge, with over 60% of patients being diagnosed at advanced stages and a five-year overall survival rate of less than 30%.15 Therefore, early identification of protective and risk factors for these cancers is essential for effective prevention and timely intervention.
Mendelian randomization (MR) study, as a research method widely used in recent years, explores the causal relationship between exposure and control through single nucleotide polymorphisms (SNPs), which can minimize the influence of different confounding factors on the results.16 Given that the causal relationship between thyroid function and female-specific cancers remains unclear, this study aims to explore this relationship through bidirectional two-sample MR (T-S MR) analysis. Additionally, the researchers examine the potential role of sex hormones as mediators in the association between thyroid function and female-specific cancers using mediation MR analysis. Furthermore, the researchers predicted the potential pro-cancer mechanisms and regulatory pathways through which androgens influence breast and endometrial cancers via bioinformatic analysis. This offers novel strategies for the early prevention and hormonal therapy of female-specific cancers.
Material and Methods
Study Design of MR Study
The researchers employed a bidirectional T-S MR study to investigate the effect of thyroid function—specifically hyperthyroidism, hypothyroidism, serum thyroid-stimulating hormone (TSH), and serum free thyroxine (FT4) levels—on the risk of developing female-specific cancers, including breast, endometrial, ovarian, and cervical cancer. Additionally, we explored the potential mediating role of sex hormones, namely total testosterone and estradiol, using mediation MR analysis (Figure 1). To confirm the validity of the study, three assumptions needed to be met:17 1) there must be a strong link between the instrumental variables (IVs) and thyroid function; 2) the IVs must not be linked to any possible confounders of female-specific cancers or thyroid function; and 3) thyroid function should be the sole pathway through which the independent variables impact the outcome variables (Figure 1). This study followed the STROBE-MR guidelines18 (Table S1).
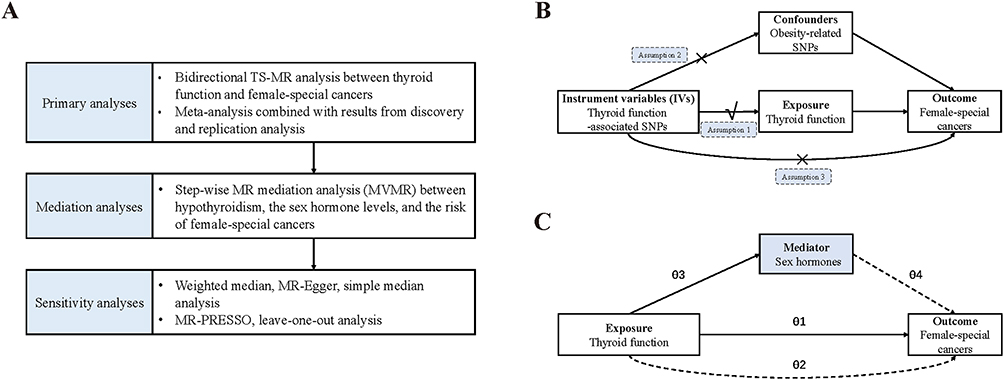 |
Figure 1 Flowchart of the Mendelian randomization Study. (A). Flowchart of the MR study; (B) Diagram of the MR assumptions of the association between thyroid function and female-specific cancers; (C) Illustrative diagram for the mediation MR analysis framework. Abbreviations: MR, mendelian randomization; TS-MR, two-sample MR; MVMR, multivariable MR; SNPs, single-nucleotide polymorphisms; √, there must be a strong link between the instrumental variables (IVs) and thyroid function; ×, the IVs must not be linked to any possible confounders of female-specific cancers or thyroid function, and thyroid function should be the sole pathway through which the independent variables impact the outcome variables; θ1, total effect of thyroid function on the risk of female-special cancers; θ2, direct effect of thyroid function on the risk of female-special cancers; θ3, direct effect of thyroid function on the sex hormones; θ4, direct effect of the sex hormones on the risk of female-special cancers. |
Data Source and IVs Selection of MR Study
Summary data related to hypothyroidism were obtained from the study by Loh et alwhich was obtained by the BOLT-LMM Bayesian mixed model association method and included a total of 473,703 participants.19 The GWAS database associated with hyperthyroidism was obtained from a study containing 484,598 participants, including 3731 cases of hyperthyroidism.20 Thyroid hormone-related databases were derived from a meta-analysis of pooled GWAS data, with pooled data for TSH from 54,288 participants and pooled data for FT4 from 49,269 participants.21 The data related to endometrial cancer used in this study were obtained from the ECAC study, which included 108,979 controls and 12,906 cases.22 Data for endometrial cancer replication analyses were derived from the UKB study that included 460,499 participants.23 Breast cancer-related data came from a meta-analysis (122,977 breast cancer cases and 21,468 controls), which is the largest GWAS pooled data related to breast cancer.24 Data for the breast cancer replication analyses were obtained from the Finnish database and the pooled UKB database, comprising 6325 cases and 73225 controls.23 The data related to ovarian cancer exploited in this study were obtained from the OCAC GWAS study, which included 25,509 cases and 40,941 controls.25 Data on ovarian cancer for replication analyses came from the UKB study, which included 1588 cases and 244932 controls.23 Cervical cancer data were obtained from a study by Sakaue et al that included 460,499 participants.23 Data from cervical cancer for replication analyses were obtained from the public database MR base (ieu-b-876). Burrows et al released the database in 2021, which included 536 cases of cervical cancer and 198,523 controls.26 The GWAS database relating to sex hormones was derived from a combination of three studies (CHARGE Consortium, Twins UK and EPIC-Norfolk) and is the largest GWAS database for sex hormones currently available.27 The GWAS databases used in this study are publicly available on the IEU open GWAS project (https://gwas.mrcieu.ac.uk/) and the ThyroidOmics Consortium (http://www.thyroidomics.com). Databases used for analysis are summarized in Table S2.
Initially, we selected SNPs with genome-wide significance (P < 5*10−8) that were co-matched in the exposure and outcome databases. Subsequently, we conducted a clustering procedure with an r2 threshold of 0.001 and a clumping window of 10,000 kb to reduce linkage disequilibrium. To eliminate horizontal pleiotropy, we excluded outlier SNPs by MR-PRESSO analysis.28 Subsequently, we excluded SNPs associated with body mass index and waist circumference by searching LDTrait.29,30 All SNPs had F-statistics greater than 10. We determined the R2 value for each SNP to explain the variance.31,32 Information on all included SNPs is summarized in Tables S3–S8.
Statistical Analysis of MR Study
Firstly, we employed a bidirectional TS-MR study to explore the causal relationship between thyroid function and female-specific cancers. If Cochran’s Q test indicated heterogeneity, the random-effects inverse-variance weighting (IVW) method was applied; otherwise, the fixed-effects IVW approach was used.26,33 To enhance the reliability of the results, two databases were employed for each outcome variable. Discovery and replication analyses were performed, and the results from both analyses were combined to derive a pooled estimate through meta-analysis. Secondly, a stepwise MR analysis was employed to explore the role of sex hormones as mediators. The coefficient product and multivariate delta methods34,35 were used to assess the mediating effect of sex hormones on the relationship between exposure and outcome.
The following methods were employed for sensitivity analyses. Initially, we performed weighted median,36 MR-Egger regression,37 and weighted mode analysis.38 MR-Egger regression analysis was employed to identify and adjust for horizontal pleiotropy, while the weighted median method ensures accurate estimates despite imperfect IVs. The weighted mode can split SNPs into groups and determine causal effects for the largest subset. Secondly, we eliminated the influence of individual SNPs on the test results through leave-one-out (LOO) analysis.38 Lastly, we conducted MR-PRESSO analysis to exclude outlier SNPs,28 and excluded the effect of obesity-related SNPs on the results by LDTrait.29,30
All analyses were conducted using R version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria). The packages of the TwoSampleMR, the MRPRESSO, and the MVMR in the R software were used.39 A P-value of 0.05 was regarded as statistically significant.
Bioinformatic Analysis
The largest global dataset of whole blood expression quantitative trait loci (eQTL) was used, obtained from the eQTGen Consortium, featuring cis-eQTLs data for 19,250 genes expressed in whole blood from 31,684 participants.40 We used the dataset to genetically annotate the SNPs of total testosterone-endometrial cancer (n-SNP=165) and total testosterone-breast cancer (n-SNP=131) data. Potentially relevant genes for the links between total testosterone with both endometrial and breast cancer were identified by selecting those with P-value under 5*10-8 and FDR under 0.05 (Tables S13 and S14).
We subsequently conducted bioinformatics analyses using these potentially relevant genes, utilizing expression profiling data from the Cancer Genome Atlas (TCGA) RNA-seq cohort (https://tcga-data.nci.nih.gov/tcga/). Specifically, we employed expression data from the Breast Invasive Carcinoma (BRCA) and Uterine Corpus Endometrial Carcinoma (UCEC) datasets. Differential gene expression analyses were conducted using the “Limma”, “dplyr”, and “tidyverse” R packages, with thresholds set at |Log2FC| > 1 and FDR < 0.05. Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analyses of differential expression were performed and plotted using “clusterProfiler”, “enrichplot”, “org.Hs.eg.db”, “ggplot2”, and “GOplot” were used for analysis and mapping. P < 0.05 was considered significant.
Results
Primary Analyses
After rigorous screening, a total of 13–124 SNPs were selected as IVs related to thyroid function and 2–16 SNPs were selected as IVs related to female-specific cancer. To minimize the potential bias caused by weak instruments, we ensured that each SNP had an F-statistic greater than 10 (Tables S3–S8). In the main analyses, we analyzed the results using the IVW method. Firstly, the results of the discovery analysis showed that hypothyroidism was negatively associated with endometrial cancer (n = 121 SNPs, OR: 0.30, P = 0.007) (Figure 2). The results of the replication analyses also showed a consistent direction (n = 124 SNPs, OR: 0.38, P = 0.102), and the final estimates of the meta-analyses were consistent with the results of the discovery analyses (OR: 0.33, P = 0.002) (Figure 2). Secondly, the results of both discovery (n = 109 SNPs, OR: 0.20, P = 0.002) and replication (n = 121 SNPs, OR: 0.52, P = 0.002) analyses suggested that hypothyroidism was negatively associated with breast cancer (Figure 2), and the final estimates of the meta-analyses also showed consistency (OR: 0.48, P < 0.001) (Figure 2). Figure 2 Continued. Figure 2 Forest plots of the causal associations between thyroid function and female-specific cancers. (A) Causal association between thyroid function and endometrial cancer; (B) Causal association between thyroid function and breast cancer; (C) Causal association between thyroid function and cervical cancer; (D) Causal association between thyroid function and ovarian cancer. Abbreviations: SNP, single-nucleotide polymorphism; OR, odds ratio; CI, confidence interval; IVW, inverse variance weighted.

Both the discovery and replication studies showed no significant connection between thyroid function and ovarian or cervical cancer (Figure 2). There was also no indication of a causal connection between female-specific cancers and thyroid function (Figure 3).
 |
Figure 3 Forest plots of the causal associations between female-specific cancers and thyroid function. Abbreviations: SNP, single-nucleotide polymorphism; OR, odds ratio; CI, confidence interval; IVW, inverse variance weighted. |
Mediation Analyses
Firstly, regarding hypothyroidism and endometrial cancer, MVMR analysis (adjusted for total testosterone) revealed a direct causal effect of hypothyroidism on the risk of endometrial cancer (OR: 0.32, P = 0.043) (Table 1), and TS-MR analysis showed a negative correlation between hypothyroidism and serum total testosterone levels (OR: 0.80, P < 0.001) (Table 1). Also, MVMR analysis (adjusted for hypothyroidism) demonstrated a causal association between serum total testosterone levels and endometrial cancer (OR: 1.47, P = 0.017) (Table 1). Taken together, we have identified a potential mediating pathway between hypothyroidism and endometrial cancer: hypothyroidism ultimately exerts an indirect causal effect on the risk of endometrial cancer by affecting total testosterone levels (θ3 × θ4) (OR: 0.92, P = 0.034) (Table 1). This pathway mediated 6.1% of the total causal effect of hypothyroidism on endometrial cancer risk. Detailed results of the mediation analyses are shown in Table 1.
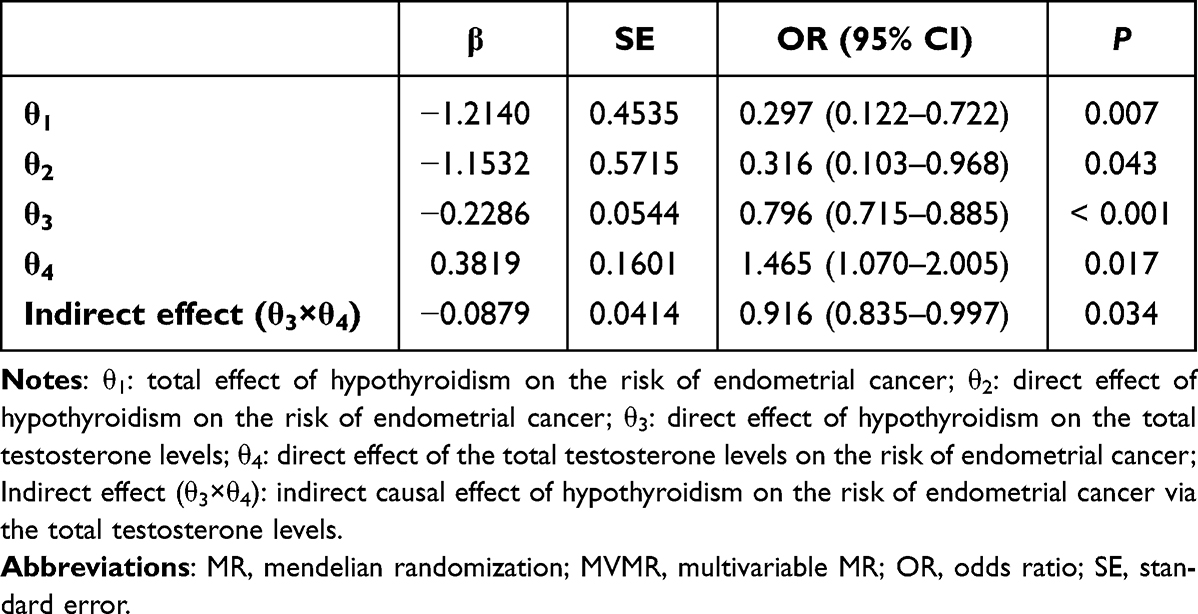 |
Table 1 Step-Wise MR Mediation Analysis (MVMR) Results Between Hypothyroidism, the Total Testosterone Levels, and the Risk of Endometrial Cancer |
Secondly, within hypothyroidism and breast cancer, the results of MVMR analysis showed a directly causal relationship between hypothyroidism and breast cancer (OR: 0.14, P = 0.001) (Table 2), and the results of TS-MR analysis revealed the role of hypothyroidism on serum total testosterone levels (OR: 0.80, P < 0.001) (Table 2). Also, the results of MVMR analysis revealed the direct effect between serum total testosterone levels and endometrial cancer (OR: 1.80, P = 0.003) (Table 2). In summary, the potential mediating pathway that exists between hypothyroidism and breast cancer is that hypothyroidism can ultimately affect the risk of breast cancer by affecting total testosterone levels (θ3 × θ4) (OR: 0.88, P = 0.003) (Table 2). This pathway explained 8.22% of the overall causal impact of hypothyroidism on the risk of breast cancer risk. A comprehensive summary of these findings is provided in Table 2.
 |
Table 2 Step-Wise MR Mediation Analysis (MVMR) Results Between Hypothyroidism, the Total Testosterone Levels, and the Risk of Breast Cancer |
Sensitivity Analyses of Mendelian Randomization Study
To eliminate the influence of various factors on the results, we conducted a series of sensitivity analyses. Firstly, the directions of the results from the MR-egger regression, the weighted median analysis and the weighted mode analysis were consistent with the findings from the IVW analysis (Tables S10–S12). Secondly, scatter plots and forest plots were used to illustrate the effect of each SNP on the outcome (Figures S1 and S3). Thirdly, we employed MR-Egger P intercepts and funnel plots to exclude the impact of horizontal pleiotropy on the results (Table S9 and Figure S2). Fourth, the LOO analyses results demonstrated that our findings were not influenced by individual SNPs (Figure S4). Finally, we removed outlier SNPs using the MR-PRESSO method and excluded obesity-related SNPs through the LDTrait database.
Bioinformatics Study
According to the MR analyses, hypothyroidism may decrease the risk of endometrial and breast cancers, with total testosterone acting as a mediator between them. This suggests that hypothyroidism may ultimately influence the risk of endometrial and breast cancers by modulating total testosterone levels. Building on these findings, we collected SNPs for the total testosterone-endometrial cancer and total testosterone-breast cancer associations, and integrated these SNPs with the cis-eQTL dataset for gene annotation. Ultimately, 256 potentially relevant genes for total testosterone-endometrial cancer and 228 for total testosterone-breast cancer were identified (Tables S13 and S14). We conducted bioinformatics analyses using these potentially relevant genes. The TCGA database provides expression profiling data for 113 cases of breast invasive para-carcinoma tissue, 1,098 cases of breast invasive carcinoma tissue, 35 cases of endometrial para-carcinoma tissue, and 544 cases of endometrial carcinoma tissue. Through KEGG analysis of these differential genes, we enriched the “Rap1 signaling pathway”, “Cellular senescence”, “Regulation of actin cytoskeleton”, “MAPK signaling pathway”, “Ras signaling pathway”, and “Neuroactive ligand-receptor interaction” in breast cancer (Figure 4). In endometrial cancer, the enriched pathways included “Rap1 signaling pathway”, “Phospholipase D signaling pathway”, “Apelin signaling pathway”, “Cellular senescence”, and “Vitamin digestion and absorption” (Figure 4). Tables S15 and S16 provide a detailed summary of the analysis results.
 |
Figure 4 Circle plots of the results of the pathway enrichment analysis between total testosterone with (A) breast cancer and (B) endometrial cancer. |
Discussion
Using the large-scale GWAS summary data, the researchers comprehensively explored the relationship between thyroid function and the risk of four female-specific cancers through MR analyses. The results revealed a negative causal relationship between hypothyroidism with endometrial cancer (OR: 0.33, P = 0.002) and breast cancer (OR = 0.48, 95% CI: 0.36–0.64, P < 0.001). However, no causal relationship was found between thyroid function and ovarian cancer or cervical cancer. Additionally, we further investigated the mediating role of sex hormones between hypothyroidism with endometrial cancer (OR: 0.92, P = 0.034) and breast cancer (OR: 0.88, P = 0.003) through mediation MR analysis. This analysis clarified that hypothyroidism could reduce the risk of both endometrial and breast cancers by lowering total testosterone levels, with mediating effects of 6.1% and 8.2%, respectively. Simultaneously, we predicted the potential oncogenic mechanisms of androgens using the expression profiles of breast invasive carcinoma and endometrial carcinoma from the TCGA database. The results suggested that androgens may influence processes such as cellular senescence, regulation of the actin cytoskeleton, neuroactive ligand-receptor interactions, vitamin digestion and absorption, as well as the modulation of the Rap1, Ras, MAPK, Apelin, and Phospholipase D signaling pathways.
Thyroid hormones (THs) play a crucial role in regulating normal growth and metabolism, influencing both basal and adaptive metabolic rates.41–43 Thyroid dysfunction, including hyperthyroidism and hypothyroidism,44 can directly or indirectly impact the development and progression of various diseases. The metabolic regulation mediated by THs links them to conditions such as coronary heart disease,45 diabetes mellitus,46 and aging-related diseases.47 Thyroid dysfunction exerts a range of effects on the body, influencing cancer-related molecular signaling pathways and thereby affecting cancer development and progression. For instance, the integrin-thyroid hormone binding region can be stimulated by T3 and T4,48 leading to the phosphorylation and activation of phosphatidylinositol 3-kinase (PI3K), as well as the activation of the oncogenic ERK1/2 pathway via the S2 site of αvβ3.49–51 Additionally, when PI3K is activated by T3 or T4, it triggers the expression of the α-subunit of hypoxia-inducible factor 1 (HIF-1), a transcription factor.52,53 The target genes of HIF-1 are primarily involved in tumor angiogenesis and adaptation to hypoxia, thereby promoting tumor migration and invasion.54 Numerous population studies have demonstrated strong associations between thyroid function and the progression of various cancers, including liver cancer,55 thyroid cancer,56–58 breast cancer,59 lung cancer,60 and colon cancer.61–63
Several cancer prognostic data analyses suggest that mild hypothyroidism may prolong survival in cancer patients. An observational study on glioblastoma indicated that mild hypothyroidism was associated with extended survival in tumor patients.64 In animal experiments, the induction of hypothyroidism using methimazole was found to inhibit tumor growth and prolong survival, compared to a thyroid function-normal animal model of lung cancer with homogeneous tumors.65 Our study obtained results consistent with previous observational and experimental studies, demonstrating that hypothyroidism can reduce the risk of female-specific cancers, particularly endometrial and breast cancers. This coincides with the findings of earlier observational studies. A prospective database study, for instance, indicated that endometrial cancer patients with hypothyroidism had better overall survival, cancer-specific survival, and a lower risk of cancer recurrence than those with normal thyroid function.10 A study by Wang et al demonstrated that in European population, hypothyroidism was linked to a lower risk of breast cancer.66 However, our research did not determine a causal relationship between hyperthyroidism and female-specific cancers. This may be due to the need for further investigation into the causal link between hyperthyroidism and female-specific tumors, as this relationship is likely influenced by additional confounding factors in clinical studies. Moreover, the physiological responses involved in the development of hyperthyroidism may be more complex, complicating the analysis of its effects on cancer risk. Other studies have reached similar conclusions. A study by Crosbie et al, involving 333 women with endometrial cancer, found that women diagnosed with hypothyroidism had improved overall survival and reduced cancer recurrence compared to those with normal thyroid function. However, the effect of hyperthyroidism on these patients did not reach statistical significance.10 Similarly, an MR study investigating the causal relationship between thyroid function and gastric cancer found only a significant negative correlation between hypothyroidism and gastric cancer.67 Building on these findings, we further explored the role of sex hormones as mediators in the association between hypothyroidism and both endometrial and breast cancers, elucidating the potential regulatory role of the “thyroid-gonadal axis” in female-specific cancers.
Sex hormones, primarily estrogens and androgens,68 are crucial for maintaining cellular balance and controlling mitosis and cell proliferation.69,70 Moreover, sex hormones also regulate the development of hormone-sensitive cancers, such as endometrial cancer, breast cancer, and prostate cancer. Studies have shown that androgens can bind to their receptors, promoting the dissociation of heat shock proteins, and facilitating the translocation of the receptor to the nucleus for dimerization. This process activates androgen-responsive elements, thereby regulating the transcription of target genes within their promoter regions and ultimately amplifying hormonal signaling cascades.71,72 Androgen receptor-mediated signaling pathways, including Wnt7B transcription and the upregulation of the β-catenin pathway, indirectly influence the pro-carcinogenic pathway associated with human epidermal growth factor signaling.73 Numerous studies based on populations have investigated the link between sex hormones and the risk of cancer; however, the findings remain inconclusive. For instance, a study by Reeves et al reported a significant increase in breast cancer risk with rising testosterone levels.74 In contrast, another study has suggested that serum testosterone levels may impact the risk of gastric and colorectal cancers, although this effect was not observed in women.75 The study results showed that increased total testosterone levels correlate with a heightened risk of breast and endometrial cancer, supporting the conclusions of various observational studies. A prospective meta-analysis further demonstrated a positive correlation between testosterone levels and the risk of developing breast cancer.76 A cohort study conducted by Yang et al using the UK Biobank database found that serum testosterone levels were a significant risk factor for the development of breast cancer.77 Similarly, an observational study by Murphy et al demonstrated that elevated levels of both total testosterone and free testosterone were positively associated with the risk of endometrial cancer in women, regardless of menopausal status.78
Hypothyroidism can lead to alterations in the female reproductive endocrine system.79 However, no studies have yet verified whether thyroid dysfunction can influence the risk of breast and endometrial cancer by modulating the secretion of sex hormones. The results of our mediation analyses indicated that hypothyroidism could ultimately reduce the risk of both endometrial and breast cancer by lowering total testosterone levels. This offers crucial insights for subsequent mechanistic studies. Firstly, hormones interact with one another to produce a “crosstalk” effect, and the “thyroid-androgen” axis may represent a potential mechanism underlying the development of breast and endometrial cancers. Evidence suggests that THs act synergistically with the androgen receptor by binding to its promoter region,80 as well as promoting the production of androgen synthase, specifically 5α-reductase.81 When hypothyroidism occurs, it inevitably leads to fluctuations in androgen levels. Under these conditions, the androgen receptor translocates between the nucleus and cytoplasm in an inactive state, disrupting normal cell growth and the cell cycle. Furthermore, this alteration interferes with the binding of initiating regions of metabolic target genes to androgen-responsive elements, which may ultimately influence the risk of breast cancer and endometrial cancer.82 On the other hand, THs can directly promote the synthesis of sex hormone-binding globulin (SHBG) in the liver. When hypothyroidism occurs, a reduction in thyroid hormone levels leads to a decline in serum SHBG levels, which in turn increases the metabolic clearance of testosterone, ultimately resulting in decreased serum total testosterone levels.83 Additionally, the thyroid and gonads are tightly regulated by both the hypothalamus and the pituitary gland.84 Thyroid dysfunction triggers feedback to the hypothalamic-pituitary axis,21 which subsequently impacts the regulatory effects of this axis on the gonads, resulting in a continuous response to fluctuations in hormone levels throughout the body.47,85 Studies have demonstrated that serum testosterone levels are significantly lower in patients with hypothyroidism compared to control populations.86,87 According to the bioinformatics analyses conducted in this study, androgen-related genes may play a role in cancer-associated pathways, such as the Rap1, Ras, and MAPK signaling pathways, in both endometrial and breast cancer. Notably, all of these pathways are either directly or indirectly regulated by thyroid hormones.88–90
The androgen receptor and estrogen receptor are widely recognized as critical therapeutic targets in various cancers, including breast cancer,91 prostate cancer,92 endometrial cancer,93 and ovarian cancer.93 Currently, androgen and androgen receptor-targeted therapies are extensively employed in the treatment of prostate cancer.94,95 Moreover, androgen receptor-targeted therapeutic approaches for breast cancer are under development and have demonstrated promising outcomes in clinical trials.96 In conjunction with the findings from this study regarding the “thyroid-androgen” regulatory axis, we suggest that a combination of multiple hormones could be considered as a therapeutic approach for breast cancer and endometrial cancer. This strategy may effectively counteract the synergistic effects of various hormones, thereby slowing disease progression and improving patient prognosis. At the same time, thyroid function in patients with breast cancer and endometrial cancer should be closely monitored, and the dosage of thyroid hormone replacement therapy should be carefully adjusted for those with hypothyroidism, avoid over-treatment of both clinical and subclinical hypothyroidism. Future large-scale, multicenter prospective studies are needed to identify optimal treatment strategies for breast cancer and endometrial cancer patients with hypothyroidism.
Our study has several advantages. Firstly, utilizing a large-scale GWAS summary dataset, it explores the causal relationship between thyroid function and the risk of four female-specific cancers in a more comprehensive manner. This approach overcomes the limitations of observational studies, which are often unable to establish causality and are susceptible to confounding factors. Secondly, we employed mediation MR analysis to investigate the role of sex hormones as mediators in the relationship between hypothyroidism and the risk of endometrial and breast cancer, providing valuable insights for future mechanistic studies. Finally, to enhance the reliability and robustness of the findings, we conducted a meta-analysis incorporating results from two independent databases. However, this study has several limitations. First, it is based solely on data from the European population, and further research involving diverse ethnic groups is necessary to validate and expand our findings. Second, the absence of relevant databases hindered our ability to focus on specific pathological subtypes of female-specific cancers, a limitation that warrants further investigation in future studies.
Conclusions
In conclusion, this study identified a causal relationship between hypothyroidism and a reduced risk of endometrial and breast cancer. Furthermore, hypothyroidism may influence the incidence of these cancers by modulating serum total testosterone levels. These findings underscore the importance of the “thyroid-androgen” regulatory axis in the pathogenesis of both endometrial and breast cancer, suggesting that it warrants further investigation. Moreover, timely monitoring of thyroid function and appropriate treatment of hypothyroidism are of significant importance for the prevention and management of endometrial and breast cancer.
Abbreviations
MR, Mendelian randomization; TS-MR, Two-sample Mendelian randomization; SNPs, Single-nucleotide polymorphisms; UKB, UK Biobank; IVs, Instrumental variables; IVW, Inverse variance weighted; LOO, Leave one out; eQTL, Expression quantitative trait loci; Cis-eQTLs, Cis-expression quantitative loci; TCGA, The Cancer Genome Atlas; BRCA, The Breast Invasive Carcinoma; UCEC, Uterine Corpus Endometrial Carcinoma; KEGG, Kyoto Encyclopedia of Genes and Genomes; GWAS, Genome-wide association studies; THs, Thyroid hormones; HIF-1, Hypoxia-inducible factor 1; SHBG, Sex hormone-binding globulin; TSH, Thyroid-stimulating hormone; FT4, Free thyroxine.
Data Sharing Statement
All datasets used in the MR analysis are publicly available through the GWAS catalog, and the data generated or analyzed are included in this article (and in the Supplementary Information File).
Ethical Approval and Consent to Participate
Since the GWAS data used in this study are derived entirely from publicly available summary-level statistics, ethical approval is not required. According to Article 32 of China’s Measures for the Ethical Review of Biomedical Research Involving Humans (effective Feb 18, 2023), biomedical research involving human participants may be exempt from ethical review under the following conditions: 1. Item 1: Research based on public databases that does not involve the identification or use of personal information. 2. Item 2: Analysis of collected data that does not involve the collection of new data or direct intervention in participants. Our analysis used only publicly available, de-identified data and involved no new data collection or human interaction, meeting the criteria for exemption.
Acknowledgments
We would like to express our sincere gratitude to the compilers of the GWAS summary dataset for their management of the data collection and data resources.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key Research and Development Program of China (grant number No.2023YFC2508303), the General Program of National Natural Science Foundation of China (grant number No.81771741), Distinguished Professor at Educational Department of Liaoning Province (grant number No. [2014]187), the Basic Scientific Research Project of Liaoning Provincial Department of Education (grant number No.LJ212410159030), the Beijing Medical Award Foundation (grant number No. YXJL-2024-0350-0089) to JL.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yang H, Xing R, Liu S, Yu H, Li P. Analysis of the protective effects of γ-aminobutyric acid during fluoride-induced hypothyroidism in male Kunming mice. Pharm Biol. 2019;57(1):28–36. doi:10.1080/13880209.2018.1563621
2. Dirinck E, Dirtu A, Malarvannan G, Covaci A, Jorens P, Van Gaal L. A Preliminary Link between Hydroxylated Metabolites of Polychlorinated Biphenyls and Free Thyroxin in Humans. Int J Environ Res Public Health. 2016;13(4):421. doi:10.3390/ijerph13040421
3. Biondi B, Cappola AR, Cooper DS. Subclinical Hypothyroidism: a Review. JAMA. 2019;322(2):153. doi:10.1001/jama.2019.9052
4. Babić Leko M, Gunjača I, Pleić N, Zemunik T. Environmental Factors Affecting Thyroid-Stimulating Hormone and Thyroid Hormone Levels. Int J Mol Sci. 2021;22(12):6521. doi:10.3390/ijms22126521
5. Mondul AM, Weinstein SJ, Bosworth T, Remaley AT, Virtamo J, Albanes D. Circulating thyroxine, thyroid-stimulating hormone, and hypothyroid status and the risk of prostate cancer. PLoS One. 2012;7(10):e47730. doi:10.1371/journal.pone.0047730
6. L’Heureux A, Wieland DR, Weng C-H, et al. Association Between Thyroid Disorders and Colorectal Cancer Risk in Adult Patients in Taiwan. JAMA Network Open. 2019;2(5):e193755. doi:10.1001/jamanetworkopen.2019.3755
7. Vanderpump MPJ. The epidemiology of thyroid disease. Br Med Bull. 2011;99(1):39–51. doi:10.1093/bmb/ldr030
8. Silva JF, Ocarino NM, Serakides R. Thyroid hormones and female reproduction. Biol Reprod. 2018;99(5):907–921. doi:10.1093/biolre/ioy115
9. Quintino-Moro A, Zantut-Wittmann DE, Tambascia M, Machado HDC, Fernandes A. High Prevalence of Infertility among Women with Graves’ Disease and Hashimoto’s Thyroiditis. Int J Endocrinol. 2014;2014:1–6. doi:10.1155/2014/982705
10. Barr CE, Njoku K, Hotchkies L, et al. Does Clinical and Biochemical Thyroid Dysfunction Impact on Endometrial Cancer Survival Outcomes? A Prospective Database Study. Cancers. 2021;13(21):5444. doi:10.3390/cancers13215444
11. Gupta A, Sagar G, Siddiqui Z, et al. A non-invasive method for concurrent detection of early-stage women-specific cancers. Sci Rep. 2022;12(1):2301. doi:10.1038/s41598-022-06274-9
12. Anbarasu S, Anbarasu A. Cancer-biomarkers associated with sex hormone receptors and recent therapeutic advancements: a comprehensive review. Med Oncol. 2023;40(6):171. doi:10.1007/s12032-023-02044-3
13. Jiang D, Niu Z, Tan X, et al. The mortalities of female-specific cancers in China and other countries with distinct socioeconomic statuses: a longitudinal study. J Adv Res. 2023;49:127–139. doi:10.1016/j.jare.2022.09.002
14. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
15. Lheureux S, Braunstein M, Oza AM. Epithelial ovarian cancer: evolution of management in the era of precision medicine. CA Cancer J Clin. 2019;69(4):280–304. doi:10.3322/caac.21559
16. Emdin CA, Khera AV, Kathiresan S. Mendelian Randomization. JAMA. 2017;318(19):1925. doi:10.1001/jama.2017.17219
17. Burgess S, Scott RA, Timpson NJ, Davey Smith G, Thompson SG, EPIC- InterAct Consortium. Using published data in Mendelian randomization: a blueprint for efficient identification of causal risk factors. Eur J Epidemiol. 2015;30(7):543–552. doi:10.1007/s10654-015-0011-z
18. Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the Reporting of Observational Studies in Epidemiology Using Mendelian Randomization: the STROBE-MR Statement. JAMA. 2021;326(16):1614. doi:10.1001/jama.2021.18236
19. Loh P-R, Kichaev G, Gazal S, Schoech AP, Price AL. Mixed-model association for biobank-scale datasets. Nat Genet. 2018;50(7):906–908. doi:10.1038/s41588-018-0144-6
20. Dönertaş HM, Fabian DK, Fuentealba M, Partridge L, Thornton JM. Common genetic associations between age-related diseases. Nat Aging. 2021;1(4):400–412. doi:10.1038/s43587-021-00051-5
21. Teumer A, Chaker L, Groeneweg S, et al. Genome-wide analyses identify a role for SLC17A4 and AADAT in thyroid hormone regulation. Nat Commun. 2018;9(1):4455. doi:10.1038/s41467-018-06356-1
22. O’Mara TA, Glubb DM, Amant F, et al. Identification of nine new susceptibility loci for endometrial cancer. Nat Commun. 2018;9(1):3166. doi:10.1038/s41467-018-05427-7
23. Sakaue S, Kanai M, Tanigawa Y, et al. A cross-population atlas of genetic associations for 220 human phenotypes. Nat Genet. 2021;53(10):1415–1424. doi:10.1038/s41588-021-00931-x
24. Michailidou K, Lindström S, Dennis J, et al. Association analysis identifies 65 new breast cancer risk loci. Nature. 2017;551(7678):92–94. doi:10.1038/nature24284
25. Phelan CM, Kuchenbaecker KB, Tyrer JP, et al. Identification of 12 new susceptibility loci for different histotypes of epithelial ovarian cancer. Nat Genet. 2017;49(5):680–691. doi:10.1038/ng.3826
26. Hemani G, Zheng J, Elsworth B, et al. The MR-Base platform supports systematic causal inference across the human phenome. eLife. 2018;7:e34408. doi:10.7554/eLife.34408
27. The Endometrial Cancer Association Consortium, Ruth KS, Day FR, Tyrrell J, et al. Using human genetics to understand the disease impacts of testosterone in men and women. Nat Med. 2020;26(2):252–258. doi:10.1038/s41591-020-0751-5.
28. Verbanck M, Chen C-Y, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
29. Lin S-H, Brown DW, Machiela MJ. LDtrait: an Online Tool for Identifying Published Phenotype Associations in Linkage Disequilibrium. Cancer Res. 2020;80(16):3443–3446. doi:10.1158/0008-5472.CAN-20-0985
30. Schizophrenia Working Group of the Psychiatric Genomics Consortium, Bulik-Sullivan BK, Loh P-R, Finucane HK, et al. LD Score regression distinguishes confounding from polygenicity in genome-wide association studies. Nat Genet. 2015;47(3):291–295. doi:10.1038/ng.3211.
31. Choi HK, McCormick N, Lu N, Rai SK, Yokose C, Zhang Y. Population Impact Attributable to Modifiable Risk Factors for Hyperuricemia. Arthritis Rheumatol. 2020;72(1):157–165. doi:10.1002/art.41067
32. Nakamura K, Sakurai M, Miura K, et al. Alcohol intake and the risk of hyperuricaemia: a 6-year prospective study in Japanese men. Nutr Metab Cardiovasc Dis. 2012;22(11):989–996. doi:10.1016/j.numecd.2011.01.003
33. Fd GM, Minelli C, Sheehan NA, Thompson JR. Detecting pleiotropy in Mendelian randomisation studies with summary data and a continuous outcome. Stat Med. 2015;34(21):2926–2940. doi:10.1002/sim.6522
34. VanderWeele TJ. Mediation Analysis: a Practitioner’s Guide. Annu Rev Public Health. 2016;37(1):17–32. doi:10.1146/annurev-publhealth-032315-021402
35. MacKinnon DP, Fairchild AJ, Fritz MS. Mediation analysis. Annu Rev Psychol. 2007;58(1):593–614. doi:10.1146/annurev.psych.58.110405.085542
36. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent Estimation in Mendelian Randomization with Some Invalid Instruments Using a Weighted Median Estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
37. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–525. doi:10.1093/ije/dyv080
38. Burgess S, Bowden J, Fall T, Ingelsson E, Thompson SG. Sensitivity Analyses for Robust Causal Inference from Mendelian Randomization Analyses with Multiple Genetic Variants. Epidemiology. 2017;28(1):30–42. doi:10.1097/EDE.0000000000000559
39. Sanderson E, Spiller W, Bowden J. Testing and correcting for weak and pleiotropic instruments in two‐sample multivariable Mendelian randomization. Stat Med. 2021;40(25):5434–5452. doi:10.1002/sim.9133
40. Võsa U, Claringbould A, Westra H-J, et al. Large-scale cis- and trans-eQTL analyses identify thousands of genetic loci and polygenic scores that regulate blood gene expression. Nat Genet. 2021;53(9):1300–1310. doi:10.1038/s41588-021-00913-z
41. Masullo LF, Magalhães RA, Lemes RPG, et al. Levothyroxine Replacement Improves Oxidative Status in Primary Hypothyroidism. Front Endocrinol. 2018;9:655. doi:10.3389/fendo.2018.00655
42. Lin S, Huang S, Deng Z, et al. Discovery of a novel, liver-targeted thyroid hormone receptor-β agonist, CS271011, in the treatment of lipid metabolism disorders. Front Endocrinol. 2023;14:1109615. doi:10.3389/fendo.2023.1109615
43. Yu S, Zhou W, Cheng X, et al. Comparison of Six Automated Immunoassays With Isotope-Diluted Liquid Chromatography-Tandem Mass Spectrometry for Total Thyroxine Measurement. Ann Lab Med. 2019;39(4):381–387. doi:10.3343/alm.2019.39.4.381
44. Reddy VS, Bukke S, Mahato K, et al. A meta-analysis of the association of serum ischaemia-modified albumin levels with human hypothyroidism and hyperthyroidism. Biosci Rep. 2017;37(1):BSR20160268. doi:10.1042/BSR20160268
45. Åsvold BO, Vatten LJ, Bjøro T, et al. Thyroid function within the normal range and risk of coronary heart disease: an individual participant data analysis of 14 cohorts. JAMA Intern Med. 2015;175(6):1037. doi:10.1001/jamainternmed.2015.0930
46. Huang K, Su S, Wang X, et al. Association Between Maternal Thyroid Function in Early Pregnancy and Gestational Diabetes: a Prospective Cohort Study. J Clin Endocrinol Metab. 2024;109(2):e780–7. doi:10.1210/clinem/dgad518
47. Gauthier BR, Sola‐García A, Cáliz‐Molina MÁ, et al. Thyroid hormones in diabetes, cancer, and aging. Aging Cell. 2020;19(11):e13260. doi:10.1111/acel.13260
48. Davis PJ, Davis FB, Mousa SA, Luidens MK, Lin H-Y. Membrane receptor for thyroid hormone: physiologic and pharmacologic implications. Annu Rev Pharmacol Toxicol. 2011;51(1):99–115. doi:10.1146/annurev-pharmtox-010510-100512
49. Lin H, Su Y, Hsieh M, et al. Nuclear monomeric integrin αv in cancer cells is a coactivator regulated by thyroid hormone. FASEB J. 2013;27(8):3209–3216. doi:10.1096/fj.12-227132
50. Lin H-Y, Sun M, Tang H-Y, et al. Thyroxine vs. 3,5,3′-triiodo- l -thyronine and cell proliferation: activation of mitogen-activated protein kinase and phosphatidylinositol 3-kinase. Am J Physiol Cell. 2009;296(5):C980–91. doi:10.1152/ajpcell.00305.2008
51. Moeller LC, Führer D. Thyroid hormone, thyroid hormone receptors, and cancer: a clinical perspective. Endocr Relat Cancer. 2013;20(2):R19–29. doi:10.1530/ERC-12-0219
52. Cordeiro A, Souza LL, Einicker-Lamas M, Pazos-Moura CC. Non-classic thyroid hormone signalling involved in hepatic lipid metabolism. J Endocrinol. 2013;216(3):R47–57. doi:10.1530/JOE-12-0542
53. Khan SR, Chaker L, Ruiter R, et al. Thyroid Function and Cancer Risk: the Rotterdam Study. J Clin Endocrinol Metab. 2016;101(12):5030–5036. doi:10.1210/jc.2016-2104
54. Semenza G. HIF-1 inhibitors for cancer therapy: from gene expression to drug discovery. Curr Pharm Des. 2009;15(33):3839–3843. doi:10.2174/138161209789649402
55. Ventura-Holman T, Mamoon A, Subauste MC, Js S. The effect of oncoprotein v-erbA on thyroid hormone-regulated genes in hepatocytes and their potential role in hepatocellular carcinoma. Mol Biol Rep. 2011;38(2):1137–1144. doi:10.1007/s11033-010-0211-2
56. Lu L, Wan B, Li L, Sun M. Hypothyroidism has a protective causal association with hepatocellular carcinoma: a two-sample Mendelian randomization study. Front Endocrinol. 2022;13:987401. doi:10.3389/fendo.2022.987401
57. Yuan S, Kar S, Vithayathil M, et al. Causal associations of thyroid function and dysfunction with overall, breast and thyroid cancer: a two-sample Mendelian randomization study. Int, J, Cancer. 2020;147(7):1895–1903. doi:10.1002/ijc.32988
58. Zhang Q, Mu Y, Jiang X, Zhao Y, Wang Q, Shen Z. Causal relationship between thyroid dysfunction and gastric cancer: a two-sample Mendelian randomization study. Front Endocrinol. 2024;15:1335149. doi:10.3389/fendo.2024.1335149
59. Tosovic A, A-G B, Bondeson L, Ericsson U-B, Malm J, Manjer J. Prospectively measured triiodothyronine levels are positively associated with breast cancer risk in postmenopausal women. Breast Cancer Res. 2010;12(3):R33. doi:10.1186/bcr2587
60. Cornelli U, Belcaro G, Recchia M, Finco A. Levothyroxine and lung cancer in females: the importance of oxidative stress. Reprod Biol Endocrinol. 2013;11(1):75. doi:10.1186/1477-7827-11-75
61. Rostkowska O, Spychalski P, Dobrzycka M, et al. Effects of thyroid hormone imbalance on colorectal cancer carcinogenesis and risk - a systematic review. Endokrynol Pol. 2019;70(2):190–197. doi:10.5603/EP.a2019.0007
62. T-V-T T, Kitahara CM, De Vathaire F, Boutron-Ruault M-C, Journy N. Thyroid dysfunction and cancer incidence: a systematic review and meta-analysis. Endocr Relat Cancer. 2020;27(4):245–259. doi:10.1530/ERC-19-0417
63. Davis FB, Tang H-Y, Shih A, et al. Acting via a cell surface receptor, thyroid hormone is a growth factor for glioma cells. Cancer Res. 2006;66(14):7270–7275. doi:10.1158/0008-5472.CAN-05-4365
64. Hercbergs A, Johnson RE, Ashur-Fabian O, Garfield DH, Davis PJ. Medically induced euthyroid hypothyroxinemia may extend survival in compassionate need cancer patients: an observational study. Oncologist. 2015;20(1):72–76. doi:10.1634/theoncologist.2014-0308
65. Kinoshita S, Sone S, Yamashita T, Tsubura E, Ogura T. Effects of experimental hyper- and hypothyroidism on natural defense activities against Lewis lung carcinoma and its spontaneous pulmonary metastases in C57BL/6 mice. Tokushima J Exp Med. 1991;38(1–2):25–35.
66. Wang B, Lu Z, Huang Y, Li R, Lin T. Does hypothyroidism increase the risk of breast cancer: evidence from a meta-analysis. BMC Cancer. 2020;20(1):733. doi:10.1186/s12885-020-07230-4
67. Zhang T, Qiao J, Wang Y, et al. Causal link between hypothyroidism and gastric cancer risk: insights gained through multivariable Mendelian randomization and mediation analysis. Front Endocrinol. 2024;15:1388608. doi:10.3389/fendo.2024.1388608
68. Wawrzkiewicz-Jałowiecka A, Lalik A, Soveral G. Recent Update on the Molecular Mechanisms of Gonadal Steroids Action in Adipose Tissue. Int J Mol Sci. 2021;22(10):5226. doi:10.3390/ijms22105226
69. Zych M, Kaczmarczyk-Sedlak I, Wojnar W, Folwarczna J. The Effects of Sinapic Acid on the Development of Metabolic Disorders Induced by Estrogen Deficiency in Rats. Oxid Med Cell Longev. 2018;2018:9274246. doi:10.1155/2018/9274246
70. Elgueta-Reyes M, Velásquez VB, Espinosa P, et al. Effects of Early Life Exposure to Sex Hormones on Neurochemical and Behavioral Responses to Psychostimulants in Adulthood: implications in Drug Addiction. Int J Mol Sci. 2022;23(12):6575. doi:10.3390/ijms23126575
71. Peluso JJ, Pru JK. Progesterone Receptor Membrane Component (PGRMC)1 and PGRMC2 and Their Roles in Ovarian and Endometrial Cancer. Cancers. 2021;13(23):5953. doi:10.3390/cancers13235953
72. Mizushima T, Miyamoto H. The Role of Androgen Receptor Signaling in Ovarian Cancer. Cells. 2019;8(2):176. doi:10.3390/cells8020176
73. Higa GM, Fell RG. Sex hormone receptor repertoire in breast cancer. Int J Breast Cancer. 2013;2013:1–14. doi:10.1155/2013/284036
74. The Endogenous Hormones And Breast Cancer Collaborative Group. Endogenous sex hormones and breast cancer in postmenopausal women: reanalysis of nine prospective studies. Cancer Spectr Knowl Environ. 2002;94:606–616.
75. Liu Z, Zhang Y, Lagergren J, et al. Circulating Sex Hormone Levels and Risk of Gastrointestinal Cancer: systematic Review and Meta-Analysis of Prospective Studies. Cancer Epidemiol Biomark Prev. 2023;32(7):936–946. doi:10.1158/1055-9965.EPI-23-0039
76. E Hormones. Steroid hormone measurements from different types of assays in relation to body mass index and breast cancer risk in postmenopausal women: reanalysis of eighteen prospective studies. Steroids. 2015;99:49–55. doi:10.1016/j.steroids.2014.09.001
77. Zhang Y, Huang X, Yu X, He W, Czene K, Yang H. Hematological and biochemical markers influencing breast cancer risk and mortality: prospective cohort study in the UK Biobank by multi-state models. Breast. 2024;73:103603. doi:10.1016/j.breast.2023.103603
78. Mullee A, Dimou N, Allen N, O’Mara T, Gunter MJ, Murphy N. Testosterone, sex hormone-binding globulin, insulin-like growth factor-1 and endometrial cancer risk: observational and Mendelian randomization analyses. Br J Cancer. 2021;125(9):1308–1317. doi:10.1038/s41416-021-01518-3
79. Shu J, Xing L, Zhang L, Fang S, Huang H. Ignored adult primary hypothyroidism presenting chiefly with persistent ovarian cysts: a need for increased awareness. Reprod Biol Endocrinol. 2011;9(1):119. doi:10.1186/1477-7827-9-119
80. Bernardo TJ, Dubrovskaya VA, Xie X, Dubrovsky EB. A view through a chromatin loop: insights into the ecdysone activation of early genes in Drosophila. Nucleic Acids Res. 2014;42(16):10409–10424. doi:10.1093/nar/gku754
81. Duarte-Guterman P, Langlois VS, Pauli BD, Trudeau VL. Expression and T3 regulation of thyroid hormone- and sex steroid-related genes during Silurana (Xenopus) tropicalis early development. Gen Comp Endocrinol. 2010;166(2):428–435. doi:10.1016/j.ygcen.2009.12.008
82. MacLean HE, Warne GL, Zajac JD. Localization of functional domains in the androgen receptor. J Steroid Biochem Mol Biol. 1997;62(4):233–242. doi:10.1016/S0960-0760(97)00049-6
83. Brown EDL, Obeng-Gyasi B, Hall JE, Shekhar S. The Thyroid Hormone Axis and Female Reproduction. Int J Mol Sci. 2023;24(12):9815. doi:10.3390/ijms24129815
84. Howe CG, Eckel SP, Habre R, et al. Association of Prenatal Exposure to Ambient and Traffic-Related Air Pollution With Newborn Thyroid Function: findings From the Children’s Health Study. JAMA Network Open. 2018;1(5):e182172. doi:10.1001/jamanetworkopen.2018.2172
85. Fonseca TL, Correa-Medina M, Campos MPO, et al. Coordination of hypothalamic and pituitary T3 production regulates TSH expression. J Clin Invest. 2013;123(4):1492–1500. doi:10.1172/JCI61231
86. Veronelli A, Masu A, Ranieri R, Rognoni C, Laneri M, Pontiroli AE. Prevalence of erectile dysfunction in thyroid disorders: comparison with control subjects and with obese and diabetic patients. Int J Impot Res. 2006;18(1):111–114. doi:10.1038/sj.ijir.3901364
87. Tagawa N, Takano T, Fukata S, et al. Serum concentration of androstenediol and androstenediol sulfate in patients with hyperthyroidism and hypothyroidism. Endocr J. 2001;48(3):345–354. doi:10.1507/endocrj.48.345
88. Shepherd R, Kim B, Saffery R, Novakovic B. Triiodothyronine (T3) Induces Limited Transcriptional and DNA Methylation Reprogramming in Human Monocytes. Biomedicines. 2022;10(3):608. doi:10.3390/biomedicines10030608
89. Lyu Y, Xiu Q, Zuo H, et al. Effect of vitamin A on the relationship between maternal thyroid hormones in early pregnancy and fetal growth: a prospective cohort study. Front Nutr. 2022;9:980853. doi:10.3389/fnut.2022.980853
90. Y-CSH Y, Ko P-J, Pan Y-S, et al. Role of thyroid hormone-integrin αvβ3-signal and therapeutic strategies in colorectal cancers. J Biomed Sci. 2021;28(1):24. doi:10.1186/s12929-021-00719-5
91. Siersbæk R, Kumar S, Carroll JS. Signaling pathways and steroid receptors modulating estrogen receptor α function in breast cancer. Genes Dev. 2018;32(17–18):1141–1154. doi:10.1101/gad.316646.118
92. Zhang Y, Zheng D, Zhou T, et al. Androgen deprivation promotes neuroendocrine differentiation and angiogenesis through CREB-EZH2-TSP1 pathway in prostate cancers. Nat Commun. 2018;9(1):4080. doi:10.1038/s41467-018-06177-2
93. Ulm M, Ramesh AV, McNamara KM, Ponnusamy S, Sasano H, Narayanan R. Therapeutic advances in hormone-dependent cancers: focus on prostate, breast and ovarian cancers. Endocr Connect. 2019;8(2):R10–26. doi:10.1530/EC-18-0425
94. Ghoochani A, Hsu E-C, Aslan M, et al. Ferroptosis Inducers Are a Novel Therapeutic Approach for Advanced Prostate Cancer. Cancer Res. 2021;81(6):1583–1594. doi:10.1158/0008-5472.CAN-20-3477
95. Xiao Q, Wang L, Supekar S, et al. Structure of human steroid 5α-reductase 2 with the anti-androgen drug finasteride. Nat Commun. 2020;11(1):5430. doi:10.1038/s41467-020-19249-z
96. Kono M, Fujii T, Lim B, Karuturi MS, Tripathy D, Ueno NT. Androgen Receptor Function and Androgen Receptor-Targeted Therapies in Breast Cancer: a Review. JAMA Oncol. 2017;3(9):1266. doi:10.1001/jamaoncol.2016.4975
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Roles of Inflammation- and Nutrition-Based Indicators for Female Patients with Cancer
Yang M, Zhang Q, Ge Y, Tang M, Hu C, Wang Z, Zhang X, Song M, Ruan G, Zhang X, Liu T, Xie H, Zhang H, Zhang K, Li Q, Li X, Liu X, Lin S, Shi H
Journal of Inflammation Research 2022, 15:3573-3586
Published Date: 17 June 2022
Gastroesophageal Reflux Disease and Preterm Birth: Univariate and Multivariate Mendelian Randomization
Han X, Wu TQ, Yao R, Liu C, Chen L, Feng X
International Journal of Women's Health 2024, 16:1389-1399
Published Date: 13 August 2024
From Phenotype to Molecules: Unveiling the Genetic and Immunological Bridges Between Autoimmune Diseases and Vitiligo
Hu Y, Wang SB, Wang K, He MJ
Clinical, Cosmetic and Investigational Dermatology 2024, 17:2475-2486
Published Date: 4 November 2024
Exploring the Causal Relationship Between Frailty and Chronic Obstructive Pulmonary Disease: Insights From Bidirectional Mendelian Randomization and Mediation Analysis
Cheng Z, Wu J, Xu C, Yan X
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:193-205
Published Date: 25 January 2025
Celiac Disease and Skin Diseases: A Bidirectional Mendelian Randomization Study
Ge C, Wang Y, Zhao X, Hao J, Zhang J, Lu M, Li C, Feng J, Zhang Q
Clinical, Cosmetic and Investigational Dermatology 2025, 18:1757-1768
Published Date: 22 July 2025