Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Case Report: Vitiligo and Alopecia Universalis Following Rituximab Therapy in a Patient with Myasthenia Gravis
Authors Alzahrani D, Niaz G, Roblah TM ![]() , Al-Osaimi AK, Alsulaimani H
, Al-Osaimi AK, Alsulaimani H ![]()
Received 3 January 2026
Accepted for publication 4 March 2026
Published 16 March 2026 Volume 2026:19 584164
DOI https://doi.org/10.2147/CCID.S584164
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michela Starace
Dhaii Alzahrani,1 Ghassan Niaz,2 Tala Musa Roblah,3 Ashwaq Kh Al-Osaimi,4 Hadeel Alsulaimani3
1College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 2Department of Dermatology, King Faisal Specialist Hospital and Research Centre, Jeddah, Saudi Arabia; 3Department of Dermatology, King Fahad General Hospital, Jeddah, Saudi Arabia; 4Department of Dermatology, Makkah Health Cluster, Makkah, Saudi Arabia
Correspondence: Dhaii Alzahrani, College of Medicine – Jeddah, King Saud bin Abdulaziz University for Health Sciences, P.O.Box.9515, Jeddah, 21423, Saudi Arabia, Email [email protected]
Abstract: Rituximab, an anti-CD20 monoclonal antibody, is being used more frequently to treat refractory autoimmune disorders such as myasthenia gravis. While it is usually well tolerated, rare cases of paradoxical immune-mediated skin reactions have been rarely reported. However, the concurrent development of vitiligo and alopecia universalis following rituximab therapy has not been previously described. We report a rare case of simultaneous vitiligo and alopecia universalis developing during long-term treatment with rituximab in a patient with myasthenia gravis and discuss the clinical course and treatment response. This case report describes a 30-year-old woman with myasthenia gravis who developed vitiligo followed by alopecia universalis during a long term of Rituximab therapy. Cutaneous findings included well-demarcated depigmented patches on the trunks and bilateral arms and diffuse non-scarring alopecia affecting the scalp, eyebrows, eyelashes, and body hair, consistent with 100% score of Severity of Alopecia tool (SALT) indicating Alopecia universalis. Rituximab was discontinued due to a possible drug-reaction. Treatment with oral Baricitinib was initiated to target both vitiligo and alopecia universalis. Within three months, there was significant scalp hair regrowth and re-pigmentation of vitiligo patches with minimal adverse effects. This case highlights a unique temporal association of rituximab therapy and the simultaneous onset of vitiligo and alopecia universalis. Although the relationship between the drug and the onset of the skin diseases cannot be established, it is important to be aware of the possibility of immune-related skin adverse effects during rituximab therapy. Early intervention and the use of Janus kinase inhibitors, such as baricitinib, may lead to good clinical outcomes.
Keywords: case report, vitiligo, alopecia universalis, baricitinib, rituximab
Introduction
Rituximab (RTX), a chimeric monoclonal antibody that targets the CD20 antigen on B lymphocytes, is widely used to treat hematologic malignancies and autoimmune disorders.1 Its off-label use has also increased in recent years for refractory neurological conditions, including myasthenia gravis(MG).1 Although RTX is generally well tolerated, rare cases of immune dysregulation due to B-cell depletion have resulted in paradoxical autoimmune events.2 Cutaneous side effects are uncommon and are usually limited to infusion related reactions or complications from infections.1 Autoimmune skin disorders such as vitiligo and alopecia areata have rarely been reported following RTX therapy. Vitiligo and alopecia areata (AA) are major health issues worldwide. Vitiligo affects 0.5% to 2% of the world’s population, while AA has a global prevalence rate close to 2%.3,4 The progression to AU, which is the most severe form of AA, is a significant clinical challenge. This condition often comes with various autoimmune diseases.5 The new trend in the literature suggests that RTX-induced loss of Breg cells leads to a Th1-skewed immune environment, which may trigger various T-cell-mediated diseases like vitiligo and AU.6,7 To the best of our knowledge, this case of simultaneous occurrence of vitiligo and AU in a patient undergoing RTX treatment for MG is unprecedented. This case report aims to highlight the novelty of this case by focusing on the simultaneous occurrence of two paradoxical reactions and their treatment with baricitinib.
Case Presentation
A 30-year-old female, a known case MG (diagnosed in 2013) based on positive acetylcholine receptor antibodies and confirmatory nerve conduction studies, presented to the dermatology clinic in November 2023 with complaints of newly developed, well-demarcated depigmented patches on the trunk and bilateral arms (Figure 1). The patient reported noticing these depigmented patches after receiving her third dose of intravenous RTX. She had previously failed multiple treatment regimens of azathioprine, pyridostigmine, tacrolimus, methotrexate, corticosteroids, and multiple sessions of intravenous immunoglobulin (IVIG). Her first dose of rituximab was administered as a loading dose of 1000 mg IV in 2021, followed by maintenance infusions of 1000 mg every six months. After the first dose, she reported significant improvement in neurological symptoms.
 |
Figure 1 Multiple well-demarcated depigmented patches on the trunk and lateral side of the left breast. |
On the other hand, she was diagnosed clinically with vitiligo. Topical tacrolimus (on weekdays) and mometasone ointment (on weekends) were prescribed, and she was initiated on phototherapy sessions. In December 2024, following her 8th dose of rituximab infusion, the patient developed diffuse sudden hair loss involving the entire scalp and body. On examination, there were confluent non-scarring alopecic patches affecting the scalp regions, with SALT score of 100%, indicating alopecia universalis. Generalized hair loss was also noted on the body, including eyebrows and eyelashes, along with mild nail pitting. A scalp biopsy was not performed due to classic clinical findings consistent with alopecia universalis. As a result, RTX therapy was discontinued out of concern for a potential adverse reaction to the drug. Surprisingly, the vitiligo progression has stopped since the discontinuation of RTX.
The myasthenia gravis condition of the patient was stable after the discontinuation of the rituximab treatment. This was ensured by the continued symptomatic management of the condition with pyridostigmine and neurological monitoring. The discontinuation of RTX was based on the weighing of the possible risk of relapse of MG against the severity and psychological effects of the adverse dermatological effects. This was because the condition of the patient was stable before the adverse effects appeared. Although various options for the management of MG in the long term were considered, the focus was on managing the adverse effects that appeared.
Despite ongoing phototherapy and topical treatments, the patient reported no improvement in vitiligo, which significantly affected her psycho-social life; therefore, we referred her to the psychiatry clinic. Upon psychiatric evaluation, our patient was diagnosed with severe depression and started on oral paroxetine 25mg daily. During a follow-up visit, initiation of oral Baricitinib was planned and the patient was counselled about the risks, benefits, and monitoring requirements. Baseline laboratory investigations, including complete blood count, hepatic, renal, and lipid profiles, as well as serology, were obtained before starting treatment.
Treatment was initiated in July 2025 with oral Baricitinib 2 mg daily. In September 2025, a follow-up examination revealed clinical improvement in both conditions: new whitish hair growth in the occipital scalp region and re-pigmentation in two patches on the right arm (Figure 2). The patient reported no adverse effects and repeat laboratory results were unremarkable.
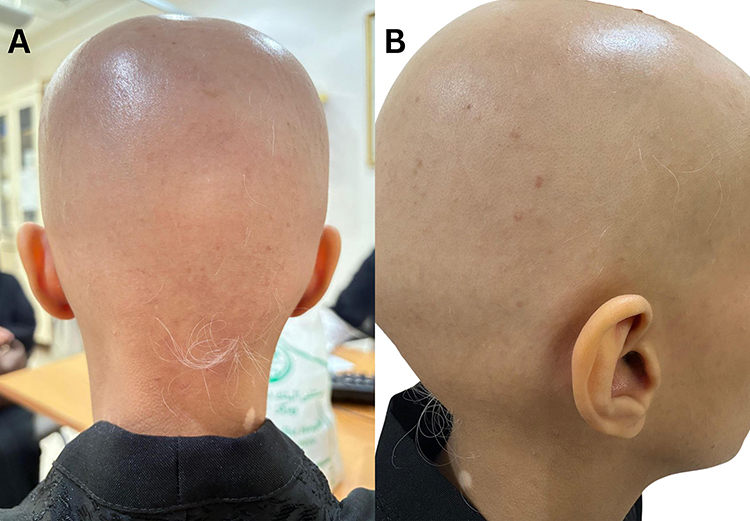 |
Figure 2 (A) Whitish hair growth in the occipital part of the scalp. (B) Whitish hair growth in the parietal parts of the scalp after 3 months of oral Baricitinib. |
The baricitinib dose was subsequently increased to 4 mg daily. By October 2025, the patient demonstrated diffuse follicular hair regrowth over the scalp and eyebrows and improvement in previously depigmented patches on the trunk (Figure 3). Our patient reported acne on the face while remaining adherent to the treatment regimen; adapalene/benzoyl peroxide was prescribed to address the acne.
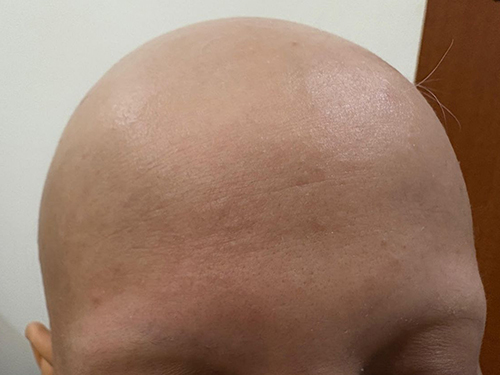 |
Figure 3 Follicular growth (black hair) in both eyebrows after 3 months of oral baricitinib. |
By January 2026, following six months of Baricitinib therapy, our patient demonstrated a partial regrowth of eyebrows and eyelashes, both of which had previously been absent (Figure 4). Additionally, the scalp also showed a moderate growth of pigmented blackish hair (Figure 5).
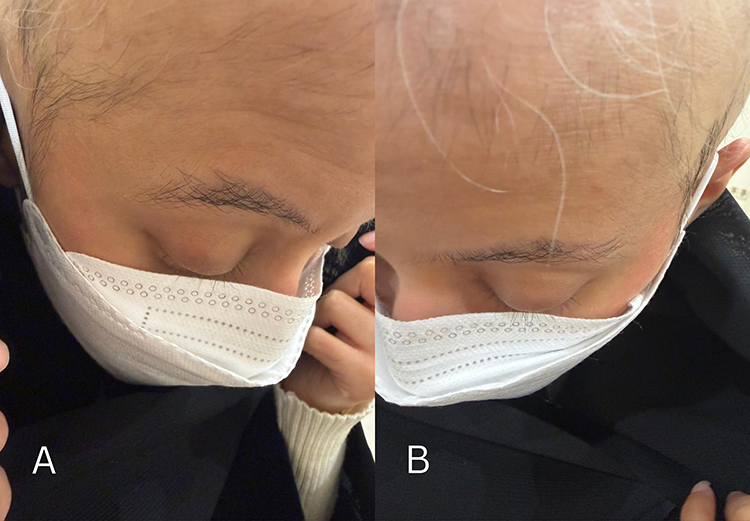 |
Figure 4 (A) Periocular view after 6 months of oral baricitinib showing eyebrow and partial upper eyelash regrowth, with early frontal scalp hair return. (B) Frontal scalp after 6 months of oral baricitinib demonstrating sparse vellus hair regrowth. |
 |
Figure 5 (A) Lateral scalp view showing minimal hair regrowth with sparse fine hairs after 6 months of oral baricitinib therapy. (B) Posterior scalp view showing sparse short, pigmented hair regrowth within the occipital region after 6 months of oral baricitinib therapy. |
Discussion
This report presents a clinical observation rather than proving a direct causal link between RTX therapy and the onset of vitiligo and alopecia universalis. Nevertheless, the timing and progression of symptoms highlight important issues concerning immune dysregulation after prolonged B-cell depletion. RTX causes broad depletion of B lymphocytes, including regulatory subsets that help maintain immune tolerance by secreting interleukin-10 and transforming growth factor-β.8 The absence of these regulatory B cells can lead to unchecked cytotoxic T-cell activity and a shift toward a Th1-dominant immune response.9 Vitiligo and alopecia universalis are both primarily T cell driven autoimmune diseases, marked by increased interferon-γ production and activation of the JAK–STAT pathway.10 There have been reports of delayed autoimmune reactions following RTX use, which may be linked to abnormal immune recovery during B cell repopulation, enabling the growth of autoreactive lymphocyte clones.6 In patients predisposed to autoimmunity, such immune disturbances might encourage epitope spreading and the development of new autoimmune symptoms.6
While direct causality in individual cases is difficult to establish, the proposed rationale for the observed paradoxical immune-mediated events is based on the significant immunomodulatory potential of rituximab (RTX). RTX-mediated depletion of CD20+ B cells not only targets pathogenic B cells but also regulatory B cells that play an essential role in the maintenance of immune tolerance. The absence or depletion of regulatory B cells could lead to an imbalance in the immune response that favors unchecked cytotoxic T-cell activity and an increased risk of a Th1-dominant immune response. Vitiligo and alopecia universalis are well-documented T-cell-mediated autoimmune diseases characterized by increased interferon gamma production and JAK/STAT pathway activation. Thus, we propose that RTX-mediated B-cell depletion, particularly regulatory B cells, may uncover an underlying risk of T-cell-mediated autoimmune diseases that ultimately manifests as vitiligo and alopecia universalis in our patient. Such a rationale is supported by reports of delayed autoimmune events in response to RTX treatment, often with abnormal immune reconstitution during B-cell repopulation that favors the outgrowth of autoreactive lymphocyte clones.
RTX has Food and Drug administration (FDA) for several hematological malignancies and autoimmune disorders such as Chronic lymphocytic leukemia, Rheumatoid arthritis, Microscopic polyangiitis, Granulomatosis with polyangiitis, and Pemphigus vulgaris.1 Based on the literature review, various adverse effects of RTX have been documented; these include acute respiratory distress syndrome, bronchiolitis obliterans, hypersensitivity pneumonitis, and diffuse alveolar hemorrhage, and Acute tumor lysis syndrome.11 To our knowledge, there was only one reported case in 2022 of a 55-year-old woman who was diagnosed with alopecia universalis a few months after successfully receiving RTX for bullous pemphigoid.2 In contrast, our patient received RTX as treatment for her MG, with a good response in terms of neurological symptoms. Notably, she exhibited sudden depigmented patches primarily over her trunk, followed by progressive severe hair loss and ultimately generalized hair loss affecting her scalp, eyebrows, and eyelashes. Similarly, our patient experienced the same pattern after cessation of RTX, which suggests a possible association between RTX treatment and the onset of hair loss and depigmentation. Nevertheless, the precise mechanism of this association remains unclear, a deeper understanding of the pathophysiology of alopecia universalis and vitiligo may elucidate and offer further insights into potential treatment alternatives.2
The importance of this particular case stems from its position as the first reported case of coexisting vitiligo and AU in the context of RTX treatment for MG, thus establishing an association between B-cell depletion therapies and the subsequent development of T-cell-mediated autoimmune skin diseases. Although previous reviews have focused on the paradoxical response in individual diseases, the present study outlines a broader spectrum of immune alterations that could be interpreted as an indication that prolonged B-cell depletion reduces the threshold for the concurrent development of various autoimmune manifestations. The findings have significant implications in terms of their potential to influence the practice of dermatological surveillance in the context of prolonged treatment with RTX in neurological diseases.
On the other hand, the positive response to Baricitinib in this case supports the involvement of JAK-STAT mediated inflammatory processes.12 Baricitinib inhibits Janus kinase 1 (JAK1) and Janus kinase 2 (JAK2), thereby reducing interferon-γ mediated immune responses involved in both melanocyte destruction and loss of immune privilege in hair follicles.12 While a causal relationship cannot be confirmed, this case suggests that JAK inhibitors may have therapeutic value in similar immune mediated skin conditions.12 In general, baricitinib is a safe and well-tolerated medication, and its effectiveness has been demonstrated in clinical trials for several off-label uses, including atopic dermatitis, psoriatic arthritis, and vitiligo.8 Therefore, Baricitinib was our preferred treatment of choice for targeting both vitiligo and alopecia universalis. Baricitinib showed good improvement in both conditions within a short time, and no major adverse effects were reported except acne, which was treated by topical treatment. This case report highlights a unique clinical observation that has not been previously described in the literature. As our case appears to be the first documented report of both conditions arising concurrently in the same patient following RTX treatment.
While the clinical efficacy of JAK inhibitors is well substantiated, there are a number of hurdles that impede their translation to real-world practice. The high cost of JAK inhibitors is one major hurdle that often limits treatment in patients without comprehensive insurance or in resource-constrained environments.13 In addition to this, regulatory hurdles in the off-label prescription of baricitinib in the treatment of coexisting autoimmune diseases are another potential hurdle that could affect treatment practices in real-world environments.14 The challenge of ensuring batch-to-batch consistency and safety in real-world environments, where patients have complex comorbid diseases like myasthenia gravis, is one major hurdle in translating JAK inhibitor treatment from a clinical trial environment to real-world practice.15 Regardless of the valuable insights provided in our case, there are several limitations. First, lack of histopathological confirmation and immunological tests makes it challenging to interpret the underlying mechanisms. Moreover, we cannot definitively attribute these findings to RTX, as the development of vitiligo and alopecia universalis may represent coincidental autoimmune comorbidities rather than a direct drug-induced effect. Second, off-label use of baricitinib can hinder the findings’ generalizability because the outcomes of a single case might not apply to larger patient populations. Third, literature comparison was limited due to the rarity of the coexistence of these conditions, comparison with similar published cases was insufficient. Finally, although a temporal relationship was observed, a direct causal link cannot be confirmed. To overcome these limitations, it is proposed that future studies should focus on the discovery of predictive biomarkers, eg, B cells and T cells, which may help identify patients at increased risk for developing a paradoxical reaction before starting RTX therapy. In addition, prospective registries to record dermatological outcomes in patients undergoing long term B-cell depletion therapy should be conducted to establish the incidence rates.16
Conclusion
In conclusion, the present case report presents a unique and significant immune-mediated cutaneous manifestation, the co-occurrence of vitiligo and alopecia universalis, which appears to be temporally associated with the administration of rituximab (RTX) for myasthenia gravis. The present findings suggest a possible link between RTX-mediated B-cell depletion and the development or exacerbation of T-cell-mediated autoimmune diseases. Notably, the present case shows the effective control of these unusual autoimmune reactions using the oral JAK inhibitor baricitinib, which resulted in significant hair growth and re-pigmentation within a short period. This shows the therapeutic efficacy of JAK inhibitors in the management of complex immune-mediated diseases. High levels of vigilance should be exercised to identify these unusual cutaneous side effects of RTX, as these reactions are significant from the point of view of the impact on the physical and mental health of the patient.
Limitations and Future Perspectives
Despite the valuable insights provided in this case report, there are certain limitations that need to be taken into consideration. One such limitation relates to the lack of histopathological and immunological investigations, which affects the understanding of the underlying pathophysiological mechanisms in the patient’s condition. Although there was a temporal association, the exact aetiopathogenic association between the administration of rituximab (RTX) and the development of vitiligo and alopecia universalis was not established, as these conditions may be considered to be “coincidental” autoimmune disorders. Another limitation relates to the off-label use of baricitinib in the patient, which may not be applicable to other patients. In addition, the rare association of vitiligo and alopecia universalis following the administration of RTX made it difficult to compare the results with the literature. To move the field forward, it is essential to have a well-defined research roadmap. The emphasis of the research should be on investigations that seek to identify predictive biomarkers that could potentially forewarn an increased risk of paradoxical autoimmune events before the initiation of RTX treatment. Another essential aspect will be the development of prospective registries to systematically monitor dermatological outcomes in patients receiving prolonged B-cell depletion treatment. Such an effort will be instrumental in providing the necessary data to accurately establish the incidence rates of these intricate immune-mediated AERs. Ongoing research to understand the exact role of B-cell depletion in modulating T-cell-mediated autoimmune events will be instrumental in the development of targeted interventions to address these events.
Ethical Statement
Written informed consent was obtained from the participant for participation in this study and for the publication of any potentially identifiable images or data included in this case report. In accordance with the policy of King Faisal Specialist Hospital and Research Centre, ethics committee approval was not required for this single anonymized case report, and no institutional approval was necessary for publication of the case details.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hanif N, Anwer F. Rituximab. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
2. Puiu T, Reimer D, Sokumbi O. Rituximab-induced alopecia universalis in a patient with bullous pemphigoid. J Drugs Dermatol. 2022;21(8):894–8. doi:10.36849/JDD.6690
3. Lu H, Li J, Ma K, et al. Regional, and national burden of alopecia areata in children and adolescents aged 0-19 years from 1990 to 2021 and projection to 2040. Clin Cosmet Investig Dermatol. 2026;19:582775. doi:10.2147/CCID.S582775
4. Gandhi K, Ezzedine K, Anastassopoulos KP, et al. Prevalence of vitiligo among adults in the United States. JAMA Dermatol. 2022;158(1):43–50. PMID: 34787670; PMCID: PMC8600454. doi:10.1001/jamadermatol.2021.4724
5. Mostaghimi A, Gao W, Ray M, et al. Trends in prevalence and incidence of alopecia areata, alopecia totalis, and alopecia universalis among adults and children in a US employer-sponsored insured population. JAMA Dermatol. 2023;159(4):411–418. PMID: 36857069; PMCID: PMC9979012. doi:10.1001/jamadermatol.2023.0002
6. Kersh AE, Feldman RJ. Autoimmune sequelae following rituximab therapy: a review of the literature and potential immunologic mechanisms. J Clin Rheumatol. 2018;24(8):427–435. PMID: 29561469. doi:10.1097/RHU.0000000000000756
7. Shao X, Chen T, Pan X, Chen S, Chen Y, Chen J. Biologic drugs induced vitiligo: case reports and review of literature. Front. Immunol. 2024;15:1455050. doi:10.3389/fimmu.2024.1455050
8. Bergantini L, d’Alessandro M, Cameli P, et al. Effects of rituximab therapy on B cell differentiation and depletion. Clin Rheumatol. 2020;39(5):1415–1421. doi:10.1007/s10067-020-04996-7
9. Björnsson GS, Sigurgrímsdóttir H, Maggadóttir SM, et al. Long-term use of rituximab increases T cell count in MS patients. Front Immunol. 2024;15:1412668. doi:10.3389/fimmu.2024.1412668
10. Yamaguchi HL, Yamaguchi Y, Peeva E. Pathogenesis of alopecia areata and vitiligo: commonalities and differences. Int J Mol Sci. 2024;25(8):4409. doi:10.3390/ijms25084409
11. Kasi PM, Tawbi HA, Oddis CV, Kulkarni HS. Clinical review: serious adverse events associated with the use of rituximab—a critical care perspective. Crit Care. 2012;16(4):231. doi:10.1186/cc11304
12. Ahmad A, Zaheer M, Balis FJ. Baricitinib. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
13. Dayem HA, Al Hammadi A, Reda A, et al. The burden of alopecia areata and management with baricitinib in the united arab emirates: a narrative review. Dermatol Ther. 2025;15(12):3463–3477. PMID: 41023528; PMCID: PMC12619884. doi:10.1007/s13555-025-01546-4
14. Needle CD, Brinks AL, Anyanwu N, et al. Investigating barriers to systemic Janus kinase inhibitor access for alopecia areata. J Am Acad Dermatol. 2026;94(2):613–615. PMID: 41061990. doi:10.1016/j.jaad.2025.10.006
15. Damsky W, King BA. JAK inhibitors in dermatology: the promise of a new drug class. J Am Acad Dermatol. 2017;76(4):736–744. PMID: 28139263; PMCID: PMC6035868. doi:10.1016/j.jaad.2016.12.005
16. Sahraian MA, Emami S, Ataei S, Nasr Esfahani F, Ghalandari N. Secondary autoimmune dermatological disorders induced by multiple sclerosis biological immunotherapy agents: a systematic review of case reports. Iran J Pharm Res. 2025;24(1):e166426. Erratum in: Iran J Pharm Res. 2025 Dec 28;24(1)e169319. doi: 10.5812/ijpr-169319. PMID: 41477116; PMCID: PMC12749207. doi:10.5812/ijpr-166426
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Excellent Repigmentation of Generalized Vitiligo with Oral Baricitinib Combined with NB-UVB Phototherapy
Li X, Sun Y, Du J, Wang F, Ding X
Clinical, Cosmetic and Investigational Dermatology 2023, 16:635-638
Published Date: 11 March 2023
Psoriasis on Lesions of Vitiligo: A Case Report
Wang L, Zhang B
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2005-2007
Published Date: 4 August 2023
Successful Treatment of Refractory Synovitis, Acne, Pustulosis, Hyperostosis, and Osteitis (SAPHO) Syndrome with Baricitinib, a Janus Kinase Inhibitor
Yang J, Yuan C, Zhou S, Teng Z, Li M
Clinical, Cosmetic and Investigational Dermatology 2024, 17:529-537
Published Date: 4 March 2024
Baricitinib Combination Therapy Demonstrates Significant Improvement in Cardiac Conduction Defects in Rapidly Progressive Systemic Sclerosis: A Case Report
Su X, Wu H, Li H, Li J, Qiao J, Li Y, Huang X, Wang L, Zeng S, Zhu L
Open Access Rheumatology: Research and Reviews 2025, 17:185-191
Published Date: 31 August 2025